Submitted:
28 January 2026
Posted:
29 January 2026
You are already at the latest version
Abstract
Background/Objectives: Direct‑acting antivirals (DAAs) cure hepatitis C virus (HCV) infection and may improve health‑related quality of life (HRQoL), but responsiveness differs across instruments. We quantified longitudinal changes using EQ‑5D‑5L, SF‑8 and CLDQ in a multicenter Japanese cohort. Methods: Adults with chronic HCV completed patient‑reported outcomes (PROs) at baseline and 12/24/36 weeks (48 weeks where available). Complete‑case panels were defined per instrument (SF‑8 n=112, CLDQ n=131, EQ‑5D‑5L n=128). Domain trajectories were summarized and compared with baseline. Results: SF‑8 improved by 36 weeks: General Health 50.42→52.47, Vitality 50.73→52.55, Mental Health 51.02→53.05. CLDQ improved in Worry 5.21→5.82 and Total 5.21→5.47. EQ‑5D‑5L utilities remained high and stable (0.913→0.920), consistent with ceiling effects at high baseline health. External real‑world data indicated better on‑treatment HRQoL with ribavirin‑free regimens. Conclusions: Interferon‑free DAAs yield early, clinically meaningful HRQoL gains in symptom‑proximal and mental domains, while generic utilities show minimal short‑term change. Combining disease‑specific PROs with utilities is essential for patient‑centered care and for parameterizing cost‑utility models in Japan.
Keywords:
hepatitis C
; direct‑acting antivirals
; patient‑reported outcomes
; EQ‑5D‑5L
; SF‑8
; CLDQ
; utilities
; quality of life
; ribavirin
; Japan
1. Introduction
Chronic viral hepatitis, particularly infection with the hepatitis C virus (HCV), impairs health-related quality of life (HRQoL) across physical, psychological, and social domains well before end-stage complications occur [1,2]. In Japan, our prior population-based study documented stepwise health-state utilities—0.821 (chronic hepatitis), 0.737 (compensated cirrhosis), and 0.671 (decompensated cirrhosis)—providing an essential benchmark for cost-utility analyses [3]. Against this background, HRQoL has become a core outcome for patient-centered hepatology and health-policy evaluation.
The advent of interferon-free direct-acting antivirals (DAAs) has transformed HCV care, delivering high sustained virologic response (SVR) rates with markedly improved tolerability compared with interferon-based regimens [2,4,5,6]. Clinical trials and meta-analyses increasingly show improvements in patient-reported outcomes (PROs) during and after DAA therapy [5,6,7]. Yet generic preference-based measures (e.g., EQ-5D-5L) sometimes exhibit limited short-term change in patients with relatively good baseline health, raising questions about instrument responsiveness and potential ceiling effects during the on-treatment phase [6,8,9].
These considerations underscore two needs. First, longitudinal data that track multiple instruments—a generic utility measure and both generic and liver-specific HRQoL scales—are required to map how symptom-proximal domains (e.g., fatigue, worry) and global health perceptions evolve during and after therapy [5,6,10,11]. Second, evidence is needed on regimen-level differences in on-treatment HRQoL burden (e.g., ledipasvir/sofosbuvir [LDV/SOF] versus sofosbuvir/ribavirin [SOF/RBV]), as such differences may influence real-world treatment experience and have implications for value assessment [5,10].
We therefore conducted a multicenter longitudinal study of adults with chronic HCV treated with interferon-free DAAs in Japan. HRQoL was assessed repeatedly using EQ-5D-5L (utilities), the Short Form-8 (SF-8), and the Chronic Liver Disease Questionnaire (CLDQ) from baseline through 12, 24, 36 (and where available 48) weeks. We hypothesized that: (i) DAA therapy would yield clinically meaningful improvements in symptom-proximal CLDQ domains and selected SF-8 domains during the treatment course; (ii) EQ-5D-5L utilities would show smaller short-term changes consistent with ceiling effects but improve with sustained wellness post-SVR; and (iii) LDV/SOF would be associated with a lower on-treatment HRQoL burden than SOF/RBV. By integrating these longitudinal outcomes with Japanese utility benchmarks, this study also informs cost-utility evaluations of HCV treatment [3].
2. Materials and Methods
We conducted a multicenter longitudinal observational study of adults with chronic HCV who initiated interferon-free DAA therapy in routine practice in Japan. Patient-reported outcomes (PROs) were collected at baseline and at 12/24/36 weeks (48 weeks where available). Reporting followed STROBE guidance [12].
Adults (≥18 years) with chronic HCV able to complete questionnaires were eligible. Regimens were prescribed per routine care. Disease categories (chronic hepatitis, cirrhosis, hepatocellular carcinoma under control) were abstracted from clinical records.
