Submitted:
02 February 2026
Posted:
04 February 2026
You are already at the latest version
Abstract
Epileptic activities can affect various aspects including neuropsychological and social functions, which lead to reductions of quality of life (QOL) for epileptic children. Accordingly, epileptic children are generally at greater risk of neuropsychological and social dysfunctions than those without epilepsy, even though the majority of epileptic children achieve favorable outcomes. Social function in epileptic children can be negatively impacted due to emotional instability, including stigma associated with having epilepsy. The parents of children with refractory epilepsy could experience severe anxiety regarding clinical seizures in their children, and this severe parental anxiety state could lead to adaptable dysfunction in their children. Moreover, associations between epilepsy and fatigue or headache are well known to clinicians but insufficiently understood. A deeper understanding of these issues in epilepsy could be important for managing the clinical course and treatment regimen. Seizure activities could be associated with impaired neuropsychological/social functions as represented by stigma, fatigue, and headache. Seizure severities are thus important QOL-related factors in terms of neuropsychological and social issues in epileptic children. A relationship between current seizure activity and perception of stigma could be evident in epileptic children. Seizure activity represented as frequent seizures could also be related to fatigue and seizure-associated headache, which can lead to reduced QOL in children with epilepsy. In addition, seizure-related factors in epileptic children including frequent seizures could lead to greater perception of stigma in their parents. Meanwhile, educational intervention about epilepsy for parents could reduce negative emotional influences in the care of children presenting with seizure attacks. Therapeutic management thus appears desirable to immediately obtain better seizure control and establish educational support for parents to improve QOL in children with epilepsy.
Keywords:
stigma
; fatigue
; headache
; seizure activity
; educational support
; quality of life (QOL)
1. Introduction
Seizure activities can affect various aspects including neuropsychological and social functions, which can reduce quality of life (QOL) in epileptic children. In particular, stigma could be a principal psychological issue for adults and children with epilepsy. In general, stigma and exclusion are considered as common features of epilepsy representing as principal issues in the psychosocial problems associated with the condition. Stigma could deteriorate social functions, including relationships around the development and maintenance of self-respect, leading to unfavorable outcomes such as isolation, high rates of unemployment and remaining unmarried, and delayed intervention [1]. Epilepsy is a disorder with social dysfunctions and should therefore not be regarded as solely a neurological disorder.
The majority of epileptic children can achieve favorable outcomes. However, epileptic children generally experience a higher risk of neuropsychological and social dysfunction than those without epilepsy. In particular, epilepsy can stigmatize adolescents and disturb psychosocial development in terms of issues such as independence, self-esteem, peer relations, mood, and cognition due to their psychological vulnerability [2]. Unfavorable influences on social function may arise in epileptic children due to emotional instability, including stigma associated with having epilepsy, so epilepsy can have major impacts on various aspects of a child’s life [3].
Meanwhile, parenting-related stress can lead to parenting dysfunction [4,5]. Epilepsy in children, particularly refractory epilepsy, involves a high risk of parenting dysfunction [6,7,8,9]. Parents of children with refractory epilepsy could show a severe anxiety state regarding clinical seizures in their children, and this severe parental anxiety state could lead to adaptable dysfunction in their children [10]. Accordingly, the clinical manifestations or severity of epilepsy in children may have major impacts on QOL from the perspective of parenting stress [11].
On the other hand, fatigue can also lead to reduced QOL among individuals with chronic neurological diseases and disorders, including epilepsy [12,13,14,15]. Fatigue is regarded as a mental and/or physical state of extreme and persistent weakness, tiredness, or exhaustion [15]. The prevalence of fatigue among individuals with chronic medical conditions is high, but fatigue has been disregarded in the evaluation and management of epileptic children [13]. Although few studies have investigated the problem of fatigue, fatigue could induce seizures [16,17,18], so a better understanding of this issue in epileptic children could be important for management of the clinical course and treatment regimens.
Both epilepsy and headache are common paroxysmal disorders. A relationship between these two disorders is well known to clinicians, but insufficiently understood. Evaluation and management of headaches associated with seizures is often disregarded at the time of eliciting the medical history, because other symptoms including impairment of consciousness or motor phenomenon are predominant in the information. Headache could be evident in association with seizures as preictal, ictal, postictal, or inter-ictal phenomenon, but tends to be disregarded because the clinical features of seizure are very serious [19]. The pathophysiology of seizure-associated headaches remains unclear due to a lack of consideration. Accordingly, the presence of seizure-associated headaches and risk factors in epileptic children needs to be considered.
The frontal cortex matures over a long period of time, and is highly vulnerable due to various factors. Frontal regional damage in children negatively affects the maturation and organization of this area, contributing to neuropsychological impairments including emotional instability [20]. Previous reports have indicated that severe seizures as represented by frequent or prolonged seizures can cause damage to the developing brain [20,21,22,23]. The results of several studies have suggested that seizure severity could lead to impairments of neuropsychological functions as represented by stigma, fatigue, and headache. Seizure severity is thus an important QOL-related factor in terms of social and neuropsychological aspects in children with epilepsy.
