
Submitted:
02 February 2026
Posted:
03 February 2026
You are already at the latest version
Abstract
Atrial fibrillation frequently coexists with chronic coronary syndrome, sharing common cardiovascular risk factors and pathophysiological mechanisms. Identifying patients with chronic coronary syndrome at increased likelihood of atrial fibrillation remains clinically relevant, particularly in the absence of overt arrhythmia. Clinical and angiographic risk scores routinely used in coronary artery disease may capture cumulative cardiovascular and structural burden and could therefore assist in atrial fibrillation risk stratification. The ABC score provides a more accurate and individualized assessment of risk than traditional clinical scores in patients with AF. Materials and Methods: This prospective, single-center, proof-of-concept study included 131 consecutive patients undergoing invasive coronary angiography for suspected coronary ischemia were enrolled. Patients with and without atrial fibrillation were included, irrespective of arrhythmia subtype. Coronary artery disease severity was assessed using the Gensini and SYNTAX (PCI and CABG) scores. Global cardiovascular risk was evaluated using established clinical scores, including Framingham, ASCVD, SCORE2, and SCORE2-OP. Comparisons were performed between patients in sinus rhythm and those with different atrial fibrillation phenotypes. Correlation analyses, receiver operating characteristic curves, and multivariate logistic regression were applied to evaluate the association between risk scores, coronary disease severity, and atrial fibrillation. Results: Clinical and angiographic risk scores differed significantly according to rhythm status and atrial fibrillation subtype. Patients with atrial fibrillation exhibited higher values of global cardiovascular risk scores and greater coronary anatomical complexity compared with patients in sinus rhythm. The ABC score demonstrated the strongest discriminative performance for atrial fibrillation detection (AUC 0.908), followed by SYNTAX PCI and SYNTAX CABG. In multivariate analysis, the ABC score and SYNTAX CABG emerged as independent predictors of atrial fibrillation. Significant correlations were observed between traditional cardiovascular risk scores and SYNTAX-derived measures of coronary complexity, whereas correlations with the Gensini score were weaker. Established clinical and angiographic risk scores used in chronic coronary syndrome are associated with the presence and phenotype of atrial fibrillation. These findings support the potential role of routinely available risk scores as practical tools for identifying chronic coronary syndrome patients at increased likelihood of atrial fibrillation, facilitating targeted rhythm screening and early risk stratification.
Keywords:
atrial fibrillation
; chronic coronary syndrome
; clinical risk scores
; SYNTAX score
; Gensini score
; cardiovascular risk stratification
; coronary artery disease
1. Introduction
Given the clinical and prognostic heterogeneity of patients with chronic coronary syndrome (CCS), risk stratification plays a central role in guiding diagnostic strategies, therapeutic decisions, and long-term follow-up. In this context, numerous risk scores have been developed and can be broadly classified into anatomical scores, based on coronary angiographic assessment, and clinical scores, designed to estimate global cardiovascular risk. Beyond their established role in coronary disease evaluation, these scores reflect cumulative exposure to cardiovascular risk factors and structural disease burden—mechanisms that are also closely linked to the development of atrial fibrillation (AF). In addition, the ABC score provides a more accurate and individualized assessment of risk than traditional clinical scores in patients with AF. Compared with traditional clinical scores, the ABC score offers more individualized risk assessment by reflecting underlying cardiac stress and injury; both of which are common in CCS due to ongoing ischemia and atherosclerotic burden. As a result, AF patients with coexisting CCS often have higher ABC scores, indicating increased risks of stroke, bleeding, and mortality [1,2].
1.1. Anatomical Scores for the Assessment of Coronary Artery Disease Severity
The Gensini score is one of the most widely used tools for quantifying the severity of coronary artery disease based on coronary angiography. It assigns a score to each lesion according to the degree of stenosis (ranging from 25% to total occlusion), which is subsequently weighted according to the functional importance of the affected coronary segment. Lesions involving the left main coronary artery or proximal segments receive higher weighting coefficients, reflecting their major hemodynamic impact. By integrating lesion extent and location, the Gensini score provides a global estimate of coronary atherosclerotic burden and is frequently used in studies exploring the relationship between anatomical disease severity, inflammatory markers, and cardiovascular prognosis. In the context of CCS, such anatomical burden may also contribute to atrial structural remodeling, creating a substrate permissive for AF [3,4].
The SYNTAX score was developed to characterize the anatomical complexity of coronary lesions rather than stenosis severity alone. It incorporates multiple lesion-related variables, including lesion location, bifurcations or trifurcations, chronic total occlusions, severe calcification, vessel tortuosity, thrombus presence, and diffuse disease extension. SYNTAX plays a pivotal role in guiding revascularization strategy, particularly in decisions between percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) in patients with multivessel disease or left main involvement. In CCS, higher SYNTAX scores are associated with increased procedural complexity, a higher risk of adverse cardiovascular events, and less favorable long-term outcomes. Importantly, diffuse and complex coronary disease quantified by SYNTAX may coexist with atrial remodeling and contribute to AF development [5].
1.2. Clinical Scores for Global Cardiovascular Risk Estimation
In addition to anatomical assessment, evaluation of global cardiovascular risk is essential in CCS, particularly for guiding secondary prevention strategies. The Framingham risk score is one of the oldest and most extensively validated models for coronary risk prediction, derived from the Framingham Heart Study cohort. It estimates 10-year coronary event risk using variables such as age, sex, total and HDL cholesterol, systolic blood pressure, antihypertensive treatment, smoking status, and diabetes mellitus. Although initially designed for primary prevention, the Framingham score has frequently been applied in CCS populations to highlight the contribution of traditional risk factors to atherosclerotic disease progression and adverse outcomes. These same risk factors may also recognized contributors to AF occurrence and persistence [6].
The ASCVD (Atherosclerotic Cardiovascular Disease) score was developed to estimate the risk of major atherosclerotic cardiovascular events, including myocardial infarction and stroke. It integrates age, sex, race, total and HDL cholesterol, systolic blood pressure, antihypertensive treatment, diabetes, and smoking status. Compared with earlier models, ASCVD focuses on clinically impactful events and is widely used to guide lipid-lowering therapy and secondary prevention strategies. In patients with CCS, ASCVD scoring may help identify residual cardiovascular risk and support intensified preventive interventions but given the shared risk factor profile, ASCVD may also reflect vulnerability to AF [7,8].
In Europe, cardiovascular risk assessment models have been updated with the introduction of SCORE2 and SCORE2-OP, which estimate the 10-year risk of fatal and non-fatal cardiovascular events. SCORE2 applies to individuals aged 40–69 years, whereas SCORE2-OP is tailored for patients aged ≥70 years. These models incorporate age, sex, smoking status, systolic blood pressure, and non-HDL cholesterol, and are calibrated according to regional cardiovascular risk levels across Europe. Although primarily intended for primary prevention, SCORE2 and SCORE2-OP are also relevant in CCS, particularly in patients with early-stage coronary disease or multiple cardiovascular risk factors, providing a standardized estimate of global atherosclerotic risk [9].
Overall, the scores applied in CCS reflect two interrelated perspectives: anatomical evaluation of coronary disease severity and complexity, and estimation of systemic cardiovascular risk. While anatomical scores such as Gensini and SYNTAX provide detailed information on the extent and morphology of coronary lesions, clinical scores such as Framingham, ASCVD, and SCORE2/SCORE2-OP capture the cumulative impact of traditional cardiovascular risk factors. Integrating these tools enables a more comprehensive and personalized approach to CCS and creates the rationale for exploring their association with other frequently coexisting cardiovascular conditions, particularly AF—one of the key focuses of the present study.
2. Materials and Methods
2.1. Study Design and Patient Population
This prospective, observational, single-center proof-of-concept study was conducted at the Emergency Clinical Hospital Saint Spiridon from Iași, Romania. Consecutive patients admitted with an indication for invasive coronary angiography for suspected CCS were enrolled between January and July 2024.
The study population consisted of 131 consecutive patients aged ≥18 years, with or without a diagnosis of AF, regardless of AF subtype (paroxysmal, persistent, or permanent). All patients were evaluated for suspected stable coronary artery disease based on clinical presentation and/or non-invasive testing. Eligible patients met one or more of the following inclusion criteria:
- Presence of major cardiovascular risk factors, including arterial hypertension, dyslipidemia, diabetes mellitus, obesity, active smoking, or a strong family history of coronary artery disease.
- Typical angina symptoms.
- Positive non-invasive ischemia testing (exercise stress test, stress echocardiography, or myocardial perfusion scintigraphy).
- Evidence of coronary artery stenosis on coronary computed tomography angiography (CCTA) with an indication for invasive confirmation.
All participants were required to have the capacity to understand the study protocol and to provide written informed consent prior to enrollment.
Although the same patient cohort has been previously used in published analyses evaluating inflammatory biomarkers [10] and cardiovascular risk scores [1] in the context of CCS, the present study addresses a distinct research objective. Specifically, the current analysis focuses on the association between clinical risk scores used in CCS and the presence of AF. No biomarker-based analyses are included in the present study.
2.2. Exclusion Criteria
Patients were excluded if they met any of the following criteria:
- Acute coronary syndrome, including ST-segment elevation myocardial infarction (STEMI), non–ST-segment elevation myocardial infarction (NSTEMI), or unstable angina.
- Advanced heart failure (NYHA functional class IV).
- Cardiomyopathies of any etiology (dilated, hypertrophic, restrictive, or arrhythmogenic).
- Hemodynamically significant valvular heart disease (greater than moderate severity).
- Presence of a permanent cardiac pacing device.
- Advanced renal or hepatic disease.
- Active infection, systemic inflammatory disease, or malignancy.
- Uncontrolled thyroid disorders or psychiatric conditions affecting compliance or biological status.
- Inability to provide informed consent (e.g., unconscious or intubated patients).
- Explicit refusal to participate in the study.
