Submitted:
02 February 2026
Posted:
03 February 2026
Read the latest preprint version here
Abstract
Background: Supported standing is commonly prescribed for children and adolescents with cerebral palsy (CP) to support musculoskeletal health and participation. However, objective data on foot loading under different positioning conditions are limited, particularly in individuals with severe motor impairment (GMFCS IV–V). This study quantified foot weight-bearing during supported standing across combinations of verticalization angle and hip/knee flexion. Methods: Twenty-six children and adolescents with CP (GMFCS IV–V; 6–17 years) were assessed using a standardized back-supported standing system. Foot loading was measured with two calibrated force plates at six verticalization angles (0°, 30°, 45°, 60°, 75°, 90°) combined with four hip/knee flexion angles (0°, 15°, 30°, 45°). Loading was expressed as percentage of body weight (% BW). Effects were analyzed using repeated-measures analysis of variance. Results: Foot loading increased progressively with increasing verticalization angles across all hip/knee flexion conditions. Clinically relevant loading levels (>70% BW) were achieved at a verticalization angle of 60° in most flexion conditions. Maximum loading was observed at 90° verticalization combined with 30° hip/knee flexion (96.4% BW). At 90° verticalization, foot loading remained substantial even with 45° hip/knee flexion (81.4% BW). Increasing hip/knee flexion did not result in a linear reduction in foot loading; a significant decrease was observed only at 45° flexion. Conclusion: Verticalization angle is the primary determinant of foot loading during supported standing in children and adolescents with severe CP. Meaningful foot loading can be achieved at moderate verticalization angles despite hip and knee flexion, supporting flexible positioning strategies.
Keywords:
cerebral palsy
; supported standing
; foot loading
; verticalization angle
; hip and knee flexion
; force plates
Introduction
Cerebral palsy (CP) is a major cause of long-term motor impairment in childhood and is associated with significant limitations in postural control, mobility and the ability to bear weight functionally [1].
Children and adolescents with GMFCS levels IV–V rely on supported standing systems to achieve an upright position. Assisted standing is associated with positive effects on bone mineral density, gastrointestinal function, joint range of motion, respiratory function and participation in everyday activities [2,3,4,5].
Despite these advantages, the biomechanical stress that actually occurs during supported standing, especially at the level of the feet, has not yet been sufficiently investigated. Adequate foot loading is crucial for bone health, joint alignment and the generation of adequate mechanical stimuli. Children and adolescents with severe CP have structural and functional factors such as hip/knee flexion contractures, altered muscle tone and reduced extensor strength, which can affect their ability to bear weight safely and effectively [6,7].
Previous studies have examined the overall load on the feet; however[8,9,10], a systematic quantification of foot load across defined combinations of verticalization angles and hip/knee flexion is not yet available. An understanding of these interactions is essential for clinicians to adapt standardised standing programmes to the individual anatomical and functional needs of each child and adolescent.
The aim of this study was to systematically quantify foot load in children and adolescents with CP (GMFCS IV–V) across six defined verticalization angles and four combined hip and knee flexion positions using integrated force plates.
Materials and Methods
Study Design
An experimental cross-sectional design was applied to analyse foot load under predefined combinations of verticalization angles and hip/knee flexion.
Participants
Twenty-six children and adolescents with a confirmed diagnosis of CP (GMFCS IV–V; age range 6–17 years) participated in the study.
Inclusion and Exclusion Criteria
The inclusion and exclusion criteria are presented in Table 1.
Recruitment
Participants were recruited from specialised educational and therapy centres in Germany.
Ethical Approval and Consent
Ethical approval was obtained from the institutional ethics committee of the University for Continuing Education Krems (reference no.: EK_GZ_24_2024-2027). Written informed consent was obtained from the legal guardians prior to participation.
Equipment and Measurement System
Trained therapists transferred participants into a horizontally aligned, back-supported reclining system. A patient lift was used when necessary, and the system was individually adjusted to each participant’s height and body proportions. Stabilisation was achieved using thoracic and pelvic pads, supplemented by a pelvic belt and vest to ensure a safe and reproducible starting position (Figure 1 and Figure 2).
