Submitted:
03 February 2026
Posted:
05 February 2026
You are already at the latest version
Abstract
Diabetes mellitus (DM) is a globally prevalent metabolic disorder affecting both pediatric and adult populations, characterized by chronic hyperglycaemia due to impaired insulin secretion, insulin resistance, or both. The rising incidence of both Type 1 Diabetes Mellitus (T1DM) in children and adolescents, and Type 2 Diabetes Mellitus (T2DM) in youth and adults, reflects complex interactions between genetic, immunological, environmental, and lifestyle factors. This review highlights recent advances in the diagnosis and management of diabetes across the lifespan, with a specific focus on pharmacological strategies particularly insulin therapy and dietary interventions. In pediatric T1DM, innovations in insulin delivery systems, including continuous subcutaneous insulin infusion and hybrid closed-loop technologies, have improved glycaemic control and quality of life. Meanwhile, in both youth-onset and adult T2DM, early and aggressive interventions integrating lifestyle changes, oral antidiabetic agents (e.g., metformin, SGLT2 inhibitors, GLP-1 receptor agonists), and timely insulin initiation are essential for mitigating complications. Dietary modifications and structured physical activity remain foundational to diabetes prevention and treatment, offering cardio metabolic benefits that transcend glycaemic regulation. The review also explores the growing role of continuous glucose monitoring, automated insulin delivery, and emerging drug delivery platforms in transforming diabetes care. Special attention is given to psychosocial factors, the transitional challenges from pediatric to adult care, and future directions in immunotherapy, stem cell research, and nanotechnology-based therapeutics. Together, these advances underscore the shift toward precision, technology-enabled, and patient-centered diabetes management across all age groups.
Keywords:
diabetes mellitus
; type 1 diabetes
; type 2 diabetes
; pediatric diabetes
; insulin therapy
; dietary intervention
; non-insulin drugs
; continuous glucose monitoring
; life-style modification
; emerging therapies
1. Introduction
Diabetes mellitus is a long-term, non-communicable condition defined by chronic hyperglycaemia, resulting from impaired insulin secretion, defective insulin action, or a combination of both. This disease has become an escalating global health concern, currently affecting over 500 million individuals worldwide [1]. If left unmanaged, diabetes can lead to significant long-term complications. Its epidemiological profile varies markedly by age, with unique patterns seen in children, adolescents, and adults. Type 1 diabetes mellitus (T1DM) is more prevalent among children and adolescents, whereas Type 2 diabetes mellitus (T2DM), historically an adult-onset condition, is increasingly diagnosed in younger populations. These shifts highlight the influence of changing demographics, environmental exposures, and lifestyle factors, necessitating age-specific public health strategies and clinical responses [2,3].
In pediatric populations, T1DM remains the predominant form of diabetes. The incidence of T1DM is rising steadily worldwide, particularly in Europe and North America, where longitudinal data indicate a 2–5% annual increase in cases among individuals under 20 years of age [4]. T1DM results from autoimmune destruction of the pancreatic beta cells responsible for insulin production. Although genetic predisposition contributes to risk, environmental factors such as viral infections, early dietary exposures, and microbiome alterations are also believed to trigger disease onset. Despite its lower overall prevalence compared to T2DM, the intensive self-management required for T1DM and the potential for acute complications like diabetic ketoacidosis (DKA) make it a major pediatric health concern [5]. At the same time, the epidemiology of pediatric diabetes is shifting with a growing incidence of T2DM among children and adolescents. This increase is especially apparent in countries facing rising childhood obesity rates and among certain ethnic minority groups. In the United States, Native American, African American, and Hispanic youth experience significantly higher rates of T2DM compared to their non-Hispanic white peers [6]. The development of T2DM in youth is closely associated with modifiable lifestyle factors such as obesity, physical inactivity, and unhealthy eating patterns. Moreover, youth-onset T2DM often presents with a more aggressive disease course than adult-onset forms, including rapid progression, early onset of complications, and a poorer response to conventional treatments [7].
Among adults, T2DM constitutes the majority of diabetes cases and represents a major cause of global morbidity and mortality. According to estimates by the International Diabetes Federation[8] , approximately 537 million adults aged 20 to 79 were living with diabetes in 2021. This figure is projected to rise to 643 million by 2030, reflecting the global scale of the problem. The burden is particularly acute in low- and middle-income countries, where rapid urbanization, dietary transitions, and reduced physical activity have fueled rising rates of obesity and T2DM. Adults with T2DM face heightened risks for serious complications, including cardiovascular disease, stroke, chronic kidney disease, retinopathy, and amputations all of which contribute to reduced quality of life and increased healthcare expenditures [9]. Age is a critical variable in the epidemiological landscape of diabetes. T2DM in adults often develops insidiously and may remain undetected for years, whereas in youth, the disease tends to progress swiftly and is more likely to cause early complications. Epidemiological research has been essential for understanding these patterns and guiding prevention efforts. Long-term cohort studies such as the Framingham Heart Study and the UK Biobank have provided valuable insights into the natural history of diabetes, highlighting the dangers of sustained hyperglycaemia and the benefits of early intervention [10]. In addition, global initiatives like the Global Burden of Disease (GBD) Study have underscored the need for comprehensive population-level strategies to reduce risk exposure and control the disease burden [11].
Effective public health responses must be tailored to the specific needs of both pediatric and adult populations. In children and adolescents, preventive strategies should prioritize obesity prevention through healthier diets, increased physical activity, and proactive screening among high-risk groups. For adults, an integrated approach to diabetes care is essential. This includes lifestyle interventions, adherence to pharmacologic therapy, management of coexisting health conditions, and efforts to address socioeconomic and racial health disparities. Across all age groups, emerging technologies such as digital health platforms, telemedicine, and community-based interventions offer promising avenues to enhance diabetes care delivery and improve patient outcomes. This review explores recent advancements in the diagnosis and management of diabetes mellitus across pediatric and adult populations, with a particular emphasis on pharmacological treatments especially insulin therapy and dietary interventions. It highlights emerging diagnostic strategies, evolving drug regimens, and the growing role of nutrition in optimizing glycaemic control and preventing complications in both Type 1 and Type 2 diabetes.
2. Pathophysiological Differences Between Pediatric and Adult Diabetes
Diabetes mellitus manifests across all age groups, but its pathophysiological profile differs markedly between pediatric and adult populations. These differences have critical implications for diagnosis, treatment, disease progression, and long-term outcomes. The increasing prevalence of both type 1 and type 2 diabetes in children and adolescents, along with improved understanding of monogenic diabetes and related conditions, has highlighted the need to differentiate diabetes types by age-related mechanisms rather than clinical appearance alone [12]. In children, type 1 diabetes mellitus (T1DM) remains the most common form, primarily caused by autoimmune destruction of pancreatic β-cells. This process tends to occur more rapidly in younger individuals, often resulting in near-total insulin deficiency by the time of diagnosis. Pediatric T1DM typically presents acutely with symptoms such as polyuria, polydipsia, and weight loss, and is frequently complicated by diabetic ketoacidosis at onset. In contrast, adults with T1DM particularly those with latent autoimmune diabetes in adults (LADA) often experience a slower autoimmune progression. They may retain partial insulin production for months or years, leading to initial misclassification as type 2 diabetes mellitus (T2DM). Immunological studies show that younger individuals are more likely to test positive for multiple autoantibodies, reflecting a more robust and aggressive autoimmune response compared to adults [13].
Type 2 diabetes in adults usually develops gradually through the combination of insulin resistance and progressive β-cell dysfunction. It is typically associated with obesity, physical inactivity, and aging. However, in youth, T2DM follows a different and more aggressive course. Adolescents diagnosed with T2DM exhibit more profound insulin resistance than adults at diagnosis, and their pancreatic β-cell function tends to decline more rapidly. This early onset is closely linked to obesity and the hormonal milieu of puberty, which further worsens insulin resistance. As a result, pediatric T2DM carries a higher risk of early microvascular complications, including nephropathy, retinopathy, and neuropathy, often within a few years of diagnosis far earlier than in adults. Moreover, youth-onset T2DM often shows poor response to standard therapies like metformin, with many children requiring insulin or multiple medications within a few years [10]. Maturity-onset diabetes of the young (MODY), a monogenic form of diabetes, also exemplifies distinct age-related pathophysiology. It typically emerges in adolescence or young adulthood and results from mutations in genes that affect insulin production. Unlike T1DM, MODY lacks autoimmune features, and unlike T2DM, it is not driven by insulin resistance. Misdiagnosis is common, leading to inappropriate treatment. Some MODY subtypes respond well to sulfonylureas instead of insulin, underscoring the importance of recognizing genetic subtypes and applying molecular diagnostics early in atypical cases [14].
The complications associated with diabetes also differ in presentation and progression between children and adults. Pediatric patients with T2DM experience a more aggressive course, with evidence of retinopathy and microalbuminuria often emerging within five years of diagnosis. In contrast, these complications usually take longer to develop in adult-onset T2DM. The pathophysiological drivers of this accelerated progression in youth are not yet fully understood but may involve earlier and more intense exposure to metabolic dysregulation during critical growth periods. Similarly, diabetic retinopathy in children appears to follow unique developmental pathways, with inflammatory and vascular factors playing a more dominant role compared to adult-onset disease [15]. Sex and gender also influence diabetes pathophysiology. Adolescent females with T2DM are more likely to develop complications like polycystic ovary syndrome (PCOS), while males may exhibit more severe insulin resistance and hepatic steatosis. These differences stem from variations in fat distribution, hormonal regulation, and hepatic metabolism during puberty. In both age groups, sex-linked differences affect susceptibility to complications and should be considered when tailoring therapeutic strategies [16].Transition from pediatric to adult care introduces an additional layer of complexity, especially for those diagnosed with diabetes in childhood or adolescence. Studies show that this period is frequently associated with a decline in glycemic control and an increased incidence of complications. Factors such as loss of structured pediatric care, psychosocial stress, and inconsistent health system engagement contribute to this deterioration.
Eight years after transitioning to adult care, many individuals continue to struggle with poor metabolic control and comorbidities, indicating that the pathophysiological burden of early-onset diabetes carries long-term consequences that require continuous and coordinated care [17]. Non-alcoholic fatty liver disease (NAFLD), a condition closely linked to insulin resistance, further illustrates pathophysiological distinctions. In pediatric patients, NAFLD tends to present with more severe histopathological changes such as portal inflammation and fibrosis, compared to the typically milder steatosis seen in adults. The interplay between hepatic insulin resistance, visceral adiposity, and systemic inflammation may be more pronounced during adolescence, contributing to the rapid development of metabolic syndrome and its complications in youth [18]. Ultimately, the biological processes underlying diabetes are not uniform across the lifespan. In children and adolescents, the disease is often more aggressive, progresses faster, and is influenced by developmental and hormonal factors that are absent or less pronounced in adults. These age-related pathophysiological differences underscore the need for targeted diagnostic criteria, tailored treatment plans, and age-specific management strategies to optimize outcomes in both pediatric and adult populations Figure 1.
