Submitted:
29 January 2026
Posted:
30 January 2026
You are already at the latest version
Abstract
Dermatophytosis is a superficial fungal skin disease of cats and dogs. The most common pathogen of small animals belongs to the genera Microsporum and Trichophyton. It is an important skin disease because it is contagious and can be transmitted to people. Refractory dermatophytosis has become an increasing concern in dermatological practice due to poor response to standard antifungal therapy. The condition is characterised by chronicity, recurrence or persistence despite adequate treatment. This study aimed to assess the clinical profile and therapeutic outcomes in patients with refractory dermatophytosis. An 8-year-old intact male Spitz dog weighing 10 kg, presented with persistent alopecia, scaling, erythema and pruritus despite multiple courses of systemic and topical antifungal agents. Diagnosis was confirmed by microscopic examination, culture and punch biopsy. Due to the lack of response to standard therapy, Posaconazole was initiated based on antifungal susceptibility testing (AFST); however, AFST is not routinely performed for dermatophytosis, although it may provide valuable guidance in refractory infections by identifying reduced susceptibility or resistance to commonly used antifungal agents. Marked clinical improvement was observed, with complete clinical and mycological cure achieved without adverse effects. This report highlights a case of refractory dermato-phytosis in which antifungal susceptibility testing guided the successful use of Posaconazole. The case highlights the diagnostic challenges associated with recurrent dermatophytosis and underscores the potential role of antifungal susceptibility-guided therapy in managing treatment-resistant infections. Hence, Posaconazole is a promising alternative antifungal agent for managing refractory dermatophytosis in dogs.

Keywords:
antifungal therapy
; dermatophytosis
; posaconazole
; spitz dog
; refractory infection
1. Introduction
Dermatophytosis is a common superficial fungal infection in dogs, typically responsive to routine antifungal therapy [1]. However, refractory dermatophytosis is characterized by persistence or recurrence despite adequate treatment, which has been increasingly reported in recent years [2]. Contributing factors include inappropriate drug selection, inadequate treatment duration, poor owner compliance and possible antifungal resistance [3]. Posaconazole, a second-generation triazole antifungal, has a broad spectrum of activity and may serve as a salvage therapy in refractory cases [4].
2. Case Presentation
An eight-year-old intact male Spitz dog weighing 10 kg was presented with a history of chronic dermatological lesions persisting for 11 months. Clinical examination revealed multifocal alopecia, erythema, scaling, and pruritus, predominantly involving the face, trunk, and limbs (Figure 1). The dog had initially been diagnosed with fungal dermatitis and treated with oral itraconazole at a dose of 10 mg/kg body weight as pulse therapy for 1 month, along with topical antifungal therapy consisting of a 2% miconazole shampoo and terbinafine dusting powder. A relapse was observed four weeks after cessation of therapy, following which the same treatment protocol was repeated multiple times by the pet owner without consultation. Subsequently, hepatotoxicity was detected, with elevated alanine aminotransferase (ALT; 275 U/L) and alkaline phosphatase (ALP; 350 U/L) levels, while the complete blood count remained within normal limits. Antifungal treatment was therefore discontinued. Upon re-evaluation, hair samples were collected for fungal culture and antifungal susceptibility testing. Deep skin scrapings were negative for ectoparasites. A direct impression smear was prepared for cytological examination, which revealed multiple fungal spores. Skin biopsies were obtained to rule out underlying immune-mediated dermatological conditions. Histopathological examination demonstrated fungal spores within the hair follicles (Figure 2). Fungal culture yielded growth of Microsporum canis after 14 days of incubation. Antifungal susceptibility testing showed sensitivity to amphotericin B, posaconazole, and voriconazole, while resistance was noted to routinely used antifungal agents (Table 1). Prior to initiating further systemic antifungal therapy, serum biochemical parameters were reassessed, and ALT and ALP values were within the normal reference range. Based on the susceptibility results, posaconazole was administered orally at a dose of 10 mg/kg once daily (Poshope DR®, Abbott Healthcare Pvt. Ltd.) for three weeks, followed by 5 mg/kg once daily for an additional three weeks. Liver enzyme levels were monitored regularly throughout the treatment period. Adjunctive topical therapy with an essential fatty acid-based shampoo (Essential 6 Sebo Shampoo®, Dermoscent Laboratoire) was administered once weekly. Progressive clinical improvement was observed within five weeks of initiating posaconazole therapy, characterised by a marked reduction in erythema and scaling, followed by gradual hair regrowth (Figure 3). During treatment, a mild elevation in serum ALT levels was noted during routine biochemical monitoring. Hepatoprotective supplements were administered throughout posaconazole therapy and continued for 2 weeks after its discontinuation. At the completion of treatment, complete clinical resolution was achieved and repeat mycological examination yielded negative results.