EQ-5D-5L utilities were calculated using the Japanese value set [8] and contextualized using Japanese population norms [9]. SF-8 (Japanese version) has established psychometrics [13]. CLDQ is a six-domain liver-specific questionnaire commonly used in hepatology [11]; its use in Japanese real-world HCV cohorts has been reported [10].
PROs were administered at baseline (pre-treatment), 12, 24, and 36 weeks (48 weeks where available) during routine visits or via mail/telephone.
The primary outcome was within-patient change from baseline in instrument scores. Complete-case panels for 1→4 timepoints were defined per instrument (SF-8, CLDQ, EQ-5D-5L).
We used repeated-measures ANOVA with Mauchly’s test of sphericity [14]; if violated, we applied Greenhouse–Geisser correction [15]. Post-hoc Tukey–Kramer pairwise comparisons accommodated unequal cell sizes [16]. Two-sided α=0.05. Missing data were handled by complete-case analysis, no imputation.
The study used anonymous, non-linkable identifiers and obtained approvals from participating institutional review boards (e.g., Daito Bunka University K-14-010; Kagawa University Heisei 26-141); written informed consent was obtained from all participants.
3. Results
3.1. Patient Characteristics and Baseline HRQoL
- At baseline, 344 patients provided HRQoL data; complete-case panels comprised approximately n=112 (SF-8), n=131 (CLDQ), and n=128 (EQ-5D-5L).
These starting levels frame the headroom for change detected by PRO instruments during and after DAA therapy.
3.2. Longitudinal Changes in PROs (SF-8, CLDQ, EQ-5D-5L)
- SF-8 domains—General Health, Vitality, and Mental Health—improved significantly by 36 weeks.
- CLDQ showed consistent gains, especially in Worry and in the Total score.
- These patterns align with meta-analytic evidence that DAA-related PROs improve during and after therapy [5].
- Japanese real-world CLDQ data report similar improvements during treatment, supporting external validity [10].
Taken together, the PRO trajectory shows early symptom-proximal gains (SF-8/CLDQ) alongside limited short-term utility movement (EQ-5D-5L), a pattern consistent with instrument responsiveness and ceiling effects in cohorts with high baseline health.

Table 1.
Baseline characteristics.
| Characteristic | Value |
|---|---|
| Total N | 344 |
| Male, n (%) | 145 (42.2) |
| Female, n (%) | 199 (57.8) |
| Hepatocellular carcinoma, n (%) | 24 (7.0) |
| Cirrhosis, n (%) | 29 (8.4) |