3. Diagnostic Criteria and Screening Approaches for All Ages
The diagnosis and screening of diabetes mellitus rely on a combination of biochemical markers and clinical criteria that must be sensitive, specific, and adaptable across diverse age groups and populations. Although core diagnostic thresholds for diabetes are consistent across most guidelines, age, race, ethnicity, and pregnancy introduce substantial variation in diagnostic accuracy and screening effectiveness. Understanding and refining these approaches across the life span is critical for improving early detection, mitigating complications, and implementing preventive interventions [19]. Current diagnostic criteria for diabetes are primarily defined by the American Diabetes Association (ADA) and the World Health Organization (WHO), emphasizing fasting plasma glucose (FPG), oral glucose tolerance test (OGTT), hemoglobin A1c (HbA1c), and random plasma glucose levels in the presence of classic symptoms. The ADA Standards of Care in Diabetes 2024 reaffirm that a diagnosis can be made if FPG is ≥126 mg/dL (7.0 mmol/L), 2-hour plasma glucose in OGTT is ≥200 mg/dL (11.1 mmol/L), HbA1c is ≥6.5%, or random plasma glucose is ≥200 mg/dL with symptoms of hyperglycemia. These criteria are standardized for adults and children; however, they may not perform uniformly across all age groups, racial/ethnic groups, or in special populations such as pregnant women or the elderly [19,20,21]. Screening strategies, while built on these biochemical thresholds, require careful population-specific calibration.
The ADA recommends routine screening for adults aged ≥35 years and younger individuals with risk factors such as obesity, family history of diabetes, sedentary lifestyle, or belonging to a high-risk ethnic group. However, emerging evidence suggests that these age-based thresholds may miss a significant proportion of younger individuals at risk, especially among ethnic minorities. A study analyzing data from the Third National Health and Nutrition Examination Survey (NHANES III) found that advancing age independently influenced diabetes prevalence and cardiovascular risk profiles, but also noted that younger adults often had undiagnosed diabetes due to outdated screening cut-offs. As a result, some researchers have advocated for lowering the age threshold for universal screening to 25 years, particularly in high-prevalence populations [22]. In pediatric populations, the increasing incidence of type 2 diabetes especially among adolescents with obesity has driven efforts to expand screening. The ADA advises screening children over the age of 10 (or earlier if puberty has begun) who have a body mass index (BMI) ≥85th percentile and one or more additional risk factors. While FPG and OGTT remain standard tests, the use of HbA1c in pediatric populations remains contentious. Research indicates that HbA1c levels may be influenced by age, race/ethnicity, and haemoglobin variants, potentially leading to under diagnoses or over diagnosis in certain populations. Screening for type 1 diabetes in children involves autoantibody testing and focuses on symptoms and risk factors, such as obesity and family history. OGTT, fasting glucose, or HbA1c are commonly used for screening adults based on their age and risk profile. For older adults, the focus switches to comorbidities and functional status, whereas glucose tolerance testing is routine for gestational diabetes during pregnancy. This age-specific variability ensures timely diagnosis and management tailored to physiological needs, as shown in Figure 2.
One study demonstrated that non-Hispanic Black individuals without diagnosed diabetes tend to have higher HbA1c levels compared to their white counterparts, even at similar glucose concentrations. These findings underscore the need for caution when relying solely on HbA1c for diagnosis, particularly in racially diverse pediatric and adult populations [23,24]. Gestational diabetes mellitus (GDM) introduces further complexity in diagnostic and screening practices. The International Association of Diabetes and Pregnancy Study Groups (IADPSG) criteria adopted by the WHO and many national bodies recommend universal screening during 24–28 weeks of gestation using a 75g OGTT with thresholds of ≥92 mg/dL fasting, ≥180 mg/dL at 1 hour, or ≥153 mg/dL at 2 hours. Despite widespread endorsement, significant global variability exists in GDM screening strategies, including the use of one-step versus two-step protocols. The GDM2 Trial compared the effectiveness of these two approaches and raised concerns about the potential for over diagnosis and overtreatment with the one-step method. In Italy, an analysis of national guidelines from 2010 to 2019 revealed inconsistencies in GDM screening, pointing to the need for more uniform implementation and evaluation frameworks. Importantly, untreated GDM increases the risk of adverse maternal and neonatal outcomes, and also predicts future type 2 diabetes in the mother and offspring, justifying more aggressive identification strategies [25].
In older adults, diabetes screening presents distinct challenges. Age-related changes in glucose metabolism and renal function can complicate interpretation of glucose levels, and traditional criteria may underestimate risk. For instance, HbA1c may be elevated in older adults due to reduced erythropoiesis, leading to potential over diagnosis. Conversely, postprandial hyperglycaemia may be more pronounced, while fasting glucose remains near-normal, resulting in underdiagnoses if only FPG is used. The heterogeneity of aging also means that some individuals may benefit from screening and aggressive intervention, while others may require more conservative approaches, depending on comorbidities, life expectancy, and functional status [26]. Recent advances in biomarker discovery aim to improve diagnostic accuracy and stratification across age groups. Novel candidates such as 1,5-anhydroglucitol, glycated albumin, and continuous glucose monitoring-derived metrics are being investigated to complement traditional markers, especially in settings where HbA1c is unreliable. These markers may offer earlier detection of glycaemic variability and postprandial dysregulation in high-risk individuals, but their use remains limited to research and specialized clinical settings [27].
The effectiveness of diabetes screening programs hinges not only on biochemical criteria but also on implementation and public health strategy. Studies show that adherence to screening recommendations remains suboptimal in many healthcare systems, particularly among underserved populations. Multifactorial barriers, including socioeconomic status, health literacy, provider awareness, and insurance coverage, reduce the effectiveness of even well-designed screening guidelines. Therefore, policies must align diagnostic accuracy with health equity by incorporating age-, race-, and sex-sensitive screening tools, culturally tailored outreach, and integrated follow-up systems [28].
4. Role of Lifestyle Modifications Including Diet and Physical Activity
Lifestyle modifications, especially dietary changes and physical activity, are central to both the prevention and management of type 2 diabetes mellitus (T2DM). Extensive research demonstrates that behavioral factors such as excessive caloric intake, poor-quality diets, physical inactivity, and obesity are key contributors to diabetes onset and progression. Addressing these modifiable behaviors has shown substantial clinical benefit in improving glycemic control, reducing complications, and delaying disease progression [29,30]. Obesity, particularly central adiposity, plays a pivotal role in insulin resistance and the pathophysiology of T2DM. Weight loss achieved through lifestyle change especially through caloric restriction and exercise can restore insulin sensitivity and improve glucose metabolism. Landmark trials like the Diabetes Prevention Program (DPP) and Finnish Diabetes Prevention Study revealed that lifestyle changes involving modest weight loss and regular physical activity reduced diabetes incidence by over 50% in high-risk individuals [31,32].
Dietary quality significantly influences diabetes outcomes. Diets rich in vegetables, fiber, whole grains, legumes, and unsaturated fats improve glycemic parameters and lipid profiles. Low-glycemic-index foods and reduced-calorie diets have been associated with improved HbA1c levels and insulin sensitivity. The Mediterranean and DASH diets have shown consistent benefits in randomized controlled trials, improving not only glycemic control but also cardiovascular risk factors [33]. Physical activity complements dietary strategies by enhancing insulin sensitivity, lowering blood glucose, and improving cardiovascular health. Both aerobic and resistance training are effective, with guidelines recommending at least 150 minutes of moderate-intensity exercise weekly for most adults with diabetes. Regular physical activity also supports weight maintenance, reduces inflammation, and improves endothelial function, independent of weight loss. Studies underscore the importance of cardiorespiratory fitness as a protective factor against diabetes, even among individuals with excess weight [34]. Lifestyle interventions also reduce the risk of diabetes-related complications. For example, increased physical activity and dietary modifications can slow the progression of diabetic kidney disease and reduce the risk of retinopathy and neuropathy. They also lower the risk of cardiovascular disease the leading cause of death in people with diabetes by improving blood pressure, lipid levels, and endothelial function [35].
Figure 3.
Lifestyle modifications including healthy diet and physical activity play a crucial role in preventing and managing type 2 diabetes by improving glycemic control and reducing complications.
Figure 3.
Lifestyle modifications including healthy diet and physical activity play a crucial role in preventing and managing type 2 diabetes by improving glycemic control and reducing complications.
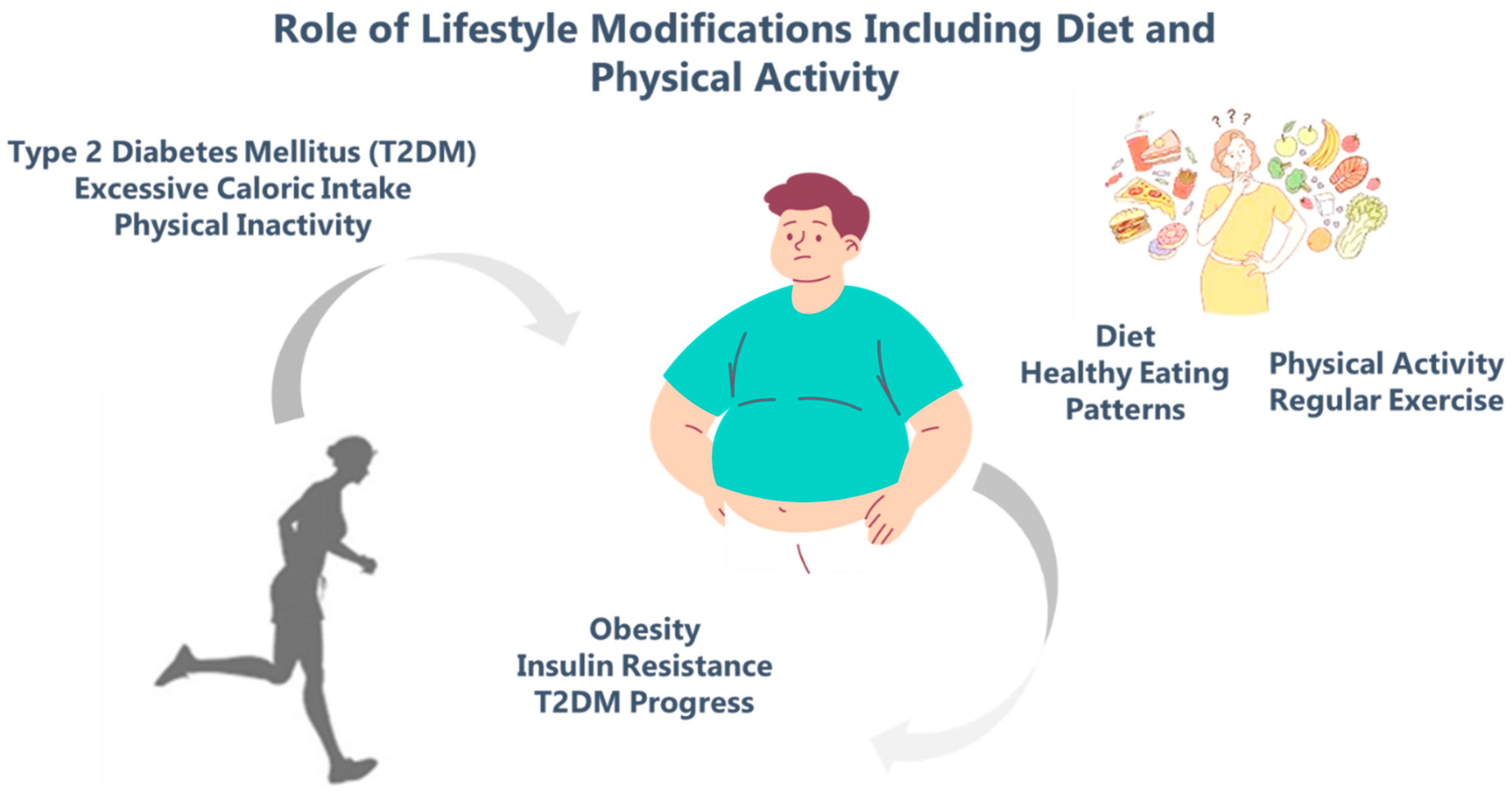
A balanced diet and regular exercise are two essential lifestyle changes for the prevention and treatment of type 2 diabetes. These therapies lower blood glucose, promote weight control, increase insulin sensitivity, and lessen the risk of cardiovascular disease and other complications associated with diabetes. Glycemic control is greatly improved by including foods high in fiber, consuming less refined sugar, and doing regular aerobic or resistance training. Patients' overall quality of life can be enhanced and the onset of diabetes in at-risk individuals can be postponed or even prevented with early adoption and adherence to these lifestyle modifications. as depicted inFigure 2. Despite strong evidence, adherence to lifestyle changes remains a challenge. Patients report difficulty sustaining multiple behavior changes simultaneously, often facing environmental, economic, or psychosocial barriers. Qualitative research highlights the importance of motivation, support systems, and structured interventions. Behavioral counseling, goal-setting, and peer support are associated with better long-term adherence and glycemic control [36]. Incorporating digital health technologies such as mobile tracking apps, wearable fitness devices, and virtual coaching has shown promise in enhancing engagement and self-monitoring. These tools may help individuals maintain consistent behavior changes, especially when face-to-face interventions are inaccessible. Technology-based strategies are particularly useful for younger patients and those in underserved or rural communities. Public health measures, including policies to promote active transportation, regulate food environments, and support school-based nutrition programs, can create supportive environments for healthy living. European initiatives targeting childhood obesity and sedentary lifestyles have shown positive trends in slowing the rise of T2DM incidence [37]. Lifestyle modification is not only effective but cost-efficient, offering a non-pharmacologic option with widespread applicability. While medications remain important in managing T2DM, behavioral interventions provide benefits that address root causes of disease and offer broader systemic health improvements [38].