4. Discussion
Canine dermatophytosis is a common contagious and zoonotic superficial fungal infection affecting keratinized tissues such as hair, stratum corneum and claws. It is most frequently caused by Microsporum Canis, Microsporum gypsum and Trichophyton mentagrophytes complex. Although the majority of the cases respond well to appropriate systemic antifungal therapy combined with topical management and environmental decontamination, treatment failures, relapses and chronic infections are increasingly recognized in clinical practice, particularly in cases with extensive disease, poor compliance, repeated empirical antifungal use, or underlying host and environmental factors [1]. There is currently no universally accepted definition of refractory dermatophytosis in veterinary medicine. Clinically, it may be defined as persistent or recurrent dermatophyte infection despite adequate duration and dosage of appropriate antifungal therapy, with confirmed owner compliance and environmental control, or failure to achieve mycological cure after repeated courses of standard antifungal agents [1,2]. Refractory disease warrants a more advanced diagnostic and therapeutic approach, including fungal species identification, histopathology, and antifungal susceptibility testing (AFST). Diagnosis of dermatophytosis is typically based on clinical presentation, direct microscopy, woods lamp examination, fungal culture, and in selected cases, histopathology. However, recurrent or refractory infections pose significant diagnostic challenges. Prior antifungal therapy can reduce the fungal load and lead to false-negative cultures, emphasising the importance of appropriate sample collection from active lesion margins and, when indicated, skin biopsy with special stains such as periodic acid-Schiff (PAS) to demonstrate fungal elements within hair follicles and the stratum corneum [1,5]. Identification of the dermatophyte species through fungal culture remains a critical step, as different species may exhibit variations in pathogenicity, environmental persistence, zoonotic potential, and antifungal susceptibility profiles [2]. In the present case, fungal culture and histopathology confirmed dermatophytosis after recurrent clinical disease, supporting the diagnosis of refractory dermatophytosis.
Antifungal susceptibility testing is not routinely recommended for uncomplicated dermatophytosis, as most infections respond to first-line agents such as itraconazole or terbinafine. Nevertheless, AFST becomes clinically relevant in refractory cases, especially when animals have been exposed to multiple antifungal drugs without sustained clinical or mycological cure [2]. In the present case, AFST demonstrated resistance to several commonly used antifungal agents, while Posaconazole showed in vitro susceptibility. This finding justified selecting Posaconazole as salvage therapy, despite its limited routine use in veterinary dermatology. Posaconazole is a second-generation triazole antifungal agent with a broad spectrum of activity against yeast and fungi. It acts by inhibiting fungal cytochrome P450-dependent 14α-demethylase, thereby disrupting ergosterol synthesis and fungal cell membrane integrity [6]. In human medicine, Posaconazole is widely used for prophylaxis and treatment of invasive fungal infections. In veterinary medicine, its use is limited, primarily due to cost, limited availability, and a lack of dermatology-specific clinical data. In vitro studies have demonstrated that Posaconazole exhibits potent activity against dermatophyte isolates with minimum inhibitory concentrations comparable to or lower than those of itraconazole in some studies [7]. However, published veterinary clinical reports on the use of posaconazole specifically for dermatophytosis are scarce. Most veterinary reports describe its use in systemic mycosis such as histoplasmosis and cryptococcosis, particularly in cats and dogs refractory to first-line azoles [8,9]. Human literature provides additional indirect support for its use, as Posaconazole has been successfully used in severe, extensive or treatment-resistant dermatophytosis, particularly in immunocompromised patients [10]. Together with AFST-guided susceptibility results, these data support the rational use of Posaconazole in refractory canine dermatophytosis. Systemic azole antifungals are associated with potential hepatotoxicity, especially during prolonged therapy. Therefore, baseline and periodic monitoring of serum biochemistry, including liver enzymes, is recommended. When posaconazole or other azoles are administered long term [1,7,11]. In the present case, routine haematology and serum biochemistry were performed to monitor hepatic function, and liver–supportive therapy was administered concurrently, which may have contributed to the favourable outcome.
