
Submitted:
02 February 2026
Posted:
03 February 2026
You are already at the latest version
Abstract
Breast-conserving therapy (BCT), consisting of lumpectomy followed by adjuvant radiation, provides oncologic outcomes equivalent to mastectomy for many patients with breast cancer. As survivorship increases, the demand for aesthetic restoration after BCT has grown; however, reconstructive strategies in this setting remain less standardized than those following mastectomy. Reconstruction after BCT presents distinct challenges due to partial tissue loss, nonuniform radiation injury, progressive fibrosis, and wide variability in patient expectations and tolerance for revision surgery. Consequently, mastectomy-based reconstructive algorithms are often insufficient for guiding care in this population. This review synthesizes contemporary reconstructive options following BCT through a personalized medicine framework, emphasizing patient-specific risk factors that influence technique selection, timing, and long-term outcomes. Key determinants include radiation exposure, breast morphology, comorbid conditions, prior breast surgery, and psychosocial preferences. Oncoplastic volume displacement, implant-based augmentation, fat grafting, and autologous reconstruction each demonstrate distinct risk profiles in the post-BCT tissue environment and require individualized application. Timing of reconstruction and willingness to undergo staged procedures play a central role in outcome durability and patient satisfaction. Across reconstructive strategies, revision burden emerges as a clinically meaningful, patient-centered outcome that is not adequately captured by traditional short-term complication metrics. A risk-stratified approach that integrates individualized risk assessment with transparent counseling and shared decision-making may improve alignment between reconstructive planning and patient goals. Personalized reconstruction after BCT requires moving beyond technique-driven paradigms toward flexible, longitudinal care pathways. Future efforts should focus on developing BCT-specific predictive models and incorporating patient-reported outcomes to advance personalized reconstructive care.
Keywords:
breast conserving therapy
; breast reconstruction
; patient reported outcomes
; aesthetic
; personalized medicine
Introduction
Breast-conserving therapy (BCT), consisting of lumpectomy followed by adjuvant radiation, has become a cornerstone of contemporary breast cancer management, offering oncologic outcomes equivalent to mastectomy for appropriately selected patients while preserving native breast tissue [1,2]. As long-term survival has improved, increasing attention has been directed toward the aesthetic and psychosocial sequelae of BCT [3,4,5,6]. Despite the widespread adoption of breast conservation, reconstructive strategies for patients who experience contour deformity, volume asymmetry, or radiation-induced tissue changes after lumpectomy remain far less standardized than those following mastectomy [7].
Reconstruction after BCT presents a distinct clinical challenge that differs fundamentally from post-mastectomy reconstruction. Unlike mastectomy patients, individuals treated with lumpectomy retain variable amounts of breast tissue that have often been exposed to nonuniform radiation fields, resulting in fibrosis, volume contraction, and compromised vascularity. These changes create a heterogeneous tissue environment in which reconstructive outcomes are less predictable, and complication profiles vary widely [8,9]. Moreover, reconstructive interventions in this setting must account for ongoing oncologic surveillance, patient tolerance for asymmetry or staged procedures, and the cumulative burden of revision surgery over time [10].
Current reconstructive paradigms are largely derived from mastectomy-based algorithms and are frequently applied to BCT patients without sufficient consideration of their unique risk profiles. Implant-based and fat grafting techniques following lumpectomy are often discussed in isolation, with limited integration of patient-specific factors such as radiation exposure, breast morphology, comorbidities, and prior surgical history [11,12,13]. As a result, counseling may inadequately reflect the true likelihood of complications, revision procedures, or delayed aesthetic dissatisfaction in this population.
Personalized medicine offers a framework through which reconstruction after BCT can be more effectively tailored to the individual patient. Rather than emphasizing a single “best” reconstructive approach, personalization prioritizes risk stratification, patient preferences, and contextual decision-making to guide technique selection and timing. In this model, outcomes such as revision burden, durability of aesthetic results, and patient-reported satisfaction become central metrics of success, complementing traditional complication rates.
This review aims to synthesize the existing literature on reconstructive options following breast-conserving therapy through a personalized medicine lens. We focus on patient-specific risk factors that influence reconstructive outcomes, examine how these risks intersect with available reconstructive techniques, and propose a risk-stratified framework to guide individualized decision-making. By integrating oncologic considerations, tissue characteristics, and patient goals, this review seeks to provide a practical and personalized approach to reconstruction after BCT that better aligns surgical planning with long-term outcomes and patient expectations.
Unique Challenges After Breast-Conserving Therapy
Reconstruction following breast-conserving therapy (BCT) occurs within a biologically and anatomically altered tissue environment that differs substantially from that encountered after mastectomy. The combination of partial tissue excision and adjuvant radiation produces variable changes in breast volume, contour, and skin quality, resulting in reconstructive challenges that can be underestimated [14,15]. Unlike mastectomy reconstruction, where the surgical field is relatively uniform and reconstruction replaces the entirety of the breast mound, post-BCT reconstruction must integrate new volume or contour correction into a variably asymmetric and potentially fibrotic, scarred breast.
Altered Tissue Biology After Lumpectomy and Radiation
Lumpectomy creates a localized volume deficit that may evolve over time as postoperative changes and radiation effects progress. Adjuvant radiation further compounds these changes by inducing fibrosis, microvascular injury, and chronic inflammation, leading to progressive tissue stiffening, skin thickening, and volume contraction [16]. Importantly, radiation fields following lumpectomy are often nonuniform, resulting in asymmetric tissue injury that can affect reconstructive predictability. This heterogeneity in tissue quality increases the risk of wound healing complications, fat necrosis, capsular contracture, and suboptimal aesthetic outcomes, particularly when implant-based or volume replacement techniques are employed [17,18].
The temporal nature of radiation-induced changes adds another layer of complexity. Tissue characteristics may continue to evolve for years after treatment, meaning that reconstructive outcomes achieved early may not be durable over time [19]. This dynamic process complicates both surgical planning and patient counseling, as the final aesthetic result may not stabilize until long after reconstruction has been completed.
Oncologic and Surveillance Considerations
Reconstructive decision-making after BCT must also remain closely aligned with oncologic priorities. Margin status, tumor biology, and the need for ongoing surveillance imaging can influence both the timing and type of reconstruction offered [14]. Concerns regarding interference with mammographic or magnetic resonance imaging surveillance persist, particularly with implant-based augmentation or extensive fat grafting. While contemporary imaging techniques have largely mitigated these issues, lingering uncertainty may influence patient and provider comfort with certain reconstructive approaches [20,21].
Additionally, reconstructive interventions following BCT must account for the possibility of future oncologic events, including ipsilateral recurrence or the need for completion mastectomy [22]. Reconstructive strategies that limit future options or increase surgical complexity in the event of recurrence may not be appropriate for all patients, underscoring the importance of individualized risk assessment [14].
Aesthetic Expectations and Asymmetry Tolerance
Patients undergoing reconstruction after BCT often seek restoration rather than replacement of the breast, with expectations that their postoperative appearance will approximate their pre-treatment baseline. However, tolerance for residual asymmetry varies widely and is influenced by breast size, pre-existing asymmetry, clothing preferences, and psychosocial factors [23]. Unlike mastectomy reconstruction, where bilateral symmetry can often be addressed concurrently, post-BCT reconstruction may require contralateral surgery, staged procedures, or acceptance of persistent asymmetry.
These considerations make reconstruction after BCT particularly sensitive to patient expectations and risk tolerance. Some patients may prioritize minimal intervention and accept modest asymmetry, while others may pursue multiple revision procedures to achieve a desired aesthetic outcome. Failure to align reconstructive strategy with these individualized preferences can lead to dissatisfaction even in the absence of surgical complications, highlighting the vitality of appropriate preoperative counseling [24].
Revision Burden as a Distinct Outcome Metric
A defining feature of reconstruction after BCT is the cumulative burden of revision surgery [8]. Many reconstructive approaches in this setting, particularly fat grafting and implant augmentation, are inherently staged and may require multiple procedures to achieve or maintain acceptable outcomes. Radiation-related changes, delayed volume loss, and progressive fibrosis further contribute to the need for secondary interventions [25].