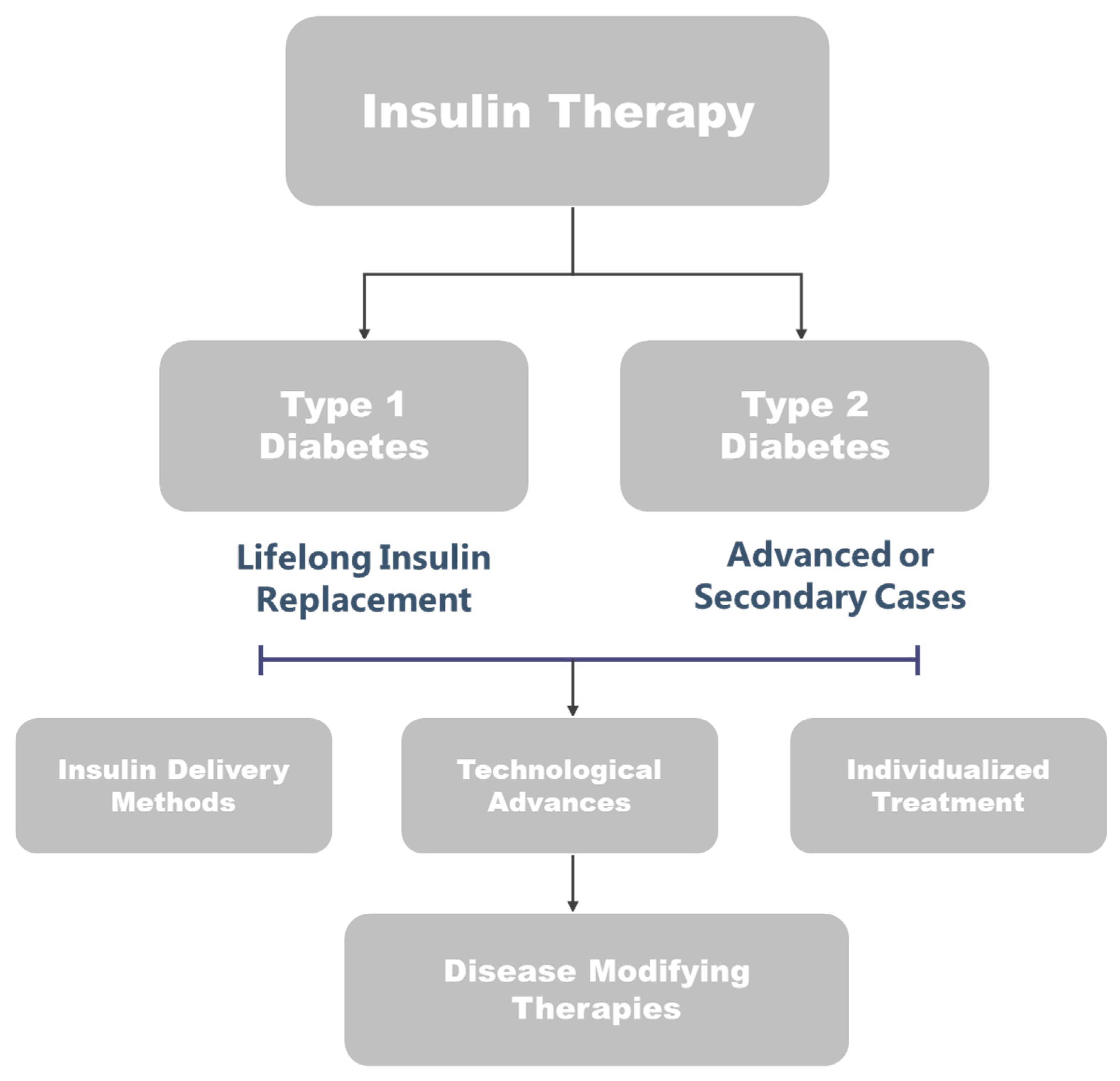
5. Insulin Therapy: Indications and Advances in Pediatric and Adult Diabetes
Insulin therapy remains the foundational treatment for individuals with Type 1 Diabetes (T1D) across all age groups. Due to autoimmune destruction of pancreatic β-cells, people with T1D experience absolute insulin deficiency, necessitating lifelong insulin administration. This holds true for both pediatric and adult populations, with insulin therapy typically initiated at the time of diagnosis. It is also used in selected cases of advanced Type 2 Diabetes (T2D) or secondary diabetes when glycemic control cannot be achieved through oral medications and lifestyle changes [39]. Insulin delivery has evolved significantly in recent decades. The traditional approach, multiple daily injections (MDI), involves administering long-acting basal insulin and rapid-acting bolus insulin before meals. While still widely used due to its cost-effectiveness and flexibility, MDI demands consistent carbohydrate counting and adherence to injection schedules. Continuous subcutaneous insulin infusion (CSII), or insulin pump therapy, provides an alternative that allows for more precise insulin dosing. Supported by international pediatric endocrine societies, pump therapy is particularly beneficial in patients with frequent hypoglycemia, poor glycemic control, or specific challenges such as the dawn phenomenon. By offering programmable basal rates and flexible bolus options, insulin pumps contribute to improved HbA1c levels and treatment satisfaction [40].
Technological advances have further improved insulin therapy outcomes. Sensor-augmented pump therapy integrates continuous glucose monitoring (CGM) with insulin delivery, allowing real-time adjustments. These systems reduce glycemic variability and enhance time-in-range metrics. Hybrid closed-loop systems, often referred to as artificial pancreas systems, combine CGM data with insulin pumps to automatically adjust insulin delivery. While users must still input mealtime carbohydrate intake, these systems significantly reduce both hyperglycaemia and hypoglycaemia. Their efficacy and safety are supported by recent guidelines, including those from the International Society for Pediatric and Adolescent Diabetes (ISPAD) 2022 update, which endorses their use in pediatric populations. Fully automated closed-loop systems are under investigation and hold the potential to eliminate the need for manual bolus administration altogether [41].Insulin therapy must be individualized. In children and adolescents, insulin dosing must adapt to age, weight, physical activity, puberty, and psychological maturity. For adults, considerations include comorbidities, lifestyle, and the risk of hypoglycaemia. Regardless of age, diabetes education, psychosocial support, and regular follow-up are essential for successful therapy. In pediatric care, family involvement plays a critical role in daily management and long-term outcomes [12].
Research into disease-modifying therapies is a rapidly advancing field. One promising area is regulatory cell therapy, which aims to modulate the immune system to preserve or restore β-cell function. Strategies include the infusion of regulatory T cells (Tregs), tolerogenic dendritic cells, and stem-cell-based approaches. Though still in experimental stages, such therapies offer the potential to reduce dependence on insulin and possibly alter the disease course. Advances in biotechnology and immunotherapy are central to these developments and are increasingly featured in clinical trials worldwide [42]. Despite these promising innovations, global disparities in access to insulin, diabetes technology, and specialized care continue to pose significant challenges. Many children and adults around the world remain without consistent access to insulin or glucose monitoring. Addressing these inequities requires coordinated efforts in healthcare policy, education, and infrastructure development. Insulin therapy remains essential for the management of T1D and select cases of insulin-dependent T2D [43]. Innovations in insulin delivery and monitoring have improved outcomes and quality of life for many patients, particularly when therapy is personalized. Research into cell-based and immune-modulating therapies provides hope for a future where insulin may no longer be required. Continued focus on education, technology access, and individualized care will be key to improving outcomes across both pediatric and adult populations.
Figure 4.
Overview of insulin therapy indications and advances, including modern delivery methods and emerging technologies for both pediatric and adult diabetes management.
Figure 4.
Overview of insulin therapy indications and advances, including modern delivery methods and emerging technologies for both pediatric and adult diabetes management.
6. Oral and Injectable Non-Insulin Drugs for Diabetes Management
Non-insulin pharmacological therapies play a critical role in the management of Type 2 Diabetes Mellitus (T2DM), offering diverse mechanisms to lower blood glucose and reduce the risk of complications. These agents are often used as first-line or adjunct therapies before or alongside insulin, especially in patients with sufficient residual β-cell function. With the increasing prevalence of T2DM globally, optimizing the use of oral and injectable non-insulin therapies is essential for individualized care [44]. Oral antidiabetic drugs include several classes with distinct mechanisms. Metformin remains the cornerstone of initial therapy due to its efficacy, safety, cardiovascular benefits, and low cost. It primarily reduces hepatic glucose production and improves insulin sensitivity. Sulfonylureas stimulate insulin secretion but carry a risk of hypoglycaemia and weight gain. Thiazolidinedione’s (e.g., pioglitazone) enhance peripheral insulin sensitivity but are associated with fluid retention and potential cardiovascular risks. DPP-4 inhibitors (e.g., sitagliptin) modestly lower glucose by prolonging the action of incretin hormones, with a favourable safety profile [45]. SGLT2 inhibitors (e.g., empagliflozin, dapagliflozin) reduce renal glucose reabsorption, promoting urinary glucose excretion. They offer notable cardiovascular and renal benefits and are now recommended in patients with heart failure or chronic kidney disease, regardless of glycaemic status. GLP-1 receptor agonists (e.g., liraglutide, semaglutide), although injectable, are non-insulin agents that mimic endogenous incretin activity. They enhance glucose-dependent insulin secretion, slow gastric emptying, and promote satiety, leading to weight loss and improved cardiovascular outcomes [46].