Successful management of refractory dermatophytosis requires a multimodal approach that combines systemic antifungal therapy guided by susceptibility testing, topical therapy to reduce the fungal burden, and strict environmental hygiene. Topical therapy, including antifungal or essential fatty acid-based shampoos, plays an important role in decreasing surface contamination, reducing environmental shedding, and limiting zoonotic transmission [1,12].
Dermatophytosis is a recognised zoonosis, and infected animals may serve as a source of infection for humans, particularly children, the elderly, and immunocompromised individuals. Owner education regarding hygiene, environmental decontamination, and avoidance of contact by high-risk individuals is therefore essential and was emphasised in the present case.
In this case, posaconazole therapy combined with topical management and liver support resulted in marked clinical improvement within four weeks and complete resolution by eight weeks. Treatment was continued beyond clinical resolution to reduce the risk of relapse. Although the cost of posaconazole remains a major limitation for long-term use, this case demonstrates that AFST-guided posaconazole therapy can be an effective and rational option in refractory canine dermatophytosis.
5. Conclusions
This case highlights the potential role of posaconazole as an effective alternative for resistant dermatophytosis in dogs. When standard antifungal therapy fails, Posaconazole may achieve both clinical and mycological cure, provided that appropriate dosing, treatment duration and monitoring protocol are followed. Due to limited veterinary-specific data, Posaconazole should be reserved for refractory infections and ideally guided by fungal culture and susceptibility testing. Further controlled clinical studies are needed to better define its efficacy, safety profile, and optimal therapeutic protocols in canine dermatophytosis.
Funding
This research received no external funding.
Author Contributions:
Conceptualisation, A.T.; Investigation, Writing – original draft: Anisha Tiwari; Data curation, Investigation: Bhanu Kirti Khajuria; Supervision, writing – review and editing: Curtis Plowgian; Supervision, writing – review and editing: Cheol-Yong Hwang.
Institutional Review Board Statement
- Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
The authors thank the clinical and technical staff of Suvidha Pet Care and Derma Centre and Suvidha Vet Care and Research Centre for their invaluable assistance in patient care and surgical support during the procedure. We are grateful to the pet owner for their cooperation and trust throughout the treatment and follow-up period.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Moriello, K.A.; Coyner, K.; Paterson, S.; Mignon, B. Diagnosis and treatment of dermatophytosis in dogs and cats: Clinical consensus guidelines of the World Association for Veterinary Dermatology. Vet. Dermatol. 2017,28, 266–e68.
- Martinez-Rossi, N.M.; Bitencourt, T.A.; Peres, N.T.A.; Lang, E.A.S.; Gomes, E.V.; Quaresemin, N.R.; Martins, M.P.; Lopes, L.; Rossi, A. Dermatophyte Resistance to Antifungal Drugs: Mechanisms and Prospectus. Front. Microbiol.2018, 9, 1108. [CrossRef]
- Moriello, K.A. Dermatophytosis in Cats and Dogs: A Practical Guide to Diagnosis and Treatment. In Pract. 2019, 41, 138–147. [CrossRef]
- Shubitz, L.F.; Trinh, H.T.; Galgiani, J.N. Posaconazole Treatment of Refractory Fungal Infections in Dogs. J. Vet. Intern. Med. 2021, 35, 2731–2738.
