
Submitted:
30 January 2026
Posted:
02 February 2026
You are already at the latest version
Abstract
Background/Objectives: Full-arch zirconia prostheses for mandibular All-on-4 rehabilitations are provided as screw-retained monolithic zirconia or as a zirconia suprastructure luted to a CAD/CAM titanium bar. Because zirconia is a brittle, flaw-sensitive ceramic, design assessment should incorporate stress-field–weighted fracture risk. This in-silico study compared zirconia tensile stress and Weibull-based reliability between monolithic (Zr-Mono) and titanium-bar–supported zirconia (Zr-TiBar) designs. Methods: A standardized 3D edentulous mandibular All-on-4 model (four 4.3×11.5-mm implants; posterior implants tilted 30°) with multi-unit abutments and Ti-bases was analyzed using linear static finite element analysis. Posterior unilateral loads were applied to the first molar (300 N axial; 300 N at 45° oblique). Outcomes were maximum principal tensile stress in zirconia (S1max), total prosthesis deformation, and Weibull-predicted probability of zirconia fracture (m = 7.41; σ0 = 576.5 MPa) derived from the tensile S1 field. Results: Under axial loading, S1max was similar (Zr-Mono 277.09 MPa; Zr-TiBar 277.13 MPa). Under oblique loading, S1max was lower for Zr-TiBar (226.94 MPa) than for Zr-Mono (233.82 MPa). Deformation was <0.07 mm and lower for Zr-TiBar (0.0607 mm axial; 0.0589 mm oblique) than for Zr-Mono (0.0635 mm axial; 0.0660 mm oblique). The Weibull-predicted probability of fracture was very low: axial 1.309×10⁻⁶ (Zr-Mono) vs 1.473×10⁻⁶ (Zr-TiBar); oblique 1.589×10⁻⁷ vs 1.790×10⁻⁷. Conclusions: Both designs showed comparably low Weibull-predicted fracture probability under single 300 N posterior loads. Titanium-bar support reduced deformation and modestly reduced peak tensile stress under oblique loading, but did not reduce the predicted fracture probability relative to monolithic zirconia.
Keywords:
All-on-4
; mandibular full-arch prosthesis
; monolithic zirconia
; CAD/CAM titanium bar
; finite element analysis
; Weibull analysis
; probability of fracture
; tensile stress
; implant-supported fixed prosthesis
; zirconia reliability
1. Introduction
Full-arch implant rehabilitation is increasingly delivered through digital workflows and CAD/CAM fabrication, with growing interest in high-strength ceramic reconstructions that reduce veneer-related technical complications and streamline maintenance. Monolithic zirconia has therefore become a frequently selected material for implant-supported complete-arch fixed dental prostheses because it offers high strength, favorable wear characteristics, and improved esthetics with newer translucent multilayer formulations. Nevertheless, technical events such as fracture, chipping (when veneering is present), decementation in multi-part concepts, and screw-related complications remain clinically relevant, and outcomes are influenced by prosthesis design, support configuration, and functional loading patterns. Large clinical datasets and reviews indicate generally favorable short- to mid-term performance for complete-arch zirconia prostheses, but also emphasize heterogeneity in designs and complication definitions across studies [1,2]. To optimize the implant–prosthesis interface and retrievability, contemporary workflows commonly employ multi-unit abutments (MUAs) together with titanium-based interfaces (Ti-bases) to create a titanium–titanium screw interface and a luted zirconia suprastructure. Beyond interface standardization, titanium bar–supported zirconia concepts have also gained attention, in which a CAD/CAM titanium bar functions as a rigid substructure and the zirconia component serves primarily as an esthetic and occlusal superstructure. The biomechanical intent of such a bar is not to “strengthen” zirconia per se, but to modify system-level stiffness and bending behavior, potentially reducing tensile stress peaks in the ceramic and redistributing loads within the implant–abutment–prosthesis complex.
In the edentulous mandible, the All-on-4 concept is widely used and supported by long-term clinical evidence [3,4,5]. Although implant survival can be high, the prosthetic superstructure is a principal determinant of load transfer and mechanical risk, particularly when brittle ceramics are used [6,7,8]. Unlike ductile metals, zirconia behaves as a flaw-sensitive brittle ceramic; catastrophic fracture typically initiates under tensile principal stress and propagates rapidly once a critical defect is activated [9,10,11]. Consequently, reporting a single peak stress value may be insufficient for comparing ceramic designs, because fracture propensity depends not only on the maximum tensile stress but also on the stressed tensile volume over which a critical flaw might exist.
Weibull weakest-link statistics provide a widely accepted framework for describing brittle fracture reliability by linking a spatial stress field to failure probability through material-specific parameters (Weibull modulus, m, and characteristic strength, σ₀). When combined with finite element analysis (FEA), Weibull post-processing can translate the computed maximum principal tensile stress field (S1) into probabilistic outcomes such as reliability (R) and probability of fracture (Pf), thereby improving clinical interpretability when nominal peak stresses are similar but stress distributions differ [12].
From a design perspective, two zirconia-based strategies are commonly discussed: (i) a screw-retained monolithic zirconia prosthesis, and (ii) a multi-component concept in which an esthetic zirconia suprastructure is luted to a screw-retained CAD/CAM titanium bar. The latter approach is intended to enhance passivity, retrievability, and repair logistics while preserving zirconia’s esthetic and wear advantages. However, it remains debated whether titanium-bar support consistently reduces zirconia fracture risk. While a stiffer framework may reduce global flexure and peak tensile stresses, it can also modify the stressed tensile volume and stress distribution, and some clinical advantages may primarily reflect improved fit, retrievability, and repair logistics rather than a direct reduction in ceramic probability of fracture. Recent clinical reports indicate that zirconia restorations luted to titanium bars can be feasible in the short term, yet the mechanical implications of this stress-transfer pathway—particularly in terms of tensile stress distribution and probabilistic fracture risk—remain a critical question for design selection [13,14]. To date, the comparative stress-field–weighted fracture reliability of monolithic versus titanium-bar–supported zirconia full-arch designs in an All-on-4 mandibular configuration remains insufficiently quantified under standardized posterior axial and oblique loading.
Accordingly, the aim of this in-silico FEA study was to compare two zirconia-based complete-arch prosthetic designs in an edentulous mandibular All-on-4 configuration—monolithic zirconia (Zr-Mono) and titanium-bar–supported zirconia (Zr-TiBar; zirconia suprastructure luted to a screw-retained titanium bar)—under 300 N axial and 45° oblique posterior loading. Primary outcomes were zirconia maximum principal tensile stress (S1) and Weibull-derived fracture metrics (reliability and probability of fracture), with total prosthesis deformation reported as a secondary clinically interpretable outcome. Therefore, Weibull post-processing of the FEA stress field may better discriminate designs than peak stress alone. The null hypothesis was that the two designs would not differ in S1-derived Weibull outcomes under either loading condition. In brief, both designs exhibited very low Weibull-predicted fracture probability under the modeled loads; titanium-bar support reduced deformation and modestly reduced oblique-load peak tensile stress but did not reduce the predicted fracture probability relative to monolithic zirconia.
