
Submitted:
28 January 2026
Posted:
29 January 2026
You are already at the latest version
Abstract
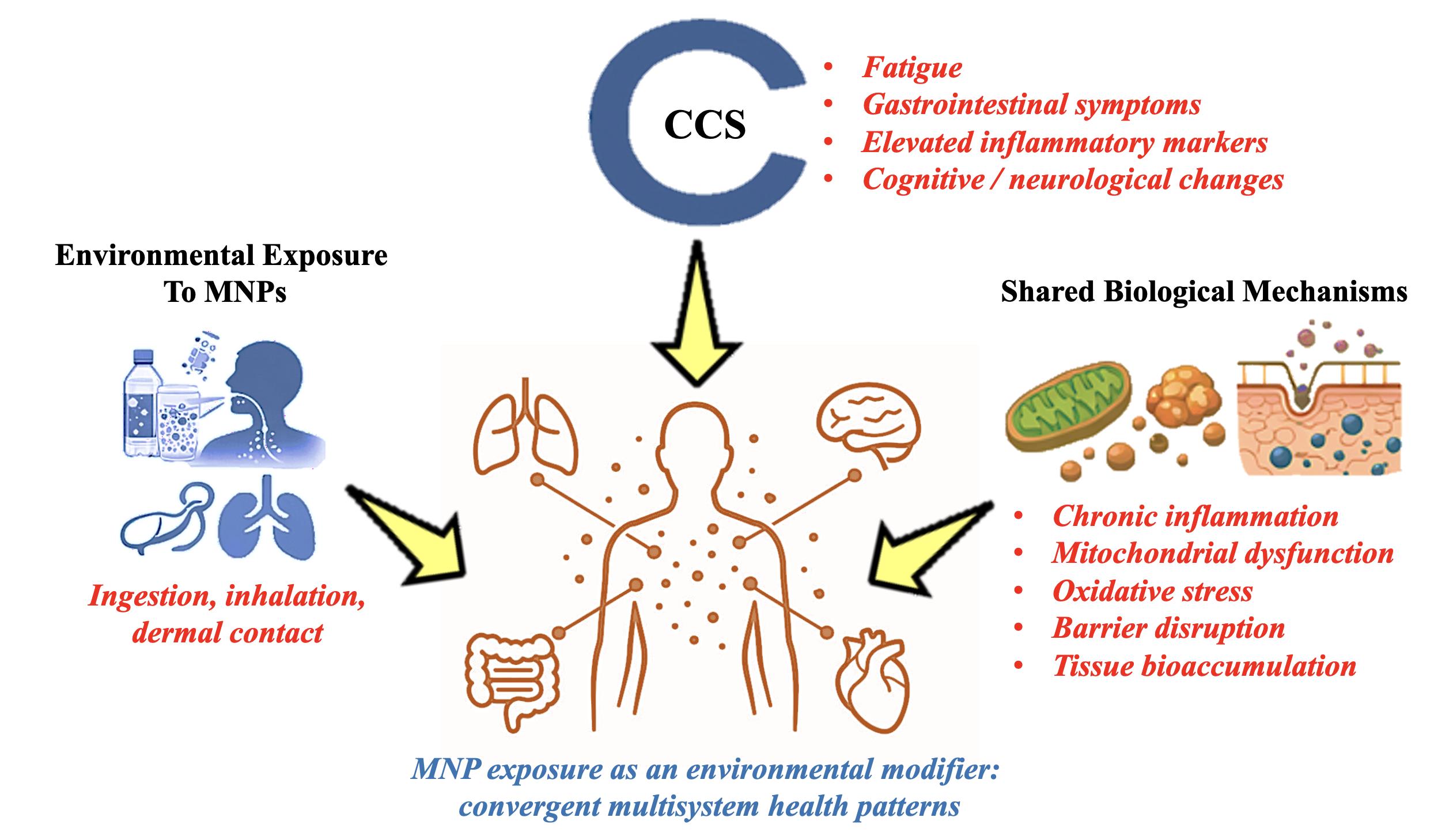
Microplastics and Nanoplastics (MNPs) have emerged as pervasive environmental contaminants with growing evidence of systemic health effects. This study characterizes the spectrum of signs and symptoms associated with MNP exposure, examining potential mechanisms of toxicity, patterns of exposure, and biological responses. By integrating clinical observations and emerging experimental data, the research aims to clarify possible links between MNPs and inflammatory, metabolic, and neurological outcomes. Clinical data from 21 different classes of diseases, comprising of 375 illness were analyzed on the base of the 26 of the most common sign and symptoms, supplemented by to 4 variables related to the environment for a total of 30 (defined as Chicago Cluster System or CCS). Illnesses characterized by at least 8 signs were considered relevant. Association was explored though integration of the current literature. 40 diseases (21 chronic and 19 acute) across 12 different Classes were found to align with the 30 sign and symptoms of the CCS. Chronic illnesses included Alzheimer’s Disease, Parkinson, Diabetes Type 2, IrritableBowel Syndrome (IBS), Chronic Obstructive Pulmonary Disease (COPD), Rheumatoid arthritis, and Post Covid-19 syndrome, Acute illnesses included illnesses while Gastroenteritis, Pancreatitis, Meningitis, Acute Pneumonia and Acute hepatitis. The most represented sign and symptoms were fatigue, dyspepsia, C-Reactive Protein (CRP) increase, fever, cognitive changes, hematological abnormalities and imaging modifications. MNP exposure is associated with a multisystemic clinical presentation. These findings underscore the need to recognize MNPs as environmental cofactors in complex disease syndromes and to integrate clinical, biochemical, and imaging evidence in future epidemiological studies.