Traditional outcome reporting, which often focuses on short-term complication rates, inadequately captures this longitudinal experience [26,27]. For BCT patients, revision burden represents a clinically meaningful and patient-centered outcome that must be incorporated into reconstructive planning and counseling [8,23]. Recognizing revision likelihood as a function of patient-specific risk factors provides a foundation for a more personalized and transparent approach to reconstruction.
Patient Factors Driving Personalized Reconstruction After Breast Conserving Therapy
Reconstruction following breast-conserving therapy (BCT) is uniquely sensitive to patient-level variability (Table 1). Unlike mastectomy reconstruction, where standardized pathways can often be applied, outcomes after BCT are heavily influenced by a constellation of demographic, treatment-related, anatomic, and psychosocial factors [3,28,29,30]. Appreciating how these variables interact is essential for tailoring reconstructive strategy, counseling patients effectively, and anticipating both complications and revision burden.
Demographic and Medical Factors
Patient comorbidities play a central role in determining reconstructive risk after BCT, particularly in the setting of irradiated tissue. Elevated body mass index, smoking history, diabetes, and connective tissue disease have all been associated with impaired wound healing, increased rates of infection, and compromised aesthetic outcomes [29,31,32,33,34]. In the post-BCT population, these risks are amplified by radiation-induced microvascular injury and fibrosis, which limit tissue reserve and reduce tolerance for additional surgical insult [35,36,37,38]. Age may also influence reconstructive decision-making, not only through physiologic considerations but through differences in aesthetic priorities, willingness to undergo staged procedures, and tolerance for asymmetry [39,40]. Importantly, these demographic factors rarely operate in isolation; rather, they compound one another, underscoring the need for holistic risk assessment rather than single-variable exclusion criteria [41].
Treatment-Related Factors
Among all patient-specific variables, prior radiation exposure exerts the most profound and consistent influence on reconstructive outcomes after BCT [42]. Radiation dose, fractionation, and field geometry affect both the severity and distribution of tissue injury [43,44]. Nonuniform radiation fields following lumpectomy create asymmetric patterns of fibrosis and volume loss that complicate reconstruction and reduce predictability, particularly for implant-based approaches [45]. The timing of reconstruction relative to radiation is another critical determinant of risk. Early intervention may occur before radiation effects have fully declared themselves, whereas delayed reconstruction must contend with established fibrosis and tissue contraction [45,46]. Chemotherapy, particularly when administered concurrently or sequentially with radiation, may further impair wound healing and influence the optimal timing of reconstruction [47,48]. These factors highlight the importance of individualized timing decisions rather than strict adherence to dogma.
Breast-Specific and Anatomic Factors
Breast morphology strongly influences reconstructive options after BCT. Breast size, degree of ptosis, and baseline asymmetry affect the feasibility of volume displacement techniques and the likelihood that contralateral symmetrization will be required [15,28,49,50]. Smaller breasts with limited tissue redundancy may be less forgiving of lumpectomy-related volume loss and may necessitate volume replacement strategies, whereas larger breasts may better accommodate oncoplastic rearrangement [17].
Tumor location also has important reconstructive implications. Defects in the lower pole or central breast often produce more visible deformities and are less amenable to simple rearrangement, while upper pole defects may be more easily concealed [29,51]. Prior breast surgery, including augmentation or reduction, introduces additional complexity by altering tissue planes, vascularity, and implant–tissue interactions [52]. Patients with pre-existing implants represent a distinct subgroup in whom implant-based augmentation after lumpectomy may be appealing but carries unique risks related to capsular contracture and implant malposition in the setting of radiation [53].
Personalized Decision-Making After Breast-Conserving Therapy: Risk-Stratified Reconstructive Options
Reconstructive decision-making after breast-conserving therapy (BCT) is best conceptualized as a continuum of options rather than a discrete set of interchangeable techniques. Patient-specific risk factors, including tissue quality, radiation exposure, breast morphology, and tolerance for revision, should guide both the selection and sequencing of reconstructive interventions [14,15,49,61,62]. A risk-stratified framework allows surgeons to match reconstructive intensity to patient context, balancing aesthetic goals against the likelihood of complications and revision burden (Figure 1) [15].
Oncoplastic Volume Displacement Techniques
Oncoplastic volume displacement remains the preferred first-line reconstructive approach for many patients undergoing BCT, particularly those with moderate to large breasts and favorable tumor location [63,64]. By rearranging remaining breast tissue to fill the lumpectomy defect, these techniques preserve native tissue characteristics and avoid the introduction of foreign material or grafted fat into irradiated fields.
Patients with larger breast volume, sufficient tissue redundancy, and lower degrees of baseline asymmetry are generally best suited for volume displacement approaches [65,66]. Tumors located in the upper pole or lateral breast are often more amenable to these techniques, whereas lower pole and central defects may pose greater challenges [29,67]. Radiation exposure remains a critical modifier of outcomes; although oncoplastic rearrangement can be performed in irradiated tissue, fibrosis and volume contraction may compromise long-term symmetry [68].
Risk stratification is particularly important when considering contralateral symmetrization. While bilateral procedures can improve symmetry, they increase operative complexity and may not align with all patients’ preferences or risk tolerance [69,70]. Personalized counseling should address the likelihood of delayed asymmetry due to radiation-related changes and the potential need for future revision even after initially successful oncoplastic reconstruction [23].
Implant-Based Augmentation After Lumpectomy
Implant-based augmentation following lumpectomy represents a distinct and under-discussed reconstructive pathway. This approach may be particularly appealing to patients with small breast volume, limited tissue redundancy, or pre-existing augmentation who desire restoration of volume rather than tissue rearrangement [17,71]. However, the introduction of implants into a partially irradiated breast fundamentally alters the risk profile and demands careful patient selection.
Radiation exposure is the dominant determinant of outcomes in this setting. Even when radiation is delivered in a partial or tangential field, capsular contracture, implant malposition, and aesthetic distortion are more common than in nonirradiated breasts [72,73]. The plane of implant placement further modulates risk. Subglandular placement may exacerbate visible contour irregularities in thin or fibrotic tissue, whereas subpectoral or prepectoral placement introduces trade-offs related to animation deformity, implant coverage, and interaction with irradiated skin [74,75,76,77,78].
Patients with prior breast augmentation constitute a unique subgroup. In these individuals, implant exchange or augmentation after lumpectomy may appear straightforward but carries heightened risk of contracture and asymmetry when radiation is added to a previously unirradiated implant pocket [53,73,79]. Risk stratification should incorporate not only implant history but also patient expectations regarding long-term implant maintenance and tolerance for potential explantation or conversion to alternative reconstructive strategies.
Given these considerations, implant-based augmentation after BCT may be most appropriate for carefully selected patients with limited radiation exposure, favorable tissue quality, and a clear understanding of the likelihood of future revision. In this context, revision burden, rather than short term surgical complications, often represents the most meaningful outcome for patients.
Fat Grafting as Volume Replacement and Tissue Modulation
Autologous fat grafting occupies a central role in personalized reconstruction after BCT, offering both volume replacement and potential mitigation of radiation-induced tissue injury [58,80,81]. Its versatility allows it to be used as a primary reconstructive modality for small defects, an adjunct to oncoplastic rearrangement, or a salvage technique following implant-based reconstruction [80,82]. Patient selection is critical. Fat grafting is best suited for individuals with sufficient donor sites, realistic expectations regarding achievable volume, and willingness to undergo staged procedures [11]. In irradiated breasts, graft take may be unpredictable, and multiple sessions are often required [11,83]. While concerns regarding oncologic safety have diminished with accumulating evidence, ongoing surveillance considerations and patient anxiety may still influence acceptance of this approach [84,85].
From a personalization standpoint, fat grafting offers granular control over reconstructive intensity [86]. Small-volume grafting may address contour irregularities with minimal morbidity, while larger-volume reconstruction increases the likelihood of fat necrosis, calcifications, and need for revision [87]. Counseling should emphasize that fat grafting is frequently iterative and that aesthetic stability may evolve over time as radiation effects continue to unfold [58,83].
