Submitted:
29 January 2026
Posted:
30 January 2026
You are already at the latest version
Abstract
Gluten-related disorders (GRDs) comprise a heterogeneous group of immune-mediated and immune-associated conditions triggered by gluten or wheat exposure, including celiac disease, non-celiac gluten sensitivity, and wheat allergy. Although traditionally regarded as gastrointestinal disorders, GRDs are increasingly recognized as systemic conditions with clinically relevant involvement of the central nervous system and the cardiovascular system. Neurological, psychiatric, autonomic, and cardiovascular manifestations are now understood to represent integral components of the disease phenotype rather than incidental comorbidities. This narrative review examines current evidence on the mechanisms linking gluten-related immune activation to brain and heart dysfunction, highlighting convergent inflammatory, autoimmune, neuroimmune, and endothelial pathways. Emphasis is placed on the gut-brain-heart axis, alterations of epithelial and blood-brain barrier integrity, autonomic dysregulation, and vascular dysfunction. The potential reversibility of selected neurocardiac manifestations through dietary and immunologically targeted interventions is also discussed. A systems-level understanding of brain-heart interactions in GRDs may improve diagnostic accuracy, inform cardiovascular and neurological risk stratification, and support more integrated, holistic management strategies for affected patients.
Keywords:
gluten-related disorders
; celiac disease
; gut-brain-heart axis
; neuroimmune interactions
; autonomic dysfunction
; cardiovascular involvement
; blood-brain barrier dysfunction
Introduction
Gluten-related disorders (GRDs) comprise a spectrum of conditions triggered by exposure to gluten or wheat proteins and have traditionally been regarded as disorders confined to the gastrointestinal tract, with small-intestinal mucosal injury and resultant malabsorption representing their defining pathological features [1]. However, celiac disease, the most extensively studied GRD, is now recognized as a multisystem immune-mediated disorder with significant extra-intestinal involvement, including neurologic and psychiatric manifestations such as ataxia, neuropathy, and cognitive dysfunction, as well as systemic features that extend beyond the gut [2]. The global prevalence of celiac disease is estimated at approximately 1% of the population, though significant geographic and ethnic variation exists, with many cases remaining undiagnosed due to atypical or subclinical presentations [3]. Extra-intestinal manifestations have been documented across dermatologic, endocrinologic, hepatic, musculoskeletal, and hematologic systems, underscoring the systemic impact of the disease [4].
The spectrum of GRDs also includes non-celiac gluten sensitivity and wheat allergy. While the immunopathogenesis of these entities differs from that of celiac disease, evidence supports their capacity to induce systemic symptoms, including neurological complaints and neuropsychiatric features that may improve following gluten exclusion [5]. This broader phenotypic variability has challenged the traditional organ-centric view and has prompted a systems-based perspective.
Advances in neuroimmunology and cardiovascular immunology have led to the concept of integrated communication networks linking the gut, brain, and heart through immune, neural, and metabolic pathways. Within this framework, immune signals originating in the gastrointestinal tract, including cytokines and other mediators associated with increased intestinal permeability, may influence central autonomic circuits, vascular function, and cardiomyocyte signaling, providing a mechanistic substrate for neurologic and cardiovascular manifestations observed in GRDs [6].
Against this background, the present narrative review aims to critically examine the influence of GRDs on brain and heart function, integrating mechanistic, clinical, and translational evidence. By adopting a brain-heart systems perspective, this work seeks to move beyond compartmentalized symptom descriptions and to provide a coherent framework for understanding gluten-driven multisystem pathology.
Methods
This narrative review was conducted and reported in accordance with the Scale for the Assessment of Narrative Review Articles (SANRA), a validated instrument developed to improve the transparency, methodological rigor, and scientific quality of narrative syntheses in biomedical research [7]. The SANRA framework was adopted prospectively to guide the conceptualization, literature selection, and synthesis process, with explicit attention to its six core domains: (i) justification of the narrative review format, (ii) clarity of objectives, (iii) adequacy of the literature search, (iv) appropriateness and consistency of referencing, (v) scientific reasoning, and (vi) balanced presentation of evidence.
A structured but flexible literature search strategy was applied to identify peer-reviewed publications addressing the neurological and cardiovascular implications of GRDs, including celiac disease, non-celiac gluten sensitivity, and wheat allergy. Searches were performed in MEDLINE/PubMed, Scopus, and Web of Science, using combinations of controlled vocabulary and free-text terms related to GRDs, extra-intestinal manifestations, neuroimmune mechanisms, autonomic dysfunction, cardiovascular involvement, and gut-brain interactions. To ensure conceptual completeness, reference lists of key articles and authoritative reviews were manually screened by two authors (YVT and PVP). The search encompassed literature published from database through December 2025, with priority given to studies published within the past 10 years to capture contemporary understanding of brain-heart interactions in GRDs.
Eligible sources included original clinical studies, epidemiological investigations, translational and mechanistic research, consensus documents, and high-quality narrative or systematic reviews published in English. Animal and in vitro studies were considered selectively when they provided mechanistic insight directly relevant to human pathophysiology. Editorials, opinion pieces, and non-peer-reviewed sources were excluded. Study selection emphasized relevance, methodological robustness, and contribution to mechanistic or clinical understanding rather than formal evidence hierarchies, consistent with the exploratory aims of a SANRA-guided narrative review.
Data extraction focused on “immuno-pathophysiology of gluten-related disorders”, “central nervous system involvement in gluten-related disorders”, “cardiovascular involvement in gluten-related disorders”, “the gut-brain-heart axis in gluten-related disorders”, “therapeutic implications and reversibility of brain-heart effects”. Evidence was synthesized qualitatively using a thematic, systems-based approach, highlighting areas of convergence, divergence, and uncertainty across disease entities (Table 1). Conflicting findings were explicitly acknowledged to minimize interpretative bias.
Results
Immuno-Pathophysiology of Gluten-Related Disorders
- Adaptive and innate immune activation
Celiac disease represents the prototypical autoimmune form of GRD and is characterized by a highly specific adaptive immune response to dietary gluten in genetically predisposed individuals. Susceptibility is strongly associated with the expression of HLA-DQ2 and/or HLA-DQ8 molecules, which present deamidated gliadin peptides to CD4⁺ T lymphocytes in the intestinal lamina propria. Approximately 90-95% of celiac disease patients carry HLA-DQ2, while most of the remaining cases express HLA-DQ8, though these alleles are necessary but not sufficient for disease development, as they are also present in approximately 30-40% of the general population [8]. Tissue transglutaminase 2 plays a central pathogenic role by deamidating gliadin peptides, thereby increasing their affinity for HLA-DQ2/DQ8 and amplifying T-cell activation. This process culminates in a Th1-skewed inflammatory response dominated by interferon-γ production, leading to crypt hyperplasia and villous atrophy [9].
Although the small intestine is the primary site of injury, celiac disease is now recognized as a systemic immune-mediated disorder. Activated gluten-specific T cells, pro-inflammatory cytokines, and circulating autoantibodies, most notably anti-tissue transglutaminase antibodies, can disseminate systemically and interact with extra-intestinal tissues. Given the widespread expression of tissue transglutaminase in the nervous system, myocardium, and vascular endothelium, autoimmune cross-reactivity provides a biologically plausible mechanism for neurological and cardiovascular involvement [9].
In contrast, non-celiac gluten sensitivity is characterized by the absence of villous atrophy and celiac-specific autoantibodies, yet increasing evidence supports a distinct biological basis. Consensus definitions describe a predominant role for innate immune activation, epithelial stress responses, and altered intestinal permeability, rather than classical adaptive autoimmunity. These mechanisms are thought to generate low-grade systemic inflammation capable of producing extra-intestinal symptoms despite preserved mucosal architecture [10].
Wheat allergy represents a mechanistically distinct entity within the spectrum of GRDs. It is mediated by IgE-dependent hypersensitivity reactions, in which allergen-specific IgE cross-linking on mast cells and basophils induces rapid release of histamine and other vasoactive mediators. These responses may produce acute gastrointestinal, neurological, and cardiovascular manifestations, reflecting transient neurovascular and hemodynamic effects rather than chronic immune-mediated tissue injury [11].