The Till supported standing system (Schuchmann, Germany) was used as the standing system (Figure 3). This system allows individually adjustable hip and knee flexion and provides uniform support for the torso and lower extremities via a continuous support surface. Individually adjusted knee pads (Figure 4) were used to reduce local pressure peaks and enhance comfort.
The feet were positioned flat on the footrests and aligned at a 90° angle relative to the lower legs, which were oriented parallel to the longitudinal axis of the torso. Foot load was measured using two digital scales (Figure 5). Body weight was determined using a patient lift with integrated scales (Figure 6). All scales were calibrated using standardised weights prior to data collection to ensure measurement accuracy.
The verticalization angle was determined using a digital inclinometer application on a smartphone attached to the standing system. Hip and knee joint angles were measured in a standardised manner using a goniometer aligned with the respective joint axes.
Positions tested (Figure 7)
- • Verticalization: 0°, 30°, 45°, 60°, 75°, 90°
- • Hip/knee flexion: 0°, 15°, 30°, 45°
Procedure
Participants were positioned in a back-support system in a standardised manner, with neutral hip alignment and controlled hip/knee flexion angles (Figure 8). Measurements were taken for each verticalization angle after a stable and reproducible position had been achieved. The order of the test conditions was identical for all participants. Foot load was expressed as a percentage of body weight (%BW) (Table 2)
Data Processing
The measurement data were exported and further processed to calculate mean values for each experimental condition. The percentage of body weight load (%BW) was calculated by normalising the measured vertical load to the individual body weight of each participant. Data sets affected by movement artefacts, insufficient postural stability, or incomplete data recording were excluded from the analysis. Data collection was conducted between January and February 2025.
Statistical Analysis
To investigate the effects of the verticalization angle (six levels) and hip/knee flexion (four levels) on foot load, a repeated measures analysis of variance (ANOVA) was performed. Greenhouse–Geisser or Huynh–Feldt corrections were applied when the assumption of sphericity was violated. The significance level was set at p < 0.05. Effect sizes were reported as partial eta squared (η²p). All statistical analyses were performed using standardised statistical software (JASP (version 0.18.00), Datatab))
Results
Foot loading increased stepwise with increasing verticalization angle. In addition, hip and knee flexion influenced the measured foot loading. Significant effects of the verticalization angle were observed for all investigated hip/knee flexion angles (p < 0.001). Partial effect sizes (η²ₚ) were 0.88 at 0° hip/knee flexion, 0.91 at 15°, 0.88 at 30°, and 0.86 at 45° (Table 3).
Influence of Hip-/Knee Flexion
Increasing hip/knee flexion did not result in a consistent reduction in foot load. Instead, foot loading varied depending on the specific combination of verticalization angle and joint flexion.
At a verticalization angle of 90°, the foot load was 88% of body weight at 0° flexion, 87% at 15° flexion, 96% (maximum value) at 30° flexion and 81% of body weight at 45° flexion.
The highest foot load was observed at a combination of a 90° verticalization angle and 30° hip/knee flexion. A foot load exceeding 70% of body weight was achieved at verticalization angles of 60° and above (Figure 9).
Discussion
To our knowledge, this is the first study to systematically investigate foot loading in children and adolescents with severe CP (GMFCS IV-V) using defined combinations of verticalization angles and hip/knee flexion during supported standing. The findings demonstrate that both the degree of verticalization and joint flexion significantly influence the proportion of body weight transmitted through the feet.
Contrary to common assumptions, the presence of hip or knee flexion does not inherently prevent effective axial loading of the lower extremities. Instead, the results indicate that flexed joint positions can maintain—and in certain configurations even increase—foot loading, depending on the applied verticalization angle. From a biomechanical perspective, knee flexion alters the alignment of the lower limb and the line of action of the ground reaction force, potentially increasing joint compression and modifying load distribution.
