
Submitted:
02 February 2026
Posted:
03 February 2026
You are already at the latest version
Abstract
Background/Objectives: Many patients with acute coronary syndrome (ACS) fail to achieve adequate low-density lipoprotein-cholesterol (LDL-C) reduction, despite re-ceiving high-intensity statin therapy. Identifying patients requiring early combination therapy remains a challenging task. This study aimed to determine the prevalence of statin hyporesponsiveness in patients with ACS and investigate the predictive role of baseline LDL-C and albumin levels. Methods: This retrospective study enrolled 366 pa-tients with ACS treated with high-intensity statins (atorvastatin 40–80 mg). Hyporesponsiveness was defined as LDL-C reduction of < 50% at 21–28 d. The baseline parameters were analyzed using logistic regression and receiver operating characteris-tic (ROC) curve analysis. Results: Hyporesponsiveness was observed in 63.1% of pa-tients. Hyporesponders had significantly lower baseline albumin (41.7 vs. 43.3 g/L, p=0.0002) and LDL-C (126.6 vs 147.3 mg/dL, p< 0.0001) levels. Categorical analysis re-vealed that the combination of baseline LDL-C < 100 mg/dL and albumin < 40 g/L pre-dicted hyporesponsiveness in 95.7% of cases. ROC curve analysis identified optimal predictive cut-offs of 128.50 mg/dL for LDL-C (AUC: 0.652) and 41.15 g/L for albumin (AUC: 0.618). Conclusions: Low baseline LDL-C and low albumin are strong predictors of statin hyporesponsiveness in patients with ACS. These routinely obtained bi-omarkers can identify very high-risk patients who may benefit from proactive combi-nation lipid-lowering therapy from hospital discharge, supporting the "strike early and strike strong" strategy and challenging the traditional stepwise approach.
Keywords:
statin response
; hyporesponsiveness
; lipid-lowering therapy
; ≥50% reduction of LDL-C
; albumin
; acute coronary syndrome
1. Introduction
Cardiovascular disease (CVD), particularly ischemic heart disease and stroke, remains the leading cause of morbidity and mortality globally. Acute coronary syndrome (ACS), the most critical manifestation of CVD, requires early and aggressive treatment strategies [1]. Despite hyperlipidemia being a modifiable risk factor for atherosclerotic cardiovascular disease (ASCVD) and the existence of categorical guidelines and evidence supporting the benefits of lipid-lowering therapy (LLT), real-world data reveal a significant treatment gap in the management of dyslipidemia [2]. Research has long established that high-intensity LLT improves the prognosis after ACS, a concept supported by the “the lower the better” principle in low-density lipoprotein-cholesterol (LDL-C) reduction [3,4]. The landmark IMPROVE-IT trial, published in 2015, revealed that lower LDL-C levels achieved by adding ezetimibe to statin therapy, elicited greater cardiovascular benefit compared with statin monotherapy [5].
In light of this evidence, the “strike early and strike strong” approach was proposed in 2022 by the European Society of Cardiology working groups, recommending the initiation of combination LLT using high-intensity statins and ezetimibe in the early period after ACS [6]. This approach has been strongly supported by the SWEDEHEART registry data, which revealed that early and sustained lowering of non-HDL cholesterol following ACS is associated with the best prognosis, and it has been argued that the traditional stepwise approach leads to potentially harmful delays [7]. The current guidelines recommend early initiation of statin and ezetimibe combination therapy [8,9,10].
Moreover, the guidelines recommend achieving an absolute LDL-C target (<55 mg/dL) along with at least 50% reduction from baseline in very high-risk patients [10]. However, the clinical importance of the equivalence of this dual target has been questioned by a striking study published recently. Fujioka et al. showed that achieving ≥50% reduction in LDL-C levels was superior to reaching the absolute LDL-C target of 55 mg/dL in reducing the rates of major adverse cardiovascular events (MACE) [11]. This crucial finding indicates that hyporesponsiveness, defined as an inadequate response to statin therapy, may be a stronger and more clinically meaningful prognostic marker than achieving a specific LDL-C value.
Identifying the determinants underlying hyporesponsiviness is crucial, owing to its clinical significance in predicting cardiovascular outcomes. In recent years, low albumin levels have been shown to be associated with poor prognosis [12,13]. Albumin serves as an indicator of nutritional status and as an important inflammatory marker, in addition to and interacting with cholesterol metabolism [12,13]. Moreover, baseline LDL-C level is an important determinant of the statin response [11,12,13,14]. These observations indicate that both albumin and baseline LDL-C may serve as independent predictors of statin hyporesponsiveness.
Therefore, this study aimed to determine the prevalence of statin hyporesponsiveness after ACS and investigate the role of baseline LDL-C and albumin levels in predicting the statin response. We hypothesized that low baseline LDL-C and low albumin levels, both individually and in combination, are strong and independent predictors of statin hyporesponsiveness. This information can help identify patients who would benefit most substantially from the “strike early and strike strong” strategy.
2. Materials and Methods
2.1. Study Population
We retrospectively analyzed 712 patients diagnosed with unstable angina pectoris (USAP), non-ST-elevation myocardial infarction (non-STEMI), and ST-elevation myocardial infarction (STEMI) at a tertiary hospital between January and December 2024. The Academic Ethics Committee of the University of Health Sciences, Antalya Training and Research Hospital, approved this retrospective study and waived the requirement for informed consent (2025-460). All procedures were conducted in accordance with the Declaration of Helsinki. The exclusion criteria were-as follow: patients not requiring percutaneous coronary intervention (PCI, n=17); patients with a history of revascularization [PCI, n=140; coronary artery bypass graft (CABG, n=24)]; in-hospital death (n=17); patients transferred to cardiovascular surgery and other departments with a plan for CABG (n=16); patients who did not attend the third-week LDL-C follow-up (n=113); patients prescribed antibiotics (n=6); patients with alanine transaminase values more than three times the upper limit (ALT×3, n=4); and patients with a glomerular filtration rate (GFR) <30 mL/min/1.73 m2 (n=9). Ultimately, 366 patients were included in our study. We recorded LDL-C values measured during coronary intensive care unit admission and at the 21–28-day follow-up. We classified patients as hyporesponders if they achieved <50% LDL-C reduction from baseline and as responders if they attained ≥50% LDL-C reduction. Atorvastatin at doses of 40 mg and 80 mg was designated as a high-intensity statin.
2.2. Blood and Lipid Measurements
Blood samples were obtained from the initial blood draws at coronary intensive care unit admission. We analyzed the biochemical and lipid parameters using the Beckman Coulter AU5800 (Beckman Coulter Inc., CA, USA), and the complete blood count using the Sysmex XT-2000i (Sysmex, Kobe, Japan). LDL-C levels were calculated using the Friedewald formula, except in cases where the triglyceride levels were >400 mg/dL [15].