2. Can epileptic activities affect the emotional state in children with epilepsy?
2.1. Relationship between seizure activities and perception of stigma
Most epileptic children can obtain favorable outcomes concerned with clinical seizures. However, individuals with epilepsy, including children, could be at significant risk of neuropsychological impairments and tend to show social dysfunctions more frequently than those without epilepsy. Clinical seizures in most children cannot go on indefinitely, but unforeseen events could give a sense of fear to the public for epilepsy [24]. In particular, epilepsy could stigmatize young people and contribute to neuropsychological and social dysfunctions [2]. Social identity in epileptic children could thus be negatively affected due to stigma associated with having epilepsy. The social impact of stigma due to epilepsy could indeed prove more significant than the actual neurological condition itself in some cases [23].
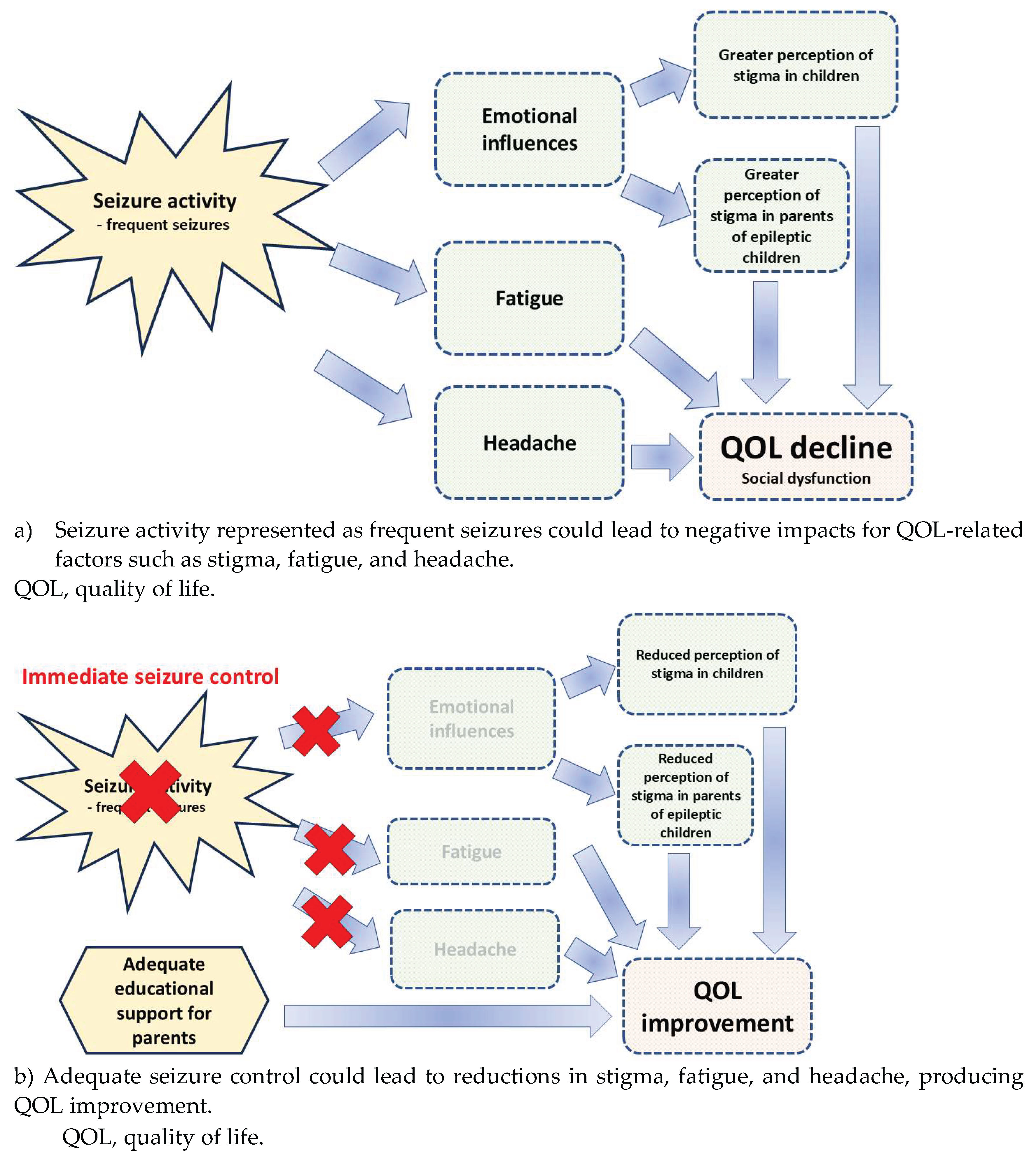
The principal aims of epilepsy management should be established so that children with epilepsy can maintain a seizure-free state with well-tolerated treatment [25]. Various studies also suggest that reduction of negative aspects, including stigma in epileptic children, seems to be an important aim of attending a patient [25,26]. How clinical seizures could influence the perception of stigma in epileptic children remains insufficiently investigated. Perception of stigma can depend on national characteristics and cultures, so this issue needs to be confirmed by country or region. In our previous study, a relationship between seizure activities and perception of stigma was evaluated using the Child Stigma Scale (CSS) [27] in Japanese epileptic children between 12 and 18 years old [28]. In CSS, children rate how often they feel or experience stigma using items scored on a 5-point scale: 1, “never”; 2, “not often”; 3, “sometimes”; 4, “often”; or 5, “very often”. Scores are summed and divided by the number of items scored, as detailed by Austin et al. [27]. With the CSS, higher scores indicate a greater degree of stigma. The results of that study revealed that children presenting with frequent seizures recognized themselves as significantly more stigmatized compared to those in a less-frequent or seizure-free state (p < 0.01) [28] (Table 1). Such findings suggest a relationship between current seizure activity and perception of stigma (Figure 1a). Children with fewer seizures could have a lower perception of stigma.