2.3. Clinical and Paraclinical Data Collection
After verification of eligibility criteria, a prospective database was created for all included patients. Data collection was performed in a standardized manner at the time of inclusion, integrating information obtained from medical history, physical examination, laboratory investigations, imaging studies, and the hospital electronic medical record system. Collected demographic and clinical variables included age, sex, smoking status, and cardiovascular comorbidities such as arterial hypertension, diabetes mellitus, heart failure, chronic kidney disease (moderate impairment), chronic obstructive pulmonary disease, dyslipidemia, peripheral arterial disease, transient ischemic attack, stroke, and documented AF. Baseline chronic medications were also recorded, including statins, beta-blockers, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, oral anticoagulants, antiplatelet agents, and proton pump inhibitors.
2.4. Coronary Angiography and Anatomical Scoring
Invasive coronary angiography was performed using a Philips Azurion 7 system. Coronary lesion severity was primarily assessed by visual estimation by experienced interventional cardiologists. Fractional flow reserve (FFR) or instantaneous wave-free ratio (iFR) measurements were selectively employed for angiographically borderline lesions, at the operator’s discretion.
The main risk scores used in CCS, together with their typology and calculation principles, are summarized in Table 1, highlighting the complementary nature of coronary anatomical assessment and global cardiovascular risk estimation.
The anatomical severity and complexity of coronary artery disease were quantified using validated angiographic scoring systems, in accordance with the study analysis plan:
- The Gensini score was used to estimate global coronary atherosclerotic burden.
- The SYNTAX score (PCI and CABG variants) was applied to assess coronary anatomical complexity.
In addition to anatomical scoring, global cardiovascular risk was assessed using established clinical risk scores, including Framingham, ASCVD, SCORE2, and SCORE2-OP and ABC score, in accordance with their original definitions and calculation algorithms (Table 1). All clinical risk scores were calculated independently by two trained investigators, blinded to angiographic results and rhythm status. In cases of discrepancy, scores were re-evaluated jointly and resolved by consensus, in order to minimize interobserver variability and ensure data consistency.
The ABC score in AF is a biomarker-based risk stratification tool used to improve clinical decision-making. It integrates age, biomarkers (such as high-sensitivity troponin and NT-proBNP), and clinical history to estimate key risks in AF patients, including stroke (ABC-stroke score), bleeding (ABC-bleeding score) and death (ABC-death score). There are different ABC models (ABC-stroke, ABC-bleeding, ABC-death), but they are assessed using the same core principles. In practice, the ABC score helps clinicians better identify high- and low-risk AF patients, supports personalized anticoagulation decisions, and complements established scores like CHA₂DS₂-VA by adding prognostic information beyond traditional risk factors [11].
These scores were subsequently analyzed in relation to rhythm status and AF subtype, as well as in multivariate and ROC analyses, to evaluate their potential role as predictors of AF in patients with CCS.
2.5. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics, version 29.0 (IBM Corp., Armonk, NY, USA). Continuous variables were summarized using descriptive statistics, including mean ± standard deviation, median, and minimum–maximum values.
Normality of data distribution was assessed using the Kolmogorov–Smirnov test. Depending on data distribution, comparisons between two groups were performed using the Student’s t-test or the Mann–Whitney U test, while comparisons across multiple groups were conducted using one-way ANOVA or the Kruskal–Wallis test, as appropriate. Post-hoc analyses were applied when global tests reached statistical significance. Associations between continuous variables were evaluated using Spearman’s rank correlation coefficient (rho), with corresponding p-values and 95% confidence intervals, to assess the strength and direction of correlations.
A two-sided p-value < 0.05 was considered statistically significant, while values < 0.01 were considered highly statistically significant. To evaluate the discriminative ability of clinical and angiographic scores for identifying AF, receiver operating characteristic (ROC) curve analysis was performed. The area under the curve (AUC), 95% confidence intervals, optimal cut-off values, sensitivity, and specificity were calculated for each parameter.
For multivariate analysis, binary logistic regression was conducted using the Forward likelihood ratio (LR) method. Variables included in the initial model were those that demonstrated statistically significant differences between patients with and without AF in univariate analyses. Model calibration and performance were assessed using the Hosmer–Lemeshow goodness-of-fit test, Nagelkerke’s R², overall classification accuracy, sensitivity, and specificity.
Potential multicollinearity among predictors was evaluated using variance inflation factors (VIFs), with all values <2.5, indicating the absence of significant collinearity.
2.6. Ethics
This proof-of-concept study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki, as revised in 2013. Upon admission, all participants provided written informed consent after receiving detailed explanations regarding the study objectives, procedures, and their rights as participants. The study protocol was reviewed and approved by the Ethics Committee of the University of Medicine and Pharmacy “Gr. T. Popa” Iași (Approval No. 352/9 October 2023) and the Ethics Committee of St. Spiridon Emergency Clinical Hospital, Iași (Approval No. 75/11 September 2023).
3. Results
Among the 131 patients included in the study, 65 patients were diagnosed with significant CCS (S-CCS), defined by the presence of ≥70% stenosis in at least one coronary artery with a diameter ≥2 mm or ≥50% stenosis of the left main coronary artery. The remaining 66 patients were classified as non-significant CCS (N-SCC), defined by coronary stenoses below these thresholds. This latter group also included patients with angina with non-obstructive coronary arteries (ANOCA), an entity increasingly recognized in recent literature, characterized by distinct pathophysiological mechanisms and growing clinical relevance.
Regarding cardiac rhythm, 54.2% of the study population had AF. Among these patients, 26.7% had permanent AF, 16.8% had paroxysmal AF, and 10.7% had persistent AF, while the remaining patients were in sinusal rhythm (SR).
Subsequently, based on coronary disease severity and rhythm status, the study population was stratified into four patient groups, as follows (Table 2):
- 25 patients with SR and N-CCS;
- 35 patients with SR and S-CCS;
- 41 patients with AF and N-CCS;
- 30 patients with AF and S-CCS.
It can be observed that the proportion of patients in SR was higher among those with significant CCS (S-SCC) compared with patients with non-significant lesions (53.8% vs. 37.9%). Among patients with permanent AF, a higher proportion was noted in the non-significant CCS (N-SCC) group (36.4% vs. 16.9%). A similar pattern was observed for persistent AF, which occurred at nearly double the frequency in patients with non-significant lesions compared with those with significant CCS (13.6% vs. 7.7%). In contrast, among patients with significant coronary lesions, paroxysmal AF was more prevalent, being observed in 21.5% of cases compared with 12.1% in the non-significant CCS group. These distributions are detailed in Table 2.
The results presented in this section focus exclusively on the analysis of clinical and angiographic risk scores in relation to AF in patients with CCS. Other clinical, biological, echocardiographic, and treatment-related characteristics of the study population have been previously reported and discussed in detail in earlier publications derived from the same cohort [1,10]. Therefore, these variables are not reiterated in the present manuscript. The current analysis specifically addresses the primary objective of this study, namely the evaluation of established risk scores used in CCS as potential predictors of AF presence and phenotype.
3.1. Potential Assessment of AF Using CCS-Related Risk Scores
To evaluate the relationship between AF subtype and coronary artery disease severity, several validated clinical risk scores, including cardiovascular risk scores and angiographic indices, were compared between patients in SR and those with different AF phenotypes. The results are summarized in Table 3, which presents the distribution of each parameter across the analyzed groups. Non-parametric tests (Mann–Whitney and Kruskal–Wallis) were applied, or ANOVA when test assumptions were met. The table reports both mean and median values for each subgroup, together with global and post-hoc statistical significance, highlighting relevant differences among AF subtypes.
Analysis of the Gensini score, used to quantify coronary atherosclerotic burden, demonstrated a decreasing trend in mean values from patients in SR toward those with more persistent forms of AF. Patients in SR exhibited the highest mean value (30.24 ± 38.64), followed closely by those with paroxysmal AF (30.86 ± 39.82), while lower values were observed in persistent AF (25.00 ± 32.68), reaching the lowest levels in permanent AF (15.29 ± 22.14). Median values followed the same descending pattern and overall group differences reached statistical significance (p = 0.043), with notable differences between paroxysmal and permanent AF, as well as between SR and permanent AF.
For the ABC score, values increased progressively from SR (0.45 ± 0.31) to paroxysmal AF (0.86 ± 0.53), persistent AF (0.90 ± 0.44), and permanent AF (1.13 ± 0.63). This increase was evident at both median and extreme values, and global differences were highly statistically significant (p < 0.001). Post-hoc analyses confirmed that patients in SR had significantly lower ABC scores compared with all AF subtypes.
Regarding SCORE2-OP, patients with paroxysmal AF exhibited the highest values (27.86 ± 8.88), followed by persistent AF (24.90 ± 14.86) and permanent AF (21.08 ± 10.18), whereas patients in SR had the lowest values (18.89 ± 10.42). Global differences were statistically significant (p = 0.004), with post-hoc analysis highlighting a significant difference between SR and paroxysmal AF.
For the Framingham risk score, mean values followed a similar progressive pattern, with the lowest values observed in SR (11.30 ± 7.60), the highest in paroxysmal AF (18.65 ± 6.99), and intermediate values in persistent AF (14.73 ± 10.34) and permanent AF (13.61 ± 8.62). Global analysis demonstrated statistically significant differences (p = 0.003), and pairwise comparisons confirmed relevant differences between SR and paroxysmal AF.
The ASCVD score showed a comparable distribution pattern. The highest values were recorded in paroxysmal AF (35.55 ± 14.10), followed by persistent AF (21.62 ± 9.77), permanent AF (20.92 ± 12.45), and SR (19.54 ± 13.23). Global differences were highly statistically significant (p < 0.001), with significant contrasts observed between SR and paroxysmal AF, as well as between paroxysmal and permanent AF.
Evaluation of the SYNTAX PCI score, applied to patients with significant coronary artery disease, revealed increasing anatomical complexity from SR (29.50 ± 8.82) to paroxysmal AF (35.90 ± 8.62), persistent AF (43.44 ± 13.28), and permanent AF (38.81 ± 12.97). Global differences were statistically significant (p = 0.007), with marked variations between SR and AF subtypes.