2.3. Statistical Methods
All statistical analyses were performed using the SAS v. 9.4 (SAS Institute, Cary, North Carolina) software package. Continuous variables in the patient dataset were presented as the mean and standard deviation (SD) or median and interquartile ranges, while categorical variables were described as numbers and percentages. The Shapiro–Wilk test was used to determine normality of distribution of the continuous variables. Statistical comparisons between the two groups were performed using the independent Student t-test for normally distributed variables and the Mann–Whitney U test for non-normally distributed variables. The chi-square test or Fisher’s exact test was used to analyze the relationship between two categorical variables.
Receiver operating characteristic (ROC) curve analysis was performed to determine the optimal cut-off values for albumin and LDL-C, calculate the sensitivity and specificity values, and determine the area under the ROC curve (AUC). The point with the largest Youden index (sensitivity + specificity - 1) was selected as the optimal cut-off point. The AUC was used to compare the predictive performance of albumin and LDL-C.
Univariate binary logistic regression analysis was performed to investigate the relationship between baseline demographic, clinical, and laboratory variables and the response status (hyporesponder or responder), followed by multivariate adjustments to identify independent predictors. The final multivariate logistic regression model was used to estimate the odds ratios (OR) and their corresponding 95% confidence intervals (CI).
A significance level of 0.05 was accepted throughout the study.
3. Results
3.1. Patient Characteristics and Statin Response Outcomes
The participants’ clinical characteristics are shown in Table 1. The mean age of the 366 patients included in the study was 58.7 years, and 84.4% were men. PCI was performed for STEMI in 59.8% of participants, for non-STEMI 36.3%, and USAP in 3.8% of participants. After high-intensity statin therapy, 231 patients (63.1%) were classified as hyporesponders. The classic cardiovascular risk factors such as diabetes mellitus, hypertension, and smoking did not differ (statistically) significantly between the two groups (p>0.05).
| .3759 |
The albumin (41.7 vs 43.3 g/dL, p=0.0002) and hemoglobin (14.2 vs 14.8 g/dL, p=0.0016) levels were significantly lower in the hyporesponder group compared with the responder group. Similarly, the total cholesterol (206.8 vs 227.6 mg/dL, p<0.0001) and LDL-C (126.6 vs 147.3 mg/dL, p<0.0001) levels were also significantly lower in the hyporesponder group. Although the follow-up LDL-C levels at 21–28 d after treatment were higher in the hyporesponder group (86.4 vs 59.4 mg/dL, p<0.0001), the percentage reduction in LDL-C was significantly lower (32.3% vs 59.5%, p<0.0001).
3.2. Association of LDL-C and Albumin Levels with Hyporesponsiveness
When patients were categorized according to the baseline LDL-C and albumin levels, a cumulative (additive) effect of these two parameters on hyporesponsiveness emerged (Table 2). Notably, patients with baseline LDL-C <100 mg/dL and albumin <40 g/L exhibited a hyporesponsiveness rate of 95.7%, revealing a nearly complete lack of response. In contrast, the hyporesponsiveness rate decreased to 47.6% in the group with LDL-C >160 mg/dL and albumin >44 g/L.
Cochran–Armitage trend analysis confirmed a statistically significant increase in the proportion of patients responding to statin therapy both the increasing albumin categories (p=0.0004) and increasing LDL-C categories (p<0.0001; Table 3). These trends are also visually presented in the mosaic plots in Figure 1 and Figure 2.
3.3. Independent Predictors of Hyporesponsiveness
Correlation analysis performed to evaluate the relationship between statin response status and variables revealed that both albumin (Somers’ D = 0.217) and LDL-C (Somers’ D = 0.308) bore a significant positive correlation with the statin response (Table 4).
In the univariate logistic regression analysis, albumin, hemoglobin, total cholesterol, and LDL-C were determined to be associated with hyporesponsiveness. However, multivariate logistic regression analysis identified hemoglobin (OR: 0.3, 95% CI: 0.1-0.9, p=0.025), baseline LDL-C (OR: 17.5, 95% CI: 5.9-52.1, p<0.0001), and LDL-C at the 21–28 d follow-up (OR: 0.0, 95% CI: 0.0-0.0, p<0.0001) as independent predictors of the statin response (Table 5).
4. Discussion
The most important finding of our study, aimed at identifying which patients would benefit most critically from the “strike early and strike strong” strategy, is that 63.1% of patients receiving high-intensity statin therapy after ACS exhibited hyporesponsiveness (<50% LDL-C reduction). More importantly, this study reveals for the first time that the combination of low baseline LDL-C (<100 mg/dL) and low albumin (<40 g/L) is a novel and powerful clinical marker predicting almost complete hyporesponsiveness to high-intensity statins (95.7%). Baseline LDL-C and albumin levels were shown to have a cumulative (additive) effect on hyporesponsiveness. This finding highlights the importance of the cumulative effect of simple biochemical parameters in predicting the statin response.
Studies have used disparate definitions of statin hyporesponsiveness. Sun et al. defined it as <30% LDL-C reduction, despite moderate- and high-intensity statin use, while Tsuda et al. used the criterion of <15% LDL-C reduction after acute myocardial infarction [16,17]. In this study, patients who failed to achieve the ≥50% LDL-C reduction target recommended by the current guidelines were defined as hyporesponders [10].
Fujioka et al. reported that a <50% reduction in LDL-C carries a greater risk of cardiovascular events than that associated with failure to achieve the absolute LDL-C target (55 mg/dL) [11]. Similarly, Amarenco et al. revealed that patients with ischemic stroke who achieved LDL-C <70 mg/dL experienced a reduction in major vascular events only when >50% LDL-C reduction was achieved, whereas no significant benefit was observed in patients achieving <50% reduction [18]. These findings support the nation that optimal therapy should entail achieving the target LDL-C as well as at least a 50% relative reduction to optimize risk reduction [11].
The clinical significance of statin hyporesponsiveness is not limited to failure to achieve target LDL-C levels. Kataoka et al. analyzed intravascular ultrasound data from 7 prospective atherosclerosis progression/regression studies, reporting that statin hyporesponders (<15% LDL-C reduction) had significantly lower baseline LDL-C levels than responders and, more importantly, these hyporesponder patients exhibited significantly greater atheroma progression [19]. These findings show that statin hyporesponsiveness is not merely a biochemical non-response but also has significant clinical implications in terms of atherosclerosis progression and cardiovascular event risk.
A comprehensive study by Zeng et al. demonstrated that the lipid paradox observed in patients with acute myocardial infarction patients (the association of low LDL-C levels with high mortality) was present only in patients with high a inflammatory risk (high-sensivity C-reactive protein ≥ 3 mg/L), whereas this phenomenon was not observed in patients with a low inflammatory risk [13]. Yao et al. reported that low albumin levels in patients with coronary artery disease were associated with a high MACE risk and that this association interacted with the total cholesterol levels [12]. Lu et al. Observed that the lipid paradox was present only in the population with a high malnutrition risk, implying that albumin functions as both a nutritional and inflammatory marker [13,20]. In our study, the association of the combination of low baseline LDL-C and low albumin with 95.7% hyporesponsiveness to high-intensity statins indicates that the inflammatory state reflected by low albumin may adversely affect the statin response.