- 2.
- Intestinal barrier dysfunction and systemic immune signaling
A unifying pathophysiological feature across gluten-related disorders is altered intestinal barrier integrity. Disruption of tight-junction regulation increases paracellular permeability, facilitating the translocation of gluten peptides, microbial products, and inflammatory mediators into the systemic circulation. The regulation of intestinal permeability through zonulin-dependent mechanisms has been proposed as a key link between gluten exposure, immune activation, and extra-intestinal disease vulnerability [12]. Systemic dissemination of these immune signals provides a mechanistic substrate for distant organ involvement, including effects on the central nervous system and the cardiovascular system.
Figure 1.
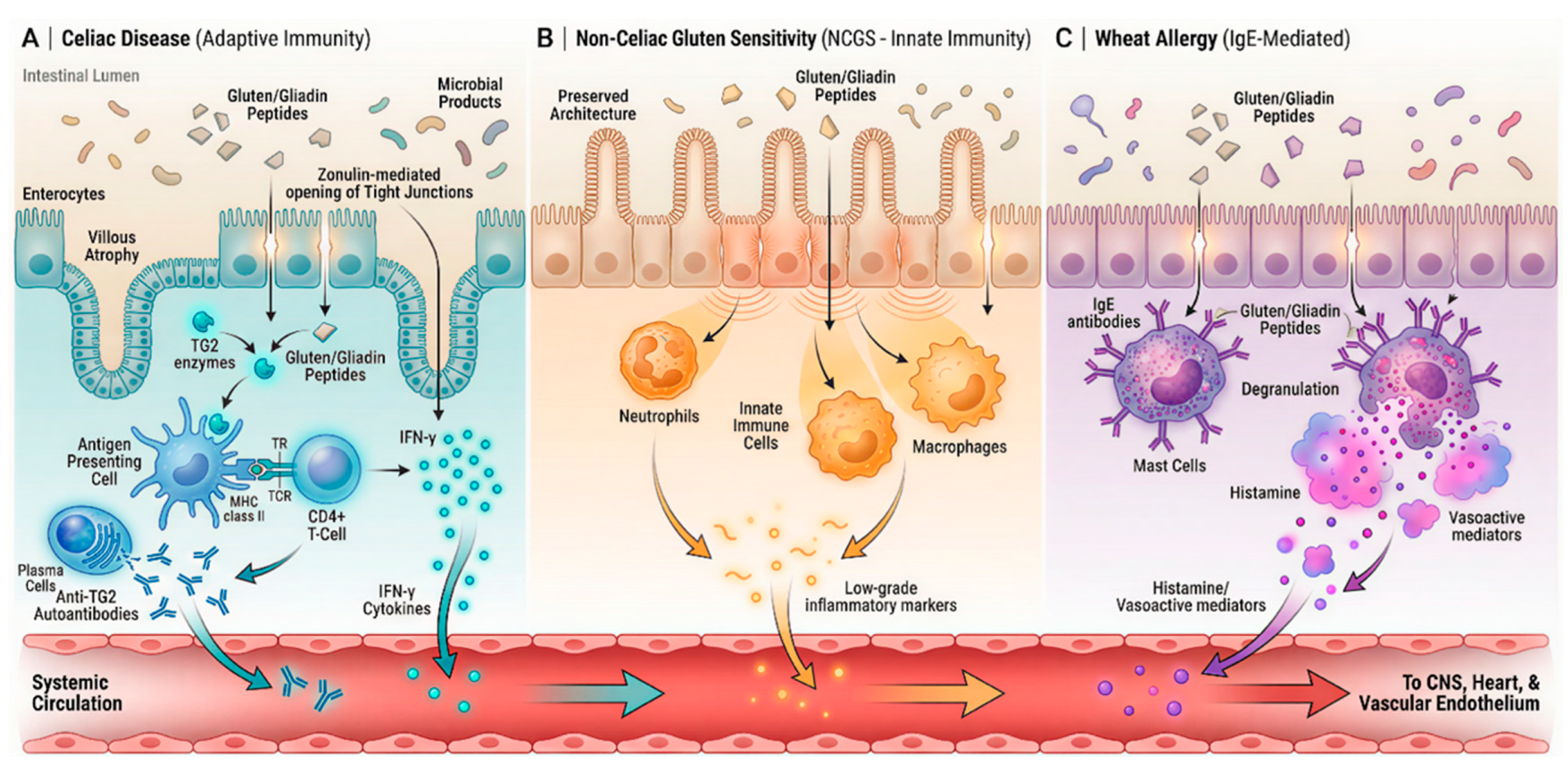
Comparative immunopathophysiology and systemic dissemination in GRDs. (A) In celiac disease, TG2 deamidates gliadin peptides, enabling HLA-DQ2/DQ8-mediated Th1 activation and anti-TG2 autoantibody production, culminating in small-intestinal villous atrophy [13]. (B) Non-celiac gluten sensitivity preserves villous architecture; innate immune activation and epithelial stress generate low-grade inflammation and varied extra-intestinal symptoms [14]. (C) Wheat allergy is an IgE-mediated hypersensitivity in which allergen-specific IgE cross-links on mast cells, releasing histamine and cytokines that cause acute reactions [15]. Across these conditions, increased intestinal permeability may allow luminal antigens and inflammatory mediators into circulation, potentially damaging distant organs including brain and heart [16].
Figure 1.
Comparative immunopathophysiology and systemic dissemination in GRDs. (A) In celiac disease, TG2 deamidates gliadin peptides, enabling HLA-DQ2/DQ8-mediated Th1 activation and anti-TG2 autoantibody production, culminating in small-intestinal villous atrophy [13]. (B) Non-celiac gluten sensitivity preserves villous architecture; innate immune activation and epithelial stress generate low-grade inflammation and varied extra-intestinal symptoms [14]. (C) Wheat allergy is an IgE-mediated hypersensitivity in which allergen-specific IgE cross-links on mast cells, releasing histamine and cytokines that cause acute reactions [15]. Across these conditions, increased intestinal permeability may allow luminal antigens and inflammatory mediators into circulation, potentially damaging distant organs including brain and heart [16].
Central Nervous System Involvement in Gluten-Related Disorders
- Neurological manifestations
Central nervous system involvement represents one of the most clinically significant extra-intestinal dimensions of gluten-related disorders. In celiac disease, neurological manifestations are well documented and include cerebellar ataxia, peripheral neuropathy, epilepsy, headache syndromes, and varying degrees of cognitive impairment [2]. Moreover, neurological complications occur in approximately 6-10% of patients with celiac disease, with peripheral neuropathy being the most common manifestation, followed by ataxia and seizure disorders [17,18]. Importantly, these manifestations may occur independently of gastrointestinal symptoms, contributing to delayed diagnosis and under-recognition of the neurological phenotype of the disease [19]. The prevalence and diversity of these manifestations support the concept that celiac disease should be regarded as a systemic disorder with direct neurological relevance rather than a purely intestinal condition [20].
Among neurological presentations, gluten ataxia constitutes a paradigmatic immune-mediated disorder characterized by progressive gait instability, limb ataxia, and cerebellar dysfunction [2]. Mechanistically, this condition is thought to arise from immune cross-reactivity, whereby antibodies generated in response to gluten-related antigens target neuronal structures within the cerebellum, leading to Purkinje cell dysfunction and neurodegeneration. Notably, neurological injury may progress despite minimal or absent enteropathy, underscoring the dissociation between intestinal and neural involvement [20].
Beyond overt neurological syndromes, many patients with GRDs report nonspecific but functionally disabling symptoms such as impaired concentration, reduced mental clarity (“brain fog”), memory difficulties, and slowed information processing [21]. These symptoms are particularly prominent in non-celiac gluten sensitivity and often lack clear correlates on conventional neuroimaging. Although their pathophysiology remains incompletely defined, proposed mechanisms include low-grade neuroinflammation, altered synaptic signaling, and immune-mediated modulation of neurotransmitter systems. Despite their subtle presentation, these cognitive complaints can substantially impair quality of life and occupational functioning.