2.2. Epileptic activities including EEG abnormality and perceived stigma; are they related?
Associations between neuropsychological functions including emotional state and findings from electroencephalography (EEG) have been indicated. Frontal asymmetrical abnormality on EEG is involved in both a susceptibility to react to emotional stimulation and variations in emotional state [29]. Frontal asymmetrical EEG abnormality could thus lead to neuropsychological impairments, including depression and anxiety [30]. Moreover, neuropsychological dysfunctions including behavioral impairments in neurodevelopmental disorders such as attention deficit/hyperactivity disorder or autism spectrum disorder could be based on the frequency of frontal interictal epileptiform discharges (IEDs) in some children [31,32]. Abnormalities on EEG in frontal regions could thus be associated with emotional and behavioral functions. The results from our previous study showed that children with epilepsy presented with significantly higher CSS scores than non-epileptic children (p < 0.01) [33]. Moreover, a group with frontal IEDs revealed higher CSS scores for all questions compared to scores from other regional IED groups (p < 0.01). That study revealed that children presenting with frontal IEDs perceived a stronger degree of stigma than those presenting with non-frontal IEDs (p < 0.01) [33]. These observations could show a relationship between frontal IEDs and a more significant perception of stigma. Frontal EEG abnormality could function as an emotional mediator including perception of stigma in epileptic children.
2.3. Seizure activities and fatigue in epileptic children; are they related?
Among clinical, statistical and social factors, fatigue is considered to reduce the QOL of epileptic patients [13]. Fatigue can also induce clinical seizures [34]. As fatigue can trigger seizures [17,18], a better comprehension of fatigue among children with epilepsy seems very important in supporting effective management of the clinical course and treatment regimens. Fatigue could be a frequent complaint in general and highly prevalent in epileptic patients, but little consideration has been given to fatigue in the assessment and management of epileptic children [13]. Our previous study evaluated the association between seizure activity and degree of fatigue in epileptic children using the Fatigue Severity Scale (FSS) [35]. The FSS is constructed using nine items that rate fatigue on a scale from 1 (strongly disagree) to 7 (strongly agree) [36]. Epileptic children were required to use a 7-point scale (1 to 7) to rate how often over the previous week they felt the ways shown by the nine items. After summation of the scores, the total score was divided by 9, resulting in values from 1 to 7 [36]. A higher score reflects a greater level of fatigue. That study showed that mean FSS scores were significantly higher in children with epilepsy than in those without (4.40 vs. 1.55, respectively; p < 0.0001). In addition, multiple linear regression analysis revealed seizure frequency as the only clinical manifestation significantly associated with fatigue (p < 0.0001) [35]. Moreover, the same study showed that children with uncontrolled seizures experienced greater fatigue levels than those with well-controlled seizures (p < 0.0001) [35]. These findings indicate that frequent seizures could lead to greater levels of fatigue (Table 1). Seizure activity represented by frequent seizures could correlate with fatigue level in children with epilepsy. Fatigue levels should thus be taken into consideration in children with epilepsy (Figure 1a).
2.4. Seizure activities and headache in epileptic children; are they related?
Both epilepsy and headache are common underlying mechanisms in functional and paroxysmal disorders. Headaches, including migraines and headaches associated with epilepsy are chronic disorders that can have a variety of underlying causes and symptoms, and patients with epilepsy often experience epilepsy-related headaches, including both seizure-related and seizure-unrelated headaches. However, the underlying mechanism of peri-ictal headaches in epilepsy is insufficiently clarified. In general, headaches in children are not yet fully diagnosed and are not appropriately regarded as a medical issue by clinicians [37]. In our previous study of 98 epileptic children and adolescents between 5 and 18 years old, 34 (34.7%) complained of epilepsy-related headaches [38]. Moreover, seizure frequency was 4.1 times per year in children with headaches and 1.3 times per year in those without headaches. That study concluded that epilepsy-related headaches were more frequent in epileptic children than in children with uncontrolled seizures [38] (Table 1). These findings indicate that seizure activity as represented by frequent seizures could be related to the presence of epilepsy-related headache, which can lead to reduced QOL among children with epilepsy (Figure 1a).