Similarly, SYNTAX CABG values followed the same ascending pattern, with the lowest values observed in patients with SR (26.35 ± 9.04) and the highest values in persistent AF (41.04 ± 11.44) and paroxysmal AF (34.90 ± 9.41). The global test confirmed statistically significant differences (p = 0.001), and post-hoc analyses demonstrated significant differences between SR and paroxysmal AF, as well as between SR and persistent AF.
Overall, all analyzed clinical and angiographic scores exhibited ordered variations across patient groups, with the highest values generally observed in paroxysmal or persistent AF, while patients in SR consistently showed the lowest values. These findings indicate a graded and consistent differentiation among AF subtypes based on clinical and anatomical scoring systems.
3.2. Diagnostic Performance of CCS-Related Risk Scores in AF
Subsequently, the seven parameters that demonstrated statistically significant differences between patients with and without AF were entered into a binary logistic regression model using the Forward LR method. The Hosmer–Lemeshow goodness-of-fit test indicated adequate model performance, as the result was not statistically significant (p = 0.471). The initial predictive accuracy for AF was 53.8%, increasing to 86.2% in the final model, indicating good discriminative ability of the identified predictors. The model explained 50.8% of the variance in AF diagnosis (Nagelkerke R² = 0.508) and demonstrated a sensitivity of 80.0% and a specificity of 91.4%.
Among the seven tested predictors, ABC score and SYNTAX CABG remained statistically significant. A one-unit increase in the ABC score increased the odds of AF by 35.160-fold, while a one-unit increase in SYNTAX CABG increased the odds of AF by 1.080-fold, with all other predictors held constant (Table 4).
The ABC score demonstrated the best performance, with an excellent discriminative ability, reflected by an AUC of 0.908, a sensitivity of 83.1%, and a specificity of 88.3% at a cut-off value of 0.615. Reasonable discriminative performance was also observed for SYNTAX PCI, which showed a moderate AUC of 0.745, with a sensitivity of 83.3% and a specificity of 62.9% at a cut-off value of 28.95, as well as for SYNTAX CABG, which demonstrated a moderate AUC of 0.760, with a sensitivity of 70.0% and a specificity of 74.3% at a cut-off value of 29.95.
To assess the utility of clinical, anatomical, and atherosclerotic burden scores in identifying patients with AF, a ROC analysis was performed for the parameters that showed statistically significant differences in comparisons between patients with and without AF. Table 5 and Figure 1, Figure 2, Figure 3 and Figure 4 present the discriminative performance of each marker, including the AUC values, 95% confidence intervals, optimal cut-off thresholds, and corresponding sensitivity and specificity. These results quantify the ability of scores traditionally used in the coronary setting—such as SYNTAX PCI/CABG and global cardiovascular risk scores—to function as clinical tools for AF prediction, enabling preliminary risk stratification in routine clinical practice.
To explore the internal relationships among the clinical scores, cardiovascular risk scores, and angiographic indicators used in the study, a Spearman correlation analysis was performed. The results are presented in Table 6, which includes the rho correlation coefficients, corresponding p values, and 95% confidence intervals for all evaluated parameter pairs.
Regarding the relationship with the Gensini score, most correlations were weak and not statistically significant. No relevant associations were identified with the ABC score (rho = −0.021, p = 0.810) or SCORE2-OP (rho = 0.104, p = 0.237). However, a weak but statistically significant positive correlation was observed between the Gensini score and both the Framingham score (rho = 0.201, p = 0.021) and the ASCVD score (rho = 0.298, p < 0.001), suggesting partial convergence between global atherosclerotic burden and clinically estimated cardiovascular risk. The correlation with SYNTAX PCI was modest and at the threshold of statistical significance (rho = 0.246, p = 0.049), whereas the association with SYNTAX CABG did not reach statistical significance (rho = 0.225, p = 0.072).
Evaluation of the relationships between the ABC score and other parameters revealed several statistically significant correlations. ABC was moderately associated with SCORE2-OP (rho = 0.260, p = 0.003) and ASCVD (rho = 0.196, p = 0.025), while its association with the Framingham score was marginal (p = 0.083). The strongest correlations were observed between ABC and the SYNTAX scores, with moderate-to-strong correlations for both SYNTAX PCI (rho = 0.559, p < 0.001) and SYNTAX CABG (rho = 0.491, p < 0.001); in all cases, the 95% confidence intervals did not include zero.
Correlations involving SCORE2-OP were consistently statistically significant. Moderate associations were identified with Framingham (rho = 0.344, p < 0.001) and ASCVD (rho = 0.681, p < 0.001), confirming the expected relationship between scores derived from similar cardiovascular risk factors. SCORE2-OP also demonstrated moderate correlations with anatomical parameters, including SYNTAX PCI (rho = 0.593, p < 0.001) and SYNTAX CABG (rho = 0.627, p < 0.001).
Similarly, the Framingham score showed strong correlations with ASCVD (rho = 0.656, p < 0.001) and a significant association with SYNTAX CABG (rho = 0.422, p < 0.001). In contrast, the relationship with SYNTAX PCI was not statistically significant (rho = 0.058, p = 0.648), indicating variable associations between global cardiovascular risk and coronary lesion complexity.
The ASCVD score demonstrated significant correlations with the Gensini score (rho = 0.298, p < 0.001), as well as with SCORE2-OP and Framingham (rho = 0.656, p < 0.001), and also with the SYNTAX scores. The correlation with SYNTAX PCI was moderate (rho = 0.321, p = 0.009), while a stronger association was observed with SYNTAX CABG (rho = 0.572, p < 0.001).
Finally, the correlation between the two SYNTAX scores—PCI and CABG—was the strongest observed in the analysis (rho = 0.663, p < 0.001), with the confidence interval indicating a consistent association (0.495–0.784). This finding was expected, as both scores quantify the same anatomical burden of coronary artery disease, albeit from different therapeutic perspectives.
Overall, the analysis revealed a coherent network of statistically significant correlations between traditional risk factor–based scores (SCORE2-OP, Framingham, ASCVD) and anatomical scores (SYNTAX PCI/CABG). In contrast, the Gensini score exhibited the weakest correlations and the fewest statistically significant associations within this analytical framework.
4. Discussion
An essential objective of the present study was to explore the feasibility of predicting AF in patients with CCS through the validation of established cardiovascular clinical risk scores and angiographic indicators. This section focuses specifically on the potential of repurposing existing clinical and anatomical risk scores—originally developed for cardiovascular risk stratification or therapeutic decision-making—as practical tools for identifying patients with previously undetected AF or those at increased risk of progression toward more sustained AF phenotypes.
This approach is supported by a clear pathophysiological rationale. AF is frequently progressive in nature, initially manifesting as an intermittent arrhythmia with silent periods of abnormal electrical activity that remain undetected in the absence of intensive rhythm monitoring. Large trials such as ASSERT and LOOP have demonstrated that up to 30% of patients at high vascular risk develop silent AF detectable only through continuous monitoring. Consequently, the development of a clinical algorithm based on parameters already collected in routine practice may represent an important strategy for screening and secondary prevention [12,13].
4.1. Atrial Fibrillation as an Expression of Systemic Cardiovascular Disease
The primary observations of the present study reinforce the concept that AF does not represent an isolated electrical disorder, but rather a marker of global cardiovascular vulnerability. Large cohort studies, including the Framingham Heart Study and ARIC, have demonstrated that hypertension, diabetes, dyslipidemia, systemic inflammation, and advancing age increase the risk of both coronary atherosclerosis and AF. Within this framework, AF may be considered the final result of a sequence of pathological processes—namely inflammatory activation, endothelial dysfunction, structural atrial remodeling, and ultimately loss of atrial electrical stability—underscoring the importance of early identification in determining long-term patient outcomes [6,14].
The findings of the present work align with this paradigm, demonstrating a graded progression of both clinical and anatomical scores with the transition from SR to paroxysmal, persistent, and permanent AF. Comparative analysis of risk scores between patients in SR and those with different AF phenotypes revealed a consistent and progressive pattern. Across all metrics, the lowest values were observed in SR, increased in paroxysmal AF, reached a peak in persistent AF, and remained elevated in permanent AF.
This progressive behavior was evident across multiple scores:
- SCORE2-OP, with significant increases from 18.9 in SR to 27.8 in paroxysmal AF (p = 0.004);
- Framingham risk score, where the mean increase from SR to paroxysmal AF exceeded 65% (p = 0.003);
- ASCVD, in which paroxysmal AF nearly doubled estimated risk (35.5 vs. 19.5, p < 0.001);
- ABC score, which, although originally designed for anticoagulation decision-making, demonstrated excellent discrimination between SR and all AF forms (p < 0.001).
These results support the hypothesis that AF does not occur randomly during the course of coronary artery disease but rather represents an evolutionary threshold in patients with a high metabolic, vascular, and inflammatory burden. Moreover, this consistent pattern is concordant with observations from EHRA and ESC registry analyses, which identify AF as a phenotypic marker of structural cardiovascular aging.
An additional finding of particular interest—frequently highlighted in contemporary literature—is that paroxysmal AF appears to concentrate the highest systemic risk, as assessed by scores such as SCORE2/OP, Framingham, and ASCVD. In the present study, patients with paroxysmal AF exhibited the highest clinical risk scores in most analyses, in some cases exceeding those observed in persistent or permanent AF. This phenomenon has been confirmed in post-hoc analyses of major trials such as AFFIRM and ATHENA, both of which reported a continuous increase in inflammatory markers and progressive deterioration of the electrical substrate during early and intermittent AF stages, before the arrhythmia becomes permanent. Paroxysmal AF may therefore represent a critical window during which preventive intervention is most effective, further justifying the use of clinical risk scores as tools for early detection [15,16].
4.2. Clinical Risk Scores—Repurposed Tools with Unexpected Utility
The ABC score and CCS are linked through shared pathophysiological pathways and overlapping risk markers, especially in patients with AF. The ABC score incorporates cardiac biomarkers (notably high-sensitivity troponin and NT-proBNP) that reflect chronic myocardial injury and wall stress. In this context, the ABC score captures the prognostic impact of stable coronary artery disease more effectively than purely clinical scores, as it reflects active myocardial disease rather than just historical risk factors. This makes it particularly useful for risk stratification and tailoring antithrombotic therapy in AF patients with CCS.