Autologous Reconstruction in Select Post-BCT Patients
Although less common, autologous tissue reconstruction may be indicated in select patients following BCT, particularly when prior reconstruction has failed or radiation-related deformity is severe [73,88]. These cases often represent salvage scenarios in which local tissue options have been exhausted or are no longer viable [88]. Risk stratification is essential when considering autologous reconstruction in this population. Patients must be evaluated for donor site suitability, overall medical fitness, and willingness to undergo more extensive surgery [73]. While autologous tissue may offer improved durability and aesthetic outcomes in heavily irradiated fields, the morbidity of flap-based reconstruction must be weighed against patient goals and expectations [42,61].
Integrating Risk Stratification into Technique Selection
Rather than viewing reconstructive options as competing alternatives, a personalized approach frames them as complementary tools that can be sequenced or combined based on evolving risk profiles. Patients with low-risk features may achieve durable results with oncoplastic rearrangement alone, whereas higher-risk individuals may require staged fat grafting, implant augmentation with careful counseling, or eventual conversion to autologous reconstruction [73,89]. This risk-stratified paradigm emphasizes adaptability over rigidity. As tissue characteristics and patient priorities change over time, reconstructive strategy should be revisited, reinforcing the importance of longitudinal planning and shared decision-making in reconstruction after BCT.
Personalized Decision-Making After Breast-Conserving Therapy: Timing of Reconstruction
The timing of reconstruction following breast-conserving therapy (BCT) is a critical and highly individualized decision that significantly influences both aesthetic outcomes and complication risk (Table 2) [45,73,90]. Unlike mastectomy reconstruction, where immediate reconstruction is often encouraged to preserve the skin envelope and streamline care, reconstruction after BCT must account for the evolving biological effects of radiation, oncologic treatment sequencing, and patient readiness for additional surgery [45].
Immediate Versus Delayed Reconstruction
Immediate reconstruction at the time of lumpectomy or shortly thereafter may be appropriate for select patients with favorable risk profiles, limited anticipated radiation effects, and clear reconstructive goals [73,90]. Oncoplastic volume displacement techniques are most employed in this setting, as they allow defect correction using native tissue before radiation-induced fibrosis becomes established [14,91,92]. For appropriately selected patients, immediate reconstruction may reduce the need for later interventions and provide early restoration of breast contour [92,93]. However, early intervention carries the risk of underestimating the extent of radiation-related changes that may emerge over time. Volume loss, skin contraction, and asymmetry may progress months to years after treatment, potentially diminishing the durability of immediate reconstructive results [19]. For patients with higher-risk features, such as extensive radiation fields, smaller breast volume, or medical comorbidities, delayed reconstruction may offer a more predictable foundation for long-term outcomes [45,94].
Reconstruction in the Post-Radiation Setting
Delayed reconstruction allows surgeons to assess the stable effects of radiation before intervening, facilitating more accurate planning and patient counseling [45,73]. In this context, reconstructive techniques such as fat grafting or implant-based augmentation can be tailored to the established tissue environment. However, delayed intervention must contend with fibrosis, reduced tissue compliance, and compromised vascularity, all of which increase the likelihood of staged procedures and revision surgery [73]. Personalization is particularly important when considering delayed implant-based reconstruction. While some patients may tolerate implant placement in a radiated breast with acceptable outcomes, others may experience progressive capsular contracture or aesthetic distortion over time [45,95,96]. Incorporating patient-specific risk factors into timing decisions helps align reconstructive strategy with long-term expectations and tolerance for revision [73,89].
Staged and Sequential Reconstruction
Many reconstructive pathways after BCT are inherently staged, reflecting both biologic realities and patient preferences. Fat grafting is often performed in multiple sessions to gradually restore volume and improve tissue quality [58,83]. Staging allows for incremental assessment of graft take, contour improvement, and patient satisfaction while minimizing morbidity [97]. Sequential approaches may also involve escalation of reconstructive intensity over time. Patients initially managed with conservative interventions may later pursue more extensive reconstruction as tissue characteristics stabilize or aesthetic priorities evolve [27,73]. This adaptability underscores the importance of framing reconstruction after BCT as a longitudinal process rather than a single operative event.
Ultimately, the optimal timing of reconstruction after BCT must integrate oncologic considerations, tissue biology, and patient-centered goals [45,73,98]. Transparent discussion of the trade-offs associated with early versus delayed intervention, including the likelihood of revision, durability of results, and impact on quality of life, is essential to personalized decision-making [98]. By tailoring timing to individual risk profiles and expectations, surgeons can better align reconstructive planning with outcomes that matter most to patients [98].
Future Directions
As the population of patients treated with breast-conserving therapy (BCT) continues to grow, there is an increasing need for reconstructive paradigms that move beyond technique-driven decision-making toward truly personalized care. Several emerging areas offer opportunities to improve risk prediction, patient selection, and long-term outcomes in this population.
First, the development of BCT-specific predictive models represents a critical unmet need. Existing reconstruction risk calculators do not adequately incorporate the heterogeneity of radiation fields, partial-volume tissue loss, or longitudinal changes in breast morphology that characterize post-BCT patients [113,114,115,116,117]. Future models should integrate treatment-specific variables, such as radiation dose distribution and timing, with patient-level factors and reconstructive technique to more accurately predict complications, revision burden, and patient-reported outcomes.
Second, advances in imaging and intraoperative assessment may enhance personalization of reconstructive planning. Preoperative imaging techniques that characterize tissue quality and vascularity, as well as intraoperative tools that assess perfusion, could help refine patient selection and guide technique choice in compromised tissue environments [118,119,120,121]. These technologies may be particularly valuable in identifying patients who are unlikely to tolerate implant-based reconstruction or who may benefit from staged fat grafting or autologous approaches.
Third, incorporation of patient-reported outcomes into both clinical practice and research is essential to advancing personalized reconstruction after BCT. Instruments that capture satisfaction, body image, and quality of life over time can provide insights into how reconstructive strategies align with patient priorities and may help identify subgroups that benefit most from specific approaches [122,123]. Embedding these measures into registries and longitudinal studies will be critical for refining shared decision-making frameworks.
Finally, future research should emphasize longitudinal follow-up and durability of outcomes [8,96,122]. Reconstruction after BCT is often an evolving process, and short-term metrics fail to capture the full patient experience [8,19]. Studies that assess outcomes over years rather than months will be essential to understanding how personalized strategies perform over time and to informing evidence-based counseling.
Conclusions
Reconstruction after breast-conserving therapy occupies a distinct and under-recognized space within breast reconstruction, characterized by heterogeneous tissue environments, evolving radiation effects, and highly individualized patient goals. A personalized, risk-stratified approach offers an effective framework for reconstructive planning after BCT. By integrating patient-specific risk factors, treatment history, and psychosocial preferences, surgeons can tailor technique selection and timing to optimize durability, minimize revision burden, and align outcomes with patient expectations. Importantly, meaningful outcomes in this setting extend beyond short-term complications to include long-term aesthetic stability and patient-reported satisfaction. By embracing personalization as a guiding principle, reconstructive strategies after breast-conserving therapy can best align with the diverse needs and priorities of patients navigating survivorship.
Author Contributions
TJS, CB, RL contributed to the conceptualization, literature search, and writing of the manuscript. NK contributed to the conceptualization, and critical review and editing of the manuscript. All authors approved the final manuscript.
Acknowledgments
The authors have no acknowledgments related to this paper to report.
Conflicts of Interest
The authors have no financial conflicts of interest related to this paper to report.
