Submitted:
28 January 2026
Posted:
29 January 2026
You are already at the latest version
Abstract
This paper introduces SNAP (Structure, Narrative, Activation, Process, Next), a multi-dimensional clinical reflection tool designed to support psychotherapists in systematically attending to phenomenological, relational, and process-oriented dimensions during therapeutic work. SNAP integrates Gestalt therapy's phenomenological foundations with complex systems theory and the Research Domain Criteria (RDoC) framework, com-prising 73 items organized across five dimensions: Structure, Narrative, Activation, Process, and Next. A preliminary validation study with 20 psychotherapists employed a retrospective pre-post design in which participants rated the utility of each SNAP item for clinical reflection before and after SNAP training. Results showed significantly higher perceived utility after training (T2: M = 6.69, SD = 0.54) compared to retrospective baseline (T1: M = 6.02, SD = 0.70), with mean increase of +0.67 points (Cohen's d = 0.29, p < 0.05 for 15/73 items). Greatest utility gains were observed in phenomenological dimensions: Next (d = 0.63), Activation (d = 0.51), Narrative (d = 0.45), and Process-Therapist (d = 0.43). Structural bio-psycho-social dimensions showed minimal gains (d = -0.02 to 0.15), sug-gesting these were already well-integrated in therapists' clinical thinking. Findings suggest SNAP enhances reflective capacity by systematically directing attention to phenomenological dimensions that are valued but inconsistently attended to. Further psychometric validation with larger samples is warranted.
Keywords:
psychotherapy process
; Gestalt therapy
; process monitoring
; clinical assessment
; integrative psychotherapy
; therapist self-reflection
; RDoC
; phenomenology
; complex systems
; supervision
1. Introduction
Psychotherapy research has historically focused on symptom reduction and diagnostic categories, often neglecting the emergent, relational, and phenomenological dimensions that characterize therapeutic encounters (Wampold & Imel, 2015; Lambert, 2013; Francesetti 2024). This outcome-oriented approach, while valuable for demonstrating efficacy, tends to reduce the therapeutic encounter to measurable endpoints, potentially overlooking the complex relational and phenomenological processes through which change occurs (Elliott et al., 2018; Greenberg, L.S. 2010).
While evidence-based practice demands measurement and systematization (Cini et al., 2019), existing assessment tools frequently fail to capture the complexity of therapeutic process as it unfolds moment-to-moment in the clinical setting. Widely used instruments such as the Clinical Outcomes in Routine Evaluation (CORE-OM; Evans et al., 2002) and the Outcome Questionnaire-45 (OQ-45; Lambert et al., 1996) excel at tracking symptom change and psychological distress but provide limited insight into how therapeutic change emerges through relational dynamics and embodied experience. Similarly, alliance measures like the Working Alliance Inventory (WAI; Horvath & Greenberg, 1989) assess the quality of the therapeutic relationship yet do not systematically explore the phenomenological dimensions of in-session engagement (Francesetti, 2024; Rainauli, 2025)—such as sensory-motor activation, embodied awareness, or metaphorical representation of process—that may be crucial to therapeutic transformation. Process-adherence instruments like the Gestalt Therapy Fidelity Scale (GTFS; Fogarty et al., 2020) assess therapist adherence to theoretical principles but do not provide a comprehensive framework for understanding patient experience and emergent process dynamics. This gap between outcome measurement and process understanding has been increasingly recognized (Castonguay & Hill, 2012; Gelo et al., 2015), with calls for assessment tools that honor both empirical rigor and phenomenological complexity.
The SNAP tool (Structure, Narrative, Activation, Process) was developed to address this gap by integrating multiple theoretical frameworks: Gestalt therapy's phenomenological approach, affective neuroscience, the Research Domain Criteria (RDoC) framework, and complex systems theory. SNAP aims to provide clinicians with a structured yet flexible instrument for systematic process analysis that honors both scientific rigor and clinical complexity.
This paper presents the theoretical foundations of SNAP, describes its development process, and reports preliminary validation findings from a pilot study with 20 psychotherapists. We examine whether SNAP enhances therapists' reflective capacity by introducing novel dimensions of process awareness beyond conventional clinical thinking.
1.1. Theoretical Foundations
SNAP integrates three complementary theoretical frameworks that together provide a comprehensive foundation for process-oriented assessment. The tool is grounded first and foremost in Gestalt Integrated Therapy, which emphasizes phenomenological exploration (Capparelli et al., 2022), embodied awareness, and the therapeutic relationship as the primary vehicle for change (Perls et al., 1951; Francesetti, 2007; Orlando, 2020). SNAP's emphasis on relational dynamics reflects contemporary Gestalt therapy's shift from individualistic to field-theoretical perspectives (Wheeler, 2000). SNAP operationalizes core Gestalt concepts including contact (the meeting between therapist and patient at the boundary of experience), awareness (moment-to-moment consciousness of sensory, affective, and cognitive experience), and the paradoxical theory of change (Quattrini & Cini, 2020) —the principle that change occurs through full acceptance of what is, rather than through striving to be different (Yontef, 1993; Beisser, 1970). This phenomenological foundation is enriched by insights from affective neuroscience, which incorporates contemporary findings on emotion regulation, attachment systems, and the fundamentally embodied nature of psychological experience (Greenberg, 2015; Panksepp, 1998). This neuroscientific perspective recognizes the biological substrates of psychological phenomena—including the neurobiological systems underlying fear, seeking, care, and play—while maintaining the Gestalt commitment to subjective, lived experience rather than reducing therapeutic process to neurological mechanisms alone. Finally, SNAP adopts the Research Domain Criteria (RDoC) framework's transdiagnostic, dimensional approach to psychopathology (Cuthbert, 2020). Rather than organizing assessment around DSM diagnostic categories, SNAP follows RDoC's strategy of assessing functioning across multiple dimensional systems including Negative Valence Systems (fear, anxiety, loss), Positive Valence Systems (reward, motivation), Cognitive Systems (attention, memory, executive function), Social Processes (attachment, social communication), and Arousal/Regulatory Systems. This dimensional approach, compatible with Gestalt therapy's holistic view of human functioning, allows SNAP to capture clinical complexity beyond categorical diagnosis while remaining attentive to the nonlinear, self-organizing dynamics of therapeutic process emphasized by complex systems theory (Schiepek et al., 2017).
2. Materials and Methods
2.1. SNAP Tool Development
SNAP was developed through an iterative, theory-driven process combining: (a) systematic literature review of Gestalt therapy, attachment theory, neuroscience, and RDoC framework; (b) clinical practice observations and case formulation refinement; (c) expert consultation with senior Gestalt therapy practitioners and researchers; and (d) pilot testing and refinement based on clinician feedback. The tool comprises 73 items organized into four core dimensions (Structure, Narrative, Activation, Process) plus a prospective section (Next).
2.2. SNAP Dimensions
2.2.1. (S) Structure (40 Items)
The Structure dimension assesses bio-psycho-social scaffolding:
Biological (8 items): General health conditions, sleep-wake cycle, nutrition, physical energy, self-care, sexual wellbeing, pain symptoms, family history for physical/psychological disorders.
Psychological (19 items): Emotional states (anxiety, sadness, anger), regulation strategies and coping, self-esteem and self-efficacy; RDoC domains including Fear, Anxiety, Loss, Trauma, Frustration, Pleasure, Attention, Social perception and interpretation, Memory, Executive functions, Attachment and affiliation, Separation and stress, Motivational systems, Reward systems; Suicidal ideation and self-harm behaviors.
Social (6 items): Family relationships (configuration, dynamics, conflicts), social network (friends, colleagues, social support), work/school context (satisfaction, conflicts, difficulties), economic and housing conditions, interests and leisure activities, cultural and religious influences.
