Submitted:
30 January 2026
Posted:
02 February 2026
You are already at the latest version
Abstract
Background/Objectives: Common femoral artery (CFA) disease often presents alongside multi-level arterial involvement, requiring complex revascularization. Traditionally, femoral endarterectomy (FEA) is the gold standard for CFA lesions due to its high durability. This study evaluates the role of FEA not merely as a localized treatment but as a strategic "platform" for simultaneous hybrid inflow and outflow revascularization.
Methods: We conducted a retrospective, single-center analysis of 52 patients treated for CFA-involved peripheral artery disease between 2010 and 2025. Patients were divided into two groups: the Hybrid (-) Group (isolated FEA, n=23) and the Hybrid (+) Group (FEA combined with simultaneous endovascular inflow or outflow procedures, n=29). In the Hybrid (+) group, the FEA site served as a "hub" for retrograde iliac stenting or antegrade distal interventions. Outcomes measured included hemodynamic improvement, primary patency rates, and safety profiles.
Results: Baseline demographics and cardiovascular risk factors were well-balanced between groups. Both groups showed significant postoperative ankle brachial index improvement (P < 0.001). The 10-year primary patency rate for the femoral segment was exceptionally high at 94.1%. Crucially, utilizing the FEA as a hybrid platform did not compromise the durability of the femoral reconstruction compared to isolated FEA (P=0.460). While inflow (iliac) patency remained stable at 94.1% over 10 years, outflow (distal) patency showed a progressive decline to 42.9% after five years. Regarding safety, the Hybrid (+) group did not show a significant increase in severe complications requiring readmission or re-procedure compared to the Hybrid (-) group (3.4% vs 4.3%, P=1.000). Interestingly, mild wound-related complications were significantly more frequent in the isolated FEA group (P=0.011).
Conclusions: Femoral endarterectomy remains a cornerstone of treatment, providing a safe and effective gateway for comprehensive, single-session revascularization in patients with multi-level diseases. The hybrid platform approach optimizes hemodynamic outcomes and limb salvage without increasing the risk of severe surgical site complications or compromising the long-term patency of the femoral segment.
Keywords:
femoral endarterectomy
; hybrid procedure
; common femoral artery
; peripheral artery disease
; patency
1. Introduction
The common femoral artery (CFA) serves as the principal inflow vessel to the lower extremity. Due to its anatomical location and physiological importance, atherosclerotic lesions isolated to the CFA can result in significant claudication and limb-threatening ischemia [1]. Furthermore, the CFA is recognized as the most common gateway for endovascular procedures, making its patency essential for both current and future vascular interventions [2].
Traditionally, femoral endarterectomy (FEA) with patch closure has been the gold standard and conventional treatment for CFA lesions [3]. While endovascular techniques have advanced rapidly for other vascular segments, FEA remains preferred for the CFA due to its durability and the technical challenges associated with stenting in a high-flexion zone like the groin [1,4]. However, many patients presenting with CFA disease also have concomitant multi-level disease involving both inflow and outflow vessels [5].
The evolution of vascular surgery has led to the development of hybrid procedures, where open surgical techniques are combined with endovascular interventions [6]. In this context, FEA can serve as more than just a localized treatment; it acts as a strategic platform for simultaneous hybrid inflow and outflow revascularization. This approach allows for the comprehensive management of complex peripheral artery disease (PAD) by addressing multiple arterial segments in a single session, potentially reducing the need for more invasive multi-stage surgeries [7].
Despite its theoretical advantages, there is a need for more longitudinal data to confirm the effectiveness and safety of FEA when used as a platform for these hybrid strategies. This study reports a retrospective analysis of clinical data collected from 2010 to 2025 to evaluate the role of femoral endarterectomy in simultaneous hybrid revascularization. By comparing hemodynamic outcomes, effectiveness, and safety profiles, we aim to highlight the durable long-term clinical outcomes and the primary patency rates associated with this integrated approach.
2. Materials and Methods
2.1. Study Design
This study was designed as a retrospective, single-center comparative analysis utilizing a prospectively collected PAD database. The primary objective was to evaluate the utility and clinical outcomes of FEA not merely as a localized treatment for CFA disease, but as a “platform” or gateway for more extensive, simultaneous hybrid revascularization procedures. The study was conducted at the Kyung Hee University Hospital at Gangdong, Seoul, Korea. The protocol adhered to the principles of the Declaration of Helsinki. Due to the retrospective nature of the analysis and the use of de-identified clinical data, the requirement for informed consent was waived by the Institutional Review Board.
2.2. Patient Selection
The study period spanned fifteen years, from 2010 to 2025, a timeframe chosen to capture the evolution of hybrid techniques and the long-term durability of FEA. A total of 52 patients who underwent surgical intervention for CFA-involved PAD were identified. Patients were included if they met the following criteria: Significant atherosclerotic stenosis (>70%) or total occlusion of the CFA confirmed by computed tomography angiography (CTA). Symptomatic presentation, including moderate-to-severe claudication (Rutherford Category 3) or chronic limb-threatening ischemia (CLTI, Rutherford Categories 4-6). Availability of complete preoperative and postoperative hemodynamic data, including Ankle-Brachial Index (ABI) measurements. Patients were excluded if they underwent emergency surgery for acute limb ischemia, had active groin infections at the time of surgery, or if the CFA was treated exclusively with endovascular means without an open endarterectomy component.
2.3. Group Allocation
To evaluate the role of FEA as a platform, the cohort was divided into two distinct groups: The Hybrid (-) Group: Patients who underwent isolated FEA. In these cases, the atherosclerotic disease was localized primarily to the CFA, and the surgical objective was limited to the restoration of patency in this specific segment. The Hybrid (+) Group: Patients who underwent FEA as a platform for simultaneous inflow or outflow revascularization. In this group, the CFA served as the anatomical “hub.” The “Hybrid” approach was defined as the combination of open surgical endarterectomy of the CFA with concurrent endovascular procedures—such as percutaneous transluminal angioplasty (PTA), stenting, or percutaneous atherectomy—performed through the same surgical access site to treat proximal inflow (iliac) or distal outflow (femoropopliteal or infrapopliteal) lesions.