The present study confirms that risk scores originally developed for stroke prediction (ABC score) or for guiding revascularization strategies (CABG versus PCI) in patients with multivessel coronary disease (SYNTAX) may have extended utility in anticipating the development of AF. Multivariate analysis identified the ABC score as the strongest independent predictor (OR = 35.16; AUC = 0.908; Sensitivity = 83.1%; Specificity = 88.3%).
This performance is consistent with findings from the literature, supported by studies such as GARFIELD-AF and ENGAGE AF-TIMI, in which the ABC score demonstrated the ability to capture biological frailty and vulnerability to adverse cardiovascular events [17,18].
Similarly, SYNTAX scores, which quantify coronary disease burden, showed a robust association with AF, demonstrating predictive capacity for this arrhythmia (AUC 0.745–0.760; superior performance in persistent/permanent AF; significant odds ratios for SYNTAX CABG in logistic regression analyses).
These observations are supported by published data suggesting that coronary disease burden, as quantified by SYNTAX, is associated with AF development. In a cohort of patients undergoing CABG, SYNTAX score was identified as an independent predictor of postoperative AF, alongside age and chronic obstructive pulmonary disease, emphasizing the role of coronary atherosclerosis severity in shaping the atrial arrhythmogenic substrate [19,20].
Furthermore, a large study published in the Korean Circulation Journal evaluated the relationship between coronary disease severity and AF occurrence following PCI. The authors demonstrated that global atherosclerotic burden, measured by the SYNTAX score, was strongly associated with AF risk, independent of other clinical and demographic factors. Patients with SYNTAX values above recommended thresholds exhibited a significantly higher incidence of AF during follow-up, suggesting that atrial arrhythmogenic substrate may coexist with complex coronary artery disease even in stable ischemic settings. The study also highlighted that additional coronary variables—such as diffuse multivessel involvement and high-risk lesion morphology—may further amplify AF susceptibility when combined with systemic factors such as hypertension or diastolic dysfunction. Consequently, the authors concluded that coronary anatomical assessment using SYNTAX is not only essential for therapeutic decision-making (PCI versus CABG), but also valuable for anticipating arrhythmic complications, positioning the score as a potential early predictor of AF, particularly in patients with extensive or severe coronary disease [20].
In contrast to SYNTAX, the Gensini score did not correlate with AF presence or subtype, suggesting a limited relationship between focal stenotic severity and arrhythmogenic remodeling. This finding reflects conceptual differences between the two tools. Gensini quantifies the percentage severity of isolated coronary stenoses without accounting for disease extent, diffuse involvement, or vascular network complexity. In AF—a condition whose substrate includes systemic inflammation, oxidative stress, endothelial dysfunction, and microvascular disease—severe epicardial lesions represent only one component of the pathogenic process. It is therefore understandable that the Gensini score demonstrated weak correlations with AF (rho < 0.25), as it accurately captures critical focal stenosis but fails to reflect atherosclerotic heterogeneity, arterial stiffness, or ischemia-generating mechanisms that may contribute to atrial remodeling [3].
The present findings confirm this distinction: while Gensini remains valuable for quantifying focal anatomical severity, SYNTAX PCI and CABG scores, which integrate lesion multiplicity, segment length, bifurcations, tortuosity, and overall complexity, appear more sensitive to the pathophysiological context of AF. This is reflected in their orderly increase from SR to paroxysmal, persistent, and permanent AF, as well as in their role as independent AF predictors in multivariate analysis. Thus, the discrepancy between Gensini and SYNTAX does not contradict, but rather supports the contemporary concept that AF is preferentially associated with diffuse and complex coronary artery disease rather than with a single critical stenosis. Consequently, scores that capture global atherosclerotic burden provide substantially more informative insights for AF prediction than those limited to focal severity assessment.
4.3. Correlations Between Scores—Pathophysiological Convergence and Structural Limitations
Spearman correlation analysis performed in the present study provides additional insight into how different clinical, metabolic, and anatomical scores reflect the global cardiovascular disease burden in the context of AF. The results outline a coherent landscape of relationships between risk factors, coronary complexity, and arrhythmia, highlighting both convergence among certain scores and limitations among others.
Robust correlations were observed between global cardiovascular risk scores—SCORE2-OP, ASCVD, and Framingham—all of which are based on cumulative traditional risk factors. Moderate to strong relationships (rho 0.34–0.68, p < 0.001) are unsurprising, given that these tools rely on similar pillars: age, hypertension, diabetes, dyslipidemia, and smoking—key contributors to both coronary atherosclerosis and the electrical substrate predisposing to AF. As emphasized by the 2021 ESC Guidelines on Cardiovascular Prevention, risk factor–based scores essentially quantify “cumulative etiological burden,” reflecting chronic exposure to disease-driving mechanisms [21].
Importantly, these risk factor–based scores also demonstrated significant and consistent correlations with anatomical SYNTAX PCI and CABG scores (rho 0.32–0.63, all p < 0.001). This convergence between clinical risk and morphological expression suggests that patients with AF are not only metabolically or inflammatorily predisposed but also exhibit angiographically detectable structural cardiac changes. The significant correlation with SYNTAX—but not necessarily with Gensini—indicates that AF is associated with diffuse, segmental, and complex coronary disease rather than isolated focal stenosis [21,22].
Overall, Spearman analysis fulfills a key role by confirming that:
- SCORE2-OP, ASCVD, and Framingham capture predisposition,
- SYNTAX PCI/CABG capture disease expression,
- Gensini, limited to focal severity, loses sensitivity in diffuse disease—precisely the scenario typical of AF.
This supports the conceptual validity of the thesis objective: AF is not an isolated phenomenon, but an integrated manifestation of an atherosclerotic and inflammatory continuum that can be anticipated through pathogenetically aligned scoring systems [23].
4.4. Clinical Utility and Practical Implications
The data obtained in the present study suggest that the analyzed scores may be used not only to describe the profile of patients with AF, but also to identify those in whom AF is likely present yet undetected. Clinical and anatomical scores may therefore shift AF management from a reactive diagnostic-therapeutic approach toward a proactive strategy. A major clinical message emerging from this analysis is that as risk scores increase, rhythm monitoring should be intensified, even in the absence of documented AF on standard electrocardiography. This conclusion aligns with evidence from studies such as ASSERT, LOOP, and mHealth-AF, which have demonstrated that the presence of advanced vascular or structural substrate dramatically increases the likelihood that AF is already present in a subclinical form [12,13,24,25].
Thresholds such as:
- ABC ≥ 0.60
- SYNTAX PCI/CABG > 30
- ASCVD or Framingham scores in the upper quartile may therefore indicate the need for more active AF surveillance.
This paradigm shift implies risk-stratified monitoring strategies that may include periodic resting ECGs, 48–72-hour Holter monitoring at 6–12-month intervals, and—in very high-risk patients, particularly those aged ≥75 years with multivessel coronary disease, elevated SYNTAX scores, or persistent clinical suspicion—implantable loop recorders. The clinical consequences of early AF identification are substantial, as prompt detection enables:
- preventive initiation of anticoagulation in eligible patients,
- stroke prevention—given that 20–30% of cryptogenic strokes are attributable to undiagnosed AF,
- optimization of blood pressure control and other risk factors,
These benefits are supported by recent evidence, including the EAST-AFNET 4 trial, which demonstrated that early AF treatment reduces cardiovascular hospitalizations and the risk of heart failure or stroke, underscoring the value of active screening in high-risk populations [27].
4.5. Strengths and Study Limitations
Several limitations of the present study should be acknowledged when interpreting these findings, particularly in relation to cardiovascular risk factor assessment and the repurposing of clinical risk scores.
First, the single-center design may limit the generalizability of the findings. Although patient evaluation, rhythm classification, and angiographic assessment were performed using standardized protocols, the distribution and clustering of cardiovascular risk factors may differ across centers and populations. Variations in age, metabolic profile, hypertension burden, and prevalence of subclinical AF could influence the performance of clinical and anatomical risk scores in predicting AF among patients with CCS.
Second, the relatively modest sample size (n = 131), while appropriate for an exploratory analysis, limits statistical power, particularly after stratification by rhythm status and AF subtype. Subgroup analyses involving paroxysmal, persistent, and permanent AF inevitably reduced the number of observations per category, potentially limiting the detection of weaker but clinically relevant associations between cumulative cardiovascular risk burden and AF phenotypes. Larger cohorts would allow more robust multivariable modeling and more precise adjustment for confounding risk factors.
Third, the cross-sectional design precludes assessment of temporal relationships between risk factor accumulation and AF development. Although the analyzed scores reflect long-term exposure to cardiovascular risk factors, the study cannot determine whether elevated scores preceded the onset of AF or represent a consequence of shared disease progression. Consequently, causal inference regarding AF prediction or progression cannot be established.
Fourth, the clinical risk scores evaluated in this study were not originally designed to predict AF in patients with CCS. Instead, they were developed to estimate global cardiovascular risk, thromboembolic risk, or to guide therapeutic decision-making. Their application in AF prediction should therefore be considered exploratory. While the observed associations support their potential utility as screening or stratification tools, their predictive accuracy is inherently constrained by their original conceptual framework.
Finally, the absence of longitudinal follow-up represents a key limitation. The study did not evaluate incident AF, AF progression, or major cardiovascular outcomes over time. As a result, the prognostic implications of elevated clinical or anatomical risk scores for future AF occurrence or adverse cardiovascular events cannot be determined.
In summary, the findings of this study should be interpreted as hypothesis-generating. While they support the concept that established clinical and anatomical risk scores may help identify patients with CCS at increased likelihood of AF, further validation in larger, multicenter, and longitudinal studies is required before routine clinical implementation.
