1. Introduction
Epiblepharon is a congenital eyelid anomaly characterized by a redundant horizontal skin fold and overriding of the orbicularis oculi muscle, causing the eyelashes to be directed upward or inward toward the cornea, resulting in the irritation of the cornea and conjunctiva.[
1,
2] This condition is commonly observed in East Asian children, including those in Korea, and typically involves the lower eyelids, particularly the medial portion.
Clinically, children with epiblepharon may exhibit symptoms including frequent eye rubbing, photophobia, tearing, and discharge.[
3] However, many cases are identified incidentally during routine examination, as both patients and parents may be unaware of any notable symptoms.
Epiblepharon often resolves spontaneously with facial bone growth progresses, and with reported incidence declining from approximately 46% in infants under 1 year of age to approximately 2% among adolescents aged 13–18 years.[
4] Due to this potential for spontaneous resolution, conservative management is typically attempted first for corneal irritation or epithelial erosion, with surgical correction typically required in cases with persistent symptoms or significant corneal erosions despite conservative therapy.
The etiology of epiblepharon is multifactorial, and the underlying mechanisms have yet to be fully elucidated. Proposed anatomical factors include overriding of the skin and orbicularis oculi muscle, lower insertion of the orbital septum, and a relative lack of vertical support for the pretarsal skin.[
5,
6] In epiblepharon, the eyelid margin remains in normal position without tarsal plate inversion, distinguishing it from entropion.
Recently, systemic factors influencing periocular soft tissue volume have been proposed as potential contributors to the development and persistence of epiblepharon. In particular, body mass index (BMI), a widely used indicator of obesity, has been associated with increased subcutaneous and orbital fat volume, which may alter eyelid contour and exert inward pressure on the eyelid margin.[
7,
8,
9,
10] Given the global rise in childhood obesity, understanding the relationship between BMI and eyelid malpositions has become increasingly clinically relevant.
From a clinical perspective, clarifying the association between obesity and epiblepharon is particularly meaningful, as obesity represents a potentially modifiable systemic factor. If increased body mass contributes to the persistence or severity of epiblepharon in certain pediatric populations, lifestyle modification and weight control could be considered for the natural course of the disease and potentially reduce or delay the need for surgical intervention. This consideration is especially important in pediatric patients, given that epiblepharon often improves spontaneously with growth and that avoiding unnecessary surgery during early childhood is a key clinical goal.
Despite this proposed association and its potential clinical implications, relatively few studies have systematically examined the relationship between BMI and epiblepharon. Therefore, in this study, we aimed to compare BMI between pediatric patients with epiblepharon and age-matched controls and to further investigate the correlation between BMI and skin fold height as an indicator of eyelid structural redundancy. This study seeks to provide a more comprehensive understanding of the potential role of obesity in the development and persistence of epiblepharon and to highlight its clinical relevance in the evaluation and management of affected children.
2. Materials and Methods
This retrospective comparative study was conducted at Pusan National University Yangsan Hospital, Republic of Korea. The medical records of 100 patients aged 3 -13 years who visited the Pediatric Ophthalmologic Clinic at Pusan National University Yangsan Hospital between January 2018 and September 2019 were reviewed. Institutional Review Board approval was obtained (IRB no. 55-2026-022, issued on 27 January 2026) and study was conducted adhering to the Declaration of Helsinki. Epiblepharon was defined as an extra fold of skin pushing the eyelashes upward while maintaining a normal eyelid margin. The study included a hundred patients (54 boys, 46 girls) who underwent surgical correction and were assigned to the epiblepharon group, with a control group consisting of 100 age-matched children (42 boys, 58 girls) without epiblepharon, recruited from pediatric ophthalmology clinics over the same period. Uncooperative patients, those who had incomplete medical records, or individuals with other underlying diseases (e.g., trichiasis or entropion) unrelated to epiblepharon were excluded.
Height and weight were obtained from medical records at the time of preoperative evaluation. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (kg/m²) and rounded to one decimal place. Lower eyelid skin fold height was assessed using standardized preoperative frontal photographs obtained in primary gaze. Measurements were assessed according to Khwarg’s classification, the severity of epiblepharon was determined by the position of the highest point of skin fold. According to Khwarg’s classification system, patients whose skin fold was located below the lower eyelid margin were classified as Class I. Those with a skin fold positioned at or just below the lower eyelid margin were assigned to Class II. Patients in whom the skin fold extended above the eyelid margin and concealed less than one-third of the medial eyelid were categorized as Class III, whereas those whose skin fold lay above the eyelid margin and concealed more than one-third of the medial eyelid were classified as Class IV [
11].
