
Submitted:
30 January 2026
Posted:
30 January 2026
You are already at the latest version
Abstract
Introduction: Delirium in older adults is strongly associated with and can predate dementia. While GLP-1 receptor agonists (GLP-1 RAs) may provide neuroprotective benefits, their role in reducing dementia risk among older patients with type 2 diabetes mellitus (T2DM) and prior delirium is unclear. This study compares the effectiveness of GLP-1 RAs and metformin in preventing dementia among patients with a history of delirium using an extensive healthcare database. Methods: A retrospective cohort study was conducted from 2005 to 2025 using data from the TriNetX Global Federated Research Network. We identified adults aged 65 and older with T2DM and delirium, who received either GLP-1 RAs (exposure) or metformin (control). Propensity score matching (PSM) was performed. We determined dementia outcomes and all-cause mortality using Kaplan–Meier survival curves, Cox proportional hazards models, and estimated odds ratio (OR). Subgroup analyses were conducted by age, sex, race, body mass index (BMI), and dementia types. Results: In a study involving 23,980 patients treated with GLP-1RAs and 23,980 matched patients treated with metformin, the mean age was 74 years, with 53% being female. The use of GLP-1RAs therapy was associated with a significantly lower risk of dementia compared to metformin among adults aged 65 years and older with T2DM with delirium with the adjusted hazard ratio (AHR) for dementia was 0.778 [95% confidence interval (CI): 0.736-0.822 p < 0.0001], and OR was 0.617 (95% CI: 0.582-0.655 p < 0.0001). The reduction in dementia risk varied by age, race, BMI , and dementia type. We observed a time-dependent decrease in mortality risk with GLP-1 RA users. Conclusion: In older adults with T2DM and delirium, GLP-1 RA therapy was associated with a reduced risk of dementia compared with metformin. Variations in subgroups suggest individualized treatment. Prospective randomized controlled trials are needed to confirm these findings and clarify differential effects across various subgroups.
Keywords:
dementia
; delirium
; metformin
; GLP-1 RA
; glucagon-like peptide-1 receptor agonist
; older adults
; type 2 diabetes mellitus
1. Introduction
T2DM is a rapidly growing health concern worldwide, affecting 537 million adults globally[1,2]. The disease is associated with cardiovascular, renal, and neurologic complications, including dementia and delirium[3]. Several studies have shown several biological pathways, such as insulin resistance, vascular complications, oxidative stress, neuroinflammation, and brain atrophy, that link T2DM to the development of dementia[4,5,6]. Preclinical studies indicate that delirium, an acute brain dysfunction, shares similar biological pathways with dementia[7]. Additionally, the presence of delirium is recognized as a significant risk factor for the acceleration of cognitive decline and progression to dementia [3]. Both delirium and dementia lead to high mortality, long-term cognitive decline, and diminished quality of life, thereby driving up health care costs and socioeconomic burden[8]. Given the intricate relationship between T2DM, delirium, and dementia, and the substantial impact on public health, investigating pharmacological interventions that might mitigate these risks is crucial.
Metformin and novel GLP-1 RAs have been shown to provide neuroprotective benefits in dementia [9,10,11]. Metformin's neuroprotective effects are attributed to its ability to alleviate insulin resistance, mitigate neuronal apoptosis, reduce oxidative stress and neuroinflammation, thereby decreasing the risk of dementia [9]. While some studies show neuroprotective benefits from metformin, others have reported inconsistent findings regarding its efficacy in reducing dementia risk[12]. In contrast, GLP-1 RAs are incretin mimetics that bind to GLP-1 receptors, thereby exerting potent antihyperglycemic effects and promoting weight loss [13]. These receptors are also expressed in the hippocampus and cortex—regions implicated in neurodegenerative diseases—enabling GLP-1 RAs to reduce neuroinflammation, oxidative stress, and apoptosis while promoting neurogenesis [13,14]. Importantly, GLP-1 RAs have been implicated in lowering beta-amyloid plaque deposition and mitigating tau hyperphosphorylation, key mechanistic pathways in Alzheimer's disease [14].
Despite the neuroprotective benefits of metformin and GLP-1 RAs in mitigating risks of dementia and delirium among older adults with type 2 diabetes mellitus, no head-to-head comparisons have evaluated their relative efficacy in preventing dementia specifically in older patients with delirium. This study aims to compare the effectiveness of GLP-1 RAs and metformin in preventing dementia among older adults with T2DM and delirium, using data from an extensive real-world cohort study. Hopefully, these findings will provide crucial insights and contribute to the evidence base, guiding clinical decisions and future research on T2DM management in older patients at risk.
2. Materials and Methods
2.1. Study Design and Data Source
We conducted a cohort retrospective study utilizing the TriNetx United States network to investigate the effect of metformin and GLP-1RAs on dementia outcomes in older adults diagnosed with delirium. TriNetX US Network is a federated research network that provides access to de-identified electronic health record data from 174 million patients and 84 healthcare organizations across the United States[15,16]. The datasets include diagnoses, procedures, medications, laboratory results, and genomic and demographic information[16]. Compliance with the Health Insurance Portability and Accountability Act (HIPAA) and the General Data Protection Regulation (GDPR) was achieved through a data de-identification process and aggregation for statistical analysis[16]. We obtained a waiver of informed consent from the University of Hawaii Institutional Review Board (IRB 2025-01053). We completed the analysis of the aggregated data on December 9, 2025. This retrospective study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines to ensure rigorous reporting of methods and results [17].
2.2. Study Population
We included older patients, defined as 65 years and older, with delirium who had a recorded diagnosis of T2DM and had taken either metformin or GLP-1 RA from 2005 to 2025. Since GLP-1 RAs were introduced to the market on June 1, 2005, we chose January 1, 2005, as the start date of our study [17,18]. The index date was defined as the onset of delirium to ensure delirium predated dementia onset, thereby mitigating reverse causation bias. Patients with 1 year of prior metformin use before the index date were excluded to minimize confounding from pre-existing metformin exposure. We used the ICD-10-CM codes R41.0 (disorientation unspecified) and F05.x (delirium due to physiological condition) to identify delirium, which are commonly used in TriNetx for this purpose. Coding trends suggested that delirium was under-reported and was preferentially coded as encephalopathy [20]. To account for delirium coded under encephalopathy, we included the ICD-10-CM codes G93.40 (encephalopathy, unspecified) and G93.41 (metabolic encephalopathy)[20]. Furthermore, to ensure a focus on incident dementia outcomes, individuals with a pre-existing diagnosis of dementia before their index date were excluded from the analysis.
2.3. Exposure Definitions
Patients were categorized into two exposure groups: those prescribed metformin and those prescribed a GLP-1 RA. Patients initiating both GLP-1 RAs and metformin at the index date were excluded. To reflect real-world practices and enhance the external validity of our findings, we allowed concomitant use of insulin and other antidiabetic medications. However, to reduce confounding bias from the use of antidiabetic medications other than metformin and GLP-RAs, we ensured that both cohorts had similar distributions of other glucose-lowering agents through propensity score matching (PSM). This comprehensive approach enables a more robust analysis of the specific effects of metformin and GLP-1 RAs on dementia outcomes, while minimizing the influence of concurrent pharmacotherapy.
