Submitted:
31 January 2026
Posted:
02 February 2026
You are already at the latest version
Abstract
Cardiac amyloidosis (CA) remains substantially under-recognized because its clinical and imaging manifestations overlap with common cardiovascular conditions, including heart failure with preserved ejection fraction, hypertrophic cardiomyopathy, hypertensive heart disease, and aortic stenosis, while traditional diagnostic “red flags” on electrocardiography and imaging are often absent, subtle, or inconsistently recognized, particularly in early disease, and atypical phenotypes. As a result, CA is frequently diagnosed late, and at an advanced stage. Artificial intelligence (AI) offers a compelling strategy to address these challenges by identifying subtle, multidimensional disease signatures distributed across electrocardiography, echocardiography, cardiac magnetic resonance imaging, and nuclear scintigraphy, and by integrating multimodal and longitudinal data beyond the limits of human pattern recognition. Contemporary AI approaches in CA include deep learning models operating directly on raw signals and imaging data, classical machine learning using engineered features, radiomics-based analysis of myocardial tissue characteristics, and increasingly, multimodal fusion frameworks that aggregate complementary information across modalities. AI-enhanced electrocardiography has emerged as a particularly scalable screening tool, demonstrating high diagnostic discrimination for both transthyretin and light-chain CA and enabling opportunistic detection months before clinical diagnosis. In parallel, echocardiography AI has evolved from feature-based models toward end-to-end video analysis, improving standardization and reducing inter-reader variability, while cardiac magnetic resonance- and scintigraphy-based AI applications enable automated quantification, reduced technical variability, and more reproducible assessment of amyloid burden. Beyond diagnosis, emerging AI models aim to support disease phenotyping, prognostication, and longitudinal treatment monitoring. However, important challenges remain, including dataset shift, heterogeneity in diagnostic reference standards, spectrum bias, and the need for prospective validation and workflow-aware implementation. Thoughtful integration of AI into multidisciplinary amyloidosis care pathways will be essential to translate technical advances into earlier diagnosis and improved clinical outcomes.
Keywords:
cardiac amyloidosis
; artificial intelligence
; ECG
; echocardiogram
; cardiac magnetic resonance imaging
; nuclear scintigraphy
Introduction
Cardiac amyloidosis (CA) is caused by myocardial infiltration of amyloid fibrils that are primarily of transthyretin (ATTR-CA) and light-chain (AL-CA) subtypes. CA remains substantially under-recognized in routine practice, largely because its clinical and imaging phenotype overlaps with more prevalent conditions such as heart failure with preserved ejection fraction (HFpEF), hypertensive heart disease, aortic stenosis, and other causes of left ventricular hypertrophy [1,2,3]. Traditional diagnostic “red flags”—including low QRS voltage, discordance between wall thickness and voltage, apical sparing of longitudinal strain, or characteristic late gadolinium enhancement patterns—are neither universally present nor consistently recognized, particularly in early disease or in women and patients with atypical phenotypes [4,5]. As a result, CA is frequently diagnosed late in its natural history, after irreversible myocardial injury has occurred.
AI is uniquely well suited to address these challenges because the diagnostic signal in CA is often subtle, multidimensional, and distributed across modalities, including high-resolution electrocardiography (ECG) waveforms, echocardiographic motion and texture patterns, cardiac magnetic resonance (CMR) tissue characterization, and nuclear scintigraphy tracer uptake. Moreover, CA diagnosis and management are inherently multimodal and longitudinal, requiring integration of imaging, biomarkers, and clinical trajectories over time—an analytic task that exceeds the capacity of human pattern recognition alone. Accordingly, contemporary studies increasingly position AI not as an experimental tool, but as a practical strategy to raise early diagnostic suspicion, reduce inter-reader variability, and standardize CA detection across diverse clinical settings.
Machine Learning Approaches for Cardiac Signal and Imaging Analysis
Machine learning approaches for cardiac imaging and signal analysis can be broadly categorized into deep learning, classical machine learning, radiomics-based models, and multimodal fusion frameworks. Supervised deep learning methods—primarily convolutional neural networks and transformer-based architectures—operate directly on raw inputs such as ECG voltage–time signals, echocardiographic video clips, CMR images, and scintigraphy data [6,7,8]. When large, well-annotated datasets are available, these models often achieve the highest diagnostic performance by learning complex spatial and temporal patterns, although their deployment may be limited by data requirements and interpretability concerns. Classical machine learning techniques, including random forests and gradient boosting, rely on engineered features derived from imaging, hemodynamic measurements, or electronic health records. These approaches are generally more interpretable and easier to implement but are sensitive to feature quality and inter-site variability [9]. Radiomics-based methods extract high-dimensional texture features from CMR sequences (e.g. T1 mapping) to quantify myocardial tissue heterogeneity that may be difficult to assess visually, though performance depends heavily on image standardization and segmentation [10]. Increasingly, multimodal fusion models integrate complementary data streams—most commonly ECG and echocardiography, with or without clinical variables—leveraging the multisystem manifestations of disease and improving robustness by aggregating weak signals across modalities.
ECG AI: Scalable Screening and Opportunistic Detection
AI-enhanced ECG (AI-ECG) has emerged as one of the most scalable and pragmatic entry points for early detection of CA [11,12,13,14,15,16,17,18] (Figure 1). Deep learning models trained on standard 12-lead ECGs can identify CA-associated electrical signatures even when routine clinical interpretation is non-diagnostic and classic red flags—such as low voltage or pseudoinfarction patterns—are absent. This is particularly relevant in early disease, ATTR-CA, and in patient subgroups with competing causes of left ventricular hypertrophy, where ECG findings are often subtle or nonspecific. Because ECGs are inexpensive, ubiquitous, and already embedded in routine clinical workflows, AI-ECG approaches are well suited for opportunistic screening and automated triage to downstream confirmatory testing.
Several single- and multicenter studies have demonstrated strong diagnostic discrimination of AI-ECG models for CA, including both ATTR and AL subtypes. In a large retrospective cohort of 4,995 individuals (2,541 with AL-CA or ATTR-CA and 2,454 matched controls), a deep learning model trained on standard 12-lead ECGs identified CA with high accuracy (AUC 0.91), substantially outperformed conventional ECG criteria, and detected disease more than six months prior to clinical diagnosis in a majority of cases. [12]. In another study, using ECG and machine learning, detailed electroanatomical mapping in CA revealed characteristic ventricular voltage and activation abnormalities that were translatable to simple 12-lead ECG patterns, enabling markedly improved diagnostic performance after focused training (AUC increasing from 0.69 to 0.97) without reliance on advanced imaging [19]. Finally, in a meta-analysis of five studies comprising seven derivation and validation cohorts (8,639 derivation and 3,843 validation participants), AI-enhanced ECG models demonstrated high pooled diagnostic performance for CA overall (AUC 0.89, 95% CI 0.86–0.91), with similarly strong discrimination for ATTR-CA (AUC 0.90, 95% CI 0.86–0.95) and more modest performance for AL-CA (AUC 0.80, 95% CI 0.80–0.93) [20]. These findings underscore both the promise of AI-ECG as a screening tool and the importance of local validation before deployment.