Table 1.
Table 1. Seizure activity and QOL-related factors in association with social aspects.
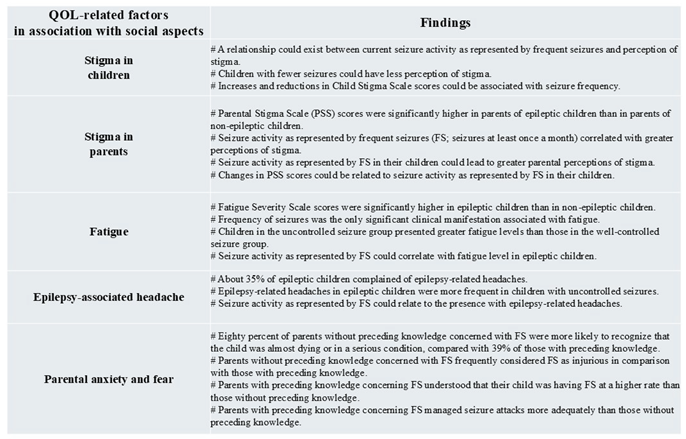 |
QOL, quality of life; CSS, Child Stigma Scale; PSS, Parental Stigma Scale; FS, febrile seizure.
3. Can seizure activities affect the emotional state in parents of epileptic children?
3.1. Fears and anxieties in parents of children presenting with first febrile seizures
Febrile seizures (FS) are a highly prevalent seizure disorder of childhood and show good outcome [39]. However, parents of children with FS may interpret the symptoms as a very shocking occurrence [40]. Insufficient knowledge concerning FS among parents could lead to misunderstandings about the possibilities of undesirable outcomes, including life-threatening illness, brain damage, later development of epilepsy, and tongue biting [41,42,43]. In fact, a child presenting with convulsive symptoms represents a shocking scene to inexperienced parents, who may consider that the child is at high risk of death [44,45]. Although FS is recognized as a highly prevalent disorder with good prognosis [46], significant differences exist between the harmful emotional state of parents and the comparatively insignificant clinical approach of clinicians. Parental fear and anxiety regarding FS can be a critical issue, with serious negative influences affecting daily familial life [44]. Pediatricians and general practitioners may not even be aware of the stress in parents of FS children [46]. In our previous study, 70% (55/78) of the parents of children with simple FS mentioned that they had considered that the child would die during the convulsive attack or conceived the child may be severely injured [47]. In another study, parental stress and stigma were evident within 3 months after convulsive episodes in their children [48]. Such studies indicate that parents could experience inappropriate thoughts and actions due to fears and anxieties. Parental thoughts and actions reflect the fear and anxiety perceived by many parents in cases where their child is experiencing convulsions.
3.2. Seizure activity and perception of stigma in parents of epileptic children; are they related?
Pediatric epileptologists recognizing the influences of stigma accompanying epilepsy seems important, given the necessity for developing and implementing management strategies to achieve better psychosocial health for both epileptic children and their parents. Stigma is a general aspect associated with epilepsy, with substantial negative influences on epileptic children and their parents and harmful effects on QOL. Epileptic patients tend to consider perception of stigma as one of their biggest problems [49]. Epileptic activity and severity could also represent major factors for parenting-related stress [11]. In a previous study [50], we assessed parental stigma in association with epilepsy among the parents of Japanese epileptic children using the Parental Stigma Scale (PSS). In the PSS, parents were required to rate five items in the questionnaire using a 5-point scale: 1, strongly disagree; 2, disagree; 3, neither; 4, agree; and 5, strongly agree. The ultimate score was calculated as the mean of each score, as described by Austin et al. [26]. In that study, PSS scores were higher in the parents of epileptic children than in parents of non-epileptic children [50]. Moreover, that study also showed that seizure activity represented by frequent seizures (defined as seizures at least once a month) correlated with greater perceptions of stigma in multiple regression analysis (p = 0.0036). These findings suggest that seizure activity as represented by frequent seizures in children could lead to greater perceptions of parental stigma [50]. However, other studies have indicated that parenting-related stress did not correlate with seizure frequency in a direct manner [6,9,13]. Papazoglou et al. showed that presence of seizures, regardless of frequency, could lead to adaptive dysfunction in epileptic children [51]. In contrast, our previous study revealed that frequent seizures could affect the perception of stigma in epileptic children [28]. In addition, the perception of stigma could lead to adaptive dysfunction in the child [27]. These findings indicate that frequent seizures could be associated with greater maternal stress (Table 1). Seizure-related factors in epileptic children as represented by frequent seizures could thus lead to greater perception of stigma by parents (Figure 1a).