The use of combination therapy oral agents with or without injectable is common in clinical practice to target multiple pathophysiological defects in T2DM. Combining metformin with SGLT2 inhibitors or GLP-1 receptor agonists provides superior glycemic control while minimizing weight gain and hypoglycemia. Several fixed-dose combination pills enhance adherence by simplifying complex regimens. Clinical evidence supports early initiation of combination therapy in patients with high HbA1c levels or progressive β-cell dysfunction [47]. In some cases, non-insulin therapies are used in combination with basal insulin. Adding oral agents like metformin or SGLT2 inhibitors to basal insulin can improve glucose control and reduce total insulin requirements. This approach helps avoid the need for complex insulin regimens and reduces the risk of weight gain and hypoglycemia often associated with intensive insulin therapy. Studies comparing insulin monotherapy with insulin plus oral agents show that the combination often yields better metabolic outcomes and improved adherence [48]. Beyond glucose lowering, many non-insulin therapies exert favorable effects on cardiovascular, renal, and hepatic outcomes. SGLT2 inhibitors and GLP-1 receptor agonists have redefined diabetes treatment paradigms by providing organ-protective effects independent of glycemic control. These benefits have been highlighted in recent international guidelines, shifting treatment priorities toward risk-based therapy rather than glucose-centric strategies alone.
In parallel, advances in drug delivery technologies have improved the tolerability and convenience of non-insulin therapies. Once-weekly injectable GLP-1 receptor agonists and the development of oral semaglutide offer improved adherence and patient preference. Non-invasive insulin and non-insulin delivery systems, such as transdermal patches, inhaled agents, and oral formulations, are in various stages of clinical trials and may further expand therapeutic options in the future [49]. Physical activity remains a crucial adjunct to pharmacological treatment, enhancing the effectiveness of glucose-lowering therapies and improving insulin sensitivity. The interaction between exercise and non-insulin drugs must be considered, as certain agents, like SGLT2 inhibitors, may increase dehydration risk during strenuous activity [50]. While non-insulin therapies are generally safe, careful monitoring is necessary in hospitalized patients or those with comorbidities. In inpatient settings, newer agents have shown potential in maintaining stable glucose control with fewer adverse events compared to insulin, although insulin remains the mainstay for critically ill patients. Meta-analyses suggest that GLP-1 receptor agonists and DPP-4 inhibitors can be safely used in general wards under appropriate clinical supervision [51,52]. Oral and injectable non-insulin agents provide effective, flexible, and often safer alternatives or complements to insulin in the management of Type 2 Diabetes. These therapies support individualized care strategies that target not only glycemic control but also weight, cardiovascular risk, and renal protection. Continued research into novel agents, combination therapies, and advanced delivery methods will further enhance diabetes management across outpatient and inpatient settings.
7. Technology in Diabetes Care: Pumps Continuous Glucose Monitoring and Automated Delivery
Advancements in diabetes technology have transformed the management of Type 1 Diabetes (T1D) and insulin-requiring Type 2 Diabetes (T2D), improving glycemic outcomes, safety, and quality of life. Central to this evolution are continuous glucose monitors (CGMs), insulin pumps, and automated insulin delivery (AID) systems, which together form an integrated approach to diabetes care. These innovations address the limitations of traditional self-monitoring and manual insulin dosing, allowing more precise and dynamic management [53].Continuous glucose monitoring technology has rapidly advanced from retrospective systems to real-time CGMs that provide near-continuous data, typically every 1–5 minutes. Modern CGMs offer trend arrows, alerts for hypo- and hyperglycemia, and predictive alarms, enabling proactive adjustments to therapy. Their accuracy and reliability have improved significantly, particularly with factory-calibrated sensors requiring minimal or no fingerstick validation. Real-world data demonstrate that CGM use improves HbA1c, increases time in range, and reduces hypoglycemia, especially when used consistently. CGMs also enhance patient engagement, allowing users to visualize the impact of meals, activity, and insulin on glucose levels [54].Insulin pumps, or continuous subcutaneous insulin infusion (CSII) devices, deliver rapid-acting insulin in a programmable basal-bolus manner. Compared to multiple daily injections, pumps provide greater flexibility and finer control of insulin delivery, with adjustable basal rates and extended bolus options. CSII is particularly beneficial in individuals with frequent hypoglycemia, variable schedules, or high insulin sensitivity. Technological improvements have led to pumps with touchscreen interfaces, Bluetooth connectivity, and integration with mobile apps, making data sharing and remote monitoring more accessible to patients and providers [55].
The convergence of CGM and insulin pump technology has paved the way for hybrid closed-loop systems, also known as automated insulin delivery. These systems use CGM data to automatically adjust basal insulin delivery via algorithms embedded in the pump or external controller. While current hybrid models still require user-initiated boluses for meals, they significantly reduce glycemic variability, increase time in range, and lessen the cognitive and emotional burden of diabetes management. The MiniMed™ 670G, the first commercial hybrid closed-loop system, demonstrated meaningful improvements in glycemic control and patient satisfaction in both clinical trials and real-world settings. Subsequent systems, including the MiniMed™ 780G and Tandem Control-IQ, have built upon these capabilities, incorporating automated correction boluses and improved adaptability to daily fluctuations [56]. Automated insulin delivery systems have shown not only glycemic benefits but also potential cardiovascular advantages. By reducing glycemic variability and hypoglycemia, these technologies may lower the risk of vascular complications over time.
Early studies suggest improved metabolic profiles, reduced inflammatory markers, and better patient adherence when using integrated systems, though long-term cardiovascular outcome data are still emerging [57]. Ease of use and personalization are central to the success of these technologies. Users can tailor target glucose ranges, insulin sensitivity factors, and carbohydrate ratios to fit their lifestyle. Education and training are critical for optimizing outcomes, as effective use requires understanding device features, interpreting CGM trends, and adjusting therapy accordingly. User experience studies highlight the importance of minimizing alarms, simplifying interfaces, and improving device wearability to enhance satisfaction and adherence [58]. Remote monitoring capabilities, supported by cloud-based data platforms, allow clinicians and caregivers to review glucose trends, insulin delivery, and behavioural patterns in real time. This has facilitated telemedicine-based diabetes care, particularly during the COVID-19 pandemic, and enabled more proactive and personalized management. Data integration across devices has also improved the ability to conduct pattern analysis, adjust therapy more precisely, and empower patients with actionable insights [59]. Looking forward, the development of fully closed-loop systems requiring minimal user input is a major goal. Research is ongoing into hormonal systems that deliver both insulin and glucagon, adaptive algorithms that learn user behaviour, and non-invasive glucose sensors. These advances aim to further reduce user burden, improve safety, and mimic physiologic glucose regulation more closely [60]. Diabetes technology has significantly advanced in recent years, providing tools that not only improve glycaemic control but also enhance quality of life. The integration of continuous glucose monitoring, insulin pumps, and automated delivery systems represents a paradigm shift in diabetes management. While these tools require proper education and support, they offer substantial benefits for individuals willing to engage with them. Ongoing innovation continues to push the boundaries of what is possible in diabetes care, moving steadily toward more automated, individualized, and effective treatment.
8. Transitioning from Pediatric to Adult Diabetes Care Services
The transition from pediatric to adult diabetes care is a critical and often vulnerable period for emerging adults with Type 1 Diabetes (T1D). Typically occurring between the ages of 18 and 25, this phase coincides with major life changes such as leaving home, starting college or employment, and navigating increased independence. Despite advancements in diabetes management, many young adults experience deterioration in glycaemic control and increased risk of acute and chronic complications during this transition, often due to gaps in care and challenges in adjusting to adult healthcare systems [61]. A well-structured transition process is essential for ensuring continuity of care, maintaining treatment adherence, and supporting long-term health outcomes. Position statements from leading diabetes and medical organizations, including the American Diabetes Association and the International Society for Pediatric and Adolescent Diabetes, emphasize the importance of planned, coordinated, and developmentally appropriate transition models. These models should begin in early adolescence and extend into young adulthood, with individualized goals based on the patient's readiness, self-management skills, and psychosocial needs rather than age alone [62].
One of the most significant barriers to successful transition is the difference in care philosophies between pediatric and adult healthcare systems. Pediatric care is often family-centered, with close monitoring and structured support, while adult care places greater emphasis on patient autonomy and self-management. Many emerging adults are unprepared for this shift, leading to missed appointments, loss of follow-up, and suboptimal engagement with adult providers. Studies reveal that a lack of preparation, inadequate communication between pediatric and adult teams, and insufficient support during the handoff period contribute to fragmented care and declining metabolic outcomes [63]. Effective transition requires collaboration between pediatric and adult providers, clear communication, and shared responsibility. Successful models include formal transition protocols with timelines, readiness assessments, transition coordinators, and joint visits between pediatric and adult teams. These practices facilitate trust-building, knowledge transfer, and patient empowerment. Early involvement of adult providers and consistent reinforcement of self-care skills—such as insulin adjustment, carbohydrate counting, and interpreting continuous glucose monitoring data—can enhance confidence and engagement [64].
Patient perspectives underscore the importance of being included in transition planning. Emerging adults report valuing continuity, emotional support, and clear expectations from new providers. They often feel anxious or abandoned when abruptly transferred without adequate preparation or follow-up. Incorporating peer support, mentoring, and technology-based resources such as mobile apps or telehealth follow-ups can ease the transition and foster a sense of connection and competence [65]. Healthcare systems also play a role in transition outcomes. Structural limitations such as lack of adult endocrinologists trained in young adult care, limited access to behavioural health resources, and inadequate insurance coverage can hinder effective transition. Policy-level interventions aimed at improving access to care, incentivizing transition planning, and integrating behavioural health into diabetes care models are essential for addressing these broader challenges [66]. From a psychosocial standpoint, emerging adults face unique stressors, including identity formation, mental health issues, and competing academic or work demands, all of which can influence diabetes self-care. Depression, diabetes distress, and substance use are more prevalent in this age group and are linked to poor glycemic outcomes. Routine screening for psychosocial issues, as well as access to mental health support, should be integrated into the transition process [67].
In recent years, there has been increasing recognition of the need for “receivership” the responsibility of adult care systems to engage and support new patients effectively. Adult providers must be prepared to meet emerging adults where they are, balancing autonomy with appropriate guidance. Training in adolescent development, communication skills, and culturally responsive care can help bridge the relational and clinical gap between pediatric and adult services [61]. Transitioning from pediatric to adult diabetes care is a complex, multidimensional process that requires careful planning, communication, and support. It should begin early, focus on patient readiness rather than age, and involve both pediatric and adult providers. Empowering patients, addressing psychosocial needs, and strengthening adult care systems are essential to ensuring that emerging adults with T1D maintain optimal health and engagement during and beyond the transition period. Continued innovation in care models and stronger health system integration will be critical for improving outcomes during this vulnerable life stage.
9. Psychological and Behavioural Aspects of Diabetes Management
Diabetes is a lifelong condition that demands constant self-management, making psychological and behavioural factors central to successful care. Beyond the physiological aspects, individuals with diabetes face a range of emotional, cognitive, and social challenges that can significantly influence disease outcomes. Addressing these psychological and behavioral dimensions is essential for promoting treatment adherence, improving glycemic control, and enhancing overall quality of life [68]. The diagnosis of diabetes often brings about emotional distress, anxiety, and a sense of loss. Patients may struggle with the burden of daily monitoring, dietary restrictions, medication adherence, and fear of complications. For many, this leads to diabetes distress a condition distinct from clinical depression characterized by frustration, burnout, and feelings of being overwhelmed by the demands of self-care. Studies show that up to 40% of people with diabetes experience significant diabetes distress at some point, which is directly linked to poor glycaemic outcomes and reduced engagement in self-care behaviours [69].
Depression and anxiety are also more prevalent among individuals with diabetes compared to the general population. These conditions can impair decision-making, reduce motivation, and lead to neglect of necessary care tasks such as insulin administration, glucose monitoring, and healthy eating. Furthermore, depressive symptoms can negatively affect physiological processes, increasing insulin resistance and inflammation, thereby worsening metabolic control. The bidirectional relationship between diabetes and mental health necessitates routine screening and timely intervention for psychological comorbidities [70]. Behavioural change is often difficult to achieve and sustain in diabetes management. Patients are required to make complex decisions multiple times a day, from counting carbohydrates and adjusting insulin to managing physical activity and stress. Motivational interviewing, goal-setting, and cognitive-behavioural strategies are effective tools in supporting individuals to develop and maintain healthier habits. These approaches encourage self-efficacy, empower patients to set realistic goals, and help them navigate obstacles to adherence [71].