2. Materials and Methods
Study Design and Reporting Framework
This in-silico comparative study used three-dimensional linear static FEA to evaluate zirconia tensile stress, Weibull-based reliability, and prosthesis deformation in an edentulous mandibular All-on-4 rehabilitation restored with two prosthetic designs: (i) screw-retained monolithic zirconia (Zr-Mono) and (ii) a monolithic zirconia suprastructure luted to a screw-retained CAD/CAM titanium bar (Zr-TiBar). Reporting was structured according to the RIFEM framework to ensure transparent documentation of geometry, meshing, boundary conditions, contact definitions, loading, and verification considerations [15].
Finite Element Mandible Model Design
A 3D digital model of a fully edentulous mandible was created based on a Frasaco acrylic phantom jaw (Frasaco GmbH, Tettnang, Germany) and constructed in CAD software (SolidWorks 2024, Dassault Systèmes, France). The mandible included anatomically representative compartments of cortical bone (uniform 2-mm shell thickness) and cancellous bone, and a 3-mm soft-tissue layer. The overall morphology corresponded to a moderately resorbed edentulous ridge consistent with Cawood and Howell Class V, characterized by a rounded/flattened ridge contour [16]. The same mandibular geometry was used for both prosthetic designs to isolate the effect of superstructure architecture.
To reduce geometric asymmetry as a confounder, the final mandible geometry was mirrored across the midline and refined to obtain a standardized, proportionally symmetric edentulous model. The model was intentionally generated in CAD and not derived from CT/CBCT/MRI segmentation, and is therefore intended for controlled comparative biomechanics rather than patient-specific prediction.
Implant Configuration (Mandibular All-on-4) and Components
All implants and restorative components were from Nobel Biocare (Gothenburg, Sweden). Four titanium (Ti) bone-level implants of identical dimensions (4.3-mm diameter × 11.5-mm length) were placed in an All-on-4 configuration, with two anterior implants positioned axially and two posterior implants tilted distally (30°) to increase anteroposterior spread. Multi-unit abutments and titanium bases were connected to each implant. Implant positions, abutments, screw-access geometry, and occlusal anatomy were kept identical between models to isolate the effect of superstructure architecture.
Prosthetic Designs
Two prosthetic designs were evaluated: Zr-Mono, a screw-retained full-arch monolithic zirconia prosthesis, and Zr-TiBar, a titanium-bar–supported zirconia design in which a CAD/CAM titanium bar was screw-retained to the abutments and a monolithic zirconia suprastructure was luted to the bar (Figure 1). Except for the presence of the titanium bar and the luted zirconia–titanium interface, all other features were matched across the two designs. To isolate the effect of superstructure architecture, both designs were modeled on MUAs with Ti-base–luted interfaces.
Material Properties
All components were assumed homogeneous, isotropic, and linearly elastic, consistent with common comparative dental FEA practice. Zirconia elastic behavior was assigned using values widely reported for dental zirconia systems [17]. The complete set of elastic moduli and Poisson’s ratios for each component were reported in a dedicated table (Table 1) to ensure reproducibility [18].
Contacts and Boundary Conditions
The bone–implant interface was modeled as bonded to represent idealized complete osseointegration. Titanium–titanium interfaces within the implant and components complex were modeled as frictional contacts (μ = 0.3) using literature-supported coefficients for implant joint modeling [19].
In the Zr-TiBar model, the zirconia–titanium bar interface was modeled as bonded to represent a fully luted connection. The interfaces between the prosthesis/bar and the multi-unit abutment titanium bases were also modeled as bonded, consistent with the intended rigid clinical connections.
To prevent rigid-body motion, the mandibular support regions (mandibular base and condylar constraints as defined in the model) were constrained in all degrees of freedom and applied identically to both designs.
Mesh Strategy and Solution
The assemblies were imported into ANSYS Workbench/Mechanical (ANSYS Inc., USA; ANSYS Mechanical APDL (MAPDL) 2024 R2 solver environment) and discretized using tetrahedral elements, with local refinement in regions expected to show high stress gradients (prosthesis connectors/screw-access regions and implant–abutment interfaces).
Mesh convergence was evaluated using three progressively refined meshes with nominal element sizes of 0.9 mm, 0.7 mm, and 0.5 mm. The primary convergence metric was the peak zirconia maximum principal tensile stress (S1) in the prosthesis. Because the maximum difference in peak S1 between successive meshes was <5%, the 0.5-mm mesh was selected for all final analyses (690,331 elements and 1,218,804 nodes).
Loading Scenarios
Two unilateral posterior loading conditions were simulated. Loads were applied to the central fossa of the first molar on the working side over an approximately 1-mm² area: an axial load of 300 N applied vertically to the posterior occlusal contact region, and an oblique load of 300 N applied at a 45° angle to the occlusal plane at the same contact region [20,21].
Outcome Measures
Consistent with the study’s emphasis on fracture-relevant zirconia mechanics, three main endpoints were extracted: (1) the maximum principal tensile stress in zirconia (S1), including its distribution and peak value within the zirconia prosthesis; (2) Weibull-based zirconia reliability, captured through the Weibull stress-integration term and corresponding reliability outputs (Weibull stress-integration term IntW, reference volume V0, reliability R, and probability of fracture Pf); and (3) overall prosthesis compliance, summarized as the maximum total deformation (mm) to provide a single clinically interpretable deformation metric.
For consistency with the Weibull post-processing, the reported peak zirconia maximum principal tensile stress (S1max) was extracted as the maximum elemental (unaveraged) S1 value over the zirconia prosthesis from MAPDL element tables. Nodal maxima displayed in the Mechanical GUI may be higher due to stress extrapolation/averaging and local numerical singularities at sharp edges or contact transitions; therefore, nodal peaks were used for visualization only and not for Weibull integration.
Weibull Post-Processing (Stress-Field to Probability)
Weibull reliability was computed from the element-wise zirconia tensile stress field using a weakest-link formulation. Only tensile principal stresses were included, consistent with brittle fracture initiation under tensile opening-mode conditions. The following relationship was used:
where σ1 is the maximum principal tensile stress (FEA-derived S1), m is the Weibull modulus, and σ0 is the characteristic strength. Weibull parameters were taken from published mechanical testing of multilayer translucent zirconia under glazing (glazed once) conditions, matching the restorative scenario. The parameter set used for the zirconia prosthesis was m=7.41 and σ0=576.5 MPa [22].