4. Management and therapeutic approach for children with epilepsy
4.1. Is immediate suppression of clinical seizures needed? Thinking from cognitive and behavioral perspectives
As described above, seizure activity could be associated with several QOL-related factors, including stigma, fatigue, and headache. In addition, seizure activities represented by frequent and prolonged seizures could lead to neuropsychological impairments, including cognitive dysfunction and behavioral disturbances [52,53]. Moreover, recovery of prefrontal lobe growth could rely on periods of high seizure activity. Our previous studies showed that growth of the prefrontal lobe could recover immediately in children with a shorter period of high seizure activity [54,55]. In contrast, this growth disturbance could be prolonged in children with a longer period of high seizure activity [54,55]. Further, prolonged seizures in children could lead to cognitive declines and behavioral disturbance in relation to growth disturbance of the prefrontal lobe [20]. Accordingly, therapeutic management is warranted to reduce clinical seizures immediately and thus avoid neuropsychological impairments in epileptic children.
4.2. Is immediate suppression of clinical seizures needed? Considerations of emotional state in epileptic children
Regarding this issue, immediate suppression of clinical seizures could be applicable to reduce emotional influences, including stigma. In our preliminary study, the relationship between reduction of clinical seizures and CSS scores was evaluated in a patient with frontal lobe epilepsy (FLE).
The clinical course of this patient is outlined briefly, as follows. The patient was a 14-year-old boy in whom psychomotor development was not significant. At 10 years old, he had developed epileptic seizures such as rightward deviation of the head and eyes. Seizures were brief (10–25 s), frequent, and stereotypic. Family history of epilepsy was absent. MRI of the brain revealed no significant findings. Left frontopolar IEDs superimposed on normal background activity were evident on EEG. FLE was diagnosed in accordance with the seizure types and the findings on EEG, including IED location. Carbamazepine was initiated, but failed to control seizures. Zonisamide was added to the treatment regimen, but control of seizures was not achieved. Carbamazepine was thus replaced with levetiracetam (LEV), leading to partial improvement of seizures. Treatment was then changed to perampanel combined with LEV and control of seizures was achieved.
Serial CSS scores were obtained from this patient every 3 months after seizure onset. CSS score was 1.9 at seizure onset. CSS scores then increased to a maximum of 4.4 at 6 months after seizure onset, in parallel with frequent seizures. However, CSS scores decreased gradually with achievement of increasing seizure control. CSS score at 24 months after onset had decreased to 1.5. These results indicate that changes in CSS scores were associated with seizure frequency (Table 1). Therapeutic management is thus desirable to immediately reduce clinical seizures and prevent emotional influences as represented by perception of stigma in epileptic children (Figure 1b).
4.3. Is immediate suppression of clinical seizures needed? Considerations of emotional state in parents of epileptic children
Immediate suppression of clinical seizures could also be applicable to reducing emotional influences, including stigma, in the parents of epileptic children. Our preliminary study evaluated the relationship between reduction of clinical seizures and PSS scores in the mother of an epileptic child.
The clinical course of this patient is outlined as follows. The patient was a 12-year-old boy for whom psychomotor development was not significant. At 10 years old, he experienced epileptic seizures such as impaired awareness and motion arrest. The duration of each seizure was about 45–90 s. Seizures were stereotypical and repeated frequently. A family history of epilepsy was absent. MRI of the brain revealed no significant findings. Diffuse spike-wave complexes superimposed on normal background EEG activity were evident. LEV was initiated, but seizures showed drug resistance. Focal to bilateral tonic-clonic seizures subsequently appeared. No response to administration of lacosamide was seen. Treatment was changed to perampanel combined with LEV, leading to immediate improvements in seizures.
Serial PSS scores were obtained every 3 months after seizure onset from the mother of this patient. PSS score at seizure onset was 2.0. PSS scores increased serially to a maximum of 4.8 at 6 months after seizure onset, in parallel with frequent seizures. However, PSS scores gradually decreased with successful seizure control in her child. PSS score decreased to 1.6 by 18 months after seizures disappeared. These results indicate that changes in PSS scores could be related to seizure activity as represented by frequent seizure in the children (Table 1). Therapeutic management is thus desirable to immediately reduce clinical seizures and prevent emotional influences in the parents of epileptic children (Figure 1b).
4.4. Is an effective educational intervention program needed for parents and the public?
Medical knowledge regarding epilepsy has recently become more widespread. Most epileptic syndromes in children represent benign conditions. However, insufficient comprehension about epilepsy in parents may be exacerbated by mistakes about the risks of brain damage and poor developmental/social outcomes. The cause, associated factors, history of clinical course, and management of epilepsy have been broadly investigated, but parental thoughts and actions after witnessing a seizure attack in their child are not widely known. Enhancing the understanding of parental knowledge and thoughts regarding seizure disorders including epilepsy could improve parent-clinician relationships and enhance the efficacy of the information provided [46]. Our previous study examined parents of 78 children who presented with their first simple-type FS regarding their thoughts and actions [47]. Approximately 77% of parents did not have preceding knowledge about FS. Almost all parents (91%) took the child directly to hospital in an ambulance after a 119-emergency call. In addition, 41% of parents had reported thinking that the child was close to dying due to the seizure attack, and 29% thought that the child was in a serious condition and had suffered severe brain damage [47]. That study also showed that 80% of parents without preceding knowledge of FS were more likely to recognize that the child was almost dying or in a serious condition, compared with 39% among parents with preceding knowledge. Parents without preceding knowledge concerned with FS frequently considered the FS as injurious compared to those with preceding knowledge (p < 0.03) (Table 1). Parents with preceding knowledge about FS understood that the child was experiencing FS at a higher rate than those without preceding knowledge (p < 0.001). Meanwhile, the emotional reaction of the first parent faced with a convulsing child was frequently one of fear and panic. Parents with preceding knowledge about FS managed seizure attacks more adequately than those without this knowledge (p < 0.03) (Table 1). These findings suggest that information concerning FS should be provided to all parents [47].