| Chronic hepatitis, n (%) | 291 (84.6) |
Table 2.
Baseline HRQoL.
| Instrument / Domain | N | Mean ± SD |
|---|---|---|
| EQ-5D-5L Utility | 128 | 0.913 ± 0.140 |
| SF-8 GH | 112 | 50.42 ± 6.14 |
| SF-8 VT | 112 | 50.73 ± 5.85 |
| SF-8 MH | 112 | 51.02 ± 5.71 |
| CLDQ Fatigue | 131 | 5.205 ± 1.167 |
| CLDQ Emotional function | 131 | 5.361 ± 1.181 |
| CLDQ Worry | 131 | 5.212 ± 1.233 |
| CLDQ Abdominal symptoms | 131 | 5.837 ± 1.087 |
| CLDQ Total | 131 | 5.214 ± 0.913 |
Table 3.
Longitudinal changes in HRQoL and utilities.
| Instrument / Domain | Time | Mean ± SD | p vs baseline |
|---|---|---|---|
| EQ-5D-5L Utility | Baseline | 0.913 ± 0.140 | - |
| EQ-5D-5L Utility | 12w | 0.914 ± 0.133 | 0.8743 |
| EQ-5D-5L Utility | 24w | 0.910 ± 0.141 | 0.783 |
| EQ-5D-5L Utility | 36w | 0.920 ± 0.137 | 0.5193 |
| SF-8 GH | Baseline | 50.42 ± 6.14 | - |
| SF-8 GH | 12w | 51.28 ± 7.02 | 0.2122 |
| SF-8 GH | 24w | 51.89 ± 7.18 | 0.0472 |
| SF-8 GH | 36w | 52.47 ± 6.18 | 0.0014 |
| SF-8 VT | Baseline | 50.73 ± 5.85 | - |
| SF-8 VT | 12w | 51.51 ± 6.70 | 0.5085 |
| SF-8 VT | 24w | 51.69 ± 7.05 | 0.6265 |
| SF-8 VT | 36w | 52.55 ± 5.93 | 0.2967 |
| SF-8 MH | Baseline | 51.02 ± 5.71 | - |
| SF-8 MH | 12w | 52.17 ± 6.33 | 0.5085 |
| SF-8 MH | 24w | 52.28 ± 6.57 | 0.6265 |
| SF-8 MH | 36w | 53.05 ± 5.70 | 0.2967 |
| CLDQ Fatigue | Baseline | 5.205 ± 1.167 | - |
| CLDQ Fatigue | 12w | 5.403 ± 1.120 | 0.0139 |
| CLDQ Fatigue | 24w | 5.409 ± 1.081 | 0.0135 |
| CLDQ Fatigue | 36w | 5.412 ± 1.048 | 0.0193 |
| CLDQ Emotional function | Baseline | 5.361 ± 1.181 | - |
| CLDQ Emotional function | 12w | 5.586 ± 1.191 | 0.0067 |
| CLDQ Emotional function | 24w | 5.489 ± 1.199 | 0.1204 |
| CLDQ Emotional function | 36w | 5.663 ± 1.077 | 0.0018 |
| CLDQ Worry | Baseline | 5.212 ± 1.233 | - |
| CLDQ Worry | 12w | 5.744 ± 1.113 | <.0001 |
| CLDQ Worry | 24w | 5.820 ± 1.094 | <.0001 |
| CLDQ Worry | 36w | 5.817 ± 1.147 | <.0001 |
| CLDQ Abdominal symptoms | Baseline | 5.837 ± 1.087 | - |
| CLDQ Abdominal symptoms | 12w | 5.804 ± 1.048 | 0.7089 |
| CLDQ Abdominal symptoms | 24w | 5.847 ± 1.053 | 0.9038 |
| CLDQ Abdominal symptoms | 36w | 5.812 ± 1.155 | 0.8046 |
| CLDQ Total | Baseline | 5.214 ± 0.913 | - |
| CLDQ Total | 12w | 5.416 ± 0.884 | 0.0021 |
| CLDQ Total | 24w | 5.419 ± 0.855 | 0.0016 |
| CLDQ Total | 36w | 5.473 ± 0.854 | 0.0006 |
Figure 1.
SF-8 domain trajectories (General Health, Vitality, Mental Health).
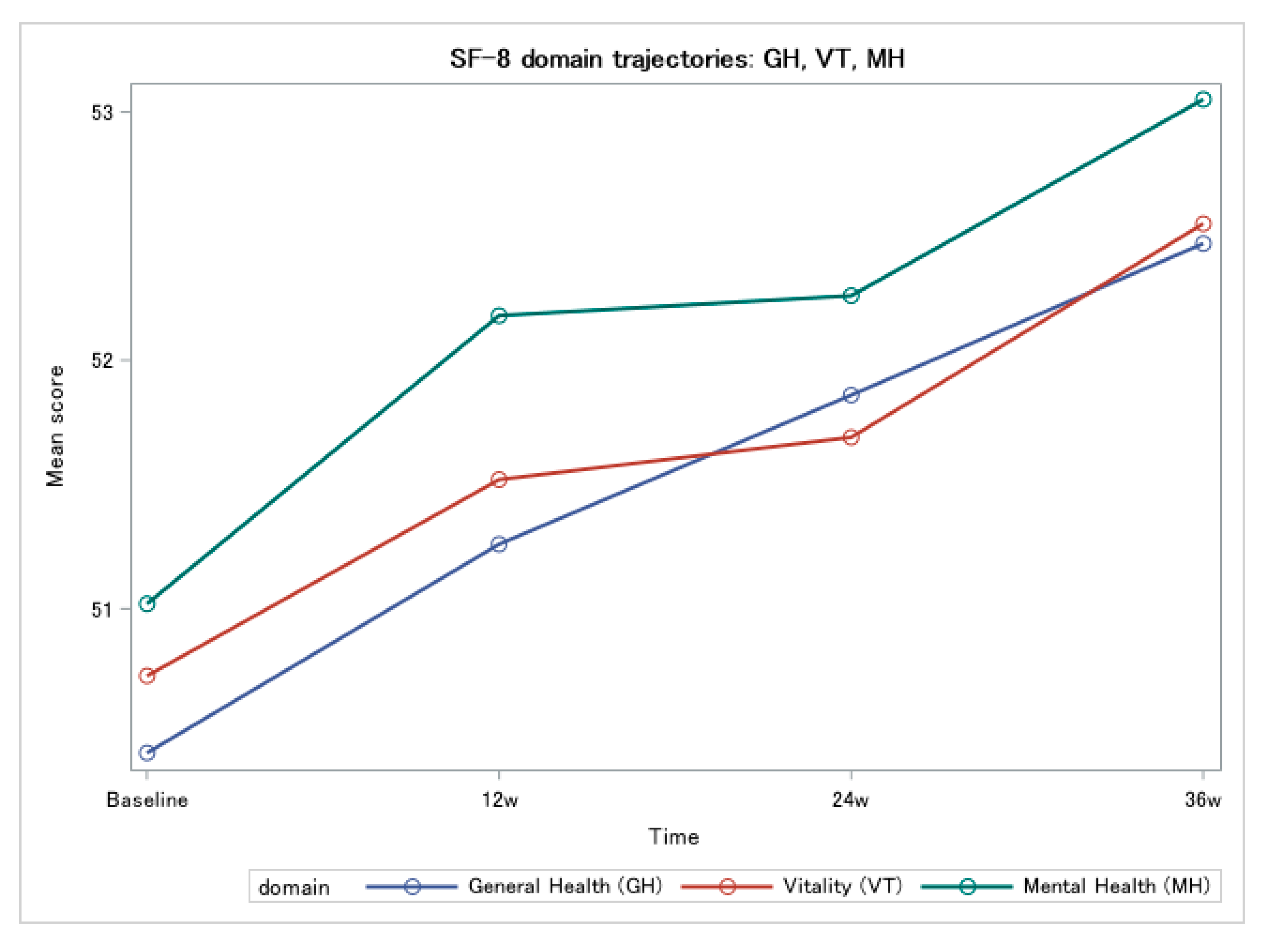
Figure 2.