Practically, Weibull integration was performed in MAPDL by extracting element S1 and element volume, accumulating the integral over the zirconia domain, and computing R and Pf. To stabilize interpretation for design-to-design comparison within the same geometric scale, the reference volume V0 was set to the total tensile-stressed zirconia volume (Vtens), yielding the reported IntW/V0, R, and Pf outputs used in the Results. Setting V0=Vtens standardizes the reference volume for within-study comparisons; absolute Pf values should be interpreted within this modeling assumption.
Data and Code Availability
MAPDL post-processing scripts are available from the corresponding author upon reasonable request.
Preregistration
This computational study was not preregistered.
Ethics Statement
This was a purely computational study with no human participants, patient data, or animal experimentation; therefore, institutional ethics approval was not required.
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.1. Maximum Principal Tensile Stress in Zirconia (S1)
Under 300 N axial loading, the peak maximum principal tensile stress (S1max) in the zirconia prosthesis was essentially identical between designs (Zr-Mono: 277.09 MPa; Zr-TiBar: 277.13 MPa). Under 300 N oblique loading, S1max decreased in both models (Zr-Mono: 233.82 MPa; Zr-TiBar: 226.94 MPa), with Zr-TiBar showing a modestly lower peak value (Δ = 6.88 MPa) (Table 2).
Figure 2 shows the nodal peak maximum principal stress distribution in the zirconia prosthesis under 300 N axial and oblique loads for the Zr-Mono and Zr-TiBar designs. Peak tensile stresses localized at the posterior connector/screw-access region on the loaded side. Reported S1max values refer to element (unaveraged) maxima extracted from MAPDL; nodal stress plots are provided for visualization only (Figure 2).
3.2. Total Prosthesis Deformation
Total deformation values were small (<0.07 mm) for both designs under both loading directions. Under axial loading, total deformation was 0.0635 mm for Zr-Mono and 0.0607 mm for Zr-TiBar. Under oblique loading, total deformation was 0.0660 mm for Zr-Mono and 0.0589 mm for Zr-TiBar (Table 2; Figure 3).
3.3. Weibull-Based Zirconia Reliability (R) and Fracture Probability (Pf)
Weibull post-processing yielded very low predicted probabilities of zirconia fracture for both designs under both loading conditions (Table 3; Figure 4). Under axial loading, the probability of fracture was 1.309×10⁻⁶ for Zr-Mono (R = 0.999998691) and 1.473×10⁻⁶ for Zr-TiBar (R = 0.999998527). Under oblique loading, the probability of fracture decreased to 1.589×10⁻⁷ for Zr-Mono (R = 0.999999841) and 1.790×10⁻⁷ for Zr-TiBar (R = 0.999999821). Across loading directions, Zr-Mono showed a slightly lower probability of fracture than Zr-TiBar (≈11% under both axial and oblique loading). The stress-integration term (IntW) was similar between designs within each loading case, whereas the tensile reference volume (V0 = Vtens, mm³) was larger in Zr-Mono than in Zr-TiBar, resulting in a lower IntW/V0 and correspondingly lower predicted fracture probability for Zr-Mono.
4. Discussion
This in-silico study compared two full-arch zirconia prosthetic architectures for a mandibular All-on-4 configuration—(i) a screw-retained monolithic zirconia prosthesis (Zr-Mono) and (ii) a titanium-bar–supported zirconia suprastructure (Zr-TiBar)—using zirconia maximum principal tensile stress (S1), Weibull-derived probabilistic fracture metrics, and total prosthesis deformation as primary outcomes. Overall, the results provided limited support for an architecture-driven reduction in Weibull-predicted fracture probability: axial peak S1 was essentially identical between designs, and although Zr-TiBar modestly reduced oblique-load peak S1 and decreased total deformation, the Weibull-predicted probability of fracture (Pf) remained very low and differed only slightly between designs under the evaluated loading conditions.
The present results should be interpreted in light of the fundamental mechanical distinction between the two prosthetic concepts. Although both reconstructions employ zirconia as the restorative material, the Zr-TiBar configuration introduces a dedicated metallic substructure that can alter global stiffness and bending behavior of the full-arch assembly, thereby influencing the magnitude and distribution of tensile stresses within the ceramic component and the load transfer pathways through the implant–abutment–prosthesis complex. Importantly, to isolate the effect of bar reinforcement from confounding interface variables, both models were standardized by using MUAs and zirconia superstructures bonded to Ti-bases, reflecting a common clinical strategy that provides a titanium–titanium screw interface while maintaining a ceramic suprastructure. This modeling choice enables a controlled comparison focused on the presence or absence of a titanium bar rather than differences in connection geometry or screw-interface material pairing. Nevertheless, passive fit in full-arch reconstructions remains multifactorial; thus, the current analysis represents an idealized condition and does not explicitly model manufacturing tolerances, luting variability, or misfit scenarios that may occur clinically. Accordingly, the findings should be considered as design-level biomechanical tendencies under standardized seating assumptions rather than as direct predictions of complication rates.
Interpretation of Stress and Deformation Findings
Under 300 N axial loading, zirconia peak S1 values were nearly identical between designs (277.09 MPa for Zr-Mono vs 277.13 MPa for Zr-TiBar), indicating that, within the boundary conditions and idealized interfaces used, the load path into the zirconia superstructure generated comparable maximum tensile hotspots. Under 300 N oblique loading, peak zirconia S1 decreased relative to axial loading and was modestly lower in the Zr-TiBar design (233.82 MPa for Zr-Mono vs 226.94 MPa for Zr-TiBar). This pattern suggests that the bar-supported architecture can slightly redistribute tensile stresses within the zirconia suprastructure under angled force vectors, plausibly by increasing global stiffness and modifying bending components of the superstructure response.
Total deformation supported this interpretation. Zr-TiBar exhibited lower prosthesis deformation under both loading directions, particularly under oblique loading (0.0589 mm vs 0.0660 mm), consistent with the well-established principle that adding a high-modulus substructure (titanium framework) can reduce overall compliance of a hybrid prosthesis. Prior FEA studies of complete-arch, framework-supported implant prostheses suggest that increasing framework rigidity generally reduces global displacement/deflection, whereas the magnitude and location of peak stresses within the superstructure remain sensitive to framework geometry (e.g., cross-section/connector design), cantilever configuration, and load application [23,24,25,26]. In full-arch contexts, reduced deformation is clinically interpretable because it may be associated with improved stability of occlusal relationships and reduced flexure-driven micro-movements; however, deformation alone does not directly predict ceramic fracture without consideration of the local tensile stress field and flaw population.