Similar to FS, knowledge of the care guide for epilepsy could make the management of epilepsy more appropriate for parents. Overall expertise concerned with epilepsy among parents and the public is insufficient and the emotional response of parents to seizure attacks is often serious and continuous. However, in cases with acquisition of knowledge prior to first FS in their child, a significant proportion of parents could recall some knowledge and recognize FS, which eased anxiety and encouraged more appropriate actions [47]. Educational interventions about epilepsy for parents could thus reduce negative emotional influences in the care of children presenting with seizure attacks. Such findings could accentuate the significance of acknowledging and addressing parental emotional responses. Reducing emotional influences including stigma and anxiety in parents through adequate education and awareness that changes perceptions and deepens understanding could be an approach to enhancing parenting function. Coordinating an assistant team and an adequate educational intervention arrangement for parents could also prove important in the care and management of epileptic children (Figure 1b).
Figure 1.
Association between seizure activity and QOL reduction.
5. Future perspectives
As shown in various studies, seizure aggravation including frequent and prolonged seizures could lead to reduced QOL in epileptic children. Adequate seizure control may improve QOL for epileptic children from several neuropsychological and social perspectives. However, interpretation of this aspect may need more consideration. Prompt seizure remission could achieve cognitive and behavioral improvements. Meanwhile, improvement or reduction of other issues, including stigma, fatigue, and headache, using antiseizure medication (ASM) has not yet been sufficiently confirmed. Regarding stigma, increases and reductions in stigma scores of epileptic children and their parents could be associated with seizure activity as represented by seizure frequency. However, this is primarily based on findings from a single case. Accordingly, definitive conclusions cannot yet be drawn. Moreover, associations between reductions in fatigue/headache levels and seizure reduction have not been fully evaluated. Further investigations of a larger cohort are needed to confirm associations between adequate seizure control and improvement of QOL-related factors in children with epilepsy.
6. Conclusions
Neuropsychological impairments and social dysfunction, including emotional instabilities and behavioral disturbances, are not necessarily present in all epileptic children. However, seizure aggravation, including frequent and prolonged seizures, could lead to these negative impacts. Clinicians should concentrate on achieving early seizure remission to prevent such impairments. In addition, coordinating an assistant team and an adequate educational intervention arrangement for parents could also lead to reductions of anxiety and stigma in the parents of epileptic children. According to the findings obtained from various studies, therapeutic management is desirable to immediately reduce clinical seizures and educational support should be established for parents to improve QOL in children with epilepsy.
Acknowledgments
The author thanks FORTE Science Communications (https://www.forte-science.co.jp/) for English language editing.
Declaration of Competing Interest
Dr. Hideaki Kanemura has received speaker’s fees from Eisai Co., Ltd.
References
- Jacoby A, Baker G, Smith D, DeweyM, Chadwick D. Measuring the impact of epilepsy: The development of a novel scale. Epilepsy Res. 1993, 16, 83-88. [CrossRef]
- Devinsky O, Westbrook L, Cramer J, Glassman M, Perrine K, Camfield C. Risk factors for poor health-related quality of life in adolescents with epilepsy. Epilepsia 1999, 40, 1715-1720. [CrossRef]
- Ronen GM, Streiner DL, Rosenbaum P; Canadian Pediatric Epilepsy Network. Health-related quality of life in children with epilepsy: Development and validation of self-report and parent proxy measures. Epilepsia 2003, 44, 598-612. [CrossRef]
- Deater-Deckard K. Parenting stress and child adjustment: some old hypotheses and new questions. Clin. Psychol. (New York) 1998, 5 314–332. [CrossRef]
- Ostberg M, Hagekull B. A structural modeling approach to the understanding of parenting stress. J. Clin. Child. Psychol. 2000, 29, 615–625. [CrossRef]
- Rodenburg R,Meijer AM, DekovicM, Aldenkamp AP. Parents of children with enduring epilepsy: predictions of parenting stress and parenting. Epilepsy Behav. 2007, 11, 197–207. [CrossRef]
- Modi AC. The impact of a new pediatric epilepsy diagnosis on parents: parenting stress and activity patterns. Epilepsy Behav. 2008, 13, 169–173. [CrossRef]
- Chiou HH, Hsieh LP. Parenting stress in patients of children with epilepsy and asthma. J. Child Neurol. 2008, 13, 301–306. [CrossRef]
- Cushner-Weinstein S, Dassoulas K, Salpekar JA, Henderson SE, Pearl PL, GaillardWD, et al. Parenting stress and childhood epilepsy: the impact of depression, learning, and seizure-related factors. Epilepsy Behav. 2008, 23: 109–114. [CrossRef]
- Kerne V, Chapieski L. Adaptive functioning in pediatric epilepsy: contributions of seizure-related variables and parental anxiety. Epilepsy Behav. 2015, 43, 48–52. [CrossRef]
- Braams O, Meekes J, Braun K, Schappin R, van Rijen PC, Hendriks MPH, et al. Parenting stress does not normalize after child's epilepsy surgery. Epilepsy Behav. 2015, 42, 147–152. [CrossRef]
- Vercoulen JH, Hommes OR, Swanink CM et al. The measurement of fatigue in patients with multiple sclerosis. A multidimensional comparison with chronic fatigue syndrome and healthy subjects. Arch. Neurol. 1996, 53, 642–649.