References
- Moo, T.A.; Sanford, R.; Dang, C.; Morrow, M. Overview of Breast Cancer Therapy. PET Clin. 2018, 13(3), 339–354. [Google Scholar] [CrossRef]
- Amro, C.; Sorenson, T.J.; Boyd, C.J.; et al. The Evolution of Implant-Based Breast Reconstruction: Innovations, Trends, and Future Directions. J Clin Med. 2024, 13(23). [Google Scholar] [CrossRef] [PubMed]
- Hanson, S.E.; Lei, X.; Roubaud, M.S.; et al. Long-term Quality of Life in Patients With Breast Cancer After Breast Conservation vs Mastectomy and Reconstruction. JAMA Surg 2022, 157(6), e220631. [Google Scholar] [CrossRef] [PubMed]
- Diao, K.; Lei, X.; He, W.; et al. Patient-reported Quality of Life After Breast-conserving Surgery With Radiotherapy Versus Mastectomy and Reconstruction. Ann Surg. 2023, 278(5), e1096–e1102. [Google Scholar] [CrossRef] [PubMed]
- Bekisz, J.M.; Boyd, C.J.; Salibian, A.A.; Choi, M.; Karp, N.S. Aesthetic Characteristics of the Ideal Female Breast. Plast Reconstr Surg Glob Open 2023, 11(1), e4770. [Google Scholar] [CrossRef]
- Aristokleous, I.; Saddiq, M. Quality of life after oncoplastic breast-conserving surgery: a systematic review. ANZ J Surg 2019, 89(6), 639–646. [Google Scholar] [CrossRef]
- Sorenson, T.J.; Boyd, C.J.; Cohen, O.; Choi, M.; Karp, N. Microsurgical Strategies in Post-Radiation and Revision Breast Reconstruction: Optimizing Outcomes in High-Risk Patients. Cancers (Basel) 2025, 17(23). [Google Scholar] [CrossRef]
- Finlay, B.; Kollias, V.; Hall, K.A.; et al. Long-term outcomes of breast reconstruction and the need for revision surgery. ANZ J Surg 2021, 91(9), 1751–1758. [Google Scholar] [CrossRef]
- Sorenson, T.J.; Boyd, C.J.; Hemal, K.; Choi, M.; Karp, N.; Cohen, O. Failure of Salvage in Prepectoral Implant Breast Reconstruction: A Single-Center Cohort. Am Surg. 2025, 31348251405560. [Google Scholar] [CrossRef]
- Hanson, S.E.; Kapur, S.K.; Garvey, P.B.; et al. Oncologic Safety and Surveillance of Autologous Fat Grafting following Breast Conservation Therapy. Plast Reconstr Surg 2020, 146(2), 215–225. [Google Scholar] [CrossRef]
- Al Qurashi, A.A.; Shah Mardan, Q.N.M.; Alzahrani, I.A.; et al. Efficacy of Exclusive Fat Grafting for Breast Reconstruction: An Updated Systematic Review and Meta-analysis. Aesthetic Plast Surg 2024, 48(23), 4979–4985. [Google Scholar] [CrossRef]
- Nelson, J.A.; Cordeiro, P.G.; Polanco, T.; et al. Association of Radiation Timing with Long-Term Satisfaction and Health-Related Quality of Life in Prosthetic Breast Reconstruction. Plast Reconstr Surg 2022, 150(1), 32e–41e. [Google Scholar] [CrossRef]
- Muntean, M.V.; Pop, I.C.; Ilies, R.A.; Pelleter, A.; Vlad, I.C.; Achimas-Cadariu, P. Exploring the Role of Autologous Fat Grafting in Implant-Based Breast Reconstruction: A Systematic Review of Complications and Aesthetic Results. J Clin Med 2025, 14(12). [Google Scholar] [CrossRef]
- Thiessen, F.E.F.; Tjalma, W.A.A.; Tondu, T. Breast reconstruction after breast conservation therapy for breast cancer. Eur J Obstet Gynecol Reprod Biol. 2018, 230, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Losken, A.; Hamdi, M. Partial breast reconstruction: current perspectives. Plast Reconstr Surg 2009, 124(3), 722–736. [Google Scholar] [CrossRef] [PubMed]
- Verginadis, I.I.; Citrin, D.E.; Ky, B.; et al. Radiotherapy toxicities: mechanisms, management, and future directions. Lancet 2025, 405(10475), 338–352. [Google Scholar] [CrossRef]
- Barnea, Y.; Friedman, O.; Arad, E.; et al. An Oncoplastic Breast Augmentation Technique for Immediate Partial Breast Reconstruction following Breast Conservation. Plast Reconstr Surg 2017, 139(2), 348e–357e. [Google Scholar] [CrossRef] [PubMed]
- Schaverien, M.V.; Stutchfield, B.M.; Raine, C.; Dixon, J.M. Implant-based augmentation mammaplasty following breast conservation surgery. Ann Plast Surg 2012, 69(3), 240–3. [Google Scholar] [CrossRef]
- Harfouche, C.; Reese, M.; Becker, M.; et al. Quantitative Evaluation of Breast Volume Changes Following Lumpectomy Combined with Oncoplastic Reduction Mammoplasty and Radiation Therapy. Plast Reconstr Surg 2025. [Google Scholar] [CrossRef]
- Mehta, T.S.; Lourenco, A.P.; Niell, B.L.; et al. ACR Appropriateness Criteria® Imaging After Breast Surgery. J Am Coll Radiol 2022, 19(11S), S341–S356. [Google Scholar] [CrossRef]
- Giannotti, E.; Pasculli, M.; Sella, T.; et al. ESR Essentials: post-treatment breast cancer surveillance from mammography to a more personalised approach-practice recommendations by the European Society of Breast Imaging. In Eur Radiol; 14 Aug 2025. [Google Scholar] [CrossRef]
- Jasper, J.M.; Vora, H.; Kantor, O.; et al. Management of ipsilateral breast tumor recurrence after prior breast conservation therapy. Breast Cancer Res Treat 2025, 212(2), 361–369. [Google Scholar] [CrossRef]
- Brands-Appeldoorn, A.; Maaskant-Braat, S.; Schenk, K.; Roumen, R. Cosmetic Consequences of Breast-Conserving Treatment for Breast Cancer: Something Worth Talking About. Oncologist 2019, 24(2), 172–177. [Google Scholar] [CrossRef]
- Gardfjell, A.; Dahlbäck, C.; Åhsberg, K. Patient satisfaction after unilateral oncoplastic volume displacement surgery for breast cancer, evaluated with the BREAST-Q™. World J Surg Oncol 2019, 17(1), 96. [Google Scholar] [CrossRef]
- Rochlin, D.H.; Sheckter, C.C.; Momeni, A. Failed Breast Conservation Therapy Predicts Higher Frequency of Revision Surgery following Mastectomy with Reconstruction. Plast Reconstr Surg 2022, 149(4), 811–818. [Google Scholar] [CrossRef]
- Flanagan, M.R.; Zabor, E.C.; Romanoff, A.; et al. A Comparison of Patient-Reported Outcomes After Breast-Conserving Surgery and Mastectomy with Implant Breast Reconstruction. Ann Surg Oncol. 2019, 26(10), 3133–3140. [Google Scholar] [CrossRef]
- Fitoussi, A.D.; Berry, M.G.; Couturaud, B.; Falcou, M.C.; Salmon, R.J. Management of the post-breast-conserving therapy defect: extended follow-up and reclassification. Plast Reconstr Surg. 2010, 125(3), 783–91. [Google Scholar] [CrossRef]