In our study, albumin showed a strong association in the univariate analysis (p<0.001); the loss of statistical significance in the multivariate analysis (p=0.539) can be explained by the correlation between variables (collinearity) and their reflection of similar physiological processes (confounding). Albumin, hemoglobin, and baseline LDL-C are all indicators of poor general health status, and when included together in the multivariate model, the independent contribution of albumin may have been masked due to shared effects. However, the association of the combination of low albumin and low baseline LDL-C with 95.7% hyporesponsiveness in the categorical analysis revealed that albumin is a clinically strong predictor.
Recently, two important studies conducted using the SWEDEHEART registry data have revealed the critical importance of the ‟strike early and strike strong” strategy. Schubert et al. reported that achieving and maintaining the non-HDL target within the first 2 months after myocardial infarction was associated with the lowest cardiovascular event risk [7]. Leosdottir et al. reported that the 1-year MACE incidence was 1.79/100 patient-years in patients who received ezetimibe within the first 12 weeks after myocardial infarction, whereas this rate increased to 2.58/100 patient-years in patients who received ezetimibe after 12 weeks [21]. These findings reveal that the stepwise approach recommended by the current guidelines (statin monotherapy first, followed by addition of non-statin agents if the response is inadequate) inevitably leads to delays in treatment intensification, is associated with preventable cardiovascular events. The findings of this study provide a practical approach for risk stratification and treatment intensification in post-ACS patients. The combination of low baseline LDL-C and low albumin can be used as a simple and inexpensive tool to identify patients at very high risk for statin hyporesponsiveness (95.7%) in the early period. In these high-risk patients, combination therapy with statins and ezetimibe should be initiated proactively from discharge, instead of statin monotherapy.
Limitations
This study has certain limitations. First, its retrospective design precluded establishment of causality and potentially introduced selection bias. Second, the follow-up period was relatively short (21–28 d), and only the LDL-C response was evaluated; long-term cardiovascular outcomes (MACE, mortality) should be assessed in future studies. Third, statin adherence was not objectively measured, and a distinction between true hyporesponsiveness and non-adherence could not be made. Fourth, the loss of significance of albumin the in multivariate analysis indicate collinearity between variables; however, the association of the combination of low albumin and low baseline LDL-C with 95.7% hyporesponsiveness in the categorical analysis demonstrates its clinical value. Fifth, genetic polymorphisms were not evaluated, and the effect of these factors on statin response should be investigated in future studies. Finally, the proportion of female patients in the study population was low, necessitating validation of the findings should in women. Despite these limitations, the findings of our study showed that the ‟strike early and strike strong” strategy after ACS should be applied to all patients but particularly as a priority to very high-risk patients (95.7% hyporesponsiveness) identified by the combination of low baseline LDL-C and low albümin, implying that the stepwise approach recommended in the current guidelines needs to be re-evaluated in this patient group.
5. Conclusions
In this study, hyporesponsiviness was observed in more than half of the patients receiving high-intensity statin therapy after ACS, and the combination of low LDL-C and low albumin at ACS onset significantly increased hyporesponsiveness. These two simple biochemical parameters are measured routinely and do not incur any additional cost. To avoid delays in intensified treatment after myocardial infarction, proactive combined LLT should be initiated from discharge in high-risk patients, instead of a stepwise approach. These simple biochemical markers can guide clinicians in identifying patients who would benefit the most from the “strike early and strike strong” strategy. Future studies should confirm these findings in prospective cohorts and evaluate the impact of early combined therapy strategies on the long-term cardiovascular outcomes.
Author Contributions
S.U.: Investigation, Data collection, Methodology, Writing. G.M.Y.O.: Data Collection, Writing, Review & Editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the University of Health Sciences, Antalya Training and Research Hospital (460) on 2025.
Informed Consent Statement
Informed consent for participation is not required as per local legislation.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors thank Professor Mehmet Ziya Fırat, PhD, for his valuable assistance with the statistical analysis of this study.
Conflicts of Interest
The authors declare no competing interests.
References
- Roth, G. A.; Mensah, G. A.; Johnson, C. O.; Addolorato, G.; Ammirati, E.; Baddour, L. M.; Barengo, N. C.; Beaton, A. Z.; Benjamin, E. J.; Benziger, C. P.; et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: Update from the GBD 2019 study. J Am Coll Cardiol 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Pogran, E.; Burger, A. L.; Zweiker, D.; Kaufmann, C. C.; Muthspiel, M.; Rega-Kaun, G.; Wenkstetten-Holub, A.; Wojta, J.; Drexel, H.; Huber, K. Lipid-lowering therapy after acute coronary syndrome. J Clin Med 2024, 13, 2043. [Google Scholar] [CrossRef]