Weibull Reliability Results and Their Meaning
A key contribution of this study is the use of Weibull field integration to translate spatially varying zirconia tensile stress (S1) into reliability indices. In brittle ceramics, strength is flaw-controlled and exhibits statistical scatter; Weibull analysis provides a formal framework to estimate survival probability under a specified stress distribution by integrating stress over a representative volume (or area) using a material’s Weibull parameters. This approach is widely established for structural ceramics and is directly relevant to dental zirconia, where strength variability and flaw sensitivity are fundamental considerations [12]. Accordingly, a probabilistic framework that accounts for stress distribution and stressed tensile volume is warranted when comparing brittle ceramic designs.
Across both designs, Pf values were extremely low (10⁻⁶ to 10⁻⁷ range) for the single-load case, consistent with the very low fracture probability predicted using the adopted Weibull parameters for translucent zirconia under glazed conditions. Importantly, direct numerical comparison between FE-derived peak principal tensile stresses in a complex full-arch geometry and flexural strength values reported from standardized laboratory tests is not straightforward, because measured strength depends on specimen geometry, surface condition, processing history, and the underlying flaw population. Accordingly, the present Weibull-based estimates should be interpreted primarily as comparative, design-sensitive indices under the stated modeling assumptions rather than as direct surrogates for laboratory strength limits or long-term clinical fracture incidence. Because V0 was defined as each design’s tensile-stressed zirconia volume (Vtens), design-to-design differences in the extent of tensile stress directly influenced IntW/V0 and hence Pf, even when S1max values were similar. This normalization was adopted to support within-study design comparisons rather than absolute clinical risk prediction. This likely explains why axial-loading Pf was slightly higher in Zr-TiBar despite nearly identical S1 maxima: the reliability integral depends on the stress distribution and the effective tensile volume used for normalization, not only on the peak value [12].
A critical interpretive point is that Weibull estimates in this study should be viewed as comparative, design-sensitive indices under the stated assumptions, rather than direct predictions of long-term clinical fracture incidence. Intraoral fracture of zirconia frameworks is influenced by subcritical crack growth, cyclic fatigue, surface damage (adjustment, sandblasting), aging (low-temperature degradation in some zirconia classes), cementation variables, and complex multi-contact loading histories. Experimental studies specifically addressing zirconia reliability and fatigue behavior underscore that survival probability depends strongly on cyclic loading conditions and environment, and that static-strength-based estimates do not fully capture fatigue degradation [27,28].
Relation to Clinical Evidence on Full-Arch Zirconia and Bar-Supported Designs
Clinical evidence indicates that full-arch implant-supported zirconia prostheses can demonstrate favorable short- to mid-term outcomes, but technical complications (e.g., chipping, fractures, occlusal wear, maintenance events) remain relevant, and outcomes depend on design and manufacturing protocols. Large cohort and systematic evidence on complete-arch implant prostheses show that technical maintenance and material-specific complications are common over time, even when implant survival is high [29,30,31].
For zirconia luted to titanium bar concepts specifically, early clinical reports and retrospective studies suggest promising short-term performance and emphasize the potential advantages of digital workflow control and framework support, while also highlighting the need for longer-term follow-up to confirm durability [13,14]. The present FE-based findings align with the general rationale for bar-supported architectures—namely reduced prosthesis deformation and modest stress redistribution—while also indicating that, under the current boundary conditions, these benefits did not translate into a materially meaningful reduction in static-load Weibull Pf compared with monolithic screw-retained zirconia. Therefore, selection between Zr-Mono and Zr-TiBar may be more strongly influenced by factors not fully captured by linear static FEA (e.g., fit accuracy, reparability, veneering strategy if present, bonding protocol, access/maintenance, and fatigue damage accumulation).
Loading Level and Clinical Plausibility
The 300 N posterior unilateral load used here is within commonly cited ranges of posterior bite forces and provides a pragmatic test magnitude for comparative analysis, although true intraoral loads are variable across individuals and conditions. Studies on maximal bite force demonstrate that posterior dentition typically experiences higher forces than anterior regions and that forces can exceed several hundred newtons in healthy adults [32,33,34]. Accordingly, while the absolute values of Pf should not be over-interpreted, the selected load level is reasonable for comparing design sensitivity in a standardized setting.
Limitations and Implications for Future Work
This study has limitations intrinsic to its modeling and to the Weibull implementation. First, the analysis used linear elastic, static loading with idealized contacts (e.g., bonded interfaces representing perfect luting and complete osseointegration), which does not capture micro-gap behavior, frictional sliding, or preload relaxation phenomena that can change stress transfer. Second, the Weibull approach applied to FE stress fields depends on the selected stress measure (here S1 in tension), the assumed representative volume, and the adopted Weibull parameters; while this is consistent with brittle fracture theory, it remains sensitive to parameter selection and does not explicitly model fatigue crack growth [12]. Third, only one load magnitude and a simplified unilateral contact were evaluated; multi-contact occlusion, parafunction, and repeated cyclic loading could yield different relative rankings. Therefore, future work should extend the present framework to (i) fatigue-informed reliability (e.g., slow crack growth or cyclic degradation models), (ii) sensitivity analysis across plausible Weibull parameter ranges reported for translucent zirconias, and (iii) validation against laboratory fatigue or fracture tests in analogous geometries where feasible.
Clinical Interpretation
Within the constraints of this in-silico model, both zirconia prosthetic architectures exhibited very low static-load Weibull fracture probability under 300 N axial and oblique loading, and peak tensile stresses were broadly comparable. Zr-TiBar demonstrated lower total deformation and slightly reduced oblique-load peak S1, but these advantages did not produce a consistent reduction in Pf relative to Zr-Mono. Clinically, these findings suggest that the choice between monolithic screw-retained zirconia and titanium-bar–supported zirconia should be guided not only by static fracture indices, but also by clinical workflow considerations, reparability, passive fit management, and fatigue-related performance—domains where long-term clinical evidence remains essential.
5. Conclusions
Within the limitations of this in-silico finite element study of an edentulous mandibular All-on-4 configuration, Zr-Mono and Zr-TiBar exhibited comparable zirconia maximum principal tensile stresses under 300 N axial loading, whereas oblique loading produced lower peak tensile stresses in both designs. Weibull post-processing of the zirconia tensile stress field yielded a very low predicted probability of zirconia fracture (Pf) for both prosthetic concepts under both loading directions, with only minor between-design differences (and lower Pf under oblique than axial loading). The titanium-bar–supported design demonstrated consistently lower total prosthesis deformation, indicating reduced structural compliance; however, this did not translate into a consistent reduction in Weibull-predicted fracture probability relative to the monolithic zirconia design.