- 2.
- Psychiatric and affective dimensions
Psychiatric manifestations are increasingly recognized as integral components of the GRD phenotype. Epidemiological and clinical studies have reported increased rates of anxiety, depressive symptoms, mood disturbances, and behavioral changes in individuals with celiac disease [22]. While psychosocial factors related to chronic illness and dietary restriction undoubtedly contribute (and this topic should be better analyzed), biological mechanisms linking immune activation to affective dysregulation are increasingly emphasized. Systemic inflammation can influence central neurotransmission, neuroendocrine stress responses, and emotional regulation, providing a plausible mechanistic bridge between gluten-driven immune activity and psychiatric symptoms. Importantly, improvement of neuropsychiatric symptoms has been observed in a subset of patients following strict gluten withdrawal, supporting a contributory role of gluten-related immune mechanisms rather than a purely reactive or psychosomatic explanation [22].
- 3.
- Blood–brain barrier dysfunction and neuroimmune interactions
A critical link between peripheral immune activation and central nervous system involvement is the integrity of the blood-brain barrier. Systemic inflammation associated with gluten-related immune responses may compromise barrier function, facilitating the entry of cytokines, immune complexes, and autoantibodies into the central nervous system [23]. The detection of anti-tissue transglutaminase or other gluten-related antibodies in cerebrospinal fluid in selected patients supports the concept of direct immune-mediated neural injury and highlights the role of neuroimmune interactions in disease expression.
Figure 2.
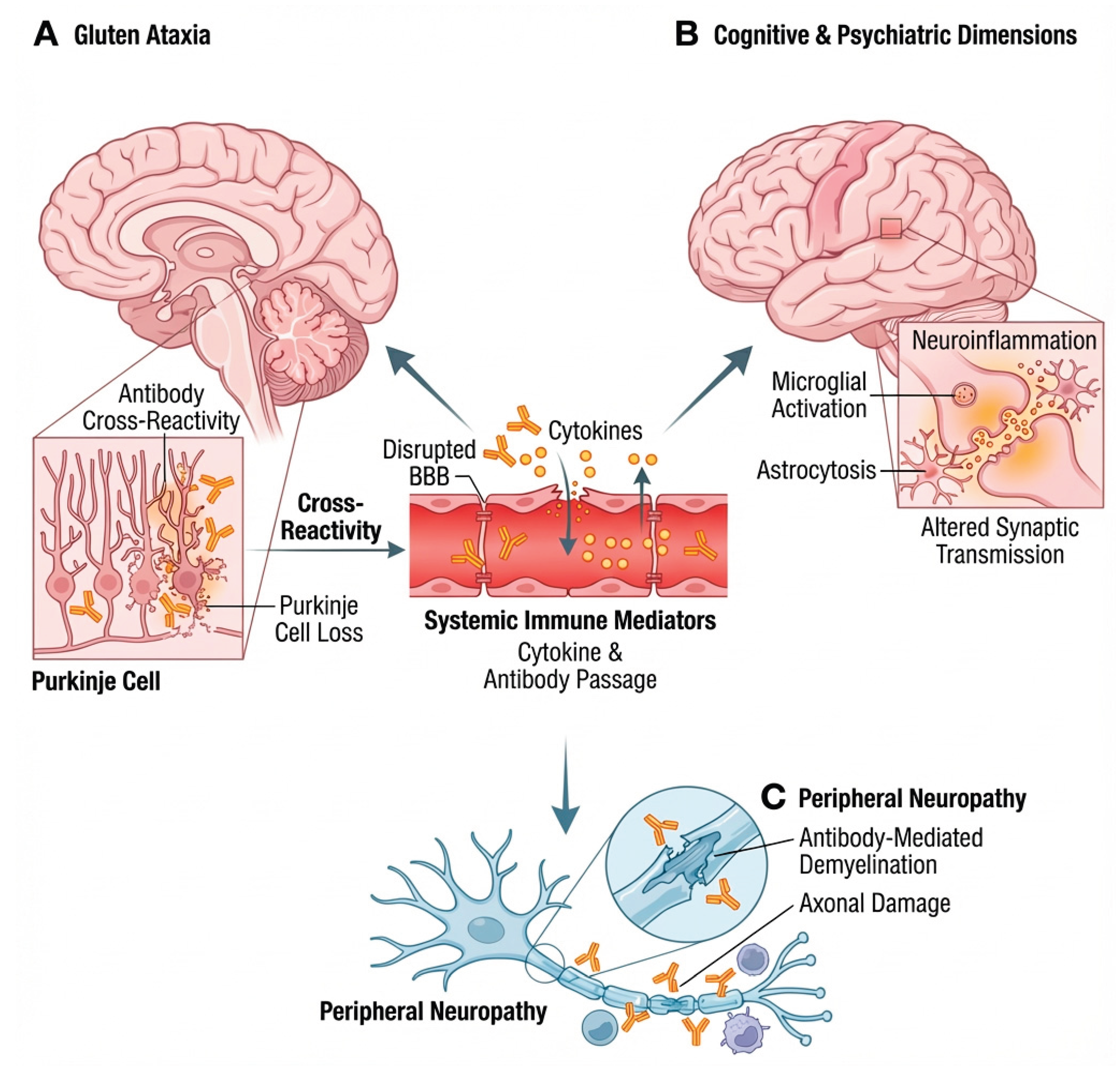
Pathophysiology of gluten-related neurological disorders. The blood-brain barrier (BBB) disruption by gluten allows cytokines and antibodies into neural tissues: (a) Gluten ataxia – Purkinje cell loss from antibody cross-reactivity; (b) Cognitive and psychiatric effects – neuroinflammation with microglial and astrocytic activation impairing synaptic signaling; (c) Peripheral neuropathy – immune-mediated demyelination and axonal damage in peripheral nerves.
Figure 2.
Pathophysiology of gluten-related neurological disorders. The blood-brain barrier (BBB) disruption by gluten allows cytokines and antibodies into neural tissues: (a) Gluten ataxia – Purkinje cell loss from antibody cross-reactivity; (b) Cognitive and psychiatric effects – neuroinflammation with microglial and astrocytic activation impairing synaptic signaling; (c) Peripheral neuropathy – immune-mediated demyelination and axonal damage in peripheral nerves.
Cardiovascular Involvement in GRDs
- Epidemiological associations
Increasing epidemiological evidence supports an association between celiac disease and adverse cardiovascular outcomes [24]. Large population-based cohort studies have demonstrated a higher incidence of ischemic heart disease, atrial fibrillation, and cerebrovascular events in individuals with celiac disease compared with the general population. Importantly, this excess risk appears to be most pronounced in the period surrounding diagnosis, suggesting that active, untreated disease and systemic inflammation may play a critical role. A nationwide cohort study based on biopsy-verified celiac disease reported a significantly increased risk of ischemic heart disease, independent of traditional cardiovascular risk factors [25].
Subsequent population-based analyses have also identified an increased risk of atrial fibrillation in celiac disease, reinforcing the link between chronic immune-mediated inflammation and arrhythmogenic vulnerability [26]. While malabsorption-related deficiencies (such as iron, folate, and vitamin B12) may contribute to endothelial dysfunction and hyperhomocysteinemia, these factors do not fully account for the observed cardiovascular risk, which persists after multivariable adjustment.
By contrast, non-celiac gluten sensitivity and wheat allergy remain underrepresented in cardiovascular epidemiology. Available data are sparse and largely observational, but clinical reports describe autonomic symptoms, palpitations, and orthostatic intolerance in selected patients. At present, these findings should be regarded as hypothesis-generating rather than conclusive.
- 2.