The GLP-1 RAs include exenatide, liraglutide, dulaglutide, lixisenatide, semaglutide, and albiglutide. We permitted crossover between these drug classes to reflect real-world practice better and reduce the risk of exposure misclassification. Additionally, allowing crossover time increases statistical power to detect the outcome. The use of a specific agent indicates that it is a GLP-1 RA, ensuring we capture the cumulative effects of GLP-1 RAs over time. This approach is consistent with the class effect of GLP-1 RA on cardiovascular benefits demonstrated in previous studies[21].
Patients were followed from the date of onset of delirium until the first diagnosis of dementia, occurrence of death, disenrollment from the healthcare network, loss to follow-up, or study completion, whichever occurred first.
2.4. Outcome Measures
The primary outcome was the first recorded diagnosis of dementia. We defined dementia using the ICD-10-CM codes G30 (Alzheimer's disease), F01 (Vascular dementia), F02 (Dementia in other diseases classified elsewhere), F03 (Unspecified dementia), G31.0 (Frontotemporal dementia), and G31.83 (Neurocognitive disorder with Lewy bodies). Although previous studies have shown neuroprotective effects of GLP-1 RAs in patients with T2DM and Alzheimer's dementia[22], we included other dementia types to enhance robustness and enable subgroup analyses across various dementia subtypes, which further allows for a more comprehensive understanding of the potential differential impacts of these medications across different subtypes of dementia.
The secondary outcome focused on "all-cause mortality." The mortality event was explicitly determined by the ICD-10 code R99 and "deceased" status in TriNetX.
Subgroup analysis was conducted by age, sex, race, dementia type, and BMI. This approach provides a comprehensive understanding of treatment effects across diverse patient characteristics and disease manifestations, enhancing the generalizability and clinical relevance of our findings.
2.5. Statistical Analysis
PSM was used to balance baseline characteristics between the metformin and GLP-1 RA groups, thereby reducing confounding by indication and enabling a direct comparison. Matching factors included demographic characteristics such as age, gender, race, and ethnicity. Metabolic and renal function parameters, including BMI, glomerular filtration rate (GFR), and hemoglobin A1c, were included. To mitigate potential medication influence on outcome, we included insulin, other oral hypoglycemics, antibiotics, antivirals, antipsychotics, and dementia medications. To mitigate indication bias, we included medical and cardiovascular diseases in the PSM. Propensity scores were estimated using logistic regression with the LogisticRegression function from scikit-learn in Python. Matching was performed using nearest-neighbor algorithms, with a caliper width of 0.1 based on the pooled standardized differences in propensity scores.
Time-to-event outcomes for dementia and all-cause mortality were analyzed using the Kaplan-Meier method and Cox proportional hazards regression to estimate AHRs with 95% confidence intervals. Logistic regression was also employed to complement the AHRs, expressed as OR with 95% confidence intervals. The proportional hazards assumption was evaluated using Schoenfeld residuals, and no major violations were detected. For all-cause mortality, we divided the follow-up period into distinct intervals (0-5 years, 5-10 years, 10+ years) to assess the time-varying risk of death across specific timeframes.
Subgroup analyses were employed to assess the effect of metformin or GLP-1 RA, using AHR, among various demographic and clinical covariates such as age groups (65-75 yo, > 75 yo), sex, race (Whites, African Americans, Hispanics, Asians), specific dementia types (Alzheimer's disease, vascular dementia, dementia of Lewy body, frontotemporal dementia, unspecified dementias), and BMI ( <30 kg/m2, >- 30 kg/m2).
All statistical tests were two-sided, using a significance level of p < 0.05. Analyses were performed on the TriNetx platform to maintain data integrity and facilitate standardized extraction of real-world data.
3. Results
3.1. Study Population
Among patients aged 65 years and older with delirium, we identified 84,403 metformin initiators and 25,906 GLP-1 RA initiators after applying the inclusion and exclusion criteria. Before propensity score matching, both cohorts had a mean age of 74-75 years and were predominantly White and non-Hispanic. Additionally, the metformin cohort was predominantly male (52%), while the GLP-1 RA cohort was predominantly female (54%). Detailed patient characteristics for both the unmatched and matched metformin and GLP-1 RA groups are summarized in Table 1.
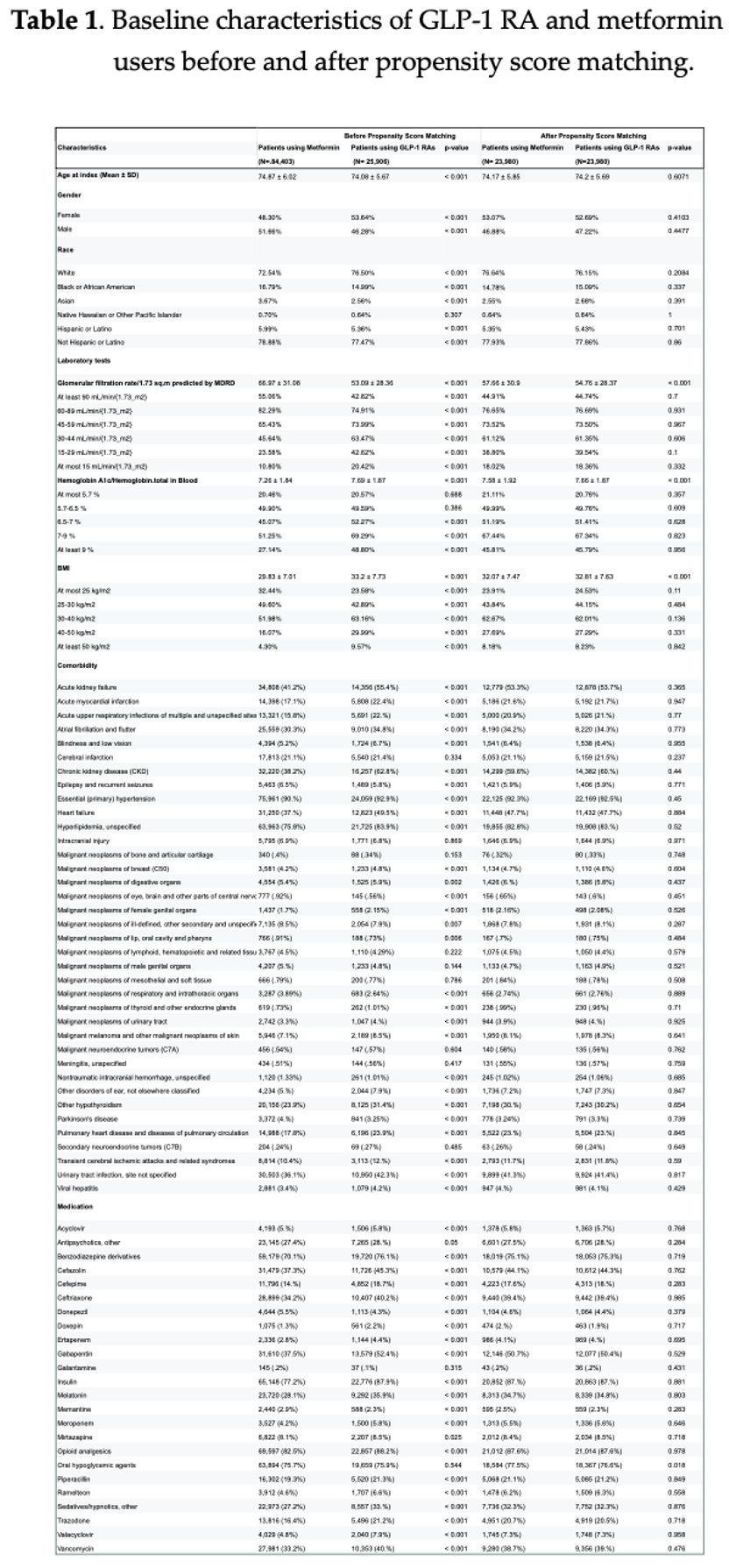
Following 74 years and 53% female in the matched groups. Hypertension emerged as the most prevalent comorbidity in both groups. Furthermore, more than 50% of patients in both groups were taking insulin, other oral hypoglycemics, gabapentin, benzodiazepines, and opioid analgesics.