- Cannon, C. P.; Braunwald, E.; McCabe, C. H.; Rader, D. J.; Rouleau, J. L.; Belder, R.; Joyal, S. V.; Hill, K. A.; Pfeffer, M. A.; Skene, A. M.; et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004, 350(15), 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S. D.; Cannon, C. P.; Morrow, D. A.; Ray, K. K.; Pfeffer, M. A.; Braunwald, E. PROVE IT-TIMI 22 Investigators. Can low-density lipoprotein be too low? The safety and efficacy of achieving very low low-density lipoprotein with intensive statin therapy: A PROVE IT-TIMI 22 substudy. J Am Coll Cardiol 2005, 46, 1411–1416. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S. A.; Cannon, C. P.; Blazing, M. A.; Giugliano, R. P.; White, J. A.; Lokhnygina, Y.; Reist, C.; Im, K.; Bohula, E. A.; Isaza, D.; et al. Reduction in total cardiovascular events with ezetimibe/simvastatin post-acute coronary syndrome: The IMPROVE-IT Trial. J Am Coll Cardiol 2016, 67, 353–361. [Google Scholar] [CrossRef]
- Krychtiuk, K. A.; Ahrens, I.; Drexel, H.; Halvorsen, S.; Hassager, C.; Huber, K.; Kurpas, D.; Niessner, A.; Schiele, F.; Semb, A. G.; et al. Acute LDL-C reduction post ACS: Strike early and strike strong: From evidence to clinical practice. A clinical consensus statement of the Association for Acute CardioVascular Care (ACVC), in collaboration with the European Association of Preventive Cardiology (EAPC) and the European Society of Cardiology Working Group on Cardiovascular Pharmacotherapy. Eur Heart J Acute Cardiovasc Care 2022, 11, 939–949. [Google Scholar] [CrossRef]
- Schubert, J.; Leosdottir, M.; Lindahl, B.; Westerbergh, J.; Melhus, H.; Modica, A.; Cater, N.; Brinck, J.; Ray, K. K.; Hagstrom, E. Intensive early and sustained lowering of non-high-density lipoprotein cholesterol after myocardial infarction and prognosis: The SWEDEHEART registry. Eur Heart J 2024, 45, 4204–4215. [Google Scholar] [CrossRef]
- Byrne, R. A.; Rossello, X.; Coughlan, J.; Barbato, E.; Berry, C.; Chieffo, A.; et al. 2023 ESC guidelines for the management of acute coronary syndromes. Eur H J 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Rao, S. V.; O’Donoghue, M. L.; Ruel, M.; Rab, T.; Tamis-Holland, J. E.; Alexander, J. H.; Baber, U.; Baker, H.; Cohen, M. G.; Cruz-Ruiz, M.; et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI guideline for the management of patients with acute coronary syndromes: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2025, 85, 2135–2237. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Koskinas, K. C.; Roeters van Lennep, J. E.; Tokgözoğlu, L.; Badimon, L.; Baigent, C.; Benn, M.; Binder, C. J.; Catapano, A. L.; De Backer, G. G.; et al. Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Developed by the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J 2025, 46, 4359–4378. [Google Scholar] [CrossRef]
- Fujioka, S.; Shishikura, D.; Kusumoto, H.; Yamauchi, Y.; Sakane, K.; Fujisaka, T.; Shibata, K.; Morita, H.; Kanzaki, Y.; Michikura, M.; et al. Clinical impact of ≥50% reduction of low density lipoprotein cholesterol following lipid lowering therapy on cardiovascular outcomes in patients with acute coronary syndrome. J Clin Lipidol 2025, 19, 247–255. [Google Scholar] [CrossRef]
- Yao, Y. F.; Chen, Z. Y.; Luo, T. Y.; Dou, X. Y.; Chen, H. B. Cholesterol affects the relationship between albumin and major adverse cardiac events in patients with coronary artery disease: a secondary analysis. Sci Rep 2022, 12, 12634. [Google Scholar] [CrossRef]
- Zeng, G.; Zhang, C.; Song, Y.; Zhang, Z.; Xu, J.; Liu, Z.; Tang, X.; Wang, X.; Chen, Y.; Zhang, Y.; et al. The potential impact of inflammation on the lipid paradox in patients with acute myocardial infarction: a multicenter study. BMC Med 2024, 22, 599. [Google Scholar] [CrossRef] [PubMed]
- Navarese, E. P.; Robinson, J. G.; Kowalewski, M.; Kołodziejczak, M.; Andreotti, F.; Bliden, K.; Tantry, U.; Kubica, J.; Raggi, P.; Gurbel, P. A. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: A systematic review and meta-analysis. JAMA 2018, 319, 1566–1579. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W. T.; Levy, R. I.; Fredrickson, D. S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Wolska, A.; Amar, M.; Zubiran, R.; Remaley, A. T. Approach to the patient with a suboptimal statin response: Causes and algorithm for clinical management. J Clin Endocrinol Metab 2023, 108, 2424–2434. [Google Scholar] [CrossRef]
- Tsuda, K.; Kataoka, Y.; Ogata, S.; Nishimura, K.; Nishikawa, R.; Doi, T.; Nakashima, T.; Hosoda, H.; Honda, S.; Kawakami, S.; et al. Diminished response to statins predicts the occurrence of heart failure after acute myocardial infarction. Cardiovasc Diagn Ther 2020, 10, 705–716. [Google Scholar] [CrossRef]
- Amarenco, P.; Lavallée, P. C.; Kim, J. S.; Labreuche, J.; Charles, H.; Giroud, M.; Lee, B.-C.; Mahagne, M.-H.; Meseguer, E.; Nighoghossian, N.; et al. More than 50 percent reduction in LDL cholesterol in patients with target LDL<70 mg/dL after a stroke. Stroke 2023, 54, 1993–2001. [Google Scholar] [CrossRef]
- Kataoka, Y.; St John, J.; Wolski, K.; Uno, K.; Puri, R.; Tuzcu, E. M.; Nissen, S. E.; Nicholls, S. J. Atheroma progression in hyporesponders to statin therapy. Arterioscler Thromb Vasc Biol 2015, 35, 990–995. [Google Scholar] [CrossRef]
- Lu, Y. W.; Lu, S. F.; Chou, R. H.; Wu, P. S.; Ku, Y. C.; Kuo, C. S.; Chang, C. C.; Tsai, Y. L.; Wu, C. H.; Huang, P. H. Lipid paradox in patients with acute myocardial infarction: Potential impact of malnutrition. Clin Nutr 2019, 38, 2311–2318. [Google Scholar] [CrossRef]
- Leosdottir, M.; Schubert, J.; Brandts, J.; Gustafsson, S.; Cars, T.; Sundstrom, J.; Jernberg, T.; Ray, K. K.; Hagstrom, E. Early ezetimibe initiation after myocardial infarction protects against later cardiovascular outcomes in the SWEDEHEART registry. J Am Coll Cardiol 2025, 85, 1550–1564. [Google Scholar] [CrossRef]
Figure 1.
Distribution of Response Status by Albumin Levels.