- Inflammation, endothelial dysfunction, and thrombosis
From a mechanistic standpoint, chronic low-grade systemic inflammation provides a plausible link between gluten-related immune activation and cardiovascular disease [2]. Untreated celiac disease is characterized by circulating pro-inflammatory cytokines and immune mediators that may impair endothelial nitric oxide signaling, promote oxidative stress, and accelerate atherosclerotic processes [27]. Inflammatory activation of coagulation pathways may further contribute to a prothrombotic milieu, potentially explaining the increased incidence of ischemic events observed in epidemiological studies. Furthermore, malabsorption-related micronutrient deficiencies, particularly of folate, vitamin B12, and vitamin B6, contribute to elevated homocysteine levels, an independent risk factor for endothelial dysfunction and atherothrombosis that has been documented in untreated celiac disease patients [28].
Autoimmune mechanisms may also contribute. Tissue transglutaminase, the primary autoantigen in celiac disease, is expressed in vascular endothelial cells, raising the possibility that circulating anti-transglutaminase antibodies interact with the vascular wall and influence endothelial integrity [27]. Although direct causal evidence remains limited, this hypothesis aligns with broader concepts linking autoimmunity and vascular dysfunction.
- 3.
- Autonomic dysregulation and cardiac electrophysiology
Autonomic nervous system dysfunction represents a critical interface between neurological and cardiovascular involvement in gluten-related disorders. Reduced heart rate variability, orthostatic intolerance, and features of dysautonomia have been described in patients with celiac disease, particularly in those with neurological manifestations [29]. Such alterations may reflect impaired central autonomic regulation or persistent inflammatory signaling. Quantitative assessments have demonstrated significantly reduced vagal modulation indices and time-domain heart rate variability parameters in celiac patients compared to healthy controls, with some studies reporting partial normalization following gluten-free diet adherence [30].
Clinically, autonomic imbalance is relevant not only because it contributes to symptoms such as palpitations, fatigue, and exercise intolerance, but also because reduced parasympathetic tone and sympathetic predominance are recognized risk factors for atrial fibrillation and adverse cardiovascular outcomes, providing a mechanistic bridge between immune activation and electrophysiological vulnerability.
Figure 3.
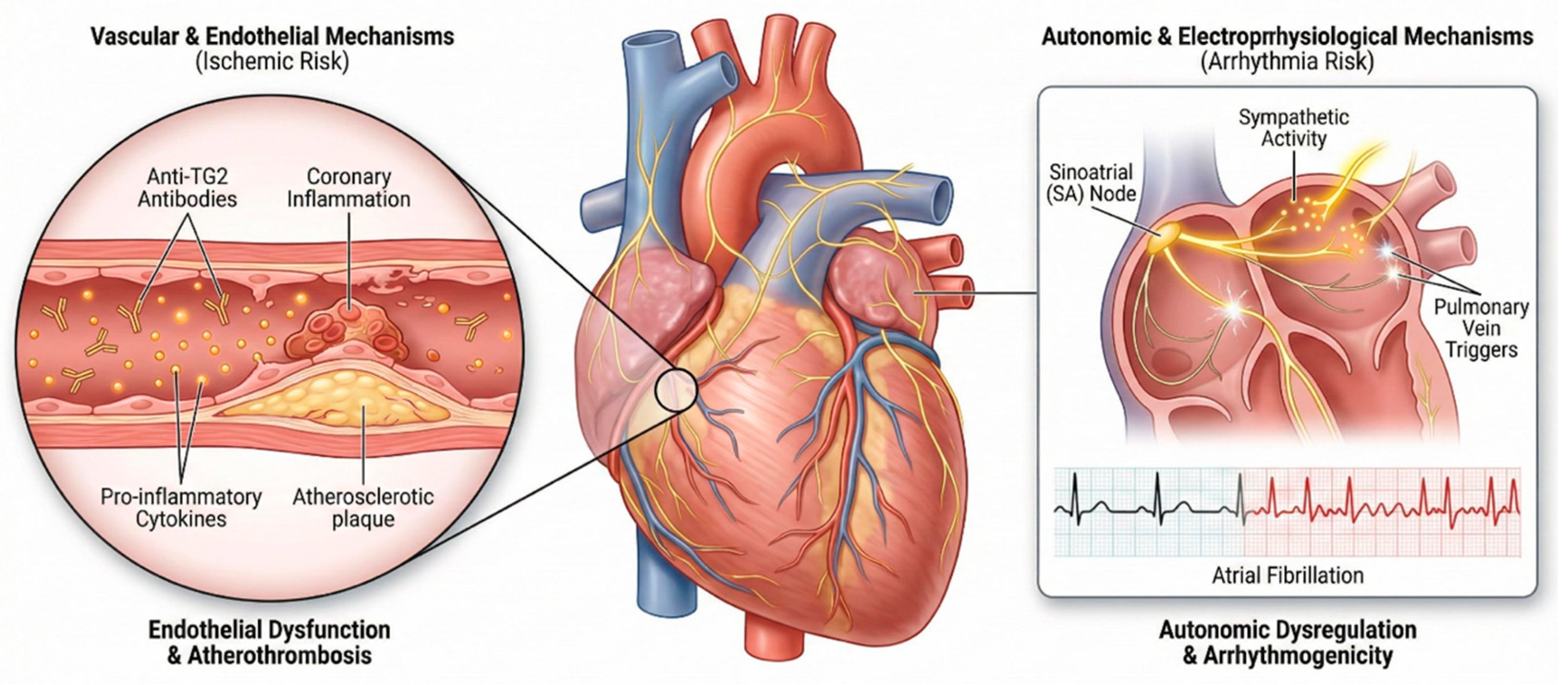
Pathophysiological pathways linking GRDs to cardiovascular risk. This schematic delineates two interrelated pathophysiologic pathways that may underlie adverse cardiovascular sequelae. (a) Chronic inflammation and anti-TG2 antibodies damage endothelium, causing oxidative stress, accelerated atherosclerosis and prothrombotic states that heighten ischemic heart disease risk [27]. (b) Sympathetic dominance with reduced vagal tone alters sinoatrial node and pulmonary vein innervation, promoting arrhythmogenic substrates and increased susceptibility to atrial fibrillation [29].
Figure 3.
Pathophysiological pathways linking GRDs to cardiovascular risk. This schematic delineates two interrelated pathophysiologic pathways that may underlie adverse cardiovascular sequelae. (a) Chronic inflammation and anti-TG2 antibodies damage endothelium, causing oxidative stress, accelerated atherosclerosis and prothrombotic states that heighten ischemic heart disease risk [27]. (b) Sympathetic dominance with reduced vagal tone alters sinoatrial node and pulmonary vein innervation, promoting arrhythmogenic substrates and increased susceptibility to atrial fibrillation [29].
The Gut-Brain-Heart Axis in GRDs
The gut-brain-heart axis refers to an integrated, bidirectional communication network linking the gastrointestinal tract, central and peripheral nervous systems, immune signaling pathways, and cardiovascular regulation [31]. This framework has emerged from converging evidence demonstrating that intestinal immune activation and barrier dysfunction can exert distal effects on brain function, autonomic control, and cardiac physiology. In GRDs, persistent or recurrent exposure to gluten represents a chronic immune stimulus capable of perturbing this interconnected system at multiple levels.
Within this axis, immune-to-brain signaling occurs through complementary humoral and neural pathways. Pro-inflammatory cytokines generated in the gut can access or signal across the BBB, while vagal afferent fibers convey immune and inflammatory information directly to brainstem nuclei and higher autonomic centers. These mechanisms are well established in the broader context of immune-brain communication and provide a biologically plausible route through which intestinal inflammation influences central autonomic regulation [32]. Emerging evidence also implicates alterations in the gut microbiome composition (dysbiosis) as a key mediator within the gut-brain-heart axis [33]. Celiac disease is associated with reduced microbial diversity, altered Firmicutes/Bacteroidetes ratios, and diminished production of short-chain fatty acids, which play regulatory roles in both intestinal barrier integrity and systemic immune modulation [34].
Central integration of interoceptive and immune signals occurs within the central autonomic network, a distributed set of cortical and subcortical regions that includes the insular cortex, anterior cingulate cortex, hypothalamus, amygdala, and brainstem autonomic nuclei. This network coordinates autonomic, neuroendocrine, and behavioral responses and exerts direct control over heart rate, vascular tone, and cardiac electrophysiology [35]. Importantly, these same regions are involved in pain modulation [36], fatigue perception, and emotional processing, providing a neuroanatomical substrate for the co-occurrence of neurological, autonomic, and cardiovascular symptoms observed in some patients with GRDs.