CLDQ trajectories (Worry and Total score).
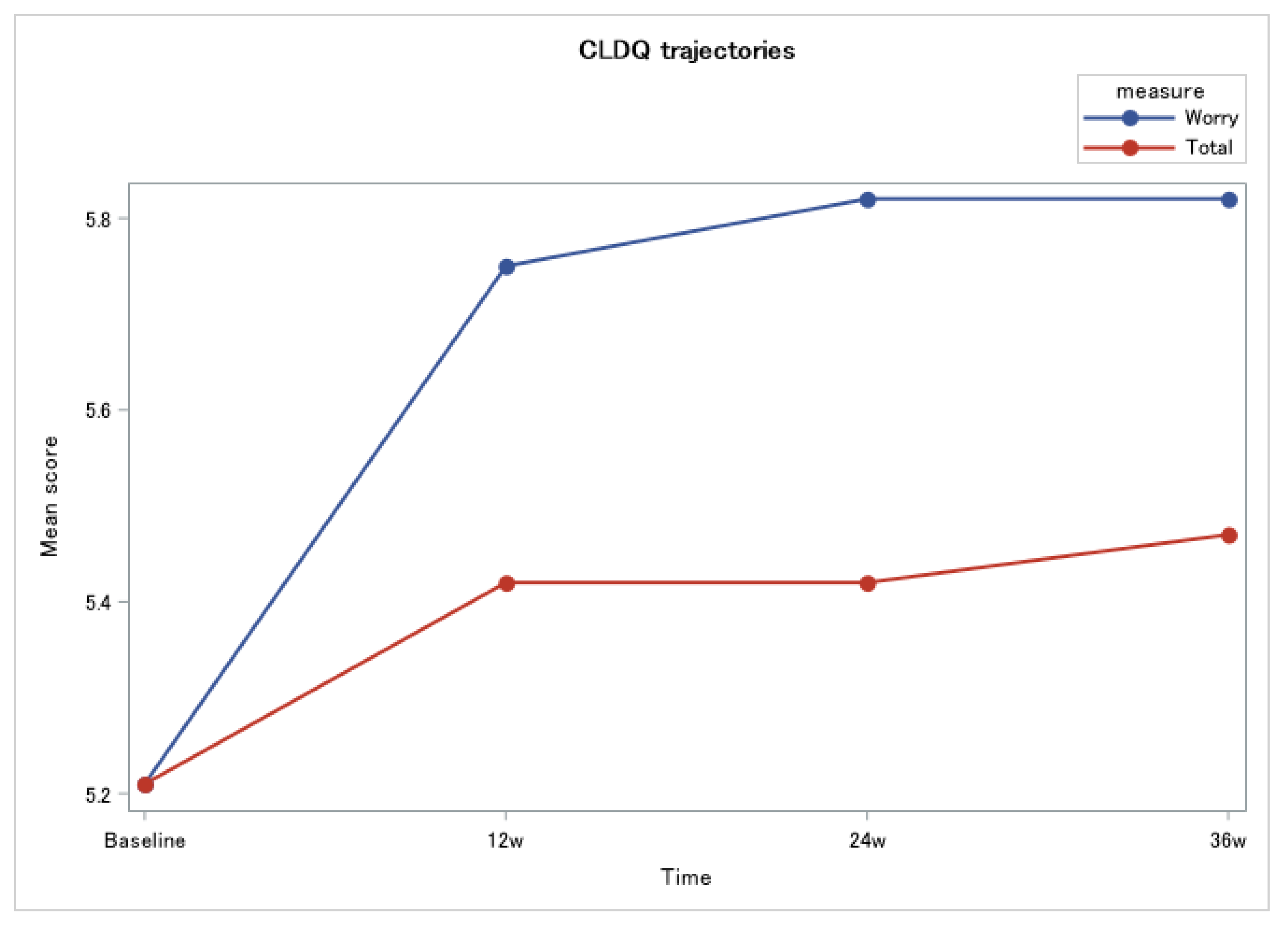
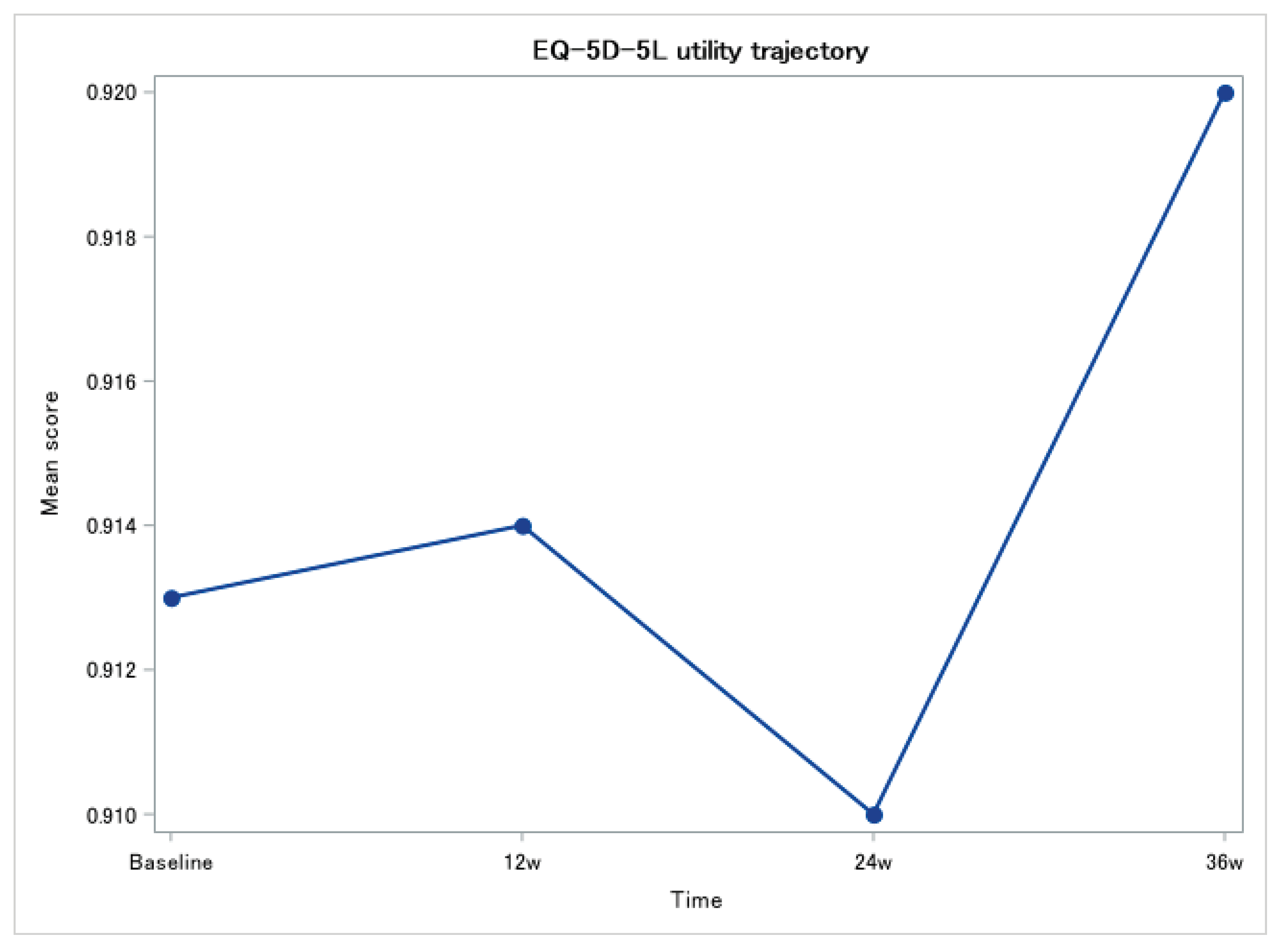
Figure 3.
EQ-5D-5L utility trajectory.
4. Discussion
In this multicenter, real-world Japanese cohort, we observed clinically meaningful improvements in PROs during and after interferon-free DAA therapy. SF-8 domains of General Health, Vitality, and Mental Health increased significantly by 36 weeks, and CLDQ showed consistent gains—most prominently in Worry and in the Total score—whereas EQ-5D-5L utilities remained high and stable over the same interval. These patterns indicate that symptom-proximal and perception-related domains are especially responsive during the on-treatment phase, while generic utilities may show limited short-term change in patients with good baseline health [5,6,8,9,11].