2.4. Preoperative Assessment
Preoperative evaluation involved a detailed physical examination. Hemodynamic status was quantified using the ABI and, where necessary, toe pressures. Anatomical assessment was primarily performed using multi-slice CTA to map the extent of calcification and the involvement of the deep femoral artery (DFA) and superficial femoral artery (SFA). The decision-making process for the surgical strategy was achieved after considering patient factors such as age, comorbid burden (specifically diabetes and end-stage renal disease), and functional status. Anatomical factors were also considered in terms of the length and calcification of inflow/outflow lesions and the suitability of the FEA.
2.5. Surgical Technique
All procedures were performed in a dedicated hybrid operating room equipped with mobile C-arm imaging systems. Under general anesthesia, a longitudinal skin incision was made in the groin to expose the CFA, the distal external iliac artery if necessary, and the bifurcation of the SFA and DFA. The detailed procedures were shown in Figure 1. Following systemic heparinization, vascular control was obtained. Longitudinal arteriotomy was performed across the CFA, usually extending from the healthy proximal segment to the transition point of the SFA or DFA. The plaque was carefully dissected in the subintimal plane. A “feathered” endpoint was prioritized at the distal transition to prevent intimal flaps. In the Hybrid (+) group, the FEA site was then utilized as the entry point for endovascular tools. Before closing the arteriotomy, a sheath was introduced directly into the artery to perform retrograde intervention (for iliac inflow disease) or antegrade intervention (for distal SFA or popliteal disease). This approach eliminated the need for a separate percutaneous puncture site, thereby reducing the risk of access-site complications in a different limb. Following the completion of both the endarterectomy and any supplementary endovascular maneuvers, the arteriotomy was closed. In all cases, patch angioplasty was performed to avoid luminal narrowing associated with primary closure. Materials used for patching included bovine pericardium, synthetic materials (PTFE), or autologous vein grafts, depending on the availability of autologous grafts.
2.6. Outcomes
The study analyzed three primary categories of outcomes to determine the efficacy of the FEA platform, including hemodynamic outcomes of the change in ABI from the preoperative baseline to the postoperative period, clinical effectiveness of primary patency rates, and safety outcomes and complications: Postoperative complications were rigorously categorized using a standardized 3-tiered grading system: mild (minor issues such as tolerable wound pain, tingling sensations, or localized numbness that resolved without medical intervention), moderate (complications requiring pharmacological management or outpatient procedures, such as lymphedema requiring venoactive medication or seromas requiring simple aspiration) and severe (complications necessitating readmission, reoperation, or intensive inpatient care).
2.7. Statistical Analysis
Categorical variables were summarized as frequencies and percentages, while continuous variables were presented as mean ± standard deviation (SD), depending on the normality of the distribution. Statistical comparisons between the Hybrid (-) and Hybrid (+) groups were performed to identify differences in baseline demographics and clinical outcomes. For categorical data, the chi-square test or Fisher’s exact test was employed. For continuous data, the independent t-test or Mann-Whitney U test was used. Long-term patency and survival outcomes were analyzed using the Kaplan-Meier method, and differences between the curves were assessed using the log-rank test. All statistical calculations were performed using MedCalc (version 23.1.7) and SPSS (version 22.0). A P-value < 0.05 was used to denote statistical significance for all tests.
3. Results
3.1. Baseline Characteristics
A total of 52 patients were enrolled in this study between 2010 and 2025. The cohort was divided into two groups: the Hybrid (-) group (n = 23, 44.2%), who underwent isolated FEA, and the Hybrid (+) group (n = 29, 55.8%), who underwent FEA as a platform for simultaneous inflow or outflow revascularization. The baseline demographics were well-balanced between the two groups, with no statistically significant differences observed (Table 1). The mean age of the total population was 70.7 ± 9.0 years, with the Hybrid (-) group averaging 69.9 ± 8.1 years and the Hybrid (+) group 71.2 ± 9.8 years (P=0.603). The majority of the patients were male (82.7%), and there was no significant difference in gender distribution between the Hybrid (-) and Hybrid (+) groups (91.3% vs. 75.9%, P=0.268). The mean body mass index (BMI) was also similar between the groups (22.6 ± 4.2 kg/m² vs. 22.8 ± 3.5 kg/m², P=0.903). The mean follow-up period for the entire cohort was 39.0 ± 42.5 months, with the Hybrid (+) group having a longer, though not statistically significant, follow-up period compared to the Hybrid (-) group (46.1 ± 8.6 months vs. 30.2 ± 36.6 months, P=0.183). Analysis of cardiovascular risk factors showed high prevalence across both groups. Hypertension was the most common comorbidity, affecting 67.3% of the total population, followed by diabetes (57.7%) and smoking history (42.3%). Statistical comparisons revealed no significant disparities in the prevalence of diabetes (P=0.781), hypertension (P=0.776), or smoking history (P=0.162) between the groups. Furthermore, there were no significant differences in the rates of dyslipidemia (P=0.310), coronary artery disease (P=1.000), cerebrovascular disease (P=0.116), or end-stage renal disease (ESRD) on hemodialysis (P=0.577).
3.2. Procedural Details
Table 2 outlines the procedural details for the 52 patients, comparing the Hybrid (-) group (n=23) and the Hybrid (+) group (n=29). There were no significant differences in the surgical site (p=0.412) or the type of patch used for closure (p=0.588). Autologous patches, primarily great saphenous vein (GSV) branches, were used in 56.5% of the Hybrid (-) group and 48.3% of the Hybrid (+) group. Artificial grafts, predominantly bovine pericardium, were utilized in the remaining cases. In the Hybrid (+) group, the femoral endarterectomy site served as a platform for additional interventions: 62.1% underwent inflow revascularization (iliac stenting), 20.7% had outflow revascularization, and 17.2% required both. Outflow procedures included balloon angioplasty, mechanical atherectomy, and aneurysm repair. Hemodynamic outcomes showed significant improvement in both groups, with postoperative ABI increasing significantly from preoperative levels (p < 0.001). While the Hybrid (-) group had higher baseline and postoperative ABIs, the mean increase (postoperative-preoperative) was robust in both cohorts (0.27 ± 0.13 vs. 0.36 ± 0.16; p=0.119).