2.2.2. (N) Narrative (11 Items)
The Narrative dimension explores developmental history and autobiographical narrative across three life periods:
Childhood (4 items): Birth context (pregnancy, delivery, first months), attachment quality (secure, insecure, disorganized), significant experiences (traumas, separations, losses), learned emotional regulation modalities.
Adolescence (3 items): Bodily changes and associated experiences, experiences of autonomy and belonging, crises or difficulties (identity, sexuality).
Adulthood (4 items): Traumatic or stressful events, significant transitions, romantic and social relationships, recent traumatic or stressful events.
2.2.3. (A) Activation (5 Items)
The Activation dimension focuses on in-session engagement and embodied communication:
(1) Prevalent sensory-communicative modalities the patient uses to relate (visual contact, listening, movement, touch, verbal language, olfactory/gustatory channels and how these influence expression and interaction during sessions);
(2) Tendency to avoid interaction during sessions;
(3) Moments when avoidance behavior manifests most frequently;
(4) Interpersonal boundaries during sessions (predominantly rigid, flexible, or confused);
(5) Prevalent expressive channels for communicating emotions and experiences (e.g., drawing, music, writing, play).
2.2.4. (P) Process (16 Items)
The Process dimension addresses moment-to-moment consciousness and awareness in the therapeutic encounter (Stern, 2004):
Patient (6 items): Recognition and distinction of pleasant/unpleasant bodily sensations, perception of body in space, breath quality, awareness level regarding thoughts/emotions/behaviors, recognition of unmet needs, presence of conflicting polarities.
Therapist (10 items): Bodily sensations emerging during interactions with patient (tensions, relaxation, warmth, cold), breath perception during session, moments when perception of bodily experiences changes (tensions, rigidity, fluidity), interaction tendency predominating during session (looking, listening, speaking, touching), awareness of how bodily state influences therapeutic process, emotion regulation during session, thought content during session, tendency to evaluate/investigate/provide solutions/support/interpret, sensations regarding relationship with patient (connection, distance, tension, collaboration), session atmosphere (safety, tension, emptiness, possibility).
2.2.5. Next (8 Items)
The Next dimension explores future direction and emergent process:
Images/metaphors/narratives representing where therapist and patient are going together, direction of relational process between therapist and patient, presence of specific goals or openness to emergence, noticed changes (general), patient's development of new awareness/behaviors/perspectives since beginning, changes in therapist in relation to patient, therapist's development of new awareness/behaviors/perspectives in relation to patient since beginning, word/image/fantasy describing the therapeutic process being experienced with this patient.
Language and Availability: SNAP was originally developed in Italian and administered in Italian for this validation study, as all participants were Italian-speaking psychotherapists working with Italian-speaking patients. An English translation of the instrument has been completed and is available for international use. Future validation studies will assess the psychometric properties of the English version with English-speaking samples to ensure cross-cultural validity and applicability.
2.3. Research Objectives
This preliminary validation study addresses the following research questions:
1. Does SNAP introduce novel dimensions of clinical thinking not already present in therapists' pre-existing practice?
2. Which SNAP dimensions are perceived as most useful by practicing therapists?
3. Are there differences in perceived utility across SNAP's Structural, Narrative, Activation, Process-oriented and Next dimensions?
4. Do items addressing phenomenological and relational aspects show greater novelty compared to bio-psycho-social assessment items?
We hypothesized that phenomenological dimensions (Activation, Process, Next) would show greater novelty and utility compared to structural assessment dimensions already familiar to clinicians.
2.4. Study Design and Participants
Design: Retrospective pre-post pilot validation study.
Participants: Twenty psychotherapists, fourteen from an Italian Gestalt therapy institute and six representing other therapeutic orientations. Each therapist applied SNAP to one individual therapy case and completed the validation questionnaire.
Procedure: (1) Therapists received SNAP and applied it to one ongoing individual therapy case; (2) After completing SNAP, therapists completed a validation questionnaire with 73 pairs of items; (3) For each SNAP item, therapists rated: T1 (retrospective pre-test): "How much did you think about this question BEFORE using the tool?" (1-9 Likert scale); T2 (post-test): "How useful was this question AFTER using the tool?" (1-9 Likert scale).
Measures: Novelty was operationalized as T1 ratings (lower scores indicate more novel dimensions); Utility as T2 ratings (higher scores indicate more useful dimensions); Utility Gain as T2 - T1 difference scores; Effect size was calculated as Cohen's d for paired samples.
2.5. Data Analysis
Statistical Software and Tools: All statistical analyses were conducted using Python 3.9 with the following libraries: pandas 1.5.3 (data manipulation), numpy 1.24.2 (numerical computations), scipy 1.10.1 (statistical tests), matplotlib 3.7.1 (data visualization), and seaborn 0.12.2 (statistical graphics).
AI-Assisted Analysis: Statistical analyses and data visualizations were conducted with the assistance of AI-powered analytical tools under direct human supervision and expert oversight. All analytical decisions, interpretations, and conclusions were validated by the research team. The use of AI enhanced computational efficiency while maintaining scientific rigor and interpretive authority.
Statistical Procedures: (1) Descriptive statistics (means, standard deviations, ranges) for all variables; (2) Paired samples t-tests comparing T1 vs T2 for each item and dimension, with t-statistic calculated as t = Mean_diff / (SD_diff / √N), where N = 20 is the sample size; (3) Wilcoxon signed-rank tests as non-parametric alternative for non-normal distributions; (4) Effect size calculation using Cohen's d for paired samples (d = Mean_diff / SD_diff); (5) Effect size interpretation following Cohen's conventions: small (d = 0.2), medium (d = 0.5), large (d = 0.8); (6) Significance levels: p < 0.05 (*), p < 0.01 (**), p < 0.001 (***); (7) Dimension-level analysis by aggregating items by SNAP dimensions; (8) Exploratory analyses identifying items with highest novelty and utility gains.
Quality Control: Missing data were handled via pairwise deletion; parametric test assumptions were checked; sensitivity analyses using non-parametric alternatives were conducted; visual inspection of data distributions and outliers was performed.
3. Results
3.1. Sample Characteristics
Therapists: N = 20 psychotherapists.
Patients: N = 20 individual therapy cases. Age: M = 27.6 years (SD = 10.2, range = 16-59). Sex: 13 female (65%), 7 male (35%). Setting: 100% Individual therapy.