3.2. Primary Outcome
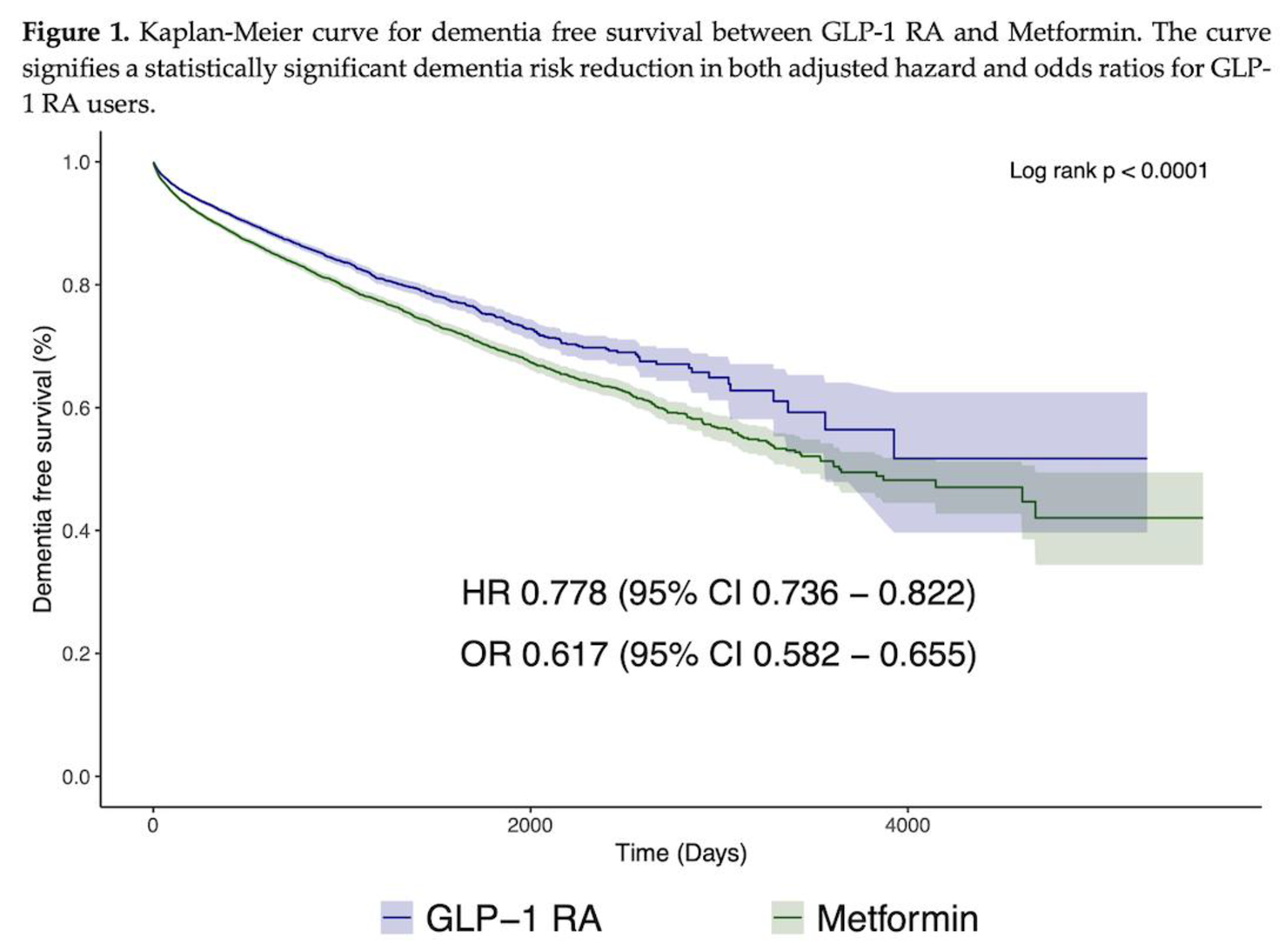
The median follow-up time for the primary outcome was 457 days in the metformin group and 374 days in the GLP-1 RA group. During this follow-up, there were 3,137 dementia events in the metformin group and 2,205 events in the GLP-1 RA group. Notably, the AHR for dementia was 0.778 (95% CI: 0.736-0.822, p < 0.0001), and the OR was 0.617 (95% CI: 0.582-0.655, p < 0.0001), both indicating a significantly lower risk of dementia in patients treated with GLP-1 RAs compared with the metformin group. This is illustrated by the Kaplan-Meier curve for dementia shown in Figure 1, where the log-rank test was significant.