Previous studies investigating supported standing in children with cerebral palsy have mainly focused on global loading effects or isolated outcome measures. However, foot loading has rarely been quantified under clearly defined and combined positional conditions. This limits the comparability of existing data and highlights the relevance of the present study’s systematic and position-specific approach.
Clinical Implications
The results of this study have several clinically relevant implications:
- • Children and adolescents with hip/knee flexion contractures are able to achieve clinically meaningful foot loading during supported standing
- • Clinically relevant loading levels (>70% of body weight) can be achieved at moderate verticalization angles of approximately 60°[3].
- • Individual adjustment of the standing system to the child’s anatomical alignment and available range of motion is essential to enable effective axial loading while minimising the risk of local pressure peaks on the joint surfaces.
- • When prescribing and adjusting standing devices, both the achievable verticalization angle and existing movement restrictions should be systematically considered.
Strengths and Limitations
The strengths of this study include the systematic investigation of 24 predefined combinations of verticalization angles and hip and knee flexion positions, the standardised positioning of participants, and the integration of force measurement within the standing system, allowing for consistent and reproducible data acquisition.
Several limitations should be acknowledged. First, the measurements were limited to static standing positions, and dynamic transitions were not assessed. Second, medio-lateral force distribution was not analysed. Finally, the study population was restricted to children and adolescents with GMFCS levels IV–V, which may limit the generalisability of the findings to less severely affected populations.
Future Research
Future research should focus on longitudinal studies investigating bone health and joint-related adaptations associated with assisted standing. In addition, the influence of orthotic use, existing joint contractures, and different standing system designs and component configurations on foot loading should be systematically examined. Further studies should also address dynamic transitions between different stages of verticalization and hip and knee flexion to better reflect loading patterns encountered in clinical practice.
Conclusion
Higher verticalization angles are associated with a significant increase in foot loading during supported standing. The presence of hip/knee flexion does not necessarily reduce foot load and may, depending on the configuration, maintain or even increase force transmission to the feet. Clinically relevant foot loading levels can be achieved at moderate verticalization angles of approximately 60°.
These findings highlight the importance of precise and individually tailored adjustment of standing systems. Considering both the verticalization angle and hip and knee flexion may facilitate axis-aligned load transfer through the feet while minimising the risk of local pressure peaks, particularly in children and adolescents with restricted range of motion or existing flexion contractures.
Statement from the Institutional Review Board
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University for Continuing Education Krems (reference number: EK_GZ_24_2024-2027).
Funding
This research received no external funding.
Informed consent statement
Written informed consent was obtained from the legal representatives of all children and adolescents involved in the study.
Data availability statement
The data presented in this study are available from the corresponding author upon reasonable request. Data availability is subject to ethical restrictions due to the inclusion of sensitive paediatric patient data.
Acknowledgments
The authors would like to thank the following institutions for their support and cooperation: Liboriusschule LWL-Förderschule Paderborn; Heinrich-Kielhorn-Schule, Hameln; Johannes-Falk-Haus Förderschule, Herford
Conflicts of Interest
The authors declare no conflict of interest.