3.2. Overall Results Across All 73 Items
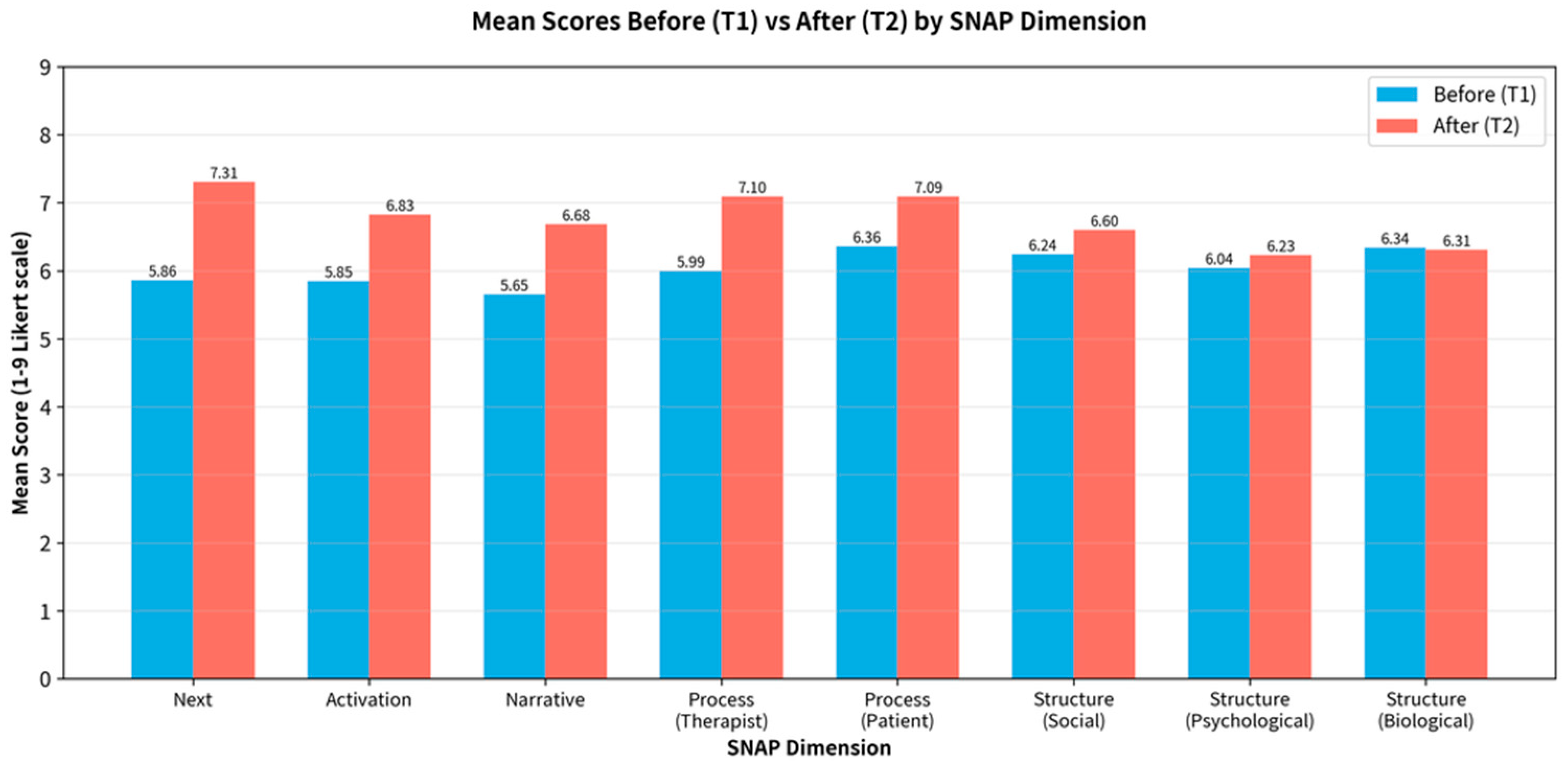
Across all 73 SNAP items, therapists reported significantly higher perceived utility after using the tool. T1 (Before): M = 6.02; T2 (After): M = 6.69; Mean Difference: +0.67; Overall Effect Size: Cohen's d = 0.29 (small-to-medium effect).
Statistical Significance: p < 0.001 (***): 2 items (2.7%); p < 0.01 (**): 4 items (5.5%); p < 0.05 (*): 9 items (12.3%); Non-significant: 58 items (79.5%); Total significant items: 15/73 (20.5%).
These findings indicate that SNAP introduces meaningful novel dimensions to therapists' clinical thinking, with approximately one-fifth of items showing statistically significant utility gains.
Figure 1.
Mean perceived utility scores before (T1, blue bars) and after (T2, red bars) using SNAP, organized by dimension and ranked by effect size (Cohen's d). Higher T2 scores indicate greater perceived utility after tool use. Next and Activation dimensions show the largest utility gains.
Figure 1.
Mean perceived utility scores before (T1, blue bars) and after (T2, red bars) using SNAP, organized by dimension and ranked by effect size (Cohen's d). Higher T2 scores indicate greater perceived utility after tool use. Next and Activation dimensions show the largest utility gains.
3.3. Results by SNAP Dimension
Table 1 presents results aggregated by SNAP dimension, ranked by effect size (Cohen's d). Phenomenological dimensions showed medium effect sizes: Next (d = 0.63), Activation (d = 0.51), Narrative (d = 0.45), and Process-Therapist (d = 0.43). The Next dimension showed highest utility gains, particularly for items addressing metaphorical representation ("word/image/fantasy describing process" d = 1.28, p < 0.001). Activation dimension items assessing sensory-motor engagement showed strong utility ("prevalent sensory-communicative modalities" d = 0.78, p < 0.01). Narrative dimension items addressing early developmental periods showed particular value ("birth context" d = 0.68, p < 0.01; "bodily changes in adolescence" d = 0.74, p < 0.01). Process-Therapist items focusing on embodied awareness showed meaningful gains ("interaction tendency" d = 0.66, p < 0.01; "breath perception" d = 0.55, p < 0.05).
In contrast, structural dimensions showed negligible effects: Structure-Biological (d = -0.02), Structure-Social (d = 0.15), Structure-Psychological (d = 0.10). High baseline T1 scores (M = 6.04-6.36) indicate these dimensions were already well-integrated into clinical practice.
Figure 2.
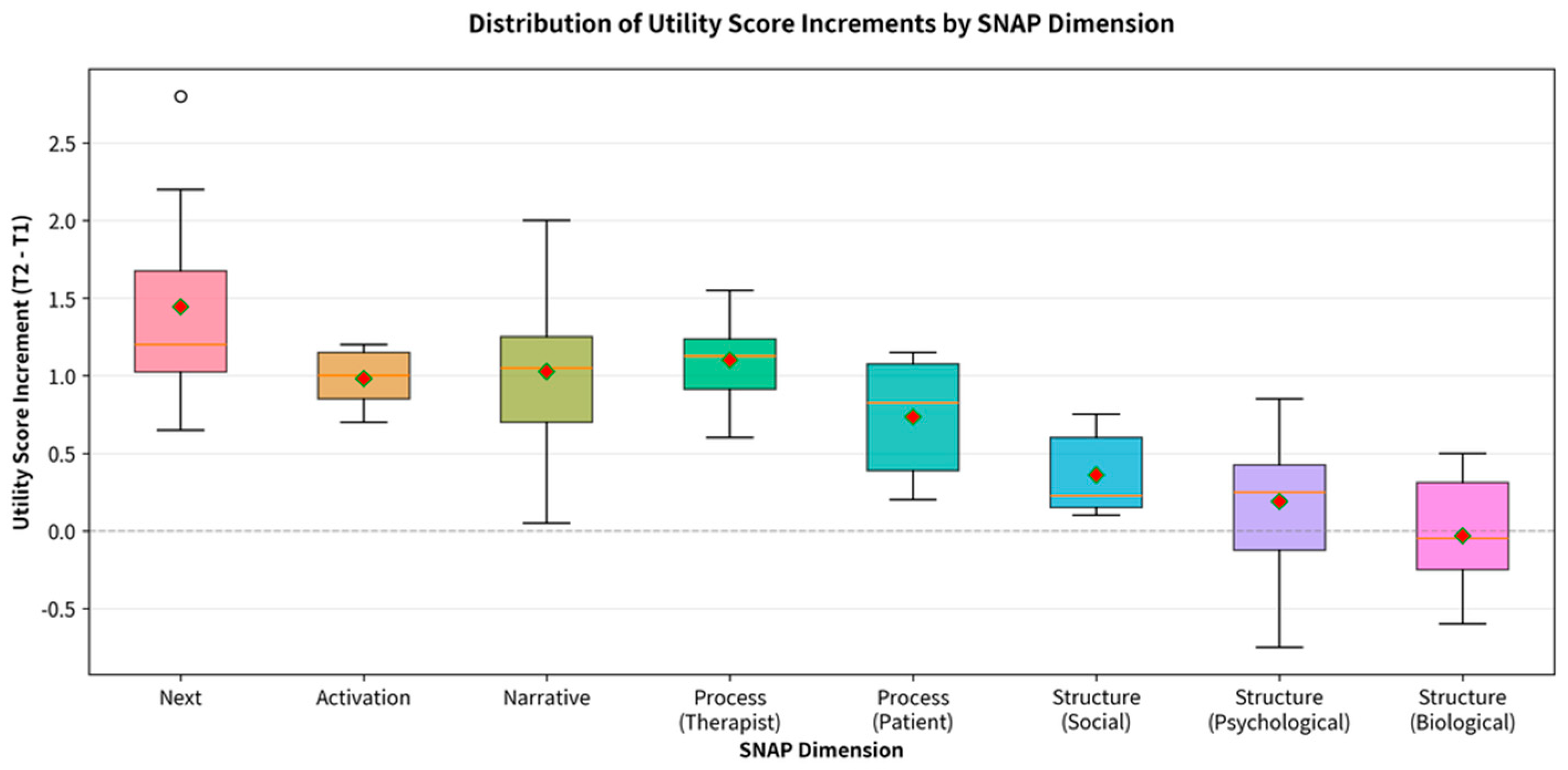
Boxplot showing distribution of utility gain scores (T2-T1) across SNAP dimensions, ranked by median gain. Diamond markers indicate mean values. The zero line represents no change.