- Volders, J.H.; Negenborn, V.L.; Haloua, M.H.; et al. Breast-specific factors determine cosmetic outcome and patient satisfaction after breast-conserving therapy: Results from the randomized COBALT study. J Surg Oncol. 2018, 117(5), 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Meshulam-Derazon, S.; Yaacobi, D.S.; Ben-David, M.A.; et al. Identifying the Variables for Oncoplastic Reconstruction: Preoperative Assessment Tool for Breast Conserving Treatment. Aesthetic Plast Surg 2024, 48(13), 2439–2446. [Google Scholar] [CrossRef] [PubMed]
- de Boniface, J.; Szulkin, R.; Johansson, A.LV. Survival After Breast Conservation vs Mastectomy Adjusted for Comorbidity and Socioeconomic Status: A Swedish National 6-Year Follow-up of 48 986 Women. JAMA Surg 2021, 156(7), 628–637. [Google Scholar] [CrossRef]
- de Blacam, C.; Ogunleye, A.A.; Momoh, A.O.; etal. High body mass index and smoking predict morbidity in breast cancer surgery: a multivariate analysis of 26,988 patients from the national surgical quality improvement program database. Ann Surg. 2012, 255(3), 551–5. [Google Scholar] [CrossRef] [PubMed]
- Adwall, L.; Hultin, H.; Mani, M.; Norlen, O. Prospective Evaluation of Complications and Associated Risk Factors in Breast Cancer Surgery. J Oncol. 2022, 2022, 6601066. [Google Scholar] [CrossRef]
- Sorensen, L.T.; Horby, J.; Friis, E.; Pilsgaard, B.; Jorgensen, T. Smoking as a risk factor for wound healing and infection in breast cancer surgery. Eur J Surg Oncol 2002, 28(8), 815–20. [Google Scholar] [CrossRef]
- Chen, A.M.; Obedian, E.; Haffty, B.G. Breast-conserving therapy in the setting of collagen vascular disease. Cancer J 2001, 7(6), 480–91. [Google Scholar] [PubMed]
- Giaj-Levra, N.; Sciascia, S.; Fiorentino, A.; et al. Radiotherapy in patients with connective tissue diseases. Lancet Oncol. 2016, 17(3), e109–e117. [Google Scholar] [CrossRef]
- Lilla, C.; Ambrosone, C.B.; Kropp, S.; et al. Predictive factors for late normal tissue complications following radiotherapy for breast cancer. Breast Cancer Res Treat 2007, 106(1), 143–50. [Google Scholar] [CrossRef] [PubMed]
- Fijardo, M.; Kwan, J.Y.Y.; Bissey, P.A.; Citrin, D.E.; Yip, K.W.; Liu, F.F. The clinical manifestations and molecular pathogenesis of radiation fibrosis. EBioMedicine 2024, 103, 105089. [Google Scholar] [CrossRef]
- Kameni, L.E.; Januszyk, M.; Berry, C.E.; et al. A Review of Radiation-Induced Vascular Injury and Clinical Impact. Ann Plast Surg 2024, 92(2), 181–185. [Google Scholar] [CrossRef]
- Rodby, K.A.; Robinson, E.; Danielson, K.K.; Quinn, K.P.; Antony, A.K. Age-dependent Characteristics in Women with Breast Cancer: Mastectomy and Reconstructive Trends at an Urban Academic Institution. Am Surg. 2016, 82(3), 227–35. [Google Scholar] [CrossRef] [PubMed]
- Hamnett, K.E.; Subramanian, A. Breast reconstruction in older patients: A literature review of the decision-making process. J Plast Reconstr Aesthet Surg 2016, 69(10), 1325–34. [Google Scholar] [CrossRef]
- Palve, J.S.; Luukkaala, T.H.; Kaariainen, M.T. Predictive risk factors of complications in different breast reconstruction methods. Breast Cancer Res Treat 2020, 182(2), 345–354. [Google Scholar] [CrossRef]
- Jagsi, R.; Momoh, A.O.; Qi, J.; et al. Impact of Radiotherapy on Complications and Patient-Reported Outcomes After Breast Reconstruction. J Natl Cancer Inst. 2018, 110(2), 157–65. [Google Scholar] [CrossRef]
- Lee, S.F.; Kennedy, S.K.F.; Caini, S.; et al. Randomised controlled trials on radiation dose fractionation in breast cancer: systematic review and meta-analysis with emphasis on side effects and cosmesis. BMJ 2024, 386, e079089. [Google Scholar] [CrossRef]
- Allali, S.; Kirova, Y. Radiodermatitis and Fibrosis in the Context of Breast Radiation Therapy: A Critical Review. Cancers (Basel) 2021, 13(23). [Google Scholar] [CrossRef]
- Ho, A.Y.; Hu, Z.I.; Mehrara, B.J.; Wilkins, E.G. Radiotherapy in the setting of breast reconstruction: types, techniques, and timing. Lancet Oncol. 2017, 18(12), e742–e753. [Google Scholar] [CrossRef]
- Frasier, L.L.; Holden, S.; Holden, T.; et al. Temporal Trends in Postmastectomy Radiation Therapy and Breast Reconstruction Associated With Changes in National Comprehensive Cancer Network Guidelines. JAMA Oncol 2016, 2(1), 95–101. [Google Scholar] [CrossRef]
- Pinnaro, P.; Giordano, C.; Farneti, A.; et al. Impact of Sequencing Radiation Therapy and Chemotherapy on Long-Term Local Toxicity for Early Breast Cancer: Results of a Randomized Study at 15-Year Follow-Up. Int J Radiat Oncol Biol Phys 2016, 95(4), 1201–9. [Google Scholar] [CrossRef]
- Toledano, A.; Garaud, P.; Serin, D.; et al. Concurrent administration of adjuvant chemotherapy and radiotherapy after breast-conserving surgery enhances late toxicities: long-term results of the ARCOSEIN multicenter randomized study. Int J Radiat Oncol Biol Phys. 2006, 65(2), 324–32. [Google Scholar] [CrossRef] [PubMed]
- Negenborn, V.L.; Volders, J.H.; Krekel, N.M.A.; et al. Breast-conserving therapy for breast cancer: Cosmetic results and options for delayed reconstruction. J Plast Reconstr Aesthet Surg 2017, 70(10), 1336–1344. [Google Scholar] [CrossRef]
- Sorenson, T.J.; Boyd, C.J.; Karp, N.S. Hot Topics in Implant-Based Breast Reconstruction. J Clin Med. 2025, 15(1). [Google Scholar] [CrossRef]
- Waljee, J.F.; Hu, E.S.; Newman, L.A.; Alderman, A.K. Predictors of breast asymmetry after breast-conserving operation for breast cancer. J Am Coll Surg 2008, 206(2), 274–80. [Google Scholar] [CrossRef] [PubMed]
- Bleicher, R.J.; Topham, N.S.; Morrow, M. Beauty and the beast: management of breast cancer after plastic surgery. Ann Surg 2008, 247(4), 680–6. [Google Scholar] [CrossRef] [PubMed]
- Mark, R.J.; Zimmerman, R.P.; Greif, J.M. Capsular contracture after lumpectomy and radiation therapy in patients who have undergone uncomplicated bilateral augmentation mammoplasty. Radiology 1996, 200(3), 621–5. [Google Scholar] [CrossRef]
- Storm-Dickerson, T.; Das, L.; Gabriel, A.; Gitlin, M.; Farias, J.; Macarios, D. What Drives Patient Choice: Preferences for Approaches to Surgical Treatments for Breast Cancer Beyond Traditional Clinical Benchmarks. Plast Reconstr Surg Glob Open 2018, 6(4), e1746. [Google Scholar] [CrossRef]