While individual study design, labeling strategy, and reference standards varied, the consistency of discrimination across cohorts supports the feasibility of AI-ECG for screening-style workflows, particularly as a rule-out or enrichment tool rather than a standalone diagnostic test. Importantly, most studies emphasize probabilistic risk outputs rather than binary classification, aligning with real-world triage and shared decision-making paradigms.
From a practical standpoint, several implementation use cases have been proposed. One approach involves EHR-integrated, background execution of AI-ECG models on all incoming ECGs, generating automated alerts for patients exceeding a predefined risk threshold and prompting targeted chart review and stepwise evaluation [21]. Another use case is pre-test enrichment, in which AI-ECG is used to selectively identify patients who may benefit most from echocardiography, CMR, or bone-avid scintigraphy, thereby improving diagnostic yield and reducing unnecessary downstream testing [12]. These strategies are particularly appealing in health systems with high ECG volumes and limited access to advanced imaging resources.
Despite these advantages, important limitations remain. Dataset shift—driven by differences in ECG acquisition hardware, filtering, lead placement conventions, and the prevalence of conduction disease or paced rhythms—can meaningfully degrade model performance outside the development environment [22]. Label noise is another major challenge, as “ground truth” CA definitions vary across studies and may rely on biopsy, imaging-based criteria, or clinician diagnosis, each with distinct sensitivities and biases [23,24]. Finally, workflow risk is nontrivial: highly sensitive AI-ECG tools can overwhelm clinics with false positives if not paired with clearly defined downstream testing pathways, referral thresholds, and capacity planning [25]. Accordingly, successful clinical deployment requires careful integration with multidisciplinary amyloidosis care pathways rather than isolated algorithmic implementation.
Echocardiography AI: From Engineered Features to Video-Level Detection
Echocardiography has long been central to the evaluation of CA, providing key structural and functional clues such as increased wall thickness, restrictive filling patterns, atrial enlargement, and characteristic abnormalities in longitudinal strain [26]. However, recognition of CA on echocardiography remains highly dependent on reader expertise, clinical suspicion, and image quality, leading to substantial inter-reader variability—particularly in early disease, atypical phenotypes, and patients with competing causes of left ventricular hypertrophy [27,28]. Even well-described markers such as relative apical sparing may be absent or subtle, limiting sensitivity in routine practice [29]. Against this backdrop, AI offers a means to standardize interpretation, surface latent patterns, and reduce reliance on subjective visual recognition.
Broadly, two complementary AI approaches have emerged in echocardiography for CA detection [13,18,30,31,32,33,34,35] (Figure 2). The first involves feature-based machine learning models that leverage conventional echocardiographic measurements, including wall thickness, Doppler indices, left atrial size, and strain-derived parameters [33]. These models often use structured data already stored in echocardiography reporting systems or electronic health records, making them relatively easy to implement and explain. Several studies have demonstrated good diagnostic performance using such approaches, particularly when strain metrics are included, although performance remains sensitive to measurement quality, vendor-specific differences, and local acquisition protocols. In a cohort of 51 patients with confirmed CA, fully automated AI-derived LVEF and GLS from apical 2- and 4-chamber echocardiographic views showed strong agreement with manual measurements (r≈0.74–0.83), with sensitivities of 70–100% and specificities of 67–86% for detecting abnormal function, while substantially reducing measurement time [31]. Nonetheless, feature-based models provide an important bridge between traditional echocardiography and AI-driven augmentation, offering interpretability and lower barriers to deployment.
More recently, the field has shifted toward video-based deep learning approaches that train directly on raw echocardiographic image sequences, most commonly apical four-chamber clips, with or without additional views [13,32,36]. By learning directly from pixel-level motion and texture patterns, these models aim to capture disease-specific signatures—such as subtle abnormalities in myocardial thickening, relaxation, and speckle texture—that are not fully represented by derived summary metrics. In a multicenter cohort of 23,745 patients, a fully automated deep learning echocardiography workflow accurately quantified left ventricular wall thickness (mean absolute error ~1–2 mm) and distinguished CA (AUC 0.79–0.83) and hypertrophic cardiomyopathy (AUC 0.89–0.98), addressing key limitations of human measurement variability and diagnostic overlap [32]. This shift from “feature engineering” to end-to-end video learning represents a major conceptual advance in echo-based CA detection.
Building on modality-specific advances, multimodal pipelines that integrate ECG and echocardiography have further strengthened performance and generalizability. A landmark Multicenter AI models using ECG and echocardiography detected CA with high discrimination (C-statistics up to 0.91 and 1.00, respectively), with ECG pre-screening improving echocardiographic PPV from 33% to 74–77% at 67% recall [13]. This work illustrated how complementary signals across modalities can be fused to improve robustness and reduce false positives, reinforcing the concept that CA is best detected through integrated, multimodal analysis rather than reliance on any single test.
Looking ahead, several trajectories are likely to shape the next phase of echocardiography AI in CA. Automated strain computation and image quality control are expected to reduce technical variability and expand access to advanced deformation analysis [37]. Opportunistic CA screening from routine echocardiograms performed for heart failure, murmurs, left ventricular hypertrophy, or aortic stenosis represents a particularly attractive use case, given the high pretest probability in these populations. Finally, longitudinal AI-driven quantification may enable more consistent assessment of disease progression and therapeutic response, reducing inter-reader variability and supporting standardized monitoring in both clinical practice and trials. Together, these developments position echocardiography AI as a central component of scalable, multimodal CA detection strategies.
CMR AI: Tissue Characterization, Radiomics, and Automated Quantification
CMR occupies a unique position in the evaluation of CA, offering unparalleled myocardial tissue characterization through late gadolinium enhancement (LGE), native T1 mapping, and extracellular volume (ECV) quantification [38,39]. These techniques enable detection of diffuse infiltration, disease staging, and prognostication across amyloid subtypes. However, CMR is time-intensive, technically demanding, and dependent on specialized expertise, which limits scalability and contributes to inter-site variability in acquisition and interpretation. AI applications in CMR are therefore focused not only on improving diagnostic performance, but also on reducing technical barriers and standardizing analysis to support broader and more consistent use in CA care.
One major axis of CMR-AI development involves workflow automation and standardization. Automated segmentation of cardiac chambers and myocardial regions, along with automated generation of parametric maps, has been shown to substantially reduce analysis time and inter-observer variability [8,40]. In AL-CA, AI-driven segmentation pipelines have been used to derive native T1 and ECV measures with diagnostic and prognostic relevance comparable to expert manual analysis, supporting both risk stratification and longitudinal follow-up [41]. More broadly, the radiology literature has demonstrated AI applications across the CMR pipeline—including accelerated image acquisition, reconstruction, motion correction, segmentation, and quantitative mapping—which is particularly relevant for CA protocols that are often lengthy and resource-intensive. These advances position AI as a key enabler of reproducible, high-throughput CMR assessment in both referral centers and emerging amyloidosis programs.