Healthcare providers play a crucial role in shaping the psychological experience of patients. A collaborative and empathetic communication style, often referred to as person-centered care, strengthens trust and improves outcomes. When providers acknowledge the emotional impact of diabetes and validate the patient's experience, it fosters engagement and reduces resistance to care plans. On the other hand, judgmental or prescriptive interactions can lead to feelings of shame, guilt, and disengagement from care [70]. Social and cultural factors further influence how individuals perceive and manage their condition. Family support, socioeconomic status, health literacy, and cultural beliefs all shape attitudes toward diabetes and self-care practices. In particular, young people, minorities, and those with limited resources face unique psychosocial barriers. Tailoring interventions to consider these contextual elements improves their effectiveness and sustainability. Peer support programs, community education, and culturally adapted care models have demonstrated positive effects on both psychological well-being and diabetes control [72].
Technology has introduced new behavioral and emotional dimensions to diabetes management. While tools like continuous glucose monitors and insulin pumps provide greater control and convenience, they may also introduce new stressors such as device fatigue, alarm burnout, or data overload. For some, constant exposure to glucose data can trigger anxiety or obsessive monitoring. Psychological support should therefore address not only the technical skills for using these tools but also the emotional responses they evoke [73]. Children, adolescents, and their caregivers face unique psychological challenges in managing diabetes. Fear of hypoglycemia, peer pressure, and concerns about normalcy can hinder adherence in youth. At the same time, parental anxiety and over-involvement can affect a child's autonomy and confidence. Structured behavioral interventions, family-based therapy, and age-appropriate education help mitigate these issues and foster resilience [74]. In clinical practice, integrating psychological care into routine diabetes management is crucial. This includes not only mental health screening and referrals but also embedding behavioral specialists within diabetes care teams. Diabetes educators, psychologists, and social workers can offer coping strategies, stress management techniques, and behavior modification support. A multidisciplinary approach that views the patient holistically ensures that psychological and behavioral aspects are not overlooked in favor of solely biomedical metrics [75]. Psychological and behavioral aspects are integral to effective diabetes management. Emotional distress, mental health disorders, and behavioral challenges can significantly impact adherence and metabolic outcomes. Recognizing and addressing these factors through patient-centered communication, tailored interventions, and integrated psychosocial support is essential to improving both clinical outcomes and the lived experience of people with diabetes.
10. Future Directions and Emerging Therapies in Diabetes Treatment
The landscape of diabetes treatment is rapidly evolving, driven by an urgent need to address the global burden of both Type 1 and Type 2 diabetes, their associated complications, and limitations of existing therapies. Traditional treatment approaches, while effective to a degree, often fall short in achieving sustained glycemic control, preventing complications, and improving long-term outcomes. Recent advances in pharmacological, technological, and regenerative therapies offer promising avenues to reshape diabetes care with a more individualized, targeted, and holistic approach [76]. One of the most notable trends is the development of agents that go beyond glycemic control to address comorbid conditions and organ-specific complications. In Type 2 diabetes, the emergence of sodium-glucose cotransporter-2 (SGLT2) inhibitors and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) represents a shift from glucose-centric models toward cardio- and reno-protective strategies. These drugs have demonstrated substantial benefits in reducing cardiovascular events, slowing renal decline, and aiding weight loss, making them foundational components of contemporary care algorithms. Future directions include expanding indications, optimizing combination therapies, and improving delivery mechanisms to enhance adherence and long-term efficacy [76].
The use of age-specific, personalized, and technologically driven approaches has greatly changed the diagnosis and treatment of diabetes in both adults and children. Current diagnostic methods go beyond standard blood glucose testing to include genetic testing for monogenic diabetes, continuous glucose monitoring (CGM), genetic testing for monogenic diabetes (e.g., MODY), as well as AI-powered prediction models, which enable the earlier and more precise identification of diabetes subtypes. By using insulin pumps, smart pens, and hybrid closed-loop systems, insulin therapies have improved glycemic control and patient adherence, particularly in pediatric populations. Ultra-long-acting analogs and customized dosage guidelines are enhancing long-term results in adults. Newer drugs like dual GIP/GLP-1 receptor agonists, SGLT2 inhibitors, and GLP-1 receptor agonists have shown promise in glycemic control and cardiovascular protection, indicating the diversification of pharmacological interventions. Although there are still few pediatric medication options, research keeps pointing to the safe extension of these treatments in young patients. All age groups benefit greatly from nutritional strategies such as low-glycemic index diets, Mediterranean and DASH diets, and customized dietary plans based on CGM data. Digital health resources and lifestyle modifications also aid in long-term care. Overall, as indicated by Table 1 and Table 2, a thorough, patient-centered approach is necessary for effective diabetes care.
The management of diabetes-related complications is also witnessing innovative progress. For example, diabetic retinopathy treatments are moving beyond traditional laser therapy and anti-VEGF injections. Novel approaches such as PPARα modulators, stem cell-based regeneration, and nanotechnology-based drug delivery systems are being explored for targeted, less invasive intervention. Similarly, in diabetic cardiomyopathy, a condition often underdiagnosed, researchers are evaluating metabolic modulators, anti-fibrotic agents, and SGLT2 inhibitors as potential therapies to preserve cardiac function and prevent progression [77]. Another significant development is the refinement of nanotechnology in diabetes therapeutics. Nano-formulations of insulin and oral antidiabetic agents are being designed to enhance bioavailability, reduce dosing frequency, and enable glucose-responsive drug release. These technologies could reduce the burden of frequent injections and monitoring, while providing tighter glucose control with fewer side effects. Research is also advancing on nanoparticle-based sensors for continuous glucose monitoring and closed-loop insulin delivery systems that may enhance precision and autonomy in self-care [78,79]. In the realm of immunotherapy and regenerative medicine, the treatment of Type 1 diabetes is entering a new phase. Advances in stem cell-derived beta-cell replacement, immune modulation, and antigen-specific tolerance therapies are gaining traction. Recent clinical trials have demonstrated the potential of encapsulated islet cell transplantation and regulatory T-cell therapy to preserve or restore endogenous insulin production. These approaches aim to modify the disease process itself, rather than merely managing its consequences [80]. Emerging therapies are also tackling the hypercoagulable and pro-inflammatory states associated with diabetes. Antiplatelet therapy remains a cornerstone of cardiovascular prevention in high-risk patients, but newer agents and combination regimens are under investigation to optimize efficacy while minimizing bleeding risks.
Personalized antithrombotic strategies based on individual risk profiles may replace the one-size-fits-all approach in the near future [81]. Despite these advances, significant challenges remain. The high cost of novel therapies, disparities in global access, long-term safety concerns, and complexities in regulatory approval can hinder widespread adoption. Moreover, real-world effectiveness often lags behind clinical trial efficacy due to variations in adherence, provider expertise, and health system limitations. There is also a critical need for more inclusive clinical trials that reflect the diversity of diabetes populations in terms of age, ethnicity, and comorbidities [82]. Looking ahead, the future of diabetes management lies in integration combining pharmacologic innovation, digital technology, lifestyle support, and patient empowerment into cohesive care models. Artificial intelligence and machine learning are being increasingly applied to personalize treatment decisions, predict complications, and optimize medication regimens. Mobile health platforms and wearable devices are transforming how patients interact with their care, shifting the paradigm toward continuous, data-driven, and patient cantered management [83]. The future of diabetes treatment is marked by transformative potential across multiple domains, from novel drug targets and organ-specific therapies to nanotechnology, regenerative medicine, and digital health integration. These emerging approaches offer hope for more effective, safer, and personalized care, but their success will depend on equitable access, interdisciplinary collaboration, and sustained investment in research and implementation.
11. Conclusions
Diabetes mellitus continues to pose a significant public health challenge across all age groups, with rising incidence in both pediatric and adult populations. The evolving epidemiological patterns marked by increasing cases of T2DM in youth and a persistently high burden of T2DM among adults demand age-specific, individualized, and integrated approaches to diagnosis and management. Understanding the distinct pathophysiological mechanisms of diabetes in children versus adults is critical for early detection, accurate classification, and effective treatment. Significant progress has been made in recent years through innovations in pharmacotherapy, particularly insulin delivery systems, oral and injectable non-insulin drugs, and the integration of technology such as continuous glucose monitoring and automated insulin delivery systems. Dietary and lifestyle interventions remain foundational, not only in preventing diabetes but also in improving glycaemic outcomes and reducing the risk of complications. Behavioural support, psychosocial care, and structured transitions from pediatric to adult services are also essential for sustaining long-term health outcomes, particularly among vulnerable adolescents and young adults with T1DM. Emerging therapies, including immunomodulatory agents, regenerative approaches, and nanotechnology-based solutions, hold promise for transforming diabetes care beyond glucose control to disease modification and prevention of long-term complications. However, equitable access to these advancements, patient education, and healthcare system integration remain pressing challenges. The future of diabetes management lies in a personalized, multidisciplinary, and technology-driven model that holistically addresses the biological, behavioural, and social dimensions of the disease, across all stages of life.
Author Contributions
Conceptualization, S.S., L.P., A.K.S., A.M.U. and R.K.M.; methodology, S.S., A.M.U., A.K.S., S.S., L.P., and R.K.M.; writing—original draft preparation, S.S., A.K.S., L.P.,and R.K.M.; writing—review and editing, S.S., A.M.U., A.K.S., D.Y., C.D.S., S.M., and R.K.M.; visualization, S.S., A.M.U., A.K.S., L.P and R.K.M.; management, S.S., A.K.S., and R.K.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Diagnosis and Classification of Diabetes Mellitus. In Diabetes Care; 2009.