- Vrouwe, S.Q.; Somogyi, R.B.; Snell, L.; McMillan, C.; Vesprini, D.; Lipa, J.E. Patient-Reported Outcomes following Breast Conservation Therapy and Barriers to Referral for Partial Breast Reconstruction. Plast Reconstr Surg 2018, 141(1), 1–9. [Google Scholar] [CrossRef]
- de Oliveira-Junior, I.; da Silva, F.C.B.; Sarri, A.J.; Vieira, R. Do non-mammary conditions influence patients’ cosmetic perception after breast conserving surgery? Front Oncol. 2024, 14, 1432206. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, H.; Wang, T.; et al. Psychosocial Predictors and Outcomes of Delayed Breast Reconstruction in Mastectomized Women in Mainland China: An Observational Study. PLoS One 2015, 10(12), e0144410. [Google Scholar] [CrossRef] [PubMed]
- van Turnhout, A.A.; Fuchs, S.; Lisabeth-Brone, K.; Vriens-Nieuwenhuis, E.J.C.; van der, S.l.u.i.s. WB. Surgical Outcome and Cosmetic Results of Autologous Fat Grafting After Breast Conserving Surgery and Radiotherapy for Breast Cancer: A Retrospective Cohort Study of 222 Fat Grafting Sessions in 109 Patients. Aesthetic Plast Surg 2017, 41(6), 1334–1341. [Google Scholar] [CrossRef] [PubMed]
- Forster, N.A.; Kunzi, W.; Giovanoli, P. The reoperation cascade after breast augmentation with implants: what the patient needs to know. J Plast Reconstr Aesthet Surg 2013, 66(3), 313–22. [Google Scholar] [CrossRef]
- Duraes, E.F.R.; Schwarz, G.S.; de Sousa, J.B.; et al. Factors Influencing the Aesthetic Outcome and Quality of Life After Breast Reconstruction: A Cross-sectional Study. Ann Plast Surg 2020, 84(5), 494–506. [Google Scholar] [CrossRef] [PubMed]
- Asaad, M.; Mitchell, D.; Murphy, B.; et al. Surgical Outcomes of Implant versus Autologous Breast Reconstruction in Patients with Previous Breast-Conserving Surgery and Radiotherapy. Plast Reconstr Surg 2023, 151(2), 190e–199e. [Google Scholar] [CrossRef]
- Khansa, I.; Colakoglu, S.; Curtis, M.S.; et al. Postmastectomy breast reconstruction after previous lumpectomy and radiation therapy: analysis of complications and satisfaction. Ann Plast Surg 2011, 66(5), 444–51. [Google Scholar] [CrossRef]
- Char, S.; Bloom, J.A.; Erlichman, Z.; Jonczyk, M.; Chatterjee, A.; Guo, L. How Does Oncoplastic Surgery Compare with Standard Partial Mastectomy? A Systematic Review of Patient-Reported Outcomes. Plast Reconstr Surg 2022, 150(5), 950e–958e. [Google Scholar] [CrossRef]
- Nyirady, L.E.; Czebely-Lenart, A.; Hoferica, J.; et al. Evaluating oncoplastic breast-conserving surgery: oncological safety, risks, and satisfaction-a systematic review and meta-analysis. Sci Rep. 2025. [Google Scholar] [CrossRef] [PubMed]
- Gozali, A.; Piper, M. Optimizing Outcomes in Oncoplastic Breast-Conserving Surgery. J Clin Med 2025, 14(13). [Google Scholar] [CrossRef]
- Nardello, S.M.; Bloom, J.A.; Gaffney, K.A.; Singhal, M.; Persing, S.; Chatterjee, A. Practical oncoplastic surgery techniques needed for practice. Ann Transl Med. 2023, 11(11), 383. [Google Scholar] [CrossRef]
- Anderson, B.O.; Masetti, R.; Silverstein, M.J. Oncoplastic approaches to partial mastectomy: an overview of volume-displacement techniques. Lancet Oncol. 2005, 6(3), 145–57. [Google Scholar] [CrossRef] [PubMed]
- Vindigni, V.; Marena, F.; Zanettin, C.; Bassetto, F. Breast Reconstruction: The Oncoplastic Approach. J Clin Med 2024, 13(16). [Google Scholar] [CrossRef] [PubMed]
- Lim, G.H.; Choo, C.H.; Allen, J.C.; Ng, R.P. Factors influencing decisions on contralateral symmetrisation procedure among patients with breast cancer. Singapore Med J 2022, 63(1), 42–46. [Google Scholar] [CrossRef]
- Millen, J.C.; Jackson, K.M.; Stern, S.L.; Orozco, J.I.J.; Fancher, C.E.; Grumley, J. Simultaneous Symmetry Procedure in Patients Undergoing Oncoplastic Breast-Conserving Surgery: An Evaluation of Patient Desire and Revision Rates. Ann Surg Oncol 2023, 30(10), 6135–6139. [Google Scholar] [CrossRef]
- Salinas, H.M.; Ainuz, B.Y.; Pourmoussa, A.J.; et al. Oncoplastic Augmentation Mastopexy in Breast Conservation Therapy: Retrospective Study and Postoperative Complications. Ann Plast Surg 2023, 90(1), 33–40. [Google Scholar] [CrossRef]
- Shammas, R.L.; Wang, J.; Boe, L.A.; et al. Radiation and Reconstructive Failure: Long-Term Outcomes in Two-Stage Flap Versus Implant Breast Reconstruction. Ann Surg Oncol 2025. [Google Scholar] [CrossRef]
- Oncology NCPGi. Breast Cancer.
- Sinnott, C.J.; Persing, S.M.; Pronovost, M.; Hodyl, C.; McConnell, D.; Ott Young, A. Impact of Postmastectomy Radiation Therapy in Prepectoral Versus Subpectoral Implant-Based Breast Reconstruction. Ann Surg Oncol 2018, 25(10), 2899–2908. [Google Scholar] [CrossRef]
- Sobti, N.; Weitzman, R.E.; Nealon, K.P.; et al. Evaluation of capsular contracture following immediate prepectoral versus subpectoral direct-to-implant breast reconstruction. Sci Rep. 2020, 10(1), 1137. [Google Scholar] [CrossRef] [PubMed]
- Kronowitz, S.J. Current status of implant-based breast reconstruction in patients receiving postmastectomy radiation therapy. Plast Reconstr Surg. 2012, 130(4), 513e–523e. [Google Scholar] [CrossRef] [PubMed]
- Ostapenko, E.; Nixdorf, L.; Devyatko, Y.; Exner, R.; Wimmer, K.; Fitzal, F. Prepectoral Versus Subpectoral Implant-Based Breast Reconstruction: A Systemic Review and Meta-analysis. Ann Surg Oncol 2023, 30(1), 126–136. [Google Scholar] [CrossRef]
- King, C.A.; Bartholomew, A.J.; Sosin, M.; et al. A Critical Appraisal of Late Complications of Prepectoral versus Subpectoral Breast Reconstruction Following Nipple-Sparing Mastectomy. Ann Surg Oncol. 2021, 28(13), 9150–9158. [Google Scholar] [CrossRef] [PubMed]
- Lesniak, D.M.; Millochau, J.; Wang, K.C.; et al. Breast-conserving therapy can be offered to women with prior breast augmentation. Eur J Surg Oncol 2020, 46(8), 1456–1462. [Google Scholar] [CrossRef]
- Krastev, T.; van Turnhout, A.; Vriens, E.; Smits, L.; van der Hulst, R. Long-term Follow-up of Autologous Fat Transfer vs Conventional Breast Reconstruction and Association With Cancer Relapse in Patients With Breast Cancer. JAMA Surg 2019, 154(1), 56–63. [Google Scholar] [CrossRef]
- Lindegren, A.; Schultz, I.; Sinha, I.; et al. Autologous fat transplantation alters gene expression patterns related to inflammation and hypoxia in the irradiated human breast. Br J Surg. 2019, 106(5), 563–573. [Google Scholar] [CrossRef]