A second, complementary line of investigation centers on radiomics and machine learning applied to CMR for CA detection and phenotyping [42]. Radiomics approaches extract high-dimensional quantitative features from LGE images—such as texture, signal heterogeneity, and spatial distribution—that extend beyond what is readily appreciated by visual inspection [10]. Several studies have demonstrated that radiomics-based models can distinguish CA from other causes of left ventricular hypertrophy, including hypertrophic cardiomyopathy and hypertensive heart disease, with promising diagnostic performance [43,44]. Importantly, these methods aim not merely to replicate expert interpretation, but to uncover latent tissue signatures that may reflect amyloid burden, infiltration patterns, or disease stage, raising the possibility of more granular phenotyping and risk assessment.
Despite these advances, key gaps remain before CMR-AI can be widely deployed in CA. Generalizability across vendors, field strengths, and pulse sequences remains a major challenge, as CMR acquisition parameters vary substantially across centers and can strongly influence quantitative outputs. Harmonization of labels is another unresolved issue, as many datasets combine ATTR-CA and AL-CA, span wide ranges of disease severity, or include patients at different treatment stages, complicating model interpretation and clinical translation. Finally, most studies to date have been retrospective and performed in highly selected populations; prospective validation in real-world “left ventricular hypertrophy clinics”—where the differential diagnosis is broad and pretest probability of CA is modest—will be essential to define clinical utility and cost-effectiveness. Addressing these gaps will determine whether CMR-AI evolves from a powerful research tool into a scalable component of routine CA evaluation.
Nuclear Scintigraphy AI: Automated Detection and Quantitative Assessment
Bone-avid radiotracer scintigraphy using agents such as 99mTc–pyrophosphate (PYP), 99mTc–DPD, or 99mTc–HMDP has become central to the noninvasive diagnosis of ATTR-CA when interpreted in the appropriate clinical context [45]. Despite its high diagnostic specificity, real-world interpretation remains vulnerable to variability in visual grading, region-of-interest (ROI) placement, planar versus SPECT assessment, and reader experience—factors that can influence both diagnostic classification and longitudinal assessment. AI applications in nuclear cardiology are therefore well aligned with the core pain points of scintigraphy: standardization, automation, and reproducible quantification.
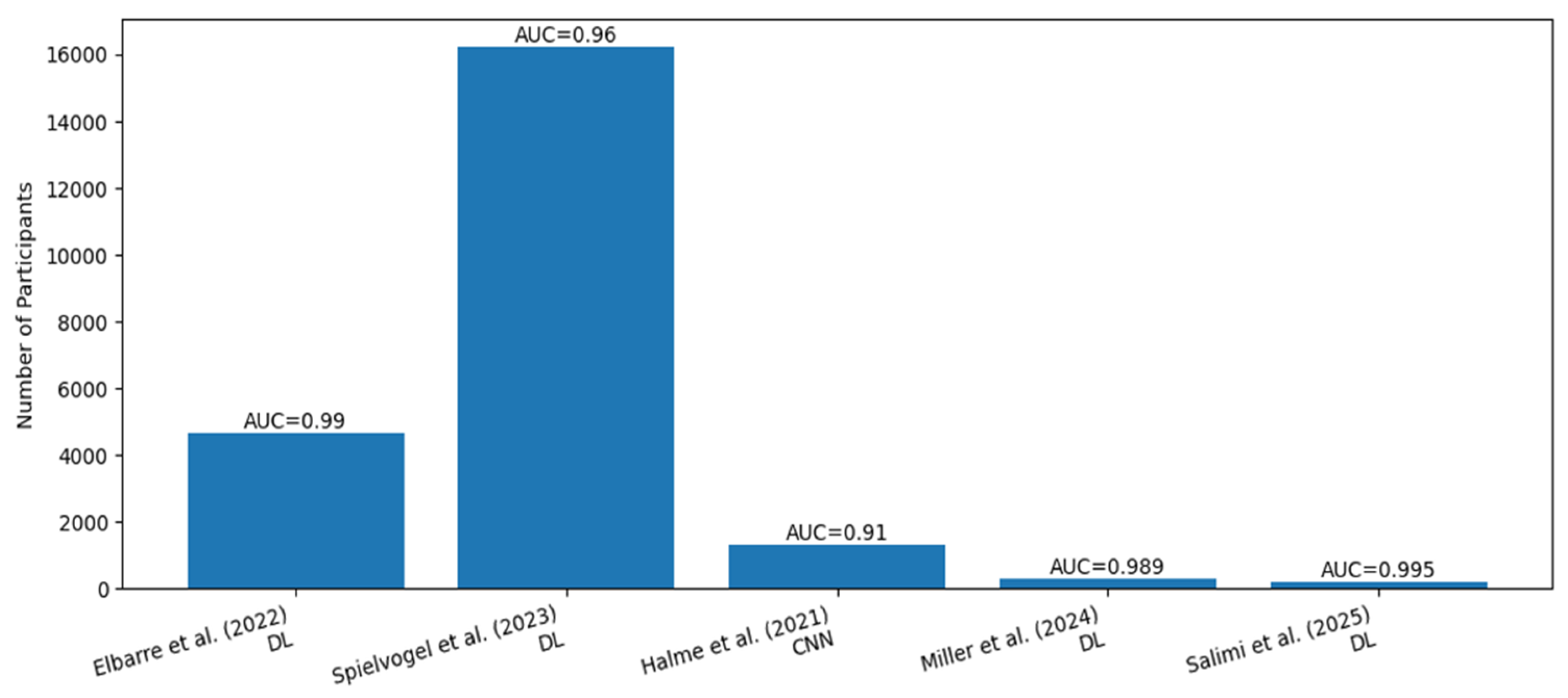
Recent advances have focused on deep learning–based quantification of cardiac radiotracer uptake, with automated myocardial segmentation enabling fully automated calculation of volumetric and intensity-based uptake metrics from SPECT or planar imaging [46,47,48,49,50,51] (Figure 3). Studies using AI-driven quantification of 99mTc-PYP uptake have demonstrated close agreement with expert-defined measurements while substantially reducing operator dependence, suggesting a pathway toward more reproducible classification and follow-up assessment. Importantly, such approaches move beyond traditional semi-quantitative heart-to-contralateral (H/CL) ratios toward more granular, three-dimensional characterization of tracer distribution, which may better reflect amyloid burden.
A parallel and increasingly compelling application involves opportunistic detection of ATTR-CA on routine scintigraphy performed for non-cardiac indications. Deep learning models trained to identify amyloid-suggestive cardiac uptake on whole-body or regional scans—originally acquired for oncologic or skeletal evaluation—have been reported, highlighting the potential to surface previously unrecognized ATTR-CA without additional imaging or radiation exposure. This screening paradigm aligns with broader trends in opportunistic imaging analytics and is particularly attractive given the aging population undergoing nuclear studies for unrelated conditions. By standardizing detection and flagging suspicious studies for confirmatory evaluation, AI could meaningfully advance earlier case finding.
More recently, investigators have extended deep learning approaches to total-body scintigraphy across different bone tracers and scanner platforms, reflecting a deliberate move toward vendor- and tracer-agnostic deployment. Models trained and validated across multiple tracers (PYP, DPD, HMDP) and institutions suggest that AI may help harmonize interpretation across international practice patterns, where tracer choice and acquisition protocols vary widely. Such generalizability is especially important for ATTR-CA, where diagnostic pathways differ substantially between North America and Europe.