Abbreviations: CI: confidence interval; OR: odds ratio; HR: hazard ratio
3.2. Secondary Outcome
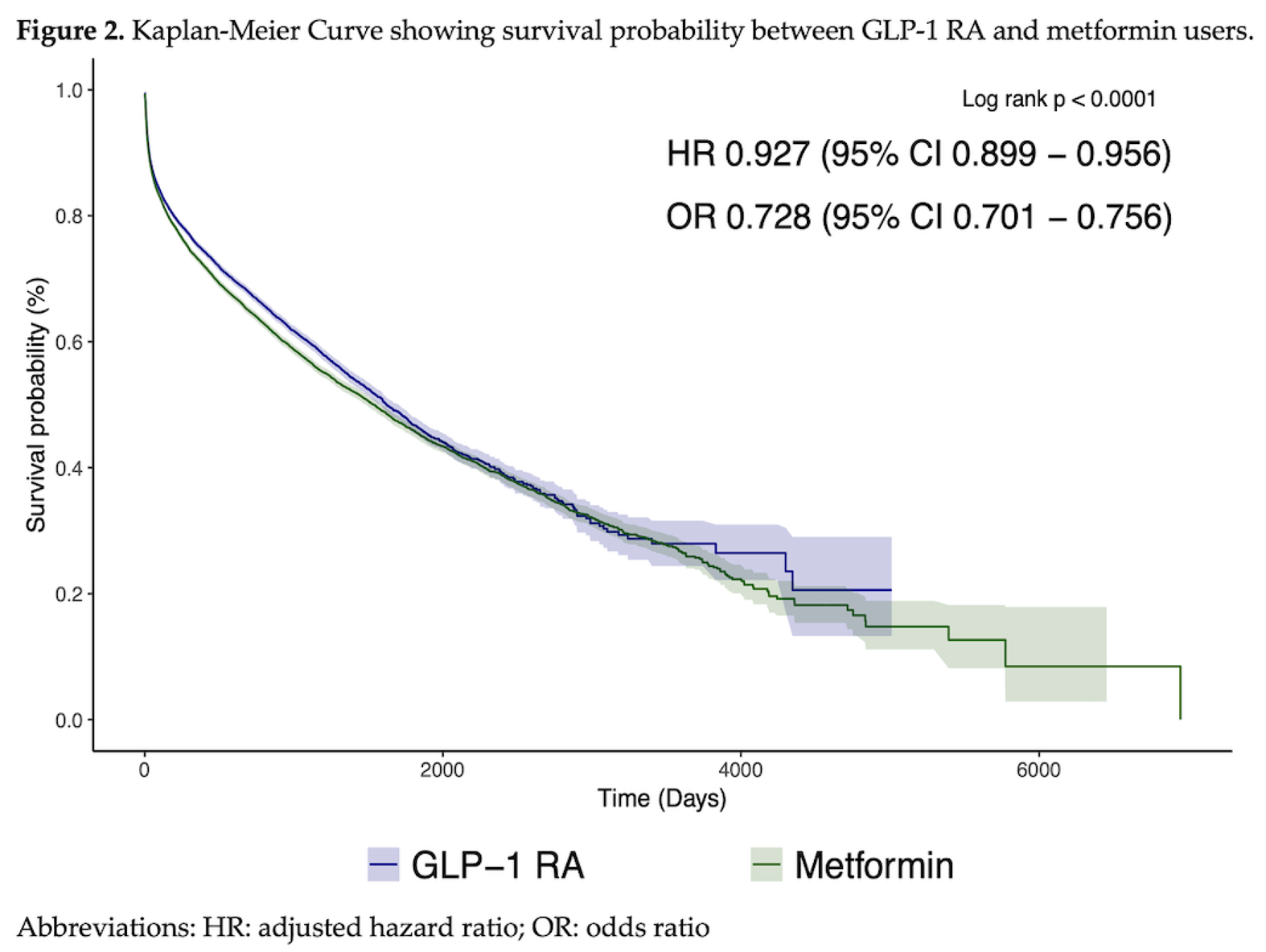
The Kaplan-Meier curve for all-cause mortality is shown in Figure 2. During the follow-up period, there were 9,188 deaths in the Metformin group and 7,489 deaths in the GLP-1 RA group, with an AHR 0.927 (95% CI 0.899 − 0.956 p < 0.0001) and an OR of 0.728 (95% CI 0.701 − 0.756 p < 0.0001), both suggesting a potential survival advantage in the GLP-1 RA cohort (Table 2). However, further assessment of temporal trends in mortality during different follow-up periods revealed a statistically significant reduction in mortality at 0-5 years of AHR 0.915 (95% CI 0.887-0.944 p < 0.0001), OR 0.765 (95% CI 0.737- 0.795 p < 0.0001), whereas the mortality at 5-10 years follow-up period was not statistically significant, AHR 1.092 (95% CI 0.911, 1.31) but the odds risk remained significantly low, OR 0.315 (95% CI 0.262, 0.378 p < 0.0001). Beyond 10+ years, we could not compute mortality due to insufficient sample size remaining in both cohorts after long-term follow-up (Table 2).
3.3. Subgroup Analysis
Figure 3 presents subgroup analyses assessing the associations between GLP-1 RAs and dementia risk across demographic and clinical variables. Across all subgroups, there was a trend towards protection from dementia risk with GLP-1 RA use. However, GLP-1 RA use was associated with a greater reduction in dementia risk among patients aged 65–75 years, AHR 0.742 (95% CI: 0.687−0.801, p < 0.001), compared with those aged >75 years, AHR 0.884 (95% CI: 0.81−0.964, p < 0.005). Additionally, a more pronounced risk reduction was observed among GLP-1 RA users with a BMI <30, AHR 0.74 (95% CI: 0.664- 0.825, p < 0.001), compared to those with a BMI >30, AHR 0.821 (95% CI: 0.77−0.876, p < 0.001). Furthermore, GLP-1 RA use was associated with a greater reduction in dementia risk among the Whites, AHR 0.763(95% CI 0.711-0.818, p < 0.001), modestly in African Americans, AHR 0.837 (95% CI 0.72-0.974, p < 0.021), the Hispanic population, AHR 0.768 (95% CI 0.6- 0.984, p < 0.036), but not statistically significant among the Asian population, AHR 0.935 (95% CI 0.63-1.389, p < 0.739).