Figure 2.
Boxplot showing distribution of utility gain scores (T2-T1) across SNAP dimensions, ranked by median gain. Diamond markers indicate mean values. The zero line represents no change.
3.4. Items with Greatest Utility Gain
Table 2 presents the top 10 items with greatest utility gains. The two highest items addressed metaphorical representation ("word/image/fantasy describing process" Δ = +2.80, d = 1.28, p < 0.001; "representative images/metaphors/narratives" Δ = +2.20, d = 1.09, p < 0.001). Developmental narrative items showed substantial gains ("birth context" Δ = +2.00, d = 0.68, p < 0.01; "bodily changes in adolescence" Δ = +1.80, d = 0.74, p < 0.01). Process-oriented items addressing therapist embodied awareness also showed meaningful utility ("interaction tendency" Δ = +1.55, d = 0.66, p < 0.01; "breath perception" Δ = +1.50, d = 0.55, p < 0.05).
Common themes across highest-utility items include: (1) metaphorical and symbolic representation of process; (2) developmental narrative, especially early life and adolescence; (3) therapist embodied awareness and countertransference; (4) future direction and emergent change; (5) attachment and relational patterns.
Figure 3.
Top 15 items ranked by utility increase.
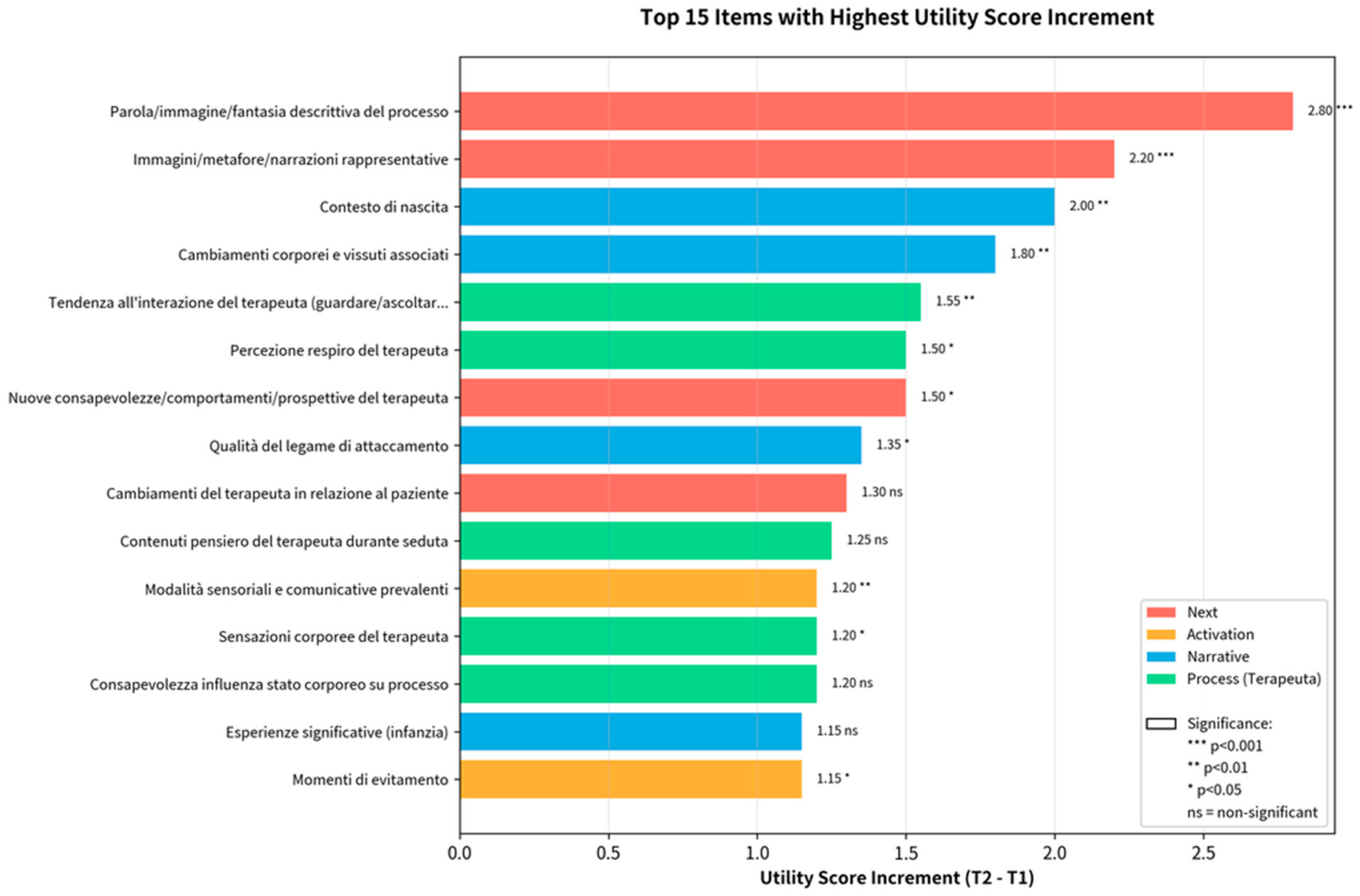
Figure 4.
Effect sizes (Cohen's d) by dimension with interpretation guidelines (dashed lines at d = 0.2, 0.5). Next and Activation reach medium effect size.
Figure 4.
Effect sizes (Cohen's d) by dimension with interpretation guidelines (dashed lines at d = 0.2, 0.5). Next and Activation reach medium effect size.