Our findings are concordant with meta-analytic and trial data showing PRO improvements during and after DAA therapy, with ribavirin-free regimens achieving greater physical-health gains [5,7]. In a meta-analysis of 1,619 patients, most SF-36 domains improved by 12–24 weeks post-treatment, with larger benefits in bodily pain for ribavirin-free regimens [5]. Japanese experiences—including longitudinal SF-8 trajectories through SVR24 to 1 year and long-term improvements in symptoms and muscle mass—provide additional support [4,6].
The limited short-term movement in EQ-5D-5L relative to SF-8/CLDQ aligns with differences in construct focus and responsiveness. Given Japanese value-set scaling and high normative utilities, modest health gains may not translate into detectable utility changes over months [8,9]. Consistent with this, a Japanese sofosbuvir-based cohort reported high baseline SF-8 with only minimal short-term changes, while overall status remained good after SVR [6]. Using disease-specific PROs alongside utilities is therefore crucial to capture patient-centered benefits [11].
Although the present dataset focused on overall trajectories, real-world Japanese data using CLDQ showed better on-treatment HRQoL with LDV/SOF than with SMV/Peg-IFN/RBV—supporting regimen choices that minimize on-treatment burden [10]. Meta-analytic subgroup results likewise favor ribavirin-free regimens for physical-health domains [5].
Beyond the 24–36-week horizon of our panel, DAA-related PRO gains often persist and can coincide with improvements in disease-related symptoms and even skeletal muscle mass, suggesting a physiological substrate for sustained well-being after viral clearance [4]. Complementary cohorts in diverse settings also report significant HRQoL improvements months after treatment end, supporting the generalizability of these benefits across populations [7]. The overall direction is consistent with meta-analytic findings of post-treatment gains [5].
For clinicians, early improvements—especially in Worry—highlight the value of addressing uncertainty, stigma, sleep and fatigue during therapy; targeted supportive care may amplify PRO gains [4,5,6,10,11]. For health technology assessment, integrating our longitudinal PROs with Japanese utility benchmarks facilitates credible QALY modelling as DAA costs fall and SVR remains high [3,7,8,9].
Another aspect is work productivity and social contributions. Improved HRQoL likely translates to better work performance and less absenteeism for employed patients, and greater engagement in daily activities for all. In economic terms, these reflect reductions in absenteeism/presenteeism and indirect costs under a societal perspective. Trial and modelling work using the Work Productivity and Activity Impairment (WPAI) instrument has shown that DAA therapy improves work productivity and that these gains can offset costs [17,18,19]. For working-age patients, the reduction in fatigue and improved well-being may increase hours worked and effectiveness, which can translate into lower indirect costs and improved cost-effectiveness when broader perspectives are considered [17,18,19]. These broader societal benefits, while beyond our study’s measurement, are part of the real-world impact of improved HRQoL and warrant scenario/sensitivity analyses that incorporate productivity (e.g., WPAI-based estimates) alongside utilities [17,18,19].
Preference-based utility is the currency that converts patient-centered benefits into QALYs. In Japan, our prior population-based benchmarks showed stepwise utilities of 0.821 (chronic hepatitis), 0.737 (compensated cirrhosis), and 0.671 (decompensated cirrhosis), which provide clinical anchors for plausible long-term gains post-SVR [3]. Anchoring utilities to the Japanese EQ-5D-5L value set and population norms [8,9], even modest post-SVR utility increments (e.g., +0.03 to +0.05) sustained over 10 years would yield ≈0.3–0.5 QALYs per patient, before accounting for avoided complications. Coupled with our observed improvements in symptom-proximal PROs (CLDQ and SF-8) [5,10], this supports a favorable cost-utility profile of interferon-free DAAs in Japan, particularly as access broadens and regimen selection minimizes on-treatment burden. Because short-term EQ-5D-5L may under-detect early benefits due to ceiling effects [6,8,9], modelling should (i) explore scenario and sensitivity analyses bounded by Japanese utility benchmarks [1,8,9]; (ii) consider mapping approaches that translate disease-specific changes (fatigue, pain, worry) into utilities; and (iii) use subgroup-specific trajectories (age, baseline utility) to avoid over- or under-estimation of incremental cost-effectiveness.
Evidence in people who inject drugs (PWID) and those on opioid agonist therapy (OAT) indicates that DAAs can deliver meaningful PRO gains when cure is achieved. In US OAT clinics, EQ-5D-3L increased from 0.66 to 0.77 with marked reductions in pain and anxiety by 12–24 weeks post-SVR [20]. In a randomized trial among OAT recipients, elbasvir/grazoprevir led to greater improvements in SF-36v2 general health, vitality, and mental health at 4 weeks post-treatment versus placebo [21]. Pooled analyses of sofosbuvir-based phase 3 data further show that IFN/RBV-free regimens produce on-treatment PRO improvements, often more pronounced in opioid substitution therapy recipients [22]. Some PWID cohorts show minimal short-term utility change despite improved employment, underscoring the need for multifaceted models of care beyond antiviral therapy [23].