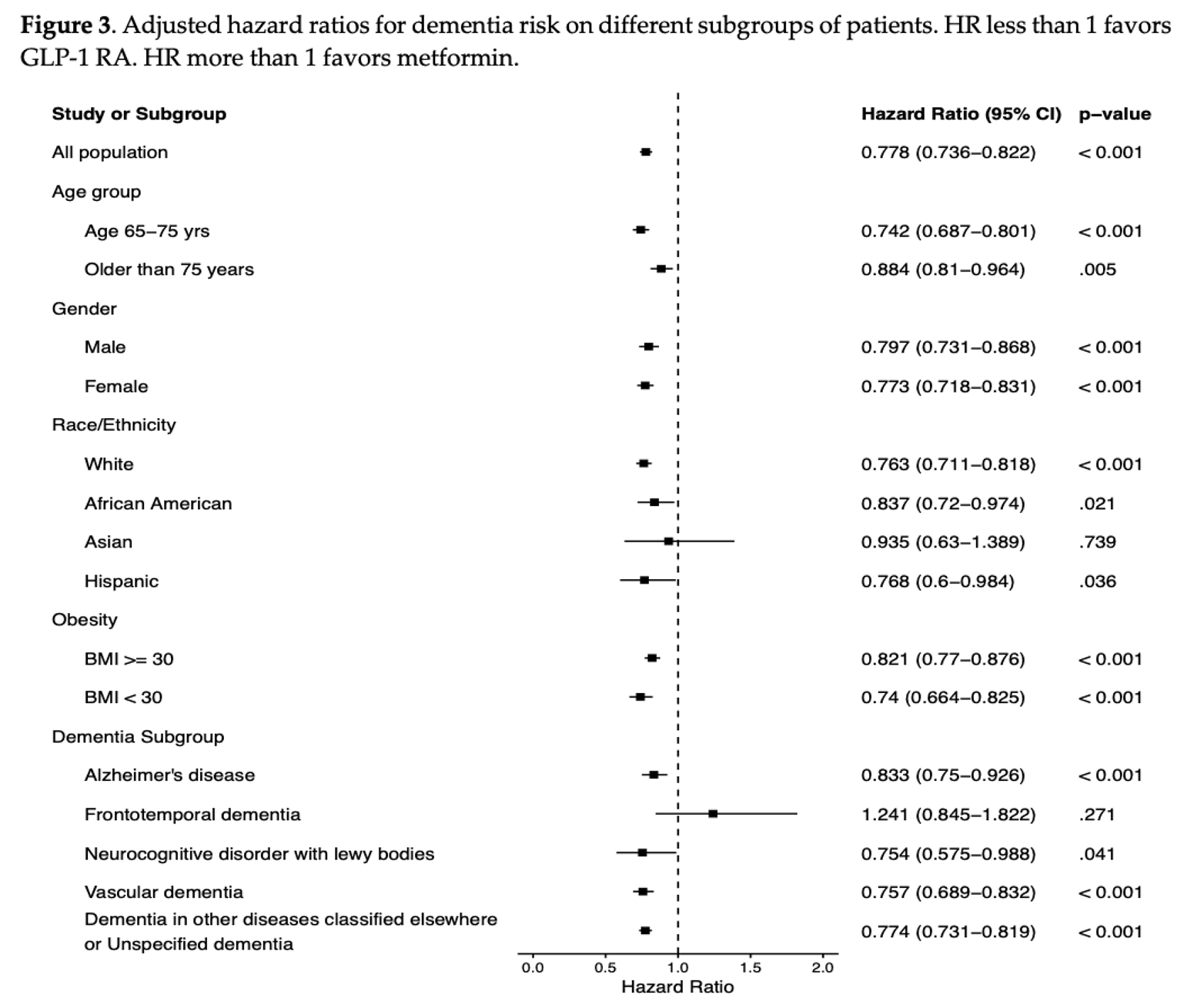
Among the different types of dementia (Figure 3), there was a discernible trend toward reduced risk among GLP-1 RA users, including for Alzheimer's dementia AHR 0.833(95% CI: 0.75−0.926, p < 0.001), vascular dementia AHR 0.757(95% CI:0.689−0.832, p < 0.001) and dementia of Lewy bodies AHR 0.754 (95% CI:0.575−0.988, p < 0.001). In contrast, protection for frontotemporal dementia risk did not reach statistical significance, AHR 1.241 (95% CI:0.845−1.822, p < 0.271).
4. Discussion
This study is the first to directly compare the dementia-reducing effects of GLP-1 RAs versus metformin in older adults with T2DM and delirium, drawing from an extensive real-world database. Although both metformin—a well-established first-line therapy for T2DM—and GLP-1 RAs have demonstrated potential neuroprotective benefits, their comparative effectiveness in reducing dementia risk in this type of population was previously unknown[9,23]. Against this background, our head-to-head analysis demonstrates that GLP-1 RAs are associated with a significantly lower risk of dementia—including Alzheimer's disease and other subtypes—compared to metformin, particularly among specific racial groups, as well as a time-dependent reduction in all-cause mortality risk. These findings offer valuable insights into GLP-1 RAs as a promising therapeutic option for mitigating dementia in this vulnerable population, with potential to inform clinical guidelines and spur prospective randomized controlled trials.
4.1. Dementia Risk
Our study demonstrated the neuroprotective benefits of GLP-1 RAs over metformin in older adults with T2DM and delirium by reducing dementia risk. Specifically, GLP-1 RA users had a 22% lower risk of dementia at any given time and 38% lower odds of developing dementia compared to metformin users. Our findings align with prior observational studies. For instance, in a cohort retrospective study of 87,229 matched patients from the TriNetX database, GLP-1 RA users had a significantly lower risk of overall dementia compared to metformin users, although those patients included in this study had no history of prior delirium[11]. Additionally, an extensive nested case-control study among Danish participants found that GLP-1 RA use was associated with a reduced risk of dementia compared to metformin and other antidiabetic medications [23]. Specifically, a target trial emulation comparing semaglutide to other antidiabetic medications, including metformin, significantly reduced the risk of dementia across all age, sex, and obesity subgroups. However, the follow-up was limited to three years [24]. Additionally, a retrospective cohort study comparing Liraglutide to DPP-4 inhibitors also noted a lower risk of dementia with liraglutide, but, like the other study, had a short follow-up of 3 years and potential confounding factors [25]. Collectively, these findings emphasize the neuroprotective advantage of GLP-1 RAs over metformin in older adults with T2DM and delirium, supporting their preferential therapeutic use in this population.
Several pathophysiological mechanisms, supported by preclinical and clinical studies, suggest that GLP-1 RAs exert neuroprotective effects that reduce dementia risk, findings that align with ours. For instance, preclinical studies in mice with postoperative-induced delirium showed that GLP-1 RA administration mitigated delirium and cognitive decline by reducing neuroinflammation, apoptosis, and oxidative stress, while strengthening neuronal integrity through enhanced synaptic plasticity [7]. These mechanistic processes observed in delirium are also evident in dementia development, further strengthening our results that GLP-1 RAs confer cognitive benefits in older adults with delirium. Specifically, a systematic review found that liraglutide and semaglutide enhanced insulin sensitivity, modulated oxidative stress and inflammation, and thereby promoted neuronal health[26]. Clinical and preclinical studies further demonstrate that GLP-1 RAs modulate pathologic hallmarks of Alzheimer's disease, such as tau protein phosphorylation and beta-amyloid synthesis[26,27]. In contrast, some randomized controlled trials in humans involving GLP-1 RAs did not demonstrate cognitive improvements or modulation of amyloid levels[29,30]. While these studies provide evidence for the neuroprotective benefits of GLP-1 RAs in mitigating dementia, more rigorous clinical trials are warranted to confirm these effects in older adults with delirium and T2DM[1,23,31].
4.2. Sub-Group Analysis
Our study highlighted the heterogeneous neuroprotective effects of GLP-1 RAs compared to metformin across diverse population subgroups. For example, we observed a more pronounced reduction in dementia risk among adults younger than 75 years compared to those aged 75 and older. This suggests that earlier initiation of GLP-1 RA therapy may offer a greater window for neuroprotection, potentially slowing the neurodegenerative processes leading to dementia[31]. Conversely, starting GLP-1 RA therapy at advanced ages may provide fewer benefits, possibly due to heightened risks of muscle loss or sarcopenia—key contributors to frailty and cognitive decline[32,33].