From a practical standpoint, nuclear scintigraphy AI offers several advantages that directly address clinical needs. Automated analysis promises more consistent reads across sites and readers, reducing variability in both diagnosis and follow-up. Improved quantitative measures may support longitudinal monitoring of disease burden and therapeutic response as disease-modifying treatments expand. Finally, opportunistic detection from non-cardiac nuclear studies represents a low-cost, high-yield strategy to identify patients earlier in the disease course. Together, these developments position AI-enhanced scintigraphy as a natural complement to ECG-, echo-, and CMR-based approaches in a comprehensive, multimodal CA detection ecosystem.
Beyond Diagnosis: Prognosis, Phenotyping, and Treatment Monitoring
Expanding the Role of AI Beyond Case Detection
As AI-based tools for CA mature, their role is increasingly framed not merely as diagnostic classifiers, but as platforms for disease phenotyping, risk stratification, and longitudinal monitoring. Rather than asking only whether CA is present, contemporary models aim to estimate the likelihood of ATTR-CA versus AL-CA, infer disease stage or burden using imaging and electrical proxies, and predict clinically meaningful outcomes such as heart failure hospitalization, arrhythmias, and mortality. These approaches typically leverage multimodal inputs—including ECG embeddings, echocardiographic deformation patterns, CMR tissue metrics, and scintigraphic quantification—to capture complementary aspects of myocardial involvement that are difficult to integrate manually.
Studies suggest that AI-derived features may carry prognostic information beyond traditional clinical and imaging markers. For example, latent ECG representations and automated strain or mapping metrics have been associated with adverse outcomes in CA cohorts, raising the possibility of AI-assisted risk stratification and treatment prioritization [52]. This highlights the prognostic dimension as a key frontier for the field. However, most prognostic models remain retrospective and require careful recalibration in the contemporary treatment era, as disease-modifying therapies such as tafamidis and emerging AL-directed treatments fundamentally alter baseline risk and disease trajectories.
AI for Treatment Response and Longitudinal Monitoring
Another rapidly evolving application is the use of AI to track therapeutic response and disease progression. Automated, reproducible quantification of longitudinal strain patterns, ECG embeddings, parametric mapping values (native T1, ECV), and scintigraphic uptake may enable more sensitive detection of subtle changes over time than conventional visual or manual approaches. This capability is particularly relevant as therapies are initiated earlier in the disease course, when absolute changes are small but clinically meaningful. Standardized AI-driven measurements could also facilitate harmonized endpoints in clinical trials and registries, addressing long-standing challenges related to inter-reader variability and site-to-site inconsistency.
Implementation: What “Good” Clinical Deployment Looks like
A practical, Stepwise Care Model
Effective clinical deployment of AI for CA requires integration into existing workflows rather than standalone algorithmic outputs. A pragmatic model begins with opportunistic AI screening—most commonly using ECG and/or echocardiography—to flag patients at elevated risk. This is followed by a clinical adjudication layer, in which heart failure phenotype, left ventricular hypertrophy context, red flags, and monoclonal protein testing are considered to refine pretest probability. Confirmatory testing with CMR and/or bone-tracer scintigraphy is then pursued as appropriate, with endomyocardial biopsy reserved for selected cases. Critically, this pathway should incorporate a feedback loop to track false positives and false negatives, support local recalibration, and monitor model drift over time.
Metrics That Matter Clinically
Traditional performance metrics such as AUC, while useful, are insufficient to judge real-world utility. Calibration is essential: a predicted risk of 0.8 should correspond to an approximately 80% observed risk in the local population. Decision-curve analysis and net benefit across clinically relevant thresholds better capture whether AI meaningfully improves decision-making compared with existing strategies. Fairness and subgroup performance—across sex, race/ethnicity, age, and device or vendor—must be explicitly evaluated, given known disparities in CA recognition. Finally, operational impact metrics, including referral volume, diagnostic yield, time-to-diagnosis, and downstream testing burden, are critical to determining whether AI deployment improves care rather than simply shifting workload.
Key Limitations and Open Problems
Several unresolved challenges continue to constrain translation. Ground-truth uncertainty remains a major issue, as diagnostic standards vary across studies and institutions, and amyloid subtype labeling may be incomplete or inferred rather than definitively established. Spectrum bias is common, with many models trained on clear-cut CA cases versus healthy controls, inflating apparent performance compared with real-world left ventricular hypertrophy or HFpEF cohorts. Generalization across sites and vendors remains difficult, given heterogeneity in ECG preprocessing, echocardiographic acquisition, and CMR protocols. Additionally, explainability remains central to clinician trust; actionable interpretability tools—such as saliency maps, exemplar-based comparisons, or transparent feature-based models—are often needed to contextualize AI outputs. Finally, there is a pressing need for prospective, pragmatic trials demonstrating that AI reduces missed CA, shortens time-to-diagnosis, or improves patient-centered outcomes, rather than simply achieving high discrimination metrics.
Future Directions
Looking forward, multimodal foundation models capable of learning unified representations across ECG, echocardiographic video, CMR, scintigraphy, and clinical text are well aligned with the complex, multi-test diagnostic journey of CA. Integration of AI-enabled care pathways directly into ECG and echocardiography lab workflows—paired with clear reflex testing algorithms (e.g., monoclonal protein screening followed by PYP or CMR and genetics referral)—may facilitate scalable adoption. As therapeutic options expand and earlier disease stages are increasingly targeted [53,54], standardized, automated response metrics are likely to become essential, positioning AI not only as a diagnostic adjunct but as a cornerstone of longitudinal CA management.
Conclusions
AI is rapidly transforming the detection and evaluation of CA by enabling earlier, more consistent recognition of disease signals that are often subtle, multimodal, and missed by conventional interpretation. While diagnostic performance across ECG, echocardiography, CMR, and nuclear imaging is promising, real-world impact will depend on rigorous external validation, calibration, and integration into clinically actionable care pathways. Ultimately, AI’s greatest value in CA may lie not as a standalone diagnostic tool, but as an embedded, longitudinal decision-support system that improves timeliness of diagnosis, risk stratification, and treatment monitoring in the modern therapeutic era.
Disclosures
None.
Funding
None.