Keywords:
Chicago cluster system
; microplastics
; nanoplastics
; microplastics syndrome
; chitosan
; procambarus clarkii
1. Introduction
Global plastic production has reached unprecedented levels, exceeding 430.9 million tons in 2024 and projected to increase by nearly 70% by 2040 [1]. The fragmentation of these materials generates micro-nanoplastics (MNPs), particles smaller than 5 mm, which are now ubiquitous in the environment and have been detected in drinking water, table salt, and food products. Human exposure is therefore continuous and widespread, raising growing concerns about potential health consequences [2,3].
Recent studies have demonstrated that MNPs can cross biological barriers, accumulate in tissues, and interfere with cellular and immune processes [4,5]. Clinical implications include oxidative stress, chronic inflammation, and possible effects on cardiovascular, respiratory, and gastrointestinal systems. While the toxicological pathways are increasingly documented, a clear clinical definition of microplastic-related disease remains elusive.
In 2025, the Microplastics Syndrome (MPSyn) was considered for the first time to determine the type and the number of sign and symptoms defined as CHICAGO CLUSTER SYSTEM (CCS) [6] and characterized by a recurring constellation of 30 signs and symptoms (26 clinical and 4 environmental) and suspected to be associated with MNP exposure. This concept represents a decisive step toward formalizing a new clinical entity linked to environmental contaminants.
Nevertheless, it remains essential to examine the overlap between this cluster and established diseases, in order to determine whether the MPSyn constitutes an autonomous entity or reflects a cross-cutting pattern within existing pathologies. Table S1 summarizes all the 26 signs and symptoms which were identified in clinical and epidemiological data as possibly related to the MPSyn [6].
2. Materials and Methods
A systematic symptom-based approach was used to deal with the lack of a unified clinical framework for assessing the health relevance of exposure to MNPs. In order to identify recurrent multisystem symptoms associated to environmental exposure, the CCS was developed with a focus on non-specific but convergent clinical characteristics.
2.1. Conceptual Framework of the CCS
The CCS was established as a practical clinical construct meant to incorporate a variety of indications and symptoms into a framework for reproducible assessment. Instead of concentrating on single-organ pathology, it represents systemic biological stress that may be brought on by long-term exposure to MNPs. Based on consistent reporting from epidemiological, clinical, and experimental studies, the system consists of four environmental exposure variables and 26 clinical signs and symptoms. In order to identify clinically significant overlap while minimizing the potential of arbitrary symptom aggregation, a threshold of at least six CCS indicators was employed. Previous research has linked a greater chance of MPSyn to higher symptom loads (≥ 8 indicators), indicating that cumulative symptoms increase specificity. In order to maintain the exploratory aspect of the study, the lower threshold was deliberately employed in the present assessment to investigate intersections between CCS and recognized disorders without establishing causality [6].
Twenty-one classes of diseases were considered, and each selected based on the presence of at least 6 signs and symptoms consistent with the CCS (Tables S2-S13). The text used for disease analysis were the most common and internationally recognized [7]. By systematically mapping these overlaps, we aim to provide a reproducible framework for clinical and epidemiological research, and to advance the dialogue on the health impacts of microplastic exposure.
2.2. Disease Selection and Symptom Mapping Procedure
Using this framework as a guide, 21 disease classes were chosen to represent the main physiological systems that are expected to be impacted by exposure to the environment. To improve reliability and minimize interpretative bias, diseases in each class were evaluated using globally accepted clinical descriptions. CCS signs and symptoms were systematically mapped against conventional clinical descriptions for every disease. Symptom overlap was only taken into account when it was specifically identified as a defining aspect of the disease. Conservative inclusion criteria were used when correspondence was ambiguous or incomplete. For additional analysis, diseases with six or more CCS indicators were considered. This systematic methodology was developed to achieve a balance among the inherent limitations of narrative integration and methodological rigor [6].
The environmental variable to be added as part of the CCS were only 4 as follows: Living in urban areas with high pollution and traffic; regularly drinks bottled water; a diet rich of small fishes; working with plastics, textiles or industrial setting. These four variables should be added to the other sign and symptoms according to the presence in the subject. As previously mentioned, there is a > 95% probability of being affected by MPSyn if the signs and symptoms are more than 8 [6].
Twenty-one classes of diseases were considered (Tables S2-S13) following each selected disease based on the presence of at least 6 signs and symptoms consistent with the CCS. By methodically mapping these overlaps, we aim to further debate on the health effects of MNP exposure and provide a reproducible framework for epidemiological and clinical research.
3. Discussion
The comparison analysis's outcomes suggest that CCS-aligned symptom patterns arise across a range of disease categories rather than being restricted to specific diseases. This result suggests the potential that the reported clinical convergence is due to similar biological pathways rather than disease-specific mechanisms.