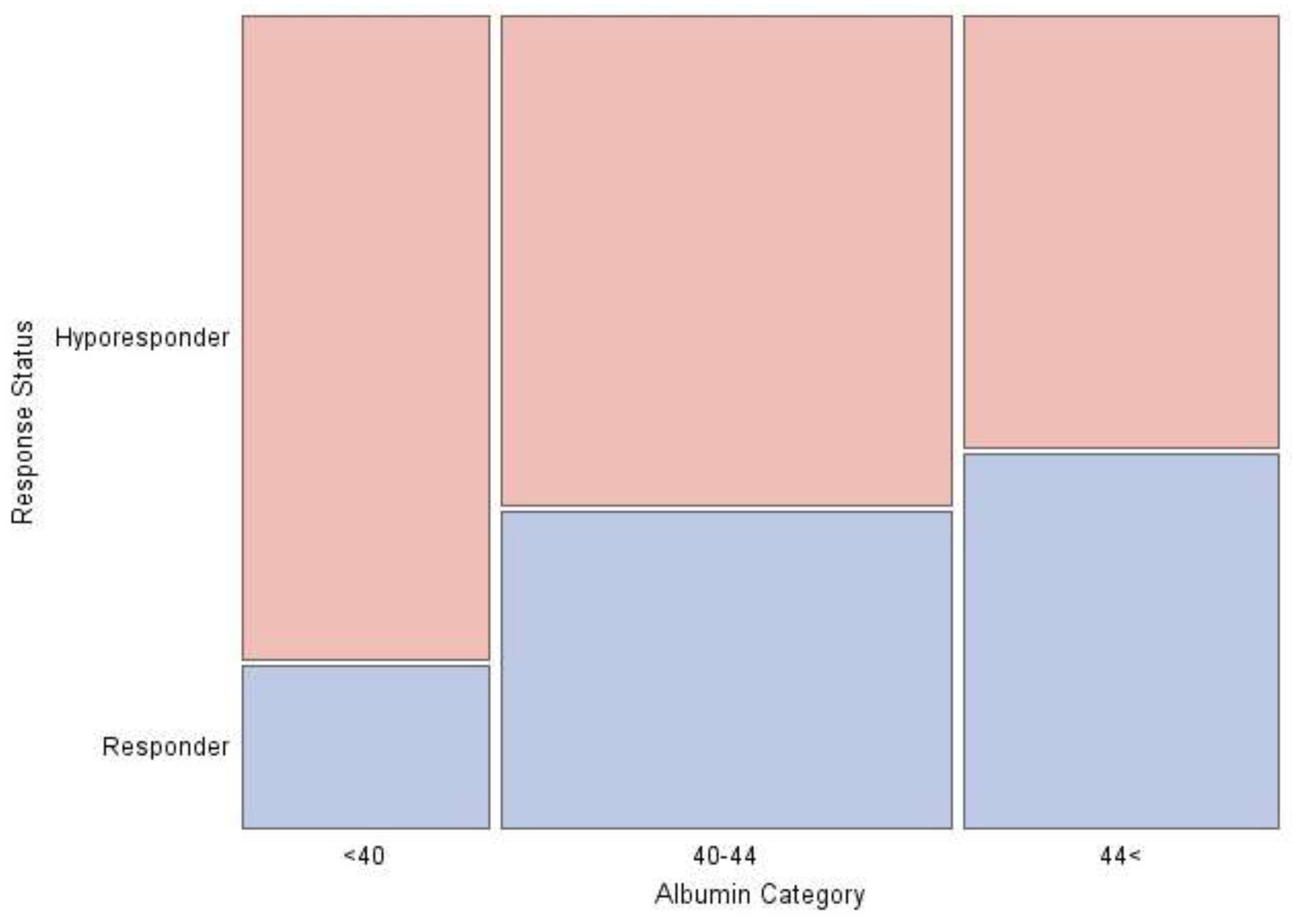
Figure 2.
Distribution of Response Status by LDL-C Levels. LDL-C; low-density lipoprotein cholesterol.
Figure 2.
Distribution of Response Status by LDL-C Levels. LDL-C; low-density lipoprotein cholesterol.
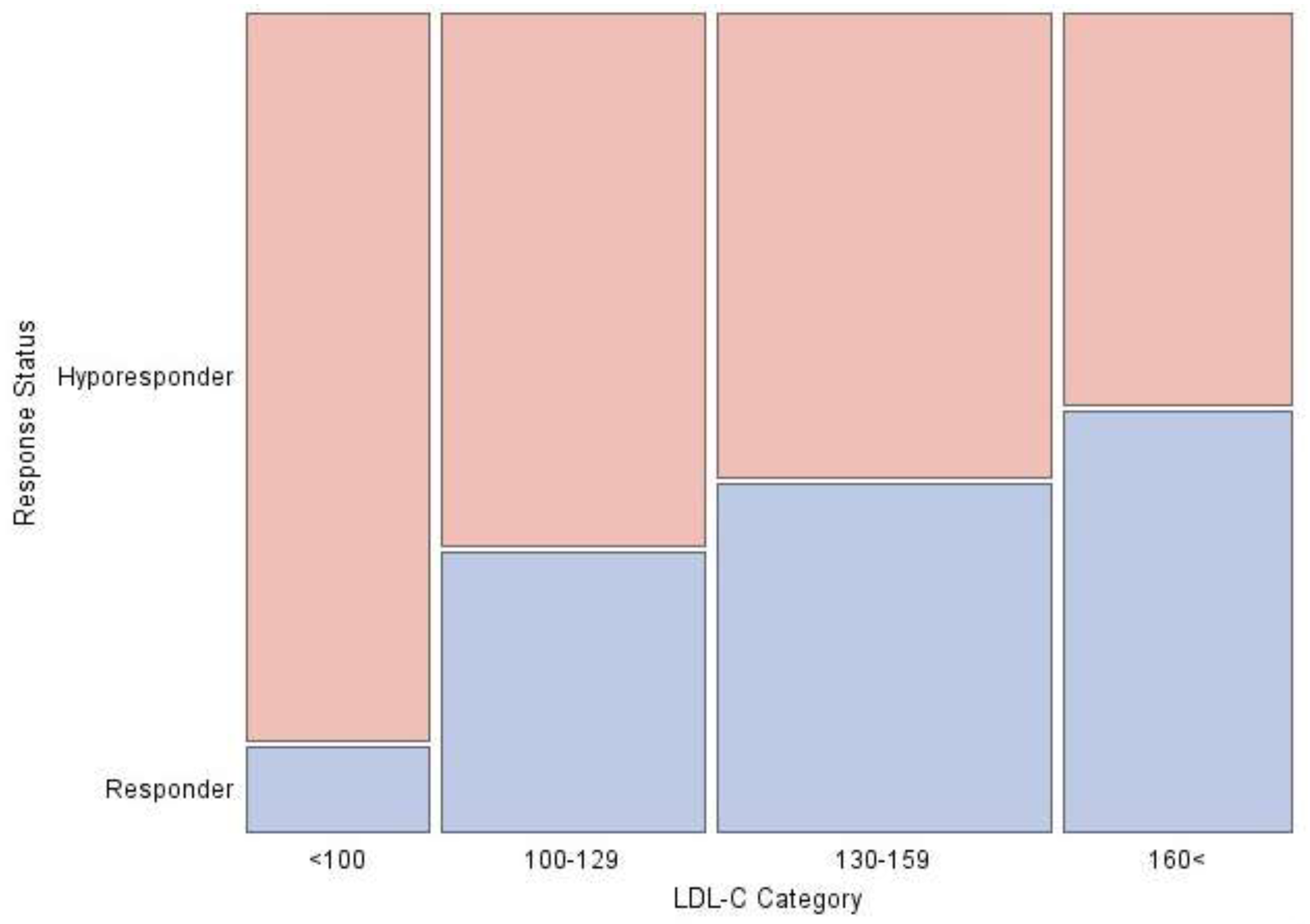
Figure 3.
Receiver Operating Characteristic Curve for Albumin.