References
- Bukhari, S. Cardiac amyloidosis: state-of-the-art review. J Geriatr Cardiol 2023, 20, 361–375. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.; Bashir, Z. Diagnostic Modalities in the Detection of Cardiac Amyloidosis. J Clin Med 2024, 13. [Google Scholar] [CrossRef]
- Gillmore, J.D.; Maurer, M.S.; Falk, R.H.; Merlini, G.; Damy, T.; Dispenzieri, A.; Wechalekar, A.D.; Berk, J.L.; Quarta, C.C.; Grogan, M.; et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation 2016, 133, 2404–2412. [Google Scholar] [CrossRef]
- Bukhari, S.; Bashir, Z.; Shah, N.; Patel, Y.; Hulten, E. Investigating Cardiac Amyloidosis: A Primer for Clinicians. R I Med J 2013, 2025(108), 49–55. [Google Scholar]
- Bukhari, S.; Barakat, A.F.; Eisele, Y.S.; Nieves, R.; Jain, S.; Saba, S.; Follansbee, W.P.; Brownell, A.; Soman, P. Prevalence of Atrial Fibrillation and Thromboembolic Risk in Wild-Type Transthyretin Amyloid Cardiomyopathy. Circulation 2021, 143, 1335–1337. [Google Scholar] [CrossRef]
- Attia, Z.I.; Noseworthy, P.A.; Lopez-Jimenez, F.; Asirvatham, S.J.; Deshmukh, A.J.; Gersh, B.J.; Carter, R.E.; Yao, X.; Rabinstein, A.A.; Erickson, B.J.; et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: a retrospective analysis of outcome prediction. Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef]
- Ouyang, D.; He, B.; Ghorbani, A.; Yuan, N.; Ebinger, J.; Langlotz, C.P.; Heidenreich, P.A.; Harrington, R.A.; Liang, D.H.; Ashley, E.A.; et al. Video-based AI for beat-to-beat assessment of cardiac function. Nature 2020, 580, 252–256. [Google Scholar] [CrossRef]
- Bai, W.; Sinclair, M.; Tarroni, G.; Oktay, O.; Rajchl, M.; Vaillant, G.; Lee, A.M.; Aung, N.; Lukaschuk, E.; Sanghvi, M.M.; et al. Automated cardiovascular magnetic resonance image analysis with fully convolutional networks. J Cardiovasc Magn Reson 2018, 20, 65. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; et al. Predictive analytics with gradient boosting in clinical medicine. Ann Transl Med 2019, 7, 152. [Google Scholar] [CrossRef] [PubMed]
- Baessler, B.; Engelhardt, S.; Hekalo, A.; Hennemuth, A.; Hullebrand, M.; Laube, A.; Scherer, C.; Tolle, M.; Wech, T. Perfect Match: Radiomics and Artificial Intelligence in Cardiac Imaging. Circ Cardiovasc Imaging 2024, 17, e015490. [Google Scholar] [CrossRef]
- Vrudhula, A.; Stern, L.; Cheng, P.C.; Ricchiuto, P.; Daluwatte, C.; Witteles, R.; Patel, J.; Ouyang, D. Impact of Case and Control Selection on Training Artificial Intelligence Screening of Cardiac Amyloidosis. JACC Adv 2024, 3, 100998. [Google Scholar] [CrossRef]
- Grogan, M.; Lopez-Jimenez, F.; Cohen-Shelly, M.; Dispenzieri, A.; Attia, Z.I.; Abou Ezzedine, O.F.; Lin, G.; Kapa, S.; Borgeson, D.D.; Friedman, P.A.; et al. Artificial Intelligence-Enhanced Electrocardiogram for the Early Detection of Cardiac Amyloidosis. Mayo Clin Proc 2021, 96, 2768–2778. [Google Scholar] [CrossRef]
- Goto, S.; Mahara, K.; Beussink-Nelson, L.; Ikura, H.; Katsumata, Y.; Endo, J.; Gaggin, H.K.; Shah, S.J.; Itabashi, Y.; MacRae, C.A.; et al. Artificial intelligence-enabled fully automated detection of cardiac amyloidosis using electrocardiograms and echocardiograms. Nat Commun 2021, 12, 2726. [Google Scholar] [CrossRef] [PubMed]
- Tison, G.H.; Zhang, J.; Delling, F.N.; Deo, R.C. Automated and Interpretable Patient ECG Profiles for Disease Detection, Tracking, and Discovery. Circ Cardiovasc Qual Outcomes 2019, 12, e005289. [Google Scholar] [CrossRef] [PubMed]
- Haimovich, J.S.; Diamant, N.; Khurshid, S.; Di Achille, P.; Reeder, C.; Friedman, S.; Singh, P.; Spurlock, W.; Ellinor, P.T.; Philippakis, A.; et al. Artificial intelligence-enabled classification of hypertrophic heart diseases using electrocardiograms. Cardiovasc Digit Health J 2023, 4, 48–59. [Google Scholar] [CrossRef]
- Goto, S.; Solanki, D.; John, J.E.; Yagi, R.; Homilius, M.; Ichihara, G.; Katsumata, Y.; Gaggin, H.K.; Itabashi, Y.; MacRae, C.A.; et al. Multinational Federated Learning Approach to Train ECG and Echocardiogram Models for Hypertrophic Cardiomyopathy Detection. Circulation 2022, 146, 755–769. [Google Scholar] [CrossRef]
- Harmon, D.M.; Mangold, K.; Suarez, A.B.; Scott, C.G.; Murphree, D.H.; Malik, A.; Attia, Z.I.; Lopez-Jimenez, F.; Friedman, P.A.; Dispenzieri, A.; et al. Postdevelopment Performance and Validation of the Artificial Intelligence-Enhanced Electrocardiogram for Detection of Cardiac Amyloidosis. JACC Adv 2023, 2. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.K.; Sangha, V.; Shankar, S.V.; Coppi, A.; Krumholz, H.M.; Nasir, K.; Miller, E.J.; Gallegos Kattan, C.; Al-Mallah, M.H.; Al-Kindi, S.; et al. Artificial intelligence-enabled electrocardiography and echocardiography to track preclinical progression of transthyretin amyloid cardiomyopathy. Eur Heart J 2025, 46, 3651–3662. [Google Scholar] [CrossRef]
- Schrutka, L.; Anner, P.; Agibetov, A.; Seirer, B.; Dusik, F.; Rettl, R.; Duca, F.; Dalos, D.; Dachs, T.M.; Binder, C.; et al. Machine learning-derived electrocardiographic algorithm for the detection of cardiac amyloidosis. Heart 2022, 108, 1137–1147. [Google Scholar] [CrossRef]
- Khan, L.A.; Shaikh, F.H.; Khan, M.S.; Zafar, B.; Farooqi, M.; Bold, B.; Aslam, H.M.; Essam, N.; Noor, I.; Siddique, A.; et al. Artificial intelligence-enhanced electrocardiogram for the diagnosis of cardiac amyloidosis: A systemic review and meta-analysis. Curr Probl Cardiol 2024, 49, 102860. [Google Scholar] [CrossRef]