3.1. Principal Outcomes
The claimed CCS combines at least six signs and symptoms with a significant number of well-established clinical diseases, demonstrated by this comparative study covering 21 classes of disease. Findings indicate that the constellation of symptoms linked to MNP exposure is not isolated but rather generally overlaps with several types of systemic diseases. The observed correlation highlights the recurrent but non-specific nature of CCS symptoms and implies that similar biological pathways, rather than disease-specific processes, are involved. These results can be understood in two primary manners. First, exposure to MNPs may serve as a common environmental stressor that can intensify, create, or reproduce symptom patterns already identified in several kinds of chronic and acute diseases. Second, the data raises the question of whether CCS is a cross-cutting condition included into current disease frameworks or a separate nosological entity. Clinically, CCS might be a systemic response to long-term exposure to the environment rather than an emerging disease group that needs to be classified separately.
The symptom distribution in the CCS reflects shared systemic pathways rather than disease-specific mechanisms. Persistent fatigue (65%) is the most frequent symptom, driven by mitochondrial dysfunction, chronic inflammation, and altered energy metabolism common across conditions. Gastrointestinal symptoms, including dyspepsia (57.5%) and abdominal pain (37.5%), highlight the gut’s role as a sentinel organ exposed to environmental factors. Altered inflammatory indices (55%) and fever (47.5%) indicate widespread immune activation. Neurological manifestations such as headache (45%) and cognitive alterations (42.5%) arise from neuroinflammation and blood–brain barrier vulnerability. Hematological disturbances (40%) reflect systemic stress, while ultrasound alterations (37.5%) confirm organ-level effects of chronic inflammatory processes. Table 2 provides the data concerning the distribution of symptoms in each disease.
3.2. Methodological Implications
From an epidemiological perspective, the > 6-symptom criteria used in this review offers a reproducible and practical method for determining the clinical significance overlap between recognized disorders and CCS. Future case-control studies, prospective cohort analyses, and biomarker-driven research aiming at discriminating MNP-associated pathology from conventional disease processes can be developed upon this requirement. Clinicians could discover the tabular synthesis offered here to be a useful tool for generating hypotheses and assisting differential diagnosis in patients with complicated, multisystem presentations. There are significant implications for public health. The broad effect of MNP exposure on human health may be overestimated if it contributes to symptom clusters across several disease categories. Overlapping clinical characteristics imply that MNPs could exacerbate pre-existing conditions, make diagnosis harder, or render treatment decisions more complicated. These outcomes lend validity to the inclusion of environmental exposure assessment in clinical evaluation, especially for patients who have multisystem, unexplained symptoms.
3.3. Microplastics in Blood: Subclinical Exposure
Human blood is known to include MNPs in biomonitoring studies [6,8,9,10], indicating cumulative exposure to a variety of polymer types with different toxicological properties. Significantly, measured concentrations of several vitamins are similar to physiological levels, highlighting their quantitative relevance. A paradox of apparent health is highlighted by the fact that detectable blood levels are often found in people without overt clinical illness [11,12]. Important considerations about latency, subclinical effects, and cumulative risk are brought up by this observation. It is possible that MNP-associated disease only appears after extended exposure or in the context of modifying variables including immunological dysregulation, metabolic stress, aging, or co-exposure to other environmental poisons. Established models of chronic environmental disease are compatible with such dynamics.
3.4. Organ Bioaccumulation and Tissue Tropism
MNPs accumulate preferentially in certain organs, including the brain and liver, according to experimental and post-mortem studies [13,14]. Several studies have shown that exposure to MNPs causes neuronal damage, including loss of dopaminergic neurons, mitochondrial dysfunction, and α-synuclein aggregation, which are important characteristics of Parkinson's disease (Xu et al., 2025). Alzheimer's disease progression is linked to similar mechanisms, such as oxidative stress and neuroinflammation [13,15,16].
According to post-mortem studies, the liver and brain serve as long-term reservoirs, indicating a restricted capacity for clearance and the possibility of long-term toxicological consequences. On the contrary, despite the fact that MNPs have been found in the kidney and have been demonstrated to cause harm, there doesn't seem to be much accumulation [17,18] perhaps because renal clearance is more effective. This organ-specific distribution emphasizes how crucial tissue tropism is to determining systemic risk. Other tissues and biological fluids, such as the lung [19,20,21,22], semen [23,24], placenta [24,25], endometrial [26], and sputum [27,28], were also found to include MNPs, confirming the possibility of widespread systemic exposure [29].
3.5. Symptom Distribution and Biological Plausibility in the CCS
Common systemic pathways rather than condition-specific processes result in the predominance of shared symptoms among various diseases. Led by neuroendocrine, immunological, and metabolic dysregulation associated with chronic inflammation and mitochondrial dysfunction, fatigue constitutes the most common manifestation [30,31,32,33,34,35]. The gut is a sentinel organ exposed to environmental stresses, where mucosal irritation, dysbiosis, and inflammatory signaling converge [36,37,38,39,40] as suggested by gastrointestinal complaints, especially dyspepsia and abdominal pain [41,42,43,44,45,46]. Fever and inflammatory markers such as CRP are signs of immune activation, emphasizing the crucial role of systemic inflammation [35,47,48,49]. Neuroinflammation, vascular dysfunction, and blood–brain barrier penetration are the root causes of neurological symptoms as headache and cognitive decline [16,35,47,50]. Immune mediators, circulating particles, and vascular integrity all interact to trigger hematological disorders [51]. Lastly, non-invasive proof of systemic involvement is provided by ultrasonographic anomalies, which show organ-level effects of long-term inflammatory and metabolic stress [51,52].