References
- Vitrikas, Kirsten; Dalton, Heather; Breish, Dakota. Cerebral Palsy: An Overview. American family physician 2020, 101, 213–220. Available online: https://pubmed.ncbi.nlm.nih.gov/32053326/. [PubMed]
- Caulton, J. M.; Ward, K. A.; Alsop, C. W.; Dunn, G.; Adams, J. E.; Mughal, M. Z. A randomised controlled trial of standing programme on bone mineral density in non-ambulant children with cerebral palsy. Archives of Disease in Childhood 2004, 89, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Paleg, Ginny S.; Smith, Beth A.; Glickman, Leslie B. Systematic review and evidence-based clinical recommendations for dosing of pediatric supported standing programs. Pediatric physical therapy: the official publication of the Section on Pediatrics of the American Physical Therapy Association 2013, 25, 232–247. [Google Scholar] [CrossRef] [PubMed]
- Uddenfeldt Wort, Ulrika; Nordmark, Eva; Wagner, Philippe; Düppe, Henrik; Westbom, Lena. Fractures in children with cerebral palsy: a total population study. Develop Med Child Neuro 2013, 55, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Hind, K.; Burrows, M. Weight-bearing exercise and bone mineral accrual in children and adolescents: a review of controlled trials. Bone 2007, 40, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Neuroorthopädie. In Disability Management, 1. Auflage; Strobl, Walter, Schikora, Nils, Pitz, Elisabeth, Abel, Claudia, Eds.; Springer Berlin: Berlin; Springer, 2020. [Google Scholar]