- Dittner AJ, Wessely SC, Brown RG. The assessment of fatigue: A practical guide for clinicians and researchers. J. Psychosom. Res. 2004, 56, 157–170.
- Christensen D, Johnsen SP, Watt T, Harder I, Kirkevold M, Andersen G. Dimensions of post-stroke fatigue: A two-year follow-up study. Cerebrovasc. Dis. 2008, 26, 134–141. [CrossRef]
- Hernandez-Ronquillo L, Moien-Afshari F, Knox K, Britz J, Tellez-Zenteno JF. How to measure fatigue in epilepsy? The validation of three scales for clinical use. Epilepsy Res. 2011, 95, 119–129. [CrossRef]
- Frucht MM, Quigg M, Schwaner C, Fountain NB. Distribution of seizure precipitants among epilepsy syndromes. Epilepsia 2000, 41, 1534–1539. [CrossRef]
- Balamurugan E, Aggarwal M, Lamba A, Dang N, Tripathi M. Perceived trigger factors of seizures in persons with epilepsy. Seizure 2013, 22, 743–747. [CrossRef]
- Ferlisi M, Shorvon S. Seizure precipitants (triggering factors) in patients with epilepsy. Epilepsy Behav. 2014, 33, 101–105. [CrossRef]
- Parisi P. Why is migraine rarely, and not usually, the sole ictal epileptic manifestation? Seizure 2009, 18, 309–312. [CrossRef]
- Kanemura, H, Sano F, Ohyama T, Aoyagi K, Sugita K, Aihara M. Sequential prefrontal lobe volume changes and cognitive dysfunctions in children with Panayiotopoulos syndrome presenting with status epilepticus. Epilepsy Res. 2015, 112, 122–129. [CrossRef]
- Binnie CD. Cognitive impairment during epileptiform discharges: Is it ever justifiable to treat the EEG? Lancet Neurol. 2003, 2, 725–730. [CrossRef]
- Fountain NB. Cellular damage and the neuropathology ofstatus epilepticus. In: Drislane FW (Ed), Status Epilepticus: A Clinical Perspective. Humana Press, New Jersey, 2005, 181—193.
- Aydemir N, Ozkara C, Unsal P, Canbeyli R. A comparative study of health related quality of life, psychological well-being, impact of illness and stigma in epilepsy and migraine. Seizure 2011, 20, 679–685. [CrossRef]
- Espinola-Nadurille M, Crail-Melendez D, Sanchez-Guzman MA. Stigma experience of people with epilepsy in Mexico and views of health care providers. Epilepsy Behav. 2014, 32, 162-169. [CrossRef]
- Baker GA, Jacoby A, Buck D, Stalgis C, Monnet D. Quality of life of people with epilepsy: A European study. Epilepsia 1997, 38, 353-362. [CrossRef]
- Cross JH, Kluger G, Lagae L. Advancing the management of childhood epilepsies. Eur. J. Paediatr. Neurol. 2013, 17, 334-347. [CrossRef]
- Austin JK, MacLeod J, Dunn DW, Shen J, Perkins SM. Measuring stigma in children with epilepsy and their parents: Instrument development and testing. Epilepsy Behav. 2004, 5, 472-482. [CrossRef]
- Kanemura H, Sano F, Sugita K, Aihara M. Presence of monthly seizures affects perceived stigma in children with epilepsy. J. Pediatr. Epilepsy 2014, 3, 85-92. [CrossRef]
- Coan JA, Allen JJB. The state and trait nature of frontal EEG asymmetry in emotion. In: Hugdahl K, Davidson RJ, editors. The Asymmetry Brain. Cambridge, MA: MIT Press; 2003, 565-615.
- Allen JJB. Editorial. Frontal EEG asymmetry, emotion, and psychopathology: the first, and the next 25 years. Biol. Psychol. 2004, 67, 1-5.