3.6. Key Symptom Domains
Multiple diseases converge on shared biological pathways, which suggests why specific signs recurring. Vascular function, energy metabolism, and immunological modulation are all disrupted by chronic inflammation, which acts as a unifying factor [35] gut, brain, and blood are among the most vulnerable organs due to their high demand on metabolism or barrier capabilities. These processes are intensified by environmental stressors, resulting in nonspecific yet consistent clinical patterns. Consequently, symptoms result from systemic dysregulation impacting interconnected physiological networks spanning multiple diseases rather than from specific organ dysfunction [16,32,53].
3.7. Integrated Mechanistic Model Linking MNP Exposure to Multisystem Symptoms
A mechanistic hypothesis based on systemic dysregulation is supported by the significant overlap between CCS signs and other diseases. Long-term exposure to MNPs could function as a chronic environmental stressor that might damage biological barriers, cause low-grade inflammation, and promote mitochondrial malfunction. The prevalence of fatigue, gastrointestinal problems, increased inflammatory markers, and cognition abnormalities seen in all CCS-aligned disorders can be explained coherently by these mechanisms.
This idea is further supported by experimental and post-mortem evidence of MNP bioaccumulation in organs including the brain and liver, which suggests prolonged tissue exposure with minimal removal. Due to dysbiosis and barrier dysfunction, the gastrointestinal tract seems to be a major site of exposure as well as an amplifier of systemic effects. Multisystem symptoms may result from the subsequent activation of the gut–blood and gut–brain axes, whereby could propagate inflammatory and neuroendocrine signals.
While hematological alterations may reflect interactions between circulating particles and blood components, neuroinflammation and enhanced blood–brain barrier permeability provide medical explanations for behavioural and cognitive anomalies. Once combined as entirety, these mechanisms provide credibility to the hypothesis that the CCS is not some sort of separate nosological entity but rather a systemic response pattern resulting from long-term exposure to the environment.
3.8. Implications for Environmental Epidemiology and Public Health Surveillance
From an epidemiological standpoint, these results raise reliance on conventional disease-centric models that might understate the adverse effects of environmental pollutants on health. In order to capture non-specific, multisystem symptom constellations involving multiple diagnostic categories, the CCS offers a supplementary framework.
Particularly in diseases with multimorbidity or uncertain etiology, incorporating CCS-based assessments into population research may increase detection of environmentally mediated health impacts and reduce diagnostic misclassification. Additionally, the CCS's inclusion of environmental exposure factors is consistent with exposome-based protocols, which makes it easier to translate environmental monitoring into clinical observation.
CCS-informed surveillance may improve the earlier identification of population-level effects associated with rising plastic pollution at the public health level, supporting evidence-based regulations and prevention strategies.
4. Putative Limitations
The observed patterns are coherent, but there are still certain limitations that require to be emphasized. The lack of individual-level clinical data limits the analysis of dose-response gradients, temporal correlations, and symptom severity thus rendering it difficult to reach conclusions regarding causality. Furthermore, due to non-specific symptoms occur frequently in many diseases regardless of environmental exposure, relying solely on established clinical descriptions raises the risk of circularity.
The current approach lacks the capacity to distinguish among potential confounders, such as genetic dependence, co-exposures, and lifestyle factors. Furthermore, quantitative measures of internal MNP burden, which are crucial for confirming exposure-effect connections, are not currently included in the CCS. Nevertheless, the ongoing pattern of symptom convergence across several disease categories is a strong signal that requires additional investigation employing prospective, biomarker-driven studies.
Furthermore, whereas typical medical textbooks offer reliable clinical descriptions, they could not adequately account for new information about MNP exposure and its systemic effects. In conclusion, the evidence supports up the belief that exposure to MNPs induces a predictable cluster of non-specific but clinically significant symptoms that span several disease categories. CCS may be a systemic response to long-term environmental exposure rather than an independent disease entity. To elucidate causality and guide preventive and therapeutic strategies, prospective studies incorporating exposure assessment, biomarkers, and long-term clinical outcomes are increasingly necessary.
5. Conclusions
The present findings provide several important insights into regional disparities in PC mortality in Italy. These results highlight the need to evaluate overall dietary patterns rather than isolated nutrients or individual food items. Approximately half of the food categories
The interpretation of MNP exposure as an overall environmental modulator of human health rather than a specific clinical condition is supported by this narrative review, which concludes by demonstrating that the CCS overlaps significantly with recognized acute and chronic diseases. Convergent, non-specific symptom patterns consistent with systemic dysregulation brought on by ongoing environmental stress are observed by the CCS.
This approach promotes exposome-based epidemiology and environmental health research by offering a formal framework for symptom aggregation. In the context of increasing global plastic pollution, additional studies incorporating quantitative exposure assessment, biological markers, and longitudinal clinical outcomes will be crucial to explain causality and suggest preventive and mitigation methods.