5. Conclusions
In conclusion, the present proof-of-concept study provides coherent evidence that clinical risk scores traditionally used to estimate global cardiovascular risk, as well as those designed to quantify and guide therapeutic management of coronary lesions, can be effectively repurposed for AF screening in patients with CCS. The high performance of the ABC score and the consistent correlations between cardiovascular risk scores and coronary anatomical complexity support a transition toward a predictive medicine model, in which AF is identified before clinical presentation. Moreover, integrating these scores into a stratification algorithm enables targeted selection of patients for intensive ECG monitoring and opens avenues for future research, including the combination of clinical scores with inflammatory biomarkers, structural imaging parameters, and continuous digital monitoring.
Author Contributions
Conceptualization, A.-F.O. and M.F.; methodology, M.L., P.C.M., and M.G.; software, A.J., I.-L.M., and R.S.M.; validation, A.R., P.S. and D.I.; formal analysis, D.-E.F., R.M. and A.V.; investigation, C.D., E.C. and I.-I.C.-E.; resources, M.L., P.C.M., and M.G.; data curation, A.J., I.-L.M., and R.S.M..; writing—original draft preparation, A.-F.O.; writing—review and editing, A.-F.O. and M.F.; visualization, A.R., P.S. and D.I.; supervision, D.-E.F., R.M. and A.V.; project administration, A.-F.O. and M.F.; funding acquisition, C.D., E.C. and I.-I.C.-E. All authors have read and agreed to the published version of the manuscript.
Funding
This research is a study from a PhD thesis of Alexandru-Florinel Oancea, and it received research funding from the University of Medicine and Pharmacy “Gr. T. Popa” (no. 352/9 October 2023).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Medicine and Pharmacy “Gr. T. Popa” (no. 352/9 October 2023) and of the St. Spiridon Emergency Clinical Hospital (no. 75/11 September 2023).
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
All data presented in this study are available within the article. The first author has all the data used in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Oancea, A.-F.; Morariu, P.C.; Godun, M.; Dobreanu, S.D.; Mihnea, M.; Iosep, D.G.; Buburuz, A.M.; Mitu, O.; Burlacu, A.; Floria, D.-E.; et al. Atrial Fibrillation Risk Scores as Potential Predictors of Significant Coronary Artery Disease in Chronic Coronary Syndrome: A Novel Diagnostic Approach. Life 2025, 15, 1134. [Google Scholar] [CrossRef] [PubMed]
- Floria, M.; Oancea, A.F.; Morariu, P.C.; Burlacu, A.; Iov, D.E.; Chiriac, C.P.; Baroi, G.L.; Stafie, C.S.; Cuciureanu, M.; Scripcariu, V.; et al. An Overview of the Pharmacokinetics and Pharmacodynamics of Landiolol (an Ultra-Short Acting Β1 Selective Antagonist) in Atrial Fibrillation. Pharmaceutics 2024, 16, 517. [Google Scholar] [CrossRef]
- Rampidis, G.P.; Benetos, G.; Benz, D.C.; Giannopoulos, A.A.; Buechel, R.R. A Guide for Gensini Score Calculation. Atherosclerosis 2019, 287, 181–183. [Google Scholar] [CrossRef]
- Oancea, A.F.; Jigoranu, R.A.; Morariu, P.C.; Miftode, R.-S.; Trandabat, B.A.; Iov, D.E.; Cojocaru, E.; Costache, I.I.; Baroi, L.G.; Timofte, D.V.; et al. Atrial Fibrillation and Chronic Coronary Ischemia: A Challenging Vicious Circle. Life 2023, 13, 1370. [Google Scholar] [CrossRef]
- Kundu, A.; Sardar, P.; O’Day, K.; Chatterjee, S.; Owan, T.; Dawn Abbott, J. SYNTAX Score and Outcomes of Coronary Revascularization in Diabetic Patients. Curr Cardiol Rep 2018, 20, 28. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, S.S.; Levy, D.; Vasan, R.S.; Wang, T.J. The Framingham Heart Study and the Epidemiology of Cardiovascular Disease: A Historical Perspective. Lancet 2014, 383, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Wong, N.D.; Budoff, M.J.; Ferdinand, K.; Graham, I.M.; Michos, E.D.; Reddy, T.; Shapiro, M.D.; Toth, P.P. Atherosclerotic Cardiovascular Disease Risk Assessment: An American Society for Preventive Cardiology Clinical Practice Statement. American Journal of Preventive Cardiology 2022, 10, 100335. [Google Scholar] [CrossRef]
- Jigoranu, R.-A.; Roca, M.; Costache, A.-D.; Mitu, O.; Oancea, A.-F.; Miftode, R.-S.; Haba, M. Ștefan C.; Botnariu, E.G.; Maștaleru, A.; Gavril, R.-S.; et al. Novel Biomarkers for Atherosclerotic Disease: Advances in Cardiovascular Risk Assessment. Life 2023, 13, 1639. [Google Scholar] [CrossRef]
- Van Trier, T.J.; Snaterse, M.; Boekholdt, S.M.; Scholte Op Reimer, W.J.M.; Hageman, S.H.J.; Visseren, F.L.J.; Dorresteijn, J.A.N.; Peters, R.J.G.; Jørstad, H.T. Validation of Systematic Coronary Risk Evaluation 2 (SCORE2) and SCORE2-Older Persons in the EPIC-Norfolk Prospective Population Cohort. European Journal of Preventive Cardiology 2024, 31, 182–189. [Google Scholar] [CrossRef]
- Oancea, A.-F.; Morariu, P.C.; Godun, M.; Dobreanu, S.D.; Jigoranu, A.; Mihnea, M.; Iosep, D.; Buburuz, A.M.; Miftode, R.S.; Floria, D.-E.; et al. Galectin-3 and Pentraxin-3 as Potential Biomarkers in Chronic Coronary Syndrome and Atrial Fibrillation: Insights from a 131-Patient Cohort. IJMS 2025, 26, 4909. [Google Scholar] [CrossRef]
- Wang, Y.-F.; Jiang, C.; He, L.; Du, X.; Guo, X.-Y.; Tang, R.-B.; Sang, C.-H.; Long, D.-Y.; Dong, J.-Z.; Lip, G.Y.H.; et al. The ABC-Death Score for Mortality Prediction in Patients With Atrial Fibrillation Undergoing Catheter Ablation. JACC Asia 2023, 3, 790–801. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, J.H.; Diederichsen, S.Z.; Højberg, S.; Krieger, D.W.; Graff, C.; Kronborg, C.; Olesen, M.S.; Nielsen, J.B.; Holst, A.G.; Brandes, A.; et al. Implantable Loop Recorder Detection of Atrial Fibrillation to Prevent Stroke (The LOOP Study): A Randomised Controlled Trial. The Lancet 2021, 398, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Rola, P.; Doroszko, A.; Trocha, M.; Gajecki, D.; Gawryś, J.; Matys, T.; Giniewicz, K.; Kujawa, K.; Skarupski, M.; Adamik, B.; et al. The Usefulness of the C2HEST Risk Score in Predicting Clinical Outcomes among Hospitalized Subjects with COVID-19 and Coronary Artery Disease. Viruses 2022, 14, 1771. [Google Scholar] [CrossRef]
- Wright, J.D.; Folsom, A.R.; Coresh, J.; Sharrett, A.R.; Couper, D.; Wagenknecht, L.E.; Mosley, T.H.; Ballantyne, C.M.; Boerwinkle, E.A.; Rosamond, W.D.; et al. The ARIC (Atherosclerosis Risk In Communities) Study. Journal of the American College of Cardiology 2021, 77, 2939–2959. [Google Scholar] [CrossRef] [PubMed]
- Wyse, D.G. The AFFIRM Trial: Main Trial and Substudies—What Can We Expect? J Interv Card Electrophysiol 2000, 4, 171–176. [Google Scholar] [CrossRef]
- Hohnloser, S.H.; Crijns, H.J.G.M.; Van Eickels, M.; Gaudin, C.; Page, R.L.; Torp-Pedersen, C.; Connolly, S.J. Effect of Dronedarone on Cardiovascular Events in Atrial Fibrillation. N Engl J Med 2009, 360, 668–678. [Google Scholar] [CrossRef]
- Kato, E.T.; Giugliano, R.P.; Ruff, C.T.; Koretsune, Y.; Yamashita, T.; Kiss, R.G.; Nordio, F.; Murphy, S.A.; Kimura, T.; Jin, J.; et al. Efficacy and Safety of Edoxaban in Elderly Patients With Atrial Fibrillation in the ENGAGE AF–TIMI 48 Trial. JAHA 2016, 5, e003432. [Google Scholar] [CrossRef]
- Kakkar, A.K.; Mueller, I.; Bassand, J.-P.; Fitzmaurice, D.A.; Goldhaber, S.Z.; Goto, S.; Haas, S.; Hacke, W.; Lip, G.Y.H.; Mantovani, L.G.; et al. International Longitudinal Registry of Patients with Atrial Fibrillation at Risk of Stroke: Global Anticoagulant Registry in the FIELD (GARFIELD). American Heart Journal 2012, 163, 13–19.e1. [Google Scholar] [CrossRef]
- Gecmen, C.; Babur Guler, G.; Erdogan, E.; Hatipoglu, S.; Guler, E.; Yilmaz, F.; Unkun, T.; Cap, M.; Bakal, R.B.; Bayram, T.; et al. SYNTAX Score Predicts Postoperative Atrial Fibrillation in Patients Undergoing On-Pump Isolated Coronary Artery Bypass Grafting Surgery. Anatol J Cardiol 2015. [Google Scholar] [CrossRef]
- Cerit, L.; Duygu, H.; Gulsen, K.; Kemal, H.S.; Ozcem, B.; Balcioglu, O.; Gunsel, A.; Tosun, O.; Emren, V. Is SYNTAX Score Predictive of Atrial Fibrillation after On-Pump Coronary Artery Bypass Graft Surgery? Korean Circ J 2016, 46, 798. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. European Heart Journal 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C.; Andreotti, F.; Koskinas, K.C.; Rossello, X.; Adamo, M.; Ainslie, J.; Banning, A.P.; Budaj, A.; Buechel, R.R.; Chiariello, G.A.; et al. 2024 ESC Guidelines for the Management of Chronic Coronary Syndromes. European Heart Journal 2024, 45, 3415–3537. [Google Scholar] [CrossRef]
- Van Gelder, I.C.; Rienstra, M.; Bunting, K.V.; Casado-Arroyo, R.; Caso, V.; Crijns, H.J.G.M.; De Potter, T.J.R.; Dwight, J.; Guasti, L.; Hanke, T.; et al. 2024 ESC Guidelines for the Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). European Heart Journal 2024, 45, 3314–3414. [Google Scholar] [CrossRef]
- Gautier, A.; Picard, F.; Ducrocq, G.; Elbez, Y.; Fox, K.M.; Ferrari, R.; Ford, I.; Tardif, J.-C.; Tendera, M.; Steg, P.G.; et al. New-Onset Atrial Fibrillation and Chronic Coronary Syndrome in the CLARIFY Registry. European Heart Journal 2024, 45, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.Y.; Huang, L.; Malwade, S.; Hsu, C.-Y.; Chen, Y.C. Diagnostic Accuracy of Ambulatory Devices in Detecting Atrial Fibrillation: Systematic Review and Meta-Analysis. JMIR Mhealth Uhealth 2021, 9, e26167. [Google Scholar] [CrossRef] [PubMed]
- Lau, Y.C.; Lane, D.A.; Lip, G.Y.H. Atrial Fibrillation in Cryptogenic Stroke: Look Harder, Look Longer, But Just Keep Looking. Stroke 2014, 45, 3184–3185. [Google Scholar] [CrossRef]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; Van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N Engl J Med 2020, 383, 1305–1316. [Google Scholar] [CrossRef]
Figure 1.