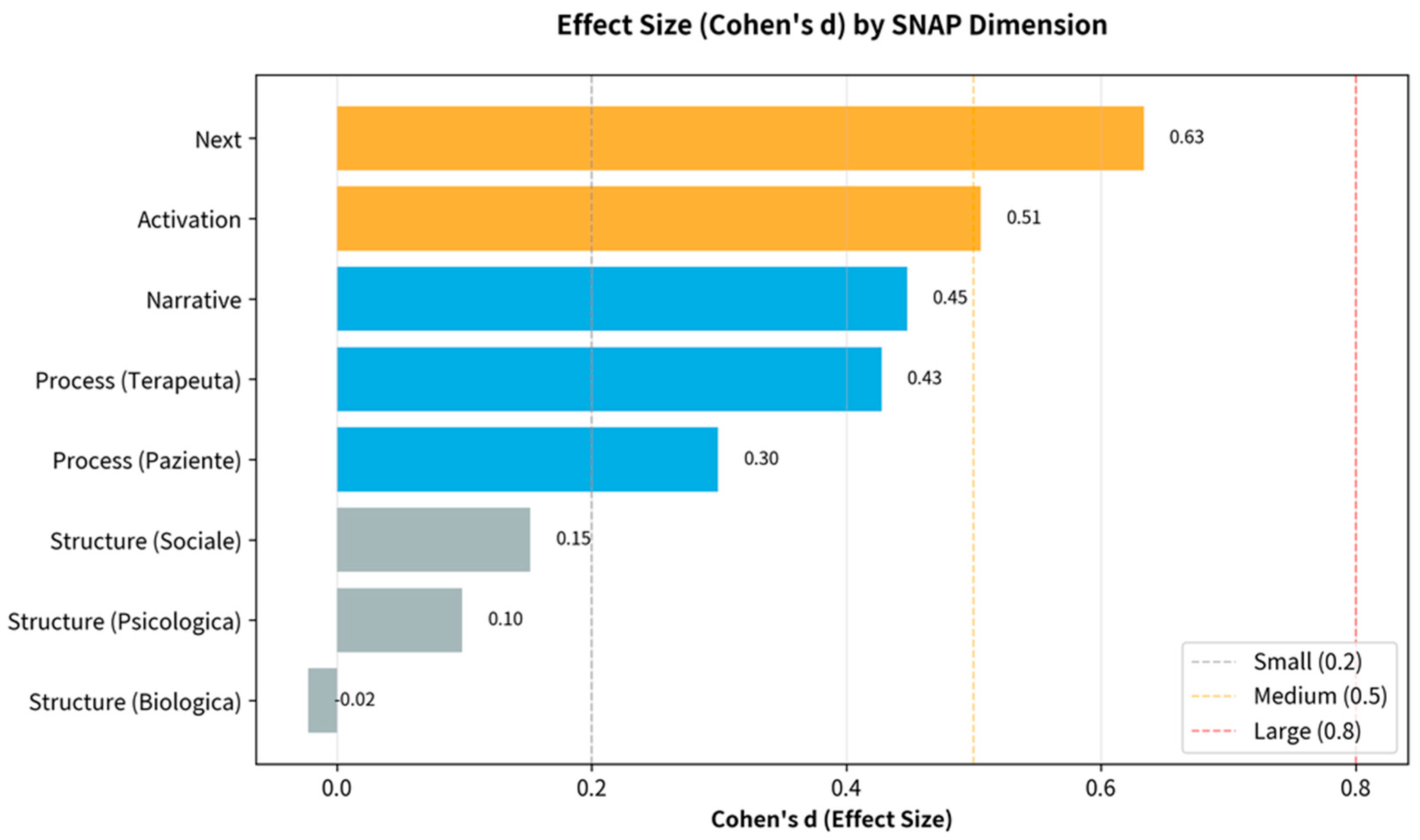
Figure 5.
Scatter plot showing relationship between T1 and T2 for all 73 items, color-coded by dimension. Diagonal line represents no change. Most items fall above the line (green area), indicating increased utility.
Figure 5.
Scatter plot showing relationship between T1 and T2 for all 73 items, color-coded by dimension. Diagonal line represents no change. Most items fall above the line (green area), indicating increased utility.
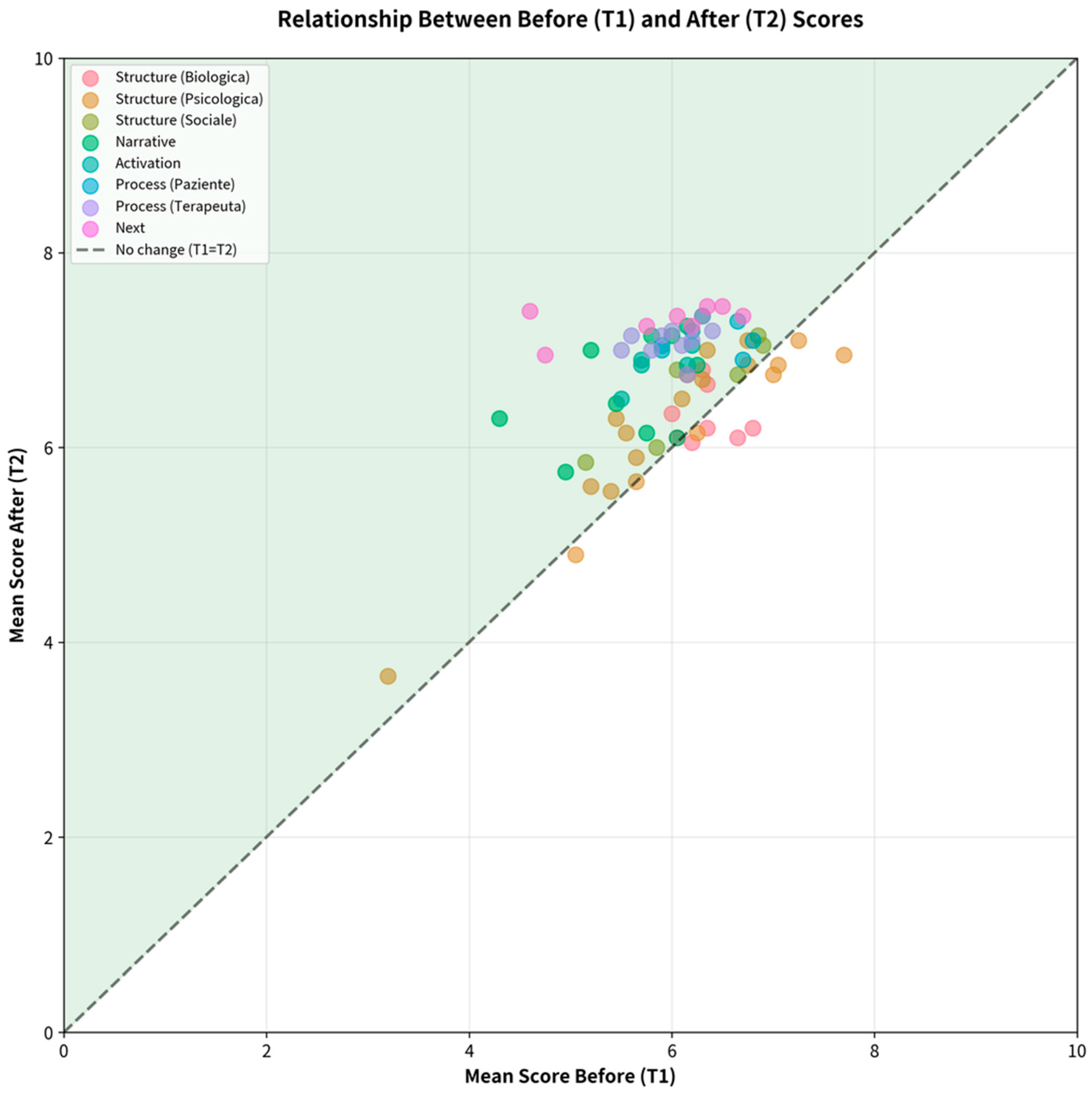
Figure 6.