- Kanemura, H.; Sano, F.; Tando, T.; Hosaka, H.; Sugita, K.; Aihara, M. EEG improvements with antiepileptic drug treatment can show a high correlation with behavior recovery in children with ADHD. Epilepsy Behav. 2013, 27, 443-448. [CrossRef]
- Kanemura, H.; Sano, F.; Hoshino, H.; Aihara, M. Efficacy of perampanel in epilepsy patients with autism spectrum disorder. Epilepsy Res. 2021, 170, 106550. [CrossRef]
- Kanemura, H.; Sano, F.; Ohyama, T.; Sugita, K.; Aihara, M. Correlation between perceived stigma and EEG paroxysmal abnormality in childhood epilepsy. Epilepsy Behav. 2015, 52, 44-48. [CrossRef]
- Frucht MM, Quigg M, Schwaner C, Fountain NB. Distribution of seizure precipitants among epilepsy syndromes. Epilepsia 2000, 41, 1534-1539. [CrossRef]
- Kanemura H, Sano F, Ohyama T, Sugita K, Aihara M. Association between seizure frequency and fatigue levels in children with epilepsy. J. Paediatr. Child Health 2018, 54, 1336-1340. [CrossRef]
- Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale for patients. Application to patients with multiple sclerosis and systematic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123.
- Colombo B, Dalla Libera D, De Feo D, Pavan G, Annovazzi PO, Comi G. Delayed diagnosis in pediatric headache: an outpatient Italian survey. Headache 2011, 51, 1267–1273. [CrossRef]
- Kanemura H, Sano F, Ishii S, Ohyama T, Sugita K, Aihara M. Characteristics of headache in children with epilepsy. Seizure 2013, 22, 647-650. [CrossRef]
- Baumann RJ, Duffer PK. Treatment of children with simple febrile seizures: AAP practice parameter. American Academy of Pediatrics. Pediatr. Neurol. 2000, 23, 11-17.
- Yilmaz D, Arhan E, Yuksel D, et al. Attitudes of parents and physicians toward febrile seizures. Clin. Pediatr. 2008, 47, 856-860. [CrossRef]
- Surpure JS. Febrile convulsion. What happens to the infant admitted to the hospital. Clin. Pediatr. 1980, 19, 361-362.
- Balslev T. Parental reactions to a child’s first febrile convulsion. A follow-up investigation. Acta. Paediatr. Scand. 1991, 80, 466-469. [CrossRef]
- Huang MC, Liu CC, Chi YC, Huang CC, Cain K. Parental concerns for the child with febrile convulsion: long-term effects of educational interventions. Acta. Neurol. Scand. 2001, 103, 288-293. [CrossRef]
- Baumer JH, David TJ, Valentine SJ, Roberts JE, Hughes BR. Many parents think their child is dying when having a first febrile convulsion. Dev. Med. Child Neurol. 1981, 23, 462-464. [CrossRef]
- Rutter N, Metcalfe DH. Febrile convulsions: what do parents do? Br. Med. J. 1978, 2, 1345-1346. [CrossRef]
- Kolahi AA, Tahmooreszadeh S. First febrile convulsions: inquiry about the knowledge, attitudes and concerns of the patients’ mothers. Eur. J. Pediatr. 2009, 168, 167-171. [CrossRef]
- Kanemura H, Sano F, Mizorogi S, Tando T, Sugita K, Aihara M. Parental thoughts and actions regarding their child’s first febrile seizure. Pediatr. Int. 2013, 55, 315-319. [CrossRef]
- Tanabe T, Kashiwagi M, Ogino M, Oba C, Iai Y, Yamamoto C, et al. Alleviating stress and perceived stigma in parents after febrile seizure in their children. Brain Dev. 2025, 47, 104445. [CrossRef]
- Scambler G, Hopkins A. Generating a model of epileptic stigma: the role of qualitative analysis. Soc. Sci. Med. 1990, 30, 1187–1194. [CrossRef]
- Kanemura H, Sano F, Ohyama T, Sugita K, Aihara M. Seizure severity in children with epilepsy is associated with their parents' perception of stigma. Epilepsy Behav. 2016, 63, 42-45. [CrossRef]
- Papazoglou A, King TZ, Burns TG. Active seizures are associated with reduced adaptive functioning in children with epilepsy. Seizure 2010, 19, 409–413. [CrossRef]
- Kanemura H. Therapeutic strategies in children with epilepsy: A quality-of-life-related perspective. J. Clin. Med. 2024, 13, 405. [CrossRef]
- Kanemura H. Association between epilepsy and attention deficit/hyperactivity disorder –correlation between interictal epileptiform discharges and behavioral disturbances–. Brain Dev. 2025, 47, 104403. [CrossRef]
- Kanemura H, Hata S, Aoyagi K, Sugita K, Aihara M. Serial changes of prefrontal lobe growth in the patients with benign childhood epilepsy with centrotemporal spikes presenting with cognitive impairments/behavioral problems. Brain Dev. 2011, 33, 106-113. [CrossRef]
- Kanemura H, Sano F, Tando T, Sugita K, Aihara M. Repeated seizures induce prefrontal growth disturbance in frontal lobe epilepsy. Brain Dev. 2012, 34, 175-180. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