3.3. Primary Outcomes
Figure 2 presents Kaplan–Meier survival analysis evaluating the 10-year longitudinal primary patency of arterial segments following FEA. The data reveal a significant dichotomy in durability between the proximal FEA platform and distal outflow revascularization. Both the femoral endarterectomy site (A) and the iliac inflow segment (B) demonstrate exceptional long-term stability, each maintaining a primary patency rate of 94.1% at 10 years. In contrast, outflow revascularization (C), involving femoropopliteal or infrapopliteal segments, shows a progressive decline in patency. While the 5-year patency remains relatively high at 85.7%, it drops sharply to 42.9% thereafter. These results suggest that while the FEA-based inflow platform is highly durable, long-term success is primarily limited by the attrition of distal outflow bypasses.
3.4. Procedural Outcomes and Clinical Effectiveness
The primary goal was to assess the role of FEA as a platform for complex revascularization. In the Hybrid (+) group, FEA provided access for various simultaneous procedures. The clinical effectiveness was high across the board. Primary patency at the femoral endarterectomy site; no statistically significant difference was observed between groups (P = 0.460), demonstrating the high durability of the surgical reconstruction. Amputation-free survival and overall survival of the two groups show no statistical significance (Figure 3).
3.5. Postoperative Safety and Complications
Table 3 shows the complications of both groups. Safety outcomes were assessed by grading postoperative complications as mild, moderate, or severe. Interestingly, the Hybrid (-) group experienced a significantly higher rate of mild complications (65.2% vs. 27.6%, P=0.011). These mild complications primarily consisted of tolerable wound pain, tingling sensations, and numbness. Moderate complications, such as wound pain requiring analgesics, lymphedema, or seromas requiring aspiration, occurred in 17.2% of the Hybrid (+) group and 4.3% of the Hybrid (-) group, though this difference was not statistically significant (P=0.210). Severe complications necessitating readmission or re-procedure were rare and occurred at similar rates in both groups (4.3% in Hybrid (-) vs. 3.4% in Hybrid (+), P=1.000). For instance, one patient in the Hybrid (-) group required readmission and vacuum-assisted closure (VAC) therapy for a combined seroma and infection. In the Hybrid (+) group, one patient was readmitted for seroma management. These findings indicate that the added complexity of a hybrid procedure does not significantly increase the risk of severe surgical site complications compared to isolated FEA.
4. Discussion
The primary finding of this study is that femoral endarterectomy (FEA) remains an exceptionally robust and versatile “platform” for the management of complex, multi-level peripheral artery disease. While the common femoral artery (CFA) is often viewed as a localized site of atherosclerotic disease, our data suggests its role is far more strategic. By utilizing the FEA site as an anatomical hub, we were able to facilitate simultaneous inflow and outflow interventions without increasing the risk of severe complications. This “platform” approach addresses the limitations of purely endovascular or purely open surgical strategies, providing a tailored, comprehensive solution for patients with extensive arterial involvement.
Historically, the gold standard for CFA disease has been open endarterectomy with patch angioplasty. Despite the rapid advancement of endovascular technologies, including drug-coated balloons and atherectomy devices, the CFA remains a challenging territory for stenting due to its proximity to the hip joint and the constant mechanical stress of flexion [8,9,10]. Our study reinforces the durability of the open approach, demonstrating a high primary patency rate of 94.1% for the femoral segment. More importantly, it highlights that the addition of endovascular maneuvers for inflow or outflow lesions (the Hybrid + group) does not compromise the long-term patency of the femoral reconstruction itself.
The safety profile of the hybrid approach is particularly noteworthy. One might expect that combining open surgery with endovascular interventions—which often involves longer procedure times and increased instrumentation—would lead to a higher rate of surgical site infections or wound complications [11,12]. However, our results indicated that severe complications requiring readmission or re-intervention were remarkably low and statistically similar between the isolated FEA and hybrid groups. Interestingly, the higher rate of mild complications in the Hybrid (-) group suggests that the complexity of the hybrid procedure does not necessarily translate to a more difficult recovery for the patient regarding wound healing or postoperative pain.
Hemodynamic improvement, as measured by ABI, was consistent across both cohorts. The ability to treat iliac inflow disease and infra-popliteal outflow disease through a single groin incision is a significant advantage of the FEA platform. This simultaneous revascularization minimizes the physiological stress of multiple staged procedures, which is especially beneficial for the aging population and those with significant comorbidities like diabetes and ESRD, who represented a large portion of our study cohort [13,14,15]. By maximizing the inflow and outflow through one “gateway,” we optimize the chances of limb salvage and wound healing in patients with chronic limb-threatening ischemia.
Both anatomical and physiological considerations should guide the strategic choice between isolated FEA and a hybrid approach. In our practice, the FEA platform allowed for the treatment of long-segment SFA occlusions or complex iliac stenoses that might have otherwise required more invasive bypass surgery or separate percutaneous access sites. By converting the CFA into a controlled access point during endarterectomy, the surgeon gains superior control over the distal and proximal endpoints of the revascularization, potentially reducing the risk of distal embolization or flow-limiting dissections often encountered in purely percutaneous procedures [16].
In a hybrid procedure, the technical point of patch closure is to facilitate arterial reconstruction while maintaining a “hub” for endovascular access. After performing the FEA, the patch is partially sutured to the arteriotomy. Before completion of the suture line, a sheath is inserted directly through the patch or the corner of the arteriotomy [17]. This allows for hemostatic access. The sheath provides a sealed entry point for wires and catheters to treat proximal inflow or distal outflow lesions under fluoroscopic guidance. Another advantage is the stable platform. The open arteriotomy offers direct visualization, reducing the risk of subintimal dissection during sheath placement compared to percutaneous access. Once the endovascular phase is finished, the sheath is removed, and the remaining patch suturing is completed. This ensures a wide, non-stenotic lumen that preserves the durability of the “platform.”