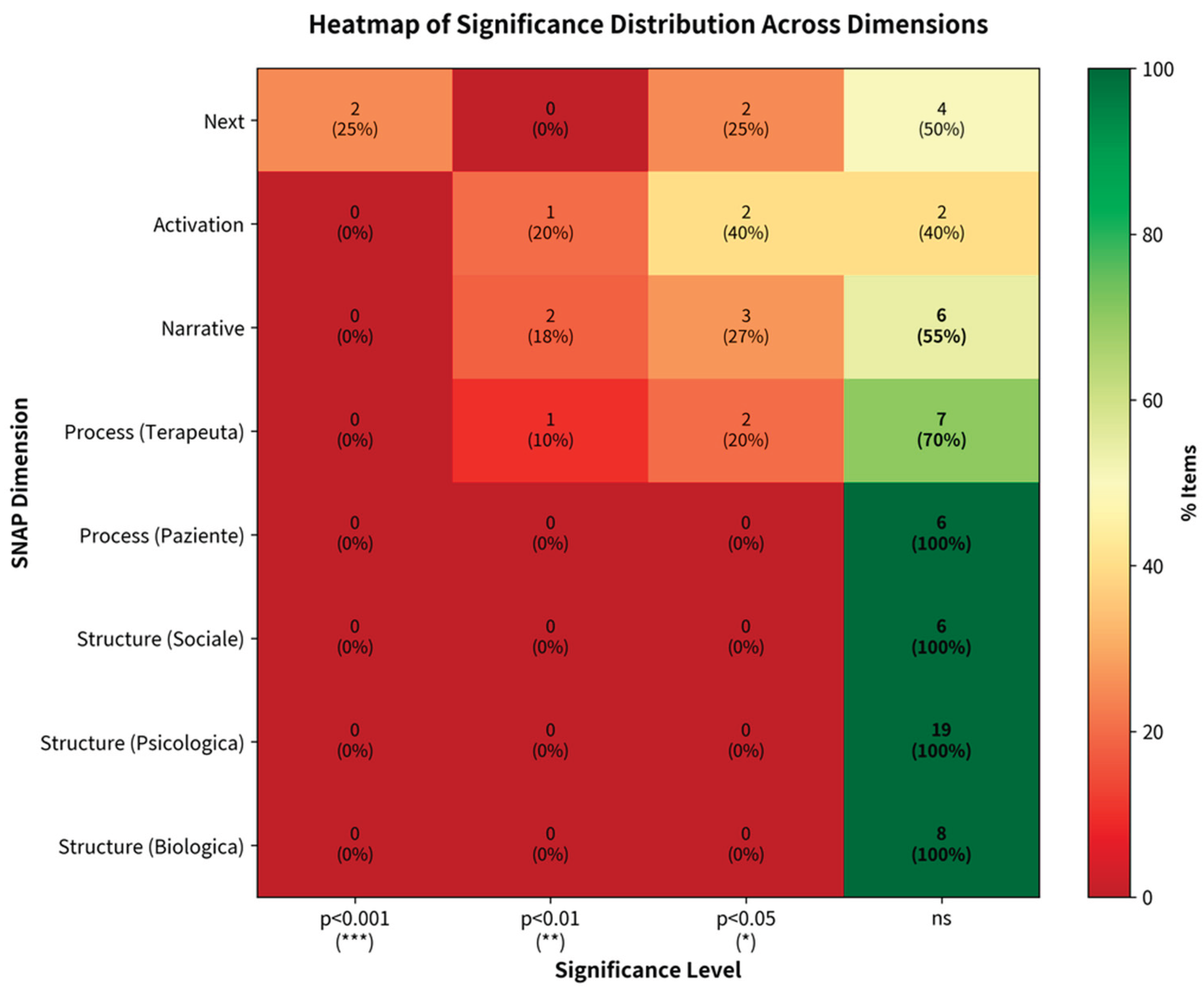
Heatmap of statistical significance distribution across SNAP dimensions. Cell values indicate count and percentage of items at each significance level (p<0.001***, p<0.01**, p<0.05*, ns). Color intensity represents percentage concentration (red=0%, green=100%). Innovative dimensions (Next, Activation, Narrative) show distributed significance patterns, while Structure dimensions show concentrated non-significance (100% ns), confirming these aspects were already present in therapists' clinical thinking prior to SNAP training.
Figure 6.
Heatmap of statistical significance distribution across SNAP dimensions. Cell values indicate count and percentage of items at each significance level (p<0.001***, p<0.01**, p<0.05*, ns). Color intensity represents percentage concentration (red=0%, green=100%). Innovative dimensions (Next, Activation, Narrative) show distributed significance patterns, while Structure dimensions show concentrated non-significance (100% ns), confirming these aspects were already present in therapists' clinical thinking prior to SNAP training.
4. Discussion
The goal of this study was to evaluate the perceived utility of the SNAP instrument (Structure, Narrative, Activation, Process, Next) as a support for clinical reflection among Gestalt therapists. The need for such an instrument emerges from the lack of multidimensional frameworks that integrate phenomenological, process-oriented, and relational aspects in psychotherapy assessment (Cuthbert, 2020; Francesetti et al., 2013; Roti et al., 2023). While established instruments such as CORE-OM and WAI measure symptomatic outcomes and therapeutic alliance, there is a lack of systematic tools that direct therapists' attention toward phenomenological and process-oriented dimensions central to Gestalt psychotherapy (Greenberg, 2015; Horvath & Greenberg, 1989).
To address this objective, we adopted a retrospective pre-post design with N=20 professional therapists, each of whom applied SNAP to a real clinical case, retrospectively evaluating the perceived utility of each of the 73 items before and after learning about SNAP. The retrospective pre-test design, while subject to potential recall bias, represents a pragmatic and effective approach for evaluating professional training and changes in reflective awareness, as it allows for partial control of response-shift bias that afflicts traditional pre-post designs (Howard et al., 1979; Drennan & Hyde, 2008). Each item was rated on a 1-9 Likert scale, enabling quantitative analysis of the distribution of perceived increments.
The results indicate that SNAP significantly enhances therapists' reflective capacity in specific dimensions, with a differentiated and theoretically coherent pattern of effects. The overall effect size (Cohen's d = 0.29, p < 0.05) indicates a global small-to-medium increment, with 20.5% of items (15/73) showing statistically significant increments (p < 0.05). However, dimensional analysis reveals a non-uniform distribution of effects: phenomenological and process-oriented dimensions (Next d = 0.63, Activation d = 0.51, Narrative d = 0.45, Process-Therapist d = 0.43) present medium effects, while structural dimensions (Structure-Biological d = -0.02, Structure-Social d = 0.15, Structure-Psychological d = 0.10) show effects approaching zero. This pattern suggests that SNAP does not replicate conventional clinical assessment but introduces innovative elements specifically aligned with the phenomenological foundations of Gestalt therapy (Perls et al., 1951; Polster & Polster, 1973). The structural dimensions, showing minimal utility gains, were likely already integrated into clinical practice through standard intake procedures, DSM/ICD training, and biopsychosocial approaches; conversely, the phenomenological and process-oriented dimensions represent areas toward which SNAP systematically directs attention, generating new reflective awareness (Joyce & Sills, 2018; Francesetti, 2007).
4.1. Clinical and Theoretical Implications
These findings have several implications for clinical practice and training. First, SNAP provides a structured framework for attending to dimensions that clinicians may value but inconsistently systematize (Geniola et al., 2025). Second, the very large effects for metaphor-oriented items suggest this represents an underutilized resource. Third, items focusing on therapist somatic experience showed meaningful utility gains, supporting the value of training in embodied self-awareness (Lommatzsch et al., 2024).
Fourth, the low baseline but high utility for early developmental items suggests more systematic attention to developmental history could enhance case formulation. Finally, SNAP integrates both structural assessment (necessary but already present) and process-oriented exploration (novel and valuable).
From a theoretical perspective, findings support the distinction between content-focused assessment (what the patient reports) and process-focused assessment (how patient and therapist engage). The Next dimension, focusing on emergent direction and metaphorical representation, addresses the nonlinear, self-organizing nature of therapeutic change—concepts less central to linear, symptom-focused assessment approaches.
4.2. Limitations and Future Directions
Several limitations must be considered. First, the small sample size (N = 20) lacks statistical power for definitive conclusions; replication with larger samples (N = 50-100) is needed. Second, the retrospective pre-test design relies on participants' ability to accurately recall their prior clinical thinking. However, this approach was methodologically necessary to control for response-shift bias, as therapists could not meaningfully evaluate the utility of SNAP dimensions before understanding the framework itself (Howard et al., 1979; Drennan & Hyde, 2008). Future studies with larger samples would reduce measurement error and strengthen confidence in findings. Third, each therapist applied SNAP to one case, limiting generalizability. Fourth, the study measured perceived utility of SNAP rather than behavioral changes in clinical practice. Future research should examine whether SNAP use leads to observable changes in therapists' reflective capacity, case formulation quality, or supervision discussions, as measured through qualitative analysis or supervisor ratings. Fifth, most participants were from a single Italian Gestalt therapy training institute, limiting generalizability across therapeutic orientations, clinical settings, and cultural contexts.