- Döderlein, L. Infantile Zerebralparese. Diagnostik, konservative und operative Therapie; Springer: Berlin, 2015; Available online: http://nbn-resolving.org/urn:nbn:de:bsz:31-epflicht-1543548.
- Herman, Daniel; May, Ryan; Vogel, Lois; Johnson, Julie; Henderson, Richard C. Quantifying weight-bearing by children with cerebral palsy while in passive standers. Pediatric physical therapy: the official publication of the Section on Pediatrics of the American Physical Therapy Association 2007, 19, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Kecskemethy, Heidi H.; Herman, Daniel; May, Ryan; Paul, Kathleen; Bachrach, Steven J.; Henderson, Richard C. Quantifying weight bearing while in passive standers and a comparison of standers. Develop Med Child Neuro 2008, 50, 520–523. [Google Scholar] [CrossRef]
- Paleg, Ginny; Altizer, Wendy; Malone, Rachel; Ballard, Katie; Kreger, Alison. Inclination, hip abduction, orientation, and tone affect weight-bearing in standing devices. Journal of pediatric rehabilitation medicine 2021, 14, 433–441. [Google Scholar] [CrossRef]
Figure 1.
Pelvic strap.

Figure 2.
Shoulder support harness.

Figure 3.
Supine standing system "Till".

Figure 4.
FKP-Knee pads.

Figure 5.
LX-02 Digital Travel Scale.

Figure 6.
Rebotec Patient lift Arnold 150 with scales.

Figure 7.
Illustration of the verticalization angles and hip/knee flexion used during the examination.
Figure 7.