In the patch closure after endarterectomy, autologous veins, particularly the great saphenous vein, offer several physiological and clinical advantages over artificial grafts. In our study, 27 (51.9%) of patients used autologous veins. The primary advantage is the presence of a viable endothelial lining, which provides natural resistance to thrombosis. Furthermore, autologous tissue possesses superior infection resistance [1,18]. The superficial tributaries of GSV can be good alternatives to the main GSV [19]. Bovine pericardial patch angioplasty has emerged as a promising alternative, offering durability and a lower risk of complications such as rupture and infection [20,21]. In our study, we used the bovine pericardium patch in 24 (46.2%) of patients. Only 2 patients used artificial graft.
Despite the positive outcomes, this study has several limitations. First, its retrospective nature and the relatively small sample size (n=52) may limit the generalizability of the findings and the statistical power to detect subtle differences in certain outcomes. Second, while the data spans a significant period (2010–2025), the evolution of endovascular devices over these 15 years could introduce a historical bias in the Hybrid (+) group. Finally, the selection of the procedural strategy was based on the surgeon’s discretion rather than randomization, which may introduce selection bias. Future prospective, randomized trials are needed to further validate the long-term superiority of the FEA-platform strategy over alternative multi-stage or purely endovascular approaches.
5. Conclusions
This study demonstrates that FEA remains the cornerstone of treatment for complex CFA disease, particularly when used as a strategic “platform” for hybrid revascularization. Our results indicate that FEA provides a safe and effective gateway for simultaneous inflow and outflow interventions, allowing for comprehensive limb revascularization in a single procedural session. The hybrid approach did not compromise the durability of the femoral reconstruction, maintaining a high primary patency rate of 94.1%. Furthermore, despite the increased technical complexity of simultaneous procedures, the safety profile remained excellent, with no significant increase in severe postoperative complications compared to isolated endarterectomy. While mild wound-related issues were noted, they were manageable and did not impede clinical recovery. Ultimately, utilizing FEA as a platform facilitates tailored revascularization strategies that are particularly beneficial for high-risk patients with multi-level arterial disease. This approach optimizes hemodynamic outcomes and limb salvage while minimizing the need for multiple staged interventions. Future prospective studies are warranted to further refine patient selection and long-term surveillance protocols for this integrated surgical strategy.
Author Contributions
Conceptualization, J.J. and S.C.; methodology, J.J.; software, J.J. and S.C.; validation, J.J. and S.C. and J.J. and S.C.; formal analysis, J.J.; investigation, J.J.; resources, J.J. and S.C.; data curation, J.J.; writing—original draft preparation, J.J.; writing—review and editing, J.J. and S.C.; visualization, J.J. and S.C.; supervision, J.J.; project administration, J.J. and S.C.; funding acquisition, NA. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Kyung Hee University Hospital at Gangdong (protocol code; KHNMC 2022-08-022 and September 5th, 2022).”.
Informed Consent Statement
Patient consent was waived due to a lack of information on the participant’s identity.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.B.; Suresh, K.R.; Murad, M.H.; et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. Eur. J. Vasc. Endovasc. Surg. 2019, 58, S1–S109.e133. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Yamamoto, S.; Kimura, M.; Sano, M.; Sato, O.; Deguchi, J. Long-Term Outcomes following Common Femoral Endarterectomy. J. Clin. Med. 2022, 11, 6388. [Google Scholar] [CrossRef]
- Mizoguchi, T.; Harada, T.; Takeuchi, Y.; Samura, M.; Kurazumi, H.; Suzuki, R.; Suehiro, K.; Hamano, K. Clinical Outcomes of Common Femoral Thromboendarterectomy for Lower-Extremity Arterial Disease: Differences Between Chronic Limb-Threatening Ischemia and Intermittent Claudication. Vasc. Specialist Int. 2025, 41, 3. [Google Scholar] [CrossRef]
- Bamdé, C.C.; Goueffic, Y.; Blitti, C.; Laubriet, A.; Davaine, J.M.; Steinmetz, E. Balloon angioplasty plus stenting or atherectomy plus drug-coated balloon angioplasty in endovascular repair of the common femoral artery. J. Vasc. Surg. 2025. In Press. [Google Scholar] [CrossRef] [PubMed]
- Joh, J.H.; Joo, SH.; Park, H.C. Simultaneous hybrid revascularization for symptomatic lower extremity arterial occlusive disease. Exp. Ther. Med. 2014, 7, 804–810. [Google Scholar] [CrossRef]
- DeCarlo, C.; Boitano, L.T.; Sumpio, B.; Latz, C.A.; Feldman, Z.; Pendleton, A.A.; Chou, E.L.; Stern, J.R.; Dua, A. Comparative Analysis of Outcomes in Patients Undergoing Femoral Endarterectomy plus Endovascular (Hybrid) or Bypass for Femoropopliteal Occlusive Disease. Ann. Vasc. Surg. 2021, 72, 227–236. [Google Scholar] [CrossRef]
- Kaneta, G.; Khandpur, M.; Saratzis, A.; Zayed, H. Mid-Term Outcomes of Hybrid Revascularisation of Symptomatic Multilevel Peripheral Arterial Disease Across Two Centres. J. Endovasc. Ther. 2025, 15266028251363532. [Google Scholar] [CrossRef]