In addition to age-related differences, we noted sex-based variations in GLP-1 RA responses. Females showed a slightly lower dementia risk than males, which may be due to greater sensitivity to GLP-1 RA therapy stemming from reduced estrogen levels and menopausal metabolic changes[34]. These results align with prior studies reporting greater reductions in dementia risk in females, suggesting a potential sex-specific benefit from GLP-1 RAs [33]. Furthermore, treatment effects varied by racial/ethnic groups. We found significant dementia risk reductions in White, African Americans, and Hispanic populations, but not in Asians. This is consistent with previous extensive population-based cohort studies showing no risk reduction for delirium or dementia in Asians initiating GLP-1 RAs compared to metformin [23,33]. Notably, while Asians exhibited the most significant cardiovascular risk reductions relative to Whites [35], delays in dementia diagnosis and evaluation in this group have been reported [36], potentially introducing a selection bias. Other factors, such as genetic differences, socio-cultural influences, and disparities in healthcare access, may also contribute to observed differences in treatment efficacy across racial groups. These heterogeneities in treatment responses across age, sex, and racial/ethnic groups emphasize the need for personalized medicine in preventing and managing dementia among older adults with delirium. Moreover, future studies should explore the mechanisms underlying these disparities and develop tailored therapeutic strategies to optimize patient outcomes.
Our results are consistent with prior observational studies demonstrating that GLP-1 RA use is generally associated with a lower risk of incident dementia compared to metformin [30]. Specifically, in the recent large population-based study, GLP-1 RAs compared to metformin significantly reduced risk of having Alzheimer's disease and non-vascular dementias. In our study, this association was observed in Alzheimer's disease, vascular dementia, and dementia with Lewy bodies, with no benefit observed in frontotemporal dementia. This observed pattern is biologically plausible, given that the dementia subtypes showing significant risk reduction share metabolic, vascular, and inflammatory pathways that may be modulated by GLP-1 signaling. In contrast, frontotemporal dementia exhibits a weaker association with metabolic dysregulation[37,38]. Although most studies on the neuroprotective effects of GLP-1 receptor agonists have primarily focused on Alzheimer's disease, the differences in metabolism, genetics, insulin sensitivity, and tau pathology related to frontotemporal dementia and GLP-1 receptor agonists necessitate further investigation [26]. Our study cohort comprised older adults who had experienced an episode of delirium; as a result, cases of frontotemporal dementia, which are typically diagnosed at younger ages, may have been excluded during the initial propensity score matching, limiting our statistical power. Furthermore, diagnostic misclassification may also have occurred within our older post-delirium cohorts. Therefore, these findings should be interpreted as generating hypotheses for further research.
We used BMI for propensity score matching. Although our subgroup analysis suggested a greater dementia risk reduction among patients with BMI < 30 compared to those with BMI > 30, this result should be interpreted with caution. For instance, since BMI was measured only at baseline, it reflects a single point in time and does not account for subsequent changes influenced by GLP-1 RA treatment (treatment-related weight change) or disease progression. Additionally, in older adults, BMI may reflect a complex interplay of factors—including frailty, sarcopenia, and a prodromal neurodegenerative process—rather than solely adipose content[39]. Therefore, relying exclusively on this baseline BMI may introduce collider bias or reverse causation bias, thereby limiting causal inference about BMI's effect modification[40]. Overall, these findings should be considered exploratory.
4.3. All-Cause Mortality
In this cohort, GLP-1 RA use was associated with reduced all-cause mortality during the first 0–5 years of follow-up, but not thereafter. Specifically, the hazard ratio for all-cause mortality was significantly reduced during the 0–5-year period; however, it gradually diminished thereafter and became non-significant during the 5–10-year follow-up. This early mortality benefit of GLP-1 RAs compared to metformin was also demonstrated in an extensive population-based cohort study, albeit with delirium as the primary outcome[33]. In this study, using the extensive TriNetX database, GLP-1 RA users showed a significantly reduced absolute risk of death, although they exhibited lower survival probability over more extended follow-up periods [33]. Our findings suggest that, although GLP-1 RAs confer neuroprotective and cardiometabolic benefits, they eventually lose their survival advantage, such that metformin may offer better long-term survival in this population of older patients with delirium[33]. Several reasons can be postulated for this time-dependent survival advantage. Studies showed that GLP-1 receptor expression diminishes with aging [41], a factor that may decrease its survival benefit. Long-term side effects from prolonged GLP-1 RA use—such as sarcopenia, appetite suppression, or malignancy—may offset their early survival advantages[32,42].
Furthermore, with advancing age among older adults, competing risks—particularly those arising from diabetes-related cardiometabolic and renal comorbidities—become more prominent, thereby compromising patient survival. The risk of survivorship bias should not be overlooked, as longer-term survivors tend to be healthier, thereby attenuating event rates and statistical power beyond 5 years. These findings further underscore that older adults with delirium constitute a high-risk population for mortality, warranting judicious selection of therapeutic strategies that optimize neuroprotective benefits alongside long-term survival[43].
4.4. Limitations and Recommendation
We acknowledge several limitations in our study. First, as this was a retrospective study, residual confounding from unmeasured factors cannot be entirely excluded despite extensive propensity score matching and subgroup analyses. Second, misclassification bias is possible due to heavy reliance on ICD coding for diagnoses, as delirium was historically coded under encephalopathy; we mitigated this by incorporating multiple diagnostic codes for delirium and encephalopathy. Third, the results may not be generalizable due to the exclusion of patients with prior metformin use. However, our study permitted concomitant use of other antidiabetic medications to better simulate real-world practice without compromising balanced exposure between study groups. Fourth, using the onset of delirium as time zero may have introduced survivorship bias; however, our results provide a nuanced understanding of the time-dependent nature of mortality benefits rather than a blanket claim of long-term survival advantage. Fifth, our results may not be generalizable to other ethnic groups, such as Native Americans, Native Hawaiians, and Pacific Islanders, due to their limited representation in our cohort. However, our study provides a basis for future health disparities research among these diverse populations. Notwithstanding these limitations, our extensive real-world dataset and rigorous propensity-score-matched analysis yield persuasive evidence that GLP-1 RAs outperform metformin in reducing dementia risk among older adults with T2DM and delirium. These results offer practical guidance for clinical practice and underscore the need for randomized controlled trials to evaluate the potential of GLP-1 RAs to attenuate cognitive decline in patients with delirium.