Sixth, this study examined face validity (perceived utility of SNAP) but did not assess internal consistency, construct validity or factor structure. Comprehensive psychometric validation is needed, with careful consideration of which reliability metrics are conceptually appropriate for an instrument assessing both stable characteristics and dynamic therapeutic processes.
Future research should pursue several complementary directions. Expanded samples with diverse theoretical orientations, countries, and clinical settings are needed to assess whether SNAP's utility generalizes beyond Gestalt therapy. Longitudinal process studies examining how SNAP dimensions evolve across therapy phases could reveal developmental patterns in the therapeutic field and identify early process indicators that predict positive outcomes. Clinical utility studies are needed (Di Sarno et al., 2025) to determine optimal administration frequency (e.g., every 5-10 sessions versus monthly) and to develop abbreviated versions for routine clinical use while preserving construct validity. Theoretical development should explore relationships between SNAP profiles and therapeutic trajectories, potentially identifying characteristic patterns associated with successful versus stalled processes, while acknowledging that each therapeutic relationship is unique. Finally, cultural adaptation and validation in multiple languages is essential to assess whether SNAP's phenomenological dimensions are culturally universal or require modifications for different therapeutic contexts and cultural frameworks.
5. Conclusions
This preliminary validation study provides initial evidence that SNAP enhances psychotherapists' reflective capacity by systematically directing attention to phenomenological and process-oriented dimensions of therapeutic encounter. The most novel and valued aspects involve metaphorical representation of process, developmental narrative, embodied therapist awareness, and in-session sensory-motor engagement. The clear differentiation between high-utility phenomenological dimensions and low-utility structural dimensions suggests SNAP introduces specific innovations aligned with Gestalt therapy's phenomenological foundations.
While limited by small sample size and methodological constraints, these preliminary findings support SNAP's potential as a tool for clinical practice, training, and research. The instrument provides a structured framework for integrating empirical rigor with phenomenological complexity. Future research with larger, more diverse samples is needed to confirm findings, establish comprehensive psychometric properties, examine relationships between SNAP dimensions and clinical outcomes, and refine the instrument. We invite the broader psychotherapy research community to engage with SNAP and contribute to its ongoing development. SNAP represents a first step toward evidence-based assessment of phenomenological and relational dimensions in psychotherapy.
Author Contributions
Conceptualization, R.S. and E.M.; methodology, R.S. and C.S.; software, S.V.; validation, R.S., L.L.M. and V.C.; formal analysis, C.S.; investigation, L.L.M., E.T. and S.V.; resources, E.M.; data curation, V.C. and E.T.; writing—original draft preparation, R.S. and C.S.; writing—review and editing, E.M., L.L.M. and V.C.; visualization, S.V.; supervision, E.M.; project administration, R.S.; no funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The SNAP Tool (Full Version, 73 items) used in this study is publicly available at: https://forms.gle/yXFw3E39tXvqDSc17. The validation questionnaire is publicly available at: https://forms.gle/qY63G3eJFe1Ecy918. The datasets generated and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions related to sensitive personal information.
Acknowledgments
The authors gratefully acknowledge the 20 psychotherapists who participated in this study. We thank the SiPGI - Postgraduate School of Integrated Gestalt Psychotherapy (Torre Annunziata) for institutional support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Beisser, A. The paradoxical theory of change. In Gestalt therapy now; Fagan, J., Shepherd, I. L., Eds.; Science and Behavior Books, 1970; pp. 77–80. [Google Scholar]
- Capparelli, T.; Langella, C.; Giannetti, C.; Scognamiglio, R.; Messina, M. Phenomenology of Shame: a Review on Genesis and Developments. Phenomena Journal - International Journal of Psychopathology, Neuroscience and Psychotherapy 2022, 4(1), 8–18. [Google Scholar] [CrossRef]
- Castonguay, L. G.; Hill, C. E. (Eds.) Transformation in psychotherapy: Corrective experiences across cognitive behavioral, humanistic, and psychodynamic approaches; American Psychological Association, 2012. [Google Scholar]
- Cini, A.; Oliva, S.; Quattrini, G. P. Well - Being: a proposal research on Gestalt therapy efficacy. Phenomena Journal - International Journal of Psychopathology, Neuroscience and Psychotherapy 2019, 1(1), 44–53. [Google Scholar] [CrossRef]
- Cuthbert, B. N. The role of RDoC in future classification of mental disorders. Dialogues in Clinical Neuroscience 2020, 22(1), 81–85. [Google Scholar] [CrossRef]
- Di Sarno, A. D.; Barone, M.; De Masis, M.; Di Gennaro, R.; Fabbricino, I.; Forino, A. A.; Luceri, J. F. Validity and effectiveness of Gestalt Play Therapy: a proposal for defining a shared research protocol. Phenomena Journal - International Journal of Psychopathology, Neuroscience and Psychotherapy 2025, 7(3), 98–105. [Google Scholar] [CrossRef]
- Drennan, J.; Hyde, A. Controlling response shift bias: The use of the retrospective pre-test design in the evaluation of a master's programme. Assessment & Evaluation in Higher Education 2008, 33(6), 699–709. [Google Scholar]
- Elliott, R.; Bohart, A. C.; Watson, J. C.; Murphy, D. Therapist empathy and client outcome: An updated meta-analysis. Psychotherapy 2018, 55(4), 339. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.; Connell, J.; Barkham, M.; Margison, F.; McGrath, G.; Mellor-Clark, J.; Audin, K. Towards a standardised brief outcome measure: Psychometric properties and utility of the CORE-OM. British Journal of Psychiatry 2002, 180(1), 51–60. [Google Scholar] [CrossRef]
- Fogarty, M.; Bhar, S.; Theiler, S. Development and validation of the gestalt therapy fidelity scale. Psychotherapy Research 2020, 30(4), 495–509. [Google Scholar] [CrossRef] [PubMed]
- Francesetti, G. Panic attacks and postmodernity: Gestalt therapy between clinical and social perspectives; FrancoAngeli, 2007. [Google Scholar]
- Francesetti, G. The phenomenal field: the origin of the self and the world. Phenomena Journal - International Journal of Psychopathology, Neuroscience and Psychotherapy 2024, 6(1), 1–5. [Google Scholar] [CrossRef]
- Francesetti, G.; Gecele, M.; Roubal, J. Gestalt therapy approach to psychopathology. In Gestalt therapy in clinical practice: From psychopathology to the aesthetics of contact; FrancoAngeli, 2013; pp. 53–72. [Google Scholar]