- Gouëffic, Y.; Della Schiava, N.; Thaveau, F.; Rosset, E.; Favre, J.P.; Salomon du Mont, L.; Alsac, J.M.; Hassen-Khodja, R.; Reix, T.; Allaire, E.; et al. Stenting or Surgery for De Novo Common Femoral Artery Stenosis. JACC Cardiovasc. Interv. 2017, 10, 1344–1354. [Google Scholar] [CrossRef] [PubMed]
- Changal, K.H.; Syed, M.A.; Dar, T.; Mangi, M.A.; Sheikh, M.A. Systematic Review and Proportional Meta-Analysis of Endarterectomy and Endovascular Therapy with Routine or Selective Stenting for Common Femoral Artery Atherosclerotic Disease. J. Interv. Cardiol. 2019, 2019, 1593401. [Google Scholar] [CrossRef]
- Tresson, P.; Hublet, A.; Holdner, A.; Bordet, M.; Millon, A.; Papillard, M.; Rouviere, O. Common Femoral Artery Curvature During Hip Flexion. Cardiovasc. Intervent. Radiol. 2023, 46, 844–851. [Google Scholar] [CrossRef]
- Fereydooni, A.; Zhou, B.; Xu, Y.; Deng, Y.; Dardik, A.; Ochoa Chaar, C.I. Rapid increase in hybrid surgery for the treatment of peripheral artery disease in the Vascular Quality Initiative database. J. Vasc. Surg. 2020, 72*, 977–986.e971. [Google Scholar] [CrossRef] [PubMed]
- Zavatta, M.; Mell, M.W. A national Vascular Quality Initiative database comparison of hybrid and open repair for aortoiliac-femoral occlusive disease. J. Vasc. Surg. 2018, 67, 199–205.e191. [Google Scholar] [CrossRef]
- Chang, R.W.; Goodney, P.P.; Baek, J.H.; Nolan, B.W.; Rzucidlo, E.M.; Powell, R.J. Long-term results of combined common femoral endarterectomy and iliac stenting/stent grafting for occlusive disease. J. Vasc. Surg. 2008, 48, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Dosluoglu, H.H.; Lall, P.; Cherr, G.S.; Harris, L.M.; Dryjski, M.L. Role of simple and complex hybrid revascularization procedures for symptomatic lower extremity occlusive disease. J. Vasc. Surg. 2010, 51, 1425–1435.e1421. [Google Scholar] [CrossRef]
- Zhou, M.; Huang, D.; Liu, C.; Liu, Z.; Zhang, M.; Qiao, T.; Liu, C.J. Comparison of hybrid procedure and open surgical revascularization for multilevel infrainguinal arterial occlusive disease. Clin. Interv. Aging 2014, 9, 1595–1603. [Google Scholar] [CrossRef] [PubMed]
- Vakhitov, D.M.; Suominen, V.; Oksala, N. Alternative femoral endarterectomies: technical aspects and short-term results. Angiol. Sosud. Khir 2021, 27, 104–113. [Google Scholar] [CrossRef]
- Katsui, S.; Igari, K.; Nishizawa, M.; Kudo, T. Safety and Ease of Sheath Insertion During Endovascular Treatment Via the Common Femoral Artery After Endarterectomy With Autologous Repair: A Retrospective Cohort Study. Vasc. Endovascular Surg. 2022, 56, 237–243. [Google Scholar] [CrossRef]
- Conte, M.S.; Pomposelli, F.B.; Clair, D.G.; Geraghty, P.J.; McKinsey, J.F.; Mills, J.L.; Moneta, G.L.; Murad, M.H.; Powell, R.J.; Reed, A.B.; et al. Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: management of asymptomatic disease and claudication. J. Vasc. Surg. 2015, 61, 2S–41S. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Uchiyama, H.; Oonuki, M. Outcomes of Femoral Endarterectomy with Superficial Tributary Vein Patch Angioplasty. Ann. Vasc. Surg. 2023, 90, 197–203. [Google Scholar] [CrossRef]
- Zatykó, D.Z.; Pomozi, E.; Pál, D.; Kovács, T.; Szeberin, Z. Utilization of Bovine Pericardium Patch During Common Femoral Endarterectomy. J. Clin. Med. 2025, 14, 11. [Google Scholar] [CrossRef]
- Li, X.; Guo, Y.; Ziegler, K.R.; Model, L.S.; Eghbalieh, S.D.; Brenes, R.A.; Kim, S.T.; Shu, C.; Dardik, A. Current usage and future directions for the bovine pericardial patch. Ann. Vasc. Surg. 2011, 25, 561–568. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Surgical techniques for isolated and hybrid femoral revascularization. (A) Primary femoral endarterectomy (FEA) with patch angioplasty utilizing an autologous ipsilateral great saphenous vein branch. (B) FEA performed with a bovine pericardium patch closure. (C–E) Utilization of the FEA site as a platform for hybrid revascularization: (C) Retrograde insertion of an introducer sheath for iliac artery (inflow) stenting. (D) Antegrade sheath placement for distal (outflow) revascularization; the sheath is secured to the skin with a stay suture to maintain stability during the endovascular procedure (dotted arrow). (E) Dual-direction access utilizing two introducer sheaths for simultaneous inflow and outflow revascularization (dotted arrows). Ligament = inguinal ligament; DFA = deep femoral artery; SFA = superficial femoral artery; CFA = common femoral artery.
Figure 1.
Surgical techniques for isolated and hybrid femoral revascularization. (A) Primary femoral endarterectomy (FEA) with patch angioplasty utilizing an autologous ipsilateral great saphenous vein branch. (B) FEA performed with a bovine pericardium patch closure. (C–E) Utilization of the FEA site as a platform for hybrid revascularization: (C) Retrograde insertion of an introducer sheath for iliac artery (inflow) stenting. (D) Antegrade sheath placement for distal (outflow) revascularization; the sheath is secured to the skin with a stay suture to maintain stability during the endovascular procedure (dotted arrow). (E) Dual-direction access utilizing two introducer sheaths for simultaneous inflow and outflow revascularization (dotted arrows). Ligament = inguinal ligament; DFA = deep femoral artery; SFA = superficial femoral artery; CFA = common femoral artery.