- Mayer-Davis, E.J.; Lawrence, J.M.; Dabelea, D.; Divers, J.; Isom, S.; Dolan, L.; Imperatore, G.; Linder, B.; Marcovina, S.; Pettitt, D.J.; et al. Incidence Trends of Type 1 and Type 2 Diabetes among Youths. N. Engl. J. Med. 2017. [Google Scholar] [CrossRef]
- Divers, J.; Mayer-Davis, E.J.; Lawrence, J.M.; Isom, S.; Dabelea, D.; Dolan, L.; Imperatore, G.; Marcovina, S.; Pettitt, D.J.; Pihoker, C.; et al. Trends in Incidence of Type 1 and Type 2 Diabetes Among Youths — Selected Counties and Indian Reservations, United States. MMWR. Morb. Mortal. Wkly. Rep. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ogle, G.D.; Wang, F.; Haynes, A.; Gregory, G.A.; King, T.W.; Deng, K.; Dabelea, D.; James, S.; Jenkins, A.J.; Li, X.; et al. Global Type 1 Diabetes Prevalence, Incidence, and Mortality Estimates 2025: Results from the International Diabetes Federation Atlas, 11th Edition, and the T1D Index Version 3.0. Diabetes Res. Clin. Pract. 2025, 225, 112277. [Google Scholar] [CrossRef]
- Roep, B.O.; Thomaidou, S.; van Tienhoven, R.; Zaldumbide, A. Type 1 Diabetes Mellitus as a Disease of the β-Cell (Do Not Blame the Immune System?). Nat. Rev. Endocrinol. 2021. [Google Scholar] [CrossRef]
- Rider, J.M. Treatment Considerations and Options for the Management of Diabetes Mellitus. J. Pharm. Pract. 2004. [Google Scholar] [CrossRef]
- Lascar, N.; Brown, J.; Pattison, H.; Barnett, A.H.; Bailey, C.J.; Bellary, S. Type 2 Diabetes in Adolescents and Young Adults. Lancet Diabetes Endocrinol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Gangwar, R.; Ahmad Zargar, A.; Kumar, R.; Sharma, A. Prevalence of Diabetes in India: A Review of IDF Diabetes Atlas 10th Edition. Curr. Diabetes Rev. 2023. [Google Scholar] [CrossRef]
- Hossain, M.J.; Al-Mamun, M.; Islam, M.R. Diabetes Mellitus, the Fastest Growing Global Public Health Concern: Early Detection Should Be Focused. Heal. Sci. Reports 2024. [Google Scholar] [CrossRef]
- Wilmot, E.; Idris, I. Early Onset Type 2 Diabetes: Risk Factors, Clinical Impact and Management. Ther. Adv. Chronic Dis. 2014. [Google Scholar] [CrossRef]
- Brauer, M.; Roth, G.A.; Aravkin, A.Y.; Zheng, P.; Abate, K.H.; Abate, Y.H.; Abbafati, C.; Abbasgholizadeh, R.; Abbasi, M.A.; Abbasian, M.; et al. Global Burden and Strength of Evidence for 88 Risk Factors in 204 Countries and 811 Subnational Locations, 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2162–2203. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.L.; Maahs, D.M.; Garvey, K.C.; Hood, K.K.; Laffel, L.M.; Weinzimer, S.A.; Wolfsdorf, J.I.; Schatz, D. Type 1 Diabetes in Children and Adolescents: A Position Statement by the American Diabetes Association. In Diabetes Care; 2018. [Google Scholar]
- Atkinson, M.A.; Eisenbarth, G.S.; Michels, A.W. Type 1 Diabetes. Lancet 2014. [Google Scholar] [CrossRef] [PubMed]
- Bobadilla-Olaje, G.F.; Calleja-López, J.R.T.; Ruibal-Tavares, E.; Rivera-Rosas, C.N.; Aguilera-Duarte, L.J. Maturity-Onset Diabetes of the Young (MODY). Rev. Mex. Pediatr. 2022. [Google Scholar] [CrossRef]
- Soheilipour, F.; Kasbi, N.A.; Imankhan, M.; Eskandari, D. Complications and Treatment of Early-Onset Type 2 Diabetes. Int. J. Endocrinol. Metab. 2023, 21. [Google Scholar] [CrossRef]
- Kautzky-Willer, A.; Harreiter, J.; Pacini, G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Lotstein, D.S.; Seid, M.; Klingensmith, G.; Case, D.; Lawrence, J.M.; Pihoker, C.; Dabelea, D.; Mayer-Davis, E.J.; Gilliam, L.K.; Corathers, S.; et al. Transition from Pediatric to Adult Care for Youth Diagnosed with Type 1 Diabetes in Adolescence. Pediatrics 2013. [Google Scholar] [CrossRef]
- Pacifico, L.; Poggiogalle, E.; Cantisani, V.; Menichini, G.; Ricci, P.; Ferraro, F.; Chiesa, C. Pediatric Nonalcoholic Fatty Liver Disease: A Clinical and Laboratory Challenge. World J. Hepatol. 2010. [Google Scholar] [CrossRef]
- Elsayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes—2023. Diabetes Care 2023. [Google Scholar] [CrossRef]
- Sacks, D.B. A1C versus Glucose Testing: A Comparison. In Diabetes Care; 2011. [Google Scholar]
- Sacks, D.B.; Arnold, M.; Bakris, G.L.; Bruns, D.E.; Horvath, A.R.; Lernmark, Å.; Metzger, B.E.; Nathan, D.M.; Kirkman, M.S. Guidelines and Recommendations for Laboratory Analysis in the Diagnosis and Management of Diabetes Mellitus. Diabetes Care 2023. [Google Scholar] [CrossRef]
- Elliott, T.L.; Pfotenhauer, K.M. Classification and Diagnosis of Diabetes. Prim. Care - Clin. Off. Pract. 2022. [Google Scholar] [CrossRef]
- Rodbard, H.W. Diabetes Screening, Diagnosis, and Therapy in Pediatric Patients with Type 2 Diabetes CME/CE. In MedGenMed Medscape Gen. Med.; 2008. [Google Scholar]
- Seino, Y.; Nanjo, K.; Tajim, N.; Kadowaki, T.; Kashiwagi, A.; Araki, E.; Ito, C.; Inagaki, N.; Iwamoto, Y.; Kasuga, M.; et al. Report of the Committee on the Classification and Diagnostic Criteria of Diabetes Mellitus. J. Diabetes Investig. 2010. [Google Scholar] [CrossRef]
- Wang, H.; Li, N.; Chivese, T.; Werfalli, M.; Sun, H.; Yuen, L.; Hoegfeldt, C.A.; Elise Powe, C.; Immanuel, J.; Karuranga, S.; et al. IDF Diabetes Atlas: Estimation of Global and Regional Gestational Diabetes Mellitus Prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diabetes Res. Clin. Pract. 2022. [Google Scholar] [CrossRef]
- Davidson, M.B.; Schriger, D.L. Effect of Age and Race/Ethnicity on HbA1c Levels in People without Known Diabetes Mellitus: Implications for the Diagnosis of Diabetes. Diabetes Res. Clin. Pract. 2010. [Google Scholar] [CrossRef] [PubMed]
- Abebe, K.Z.; Scifres, C.; Simhan, H.N.; Day, N.; Catalano, P.; Bodnar, L.M.; Costacou, T.; Matthew, D.; Illes, A.; Orris, S.; et al. Comparison of Two Screening Strategies for Gestational Diabetes (GDM2) Trial: Design and Rationale. Contemp. Clin. Trials 2017. [Google Scholar] [CrossRef]
- Dallo, F.J.; Weller, S.C. Effectiveness of Diabetes Mellitus Screening Recommendations. Proc. Natl. Acad. Sci. U. S. A., 2003. [Google Scholar] [CrossRef]
- Wing, R.R.; Goldstein, M.G.; Acton, K.J.; Birch, L.L.; Jakicic, J.M.; Sallis, J.F.; Smith-West, D.; Jeffery, R.W.; Surwit, R.S. Behavioral Science Research in Diabetes: Lifestyle Changes Related to Obesity, Eating Behavior, and Physical Activity. In Diabetes Care; 2001. [Google Scholar]
- Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Care in Diabetes—2024. Diabetes Care 2024. [CrossRef]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of Type 2 Diabetes Mellitus by Changes in Lifestyle among Subjects with Impaired Glucose Tolerance. N. Engl. J. Med. 2001. [Google Scholar] [CrossRef] [PubMed]
- Reduction of the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin. In Int. Urol. Nephrol.; 2002.
- Esposito, K.; Maiorino, M.I.; Ceriello, A.; Giugliano, D. Prevention and Control of Type 2 Diabetes by Mediterranean Diet: A Systematic Review. Diabetes Res. Clin. Pract. 2010. [Google Scholar] [CrossRef]
- Ross, R.; Chaput, J.P.; Giangregorio, L.M.; Janssen, I.; Saunders, T.J.; Kho, M.E.; Poitras, V.J.; Tomasone, J.R.; El-Kotob, R.; McLaughlin, E.C.; et al. Canadian 24-Hour Movement Guidelines for Adults Aged 18-64 Years and Adults Aged 65 Years or Older: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. In Proceedings of the Applied physiology, nutrition, and metabolism = Physiologie appliquee, nutrition et metabolisme, 2020. [Google Scholar]
- Cardiovascular Effects of Intensive Lifestyle Intervention in Type 2 Diabetes. Zeitschrift fur Gefassmedizin 2013.
- Qin, Y.; Aqeel, M.; Zhu, F.; Delp, E.J.; Eicher-Miller, H.A. Dietary Aspects to Incorporate in the Creation of a Mobile Image-Based Dietary Assessment Tool to Manage and Improve Diabetes. Nutrients 2021. [Google Scholar] [CrossRef]
- Sassi, F.; Cecchini, M.; Lauer, J.; Chisholm, D. IMPROVING LIFESTYLES, TACKLING OBESITY: THE HEALTH AND ECONOMIC IMPACT OF PREVENTION STRATEGIES. In OECD Heal. Work. Pap.; 2009. [Google Scholar]
- Malpass, A.; Andrews, R.; Turner, K.M. Patients with Type 2 Diabetes Experiences of Making Multiple Lifestyle Changes: A Qualitative Study. Patient Educ. Couns. 2009. [Google Scholar] [CrossRef]
- Goudy, K.S.; Tisch, R. Immunotherapy for the Prevention and Treatment of Type 1 Diabetes. Int. Rev. Immunol. 2005. [Google Scholar] [CrossRef]
- Candido, R.; Wyne, K.; Romoli, E. A Review of Basal-Bolus Therapy Using Insulin Glargine and Insulin Lispro in the Management of Diabetes Mellitus. Diabetes Ther. 2018. [Google Scholar] [CrossRef]
- Cengiz, E.; Sherr, J.L.; Weinzimer, S.A.; Tamborlane, W. V. New-Generation Diabetes Management: Glucose Sensor-Augmented Insulin Pump Therapy. Expert Rev. Med. Devices 2011. [Google Scholar] [CrossRef]
- Passerini, L.; Forlani, A.; Gregori, S. Advances in Regulatory Cell Therapy for Type 1 Diabetes: Emerging Strategies and Future Directions. Eur. J. Immunol. 2025, 55, 1–9. [Google Scholar] [CrossRef]