5. Conclusions
This study is the first to demonstrate the comparative effectiveness of GLP-1 RAs versus metformin in reducing dementia risk following an episode of delirium in older adults with T2DM. These findings support a paradigm shift in therapeutic approaches, positioning GLP-1 RAs as a promising neuroprotective option for older adults experiencing delirium. Additionally, our results indicate a time-dependent survival benefit associated with GLP-1 RA use in this population, which diminishes over time. Moving forward, these findings provide a robust foundation for future randomized controlled trials to establish the causal relationship between GLP-1 RA use and reduced dementia incidence in this patient population, incorporating patient-specific factors, greater inclusivity, and extended treatment durations and follow-up periods.
Author Contributions
Conceptualization, F. M.; methodology, F.M. and A.O.; software, A.O.; validation, F.M., A. O.; formal analysis, F.M., A.O., and S.V.; investigation, F.M; resources, F.M; data curation, A.O.; writing—original draft preparation, F.M., S.A., S.V., R.S.; writing—review and editing, F.M., A.O., S.V., R.S., and S.A; visualization, S.V.; supervision, F.M.; project administration, F.M.; funding acquisition, not applicable. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of the University of Hawaii (protocol code 2025-01053 on January 23, 2026, for studies involving humans.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing does not apply to this article.
Acknowledgments
With many thanks to Dr. Scott Kuwada for supporting this research.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AHR | Adjusted Hazard ratio |
| BMI | Body mass index |
| CI | Confidence interval |
| GLP-1 RAs | GLP-1 receptor agonists |
| OR | Odds ratio |
| PSM | Propensity score matching |
| T2DM | Type 2 diabetes mellitus |
References
- Chen, X.; Huang, Y.; Xiong, X. Mechanisms underlying cognitive impairment and management strategies in type 2 diabetes. In Frontiers in Endocrinology; Frontiers Media, Oct 2025; vol. 16, pp. 1655768–1655768. [Google Scholar] [CrossRef]
- Lagonigro, E.; Pansini, A.; Mone, P.; Guerra, G.; Komici, K.; Fantini, C. The Role of Stress Hyperglycemia on Delirium Onset. JCM 2025, vol. 14(no. 2), 407. [Google Scholar] [CrossRef] [PubMed]
- Sun, M. , Delirium as a Precursor to Dementia in Elderly Type 2 Diabetes Mellitus Patients. The Journal of Clinical Psychiatry 2025, vol. 86(no. 2). [Google Scholar] [CrossRef] [PubMed]
- Akhtar, S. O. , The Triad of Atrial Fibrillation, Dementia, and Type 2 Diabetes: A Narrative Review of a Complex Interplay. Fortune Journal of Health Sciences 2024, vol. 7(no. 3). [Google Scholar] [CrossRef]
- Moran, C. A study of mechanisms linking type 2 diabetes mellitus and dementia. In OPAL (Open@LaTrobe); La Trobe University, Jan 2017. [Google Scholar] [CrossRef]
- Aslam, M.; Arif, H. The link between type 2 Diabetes Mellitus and Early Onset Alzheimer’s Disease: A Review of shared of Pathophysiological Mechanism. 2025. [Google Scholar] [CrossRef]
- Mercado, F.; Kop, M.; Trinh, M. GLP-1 receptor agonists in delirium and encephalopathies: a neuroprotective scoping review. Discov Med 2025, vol. 2(no. 1), 207. [Google Scholar] [CrossRef]
- Fong, T. G.; Inouye, S. K.; Jones, R. N. Delirium, Dementia, and Decline. JAMA Psychiatry 2017, vol. 74(no. 3), 212–212. [Google Scholar] [CrossRef]
- Cui, W. , Novel targets and therapies of metformin in dementia: old drug, new insights. Frontiers in Pharmacology 2024, vol. 15, 1415740–1415740. [Google Scholar] [CrossRef]
- Sun, M. , Metformin Use and Risk of Delirium in Older Adults With Type 2 Diabetes. Diabetes Care 2024, vol. 48(no. 7), 1172–1179. [Google Scholar] [CrossRef]
- Sun, M. Comparative effectiveness of SGLT2 inhibitors and GLP-1 receptor agonists in preventing Alzheimer’s disease, vascular dementia, and other dementia types among patients with type 2 diabetes. Diabetes Metab 2025, vol. 51(no. 2), 101623. [Google Scholar] [CrossRef]
- Yamanashi, T. , The potential benefit of metformin to reduce delirium risk and mortality: a retrospective cohort study. Aging 2022, vol. 14(no. 22), 8927–8943. [Google Scholar] [CrossRef]
- Grieco, M. , Glucagon-Like Peptide-1: A Focus on Neurodegenerative Diseases. Frontiers Media 2019, vol. 13. [Google Scholar] [CrossRef]
- Gandhi; Parhizgar, A. GLP-1 receptor agonists in Alzheimer’s and Parkinson’s disease: endocrine pathways, clinical evidence, and future directions. Frontiers in Endocrinology 2025, vol. 16. [Google Scholar] [CrossRef]
- TriNetx Networ, LLC, TriNetX Network. Accessed: Jan. 27, 2026. [Online]. Available: https://trinetx.com/.