- Attia, Z.I.; Friedman, P.A.; Noseworthy, P.A.; Lopez-Jimenez, F.; Ladewig, D.J.; Satam, G.; Pellikka, P.A.; Munger, T.M.; Asirvatham, S.J.; Scott, C.G.; et al. Age and Sex Estimation Using Artificial Intelligence From Standard 12-Lead ECGs. Circ Arrhythm Electrophysiol 2019, 12, e007284. [Google Scholar] [CrossRef] [PubMed]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat Med 2019, 25, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.S.; Bokhari, S.; Damy, T.; Dorbala, S.; Drachman, B.M.; Fontana, M.; Grogan, M.; Kristen, A.V.; Lousada, I.; Nativi-Nicolau, J.; et al. Expert Consensus Recommendations for the Suspicion and Diagnosis of Transthyretin Cardiac Amyloidosis. Circ Heart Fail 2019, 12, e006075. [Google Scholar] [CrossRef]
- Bashir, Z.; Younus, A.; Dhillon, S.; Kasi, A.; Bukhari, S. Epidemiology, diagnosis, and management of cardiac amyloidosis. J Investig Med 2024, 72, 620–632. [Google Scholar] [CrossRef]
- Liu, X.; Faes, L.; Kale, A.U.; Wagner, S.K.; Fu, D.J.; Bruynseels, A.; Mahendiran, T.; Moraes, G.; Shamdas, M.; Kern, C.; et al. A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: a systematic review and meta-analysis. Lancet Digit Health 2019, 1, e271–e297. [Google Scholar] [CrossRef]
- Bashir, Z.; Musharraf, M.; Azam, R.; Bukhari, S. Imaging modalities in cardiac amyloidosis. Curr Probl Cardiol 2024, 49, 102858. [Google Scholar] [CrossRef]
- Kikuchi, D.S.; Quinaglia, T.; Bukhari, S.; Sharma, K.; Coelho-Filho, O.R.; Hays, A.G. Cardiac Magnetic Resonance Imaging in Heart Failure With Preserved Ejection Fraction. Circ Cardiovasc Imaging 2025, 18, e018519. [Google Scholar] [CrossRef] [PubMed]
- Quinaglia, T.; Bukhari, S.; Kikuchi, D.S.; Bau, A.A.; Nicolela Geraldo Martins, C.; Sharma, K.; Jerosch-Herold, M.; Hays, A.G.; Coelho-Filho, O.R. How to Use Imaging: Cardiac Magnetic Resonance Imaging in Heart Failure With Preserved Ejection Fraction: a Stepwise Differential Diagnosis Approach. Circ Cardiovasc Imaging 2026, e019000. [Google Scholar] [CrossRef]
- Bukhari, S.; Younus, A.; Bashir, Z. Emerging Insights into Granulomatous and Amyloidogenic Cardiomyopathies. J Clin Med 2025, 14. [Google Scholar] [CrossRef]
- Chang, R.S.; Chiu, I.M.; Tacon, P.; Abiragi, M.; Cao, L.; Hong, G.; Le, J.; Zou, J.; Daluwatte, C.; Ricchiuto, P.; et al. Detection of cardiac amyloidosis using machine learning on routine echocardiographic measurements. Open Heart 2024, 11. [Google Scholar] [CrossRef]
- Cotella, J.I.; Slivnick, J.A.; Sanderson, E.; Singulane, C.; O’Driscoll, J.; Asch, F.M.; Addetia, K.; Woodward, G.; Lang, R.M. Artificial intelligence based left ventricular ejection fraction and global longitudinal strain in cardiac amyloidosis. Echocardiography 2023, 40, 188–195. [Google Scholar] [CrossRef]
- Duffy, G.; Cheng, P.P.; Yuan, N.; He, B.; Kwan, A.C.; Shun-Shin, M.J.; Alexander, K.M.; Ebinger, J.; Lungren, M.P.; Rader, F.; et al. High-Throughput Precision Phenotyping of Left Ventricular Hypertrophy With Cardiovascular Deep Learning. JAMA Cardiol 2022, 7, 386–395. [Google Scholar] [CrossRef]
- Zhang, J.; Gajjala, S.; Agrawal, P.; Tison, G.H.; Hallock, L.A.; Beussink-Nelson, L.; Lassen, M.H.; Fan, E.; Aras, M.A.; Jordan, C.; et al. Fully Automated Echocardiogram Interpretation in Clinical Practice. Circulation 2018, 138, 1623–1635. [Google Scholar] [CrossRef]
- Chao, C.J.; Jeong, J.; Arsanjani, R.; Kim, K.; Tsai, Y.L.; Yu, W.C.; Farina, J.M.; Mahmoud, A.K.; Ayoub, C.; Grogan, M.; et al. Echocardiography-Based Deep Learning Model to Differentiate Constrictive Pericarditis and Restrictive Cardiomyopathy. JACC Cardiovasc Imaging 2024, 17, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chao, C.J.; Jeong, J.J.; Farina, J.M.; Seri, A.R.; Barry, T.; Newman, H.; Campany, M.; Abdou, M.; O’Shea, M.; et al. Developing an Echocardiography-Based, Automatic Deep Learning Framework for the Differentiation of Increased Left Ventricular Wall Thickness Etiologies. J Imaging 2023, 9. [Google Scholar] [CrossRef]
- Slivnick, J.A.; Hawkes, W.; Oliveira, J.; Woodward, G.; Akerman, A.; Gomez, A.; Hamza, I.; Desai, V.K.; Barrett-O’Keefe, Z.; Grogan, M.; et al. Cardiac amyloidosis detection from a single echocardiographic video clip: a novel artificial intelligence-based screening tool. Eur Heart J 2025, 46, 4090–4101. [Google Scholar] [CrossRef] [PubMed]
- Narang, A.; Bae, R.; Hong, H.; Thomas, Y.; Surette, S.; Cadieu, C.; Chaudhry, A.; Martin, R.P.; McCarthy, P.M.; Rubenson, D.S.; et al. Utility of a Deep-Learning Algorithm to Guide Novices to Acquire Echocardiograms for Limited Diagnostic Use. JAMA Cardiol 2021, 6, 624–632. [Google Scholar] [CrossRef]
- Olausson, E.; Wertz, J.; Fridman, Y.; Bering, P.; Maanja, M.; Niklasson, L.; Wong, T.C.; Fukui, M.; Cavalcante, J.L.; Cater, G.; et al. Diffuse myocardial fibrosis associates with incident ventricular arrhythmia in implantable cardioverter defibrillator recipients. medRxiv 2023. [Google Scholar] [CrossRef]
- Masri, A.; Bukhari, S.; Eisele, Y.S.; Soman, P. Molecular Imaging of Cardiac Amyloidosis. J Nucl Med 2020, 61, 965–970. [Google Scholar] [CrossRef]