- Sherr, J.L.; Heinemann, L.; Fleming, G.A.; Bergenstal, R.M.; Bruttomesso, D.; Hanaire, H.; Holl, R.W.; Petrie, J.R.; Peters, A.L.; Evans, M. Automated Insulin Delivery: Benefits, Challenges, and Recommendations. A Consensus Report of the Joint Diabetes Technology Working Group of the European Association for the Study of Diabetes and the American Diabetes Association. Diabetologia 2023. [Google Scholar] [CrossRef]
- Padhi, S.; Nayak, A.K.; Behera, A. Type II Diabetes Mellitus: A Review on Recent Drug Based Therapeutics. In Biomed. Pharmacother.; 2020. [Google Scholar]
- Feingold, K.R. Oral and Injectable (Non-Insulin) Pharmacological Agents for Type 2 Diabetes; 2000. [Google Scholar]
- Padda, I.S.; Mahtani, A.U.; Parmar, M. Sodium-Glucose Transport Protein 2 (SGLT2) Inhibitors; 2022. [Google Scholar]
- Kalra, S.; Kesavadev, J.; Chadha, M.; Vijaya Kumar, G. Sodium-Glucose Cotransporter-2 Inhibitors in Combination with Other Glucose-Lowering Agents for the Treatment of Type 2 Diabetes Mellitus. Indian J. Endocrinol. Metab. 2018. [Google Scholar] [CrossRef] [PubMed]
- Blonde, L.; Dipp, S.; Cadena, D. Combination Glucose-Lowering Therapy Plans in T2DM: Case-Based Considerations. Adv. Ther. 2018. [Google Scholar]
- Bae, J.H. SGLT2 Inhibitors and GLP-1 Receptor Agonists in Diabetic Kidney Disease: Evolving Evidence and Clinical Application. Diabetes Metab. J. 2025, 49, 386–402. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, M.L.; Williams, D.M.; O’Neil, L.K.; Hayes, J.; Stephens, J.W.; Bracken, R.M. Physical Exercise and Non-Insulin Glucose-Lowering Therapies in the Management of Type 2 Diabetes Mellitus: A Clinical Review. Diabet. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Groop, L.; Widén, E.; Franssila-Kallunki, A.; Ekstrand, A.; Saloranta, C.; Schalin, C.; Eriksson, J. Different Effects of Insulin and Oral Antidiabetic Agents on Glucose and Energy Metabolism in Type 2 (Non-Insulin-Dependent) Diabetes Mellitus. Diabetologia 1989. [Google Scholar] [CrossRef]
- Easa, N.; Alany, R.G.; Carew, M.; Vangala, A. A Review of Non-Invasive Insulin Delivery Systems for Diabetes Therapy in Clinical Trials over the Past Decade. Drug Discov. Today 2019. [Google Scholar] [CrossRef]
- Zahid, M.; Dowlatshahi, S.; Kansara, A.H.; Sadhu, A.R. The Evolution of Diabetes Technology – Options Toward Personalized Care. Endocr. Pract. 2023. [Google Scholar] [CrossRef]
- Marks, B.E.; Williams, K.M.; Sherwood, J.S.; Putman, M.S. Practical Aspects of Diabetes Technology Use: Continuous Glucose Monitors, Insulin Pumps, and Automated Insulin Delivery Systems. J. Clin. Transl. Endocrinol. 2022. [Google Scholar] [CrossRef]
- Forlenza, G.P.; Buckingham, B.; Maahs, D.M. Progress in Diabetes Technology: Developments in Insulin Pumps, Continuous Glucose Monitors, and Progress towards the Artificial Pancreas. J. Pediatr. 2016. [Google Scholar] [CrossRef]
- Aleppo, G.; Webb, K.M. Integrated Insulin Pump and Continuous Glucose Monitoring Technology in Diabetes Care Today: A Perspective of Real-Life Experience with the MinimedTM 670G Hybrid Closed-Loop System. Endocr. Pract. 2018. [Google Scholar] [CrossRef] [PubMed]
- Pauley, M.E.; Tommerdahl, K.L.; Snell-Bergeon, J.K.; Forlenza, G.P. Continuous Glucose Monitor, Insulin Pump, and Automated Insulin Delivery Therapies for Type 1 Diabetes: An Update on Potential for Cardiovascular Benefits. Curr. Cardiol. Rep. 2022. [Google Scholar] [CrossRef]
- Klonoff, D.C.; Ahn, D.; Drincic, A. Continuous Glucose Monitoring: A Review of the Technology and Clinical Use. Diabetes Res. Clin. Pract. 2017. [Google Scholar] [CrossRef] [PubMed]
- Almurashi, A.M.; Rodriguez, E.; Garg, S.K. Emerging Diabetes Technologies: Continuous Glucose Monitors/Artificial Pancreases. J. Indian Inst. Sci. 2023. [Google Scholar] [CrossRef]
- Anandhakrishnan, A.; Hussain, S. Automating Insulin Delivery through Pump and Continuous Glucose Monitoring Connectivity: Maximizing Opportunities to Improve Outcomes. Diabetes, Obes. Metab. 2024, 26, 27–46. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, J.; Thomas, I.H.; Soleimanpour, S.A. Transition from Pediatric to Adult Care in Emerging Adults with Type 1 Diabetes: A Blueprint for Effective Receivership. Clin. Diabetes Endocrinol. 2019. [Google Scholar] [CrossRef]
- Peters, A.; Laffel, L. Diabetes Care for Emerging Adults: Recommendations for Transition from Pediatric to Adult Diabetes Care Systems. Diabetes Care 2012. [Google Scholar]
- Moses, J.; Kim, S.C. Transition from Pediatric to Adult Care. In Pediatric Inflammatory Bowel Disease; 2023; ISBN 9783031147449. [Google Scholar]
- Rajchert, J.; Rosa, M.; Pawłowska, J.; Parczewski, M.; Wawrzynowicz-Syczewska, M. Follow-up of Pediatric Liver Transplant Patients after Reaching Adulthood. Ann. Transplant. 2016. [Google Scholar] [CrossRef]
- O’Higgins, A.; Sebba, J.; Luke, N. What Is the Relationship between Being in Care and the Educational Outcomes of Children? Child Fam. Soc. Work 2015. [Google Scholar]
- White, P.H.; Cooley, W.C. Supporting the Health Care Transition from Adolescence to Adulthood in the Medical Home. Pediatrics 2018. [Google Scholar] [CrossRef]
- Mangoulia, P.; Milionis, C.; Vlachou, E.; Ilias, I. The Interrelationship between Diabetes Mellitus and Emotional Well-Being: Current Concepts and Future Prospects. Healthc. 2024, 12. [Google Scholar] [CrossRef] [PubMed]
- Kalra, S.; Jena, B.N.; Yeravdekar, R. Emotional and Psychological Needs of People with Diabetes. Indian J. Endocrinol. Metab. 2018. [Google Scholar]
- Chew, B.-H. Psychological Aspects of Diabetes Care: Effecting Behavioral Change in Patients. World J. Diabetes 2014. [Google Scholar] [CrossRef]
- Davies, M. Psychological Aspects of Diabetes Management. In Med. (United Kingdom); 2022. [Google Scholar]
- Tareen, R.S.; Tareen, K. Psychosocial Aspects of Diabetes Management: Dilemma of Diabetes Distress; Pediatr., 2017. [Google Scholar]
- Adili, F.; Larijani, B.; Haghighatpanah, M. Diabetic Patients: Psychological Aspects. In Proceedings of the Annals of the New York Academy of Sciences, 2006. [Google Scholar]
- Winterdijk, P.; Aanstoot, H.J.; Nefs, G. The Impact of Real-Time Sensor Technology on Quality of Life for Adults with Type 1 Diabetes: A Dutch National Survey. Diabetes Res. Clin. Pract. 2023. [Google Scholar] [CrossRef]
- de Wit, M.; Gajewska, K.A.; Goethals, E.R.; McDarby, V.; Zhao, X.; Hapunda, G.; Delamater, A.M.; DiMeglio, L.A. ISPAD Clinical Practice Consensus Guidelines 2022: Psychological Care of Children, Adolescents and Young Adults with Diabetes. Pediatr. Diabetes 2022. [Google Scholar] [CrossRef]
- Young-Hyman, D.; De Groot, M.; Hill-Briggs, F.; Gonzalez, J.S.; Hood, K.; Peyrot, M. Psychosocial Care for People with Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016. [Google Scholar] [CrossRef]
- Ansari, M.A.; Chauhan, W.; Shoaib, S.; Alyahya, S.A.; Ali, M.; Ashraf, H.; Alomary, M.N.; Al-Suhaimi, E.A. Emerging Therapeutic Options in the Management of Diabetes: Recent Trends, Challenges and Future Directions. Int. J. Obes. 2023. [Google Scholar] [CrossRef] [PubMed]
- Wagman, A.S.; Nuss, J.M. Current Therapies and Emerging Targets for the Treatment of Diabetes. Front. Med. Chem. - Online 2005. [Google Scholar] [CrossRef]
- Kąpa, M.; Koryciarz, I.; Kustosik, N.; Jurowski, P.; Pniakowska, Z. Future Directions in Diabetic Retinopathy Treatment: Stem Cell Therapy, Nanotechnology, and PPARα Modulation. J. Clin. Med. 2025, 14. [Google Scholar] [CrossRef]
- Sharma, R.; Borah, S.J.; Bhawna, N.; Kumar, S.; Gupta, A.; Kumari, V.; Kumar, R.; Dubey, K.K.; Kumar, V. Emerging Trends in Nano-Based Antidiabetic Therapeutics: A Path to Effective Diabetes Management. Mater. Adv. 2023. [Google Scholar] [CrossRef]
- Kopan, C.; Tucker, T.; Alexander, M.; Mohammadi, M.R.; Pone, E.; Lakey, J.R.T. Approaches in Immunotherapy, Regenerative Medicine, and Bioengineering for Type 1 Diabetes. Front. Immunol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D. Antiplatelet Therapy in Diabetes: Efficacy and Limitations of Current Treatment Strategies and Future Directions. In Diabetes Care; 2009. [Google Scholar]
- Pimenta, C.; Bettiol, V.; Alencar-Silva, T.; Franco, O.L.; Pogue, R.; Carvalho, J.L.; Felipe, M.S.S. Advanced Therapies and Regulatory Framework in Different Areas of the Globe: Past, Present, and Future. Clin. Ther. 2021. [Google Scholar] [CrossRef] [PubMed]
- Guan, Z.; Li, H.; Liu, R.; Cai, C.; Liu, Y.; Li, J.; Wang, X.; Huang, S.; Wu, L.; Liu, D.; et al. Artificial Intelligence in Diabetes Management: Advancements, Opportunities, and Challenges. Cell Reports Med. 2023. [Google Scholar] [CrossRef]
Figure 1.
Comparison of pediatric and adult diabetes showing age-specific pathophysiology, with faster progression and more aggressive disease in children.
Figure 1.
Comparison of pediatric and adult diabetes showing age-specific pathophysiology, with faster progression and more aggressive disease in children.
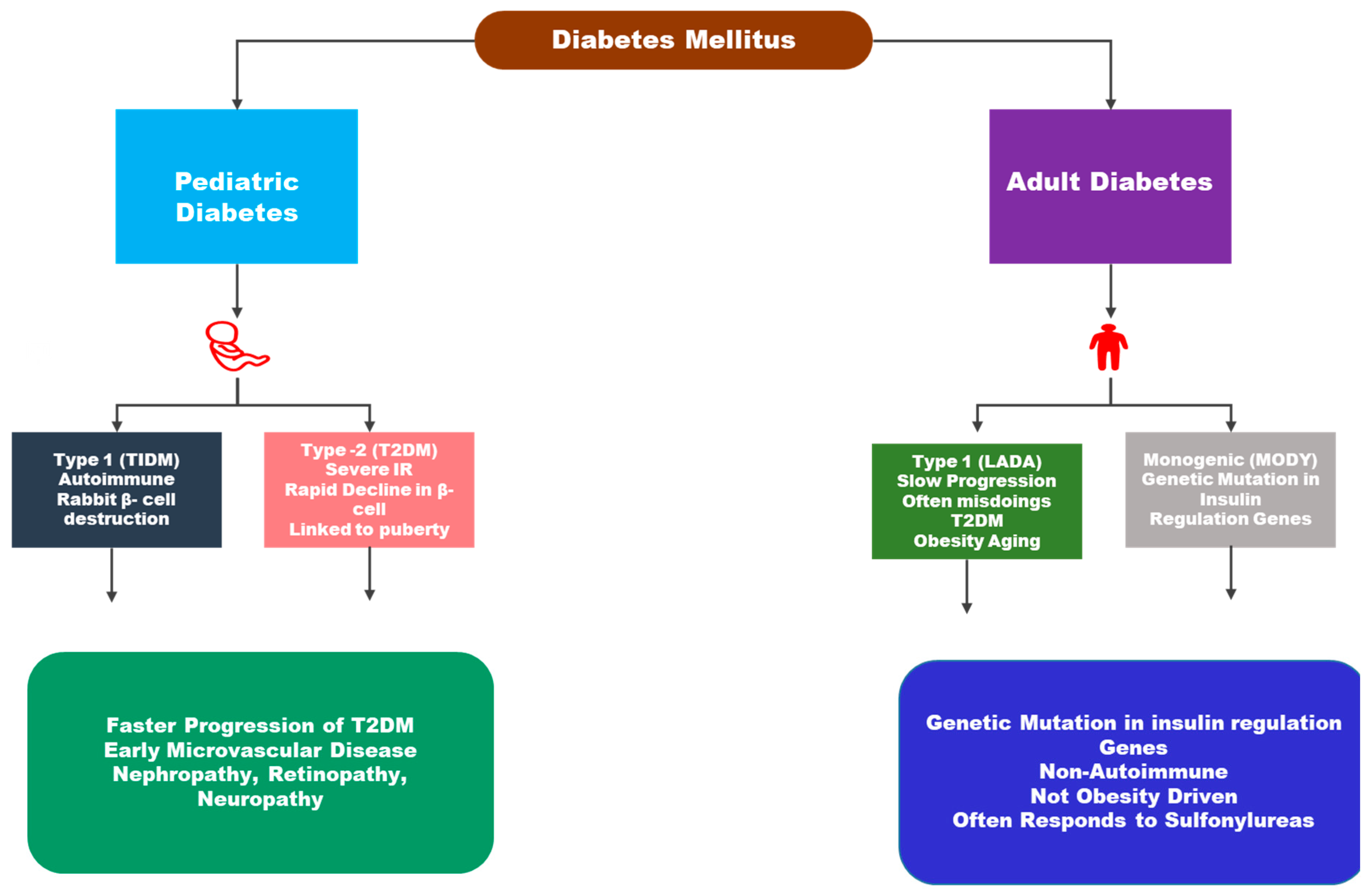
Figure 2.