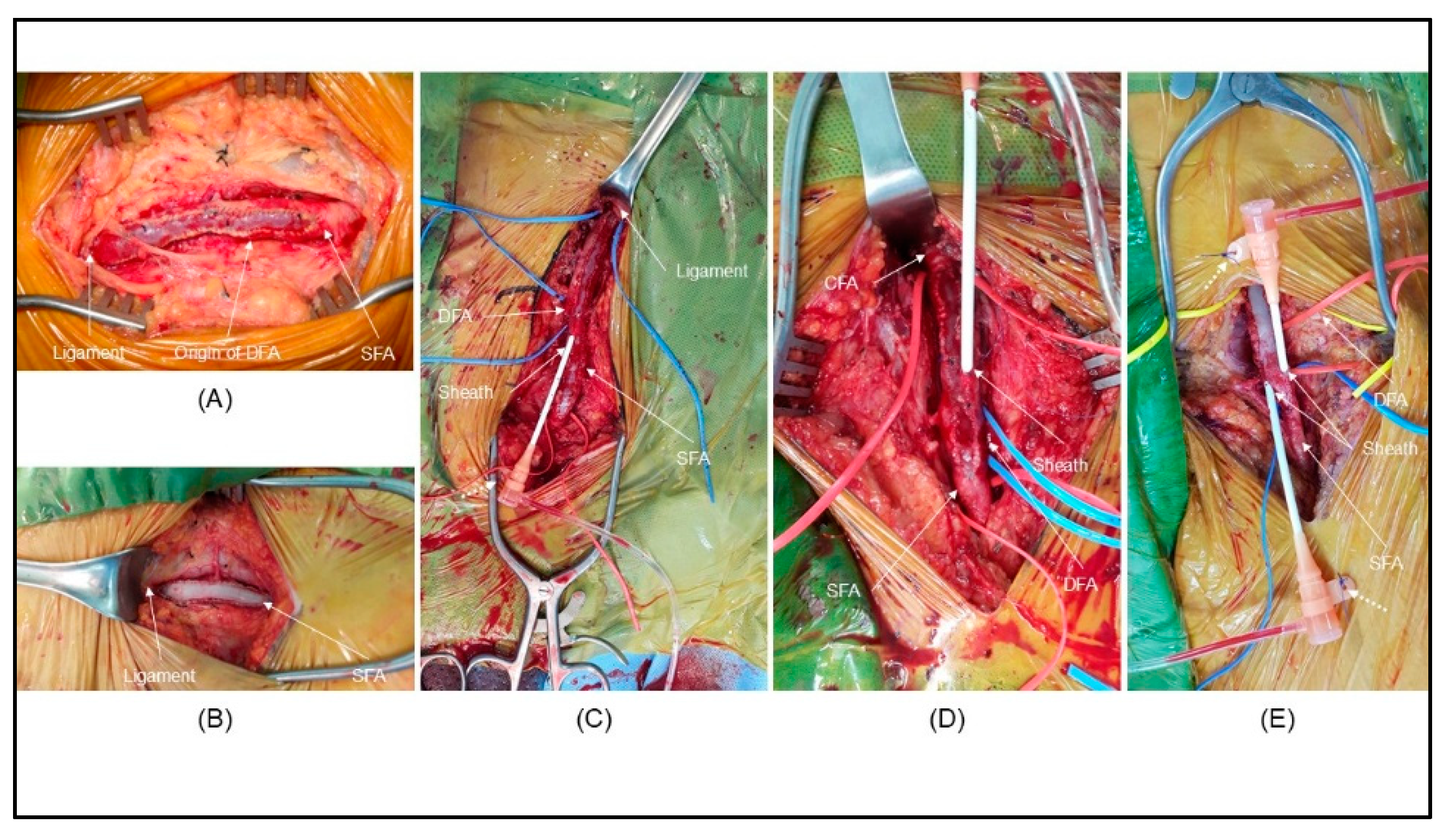
Figure 2.
Long-term primary patency outcomes over a 10-year follow-up period. Kaplan–Meier survival curves illustrate the 10-year primary patency rates for different arterial segments. (A) Primary patency at the femoral endarterectomy site shows high durability (94.4% at 10 years). (B) Primary patency of the inflow revascularization (iliac segment) facilitated by the FEA platform demonstrates high durability (94.4% at 10 years). (C) Primary patency of the outflow revascularization (femoropopliteal or infrapopliteal segments) up to 5 years (85.7%).
Figure 2.
Long-term primary patency outcomes over a 10-year follow-up period. Kaplan–Meier survival curves illustrate the 10-year primary patency rates for different arterial segments. (A) Primary patency at the femoral endarterectomy site shows high durability (94.4% at 10 years). (B) Primary patency of the inflow revascularization (iliac segment) facilitated by the FEA platform demonstrates high durability (94.4% at 10 years). (C) Primary patency of the outflow revascularization (femoropopliteal or infrapopliteal segments) up to 5 years (85.7%).