- Bernard, O.; Lalande, A.; Zotti, C.; Cervenansky, F.; Yang, X.; Heng, P.A.; Cetin, I.; Lekadir, K.; Camara, O.; Gonzalez Ballester, M.A.; et al. Deep Learning Techniques for Automatic MRI Cardiac Multi-Structures Segmentation and Diagnosis: Is the Problem Solved? IEEE Trans Med Imaging 2018, 37, 2514–2525. [Google Scholar] [CrossRef]
- Bhatt, N.; Ramanan, V.; Orbach, A.; Biswas, L.; Ng, M.; Guo, F.; Qi, X.; Guo, L.; Jimenez-Juan, L.; Roifman, I.; et al. A Deep Learning Segmentation Pipeline for Cardiac T1 Mapping Using MRI Relaxation-based Synthetic Contrast Augmentation. Radiol Artif Intell 2022, 4, e210294. [Google Scholar] [CrossRef] [PubMed]
- Raisi-Estabragh, Z.; Izquierdo, C.; Campello, V.M.; Martin-Isla, C.; Jaggi, A.; Harvey, N.C.; Lekadir, K.; Petersen, S.E. Cardiac magnetic resonance radiomics: basic principles and clinical perspectives. Eur Heart J Cardiovasc Imaging 2020, 21, 349–356. [Google Scholar] [CrossRef]
- Jiang, S.; Zhang, L.; Wang, J.; Li, X.; Hu, S.; Fu, Y.; Wang, X.; Hao, S.; Hu, C. Differentiating between cardiac amyloidosis and hypertrophic cardiomyopathy on non-contrast cine-magnetic resonance images using machine learning-based radiomics. Front Cardiovasc Med 2022, 9, 1001269. [Google Scholar] [CrossRef]
- Zhang, S.; Guo, Y.; Gao, Y.; Wu, M.; Zhuang, S.; Li, X.; Chen, T.; Li, J.; Tian, Z.; Wang, Y.; et al. Differentiation of light chain cardiac amyloidosis and hypertrophic cardiomyopathy by ensemble machine learning-based radiomic analysis of cardiac magnetic resonance. Orphanet J Rare Dis 2025, 20, 557. [Google Scholar] [CrossRef]
- Masri, A.; Bukhari, S.; Ahmad, S.; Nieves, R.; Eisele, Y.S.; Follansbee, W.; Brownell, A.; Wong, T.C.; Schelbert, E.; Soman, P. Efficient 1-Hour Technetium-99 m Pyrophosphate Imaging Protocol for the Diagnosis of Transthyretin Cardiac Amyloidosis. Circ Cardiovasc Imaging 2020, 13, e010249. [Google Scholar] [CrossRef]
- Miller, R.J.H.; Shanbhag, A.; Michalowska, A.M.; Kavanagh, P.; Liang, J.X.; Builoff, V.; Fine, N.M.; Dey, D.; Berman, D.S.; Slomka, P.J. Deep Learning-Enabled Quantification of (99m)Tc-Pyrophosphate SPECT/CT for Cardiac Amyloidosis. J Nucl Med 2024, 65, 1144–1150. [Google Scholar] [CrossRef]
- Scully, P.R.; Morris, E.; Patel, K.P.; Treibel, T.A.; Burniston, M.; Klotz, E.; Newton, J.D.; Sabharwal, N.; Kelion, A.; Manisty, C.; et al. DPD Quantification in Cardiac Amyloidosis: A Novel Imaging Biomarker. JACC Cardiovasc Imaging 2020, 13, 1353–1363. [Google Scholar] [CrossRef]
- Delbarre, M.A.; Girardon, F.; Roquette, L.; Blanc-Durand, P.; Hubaut, M.A.; Hachulla, E.; Semah, F.; Huglo, D.; Garcelon, N.; Marchal, E.; et al. Deep Learning on Bone Scintigraphy to Detect Abnormal Cardiac Uptake at Risk of Cardiac Amyloidosis. JACC Cardiovasc Imaging 2023, 16, 1085–1095. [Google Scholar] [CrossRef]
- Spielvogel, C.P.; Haberl, D.; Mascherbauer, K.; Ning, J.; Kluge, K.; Traub-Weidinger, T.; Davies, R.H.; Pierce, I.; Patel, K.; Nakuz, T.; et al. Diagnosis and prognosis of abnormal cardiac scintigraphy uptake suggestive of cardiac amyloidosis using artificial intelligence: a retrospective, international, multicentre, cross-tracer development and validation study. Lancet Digit Health 2024, 6, e251–e260. [Google Scholar] [CrossRef] [PubMed]
- Halme, H.L.; Ihalainen, T.; Suomalainen, O.; Loimaala, A.; Matzke, S.; Uusitalo, V.; Sipila, O.; Hippelainen, E. Convolutional neural networks for detection of transthyretin amyloidosis in 2D scintigraphy images. EJNMMI Res 2022, 12, 27. [Google Scholar] [CrossRef] [PubMed]
- Salimi, Y.; Shiri, I.; Mansouri, Z.; Sanaat, A.; Hajianfar, G.; Hervier, E.; Bitarafan, A.; Caobelli, F.; Hundertmark, M.; Mainta, I.; et al. Artificial intelligence-based cardiac transthyretin amyloidosis detection and scoring in scintigraphy imaging: multi-tracer, multi-scanner, and multi-center development and evaluation study. Eur J Nucl Med Mol Imaging 2025, 52, 2513–2528. [Google Scholar] [CrossRef]
- Amadio, J.M.; Grogan, M.; Muchtar, E.; Lopez-Jimenez, F.; Attia, Z.I.; AbouEzzeddine, O.; Lin, G.; Dasari, S.; Kapa, S.; Borgeson, D.D.; et al. Predictors of mortality by an artificial intelligence enhanced electrocardiogram model for cardiac amyloidosis. ESC Heart Fail 2025, 12, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.; Hamza, M.; Malik, A. Transthyretin Cardiac Amyloidosis and Heart Failure: State-of-the-Art Review and Practice Guidance. Rev Cardiovasc Med 2025, 26, 46181. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.; Khan, S.Z.; Ghoweba, M.; Khan, B.; Bashir, Z. Arrhythmias and Device Therapies in Cardiac Amyloidosis. J Clin Med 2024, 13. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
AI-ECG in Cardiac Amyloidosis: Sample Size and Performance in Studies. AI, artificial intelligence; AUC, area under the receiver operating characteristic curve; CNN, convolutional neural network; DL, deep learning; ECG, electrocardiogram; LV, left ventricle; LVH, left ventricular hypertrophy; ML, machine learning; DNN, deep neural network.
Figure 1.
AI-ECG in Cardiac Amyloidosis: Sample Size and Performance in Studies. AI, artificial intelligence; AUC, area under the receiver operating characteristic curve; CNN, convolutional neural network; DL, deep learning; ECG, electrocardiogram; LV, left ventricle; LVH, left ventricular hypertrophy; ML, machine learning; DNN, deep neural network.