Patients were stratified into age subgroups (3–4, 5–6, 7–8, 9–10, and 11–13 years) and analyzed separately by sex to evaluate age- and sex- dependent differences in BMI and eyelid morphology.
All patients underwent standard cilia rotation suture techniques. A crescentic resection of the skin and orbicularis muscle was performed 1–2 mm below the lower eyelid margin, followed by three to four non-absorbable rotational sutures between the pretarsal orbicularis oculi muscle and the tarsus. The skin was closed using continuous sutures of an absorbable material
All analyses were conducted by SPSS Statistics 25 (IBM, Corp, Armonk, NY, USA) software. For comparisons of BMI between epiblepharon group and control group, continuous variables were analyzed using independent t-tests. To find correlations between BMI and skin fold height, data was analyzed using Spearman correlation. A p-value <0.05 was considered statistically significant.
3. Results
3.1. Patient Characteristics
Of 100 children with epiblepharon, 54 were boys and 46 were girls. The mean age of children with epiblepharon was 6.38 ± 2.46 years. 100 children who were assigned to the control group, consisted of 42 boys and 58 girls. Mean age of control group was 6.02 ± 2.64 years. There were no significant differences in age or sex distribution between groups. (p>0.05) (
Table 1). Also, there were no significant differences between BMI between 2 groups.
3.2. Correlation Between BMI and Epiblepharon
Analysis of the correlation between the occurrence of epiblepharon and BMI demonstrated no significant correlation in girls (
Table 2). However, boys with epiblepharon in the 7–8 and 9–10 age groups exhibited significantly higher BMI compared with their counterparts without epiblepharon (p < 0.05). Interestingly, boys aged 3–4 years with epiblepharon showed significantly lower BMI than age-matched controls (p < 0.05).
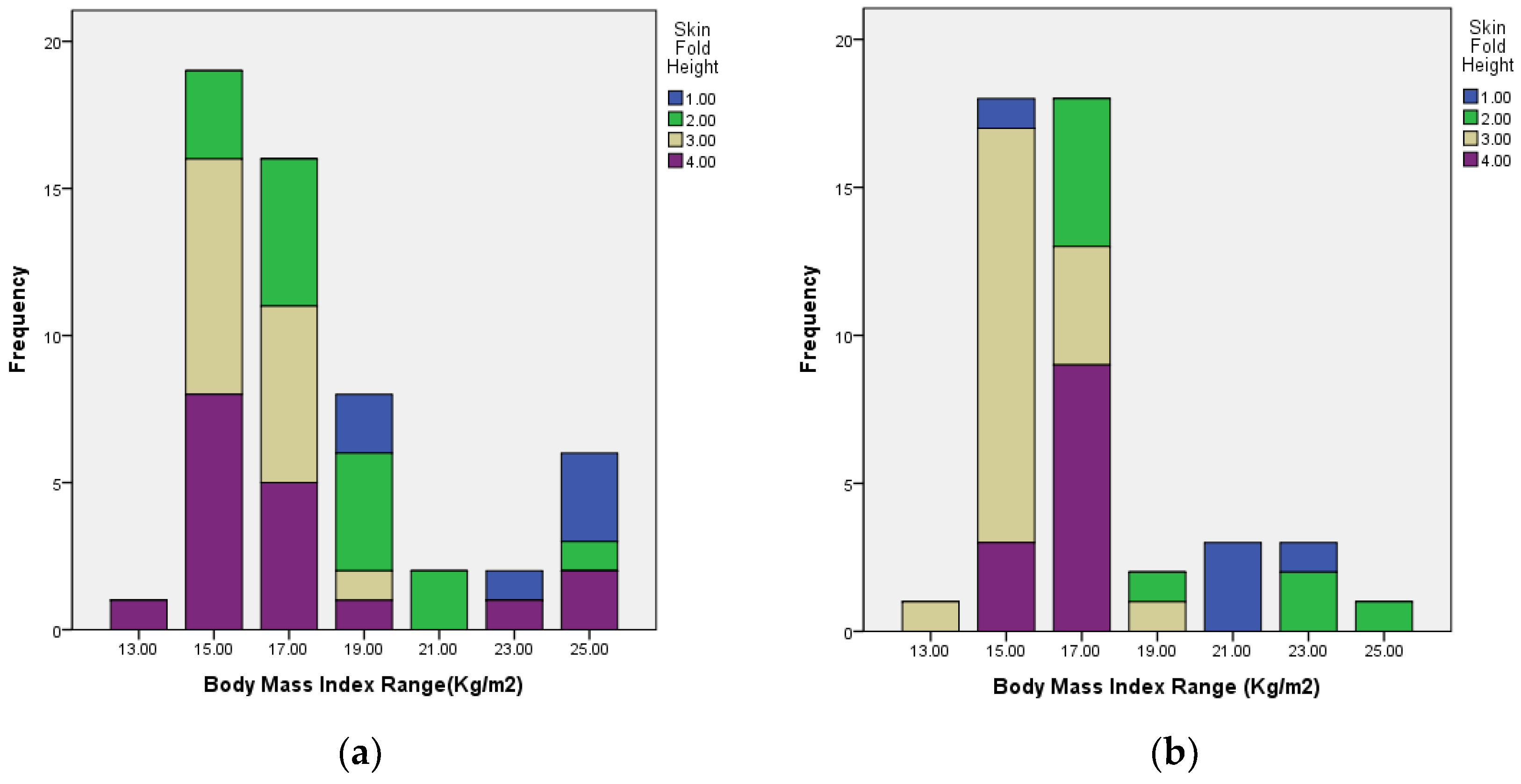
3.3. Correlation Between BMI and Skin Fold Height
The skinfold height classifications according to BMI categories are demonstrated in
Table 3 and
Figure 1. Among patients with epiblepharon, a higher BMI was significantly associated with a lower skinfold height class (p < 0.05), suggesting that obese children tend to have less prominent skinfolds and greater orbicularis muscle redundancy (
Table 4). This correlation between BMI and skinfold height was significant in both subgroups (p < 0.05).
4. Discussion
Epiblepharon is a common congenital eyelid anomaly in East Asian children, predominantly affecting the lower eyelids. Although epiblepharon may remain asymptomatic in many cases, some patients experience foreign body sensations, photophobia, tearing, and discharge. In severe cases, corneal involvement such as keratopathy can occur, requiring surgical correction[
3,
4].
We investigated the relationship between BMI and epiblepharon by comparing children with moderate-to-severe disease who underwent surgical correction to age-matched controls without epiblepharon. This study demonstrated an age- and sex-dependent association between BMI and epiblepharon in pediatric patients, with significantly higher BMI observed among boys aged 7–10 years with epiblepharon suggesting that eyelid anomalies may be influenced not only by genetic and anatomical factors, but also by systemic conditions such as obesity. These findings suggest that systemic factors influencing soft tissue volume may contribute to the persistence or severity of epiblepharon during specific stages of growth.