Strengths include a multicenter design; repeated measures across complementary, validated instruments (EQ-5D-5L, SF-8, CLDQ); and pre-specified complete-case longitudinal panels. Limitations include potential selection bias inherent to complete-case analysis, limited regimen-stratified detail (precluding full comparative effectiveness within this dataset), and a short-term utility horizon relative to the longer timeframe over which economic benefits accrue; moreover, psychosocial factors (e.g., depression/anxiety, stigma) were not formally measured and may modulate the magnitude of HRQoL gains [5,6,8,9,10,12].
Priorities include longer-term utilities post-SVR to better parameterize QALY gains, explicit assessment of psychosocial mediators (depression/anxiety, stigma, sleep/fatigue), and head-to-head comparisons of pangenotypic ribavirin-free regimens with PROs as co-primary outcomes [5,6,16]. Given the burden in PWID, pragmatic designs embedded in OAT/low-threshold settings would strengthen external validity [20,21,22].
5. Conclusions
Interferon-free DAA therapy for HCV yields early, clinically meaningful improvements in patient-centered outcomes captured by SF-8 and CLDQ, while EQ-5D-5L utilities show minimal short-term change—a pattern consistent with instrument responsiveness and ceiling effects in populations with high baseline health. Integrating disease-specific PROs with utilities and anchoring to Japanese benchmarks provides a practical pathway to robust cost-utility evaluation.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: SF-8 domain scores by week (mean ± SD; complete-case panel, n=112 at all-time points); Table S2: CLDQ domain scores by week (mean ± SD; p values vs baseline); Table S3: EQ-5D-5L utility by week (mean ± SD; p values vs baseline); Figure S1: SF-8 domain trajectories over time (0, 12, 24, 36 weeks); Supplementary Methods: scoring, assessment schedule, and statistical procedures.
Author Contributions
Conceptualization, H.S. and M.H.; methodology, A.I. and S.I.; formal analysis, M.H. and T.H.; investigation, H.Y., H.Y. and N.M.; data curation, N.I. and T.O.; writing—original draft preparation, M.H. and T.H.; writing—review and editing, all authors; visualization, M.H. and T.H.; supervision, H.S., T.S., T.T., T.Y. M.A. and M.S.; project administration, H.S.; funding acquisition, S.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Health and Labor Sciences Research Grants for Research on Hepatitis, grant number 201619003A and 201619003B (Hirao group).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Daito Bunka University (protocol code K-14-010) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
De-identified data are available from the corresponding author upon reasonable request and subject to institutional approvals.
Acknowledgments
We thank all participating patients and clinical staff at the collaborating centers for their valuable contributions.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| DAA | direct-acting antiviral |
| SVR | sustained virologic response |
| HRQoL | health-related quality of life |
| PRO | patient-reported outcome |
| EQ-5D-5L | EuroQol five-dimension five-level |
| SF-8 | Short Form-8 |
| CLDQ | Chronic Liver Disease Questionnaire |
| PCS | Physical Component Summary (SF-8) |
| MCS | Mental Component Summary (SF-8) |
| QALY | quality-adjusted life-year |
| ICER | incremental cost-effectiveness ratio |
| RBV | ribavirin |
| IFN | interferon |
| LDV/SOF | ledipasvir/sofosbuvir |
| SOF/RBV | sofosbuvir/ribavirin |
| SMV | simeprevir |
| Peg-IFN | pegylated interferon |
| WPAI | Work Productivity and Activity Impairment |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
References
- Spiegel, B.M.; Younossi, Z.M.; Hays, R.D.; Revicki, D.; Robbins, S.; Kanwal, F. Impact of hepatitis C on health related quality of life: a systematic review and quantitative assessment. Hepatology 2005, 41, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Dusheiko, G. The impact of antiviral therapy for hepatitis C on the quality of life: a perspective. Liver International 2017, 37, 7–12. [Google Scholar] [CrossRef]