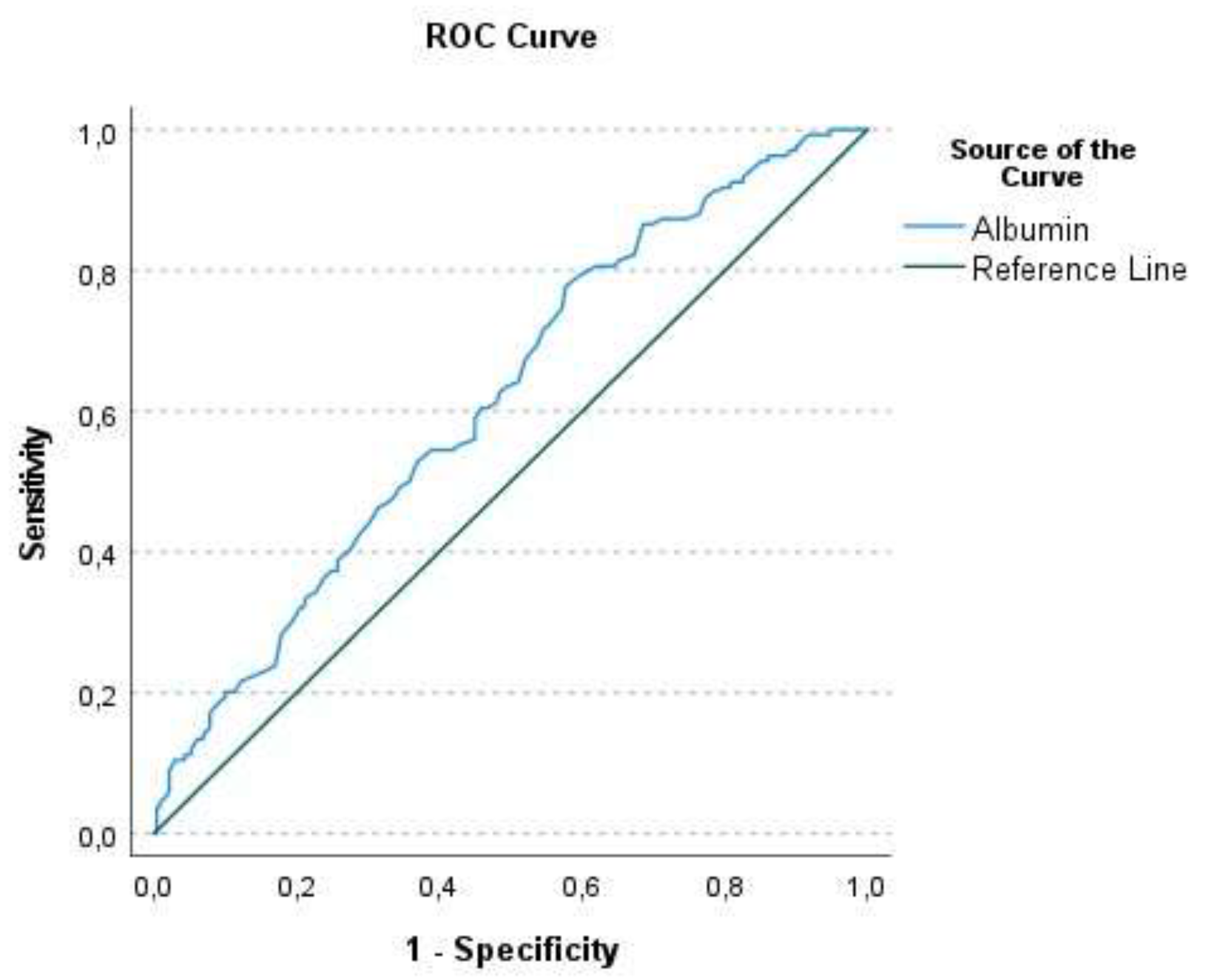
Figure 4.
ROC curve for LDL Cholesterol.
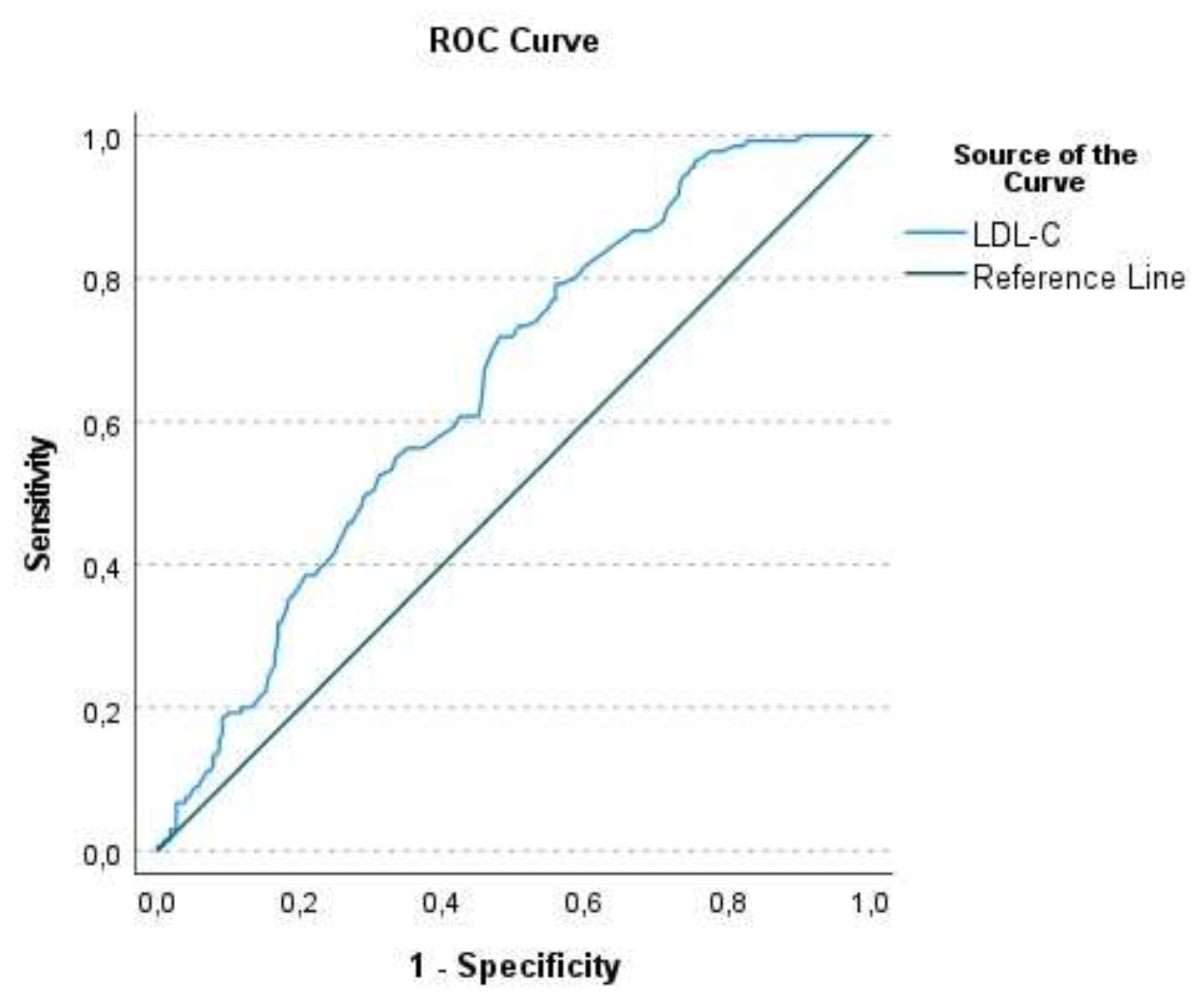

Table 1.