Overview of diagnostic criteria and age-specific screening strategies for diabetes, emphasizing variability across children, adults, elderly, and pregnant populations.
Figure 2.
Overview of diagnostic criteria and age-specific screening strategies for diabetes, emphasizing variability across children, adults, elderly, and pregnant populations.
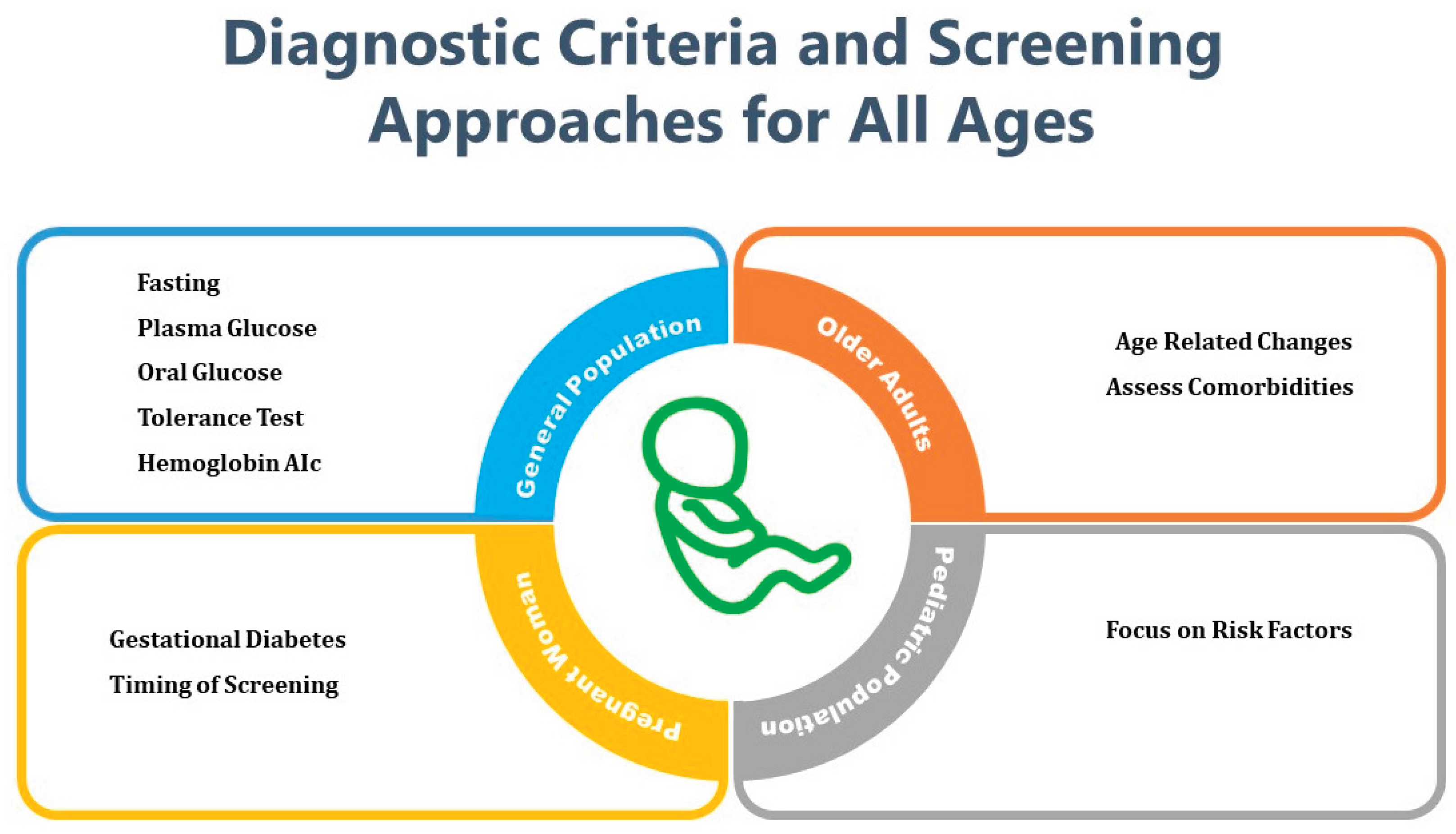

Table 1.
Integrated strategies for the diagnosis and management of diabetes in children and adults: Updates on medications, insulin therapies, and nutritional approaches.
Table 1.
Integrated strategies for the diagnosis and management of diabetes in children and adults: Updates on medications, insulin therapies, and nutritional approaches.
| Component | Pediatric (Children) Population | Adult Population | Recent Advances |
| Diagnostic Approaches |
- HbA1c, Fasting Blood Glucose, OGTT- Autoantibody Testing (T1DM)- Genetic Testing (MODY) | - HbA1c, OGTT, Fasting Glucose- Risk Scoring Tools (e.g., ADA, FINDRISC)- Retinal and Renal Screening | - Continuous Glucose Monitoring (CGM)- AI-based Predictive Tools- Non-invasive Glucose Sensors |
| Insulin Therapy | - Multiple Daily Injections (MDI)- Insulin Pumps- Hybrid Closed-Loop Systems | - MDI or Premixed Insulin- Long-acting and Ultra-long-acting Analogues | - Smart Insulin Delivery Systems- Artificial Pancreas Systems- Personalized Insulin Algorithms |
| Pharmacologic Interventions | - Metformin (in pediatric T2DM)- GLP-1 Receptor Agonists (limited use) | - Metformin, SGLT2 Inhibitors, DPP-4 Inhibitors, GLP-1 RAs, Thiazolidinediones | - Dual GIP/GLP-1 Agonists (e.g., Tirzepatide)- Expanded use of SGLT2 inhibitors in T1DM (investigational) |
| Dietary Management | - Carbohydrate Counting- Low-Glycemic Index Diets- Parental Education Programs | - Mediterranean, DASH, or Low-Carb Diets- Structured Meal Planning | - Personalized Nutrition via CGM Data- Gut Microbiota-Based Dietary Modulation |
| Lifestyle Modifications | - Age-appropriate Exercise Programs- School and Family Engagement | - Structured Physical Activity- Smoking and Alcohol Cessation | - Mobile Health (mHealth) Tools- Digital Coaching Platforms- Behavioral Modification Apps |
| Monitoring and Follow-Up | - Pediatric Endocrinologist Follow-up- Monitoring of Growth and Puberty | - Routine Monitoring for Complications (CVD, Nephropathy, Retinopathy) | - Remote Patient Monitoring- Integrated EHR Systems with Predictive Analytics |
| Complication Prevention | - Early Screening for Microvascular Complications- Vaccination Compliance | - Cardiometabolic Risk Control- Nephropathy and Neuropathy Screening | - Use of Novel Biomarkers- Early Intervention with Renoprotective and Cardioprotective Drugs |
Table 2.
Advances in drug, insulin, and dietary interventions in the management of diabetes in children and adults.
Table 2.
Advances in drug, insulin, and dietary interventions in the management of diabetes in children and adults.
| Intervention | Target Group | Advantages | Disadvantages |
| Metformin | Adults | - First-line for Type 2 diabetes- Weight neutral or slight loss- Cardiovascular benefits | - GI side effects- Lactic acidosis (rare)- Contraindicated in renal impairment |
| Children (≥10 yrs) | - Approved for pediatric Type 2 diabetes- Delays insulin initiation | - GI intolerance- Limited monotherapy efficacy in some children | |
| Sulfonylureas | Adults | - Cost-effective- Rapid glucose reduction | - High risk of hypoglycemia- Weight gain |
| Children | - Used in neonatal and MODY forms of diabetes | - Not typically first-line- Risk of hypoglycemia | |
| DPP-4 Inhibitors | Adults | - Well-tolerated- No weight gain- Low hypoglycemia risk | - Moderate efficacy- Expensive |
| Children | - Limited pediatric data | - Off-label use in most settings- Cost-prohibitive in some regions | |
| SGLT2 Inhibitors | Adults | - Promotes weight loss- Cardiovascular and renal benefits | - Genital infections- Risk of ketoacidosis |
| Children (>10 yrs) | - Emerging evidence in adolescents- FDA approval for dapagliflozin (2023) | - Long-term safety unknown- Risk of dehydration and DKA | |
| GLP-1 Receptor Agonists |
Adults | - Weight loss- Improved cardiovascular outcomes- Delays insulin requirement | - Injectable- GI side effects- Expensive |
| Children (≥10 yrs) | - FDA-approved for pediatric Type 2 diabetes (liraglutide, 2020) | - GI intolerance- Fear of injection- High cost | |
| Basal-Bolus Insulin | Adults | - Flexible dosing- Better postprandial control | - Frequent injections- Hypoglycemia risk- Weight gain |
| Children | - Essential for Type 1 diabetes- Mimics physiologic insulin profile | - Requires strong parental involvement- Psychosocial burden | |
| Insulin Pumps (CSII) | Adults | - Improved glycemic control- Reduced variability- Quality of life | - High cost- Technical learning curve- Risk of DKA if malfunction |
| Children | - Enhanced quality of life- Better HbA1c control in some studies | - Device burden- Requires family support and monitoring | |
| Closed-Loop Systems | Adults | - Automated insulin delivery- Reduces hypo- and hyperglycemia | - Very expensive- Requires CGM calibration |
| Children | - Safe in children ≥6 yrs (e.g., MiniMed 780G)- Reduces parental stress | - High initial cost- Sensor wear and data interpretation challenges | |
| Low-Glycemic Index Diet | Adults | - Improves postprandial glucose- Sustainable eating habits | - Requires dietary planning- May conflict with cultural preferences |
| Children | - Prevents glucose spikes- Can be incorporated into school lunches | - Adherence challenges- Peer influence | |
| Carbohydrate Counting | Adults | - Supports flexible insulin dosing- Better control with bolus insulin | - Requires nutritional literacy- Time-consuming |
| Children | - Educational tool for families- Encourages healthy food choices | - Requires constant parental involvement- Difficult in social settings (e.g., school, parties) | |
| Mediterranean Diet | Adults | - Cardioprotective- Rich in fiber and healthy fats | - Can be expensive- May require lifestyle shift |
| Children | - Family-friendly and balanced | - Adherence in picky eaters or selective diets can be difficult |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