Author Contributions
Conceptualization, M.T., N.B., and E.B.; methodology, M.T. and E.B.; software, M.T. and E.B.; validation, M.T., G.Y.A., and E.B.; formal analysis, M.T. and E.B.; investigation, M.T.; resources, M.T., N.B., and G.Y.A.; data curation, M.T. and E.B.; writing—original draft preparation M.T. and N.B.; writing—review and editing, M.T., N.B., G.Y.A., and E.B.; visualization, M.T.; supervision, E.B.; project administration, M.T.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data available on request from the authors.
Acknowledgments
During the preparation of this work authors used [Google Translate, DeepL, ChatGPT, Paperpal, and Grammarly] in order to enhance language clarity and accuracy of scientific writing. After using these tools, the authors reviewed and edited the content as needed and took full respon-sibility for the content of the publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| 3D | Three-dimensional |
| All-on-4 | Four-implant full-arch rehabilitation concept |
| APDL | ANSYS Parametric Design Language |
| CAD/CAM | Computer-aided design/computer-aided manufacturing |
| CBCT | Vone-beam computed tomography |
| CT | Vomputed tomography |
| FEA | Finite element analysis |
| GUI | Graphical user interface |
| IntW | Weibull stress-integration term |
| MAPDL | ANSYS Mechanical APDL |
| MRI | Magnetic resonance imaging |
| MUA | Multi-unit abutment |
| Pf | Probability of fracture |
| R | Reliability (survival probability) |
| RIFEM | Reporting guidelines for in-silico studies using finite element analysis in medicine |
| S1 | Maximum principal tensile stress |
| S1max | Peak maximum principal tensile stress |
| Ti | Titanium |
| Ti-base | Titanium base |
| V0 | Reference volume |
| Vtens | Tensile-stressed zirconia volume |
References
- Bidra, A.S.; Tischler, M.; Patch, C. Survival of 2039 complete arch fixed implant-supported zirconia prostheses: A retrospective study. J Prosthet Dent 2018, 119, 220-224. [CrossRef]
- Abdulmajeed, A.A.; Lim, K.G.; Närhi, T.O.; Cooper, L.F. Complete-arch implant-supported monolithic zirconia fixed dental prostheses: A systematic review. J Prosthet Dent 2016, 115, 672-677.e671. [CrossRef]
- Malo, P.; de Araújo Nobre, M.; Lopes, A.; Moss, S.M.; Molina, G.J. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. J Am Dent Assoc 2011, 142, 310-320. [CrossRef]
- Maló, P.; de Araújo Nobre, M.; Lopes, A.; Ferro, A.; Botto, J. The All-on-4 treatment concept for the rehabilitation of the completely edentulous mandible: A longitudinal study with 10 to 18 years of follow-up. Clin Implant Dent Relat Res 2019, 21, 565-577. [CrossRef]
- Maló, P.; de Araújo Nobre, M.; Lopes, A.; Ferro, A.; Nunes, M. The All-on-4 concept for full-arch rehabilitation of the edentulous maxillae: A longitudinal study with 5-13 years of follow-up. Clin Implant Dent Relat Res 2019, 21, 538-549. [CrossRef]
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin Oral Implants Res 2012, 23 Suppl 6, 22-38. [CrossRef]
- Pieralli, S.; Kohal, R.J.; Rabel, K.; von Stein-Lausnitz, M.; Vach, K.; Spies, B.C. Clinical outcomes of partial and full-arch all-ceramic implant-supported fixed dental prostheses. A systematic review and meta-analysis. Clin Oral Implants Res 2018, 29 Suppl 18, 224-236. [CrossRef]
- Ferreira, M.B.; Barão, V.A.; Faverani, L.P.; Hipólito, A.C.; Assunção, W.G. The role of superstructure material on the stress distribution in mandibular full-arch implant-supported fixed dentures. A CT-based 3D-FEA. Mater Sci Eng C Mater Biol Appl 2014, 35, 92-99. [CrossRef]
- Denry, I.; Kelly, J.R. State of the art of zirconia for dental applications. Dent Mater 2008, 24, 299-307. [CrossRef]
- Kelly, J.R.; Cesar, P.F.; Scherrer, S.S.; Della Bona, A.; van Noort, R.; Tholey, M.; Vichi, A.; Lohbauer, U. ADM guidance-ceramics: Fatigue principles and testing. Dent Mater 2017, 33, 1192-1204. [CrossRef]
- Taskonak, B.; Griggs, J.A.; Mecholsky, J.J., Jr.; Yan, J.H. Analysis of subcritical crack growth in dental ceramics using fracture mechanics and fractography. Dent Mater 2008, 24, 700-707. [CrossRef]
- Quinn, J.B.; Quinn, G.D. A practical and systematic review of Weibull statistics for reporting strengths of dental materials. Dent Mater 2010, 26, 135-147. [CrossRef]
- Mijiritsky, E.; Elad, A.; Krausz, R.; Ivanova, V.; Zlatev, S. Clinical performance of full-arch implant-supported fixed restorations made of monolithic zirconia luted to a titanium bar: A retrospective study with a mean follow-up of 16 months. J Dent 2023, 137, 104675. [CrossRef]
- Scarano, A.; Stoppaccioli, M.; Casolino, T. Zirconia crowns cemented on titanium bars using CAD/CAM: a five-year follow-up prospective clinical study of 9 patients. BMC Oral Health 2019, 19, 286. [CrossRef]
- Mathur, V.P.; Atif, M.; Duggal, I.; Tewari, N.; Duggal, R.; Chawla, A. Reporting guidelines for in-silico studies using finite element analysis in medicine (RIFEM). Comput Methods Programs Biomed 2022, 216, 106675. [CrossRef]
- Cawood, J.I.; Howell, R.A. A classification of the edentulous jaws. Int J Oral Maxillofac Surg 1988, 17, 232-236. [CrossRef]