From a cardiovascular perspective, brain-heart coupling is further conceptualized by the neurovisceral integration model, which links central regulatory circuits to cardiac autonomic output and cardiovascular risk. Dysregulation within these circuits is associated with reduced heart rate variability, impaired stress adaptation, and increased vulnerability to arrhythmias [37]. Immune signaling intersects with this system through the inflammatory reflex, a vagus-mediated pathway by which immune activation modulates both central autonomic function and peripheral organ inflammation [38].
Figure 4.
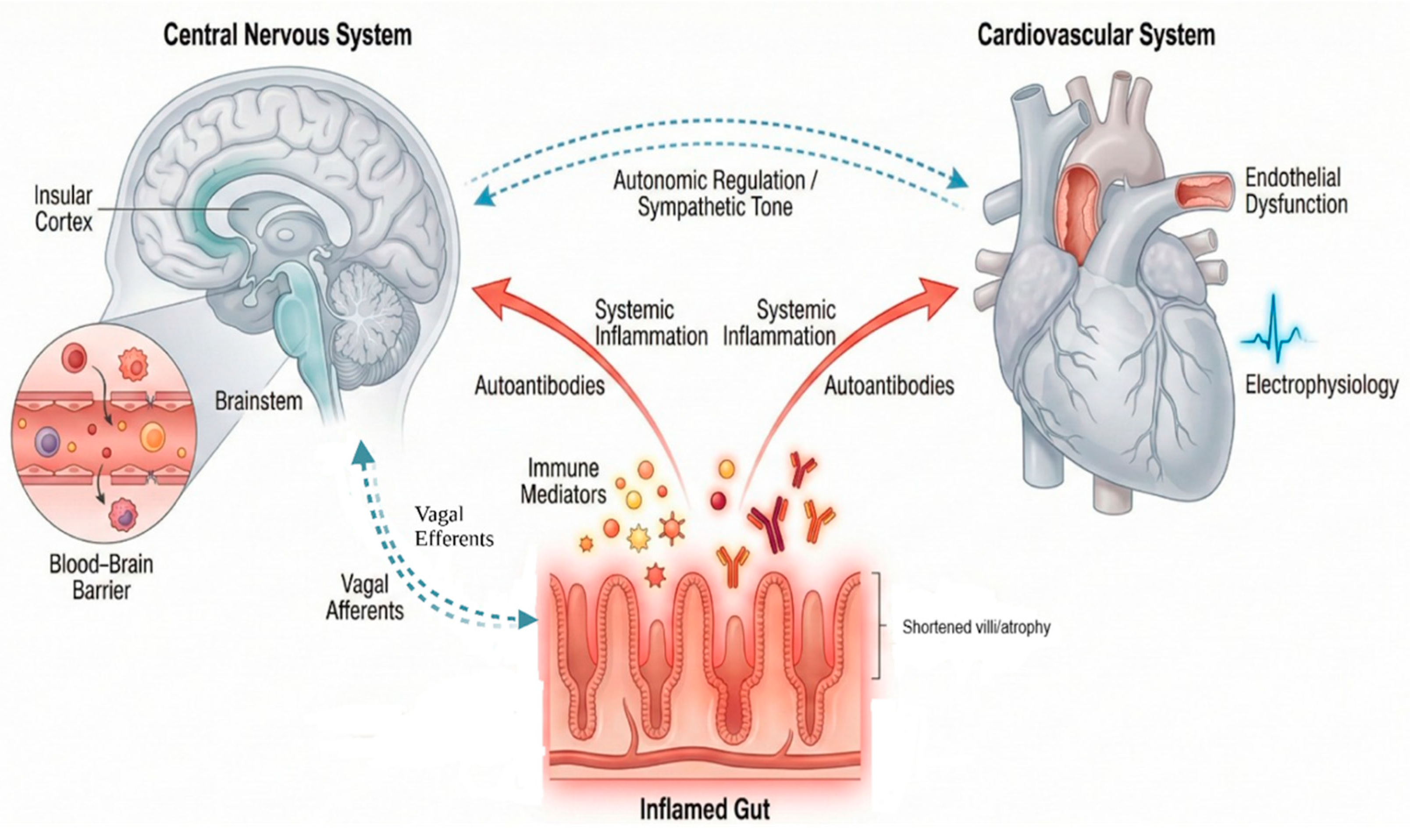
The gut–brain–heart axis: integrated immune and neural signaling networks. This schematic summarizes bidirectional pathways through which intestinal pathology may contribute to neurocardiac dysfunction in gluten-related disorders. (a) Gut inflammation releases cytokines and autoantibodies, disrupting the BBB, promoting neuroinflammation and endothelial dysfunction with thrombotic risk. (b) Vagal afferent signaling causes sympathetic predominance and reduced parasympathetic tone. (c) Combined immune–neural effects manifest as fatigue, brain fog, palpitations, orthostatic intolerance, and increased arrhythmia and ischemic heart disease susceptibility.
Figure 4.
The gut–brain–heart axis: integrated immune and neural signaling networks. This schematic summarizes bidirectional pathways through which intestinal pathology may contribute to neurocardiac dysfunction in gluten-related disorders. (a) Gut inflammation releases cytokines and autoantibodies, disrupting the BBB, promoting neuroinflammation and endothelial dysfunction with thrombotic risk. (b) Vagal afferent signaling causes sympathetic predominance and reduced parasympathetic tone. (c) Combined immune–neural effects manifest as fatigue, brain fog, palpitations, orthostatic intolerance, and increased arrhythmia and ischemic heart disease susceptibility.
Clinically, disruption of the gut-brain-heart axis offers a coherent explanation for complex symptom constellations reported in GRDs, including cognitive dysfunction, fatigue, palpitations, orthostatic intolerance, and reduced exercise capacity, often in the absence of overt structural disease. Recognizing GRDs as conditions capable of engaging this integrated axis supports a systems-based approach to diagnosis and management, bridging gastroenterology, neurology, and cardiovascular medicine.
Therapeutic Implications and Reversibility of Brain-Heart Effects
The gluten-free diet (GFD) remains the cornerstone of therapy for celiac disease and is commonly adopted in individuals with non-celiac gluten sensitivity. From a pathophysiological perspective, strict and sustained gluten withdrawal represents the only currently available disease-modifying intervention capable of suppressing antigen-driven immune activation, restoring intestinal barrier integrity, and reducing systemic inflammatory signaling. Contemporary clinical guidance emphasizes that early diagnosis and rigorous dietary adherence are essential not only for achieving intestinal mucosal healing, but also for limiting or preventing extra-intestinal complications, including neurological and cardiovascular manifestations [39]. However, strict adherence to a GFD remains challenging, with studies reporting non-adherence rates ranging from 42% to 91% depending on assessment methods, primarily due to inadvertent gluten exposure, social constraints, cost, and palatability concerns [40,41].
Clinical observations and longitudinal studies indicate that adherence to a GFD may be associated with partial or complete improvement in selected neurological symptoms, affective disturbances, and cardiac complaints, particularly when treatment is initiated early in the disease course [2,4,42]. These findings support the concept that a proportion of brain-heart alterations in gluten-related disorders are functionally mediated and potentially reversible, rather than exclusively structural or degenerative. Improvement in systemic inflammation and nutritional status may further contribute to normalization of vascular and autonomic function over time.
Figure 5.