- Miller, W.H.; Griffin, C.E.; Campbell, K.L. Muller and Kirk’s Small Animal Dermatology, 7th ed.; Elsevier: St. Louis, MO, USA, 2013; pp. 223–261.
- Groll, A.H.; Walsh, T.J. Posaconazole: Clinical Pharmacology and Potential for Management of Fungal Infections. Expert Rev. Anti Infect. Ther. 2005, 3, 467–487. [CrossRef]
- Pennisi, M.G.; Hartmann, K.; Lloret, A.; Ferrer, L.; Addie, D.; Belák, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; et al. Cryptococcosis in Cats: ABCD Guidelines on Prevention and Management. J. Feline Med. Surg. 2013, 15, 611–618. [CrossRef]
- Pennisi, M.G.; Hartmann, K.; Lloret, A.; Ferrer, L.; Addie, D.; Belák, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; et al. Cryptococcosis in Cats: ABCD Guidelines on Prevention and Management. J. Feline Med. Surg. 2013, 15, 611–618. https://doi.org/10.1177/1098612x13489224.
- Plumb, D.C. Plumb’s Veterinary Drug Handbook, 9th ed.; Wiley-Blackwell: Ames, IA, USA, 2018.
- Ebert, A.; Monod, M.; Salamin, K.; Burmester, A.; Uhrlaß, S.; Wiegand, C.; Hipler, U.-C.; Krüger, C.; Koch, D.; Wittig, F.; et al. Alarming India-Wide Phenomenon of Antifungal Resistance in Dermatophytes: A Multicentre Study. Mycoses 2020, 63, 717–728. https://doi.org/10.1111/myc.13091. [CrossRef]
- Plumb, D.C. Plumb’s Veterinary Drug Handbook, 9th ed.; Wiley-Blackwell: Ames, IA, USA, 2018.
- Hobi, S.; Cafarchia, C.; Romano, V.; Barrs, V.R. Malassezia: Zoonotic Implications, Parallels and Differences in Colonization and Disease in Humans and Animals. J. Fungi 2022, 8, 708. [CrossRef]
Figure 1.
(a) Fascial dermatologic lesions at initial presentation, characterised by alopecia, erythema and crusting, (b) Diffuse erythema with multifocal hyperpigmentation and alopecia on the dorsolateral trunk.
Figure 1.
(a) Fascial dermatologic lesions at initial presentation, characterised by alopecia, erythema and crusting, (b) Diffuse erythema with multifocal hyperpigmentation and alopecia on the dorsolateral trunk.