- Bulaqi, H.A.; Mousavi Mashhadi, M.; Safari, H.; Samandari, M.M.; Geramipanah, F. Dynamic nature of abutment screw retightening: finite element study of the effect of retightening on the settling effect. J Prosthet Dent 2015, 113, 412-419. [CrossRef]
- Kaleli, N.; Sarac, D.; Külünk, S.; Öztürk, Ö. Effect of different restorative crown and customized abutment materials on stress distribution in single implants and peripheral bone: A three-dimensional finite element analysis study. J Prosthet Dent 2018, 119, 437-445. [CrossRef]
- Emam, M.; Keilig, L.; Bourauel, C. Biomechanical effect of different abutment and crown restoration materials in a single anterior dental implant and surrounding bone: A 3D finite element analysis. J Prosthet Dent 2025. [CrossRef]
- Yoon, H.G.; Oh, H.K.; Lee, D.Y.; Shin, J.H. 3-D finite element analysis of the effects of post location and loading location on stress distribution in root canals of the mandibular 1st molar. J Appl Oral Sci 2018, 26, e20160406. [CrossRef]
- Bokor, B.; Objelean, A.; Bran, S.; Campian, R.S.; Vilău, C. The impact of physiological and parafunctional posterior occlusal forces on experimental Ti-15Zrsupracrestal dental implant - a finite element analysis. Med Pharm Rep 2025, 98, 511-521. [CrossRef]
- Jeong, J.I.; Kwon, Y.H.; Seol, H.J. In Vitro Evaluation of Speed Sintering and Glazing Effects on the Flexural Strength and Microstructure of Highly Translucent Multilayered 5 mol% Yttria-Stabilized Zirconia. Materials (Basel) 2024, 17. [CrossRef]
- Menini, M.; Pesce, P.; Bevilacqua, M.; Pera, F.; Tealdo, T.; Barberis, F.; Pera, P. Effect of Framework in an Implant-Supported Full-Arch Fixed Prosthesis: 3D Finite Element Analysis. Int J Prosthodont 2015, 28, 627-630. [CrossRef]
- Tribst, J.P.M.; Campanelli de Morais, D.; Melo de Matos, J.D.; Lopes, G.; Dal Piva, A.M.O.; Souto Borges, A.L.; Bottino, M.A.; Lanzotti, A.; Martorelli, M.; Ausiello, P. Influence of Framework Material and Posterior Implant Angulation in Full-Arch All-on-4 Implant-Supported Prosthesis Stress Concentration. Dent J (Basel) 2022, 10. [CrossRef]
- Dayan, S.C.; Geckili, O. The influence of framework material on stress distribution in maxillary complete-arch fixed prostheses supported by four dental implants: a three-dimensional finite element analysis. Comput Methods Biomech Biomed Engin 2021, 24, 1606-1617. [CrossRef]
- Kupprano, P.; Kamonkhantikul, K.; Homsiang, W.; Takahashi, H.; Arksornnukit, M. Finite element analysis on implant-supported bar with different geometric shapes. BMC Oral Health 2024, 24, 1572. [CrossRef]
- Pereira, G.K.R.; Guilardi, L.F.; Dapieve, K.S.; Kleverlaan, C.J.; Rippe, M.P.; Valandro, L.F. Mechanical reliability, fatigue strength and survival analysis of new polycrystalline translucent zirconia ceramics for monolithic restorations. J Mech Behav Biomed Mater 2018, 85, 57-65. [CrossRef]
- Bruhnke, M.; Awwad, Y.; Müller, W.D.; Beuer, F.; Schmidt, F. Mechanical Properties of New Generations of Monolithic, Multi-Layered Zirconia. Materials (Basel) 2022, 16. [CrossRef]
- Papaspyridakos, P.; Bordin, T.B.; Natto, Z.S.; Kim, Y.J.; El-Rafie, K.; Tsigarida, A.; Chochlidakis, K.; Weber, H.P. Double Full-Arch Fixed Implant-Supported Prostheses: Outcomes and Complications after a Mean Follow-Up of 5 Years. J Prosthodont 2019, 28, 387-397. [CrossRef]
- Luo, J.; Zhang, Y.; Yu, Z.; Jiang, X.; Li, J.; Chen, B.; Di, P.; Lin, Y.; Zhang, Y. A retrospective single cohort study on the 5-13 year clinical outcomes of implant-supported cross-arch fixed dental prostheses with monolithic zirconia-based frameworks. J Prosthodont 2025, 34, 365-375. [CrossRef]
- Esquivel-Upshaw, J.F.; Mecholsky, J.J., Jr.; Clark, A.E.; Jenkins, R.; Hsu, S.M.; Neal, D.; Ren, F. Factors influencing the survival of implant-supported ceramic-ceramic prostheses: A randomized, controlled clinical trial. J Dent 2020, 103s, 100017. [CrossRef]
- Ferrario, V.F.; Sforza, C.; Zanotti, G.; Tartaglia, G.M. Maximal bite forces in healthy young adults as predicted by surface electromyography. J Dent 2004, 32, 451-457. [CrossRef]
- Waltimo, A.; Könönen, M. A novel bite force recorder and maximal isometric bite force values for healthy young adults. Scand J Dent Res 1993, 101, 171-175. [CrossRef]
- Khubchandani, S.R.; Bhoyar, A.; Sathe, S. Evaluation and Correlation of Bite Force With Electromyography (EMG) Activity Before and After Rehabilitation of the First Molar With an Implant-Supported Prosthesis. Cureus 2022, 14, e31085. [CrossRef]
Figure 1.
Transparent CAD renderings (SolidWorks) of the 2 full-arch prosthetic designs evaluated. A, Monolithic zirconia superstructure (Zr-Mono) supported by implants with multi-unit abutments and titanium bases. B, Titanium-bar–reinforced zirconia design (Zr-TiBar), comprising a CAD/CAM titanium bar supported by the same implant–abutment–titanium base configuration and a zirconia suprastructure.
Figure 1.
Transparent CAD renderings (SolidWorks) of the 2 full-arch prosthetic designs evaluated. A, Monolithic zirconia superstructure (Zr-Mono) supported by implants with multi-unit abutments and titanium bases. B, Titanium-bar–reinforced zirconia design (Zr-TiBar), comprising a CAD/CAM titanium bar supported by the same implant–abutment–titanium base configuration and a zirconia suprastructure.