ROC curves illustrating the performance of the Gensini score (left) and the ABC score (right) in predicting atrial fibrillation.
Figure 1.
ROC curves illustrating the performance of the Gensini score (left) and the ABC score (right) in predicting atrial fibrillation.
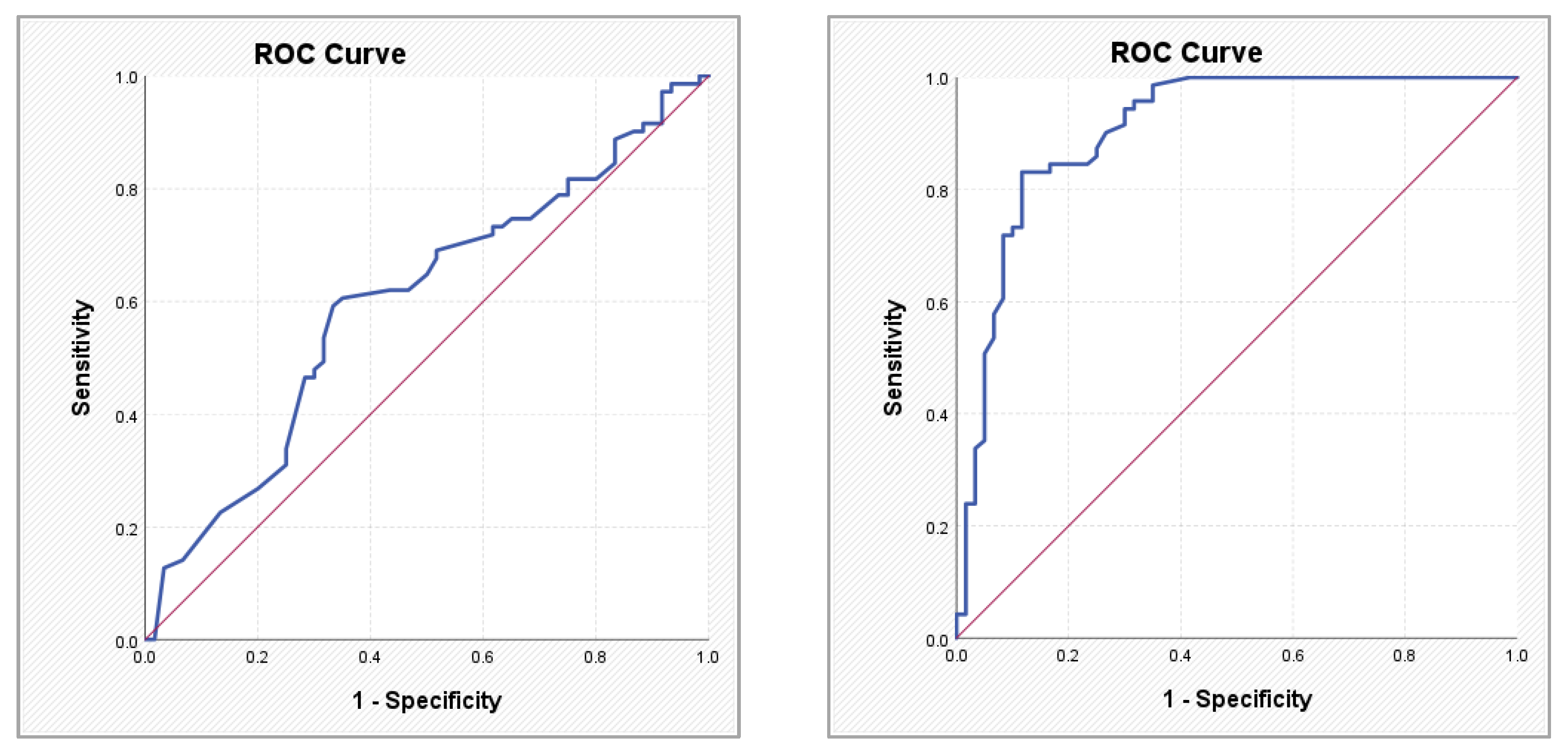
Figure 2.
ROC curves illustrating the performance of the SCORE2-OP score (left) and the Framingham score (right) in predicting atrial fibrillation.
Figure 2.
ROC curves illustrating the performance of the SCORE2-OP score (left) and the Framingham score (right) in predicting atrial fibrillation.
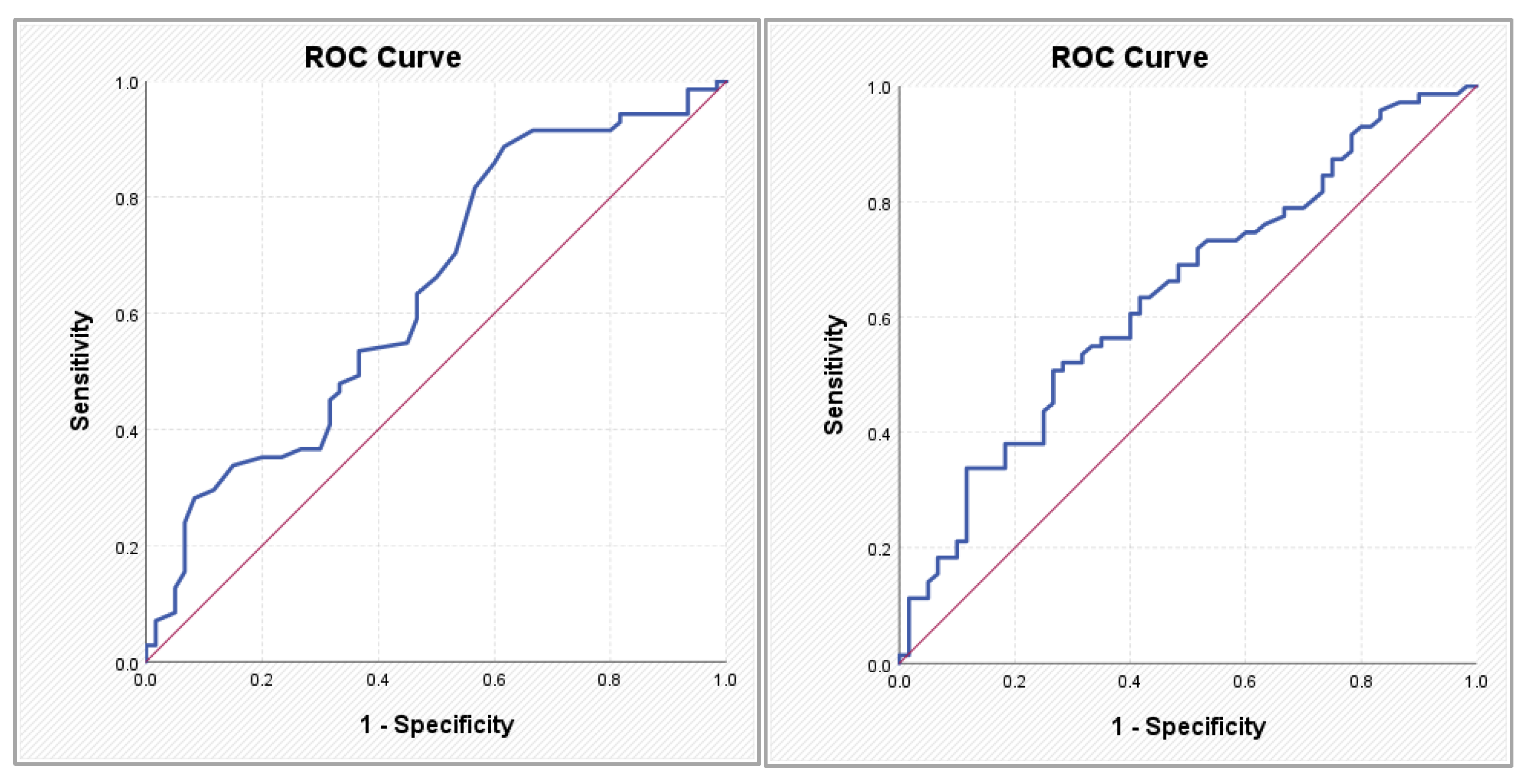
Figure 3.
ROC curves illustrating the performance of the ASCVD score (left) and the SYNTAX PCI score (right) in predicting atrial fibrillation.
Figure 3.
ROC curves illustrating the performance of the ASCVD score (left) and the SYNTAX PCI score (right) in predicting atrial fibrillation.