Preliminary research indicates that oral chitosan could improve the excretion of MNPs in the stools [54], and clinical trials are being carried out to determine its potential efficacy, even though there are presently no effective treatments for MPSyn. To establish its therapeutic effectiveness in lowering blood levels of MNPs in healthy volunteers, we are currently conducting clinical trials.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1: CCS-26 Non-Specific signs and symptoms; Table S2: Endocrine, Metabolic, and Nutritional Diseases; Table S3: Gastrointestinal, Liver and Biliary Tract Diseases; Table S4: Musculoskeletal and Connective Tissues Diseases; Table S5: Respiratory Diseases; Table S6: Hematological and Oncological Diseases; Table S7: Immunological and Allergic Diseases; Table S8: Infectious Diseases; Table S9: Nervous System Diseases; Table S10: Psychiatric Diseases; Table S11: Genito-urinary Diseases; Table S12: Gynecological and Obstetric Diseases; Table S13: Poisonings; Table S14: Diseases classes with signs and symptoms of CCS.
Author Contributions
U.C.: Conceptualization, methodology, validation, visualization, formal analysis, investigation, supervision, writing—original draft preparation, writing—review and editing; C..C.: Conceptualization, methodology, validation, visualization, investigation, writing—original draft preparation, writing—review and editing; G.B.: Validation, visualization, writing—review and editing; M.R.C.: Validation, visualization, writing—review and editing; S.M.: Validation, visualization, writing—review and editing; M.R.: Data curation, statistical analysis, visualization, writing—review and editing; Ma.R.: Data curation, software, statistical analysis; G.Z.: Validation, visualization, writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Acknowledgments
This article is dedicated to Alexander Santiago Casella Flores.
Conflicts of Interest
The authors declare that they have no known competing financial interest or personal relationships that could have influenced the work reported in this paper.:.
Abbreviations
The following abbreviations are used in this manuscript:
| CCS | Chicago Cluster System |
| COPD | Chronic Obstructive Pulmonary Disease |
| CRP | C-Reactive Protein |
| IBS | Irritable Bowel Syndrome |
| MNPs | Micro-Nanoplastics |
| MPSyn | Microplastic Syndrome |
References
- Plastic Europe 2025 Plastics—The Fast Facts 2025 Plastics Europe. 2025. Available online: https://plasticseurope.org/wp-content/uploads/2025/09/PE_TheFacts_25_digital-1pager-scrollable.pdf (accessed on 03 November 2025).
- Chen, L.; Han, B.; Yang, S.; Guo, L.; Zhao, L.; Liu, P.; Chen, Y. Toxicological effects and mechanisms of renal injury induced by inhalation exposure to airborne nanoplastics. J. Hazard. Mater. 2025, 488, 137393. [Google Scholar] [CrossRef] [PubMed]
- Mahalingaiah, S.; Nadeau, K. C.; Christiani, D. C. Microplastics and human health. JAMA 2025, 334(21), 1941–1942. [Google Scholar] [CrossRef] [PubMed]
- Pathak, D. Enemies of the hormones: microplastics and endocrine disruptors impacting public health. Health and Climate Change. 2025, pp. 119–150. (accessed on 03 November 2025). [CrossRef]
- Prattichizzo, F.; Ceriello, A.; Pellegrini, V.; La Grotta, R.; Graciotti, L.; Olivieri, F.; Paolisso, G. Micro-nanoplastics and cardiovascular diseases: evidence and perspectives. Eur. Heart J. 2024, 45(38), 4099–4110. [Google Scholar] [CrossRef] [PubMed]
- Cornelli, U; Casella, C; Belcaro, G; Cesarone, MR; Marucci, S; Rondanelli, M; Recchia, M; Zanoni, G. Definition of Emerging Microplastic Syndrome Based on Clinical and Epidemiological Evidence: A Narrative Review. Microplastics 2025, 4(4), 93. [Google Scholar] [CrossRef]
- Kumar, V.; Abbas, A. K.; Aster, J. C.; Debnath, J.; Das, A. Robbins, Cotran & Kumar Pathologic Basis of Disease-E-BOOK. Elsevier Health Sciences, 2025. Available online: https://dn790006.ca.archive.org/0/items/bazbazbaz1/PathologyRobbins7ed.pdf (accessed on 03 November 2025).