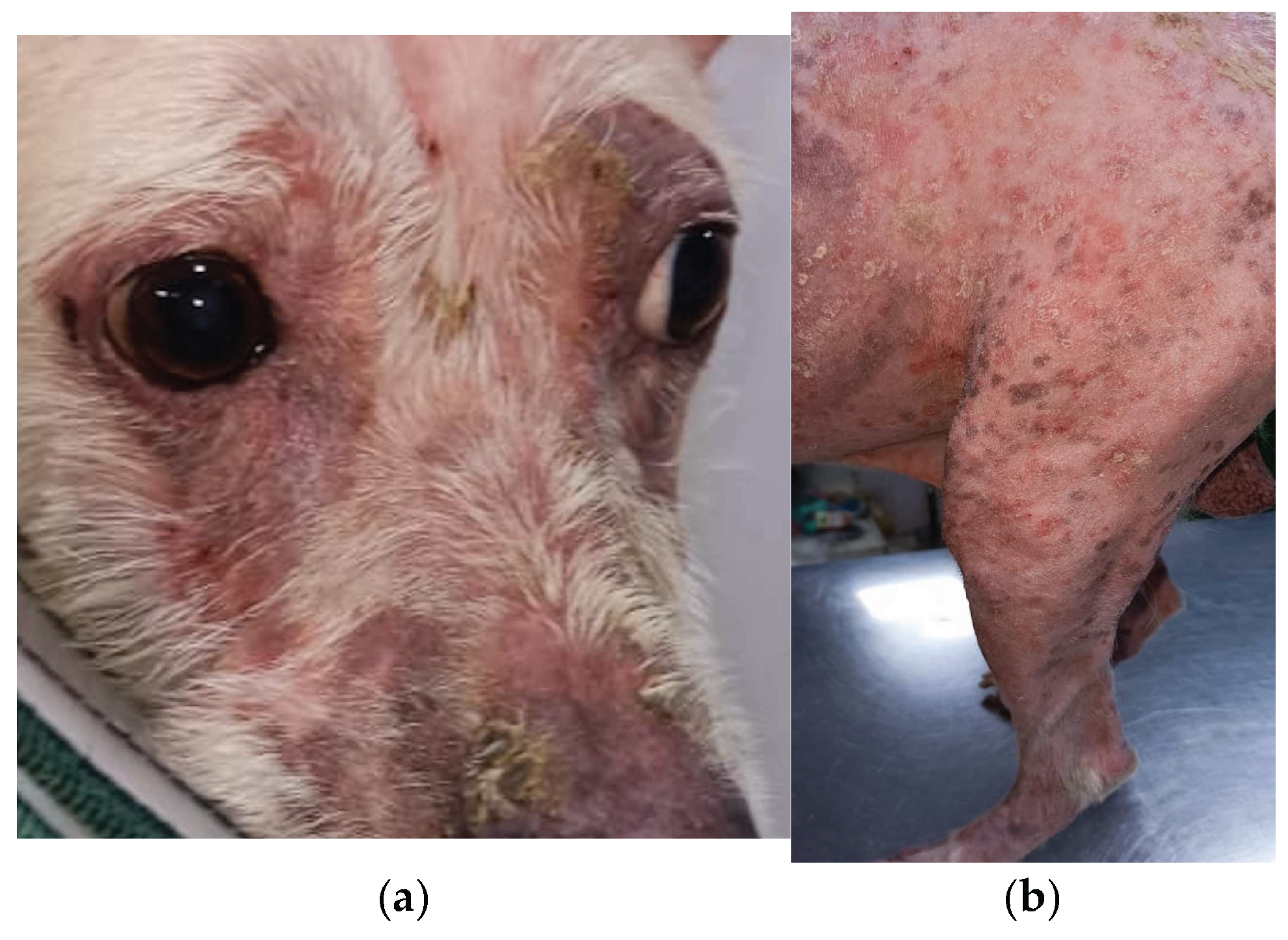
Figure 2.
(c) Fungal spores observed on cytology (x100) using Diff-Quik stain (d) Punch biopsy (PAS, x10) showing fungal spores within the hair follicle.
Figure 2.
(c) Fungal spores observed on cytology (x100) using Diff-Quik stain (d) Punch biopsy (PAS, x10) showing fungal spores within the hair follicle.