Demographic, clinical and laboratory characteristics of patients by response status.
| Response Status | |||||
| Hyporesponder (n=231) |
Responder (n=135) |
Total (N=366) |
P-value | ||
| Age, years | 58.8 (10.87) | 58.5 (10.97) | 58.7 (10.89) | .9042 | |
| Male, n (%) | 200 (86.6%) | 109 (80.7%) | 309 (84.4%) | .1372 | |
| Diagnosis | .2022 | ||||
| STEMI, n (%) | 136 (58.9%) | 83 (61.5%) | 219 (59.8%) | ||
| Non-STEMI, n (%) | 83 (35.9%) | 50 (37.0%) | 133 (36.3%) | ||
| USAP, n (%) | 12 (5.2%) | 2 (1.5%) | 14 (3.8%) | ||
| DM, n (%) | 91 (39.4%) | 50 (37.0%) | 141 (38.5%) | .6548 | |
| HT, n (%) | 87 (37.7%) | 55 (40.7%) | 142 (38.8%) | .5598 | |
| Smoking Status | .6782 | ||||
| Non-smoker, n (%) | 61 (26.4%) | 41 (30.4%) | 102 (27.9%) | ||
| Smoker, n (%) | 142 (61.5%) | 80 (59.3%) | 222 (60.7%) | ||
| Ex-smoker, n (%) | 28 (12.1%) | 14 (10.4%) | 42 (11.5%) | ||
| EF, % | 50.3 (8.52) | 50.0 (9.59) | 50.2 (8.92) | .9338 | |
| Glucose, mg/dL | 152.0 (81.73) | 148.3 (68.48) | 150.6 (77.03) | .9404 | |
| BUN, mg/dL | 16.3 (5.85) | 15.3 (4.57) | 15.9 (5.43) | .2647 | |
| Creatinine, mg/dL | 1.0 (0.21) | 1.0 (0.18) | 1.0 (0.20) | .5873 | |
| GFR, mL/min/1.73 m2 | 80.0 (17.54) | 80.3 (16.18) | 80.1 (17.03) | .9579 | |
| Sodium, mmol/L | 137.6 (3.06) | 137.4 (3.11) | 137.6 (3.08) | .3769 | |
| ALT, U/L | 30.0 (20.06) | 28.6 (15.90) | 29.5 (18.62) | .9488 | |
| Albumin, g/L | 41.7 (3.78) | 43.3 (3.31) | 42.3 (3.70) | .0002 | |
| Uric Acid, mg/dL | 5.6 (1.60) | 5.5 (1.42) | 5.6 (1.53) | .7185 | |
| CRP, mg/L | 15.1 (33.08) | 10.3 (24.39) | 13.3 (30.19) | .9837 | |
| WBC, 103/mm3 | 11.4 (3.66) | 11.5 (3.61) | 11.4 (3.63) | .9975 | |
| HGB, g/dL | 14.2 (1.89) | 14.8 (1.72) | 14.4 (1.85) | .0016 | |
| NEU, 103/mm3 | 8.3 (3.53) | 8.1 (3.40) | 8.2 (3.48) | .7021 | |
| LYM, 103/mm3 | 2.2 (1.12) | 2.4 (1.14) | 2.3 (1.13) | .0931 | |
| Total Cholesterol, mg/dL | 206.8 (49.90) | 227.6 (50.43) | 214.5 (51.03) | <.0001 | |
| HDL-C, mg/dL | 46.3 (11.10) | 47.6 (11.18) | 46.8 (11.13) | .2814 | |
| VLDL-C, mg/dL | 38.8 (36.87) | 41.7 (35.27) | 39.8 (36.26) | .3759 | .3759 |
| .3759 | |||||
| Triglyceride, mg/dL | 193.8 (184.33) | 208.4 (176.33) | 199.2 (181.31) | .3749 | |
| LDL-C, mg/dL | 126.6 (39.90) | 147.3 (37.45) | 134.2 (40.23) | <.0001 | |
| Follow-up LDL-C, mg/dL | 86.4 (27.28) | 59.4 (17.09) | 76.4 (27.33) | <.0001 | |
| % Reduction | 32.3 (13.45) | 59.5 (7.40) | 42.3 (17.50) | <.0001 | |
| Statin Dose, n (%) | .3733 | ||||
| 40 mg | 222 (96.1%) | 127 (94.1%) | 349 (95.4%) | ||
| 80 mg | 9 (3.9%) | 8 (5.9%) | 17 (4.6%) | ||
1Chi-square p-value; 2Mann–Whitney U p-value; ALT, alanine transaminase; BUN, blood urea nitrogen; CRP, C-reactive protein; DM, diabetes mellitus; EF, ejection fraction; GFR, glomerular filtration rate; HGB, hemoglobin; HDL-C, high-density lipoprotein cholesterol; HT, hypertension; LDL-C, low-density lipoprotein cholesterol; LYM, lymphocyte; NEU, neutrophil; STEMI, ST-elevation myocardial infarction; USAP, unstable angina pectoris; VLDL-C, very low-density lipoprotein cholesterol; WBC, white blood cell.
Table 2.
Relationship between LDL-C categories and albumin with hyporesponsiveness.
| Albumin Category | ||||||
| LDL-C Category |
<40 | 40-44 | 44< | Total | P-value | |
| <100 | (n=23) | (n=31) | (n=12) | (n=66) | ||
| Response Status, n (%) | .4521 | |||||
| Hyporesponder | 22 (95.7%) | 27 (87.1%) | 10 (83.3%) | 59 (89.4%) | ||
| Responder | 1 (4.3%) | 4 (12.9%) | 2 (16.7%) | 7 (10.6%) | ||
| p-value | .000 | .000 | .022 | .000 | ||
| 100–129 | (n=30) | (n=41) | (n=25) | (n=96) | ||
| Response Status, n (%) | .0865 | |||||
| Hyporesponder | 24 (80.0%) | 26 (63.4%) | 13 (52.0%) | 63 (65.6%) | ||
| Responder | 6 (20.0%) | 15 (36.6%) | 12 (48.0%) | 33 (34.4%) | ||
| p-value | .001 | .088 | .845 | .002 | ||
| 130–159 | (n=30) | (n=56) | (n=35) | (n=121) | ||
| Response Status, n (%) | .1147 | |||||
| Hyporesponder | 22 (73.3%) | 29 (51.8%) | 18 (51.4%) | 69 (57.0%) | ||
| Responder | 8 (26.7%) | 27 (48.2%) | 17 (48.6%) | 52 (43.0%) | ||
| p-value | .011 | .791 | .868 | .123 | ||
| ≥160 | (n=6) | (n=35) | (n=42) | (n=83) | ||
| Response Status, n (%) | .9923 | |||||
| Hyporesponder | 3 (50.0%) | 17 (48.6%) | 20 (47.6%) | 40 (48.2%) | ||
| Responder | 3 (50.0%) | 18 (51.4%) | 22 (52.4%) | 43 (51.8%) | ||
| p-value | 1.000 | .868 | .761 | .744 | ||
| 1Chi-square p-value; LDL-C, low-density lipoprotein cholesterol | ||||||
Table 3.