Previous studies have reported similar associations between obesity and epiblepharon, although the affected age ranges varied [
7,
8,
9,
10]. Ahn et al. reported an association between obesity and epiblepharon in 223 girls aged 12–15 years diagnosed with epiblepharon[
7]. Hayasaka et al. identified that Japanese children aged 6–11 years with epiblepharon had a significantly higher mean BMI than age-matched controls; in a consecutive study, 44% of children with a high BMI were diagnosed with epiblepharon[
8,
9]. Similarly, Yan et al. reported that Chinese children with epiblepharon had a higher mean BMI across all age groups than that noted in controls, although a statistically significant difference was only observed in boys aged 4–6 years[
10]. Additionally, Takahashi et al. analyzed 509 patients with congenital lower eyelid epiblepharon and found that higher BMI showed a trend toward increased risk of severe corneal involvement [
13], suggesting that elevated BMI may not only be associated with the presence of epiblepharon but also with its clinical severity, although the association did not reach statistical significance in their logistic regression model. Furthermore, Wang et al. reported in a large retrospective case-control study that the median BMI was significantly higher in children with epiblepharon than in age- and sex-matched controls, and that overweight boys aged 4–9 years and adolescent girls aged 13–18 years had a significantly increased risk of epiblepharon, highlighting a sex-specific effect of obesity on disease risk [
14]. Despite minor variations in age and sex distribution across studies, the prevailing view is that increased subcutaneous and orbicularis muscle tissues in the malar and lower eyelid regions can exert inward pressure on the eyelid margin, thereby contributing to the development or persistence of epiblepharon in children with a higher BMI.
However, in our study, boys aged 3–4 years with epiblepharon had a significantly lower BMI than those without epiblepharon, suggesting that structural and developmental factors may play a more dominant role than obesity in this early stage of growth. Further longitudinal studies are required to elucidate the age-dependent relationship between changes in BMI and eyelid morphology.
A key finding of this study is the significant negative correlation between BMI and skin fold height. Higher BMI was associated with less prominent skin folds, suggesting that orbicularis oculi muscle and subcutaneous tissue hypertrophy, rather than skin redundancy alone. The pathophysiology of epiblepharon in obese children may be related with soft tissue hypertrophy than to skin redundancy. Future studies using dynamic imaging modalities, such as ultrasound or magnetic resonance imaging, could further elucidate the soft tissue changes and anatomical mechanisms underlying epiblepharon in older children.