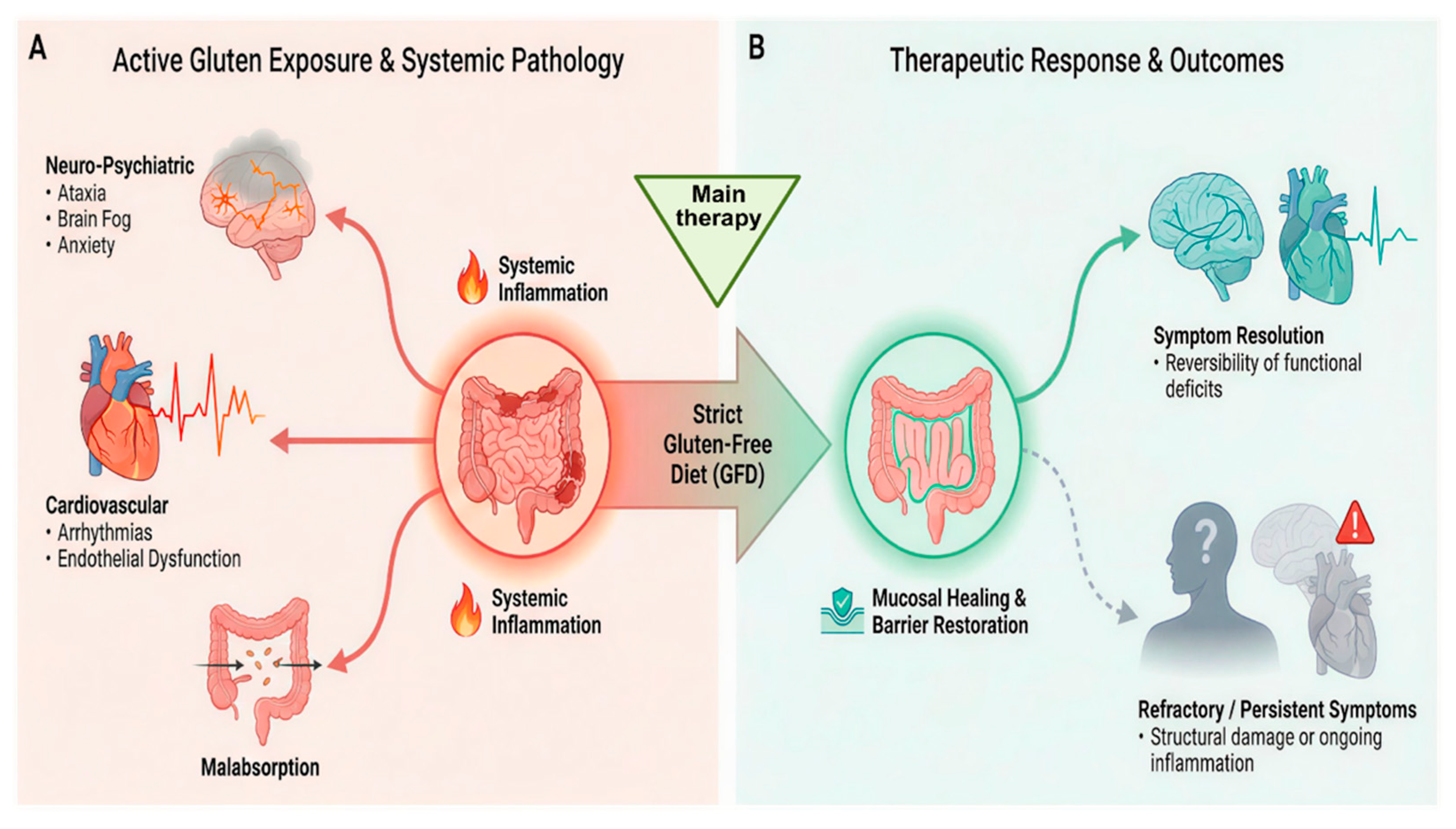
Systemic clinical manifestations and differential responses to dietary intervention. This flowchart contrasts the multisystem impact of active gluten-related disorders with outcomes following therapeutic dietary treatment. (a) Active gluten-related disorders maintain barrier disruption and systemic inflammation, yielding malabsorption and extra-intestinal neurological (ataxia, cognitive impairment) and cardiovascular (arrhythmias, ischemic) complications. (b) Gluten-free diet fosters mucosal healing, barrier restoration, and reduced immune signaling, often improving neurocardiac symptoms, although some patients experience persistent signs, suggesting structural injury, central sensitization, or refractory inflammation requiring adjunctive strategies.
Figure 5.
Systemic clinical manifestations and differential responses to dietary intervention. This flowchart contrasts the multisystem impact of active gluten-related disorders with outcomes following therapeutic dietary treatment. (a) Active gluten-related disorders maintain barrier disruption and systemic inflammation, yielding malabsorption and extra-intestinal neurological (ataxia, cognitive impairment) and cardiovascular (arrhythmias, ischemic) complications. (b) Gluten-free diet fosters mucosal healing, barrier restoration, and reduced immune signaling, often improving neurocardiac symptoms, although some patients experience persistent signs, suggesting structural injury, central sensitization, or refractory inflammation requiring adjunctive strategies.
Nevertheless, dietary therapy is not universally effective. A substantial subset of patients continues to report persistent cognitive complaints, fatigue, dysautonomia, or cardiovascular symptoms despite strict adherence to a GFD and documented intestinal recovery. This dissociation suggests that immune-mediated, neurovascular, or autonomic alterations may become partially self-sustaining or only incompletely responsive to gluten exclusion. Current clinical guidelines acknowledge this limitation and highlight the need for careful follow-up and evaluation of ongoing extra-intestinal symptoms [43]. Collectively, these observations underscore the importance of moving beyond a diet-only paradigm in selected patients and support the development of adjunctive strategies targeting residual inflammation, barrier dysfunction, and maladaptive neuroimmune-autonomic signaling.
Knowledge Gaps and Future Directions
Despite increasing recognition of GRDs as systemic conditions, major knowledge gaps remain regarding their impact on the brain-heart axis. Mechanistic studies directly linking gluten exposure to defined neurocardiac outcomes are limited, and most available data derive from observational or associative research, restricting causal inference. In particular, the biological pathways connecting intestinal immune activation with autonomic regulation, vascular function, and cardiac electrophysiology remain incompletely characterized. Evidence is unevenly distributed across the spectrum of GRDs. Celiac disease is relatively well studied, whereas non-celiac gluten sensitivity and wheat allergy are markedly underrepresented in neurological and cardiovascular research. This imbalance limits generalizability and hampers the development of phenotype-specific risk stratification strategies. In addition, autonomic and neurovascular dysfunction are inconsistently assessed across studies, reflecting the lack of standardized diagnostic tools and outcome measures applicable to clinical and research settings. A critical unmet need is the development and validation of non-invasive biomarkers capable of detecting subclinical neurocardiac involvement and monitoring treatment response. Candidate markers may include circulating neurofilament light chain for neuronal injury, high-sensitivity cardiac troponin for myocardial stress, and advanced autonomic function indices, though their clinical utility in GRDs requires prospective validation.
Importantly, brain-heart outcomes are rarely incorporated as predefined endpoints in clinical trials evaluating dietary or adjunctive interventions in GRDs. As a result, the reversibility, persistence, and clinical significance of neurocardiac alterations remain poorly defined. Future research should therefore adopt multimodal, systems-level approaches integrating immunological profiling, autonomic testing, neuroimaging, and cardiovascular assessment. Such designs are essential to delineate shared mechanisms, identify clinically meaningful biomarkers, and inform targeted, personalized management strategies for patients with gluten-related disorders.