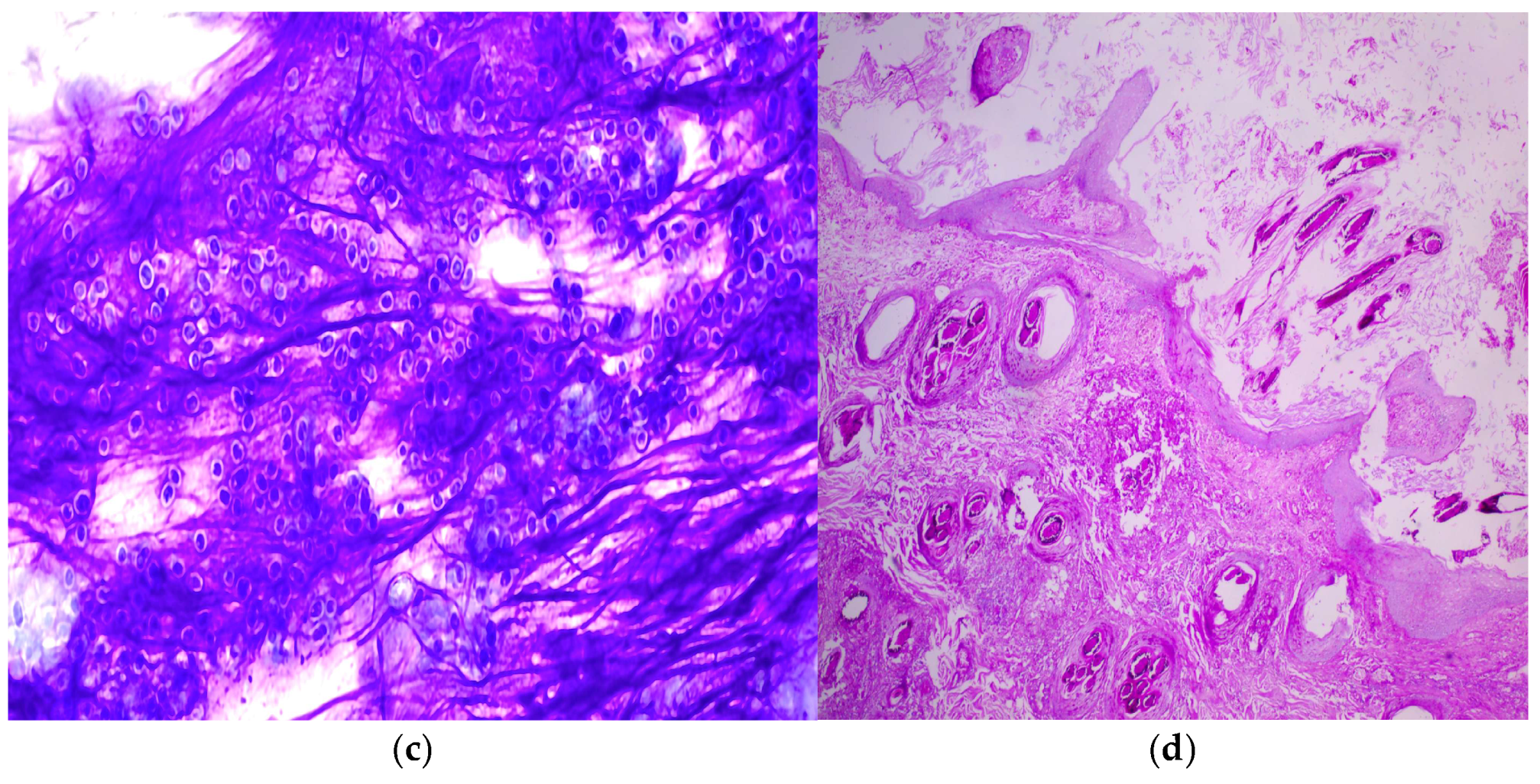
Figure 3.
(e & f) Hair regrowth and resolution of cutaneous lesions after 8 weeks of posaconazole therapy.
Figure 3.
(e & f) Hair regrowth and resolution of cutaneous lesions after 8 weeks of posaconazole therapy.


Table 1.
Anti – Fungal Drug Sensitivity Test.
| Anti-Fungal Drug | Interpretation |
|---|---|
| Amphotericin B | Susceptible dose dependent |
| Itraconazole | Resistant |
| Ketaconazole | Resistant |
| Fluconazole | Resistant |
| Posaconazole | Susceptible dose dependent |
| Variconazole | Susceptible dose dependent |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