- Katzel, E.B.; Bucky, L.P. Fat Grafting to the Breast: Clinical Applications and Outcomes for Reconstructive Surgery. Plast Reconstr Surg 2017, 140(5S Advances in Breast Reconstruction), 69S–76S. [Google Scholar] [CrossRef] [PubMed]
- Herly, M.; Orholt, M.; Larsen, A.; et al. Efficacy of breast reconstruction with fat grafting: A systematic review and meta-analysis. J Plast Reconstr Aesthet Surg 2018, 71(12), 1740–1750. [Google Scholar] [CrossRef]
- Wang, K.; Yu, Z.; Rong, X.; et al. Meta-Analysis of the Oncological Safety of Autologous Fat Grafting After Breast Cancer on Basic Science and Clinical Studies. Aesthetic Plast Surg 2023, 47(4), 1245–1257. [Google Scholar] [CrossRef]
- Kuruvilla, A.S.; Yan, Y.; Rathi, S.; Wang, F.; Weichman, K.E.; Ricci, J.A. Oncologic Safety in Autologous Fat Grafting After Breast Conservation Therapy: A Systematic Review and Meta-analysis of the Literature. Ann Plast Surg 2023, 90(1), 106–110. [Google Scholar] [CrossRef]
- Kanchwala, S.K.; Glatt, B.S.; Conant, E.F.; Bucky, L.P. Autologous fat grafting to the reconstructed breast: the management of acquired contour deformities. Plast Reconstr Surg 2009, 124(2), 409–418. [Google Scholar] [CrossRef]
- Chang, C.S.; Lanni, M.A.; Mirzabeigi, M.N.; Bucky, L.P. Large-Volume Fat Grafting: Identifying Risk Factors for Fat Necrosis. Plast Reconstr Surg 2022, 150(5), 941e–949e. [Google Scholar] [CrossRef]
- Manyam, B.V.; Shah, C.; Woody, N.M.; et al. Long-term complications and reconstruction failures in previously radiated breast cancer patients receiving salvage mastectomy with autologous reconstruction or tissue expander/implant-based reconstruction. Breast J 2019, 25(6), 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- Kronowitz, S.J.; Kuerer, H.M. Advances and surgical decision-making for breast reconstruction. Cancer 2006, 107(5), 893–907. [Google Scholar] [CrossRef]
- van Loevezijn, A.A.; Geluk, C.S.; van den Berg, M.J.; et al. Immediate or delayed oncoplastic surgery after breast conserving surgery at the Netherlands Cancer Institute: a cohort study of 251 cases. Breast Cancer Res Treat 2023, 198(2), 295–307. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, H.R.; Losken, A. Modern Approaches to Oncoplastic Surgical Treatment. Clin Plast Surg 2023, 50(2), 211–221. [Google Scholar] [CrossRef]
- Egro, F.M.; Pinell-White, X.; Hart, A.M.; Losken, A. The use of reduction mammaplasty with breast conservation therapy: an analysis of timing and outcomes. Plast Reconstr Surg 2015, 135(6), 963e–971e. [Google Scholar] [CrossRef]
- Yesantharao, P.S.; Shaheen, M.S.; Hui, G.; Gombar, S.; Momeni, A. Oncoplastic Breast Surgery: Optimizing Resection Margins in Addition to Aesthetic Outcomes. In Aesthetic Plast Surg; 19 Nov 2025. [Google Scholar] [CrossRef]
- Wang, D.; Yang, X.; He, J.; et al. Impact of Regional Nodal Irradiation and Hypofractionated Whole-Breast Radiation on Long-Term Breast Retraction and Poor Cosmetic Outcome in Breast Cancer Survivors. Clin Breast Cancer 2020, 20(1), e75–e81. [Google Scholar] [CrossRef] [PubMed]
- de Boniface, J.; Coude Adam, H.; Frisell, A.; etal. Long-term outcomes of implant-based immediate breast reconstruction with and without radiotherapy: a population-based study. Br J Surg 2022, 109(11), 1107–1115. [Google Scholar] [CrossRef]
- Cordeiro, P.G.; Albornoz, C.R.; McCormick, B.; Hu, Q.; Van Zee, K. The impact of postmastectomy radiotherapy on two-stage implant breast reconstruction: an analysis of long-term surgical outcomes, aesthetic results, and satisfaction over 13 years. Plast Reconstr Surg. 2014, 134(4), 588–595. [Google Scholar] [CrossRef]
- Juhl, A.A.; Redsted, S.; Engberg Damsgaard, T. Autologous fat grafting after breast conserving surgery: Breast imaging changes and patient-reported outcome. J Plast Reconstr Aesthet Surg 2018, 71(11), 1570–1576. [Google Scholar] [CrossRef]
- Guest, E.; Paraskeva, N.; Griffiths, C.; et al. The nature and importance of women’s goals for immediate and delayed breast reconstruction. J Plast Reconstr Aesthet Surg 2021, 74(9), 2169–2175. [Google Scholar] [CrossRef]
- Politi, M.C.; Myckatyn, T.M.; Cooksey, K.; et al. A Randomized Controlled Trial of the Implementation of BREASTChoice, a Multilevel Breast Reconstruction Decision Support Tool With Personalized Risk Prediction. Ann Surg 2024. [Google Scholar] [CrossRef]
- Aristokleous, I.; Oberg, J.; Pantiora, E.; et al. Effect of standardised surgical assessment and shared decision-making on morbidity and patient satisfaction after breast conserving therapy: A cross-sectional study. Eur J Surg Oncol 2023, 49(1), 60–67. [Google Scholar] [CrossRef]
- Khavanin, N.; Kim, J.Y.S.; Davila, A.A.; et al. Abstract 46: The BRA Score: Creating a General Risk Calculator for Breast Reconstruction Outcomes. Plast Reconstr Surg 2014, 133((3) Suppl, 56–57. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.P.; Wes, A.M.; Tuggle, C.T.; Serletti, J.M.; Wu, L.C. Risk analysis and stratification of surgical morbidity after immediate breast reconstruction. J Am Coll Surg 2013, 217(5), 780–7. [Google Scholar] [CrossRef] [PubMed]
- Deek, R.P.; Lee, I.O.K.; van Essen, P.; Crittenden, T.; Dean, N.R. Predicted versus actual complications in Australian women undergoing post-mastectomy breast reconstruction: a retrospective cohort study using the BRA Score tool. J Plast Reconstr Aesthet Surg 2021, 74(12), 3324–3334. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Mlodinow, A.S.; Khavanin, N.; et al. Individualized Risk of Surgical Complications: An Application of the Breast Reconstruction Risk Assessment Score. Plast Reconstr Surg Glob Open 2015, 3(5), e405. [Google Scholar] [CrossRef]
- Jimenez, R.B.; Packowski, K.; Horick, N.; et al. The Timing of Acute and Late Complications Following Mastectomy and Implant-based Reconstruction. Ann Surg 2023, 278(1), e203–e208. [Google Scholar] [CrossRef]
- Bennett, K.G.; Qi, J.; Kim, H.M.; Hamill, J.B.; Pusic, A.L.; Wilkins, E.G. Comparison of 2-Year Complication Rates Among Common Techniques for Postmastectomy Breast Reconstruction. JAMA Surg 2018, 153(10), 901–908. [Google Scholar] [CrossRef]