Limitations
This narrative review has several limitations that should be considered when interpreting its conclusions. First, by design, narrative reviews do not employ the exhaustive, protocol-driven search strategies or formal risk-of-bias assessments characteristic of systematic reviews. Although this work was conducted and reported in accordance with the SANRA, the possibility of incomplete literature capture cannot be fully excluded. To mitigate this limitation, the review objectives were clearly defined a priori, the narrative format was explicitly justified, and evidence selection emphasized conceptual relevance, methodological robustness, and balanced interpretation in line with SANRA criteria. Second, the heterogeneity of GRDs (including autoimmune, innate immune-mediated, and IgE-mediated phenotypes) limits the ability to draw uniform mechanistic conclusions, particularly with respect to brain-heart interactions. Available evidence is unevenly distributed across disease entities, with celiac disease substantially overrepresented relative to non-celiac gluten sensitivity and wheat allergy. As a result, conclusions pertaining to non-celiac entities should be interpreted with appropriate caution. Moreover, much of the literature addressing neurological, autonomic, and cardiovascular involvement in gluten-related disorders is observational or hypothesis-generating in nature. This limits causal inference and increases susceptibility to residual confounding, particularly in studies assessing complex outcomes such as autonomic function or cardiovascular risk. Additionally, publication bias may favor positive associations, particularly for rare or novel extra-intestinal manifestations, potentially leading to overestimation of effect sizes and clinical significance. Finally, the integration of brain and heart outcomes is constrained by variability in outcome definitions, non-standardized assessment tools, and inconsistent reporting across studies. These factors restrict cross-study comparability and synthesis. Despite these limitations, adherence to SANRA standards supports the methodological credibility of this review and underscores its role in providing a coherent conceptual framework, identifying knowledge gaps, and informing the design of future mechanistic and translational research rather than delivering definitive effect estimates.
Conclusions
GRDs manifest systemic immune-mediated effects that extend beyond the gastrointestinal tract to include the central nervous and cardiovascular systems. Evidence implicates interconnected mechanisms involving immune activation, barrier dysfunction, and autonomic dysregulation in driving neurological, psychiatric, and cardiovascular manifestations. Conceptualizing GRDs through a gut–brain–heart axis unifies these immunological and neurovascular processes and clarifies that extra-intestinal features are integral to disease expression. Clinically, prompt recognition of systemic involvement and strict adherence to a GFD are crucial, with early intervention offering partial reversibility of selected neurocardiac alterations. However, persistence of symptoms in a substantial minority underscores the need for comprehensive evaluations and adjunctive therapies. Interdisciplinary research integrating immunology, neuroscience, and cardiology is essential to refine pathophysiological understanding, improve risk stratification, and facilitate personalized care for individuals with GRDs.
Author Contributions
Conceptualization, G.V.; methodology, G.V., M.L.G.L.; formal analysis, A.A.A.A., YV.T., P.V.P., D.M., AC; writing — original draft preparation, G.V., M.L.G.L., A.C., YV.T., P.V.P.; writing — review and editing, G.V., M.L.G.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Acknowledgments
We extend our sincere gratitude to the Fondazione Paolo Procacci for their invaluable support and assistance throughout the publication process. In particular, their assistance was indispensable in researching bibliographic sources and preparing the illustrations.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| BBB | Blood-brain barrier |
| CD4 | The cluster of differentiation marker CD4 |
| GFD | Gluten free diet |
| GRDs | Gluten-related disorders |
| HLA-DQ2 | Human leukocyte antigen (HLA) class II molecule (DQ2) |
| HLA-DQ8 | Human leukocyte antigen (HLA) class II molecule (DQ8) |
| HLA | Human leukocyte antigen |
| IgE | Immunoglobulin E |
| SANRA | Scale for the assessment of narrative review articles |
| Th1 | T helper 1 cells |
| TG2 | Tissue transglutaminase 2 |
References
- Taraghikhah, N; Ashtari, S; Asri, N; Shahbazkhani, B; Al-Dulaimi, D; Rostami-Nejad, M; Rezaei-Tavirani, M; Razzaghi, MR; Zali, MR. An updated overview of spectrum of gluten-related disorders: clinical and diagnostic aspects. BMC Gastroenterol 2020, 20(1), 258. [Google Scholar] [CrossRef] [PubMed]
- Giuffrè, M; Gazzin, S; Zoratti, C; Llido, JP; Lanza, G; Tiribelli, C; Moretti, R. Celiac Disease and Neurological Manifestations: From Gluten to Neuroinflammation. Int J Mol Sci. 2022, 23(24), 15564. [Google Scholar] [CrossRef]
- Singh, P; Arora, A; Strand, TA; Leffler, DA; Catassi, C; Green, PH; Kelly, CP; Ahuja, V; Makharia, GK. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol 2018, 16(6), 823–836.e2. [Google Scholar] [CrossRef]
- Santonicola, A; Wieser, H; Gizzi, C; Soldaini, C; Ciacci, C. Associations between Celiac Disease, Extra-Gastrointestinal Manifestations, and Gluten-Free Diet: A Narrative Overview. Nutrients 2024, 16(12), 1814. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, L. Celiac Disease and Associated Extraintestinal Manifestations, with Special Reference to Neurological Disorders. OBM Neurobiology 2020, 4(4), 074. [Google Scholar] [CrossRef]
- Eng, S; Gabr, A; Raghav, S; Frishman, WH; Aronow, WS. The Gut-Heart Connection: Unraveling Cardiovascular Risks in Celiac Disease. Cardiol Rev 2025. [Google Scholar] [CrossRef] [PubMed]
- Baethge, C; Goldbeck-Wood, S; Mertens, S. SANRA-a scale for the quality assessment of narrative review articles. Res Integr Peer Rev 2019, 4, 5. [Google Scholar] [CrossRef]
- Aboulaghras, S; Piancatelli, D; Taghzouti, K; Balahbib, A; Alshahrani, MM; Al Awadh, AA; Goh, KW; Ming, LC; Bouyahya, A; Oumhani, K. Meta-Analysis and Systematic Review of HLA DQ2/DQ8 in Adults with Celiac Disease. Int J Mol Sci. 2023, 24(2), 1188. [Google Scholar] [CrossRef]
- Sollid, LM. Coeliac disease: dissecting a complex inflammatory disorder. Nat Rev Immunol 2002, 2(9), 647–55. [Google Scholar] [CrossRef]
- Sapone, A; Bai, JC; Ciacci, C; Dolinsek, J; Green, PH; Hadjivassiliou, M; Kaukinen, K; Rostami, K; Sanders, DS; Schumann, M; Ullrich, R; Villalta, D; Volta, U; Catassi, C; Fasano, A. Spectrum of gluten-related disorders: consensus on new nomenclature and classification. BMC Med. 2012, 10, 13. [Google Scholar] [CrossRef]
- Sicherer, SH; Sampson, HA. Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol. 2014, 133(2), 291–307; quiz 308. [Google Scholar] [CrossRef]
- Fasano, A. Zonulin and its regulation of intestinal barrier function: the biological door to inflammation, autoimmunity, and cancer. Physiol Rev. 2011, 91(1), 151–75. [Google Scholar] [CrossRef]
- Voisine, J; Abadie, V. Interplay Between Gluten, HLA, Innate and Adaptive Immunity Orchestrates the Development of Coeliac Disease. Front Immunol 2021, 12, 674313. [Google Scholar] [CrossRef]
- Serena, G; D’Avino, P; Fasano, A. Celiac Disease and Non-celiac Wheat Sensitivity: State of Art of Non-dietary Therapies. Front Nutr 2020, 7, 152. [Google Scholar] [CrossRef]
- Patel, N; Samant, H. Wheat Allergy. In StatPearls [Internet]; StatPearls Publishing: Treasure Island (FL), 25 Jun 2023. [Google Scholar] [PubMed]