- Lee, D. W.; Jung, J.; Park, S. A.; Lee, Y.; Kim, J.; Han, C.; Hong, Y. C. Microplastic particles in human blood and their association with coagulation markers. Sci. Rep. 2024, 14(1), 30419. [Google Scholar] [CrossRef]
- Leonard, S. V.; Liddle, C. R.; Atherall, C. A.; Chapman, E.; Watkins, M.; Calaminus, S. D.; Rotchell, J. M. Microplastics in human blood: Polymer types, concentrations and characterisation using μFTIR. Environ. Int. 2024, 188, 108751. [Google Scholar] [CrossRef]
- Wang, T.; Yi, Z.; Liu, X.; Cai, Y.; Huang, X.; Fang, J.; Guo, S. Multimodal detection and analysis of microplastics in human thrombi from multiple anatomically distinct sites. EBioMedicine 2024, 103. [Google Scholar] [CrossRef]
- Bu, S.; Xu, Y.; Fu, Y.; Guo, Y.; Wu, D.; Zhang, Y. Qualitative and quantitative analysis of microplastics in healthy central nervous and its blood-brain barrier transmission efficiency-A pilot study. Environ. Pollut. 2025, 388, 127392. [Google Scholar] [CrossRef]
- Casella, C.; Cornelli, U.; Zanoni, G.; Moncayo, P.; Ramos-Guerrero, L. Health Risks from Microplastics in Intravenous Infusions: Evidence from Italy, Spain, and Ecuador. Toxics 2025, 13(7), 597. [Google Scholar] [CrossRef]
- Nihart, A. J.; Garcia, M. A.; El Hayek, E.; Liu, R.; Olewine, M.; Kingston, J. D.; Campen, M. J. Bioaccumulation of microplastics in decedent human brains. Nat. Med. 2025, 31(4), 1114–1119. [Google Scholar] [CrossRef]
- Dzierżyński, E.; Blicharz-Grabias, E.; Komaniecka, I.; Panek, R.; Forma, A.; Gawlik, P. J.; Flieger, J. Post-mortem evidence of microplastic bioaccumulation in human organs: insights from advanced imaging and spectroscopic analysis. Arch. Toxicol. 2025, 1–16. [Google Scholar] [CrossRef]
- Ping, H.; Wang, F.; Xi, G.; Li, Y.; Wang, F.; Wang, H.; Li, L.; Han, Y.; Ma, X.; Han, Y.; Shi, Y. Association of microplastics in human cerebrospinal fluid with Alzheimer’s disease-related changes. J. Hazard. Mater. 2025, 494, 138748. [Google Scholar] [CrossRef]
- Siu, A. C. W.; Paudel, K. R.; Singh, G.; Gupta, G.; Singh, S. K.; Chellappan, D. K.; De Rubis, G.; Pathak, S.; George, B. G.; Oliver, G.; Dua, K.; Dhanasekaran, M. Do microplastics play a role in the pathogenesis of neurodegenerative diseases? Shared pathophysiological pathways for Alzheimer’s and Parkinson’s disease. Molecul. Cell. Biochem. 2025, 482(1), 45–62. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Katsouli, J.; Auyang, E.; de la Serna, J. B. Microplastic and nanoplastic pollution and associated potential disease risks. Lancet Planet. Health 2025. [Google Scholar] [CrossRef] [PubMed]
- Chen, C. Y.; Chen, S. Y.; Liao, C. M. Regional and population-scale trends in human inhalation exposure to airborne microplastics: Implications for health risk assessment. Environ. Pollut. 2025, 371, 125950. [Google Scholar] [CrossRef]
- Jenner, L. C.; Rotchell, J. M.; Bennett, R. T.; Cowen, M.; Tentzeris, V.; Sadofsky, L. R. Detection of microplastics in human lung tissue using μFTIR spectroscopy. Sci. Total Environ. 2022, 831, 154907. [Google Scholar] [CrossRef]
- Lu, K.; Zhan, D.; Fang, Y.; Li, L.; Chen, G.; Chen, S.; Wang, L. Microplastics, potential threat to patients with lung diseases. Front. Toxicol. 2022, 4, 958414. [Google Scholar] [CrossRef]
- Taş, B. M.; Tuna, A.; Başaran Kankılıç, G.; Koçak, F. M.; Şencan, Z.; Cömert, E.; Bayar Muluk, N. Role of microplastics in chronic rhinosinusitis without nasal polyps. Laryngoscope 2024, 134(3), 1077–1080. [Google Scholar] [CrossRef]
- Vasse, G. F.; Melgert, B. N. Microplastic and plastic pollution: impact on respiratory disease and health. Eur. Resp. Rev. 2024, 33(172). [Google Scholar] [CrossRef]
- Guo, Y.; Rong, M.; Fan, Y.; Teng, X.; Jin, L.; Zhao, Y. The Presence of Microplastics in Human Semen and Their Associations with Semen Quality. Toxics 2025, 13(7), 566. [Google Scholar] [CrossRef]
- Zhao, Q.; Zhu, L.; Weng, J.; Jin, Z.; Cao, Y.; Jiang, H.; Zhang, Z. Detection and characterization of microplastics in the human testis and semen. Sci. Total Environ. 2023, 877, 162713. [Google Scholar] [CrossRef]
- Braun, T.; Ehrlich, L.; Henrich, W.; Koeppel, S.; Lomako, I.; Schwabl, P.; Liebmann, B. Detection of microplastic in human placenta and meconium in a clinical setting. Pharmaceutics 2021, 13(7), 921. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.; Lee, J.H.; Lee, I.; Park, J.H.; Jung, G.S.; Lee, M. J.; Im, W.; Cho, S.; Choi, S. Investigation of potential toxic of nano-and microplastics on human endometrial stromal cells. Reprod. Toxicol. 2025, 132, 108848. [Google Scholar] [CrossRef] [PubMed]
- Amiri, H.; Moradalizadeh, S.; Jahani, Y.; Nasiri, A. Biomonitoring of microplastics in saliva and hands of young children in kindergartens: identification, quantification, and exposure assessment. Environ. Monit. Assess. 2025, 197(8), 859. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Huang, X.; Bi, R.; Guo, Q.; Yu, X.; Zeng, Q.; Guo, P. Detection and analysis of microplastics in human sputum. Environ. Sci. Technol. 2022, 56(4), 2476–2486. [Google Scholar] [CrossRef]