- Ho, A.L.; Klassen, A.F.; Cano, S.; Scott, A.M.; Pusic, A.L. Optimizing patient-centered care in breast reconstruction: the importance of preoperative information and patient-physician communication. Plast Reconstr Surg 2013, 132(2), 212e–220e. [Google Scholar] [CrossRef]
- Shammas, R.L.; Hung, A.; Mullikin, A.; et al. Patient Preferences for Postmastectomy Breast Reconstruction. JAMA Surg 2023, 158(12), 1285–1292. [Google Scholar] [CrossRef]
- Berger, Z. Navigating the unknown: shared decision-making in the face of uncertainty. J Gen Intern Med 2015, 30(5), 675–8. [Google Scholar] [CrossRef] [PubMed]
- Raphael, D.B.; Russell, N.S.; Immink, J.M.; et al. Risk communication in a patient decision aid for radiotherapy in breast cancer: How to deal with uncertainty? Breast 2020, 51, 105–113. [Google Scholar] [CrossRef]
- Yu, L.; Gong, J.; Sun, X.; Zang, M.; Liu, L.; Yu, S. Assessing the Content and Effect of Web-Based Decision Aids for Postmastectomy Breast Reconstruction: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Med Internet Res 2024, 26, e53872. [Google Scholar] [CrossRef] [PubMed]
- Yen, R.W.; Durand, M.A.; Harris, C.; et al. Text-only and picture conversation aids both supported shared decision making for breast cancer surgery: Analysis from a cluster randomized trial. Patient Educ Couns. 2020, 103(11), 2235–2243. [Google Scholar] [CrossRef]
- Xu, C.; Pfob, A.; Mehrara, B.J.; et al. Enhanced Surgical Decision-Making Tools in Breast Cancer: Predicting 2-Year Postoperative Physical, Sexual, and Psychosocial Well-Being following Mastectomy and Breast Reconstruction (INSPiRED 004). Ann Surg Oncol. 2023, 30(12), 7046–7059. [Google Scholar] [CrossRef]
- Naoum, G.E.; Ho, A.Y.; Shui, A.; et al. Risk of Developing Breast Reconstruction Complications: A Machine-Learning Nomogram for Individualized Risk Estimation with and without Postmastectomy Radiation Therapy. Plast Reconstr Surg 2022, 149(1), 1e–12e. [Google Scholar] [CrossRef]
- Chen, J.; Gabay, A.; Boe, L.A.; et al. Machine Learning Accurately Predicts Patient-Reported Outcomes 1 Year After Breast Reconstruction. Ann Surg 2025. [Google Scholar] [CrossRef]
- Hassan, A.M.; Biaggi-Ondina, A.; Asaad, M.; et al. Artificial Intelligence Modeling to Predict Periprosthetic Infection and Explantation following Implant-Based Reconstruction. Plast Reconstr Surg 2023, 152(5), 929–938. [Google Scholar] [CrossRef]
- Pfob, A.; Mehrara, B.J.; Nelson, J.A.; Wilkins, E.G.; Pusic, A.L.; Sidey-Gibbons, C. Towards Patient-centered Decision-making in Breast Cancer Surgery: Machine Learning to Predict Individual Patient-reported Outcomes at 1-year Follow-up. Ann Surg 2023, 277(1), e144–e152. [Google Scholar] [CrossRef]
- Nguyen, C.L.; Zhou, M.; Easwaralingam, N.; et al. Mastectomy Skin Flap Necrosis after Implant-Based Breast Reconstruction: Intraoperative Predictors and Indocyanine Green Angiography. Plast Reconstr Surg 2026, 157(1), 19–28. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Vascular, I.; Singh, N.; Aghayev, A.; et al. ACR Appropriateness Criteria(R) Imaging of Deep Inferior Epigastric Arteries for Surgical Planning (Breast Reconstruction Surgery): 2022 Update. J Am Coll Radiol 2022, 19(11S), S357–S363. [Google Scholar] [CrossRef]
- Pruimboom, T.; Schols, R.M.; Van Kuijk, S.M.; Van der Hulst, R.R.; Qiu, S.S. Indocyanine green angiography for preventing postoperative mastectomy skin flap necrosis in immediate breast reconstruction. Cochrane Database Syst Rev 2020, 4(4), CD013280. [Google Scholar] [CrossRef] [PubMed]
- Pagliara, D.; Schiavone, L.; Garganese, G.; et al. Predicting Mastectomy Skin Flap Necrosis: A Systematic Review of Preoperative and Intraoperative Assessment Techniques. Clin Breast Cancer 2023, 23(3), 249–254. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.A.; Allen, R.J.; Jr Polanco, T.; et al. Long-term Patient-reported Outcomes Following Postmastectomy Breast Reconstruction: An 8-year Examination of 3268 Patients. Ann Surg 2019, 270(3), 473–483. [Google Scholar] [CrossRef]
- Santosa, K.B.; Qi, J.; Kim, H.M.; Hamill, J.B.; Wilkins, E.G.; Pusic, A.L. Long-term Patient-Reported Outcomes in Postmastectomy Breast Reconstruction. JAMA Surg 2018, 153(10), 891–899. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Framework for guiding personalized breast reconstruction after breast-conserving therapy.
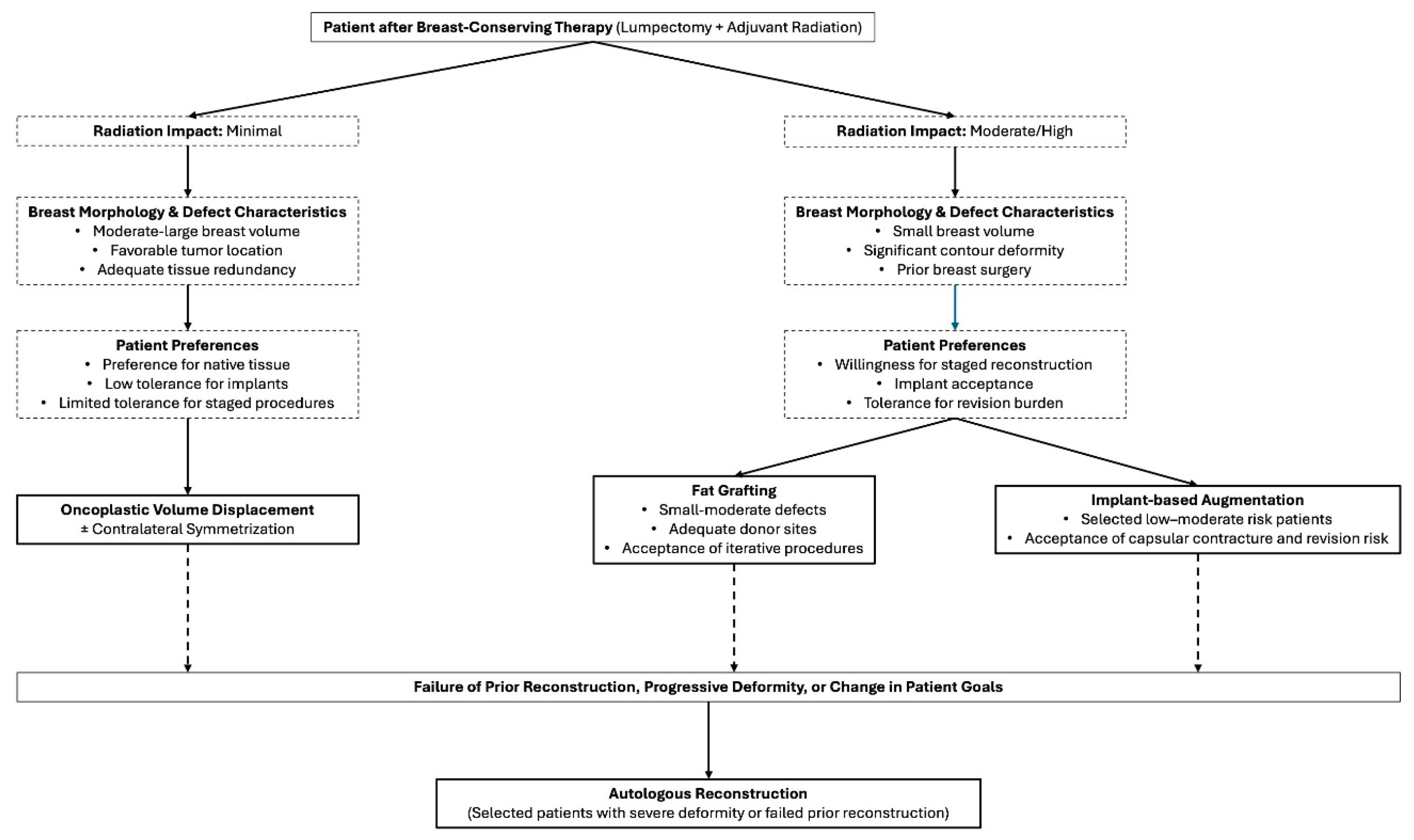

Table 1.
Patient-level variables that influence reconstructive strategy, timing, and anticipated revision burden following breast-conserving therapy.
Table 1.
Patient-level variables that influence reconstructive strategy, timing, and anticipated revision burden following breast-conserving therapy.
| Risk Factor Category | Specific Factors | Reconstructive Implications |
|---|---|---|
| Demographic | Age, BMI, smoking status | Influences wound healing, tolerance for staged reconstruction, revision risk |
| Medical comorbidities | Diabetes, connective tissue disease | Increased complication risk in irradiated tissue |
| Treatment-related | Radiation dose/field, chemotherapy | Drives fibrosis, volume loss, capsular contracture risk |
| Breast morphology | Breast size, ptosis, baseline asymmetry | Determines feasibility of volume displacement vs replacement |
| Tumor characteristics | Location, size, margin status | Affects defect visibility and reconstructive options |
| Prior breast surgery | Augmentation, reduction, mastopexy | Alters tissue planes and implant-related risk |
| Psychosocial factors | Aesthetic priorities, revision tolerance | Critical determinant of satisfaction |
Table 2.
Personalized timing strategies for reconstruction after breast-conserving therapy.
| Reconstruction Timing | Advantages | Limitations | Best Candidates |
|---|---|---|---|
| Immediate | Early contour restoration | Radiation effects may evolve | Low-risk, favorable anatomy |
| Delayed | Stable tissue assessment | Fibrosis, staged care | Higher-risk, irradiated tissue |
| Staged | Adaptable, incremental | Multiple procedures | Patients tolerant of revisions |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