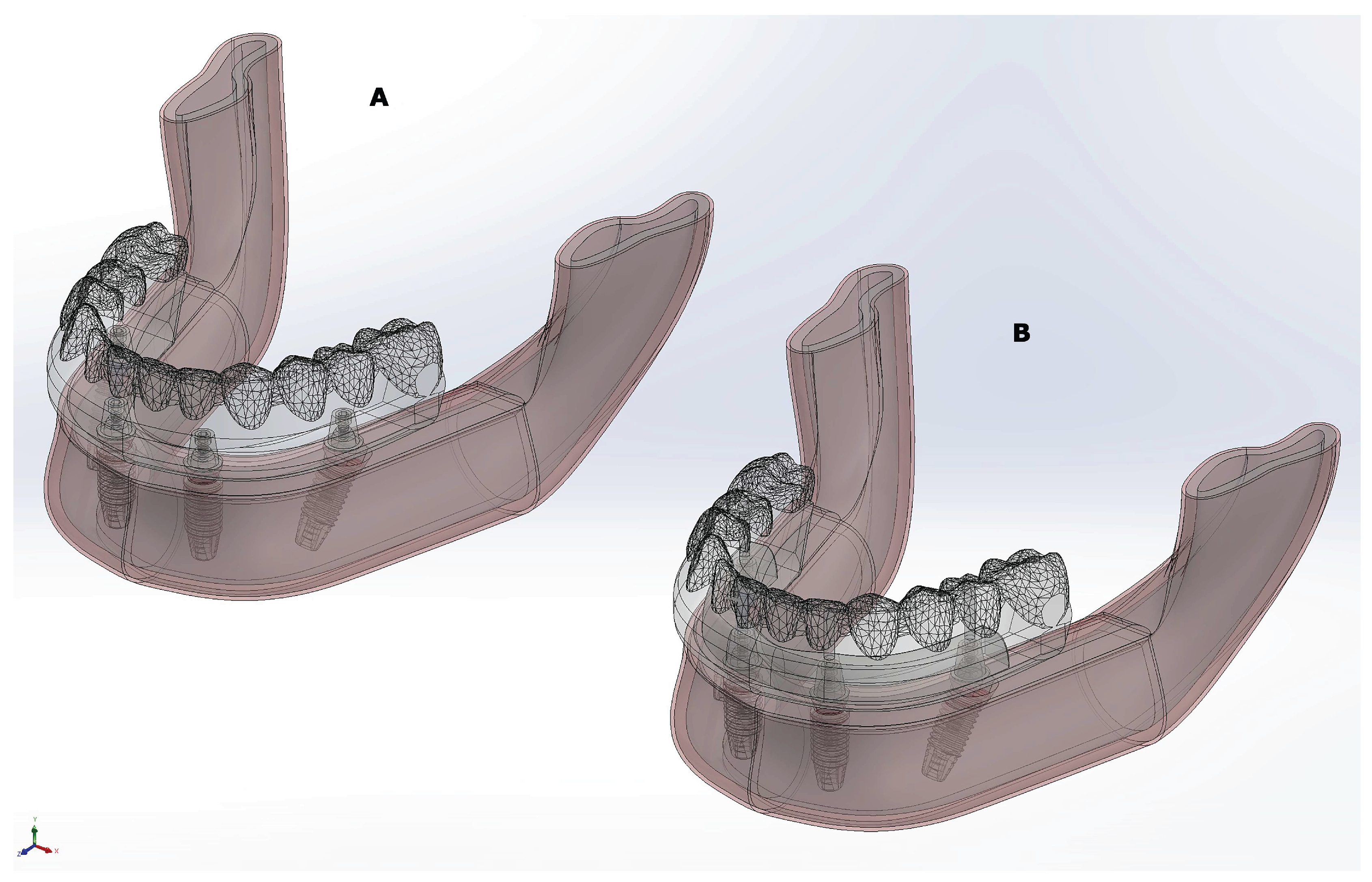
Figure 2.
Nodal peak maximum principal stress (S1) distribution in the zirconia prosthesis under 300-N axial and oblique loading for the Zr-Mono and Zr-TiBar designs. Color maps were obtained from ANSYS Mechanical post-processing and represent nodal maximum principal stress values.
Figure 2.
Nodal peak maximum principal stress (S1) distribution in the zirconia prosthesis under 300-N axial and oblique loading for the Zr-Mono and Zr-TiBar designs. Color maps were obtained from ANSYS Mechanical post-processing and represent nodal maximum principal stress values.
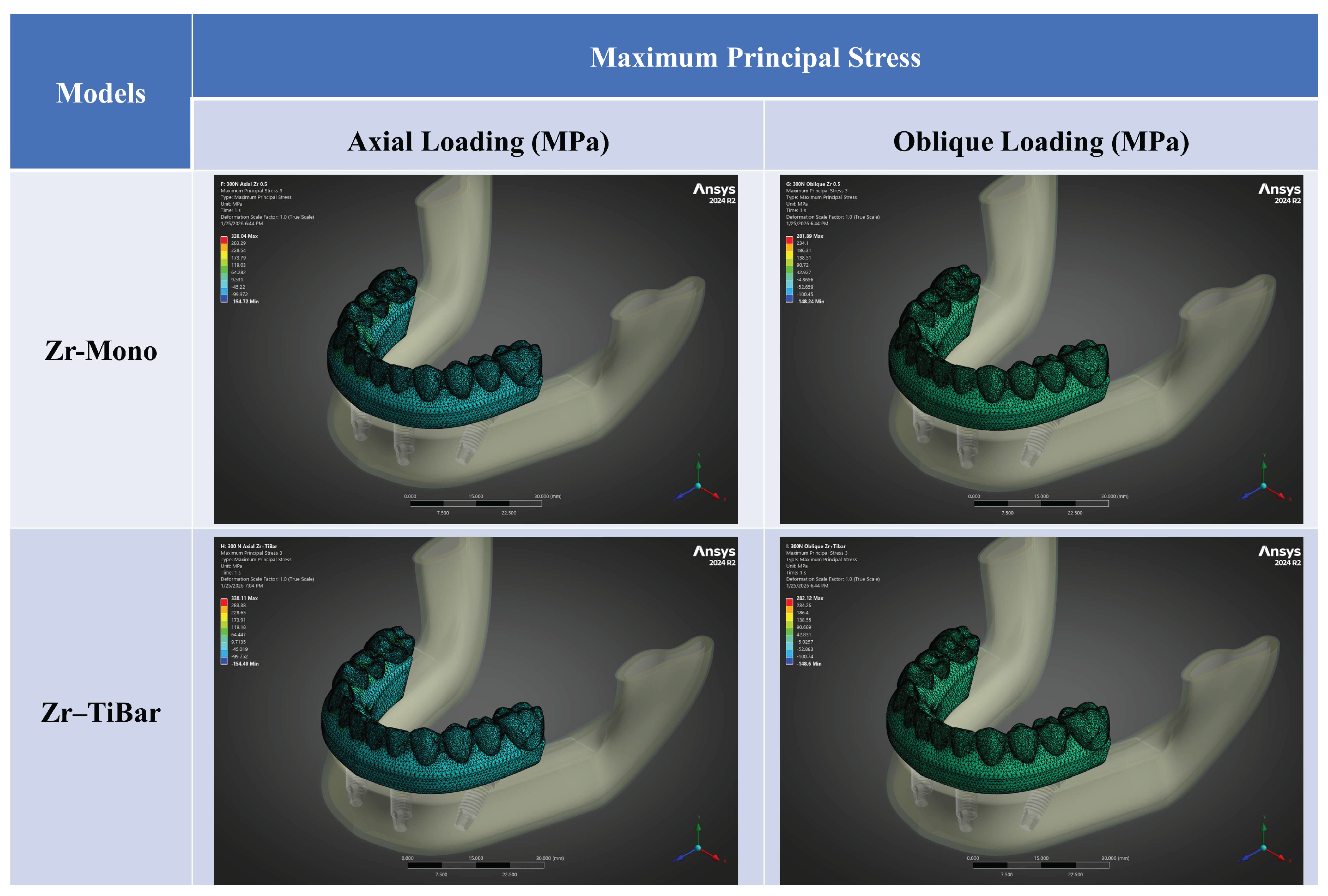
Figure 3.