- Marfella, R.; Prattichizzo, F.; Sardu, C.; Fulgenzi, G.; Graciotti, L.; Spadoni, T.; Paolisso, G. Microplastics and nanoplastics in atheromas and cardiovascular events. N. Engl. J. Med. 2024, 390(10), 900–910. [Google Scholar] [CrossRef]
- Karshikoff, B.; Sundelin, T.; Lasselin, J. Role of inflammation in human fatigue: relevance of multidimensional assessments and potential neuronal mechanisms. Front. Immunol. 2017, 8, 21. [Google Scholar] [CrossRef]
- Katleen, B.; Ynse, D.; Iris, C.; Stephan, C.; Elfi, V.; den Bergh Omer, V.; Lukas, V. O. Fatigability and stress reactivity in patients with chronic fatigue syndrome versus healthy controls. J. Psychos. Res. 2024, 181, 111707. [Google Scholar] [CrossRef]
- Kujawski, S.; Hodges, L.; Morten, K.; Zalewski, P. Fatigue: Exploring Chronic Fatigue: Neural Correlates, Mechanisms, and Therapeutic Strategies. Front. Neurosci. 2025, 19, 1751667. [Google Scholar] [CrossRef]
- Omdal, R. The biological basis of chronic fatigue: neuroinflammation and innate immunity. Curr. Opin. Neurol. 2020, 33(3), 391–396. [Google Scholar] [CrossRef]
- Peeples, L. Is your brain tired? Researchers are discovering the roots of mental fatigue. Nature 2025, 648(8093), 262–264. [Google Scholar] [CrossRef]
- Yang, X.; Li, F.; Liu, Y.; Li, D.; Li, J. Study on the correlation between NF-κB and central fatigue. J. Molecul. Neurosci. 2021, 71(10), 1975–1986. [Google Scholar] [CrossRef]
- Casella, C.; Ballaz, S. J. Genotoxic and neurotoxic potential of intracellular nanoplastics: A review. J. Appl. Toxicol. 2024, 44(11), 1657–1678. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, Y. S.; Tuan Anuar, S.; Azmi, A. A.; Wan Mohd Khalik, W. M. A.; Lehata, S.; Hamzah, S. R.; Lee, Y. Y. Detection of microplastics in human colectomy specimens. JGH Open 2021, 5(1), 116–121. [Google Scholar] [CrossRef] [PubMed]
- Samms, G. L.; Ponting, C. P. Defining a High-Quality Myalgic Encephalomyelitis/Chronic Fatigue Syndrome cohort in UK Biobank. NIHR Open Res. 2025, 5, 39. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Saini, V.; Varshney, N.; Pandey, R. K.; Jha, H.C. The infiltration of microplastics in human systems: gastrointestinal accumulation and pathogenic impact. Heliyon 2025, 11(4), e42606. [Google Scholar] [CrossRef]
- Wang, Y. F.; Wang, X. Y.; Chen, B. J.; Yang, Y. P.; Li, H.; Wang, F. Impact of microplastics on the human digestive system: From basic to clinical. World J. Gastroenterol. 2025, 31(4), 100470. [Google Scholar] [CrossRef]
- Chen, X.; Zhuang, J.; Chen, Q.; Xu, L.; Yue, X.; Qiao, D. Polyvinyl chloride microplastics induced gut barrier dysfunction, microbiota dysbiosis and metabolism disorder in adult mice. Ecotoxicol. Environ. Saf. 2022, 241, 113809. [Google Scholar] [CrossRef]
- Feng, C.; Zhang, Q.; Wang, L.; Li, S.; Wang, K.; Xu, Y.; Qiu, Y. Take-out containers as nano-and microplastics reservoirs: Diet-driven gut dysbiosis in university students. Environ. Pollut. 2025, 384, 126985–126985. [Google Scholar] [CrossRef]
- Li, J.; Li, W.; Xue, Y.; Zhu, H.; Zhang, D.; Ren, Y.; Huang, H. Oral Ingestion of Polystyrene Microplastics Aggravates Chronic Pancreatitis Through ROS Induced NF-κb/TGF-β Signaling Pathway and Alteration of Gut Microbiota. FASEB J. 2025, 39(22), e71223. [Google Scholar] [CrossRef]
- Mashayekhi-Sardoo, H.; Askarpour, H.; Arefinia, N.; Ali-Hassanzadeh, M. The clinical relevance of microplastic exposure on colorectal cancer: A systematic review. Cancer Epidemiol. 2025, 97, 102840. [Google Scholar] [CrossRef] [PubMed]
- Sofield, C. E.; Anderton, R. S.; Gorecki, A. M. Mind over microplastics: exploring microplastic-induced gut disruption and gut-brain-axis consequences. Curr. Issues Molecul. Biol. 2024, 46(5), 4186–4202. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Wu, F.; Liu, X.; Xie, W.; Liang, Y.; Ye, Y.; Liu, Z. Microplastic accumulation in fibrotic intestinal tissue and mesenteric adipose tissue in Crohn’s disease patients. Environ. Res. 2025, 271, 121077. [Google Scholar] [CrossRef] [PubMed]
- Casella, C.; Dondi, D.; Vadivel, D. Do microplastics (MPs) and nanoplastics (NPs) directly contribute to human carcinogenesis? Environ. Pollut. 2025, 127343. [Google Scholar] [CrossRef]
- Newey, C.; Skaar, J. R.; O'Hara, M.; Miao, B.; Post, A.; Kelly, T. Systematic literature review of the association of fever and elevated temperature with outcomes in critically ill adult patients. Ther. Hypothermia Temp. Manag. 2024, 14(1), 10–23. [Google Scholar] [CrossRef]
- Singh, B; Goyal, A; Patel, BC. C-Reactive Protein: Clinical Relevance and Interpretation. In StatPearls; StatPearls: Treasure Island (FL), 2025; Available online: https://www.ncbi.nlm.nih.gov/books/NBK441843/ (accessed on 03 November 2025).