Results of the Cochran–Armitage Trend analysis.
| Response Status | ||||
| Hyporesponder (n=231) |
Responder (n=135) |
Total (n=366) |
P-value | |
| Albumin Category, n (%) | .0004 | |||
| <40 | 71 (30.7%) | 18 (13.3%) | 89 (24.3%) | |
| 40–44 | 99 (42.9%) | 64 (47.4%) | 163 (44.5%) | |
| ≥44 | 61 (26.4%) | 53 (39.3%) | 114 (31.1%) | |
| LDL-C Category, n (%) | <.0001 | |||
| <100 | 59 (25.5%) | 7 (5.2%) | 66 (18.0%) | |
| 100–129 | 63 (27.3%) | 33 (24.4%) | 96 (26.2%) | |
| 130–159 | 69 (29.9%) | 52 (38.5%) | 121 (33.1%) | |
| ≥160 | 40 (17.3%) | 43 (31.9%) | 83 (22.7%) | |
1 p-value for the Cochran–Armitage Trend Test.
Table 4.
Measures of Association.
| Albumin | LDL-C | |||||||
| Value | ASE | Lower95% CI | Upper95% CI | Value | ASE | Lower95% CI | Upper95% CI | |
| Somers’ D C|R | .2171 | .0552 | .1089 | .3253 | .3086 | .0547 | .2013 | .4159 |
| Somers’ D R|C | .1566 | .0398 | .0785 | .2346 | .1947 | .0347 | .1267 | .2627 |
| Pearson Correlation | .1968 | .0491 | .1005 | .2931 | .2730 | .0464 | .1821 | .3639 |
| Spearman Correlation | .1948 | .0495 | .0978 | .2918 | .2677 | .0475 | .1745 | .3608 |
ASE, average square error; CI, confidence interval; LDL-C, low-density lipoprotein cholesterol.
Table 5.
Univariate and multivariate logistic regression analysis for the predictors of response status (hyporesponder or responder).
Table 5.
Univariate and multivariate logistic regression analysis for the predictors of response status (hyporesponder or responder).
| Response Status = Responder | ||||
| Univariate analysis | Multivariate aanalysis | |||
| Covariate | Odds Ratio (95% CI) |
OR P-value | Odds Ratio (95% CI) |
OR P-value |
| Age | 1.0 (1.0-1.0) | 0.815 | ||
| Sex (Female) | 1.5 (0.9-2.7) | 0.140 | ||
| MI Type | ||||
| non-STEMI | 1.0 (0.6-1.5) | 0.954 | ||
| USAP | 0.3 (0.1-1.3) | 0.096 | ||
| DM | 1.1 (0.7-1.7) | 0.656 | ||
| HT | 0.9 (0.6-1.4) | 0.561 | ||
| Smoking Status | ||||
| Ex-smoker | 0.9 (0.4-1.8) | 0.738 | ||
| Non-smoker | 1.2 (0.7-1.9) | 0.474 | ||
| EF | 1.0 (1.0-1.0) | 0.755 | ||
| Glucose | 1.0 (1.0-1.0) | 0.643 | ||
| Bun | 1.0 (0.9-1.0) | 0.066 | ||
| Creatinine | 0.6 (0.2-1.7) | 0.362 | ||
| GFR | 1.0 (1.0-1.0) | 0.897 | ||
| Sodium | 1.0 (0.9-1.0) | 0.465 | ||
| ALT | 1.0 (1.0-1.0) | 0.484 | ||
| Albumin | 1.1 (1.1-1.2) | 0.000 | 0.8 (0.5-1.5) | 0.539 |
| Uric Acid | 1.0 (0.9-1.1) | 0.907 | ||
| WBC | 1.0 (0.9-1.1) | 0.940 | ||
| HGB | 1.2 (1.1-1.4) | 0.003 | 0.3 (0.1-0.9) | 0.025 |
| NEU | 1.0 (0.9-1.1) | 0.702 | ||
| LYM | 1.2 (1.0-1.4) | 0.133 | ||
| Total Cholesterol | 1.0 (1.0-1.0) | 0.000 | 1.0 (0.9-1.1) | 0.828 |
| HDL-C | 1.0 (1.0-1.0) | 0.288 | ||
| LDL-C | 1.0 (1.0-1.0) | 0.000 | 17.5 (5.9-52.1) | 0.000 |
| % Reduction | 1.7 (1.0-3.0) | 0.066 | ||
| Follow-up LDL-C | 0.9 (0.9-1.0) | 0.000 | 0.0 (0.0-0.0) | 0.000 |
| VLDL-C | 1.0 (1.0-1.0) | 0.471 | ||
| Triglycerides | 1.0 (1.0-1.0) | 0.469 | ||
| C-Reactive Protein | 1.0 (1.0-1.0) | 0.243 | ||
| Statin Dose (40 mg) | 0.6 (0.2-1.7) | 0.378 | ||
ALT, alanine transaminase; BUN, blood urea nitrogen; CI, confidence interval; DM, diabetes mellitus; EF, ejection fraction; GFR, glomerular filtration rate; HGB, hemoglobin; HDL-C, high-density lipoprotein-cholesterol; HT, hypertension; LDL-C, low-density lipoprotein-cholesterol; LYM, lymphocyte; MI, myocardial infarction; NEU, neutrophil; OR, odds ratio; STEMI, ST-elevation myocardial infarction; USAP, unstable angina pectoris; VLDL-C, very low-density lipoprotein cholesterol; WBC, white blood cell.
Table 6.
ROC Analysis Results for Albumin and LDL-C.
| AUC | SE | 95%CI | p | Cut off | Sensitivity | Specificity | ||
| Albumin | 0.618 | 0.030 | 0.559 | 0.676 | 0.000 | 41.15 | 0.776 | 0.424 |
| LDL-C | 0.652 | 0.029 | 0.596 | 0.708 | 0.000 | 128.50 | 0.719 | 0.519 |
AUC, area under the curve; CI, confidence interval; LDL-C, low-density lipoprotein cholesterol; ROC, receiver operating characteristic; SE, standard error.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