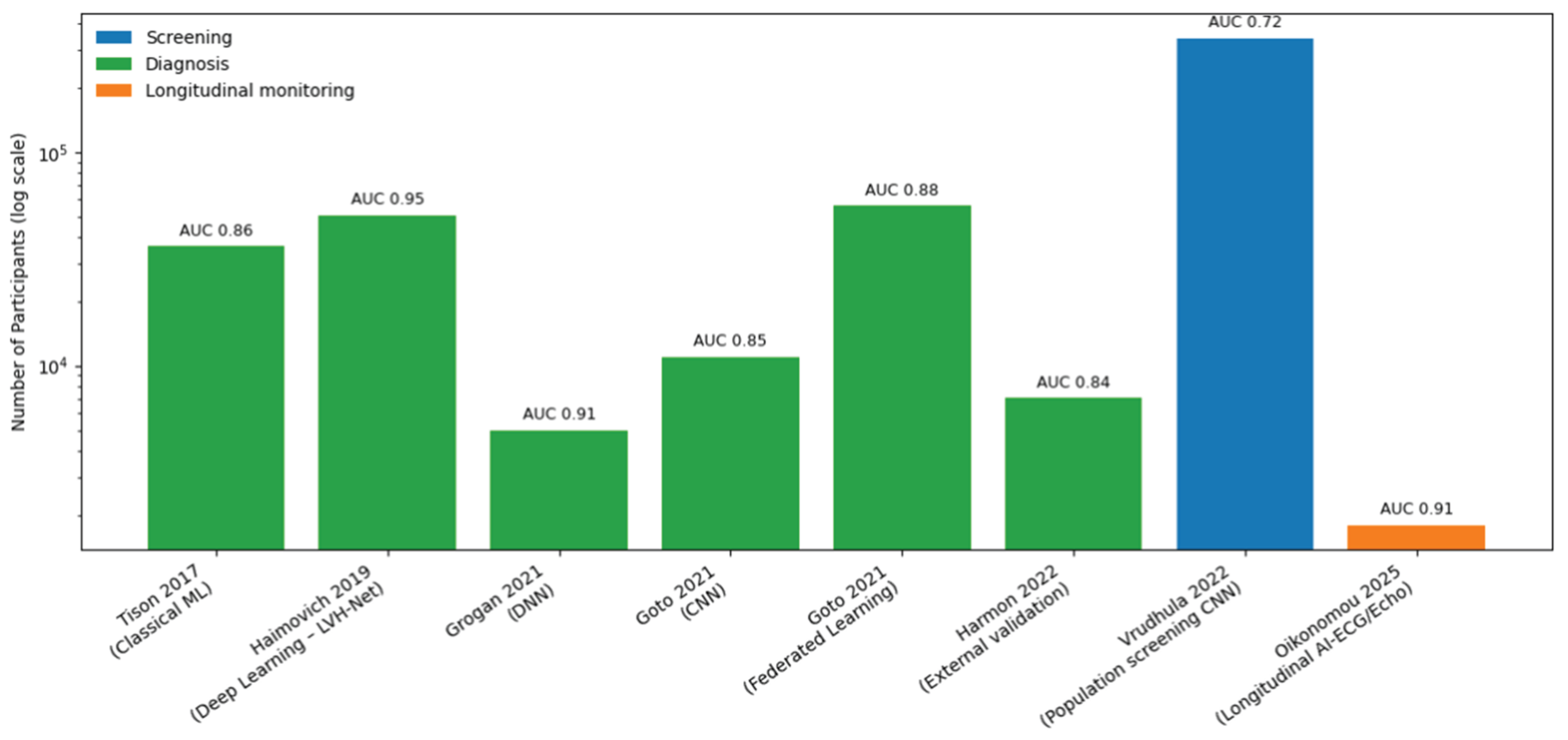
Figure 2.
AI-echocardiography in Cardiac Amyloidosis: Sample Size and Performance in Studies. AI, artificial intelligence; AUC, area under the receiver operating characteristic curve; CA, cardiac amyloidosis; ATTR, transthyretin amyloidosis; CNN, convolutional neural network; DL, deep learning; ECG, electrocardiogram; LV, left ventricle; LVH, left ventricular hypertrophy; ML, machine learning.
Figure 2.
AI-echocardiography in Cardiac Amyloidosis: Sample Size and Performance in Studies. AI, artificial intelligence; AUC, area under the receiver operating characteristic curve; CA, cardiac amyloidosis; ATTR, transthyretin amyloidosis; CNN, convolutional neural network; DL, deep learning; ECG, electrocardiogram; LV, left ventricle; LVH, left ventricular hypertrophy; ML, machine learning.
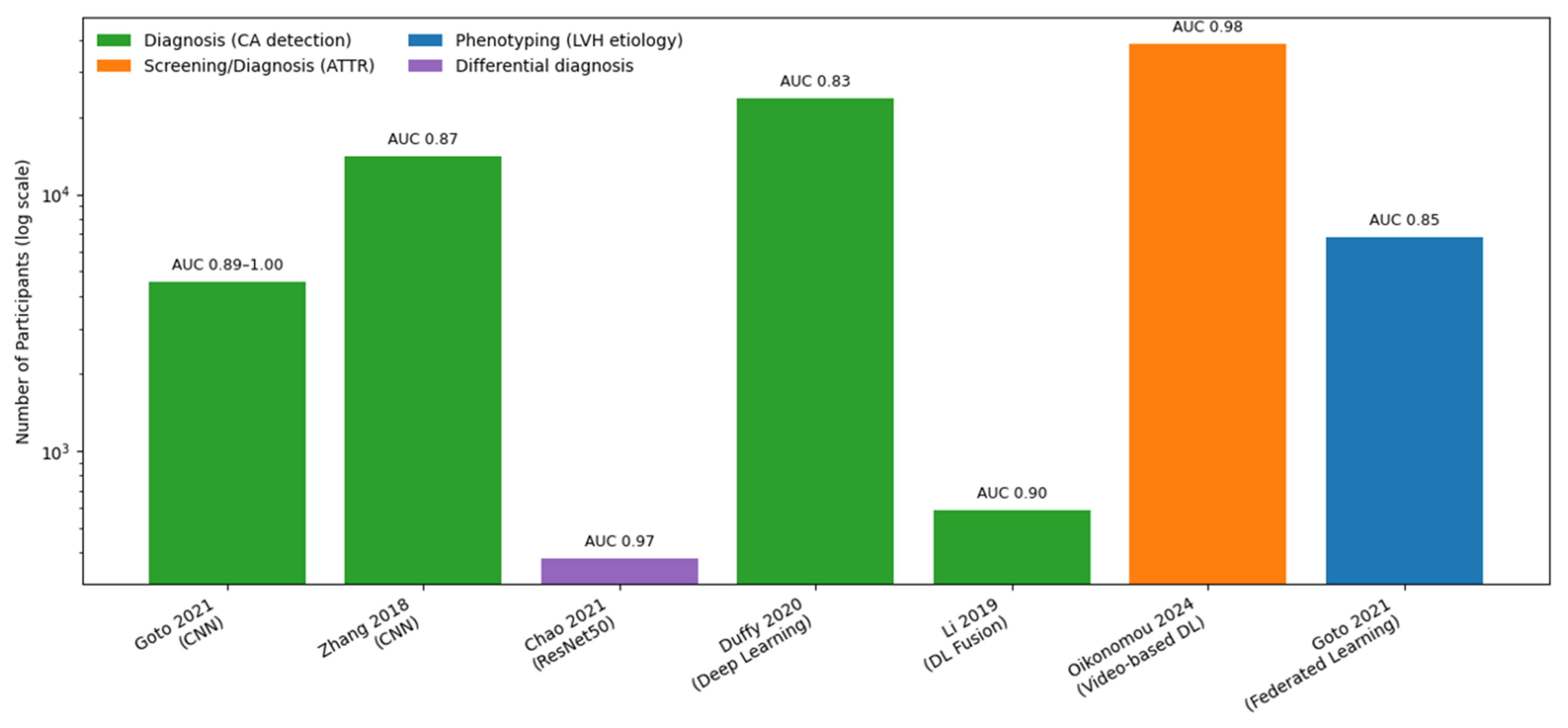
Figure 3.
AI-Nuclear scintigraphy in Cardiac Amyloidosis: Sample Size and Performance in Studies. AI, artificial intelligence; AUC, area under the receiver operating characteristic curve; DL, deep learning; CNN, convolutional neural network.
Figure 3.
AI-Nuclear scintigraphy in Cardiac Amyloidosis: Sample Size and Performance in Studies. AI, artificial intelligence; AUC, area under the receiver operating characteristic curve; DL, deep learning; CNN, convolutional neural network.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