Illustration of the verticalization angles and hip/knee flexion used during the examination.
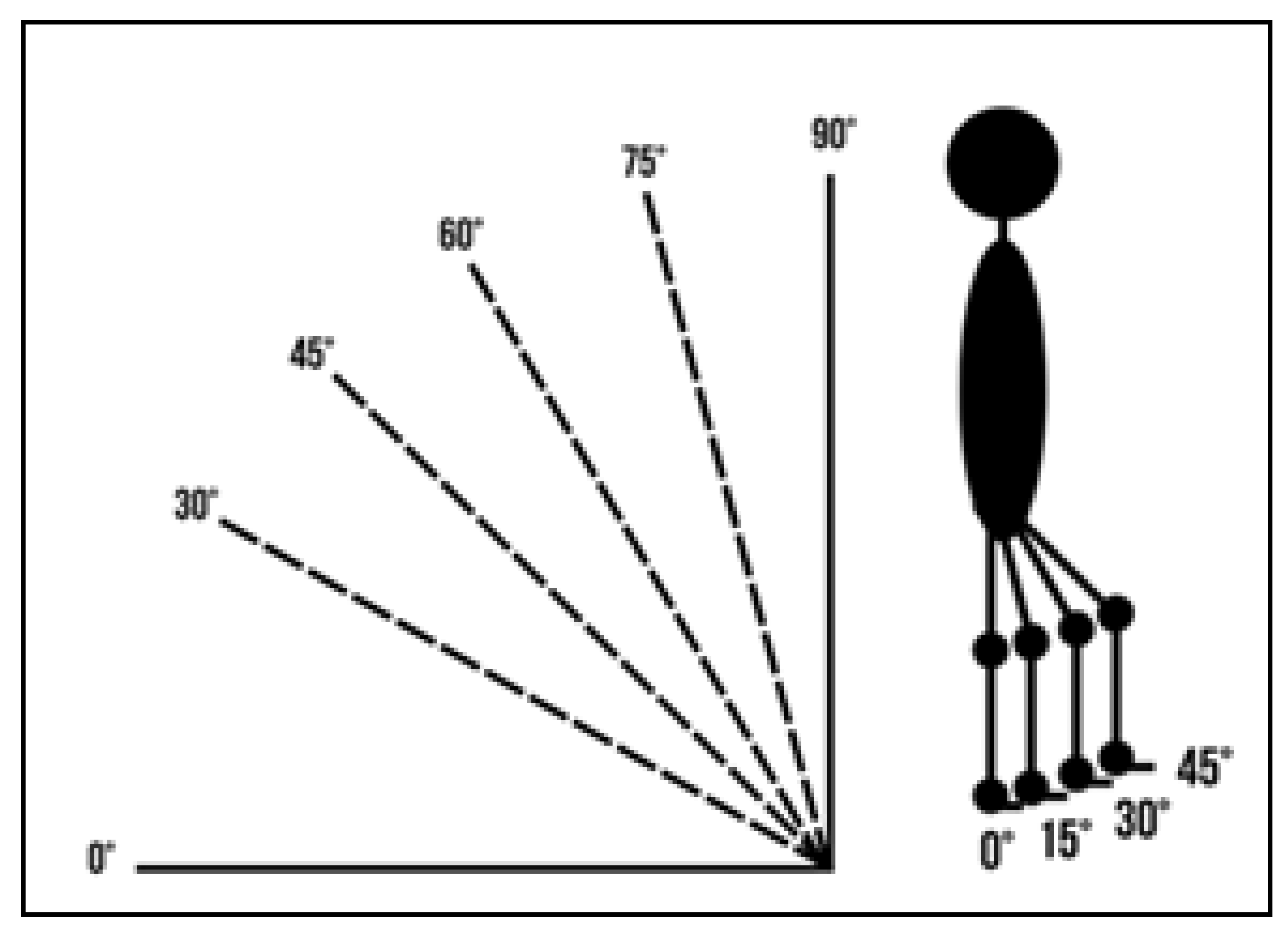
Figure 8.
Positioning examples for HK 30° and V 90°, 30°, 0°.

Figure 9.
Percentage of weight bearing (%BW) for different combinations of verticalization angle and hip/knee flexion.
Figure 9.
Percentage of weight bearing (%BW) for different combinations of verticalization angle and hip/knee flexion.
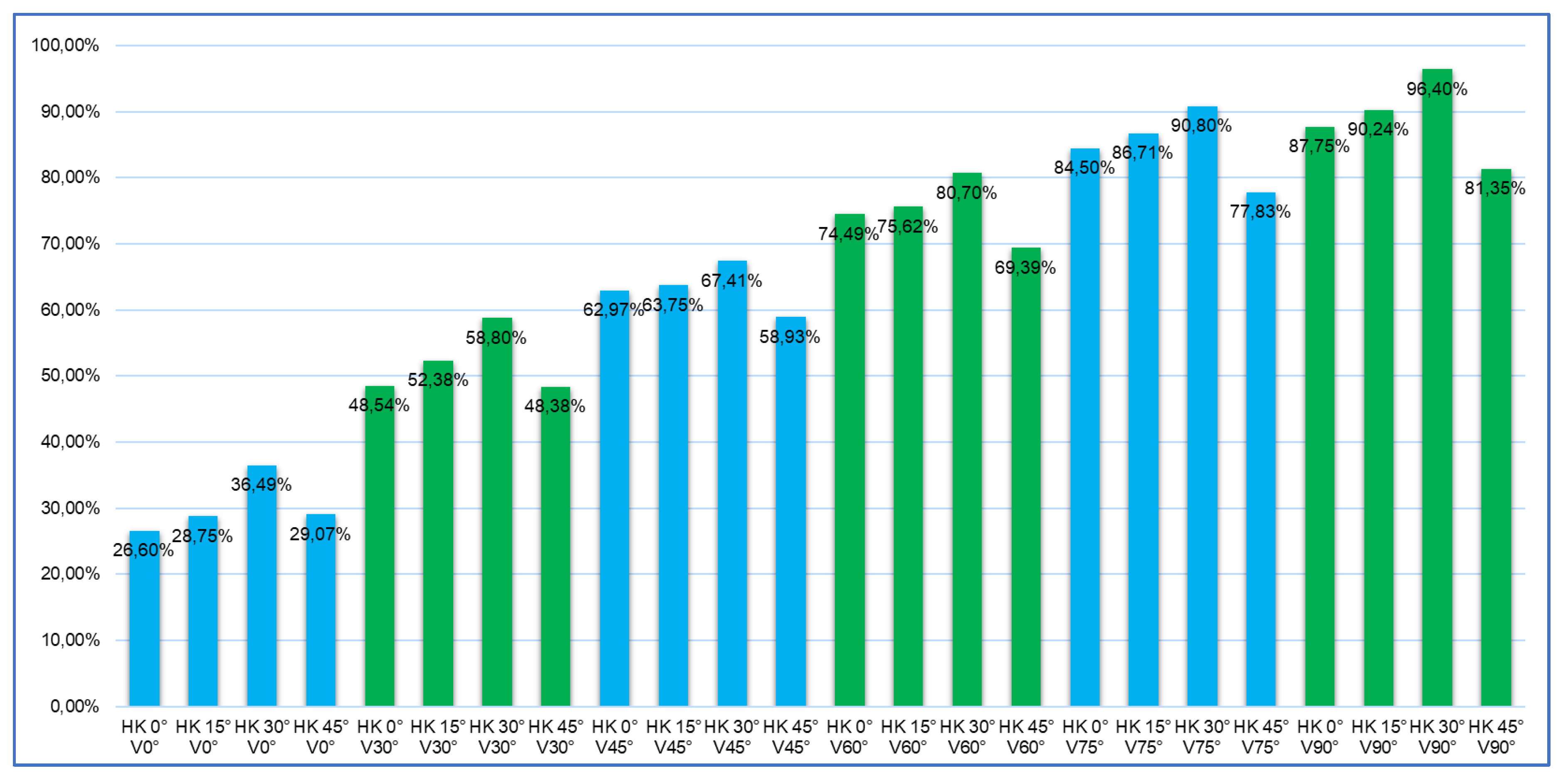

Table 1.
Inclusion and exclusion criteria.
| Inclusion criteria | Exclusion criteria |
| Diagnosis of cerebral palsy (CP) | Other neurological disease |
| GMFCS Level IV or V | GMFCS Level I-III |
| Regular standing therapy | Absence of regular standing therapy |
| Age 4-18 years | age <4 years or > 18 years |
| Lack of compliance |
Table 2.
Positions and corresponding hip/knee flexion and verticalization angle.
| Position | Hip flexion angle | Knee flexion angle | Verticalization angles |
| 1 | 0° | 0° | 0°, 30°, 45°, 60°, 75°, 90° |
| 2 | 15° | 15° | 0°, 30°, 45°, 60°, 75°, 90° |
| 3 | 30° | 30° | 0°, 30°, 45°, 60°, 75°, 90° |
| 4 | 45° | 45° | 0°, 30°, 45°, 60°, 75°, 90° |
Table 3.
Foot load (%BW) across different verticalization angles.
| Verticalization | %BW | p |
| 0° | 12-15% | <0,001 |
| 30° | 28-52% | <0,001 |
| 45° | 45-63% | <0,001 |
| 60° | 60-75% | <0,001 |
| 75° | 70-85% | <0,001 |
| 90° | 81-96% | <0,001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