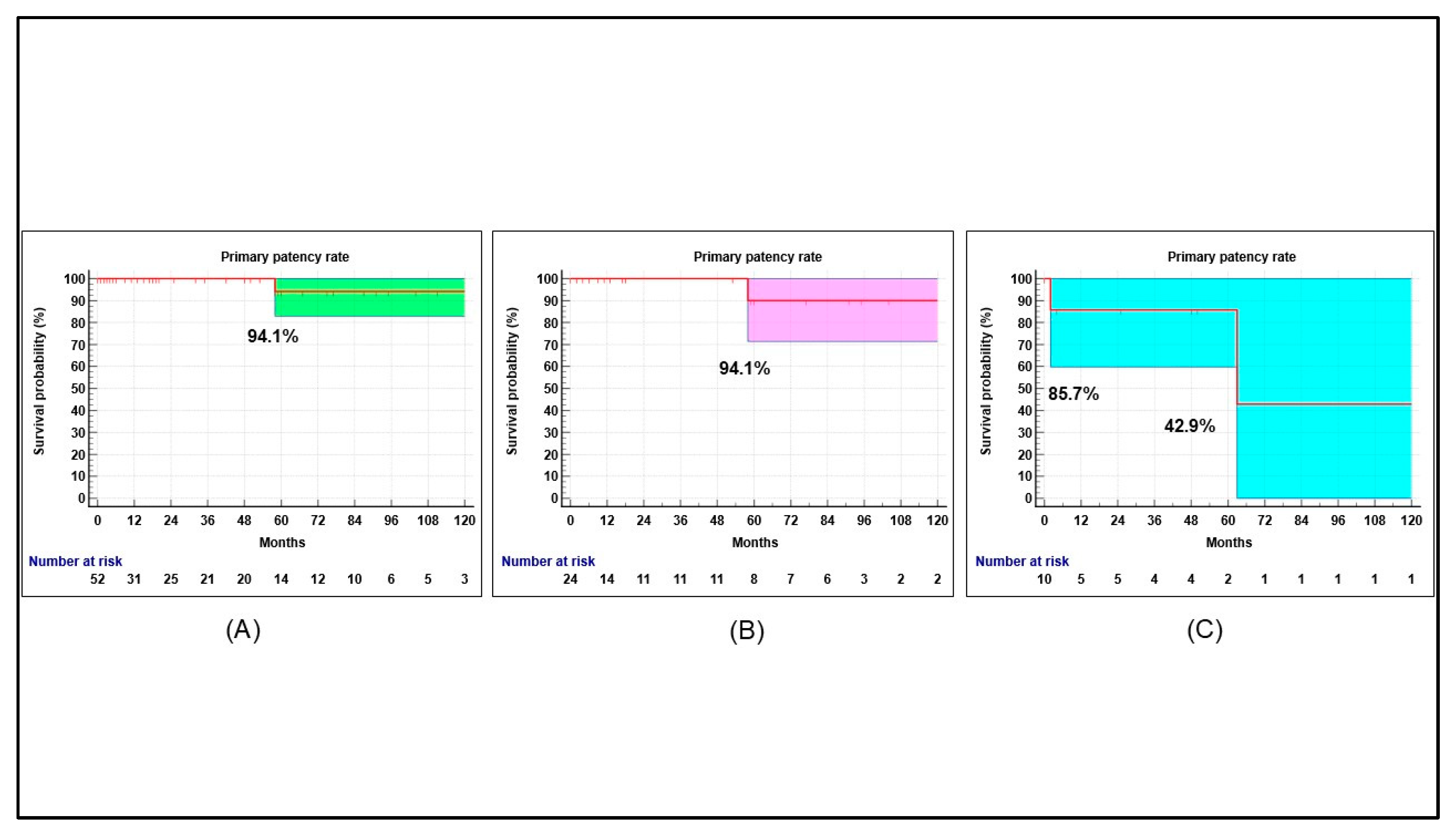
Figure 3.
Long-term patency outcomes following femoral endarterectomy Kaplan–Meier survival curves illustrate the 10-year primary patency rates, amputation free survival and overall survival comparing isolated FEA [Hybrid (–), blue line] with the hybrid platform approach [Hybrid (+), red line]. (A) Primary patency at the femoral endarterectomy site; no statistically significant difference was observed between groups (P = 0.460), demonstrating the high durability of the surgical reconstruction. (B and C) Amputation free survival and overall survival of two groups show no statistical significance. The results indicate that utilizing the common femoral artery as a platform for multi-level intervention does not compromise the long-term patency of the treated segments.
Figure 3.
Long-term patency outcomes following femoral endarterectomy Kaplan–Meier survival curves illustrate the 10-year primary patency rates, amputation free survival and overall survival comparing isolated FEA [Hybrid (–), blue line] with the hybrid platform approach [Hybrid (+), red line]. (A) Primary patency at the femoral endarterectomy site; no statistically significant difference was observed between groups (P = 0.460), demonstrating the high durability of the surgical reconstruction. (B and C) Amputation free survival and overall survival of two groups show no statistical significance. The results indicate that utilizing the common femoral artery as a platform for multi-level intervention does not compromise the long-term patency of the treated segments.
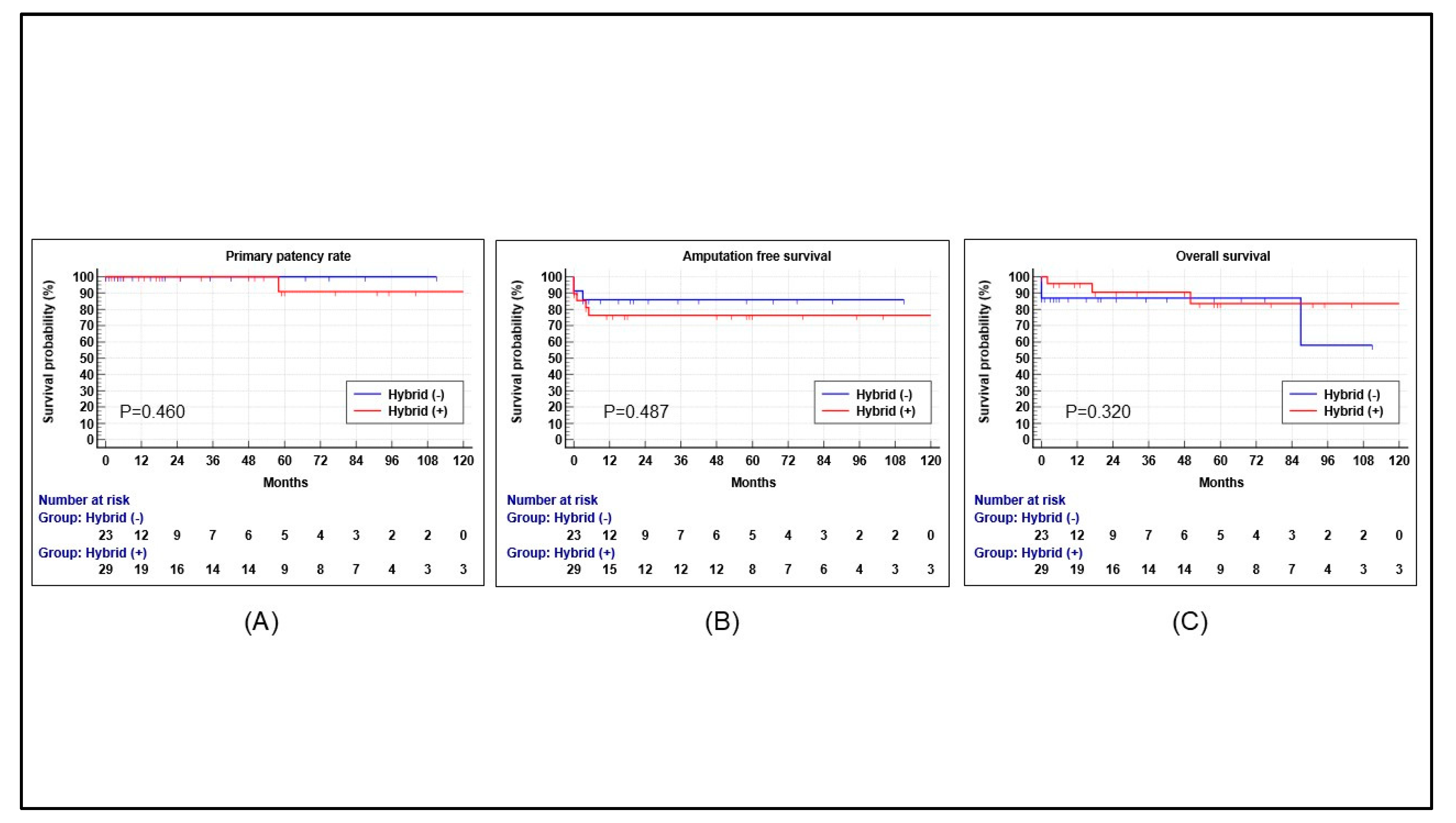

Table 1.