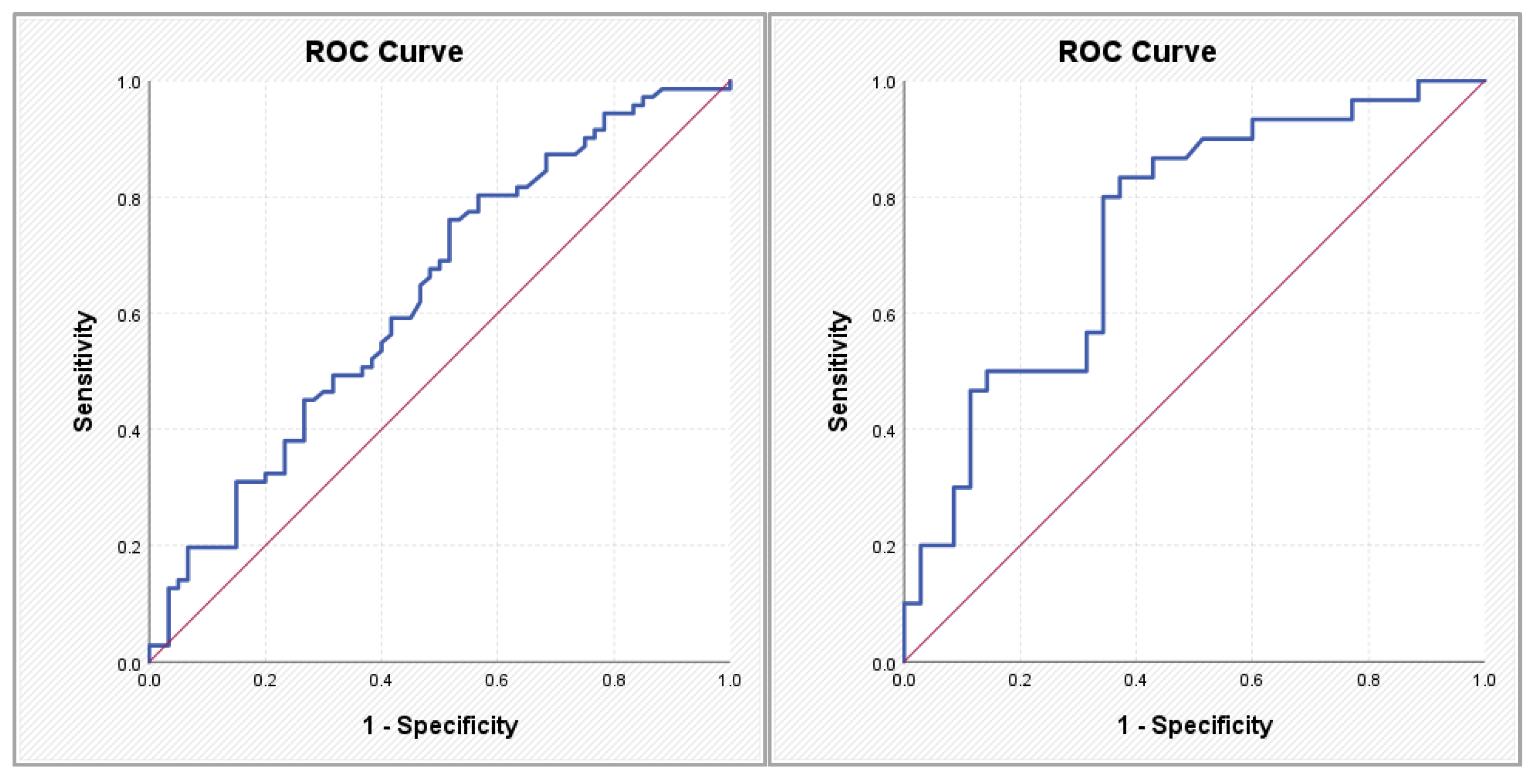
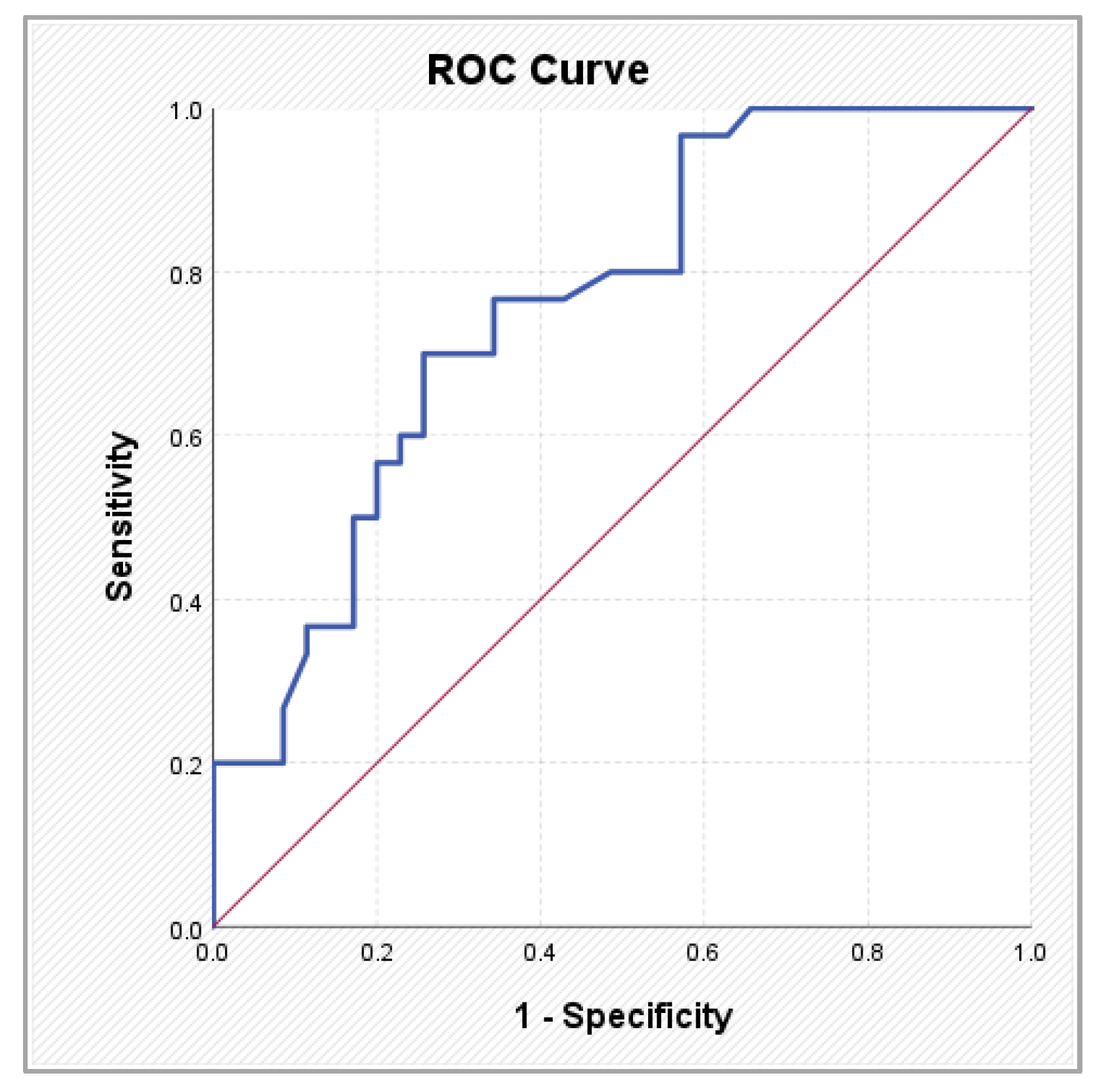
Figure 4.
ROC curve illustrating the performance of the SYNTAX CABG score in predicting atrial fibrillation.
Figure 4.
ROC curve illustrating the performance of the SYNTAX CABG score in predicting atrial fibrillation.

| Risk Score | Score Type | Components and Calculation Method |
|---|---|---|
| Gensini | Anatomical (angiographic) | Each coronary lesion is assigned a score according to the degree of stenosis: 25% (1 point), 50% (2 points), 75% (4 points), 90% (8 points), 99% (16 points), total occlusion (32 points); the score is subsequently weighted based on lesion location (e.g., left main coronary artery, left anterior descending artery); the final score represents the sum of all lesion scores |
| SYNTAX | Anatomical (lesion complexity) | Assesses each coronary lesion ≥50% in vessels ≥1.5 mm; incorporates lesion location, bifurcations/trifurcations, chronic total occlusions, severe calcification, vessel tortuosity, thrombus presence, and diffuse disease; the final score reflects the overall complexity of coronary anatomy |
| Framingham | Clinical (global cardiovascular risk and primary prevention) | Age; sex; total cholesterol; HDL cholesterol; systolic blood pressure; antihypertensive treatment; smoking; diabetes mellitus; estimates 10-year risk of coronary events |
| ASCVD | Clinical (atherosclerotic risk and primary prevention) | Age; sex; race; total cholesterol; HDL cholesterol; systolic blood pressure; antihypertensive treatment; diabetes mellitus; smoking; estimates 10-year risk of myocardial infarction and stroke |
| SCORE2 | Clinical (primary and secondary prevention) | Age (40–69 years); sex; smoking; systolic blood pressure; non-HDL cholesterol; estimates 10-year risk of fatal and non-fatal cardiovascular events, regionally calibrated |
| SCORE2-OP | Clinical (older populations) | Age ≥70 years; sex; smoking; systolic blood pressure; non-HDL cholesterol; adaptation of SCORE2 for older individuals, estimating 10-year cardiovascular risk |
CCS: chronic coronary syndrome; HDL: high-density lipoproteins; ASCVD: Atherosclerotic Cardiovascular Disease score; SCORE2: Systematic Coronary Risk Estimation 2; SCORE2-OP: Systematic Coronary Risk Estimation 2 – older persons.
Table 2.