- Cornelli, U.; Recchia, M.; Belcaro, G. COVID-19 Total Mortality and Relative Waves: the Reasons for the Differences among European Countries. Eur. J. Med. Health Sci. 2022, 4(1), 108–113. [Google Scholar] [CrossRef]
- Remigante, A.; Spinelli, S.; Gambardella, L.; Bozzuto, G.; Vona, R.; Caruso, D.; Straface, E. Internalization of nano-and micro-plastics in human erythrocytes leads to oxidative stress and estrogen receptor-mediated cellular responses. Free Rad. Biol. Med. 2024, 223, 1–17. [Google Scholar] [CrossRef]
- Yang, Z.; Wang, M.; Feng, Z.; Wang, Z.; Lv, M.; Chang, J.; Wang, C. Human microplastics exposure and potential health risks to target organs by different routes: A review. Curr. Pollut. Rep. 2023, 9(3), 468–485. [Google Scholar] [CrossRef]
- Radbakhsh, S.; Norouzzadeh, R. Microplastic Neurotoxicity: Pathways, Mechanisms, and Implications for Neurodegenerative Disease. Pers. Med. J. 2025, 10(37), 31–38. [Google Scholar] [CrossRef]
- Casella, C.; Cornelli, U.; Ballaz, S.; Recchia, M.; Zanoni, G.; Ramos-Guerrero, L. Preliminary Study on PCC-Chitosan’s Ability to Enhance Microplastic Excretion in Human Stools from Healthy Volunteers. Foods 2025, 14(13), 2190. [Google Scholar] [CrossRef]

Table 1.
Total number and disease classes considered for the existence of CCS signs and symptoms [6].
Table 1.
Total number and disease classes considered for the existence of CCS signs and symptoms [6].
| Class | Name | N. of Disease |
|---|---|---|
| 1 | Endocrine, metabolic, nutritional diseases | 33 |
| 2 | Infectious diseases | 23 |
| 3 | Nervous System diseases | 22 |
| 4 | Hematological, oncological diseases | 22 |
| 5 | Pediatric diseases | 20 |
| 6 | Gynecological, obstetric diseases | 20 |
| 7 | Cardiovascular diseases | 20 |
| 8 | Dermatological diseases | 19 |
| 9 | Major tumours | 19 |
| 10 | Genitourinary diseases | 18 |
| 11 | Gastrointestinal, liver, biliary tract diseases | 18 |
| 12 | Ophthalmological diseases | 16 |
| 13 | Poisoning | 16 |
| 14 | Ear, nose, throat (ENT) diseases | 15 |
| 15 | Psychiatric diseases | 15 |
| 16 | Special causes diseases | 14 |
| 17 | Immunology, allergic diseases | 14 |
| 18 | Dental, oral cavity diseases | 13 |
| 19 | Muscoskeletal and connective tissue diseases | 13 |
| 20 | Respiratory diseases | 13 |
| 21 | Physical agents diseases | 12 |
| TOTAL DISEASES | 375 | |
Table 2.
Frequency of symptoms and signs in the 40 diseases under consideration.
| Sign and Symptoms | Number of Times | % of Diseases Incidence |
|---|---|---|
| Persistent fatigue | 26 | 65.0 |
| Dyspeptic symptoms | 23 | 57.5 |
| CRP increase | 22 | 55.0 |
| Fever | 19 | 47.5 |
| Headache | 18 | 45.0 |
| Cognitive changes | 17 | 42.5 |
| Blood disorders | 16 | 40.0 |
| Ultrasound alteration | 15 | 37.5 |
| Abdominal pain | 15 | 37.5 |
| Dysbiosis | 13 | 32.5 |
| Sensorial alteration | 10 | 25.0 |
| Behavioral alteration | 8 | 20.0 |
| Cough/dyspnea | 7 | 17.5 |
| Liver enzyme alteration | 5 | 12.5 |
| Dyslipidemia | 5 | 12.5 |
| Creatinine alteration | 5 | 12.5 |
| Sexuality alteration | 5 | 12.5 |
| Visual alteration | 4 | 10.0 |
| Hypertension | 4 | 10.0 |
| Glucose alteration | 4 | 10.0 |
| Menstrual alteration | 3 | 7.5 |
| Blood in stools | 3 | 7.5 |
| Dermatitis | 2 | 5.0 |
| Pancreas enzymes alteration | 2 | 5.0 |
| Allergies | 1 | 2.5 |
| Vascular alteration | 1 | 2.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