Total deformation of the full-arch zirconia prosthesis under 300-N axial and 300-N oblique loading for the Zr-Mono and Zr-TiBar designs. Deformation contour plots were obtained from ANSYS Mechanical post-processing and report displacement magnitude (mm).
Figure 3.
Total deformation of the full-arch zirconia prosthesis under 300-N axial and 300-N oblique loading for the Zr-Mono and Zr-TiBar designs. Deformation contour plots were obtained from ANSYS Mechanical post-processing and report displacement magnitude (mm).
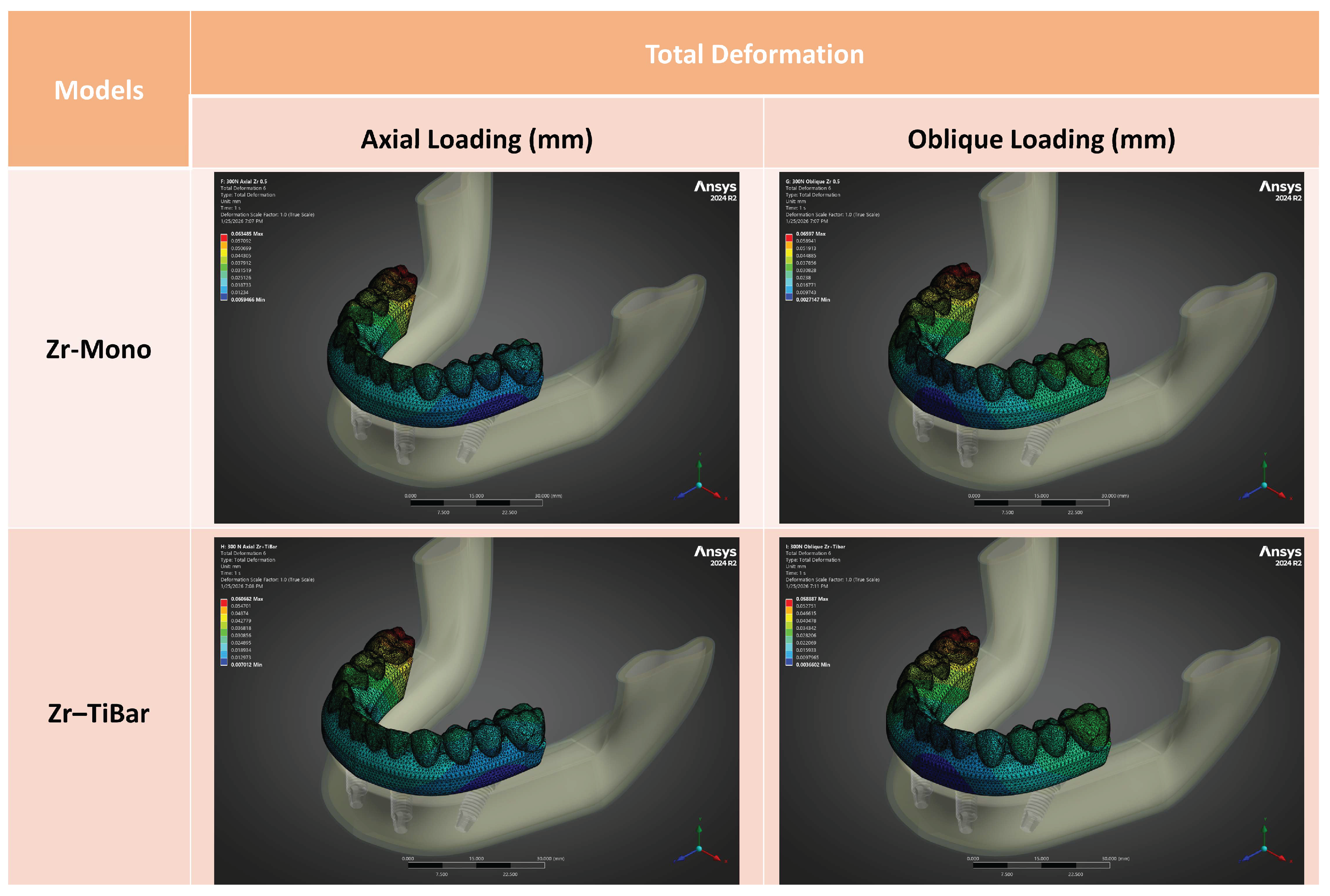

Table 1.
Mechanical properties of the materials.
| Materials | Young’s modulus (MPa) | Poisson’s ratio |
|---|---|---|
| Cortical bone | 13700 | 0.30 |
| Cancellous bone | 1000 | 0.30 |
| Implant, components, and bar (Titanium grade 5) | 110000 | 0.35 |
| Luting agent (Adhesive resin) | 18 600 | 0.28 |
| Zirconia prosthesis | 210 000 | 0.30 |
Table 2.
Finite element outcomes and Weibull-based zirconia reliability metrics for the monolithic zirconia (Zr-Mono) and titanium-bar–supported zirconia (Zr-TiBar) designs under 300 N posterior axial and 45° oblique loading.
Table 2.
Finite element outcomes and Weibull-based zirconia reliability metrics for the monolithic zirconia (Zr-Mono) and titanium-bar–supported zirconia (Zr-TiBar) designs under 300 N posterior axial and 45° oblique loading.
| Model | Loading (300 N) | S1max in zirconia (MPa) | Total deformation (mm) | IntW | V0 (=Vtens, mm³) | IntW/V0 | Reliability (R) | Fracture (Pf) |
|---|---|---|---|---|---|---|---|---|
| Zr-Mono | Axial | 277.09 | 0.0635 | 1.022386654E−02 | 7808.94222 | 1.309250288E−06 | 0.999998691 | 1.309250288E−06 |
| Zr-Mono | Oblique | 233.82 | 0.0660 | 1.247934465E−03 | 7855.53945 | 1.588604288E−07 | 0.999999841 | 1.588604288E−07 |
| Zr-TiBar | Axial | 277.13 | 0.0607 | 1.022325867E−02 | 6942.60491 | 1.472538229E−06 | 0.999998527 | 1.472538229E−06 |
| Zr-TiBar | Oblique | 226.94 | 0.0589 | 1.253586782E−03 | 7003.51812 | 1.789938499E−07 | 0.999999821 | 1.789938499E−07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