- Fasano, A. All disease begins in the (leaky) gut: role of zonulin-mediated gut permeability in the pathogenesis of some chronic inflammatory diseases. F1000Res 2020, 9, F1000 Faculty Rev–69. [Google Scholar] [CrossRef]
- Varrassi, G; Leoni, MLG; Farì, G; Al-Alwany, AA; Al-Sharie, S; Fornasari, D. Neuromodulatory Signaling in Chronic Pain Patients: A Narrative Review. Cells 2025, 14(17), 1320. [Google Scholar] [CrossRef] [PubMed]
- Leoni, MLG; Mercieri, M; Viswanath, O; Cascella, M; Rekatsina, M; Pasqualucci, A; Caruso, A; Varrassi, G. Neuropathic Pain: A Comprehensive Bibliometric Analysis of Research Trends, Contributions, and Future Directions. Curr Pain Headache Rep. 2025, 29(1), 73. [Google Scholar] [CrossRef]
- Therrien, A; Kelly, CP; Silvester, JA. Celiac Disease: Extraintestinal Manifestations and Associated Conditions. J Clin Gastroenterol. 2020, 54(1), 8–21. [Google Scholar] [CrossRef] [PubMed]
- Hadjivassiliou, M; Sanders, DD; Aeschlimann, DP. Gluten-related disorders: gluten ataxia. Dig Dis. 2015, 33(2), 264–268. [Google Scholar] [CrossRef]
- Yelland, GW. Gluten-induced cognitive impairment (“brain fog”) in coeliac disease. J Gastroenterol Hepatol. 2017, 32 Suppl 1, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Addolorato, G; Leggio, L; D’Angelo, C; Mirijello, A; Ferrulli, A; Cardone, S; Vonghia, L; Abenavoli, L; Leso, V; Nesci, A; Piano, S; Capristo, E; Gasbarrini, G. Affective and psychiatric disorders in celiac disease. Dig Dis. 2008, 26(2), 140–8. [Google Scholar] [CrossRef]
- Hadjivassiliou, M; Sanders, DS; Grünewald, RA; Woodroofe, N; Boscolo, S; Aeschlimann, D. Gluten sensitivity: from gut to brain. Lancet Neurol 2010, 9(3), 318–30. [Google Scholar] [CrossRef]
- Huang, J. Assessment of the causal association between celiac disease and cardiovascular diseases. Front Cardiovasc Med 2022, 9, 1017209. [Google Scholar] [CrossRef]
- Ludvigsson, JF; James, S; Askling, J; Stenestrand, U; Ingelsson, E. Nationwide cohort study of risk of ischemic heart disease in patients with celiac disease. Circulation 2011, 123(5), 483–90. [Google Scholar] [CrossRef]
- Emilsson, L; Smith, JG; West, J; Melander, O; Ludvigsson, JF. Increased risk of atrial fibrillation in patients with coeliac disease: a nationwide cohort study. Eur Heart J 2011, 32(19), 2430–7. [Google Scholar] [CrossRef] [PubMed]
- Batty, M; Bennett, MR; Yu, E. The Role of Oxidative Stress in Atherosclerosis. Cells 2022, 11(23), 3843. [Google Scholar] [CrossRef] [PubMed]
- Hadithi, M; Mulder, CJ; Stam, F; et al. Effect of B vitamin supplementation on plasma homocysteine levels in celiac disease. World J Gastroenterol. 2009, 15(8), 955–960. [Google Scholar] [CrossRef] [PubMed]
- Furgala, A; Przybylska-Felus, M; Ciesielczyk, K; Gil, K; Zwolinska-Wcislo, M. Effects of water ingestion on autonomic activity and gastric motility in patients with celiac disease. J Physiol Pharmacol. 2023, 74(2). [Google Scholar] [CrossRef]
- Giorgetti, GM; Tursi, A; Iani, C; Arciprete, F; Brandimarte, G; Capria, A; Fontana, L. Assessment of autonomic function in untreated adult coeliac disease. World J Gastroenterol 2004, 10(18), 2715–8. [Google Scholar] [CrossRef]
- Calvillo, L; Vanoli, E; Ferrara, F; Caradonna, E. Interplay Among Gut Microbiota-Derived TMAO, Autonomic Nervous System Dysfunction, and Heart Failure Progression. Int J Mol Sci 2025, 27(1), 203. [Google Scholar] [CrossRef]
- Banks, WA. Blood-brain barrier transport of cytokines: a mechanism for neuropathology. Curr Pharm Des. 2005, 11(8), 973–84. [Google Scholar] [CrossRef]
- Inayat, N; Zahir, A; Hashmat, AJ; Khan, A; Ahmad, A; Sikander, M; Zakir, S; Ahmad, S; Awan, SK; Raza, SS; Varrassi, G. Gut Microbiota as a Key Modulator of Chronic Disease: Implications for Diabetes, Autoimmunity, and Cancer. Cureus 2025, 17(5), e84687. [Google Scholar] [CrossRef]
- Wacklin, P; Laurikka, P; Lindfors, K; Collin, P; Salmi, T; Lähdeaho, ML; Saavalainen, P; Mäki, M; Mättö, J; Kurppa, K; Kaukinen, K. Altered duodenal microbiota composition in celiac disease patients suffering from persistent symptoms on a long-term gluten-free diet. Am J Gastroenterol 2014, 109(12), 1933–41. [Google Scholar] [CrossRef]
- Benarroch, EE. The central autonomic network: functional organization, dysfunction, and perspective. Mayo Clin Proc. 1993, 68(10), 988–1001. [Google Scholar] [CrossRef]
- Varrassi, G.; Paladini, A.; Tran, Y. V.; Pham, V. P.; Al Alwany, A. A.; Farì, G.; Caruso, A.; Mercieri, M.; Pergolizzi, J. V.; Kaye, A. D.; Breve, F.; Corriero, A.; Gharibo, C.; Leoni, M. L. G. Advances in the Pathophysiology and Management of Cancer Pain: A Scoping Review. Cancers 2026, 18(2), 259. [Google Scholar] [CrossRef] [PubMed]
- Thayer, JF; Lane, RD. A model of neurovisceral integration in emotion regulation and dysregulation. J Affect Disord. 2000, 61(3), 201–16. [Google Scholar] [CrossRef] [PubMed]
- Tracey, KJ. The inflammatory reflex. Nature 2002, 420(6917), 853–9. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B; Rubio-Tapia, A. Epidemiology, Presentation, and Diagnosis of Celiac Disease. Gastroenterology 2021, 160(1), 63–75. [Google Scholar] [CrossRef]
- Hall, NJ; Rubin, G; Charnock, A. Systematic review: adherence to a gluten-free diet in adult patients with coeliac disease. Aliment Pharmacol Ther. 2009, 30(4), 315–330. [Google Scholar] [CrossRef]
- Varrassi, G; Cereda, E; Ruoppolo, GA; Mercieri, M; Muscaritoli, M. The drug called food and its role as a therapy for chronic patients: a comprehensive narrative review. Adv Health Res. cited. 2024, 1 1(1). [Google Scholar] [CrossRef]
- Schmucker, C; Eisele-Metzger, A; Meerpohl, JJ; Lehane, C; Kuellenberg de Gaudry, D; Lohner, S; Schwingshackl, L. Effects of a gluten-reduced or gluten-free diet for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev 2022, 2(2), CD013556. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A; Hill, ID; Semrad, C; Kelly, CP; Greer, KB; Limketkai, BN; Lebwohl, B. American College of Gastroenterology Guidelines Update: Diagnosis and Management of Celiac Disease. Am J Gastroenterol 2023, 118(1), 59–76. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Summary of all the selected and analyzed studies.
| Topics | Sub-topics | References | Results |
| Immuno-pathophysiology of gluten-related disorders |
|
[8,9,10,11,12,13,14,15,16] | Celiac disease: autoimmune gluten response affecting gut, nerves, heart. Non-celiac sensitivity/allergy: innate/IgE pathways causing systemic low-level inflammation. |
| Central nervous system involvement in gluten-related disorders |
|
[17,18,19,20,21,22,23] | Gluten-induced autoimmunity can cause cerebellar ataxia, peripheral neuropathy, epilepsy, headaches and cognitive/psychiatric symptoms through blood-brain-barrier disruption and anti-tTG antibodies, even without gut disease. |
| Cardiovascular involvement in gluten-related disorders |
|
[24,25,26,27,28,29,30] | Studies link celiac disease to higher ischemic heart disease, atrial fibrillation and stroke risk, independent of traditional factors, likely via inflammation, endothelial dysfunction and autonomic dysregulation; non-celiac evidence remains preliminary. |
| The gut-brain-heart axis in gluten-related disorders | [31,32,33,34,35,36,37,38] | The gut-brain-heart axis describes bidirectional immune and neural communication from gut inflammation to brain and heart, influencing autonomic control and symptoms like fatigue, palpitations. | |
| Therapeutic implications and reversibility of brain-heart effects | [39,40,41,42,43] | Gluten-free diet is main therapy; adherence restores barrier, reduces inflammation and extra-intestinal symptoms; however, some patients need adjunctive measures. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