Clinically, these findings suggest that BMI should be considered in the evaluation and management of pediatric epiblepharon. High BMI may contribute to the persistence or recurrence of the condition, highlighting the importance of targeting the redundant orbicularis muscle during surgical correction rather than performing skin excision alone in obese children. Lifestyle modifications and weight management may also aid in reducing disease severity and recurrence risk in this population.
This study had several limitations. First, this was a retrospective study conducted at a single tertiary center with a relatively small sample size. Second, BMI was employed as the sole indicator of obesity, without direct assessment of fat distribution (e.g., orbital fat volume). Third, the long-term relationship between the BMI and surgical outcomes could not be analyzed. Nevertheless, this study provides valuable clinical insights, being one of the few to systematically explore the association between obesity and epiblepharon, underscoring the significance of considering systemic factors in the pathophysiology of pediatric eyelid anomalies.
Author Contributions
Conceptualization, J.A.; methodology, J.A.; formal analysis, J.A.; investigation, J.A.; resources, J.A.; data curation, J.A.; writing—original draft preparation, H.Y.; writing—review and editing, H.Y.; visualization, H.Y.; supervision, J.A.; project administration, J.A.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Pusan National University Yangsan Hospital. (IRB no. 55-2026-022, issued on 27 January 2026).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author. The data are not publicly available due to privacy and ethical re-strictions.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Levitt J.M.; Epiblepharon and congenital entropion. Am J Ophthalmol 1957, 44(1), 112-113. [CrossRef]
- Johnson C.C.; Epiblepharon. Am J Ophthalmol 1968, 66(6), 1172-1175. [CrossRef]
- Kim J.S., Jin S.W., Hur M.C., Yoon H.K., Ryu W.Y., Jeong W.J., Ahn H.B.; The clinical characteristics and surgical outcomes of epiblepharon in Korean children: a 9-year experience. J Ophthalmol 2014,e156501. [CrossRef]
- Noda S., Hayasaka S., Stowaway T.; Epiblepharon with inverted eyelashes in Japanese children. I. Incidence and symptoms. Br J Ophthalmol 1989, 73(2), 126-127. [CrossRef]
- Lim W.K., Rajendran K., Choo C.T.; Microscopic anatomy of the lower eyelid in Asians. Ophthalmic Plast Reconstr Surg 2004, 20, 207-211. [CrossRef]
- Carter S.R., Seiff S.R., Grant E., Vigneron D.B.; The Asian lower eyelid: a comparative anatomic study using high-resolution magnetic resonance imaging. Ophthalmic Plast Reconstr Surg 1998, 14, 227-234. [CrossRef]
- Ahn H.B., Seo J.W., Yoo J.H., Jeong W.J., Park W.C., Rho S.H.; Epiblepharon related to high body mass index in Korean children. J Pediatr Ophthalmol Strabismus 2011, 48, 57-60. [CrossRef]
- Hayasaka Y., Hayasaka S.; Epiblepharon with inverted eyelashes and high body mass index in Japanese children. J Pediatr Ophthalmol Strabismus 2005, 42, 300-303. [CrossRef]
- Hayasaka Y., Hayasaka S., Matsukura H.; Ocular findings Japanese children with nephrotic syndrome receiving prolonged corticosteroid therapy. Ophthalmologica 2006, 220, 181–185. [CrossRef]
- Yan Y., Chen T., Wei W., Li D.; Epiblepharon in Chinese children: relationship with body mass index and surgical treatment. J Am Assoc Pediatr Ophthalmol Strabismus 2016, 20, 148-152. [CrossRef]
- Khwarg SI, Choung HK. Epiblepharon of the lower eyelid: technique of surgical repair and quantification of excision according to the skin fold height. [CrossRef]
- Seo J.W., Kang S., Ahn C., Esmaeli B., Sa H.S.; Non-incisional eyelid everting suture technique for treating lower lid epiblepharon. Br J Ophthalmol 2018, 102, 1504-1509. [CrossRef]
- Takahashi Y, Kono S, Vaidya A, Yokoyama T, Kakizaki H. Severe corneal involvement secondary to congenital lower eyelid epiblepharon. Graefes Arch Clin Exp Ophthalmol 2023; 261(5):1451-1457. [CrossRef]
- Wang JJ, Lai CH, Kuo TY, Lin MH, Yang YH, Chen CY. Sex-Specific Effect of Obesity on Epiblepharon in Different Age Groups: A Case-Control Study. Int J Environ Res Public Health 2022; 19(19):12839. [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).