- Palchuk, M. B. A global federated real-world data and analytics platform for research. JAMIA Open 2023, vol. 6(no. 2). [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D. G.; Egger, M.; Pocock, S.; Gøtzsche, P. C.; Vandenbroucke, J. P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. The Lancet 2007, vol. 370(no. 9596), 1453–1457. [Google Scholar] [CrossRef]
- Simon, T. G.; Patorno, E.; Schneeweiss, S. Glucagon-Like Peptide-1 Receptor Agonists and Hepatic Decompensation Events in Patients With Cirrhosis and Diabetes. Clin Gastroenterol Hepatol 2022, vol. 20(no. 6), 1382–1393.e19. [Google Scholar] [CrossRef]
- Tsipas, S.; Khan, T.; Loustalot, F.; Myftari, K.; Wozniak, G. Spending on Glucagon-Like Peptide-1 Receptor Agonists Among US Adults. JAMA Network Open 2025, vol. 8(no. 4). [Google Scholar] [CrossRef] [PubMed]
- Oldham, M.; Heinrich, T.; Luccarelli, J. Requesting That Delirium Achieve Parity With Acute Encephalopathy in the MS-DRG System. Journal of the Academy of Consultation-Liaison Psychiatry 2024, vol. 65(no. 3), 302–312. [Google Scholar] [CrossRef] [PubMed]
- Piccini, S. , Time-dependent effect of GLP-1 receptor agonists on cardiovascular benefits: a real-world study. In Research Square (Research Square); Jan 2023. [Google Scholar] [CrossRef]
- Chuansangeam, M.; Phadungsaksawasdi, P.; Park, H. J.; Yang, Y.-H. Exploring the link between GLP-1 receptor agonists and dementia: A comprehensive review. In Journal of Alzheimer s Disease Reports; IOS Press, Jan 2025; vol. 9. [Google Scholar] [CrossRef]
- Wium-Andersen, K.; Osler, M.; Jørgensen, M. B.; Rungby, J.; Wium-Andersen, M. K. Antidiabetic medication and risk of dementia in patients with type 2 diabetes: A nested case-control study. Eur. J. Endocrinol. 2019, vol. 181(no. 5), 499–507. [Google Scholar] [CrossRef] [PubMed]
- Wang, W. Associations of semaglutide with first-time diagnosis of Alzheimer’s disease in patients with type 2 diabetes: Target trial emulation using nationwide real-world data in the US. Alzheimers Dement 2024, vol. 20(no. 12), 8661–8672. [Google Scholar] [CrossRef]
- Wang, T.; Buse, J. B.; Pate, V.; Garden, G. A.; Stürmer, T. Liraglutide as a potential drug repurposing candidate for Alzheimer’s disease and related dementia: Real World Evidence. Alzheimer s & Dementia 2023, vol. 19. [Google Scholar] [CrossRef]
- Gupta, D. K.; Chaudhuri, A. The Role of Glucagon-Like Peptide-1 Receptor Agonists in Cognitive Decline and Dementia Prevention: A Systematic Review and Semiquantitative Synthesis. Journal of Mental Health and Human Behaviour 2025, vol. 30(no. 2), 77–83. [Google Scholar] [CrossRef]
- Tipa, R. O. , A Systematic Review of Semaglutide’s Influence on Cognitive Function in Preclinical Animal Models and Cell-Line Studies. IJMS 2024, vol. 25(no. 9), 4972. [Google Scholar] [CrossRef] [PubMed]
- Gejl, M. , In Alzheimer’s disease, 6-month treatment with GLP-1 analog prevents decline of brain glucose metabolism: Randomized, placebo-controlled, double-blind clinical trial. Front. Aging Neurosci. 2016, vol. 8, no. MAY. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Doré, V.; Rowe, C. C.; Krishnadas, N. Clinical Evidence for GLP-1 Receptor Agonists in Alzheimer’s Disease: A Systematic Review. Journal of Alzheimer’s Disease Reports 2024, vol. 8(no. 1), 777–789. [Google Scholar] [CrossRef]
- Sun, M. , Evaluating GLP-1 receptor agonists versus metformin as first-line therapy for reducing dementia risk in type 2 diabetes. BMJ Open Diabetes Res Care 2025, vol. 13(no. 4), e004902. [Google Scholar] [CrossRef]
- Seminer. Cardioprotective Glucose-Lowering Agents and Dementia Risk. In JAMA Neurology; American Medical Association, Apr 2025; vol. 82, no. 5, pp. 450–450. [Google Scholar] [CrossRef]
- Ceasovschih. , Glucagon-like peptide-1 receptor agonists and muscle mass effects. Pharmacological Research 2025, vol. 220, 107927–107927. [Google Scholar] [CrossRef]
- Sun, M. , Long-term delirium and survival outcomes in patients treated with GLP -1 receptor agonists versus metformin in type 2 diabetes: A population-based cohort study. Diabetes Obesity Metabolism 2025, vol. 27(no. 7), 3984–3996. [Google Scholar] [CrossRef]
- Rahman. , Sex and Gender Driven Modifiers of Alzheimer’s: The Role for Estrogenic Control Across Age, Race, Medical, and Lifestyle Risks. Frontiers in Aging Neuroscience 2019, vol. 11, 315–315. [Google Scholar] [CrossRef]
- Lee, M. M. Y. Comparative Efficacy of Glucagon-Like Peptide 1 Receptor Agonists for Cardiovascular Outcomes in Asian Versus White Populations: Systematic Review and Meta-analysis of Randomized Trials of Populations With or Without Type 2 Diabetes and/or Overweight or Obesity. Diabetes Care 2025, vol. 48(no. 3), 489–493. [Google Scholar] [CrossRef]
- Tsoy, E. , Assessment of Racial/Ethnic Disparities in Timeliness and Comprehensiveness of Dementia Diagnosis in California. JAMA Neurology 2021, vol. 78(no. 6), 657–657. [Google Scholar] [CrossRef]
- Cheng, C.-K.; Tsao, Y.-C.; Su, Y.-C.; Sung, F.-C.; Tai, H.-C.; Kung, W.-M. Metabolic Risk Factors of Alzheimer’s Disease, Dementia with Lewy Bodies, and Normal Elderly: A Population-Based Study. Behavioural Neurology 2018, vol. 2018, 1–8. [Google Scholar] [CrossRef]
- Ahmed, R. M. Metabolism in frontotemporal dementia. Alzheimer s & Dementia 2021, vol. 17. [Google Scholar] [CrossRef]
- Prado, M.; Batsis, J. A.; Donini, L. M.; González, M. C.; Siervo, M. Sarcopenic obesity in older adults: a clinical overview. In Nature Reviews Endocrinology; Nature Portfolio, Feb 2024; vol. 20, no. 5, pp. 261–277. [Google Scholar] [CrossRef]
- Holmberg, M. J.; Andersen, L. W. Collider Bias. JAMA 2022, vol. 327(no. 13), 1282–1282. [Google Scholar] [CrossRef]
- Barrett, E. , Reduced GLP-1R availability in the caudate nucleus with Alzheimer’s disease. Frontiers in Aging Neuroscience 2024, vol. 16, 1350239–1350239. [Google Scholar] [CrossRef]
- Lu, Y. Association of Glucagon-Like Peptide-1 Receptor Agonists With Cancer Risk in Older Adults With Type 2 Diabetes. Obesity 2025. [Google Scholar] [CrossRef]
- Bradley. Persistent inpatient delirium associated with increased length of stay and mortality. PLoS ONE 2025, vol. 20(no. 9). [Google Scholar] [CrossRef]

Table 2.
Time-dependent AHR and OR for all-cause mortality for older adults with T2DM receiving GLP-1 RA compared to metformin. This table shows a consistent odds reduction in all-cause mortality up to 10 years of follow-up; the hazard ratio for all-cause mortality diminishes over time and becomes not statistically significant from 5 to 10 years of follow-up.
Table 2.
Time-dependent AHR and OR for all-cause mortality for older adults with T2DM receiving GLP-1 RA compared to metformin. This table shows a consistent odds reduction in all-cause mortality up to 10 years of follow-up; the hazard ratio for all-cause mortality diminishes over time and becomes not statistically significant from 5 to 10 years of follow-up.
| All-cause mortality | OR | AHR |
| Complete follow-up | 0.728 (95% CI 0.701 −0.756) p < 0.001 | 0.927 (95% CI 0.899 −0.956) p < 0.001 |
| 0-5 years follow-up | 0.765 (95% CI 0.737, 0.795) p < 0.001 | 0.915 (95% CI 0.887, 0.944) p < 0.001 |
| 5-10 years follow-up | 0.315 (95% CI 0.262, 0.378) p < 0.001 | 1.092 (95% CI 0.911, 1.31) p 0.342 |
Abbreviations: CI: confidence interval; OR: odds ratio; AHR: adjusted hazard ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