Baseline demographics.
| Factors | Total | Hybrid (-) | Hybrid (+) | P value |
|---|---|---|---|---|
| Number | 52 (100) | 23 (44.2) | 29 (55.8) | NA |
| Age, year | 70.7 ± 9.0 | 69.9 ± 8.1 | 71.2 ± 9.8 | 0.603 |
| Gender (male) | 43 (82.7) | 21 (91.3) | 22 (75.9) | 0.268 |
| Body mass index, kg/m2 | 22.7 ± 3.8 | 22.6 ± 4.2 | 22.8 ± 3.5 | 0.903 |
| Follow-up, months | 39.0 ± 42.5 | 30.2 ± 36.6 | 46.1 ± 8.6 | 0.183 |
| Risk factors Diabetes Hypertension Dyslipidemia Coronary artery disease Cerebrovascular disease ESRD on hemodialysis Smoking history |
30 (57.7) 35 (67.3) 4 (7.7) 9 (17.3) 14 (26.9) 3 (5.8) 22 (42.3) |
14 (60.9) 16 (69.6) 3 (13.0) 4 (17.4) 9 (39.1) 2 (8.7) 7 (30.4) |
16 (55.2) 19 (65.5) 1 (3.4) 5 (17.2) 5 (17.2) 1 (3.4) 15 (51.7) |
0.781 0.776 0.310 1.000 0.116 0.577 0.162 |
NA=not applicable; ESRD=end stage renal disease. Data are presented as numbers (%) or mean ± standard deviation.
Table 2.
Procedure details.
| Procedure | Hybrid (-) | Hybrid (+) | P value |
|---|---|---|---|
| Number | 23 (44.2) | 29 (55.8) | NA |
| Site (right : left) | 9 (39.1) : 14 (60.9) | 15 (51.7) : 14 (48.3) | 0.412 |
| Patch type Autologous GSV GSV branch Artificial graft Bovine pericardium PTFE |
13 (56.5) 7 (53.8) 6 (46.2) 10 (43.5) 9 (90.0) 1 (10.0) |
14 (48.3) 5 (35.7) 9 (64.3) 15 (51.7) 14 (93.3) 1 (6.7) |
0.588 0.449 NA NA 1.000 NA NA |
| Inflow revascularization1 | NA | 18 (62.1) | NA |
| Outflow revascularization2 | NA | 6 (20.7) | NA |
| Inflow and outflow revascularization3 | NA | 5 (17.2) | NA |
| Ankle-brachial index Preoperative Postoperative Postoperative-preoperative P value |
0.77 ± 0.19 1.04 ± 0.17 0.27 ± 0.13 < 0.001 |
0.52 ± 0.17 0.88 ± 0.18 0.36 ± 0.16 < 0.001 |
0.001 0.024 0.119 |
1 Inflow revascularization included all patients with iliac stenting. 2 Outflow revascularization included balloon angioplasty of the femoropopliteal artery (4), directional atherectomy of the femoropopliteal artery and balloon angioplasty of the tibial artery (1), and endovascular repair of the popliteal artery aneurysm (1). 3 Both inflow and outflow revascularization included iliac stenting combined with thrombectomy of the superficial femoral artery (2), directional atherectomy of the superficial femoral artery (1), balloon angioplasty of the superficial femoral artery (1), and balloon angioplasty of the tibial artery (1).
Table 3.
Complications.
| Grade | Definition | Hybrid (-) | Hybrid (+) | P value |
|---|---|---|---|---|
| Mild | Controlled without medication | n = 15 (65.2) 7 Tolerable wound pain 5 Tingling sensation of wound 3 Numbness |
n = 8 (27.6) 5 Tolerable wound pain 3 Tingling sensation of wound |
0.011 |
| Moderate | Managed with medication or an outpatient-based procedure after discharge | n = 1 (4.3) 1 Lymphedema (venoactive medication) |
n = 5 (17.2) 3 Wound pain (analgesics) 1 Lymphedema (venoactive medication) 1 Seroma (aspiration) |
0.210 |
| Severe | Need to re-admission or procedure | n = 1 (4.3) 1 Seroma + Infection (readmission + evacuation + antibiotics + VAC apply) |
n = 1 (3.4) 1 Seroma (readmission) |
1.000 |
Data are presented as numbers (%).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