- Gelo, O. C. G.; Pritz, A.; Rieken, B. (Eds.) Psychotherapy research: Foundations, process, and outcome; Springer, 2015. [Google Scholar] [CrossRef]
- Geniola, N.; Cini, A.; Ballotti, S.; Roti, S.; Gabriele, G.; Verardo, A. Well-being and quality of life for the psychotherapist: a research proposal. Phenomena Journal - International Journal of Psychopathology, Neuroscience and Psychotherapy 2025, 7(2), 77–81. [Google Scholar] [CrossRef]
- Greenberg, L. S. Emotion-focused therapy: A clinical synthesis. FOCUS: The Journal of Lifelong Learning in Psychiatry 2010, 8(1), 32–42. [Google Scholar] [CrossRef]
- Greenberg, L. S. Emotion-focused therapy: Coaching clients to work through their feelings, 2nd ed.; American Psychological Association, 2015. [Google Scholar]
- Horvath, A. O.; Greenberg, L. S. Development and validation of the Working Alliance Inventory. Journal of Counseling Psychology 1989, 36(2), 223–233. [Google Scholar] [CrossRef]
- Howard, G. S.; Ralph, K. M.; Gulanick, N. A.; Maxwell, S. E.; Nance, D. W.; Gerber, S. K. Internal invalidity in pretest-posttest self-report evaluations and a re-evaluation of retrospective pretests. Applied Psychological Measurement 1979, 3(1), 1–23. [Google Scholar] [CrossRef]
- Joyce, P.; Sills, C. Skills in Gestalt counselling & psychotherapy, 4th ed.; SAGE, 2018. [Google Scholar]
- Lambert, M. J. Outcome in psychotherapy: The past and important advances. Psychotherapy 2013, 50(1), 42–51. [Google Scholar] [CrossRef] [PubMed]
- Lambert, M. J.; Burlingame, G. M.; Umphress, V.; Hansen, N. B.; Vermeersch, D. A.; Clouse, G. C.; Yanchar, S. C. The reliability and validity of the Outcome Questionnaire. Clinical Psychology & Psychotherapy 1996, 3(4), 249–258. [Google Scholar]
- Lommatzsch, A.; Cirasino, D..; De Fabrizio, M..; Orlando, S..; Terzi, C.; Antoncecchi, M. The Working on the emotion of anger in panic disorder: a phenomenological-existential and Gestalt psychotherapy approach. Phenomena Journal - International Journal of Psychopathology, Neuroscience and Psychotherapy 2024, 6(1), 6–11. [Google Scholar] [CrossRef]
- Orlando, G. Gestalt Therapy and Panic attacks: Base Relational Model, life cycle and clinic in GTK. Phenomena Journal - International Journal of Psychopathology, Neuroscience and Psychotherapy 2020, 2(2), 82–91. [Google Scholar] [CrossRef]
- Panksepp, J. Affective neuroscience: The foundations of human and animal emotions; Oxford University Press, 1998. [Google Scholar]
- Perls, F. Ego, hunger and aggression: A revision of Freud's theory and method; Allen & Unwin, 1947. [Google Scholar]
- Perls, F. The Gestalt approach & eye witness to therapy; Science and Behavior Books, 1973. [Google Scholar]
- Perls, F.; Hefferline, R.; Goodman, P. Gestalt therapy: Excitement and growth in the human personality.; Julian Press, 1951. [Google Scholar]
- Polster, E.; Polster, M. Gestalt therapy integrated: Contours of theory and practice; Brunner/Mazel, 1973. [Google Scholar]
- Quattrini, P.; Cini, A. Theory, Practice and Technique: Self-supervision in Gestalt psychotherapy. Phenomena Journal - International Journal of Psychopathology, Neuroscience and Psychotherapy 2020, 2(1), 78–88. [Google Scholar] [CrossRef]
- Rainauli, A. Through the eyes of Gestalt therapy: The emergence of existential experience on the contact boundary. Phenomena Journal - International Journal of Psychopathology, Neuroscience and Psychotherapy 2025, 7(1), 20–30. [Google Scholar] [CrossRef]
- Roti, S.; Berti, F.; Geniola, N.; Zajotti, S.; Calvaresi, G.; Defraia, M.; Cini, A. A Gestalt journey: how the well-being changes during a Gestalt treatment. Phenomena Journal - International Journal of Psychopathology, Neuroscience and Psychotherapy 2023, 5(2). [Google Scholar] [CrossRef]
- Schiepek, G.; Tominschek, I.; Heinzel, S. Self-organization in psychotherapy: testing the synergetic model of change processes. Frontiers in Psychology 2014, 5, 1089. [Google Scholar] [CrossRef] [PubMed]
- Stern, D. N. The present moment in psychotherapy and everyday life (norton series on interpersonal neurobiology); WW Norton & Company, 2004. [Google Scholar]
- Wampold, B. E.; Imel, Z. E. The great psychotherapy debate: The evidence for what makes psychotherapy work, 2nd ed.; Routledge, 2015. [Google Scholar]
- Wheeler, G. Beyond individualism: Toward a new understanding of self, relationship, and experience.; Gestalt Journal Press, 2000. [Google Scholar]
- Yontef, G. M. Awareness, dialogue, and process: Essays on Gestalt therapy; Gestalt Journal Press, 1993. [Google Scholar]

Table 1.
1 Results by SNAP Dimension (Ranked by Cohen's d). 1 T1 = retrospective pre-test; T2 = post-test; Δ = difference; d = Cohen's d; Sig% = percentage of items with p < 0.05.
Table 1.
1 Results by SNAP Dimension (Ranked by Cohen's d). 1 T1 = retrospective pre-test; T2 = post-test; Δ = difference; d = Cohen's d; Sig% = percentage of items with p < 0.05.
| Dimension | N | T1 M(SD) | T2 M(SD) | Δ M(SD) | d | Sig% |
|---|---|---|---|---|---|---|
| Next | 8 | 5.86 (1.80) |
7.31 (1.65) |
1.44 (2.34) |
0.63 | 50 |
| Activation | 5 | 5.85 (1.90) |
6.83 (1.95) |
0.98 (2.06) |
0.51 | 60 |
| Narrative | 11 | 5.65 (2.18) |
6.68 (2.14) |
1.03 (2.26) |
0.45 | 45 |
|
Process (Therapist) |
10 | 5.99 (1.93) |
7.10 (1.77) |
1.10 (2.62) |
0.43 | 30 |
|
Process (Patient) |
6 | 6.36 (1.84) |
7.09 (2.07) |
0.73 (2.48) |
0.30 | 0 |
|
Structure (Social) |
6 | 6.24 (2.07) |
6.60 (2.04) |
0.36 (2.30) |
0.15 | 0 |
|
Structure (Psychological) |
19 | 6.04 (2.13) |
6.23 (2.25) |
0.19 (2.17) |
0.10 | 0 |
|
Structure (Biological) |
8 | 6.34 (2.13) |
6.31 (2.16) |
-0.03 (2.65) |
-0.02 | 0 |
Table 2.
Top 10 Items with Greatest Utility Increase2. 2 . Items showing greatest increase from T1 to T2. Δ = T2-T1 difference; d = Cohen's d effect size.
Table 2.
Top 10 Items with Greatest Utility Increase2. 2 . Items showing greatest increase from T1 to T2. Δ = T2-T1 difference; d = Cohen's d effect size.
| Rank | Item | Dimension | T1 | T2 | Δ | d |
|---|---|---|---|---|---|---|
| 1 | Parola/immagine/fantasia descrit... | Next | 4.60 | 7.40 | 2.80 | 1.28 |
| 2 | Immagini/metafore/narrazioni rap... | Next | 4.75 | 6.95 | 2.20 | 1.09 |
| 3 | Contesto di nascita | Narrative | 4.30 | 6.30 | 2.00 | 0.68 |
| 4 | Cambiamenti corporei e vissuti a... | Narrative | 5.20 | 7.00 | 1.80 | 0.74 |
| 5 | Tendenza all'interazione del ter... | Process (Therapist) |
5.60 | 7.15 | 1.55 | 0.66 |
| 6 | Percezione respiro del terapeuta | Process (Therapist) |
5.50 | 7.00 | 1.50 | 0.55 |
| 7 | Nuove consapevolezze/comportamen... | Next | 5.75 | 7.25 | 1.50 | 0.55 |
| 8 | Qualità del legame di attaccamento | Narrative | 5.80 | 7.15 | 1.35 | 0.50 |
| 9 | Cambiamenti del terapeuta in rel... | Next | 6.05 | 7.35 | 1.30 | 0.45 |
| 10 | Contenuti pensiero del terapeuta... | Process (Therapist) |
5.90 | 7.15 | 1.25 | 0.45 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