Distribution of patients with AF according to CCS severity.
| CCS | Total | Pearson Chi-squared test | ||||||
|---|---|---|---|---|---|---|---|---|
| N-CCS | S-CCS | |||||||
| N | % | N | % | N | % | |||
| Rythm | SR | 25 | 37.9% | 35 | 53.8% | 60 | 45.8% | Chi2 = 9.267 |
| PAROX | 8 | 12.1% | 14 | 21.5% | 22 | 16.8% | p = 0.026* | |
| PERS | 9 | 13.6% | 5 | 7.7% | 14 | 10.7% | ||
| PERM | 24 | 36.4% | 11 | 16.9% | 35 | 26.7% | ||
| Total | 66 | 100.0% | 65 | 100.0% | 131 | 100.0% | ||
*p < 0.05; CCS: chronic coronary syndrome; N-SCC: non-significant CCS; S-SCC: significant CCS; AF: atrial fibrillation; SR: sinusal rhythm; PAROX: paroxysmal atrial fibrillation; PERS: persistent atrial fibrillation; PERM: permanent atrial fibrillation.
Table 3.
Comparison of clinical risk scores in CCS according to AF type.
| Parameter | Group | N | Mean ± SD | Median (IQR:25-75) | p Value |
|---|---|---|---|---|---|
| Gensini score | SR | 60 | 30.24 ± 38.64 | 16.50 (0.04–200.00) | 0.043* |
| PAROX | 22 | 30.86 ± 39.82 | 10.50 (2.50–154.00) | ||
| PERS | 14 | 25.00 ± 32.68 | 8.00 (1.00–94.00) | ||
| PERM | 35 | 15.29 ± 22.14 | 5.00 (1.00–100.00) | ||
| All types of AF | 71 | 22.03 ± 31.01 | 8.00 (1.00–154.00) | 0.052+ Post-hoc: PAROX versus PERM p = 0.038*; SR versus PERM p = 0.007** |
|
| ABC score | SR | 60 | 0.45 ± 0.31 | 0.36 (0.15–2.36) | < 0.001** |
| PAROX | 22 | 0.86 ± 0.53 | 0.76 (0.39–2.74) | ||
| PERS | 14 | 0.90 ± 0.44 | 0.79 (0.49–2.07) | ||
| PERM | 35 | 1.13 ± 0.63 | 0.88 (0.40–3.49) | ||
| All types of AF | 71 | 1.00 ± 0.57 | 0.85 (0.39–3.49) | < 0.001** Post-hoc: p = 0.000**for SR versus all types of AF |
|
| Score 2/OP | SR | 60 | 18.89 ± 10.42 | 16.50 (2.60–48.00) | 0.004** |
| PAROX | 22 | 27.86 ± 8.88 | 29.00 (15.00–47.00) | ||
| PERS | 14 | 24.90 ± 14.86 | 21.00 (7.70–55.00) | ||
| PERM | 35 | 21.08 ± 10.18 | 18.00 (3.10–41.00) | ||
| All types of AF | 71 | 23.93 ± 11.14 | 21.00 (3.10–55.00) | 0.006* Post-hoc: SR versus PAROX p = 0.002* |
|
| Framingham score | SR | 60 | 11.30 ± 7.60 | 10.15 (0.50–35.00) | 0.003** |
| PAROX | 22 | 18.65 ± 6.99 | 20.35 (5.10–29.10) | ||
| PERS | 14 | 14.73 ± 10.34 | 12.55 (4.20–44.50) | ||
| PERM | 35 | 13.61 ± 8.62 | 13.70 (1.20–31.30) | ||
| All types of AF | 71 | 15.39 ± 8.70 | 15.10 (1.20–44.50) | 0.007** Post-hoc: SR versus PAROX p = 0.001** |
|
| ASCVD score | SR | 60 | 19.54 ± 13.23 | 18.05 (1.50–59.50) | < 0.001** |
| PAROX | 22 | 35.55 ± 14.10 | 32.40 (15.10–60.80) | ||
| PERS | 14 | 21.62 ± 9.77 | 19.90 (4.80–39.70) | ||
| PERM | 35 | 20.92 ± 12.45 | 18.50 (1.10–63.90) | ||
| All types of AF | 71 | 25.59 ± 14.07 | 21.30 (1.10–63.90) | 0.010* Post-hoc: SR versus PAROX p = 0.000**; PERM versus PAROX p = 0.002* |
|
| SYNTAX PCI | SR | 35 | 29.50 ± 8.82 | 26.80 (16.0–51.7) | 0.007** |
| PAROX | 14 | 35.90 ± 8.62 | 31.85 (25.5–51.3) | ||
| PERS | 5 | 43.44 ± 13.28 | 45.60 (22.8–57.6) | ||
| PERM | 11 | 38.81 ± 12.97 | 34.60 (20.3–67.4) | ||
| All types of AF | 71 | 38.22 ± 11.09 | 36.30 (20.3–67.4) | <0.001** | |
| SYNTAX CABG | SR | 35 | 26.35 ± 9.04 | 26.30 (7.8–47.3) | 0.001** |
| PAROX | 14 | 34.90 ± 9.41 | 35.00 (21.6–54.2) | ||
| PERS | 5 | 41.04 ± 11.44 | 39.10 (24.3–54.6) | ||
| PERM | 11 | 34.31 ± 9.94 | 30.10 (23.5–53.6) | ||
| All types of AF | 71 | 35.71 ± 9.89 | 35.00 (21.6–54.6) | <0.001** Post-hoc: SR versus PAROX p = 0.029*; SR versus PERS p = 0.010* |
* statistically significant difference (p < 0.05); ** statistically highly significant difference (p < 0.01); + value close to statistical significance; SR: sinusal rhythm; PAROX: paroxysmal atrial fibrillation; PERS: persistent atrial fibrillation; PERM: permanent atrial fibrillation; AF: atrial fibrillation.
Table 4.
Multivariate analysis: predictors of atrial fibrillation.
| B | S.E. | Wald | df | Sig. | Exp(B) = OR | 95% CI for EXP(B) | |||
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| ABC | 3.560 | 1.154 | 9.512 | 1 | 0.002** | 35.160 | 3.660 | 337.734 | |
| SYNTAX CABG | 0.077 | 0.038 | 4.208 | 1 | 0.040* | 1.080 | 1.003 | 1.163 | |
| Constant | -1.069 | 0.772 | 1.918 | 1 | 0.166 | 0.343 | |||
* statistically significant difference (p < 0.05).
Table 5.
ROC analysis results for parameters showing statistically significant variations in patients with atrial fibrillation.
Table 5.
ROC analysis results for parameters showing statistically significant variations in patients with atrial fibrillation.
| AUC | p | 95% CI | Cut-off value | Sensibility | Specificity | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Gensini (-) score | 0.598 | 0.053 | 0.501 | 0.696 | 10.50 | 0.592 | 0.667 |
| ABC | 0.908 | 0.000** | 0.854 | 0.961 | 0.615% | 0.831 | 0.883 |
| SCORE 2/OP | 0.639 | 0.006** | 0.543 | 0.734 | 12.50% | 0.887 | 0.383 |
| FRAMINGHAM | 0.638 | 0.007** | 0.543 | 0.732 | 15.05% | 0.507 | 0.733 |
| ASCVD | 0.631 | 0.010* | 0.535 | 0.727 | 16.55% | 0.761 | 0.483 |
| SYNTAX PCI | 0.745 | 0.001** | 0.625 | 0.865 | 28.95 | 0.833 | 0.629 |
| SYNTAX CABG | 0.760 | 0.000** | 0.644 | 0.875 | 29.95 | 0.700 | 0.743 |
* statistically significant difference (p < 0.05); ** statistically highly significant difference (p < 0.01).
Table 6.
Pearson correlations between clinical scores, cardiovascular risk scores, and angiographic indicators.
Table 6.
Pearson correlations between clinical scores, cardiovascular risk scores, and angiographic indicators.
| Confidence intervals for the Spearman rho coefficient | ||||
|---|---|---|---|---|
| Spearman’s rho | p | 95% CI | ||
| Lower | Upper | |||
| Gensini - ABC | -0.021 | 0.810 | -0.197 | 0.156 |
| Gensini - SCORE 2/OP | 0.104 | 0.237 | -0.074 | 0.276 |
| Gensini - FRAMINGHAM | 0.201 | 0.021* | 0.025 | 0.365 |
| Gensini - ASCVD | 0.298 | <0.001** | 0.128 | 0.451 |
| Gensini - SYNTAX PCI | 0.246 | 0.049* | -0.006 | 0.468 |
| Gensini - SYNTAX CABG | 0.225 | 0.072 | -0.027 | 0.450 |
| ABC - SCORE 2/OP | 0.260 | 0.003** | 0.088 | 0.418 |
| ABC - FRAMINGHAM | 0.152 | 0.083 | -0.025 | 0.320 |
| ABC - ASCVD | 0.196 | 0.025* | 0.020 | 0.360 |
| ABC - SYNTAX PCI | 0.559 | <0.001** | 0.358 | 0.710 |
| ABC - SYNTAX CABG | 0.491 | <0.001** | 0.273 | 0.660 |
| SCORE 2/OP - FRAMINGHAM | 0.344 | <0.001** | 0.178 | 0.491 |
| SCORE 2/OP - ASCVD | 0.681 | <0.001** | 0.574 | 0.766 |
| SCORE 2/OP - SYNTAX PCI | 0.593 | <0.001** | 0.402 | 0.735 |
| SCORE 2/OP - SYNTAX CABG | 0.627 | <0.001** | 0.447 | 0.759 |
| FRAMINGHAM - ASCVD | 0.656 | <0.001** | 0.542 | 0.746 |
| FRAMINGHAM - SYNTAX PCI | 0.058 | 0.648 | -0.196 | 0.304 |
| FRAMINGHAM - SYNTAX CABG | 0.422 | <0.001** | 0.191 | 0.608 |
| ASCVD - SYNTAX PCI | 0.321 | 0.009** | 0.077 | 0.530 |
| ASCVD - SYNTAX CABG | 0.572 | <0.001** | 0.375 | 0.719 |
| SYNTAX PCI - SYNTAX CABG | 0.663 | <0.001** | 0.495 | 0.784 |
* statistically significant difference (p < 0.05); ** statistically highly significant difference (p < 0.01);.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