- Sugimori, H.; Hirao, M.; Igarashi, A.; Yatsuhashi, H.; Ikeda, S.; Masaki, N.; Yotsuyanagi, H.; Yoda, T.; Odajima, T.; Takura, T.; et al. Health state utilities of patients with hepatitis B and C and hepatitis-related conditions in Japan. Sci Rep 2022, 12, 17139. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, T.; Miyaaki, H.; Miuma, S.; Motoyoshi, Y.; Yamashima, M.; Yamamichi, S.; Koike, M.; Nakano, Y.; Honda, T.; Yajima, H.; et al. Direct-acting Antivirals Improved the Quality of Life, Ameliorated Disease-related Symptoms, and Augmented Muscle Volume Three Years Later in Patients with Hepatitis C Virus. Intern Med 2020, 59, 2653–2660. [Google Scholar] [CrossRef]
- He, N.; Feng, G.; Hao, S.; Xu, M.; Liu, J.; Kong, F.; Ren, Z.; Dou, W.; Yao, C.; Liang, T.; et al. The impact of direct-acting antivirals on quality of life in patients with hepatitis C virus infection: a meta-analysis. Annals of Hepatology 2022, 27, 100705. [Google Scholar] [CrossRef]
- Miyasaka, A.; Yoshida, Y.; Suzuki, A.; Takikawa, Y. Health-related quality of life in patients with chronic hepatitis C treated with sofosbuvir-based treatment at 1-year post-sustained virological response. Qual Life Res 2021, 30, 3501–3509. [Google Scholar] [CrossRef] [PubMed]
- Marcellin, F.; Mourad, A.; Lemoine, M.; Kouanfack, C.; Seydi, M.; Carrieri, P.; Attia, A.; Protopopescu, C.; Lacombe, K.; Boyer, S. Patient-reported outcomes with direct-acting antiviral treatment for hepatitis C in West and Central Africa (TAC ANRS 12311 trial). JHEP Reports 2023, 5. [Google Scholar] [CrossRef]
- Shiroiwa, T.; Ikeda, S.; Noto, S.; Igarashi, A.; Fukuda, T.; Saito, S.; Shimozuma, K. Comparison of Value Set Based on DCE and/or TTO Data: Scoring for EQ-5D-5L Health States in Japan. Value Health 2016, 19, 648–654. [Google Scholar] [CrossRef]
- Shiroiwa, T.; Noto, S.; Fukuda, T. Japanese Population Norms of EQ-5D-5L and Health Utilities Index Mark 3: Disutility Catalog by Disease and Symptom in Community Settings. Value in Health 2021, 24, 1193–1202. [Google Scholar] [CrossRef]
- Aimono, Y.; Kohyama, N.; Kamoshida, T.; Yamamoto, T.; Kogo, M. [QOL Assessment in Chronic Hepatitis C Patients Receiving Ledipasvir/ Sofosbuvir or Simeprevir/Peginterferon/Ribavirin in Clinical Practice]. Yakugaku Zasshi 2019, 139, 1427–1434. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Guyatt, G.; Kiwi, M.; Boparai, N.; King, D. Development of a disease specific questionnaire to measure health related quality of life in patients with chronic liver disease. Gut 1999, 45, 295–300. [Google Scholar] [CrossRef]
- Elm, E.v.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef]
- Tokuda, Y.; Okubo, T.; Ohde, S.; Jacobs, J.; Takahashi, O.; Omata, F.; Yanai, H.; Hinohara, S.; Fukui, T. Assessing Items on the SF-8 Japanese Version for Health-Related Quality of Life: A Psychometric Analysis Based on the Nominal Categories Model of Item Response Theory. Value in Health 2009, 12, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Mauchly, J.W. Significance Test for Sphericity of a Normal n-Variate Distribution. The Annals of Mathematical Statistics 1940, 11, 204–209. [Google Scholar] [CrossRef]
- Greenhouse, S.W.; Geisser, S. On methods in the analysis of profile data. Psychometrika 1959, 24, 95–112. [Google Scholar] [CrossRef]
- Kramer, C.Y. Extension of Multiple Range Tests to Group Means with Unequal Numbers of Replications. Biometrics 1956, 12, 307–310. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Stepanova, M.; Afdhal, N.; Kowdley, K.V.; Zeuzem, S.; Henry, L.; Hunt, S.L.; Marcellin, P. Improvement of health-related quality of life and work productivity in chronic hepatitis C patients with early and advanced fibrosis treated with ledipasvir and sofosbuvir. J Hepatol 2015, 63, 337–345. [Google Scholar] [CrossRef]
- Younossi, Z.; Brown, A.; Buti, M.; Fagiuoli, S.; Mauss, S.; Rosenberg, W.; Serfaty, L.; Srivastava, A.; Smith, N.; Stepanova, M.; et al. Impact of eradicating hepatitis C virus on the work productivity of chronic hepatitis C (CH-C) patients: an economic model from five European countries. J Viral Hepat 2016, 23, 217–226. [Google Scholar] [CrossRef]
- Sulkowski, M.; Ionescu-Ittu, R.; Macaulay, D.; Sanchez-Gonzalez, Y. The Economic Value of Improved Productivity from Treatment of Chronic Hepatitis C Virus Infection: A Retrospective Analysis of Earnings, Work Loss, and Health Insurance Data. Advances in Therapy 2020, 37, 4709–4719. [Google Scholar] [CrossRef]
- Gormley, M.A.; Akiyama, M.J.; Rennert, L.; Howard, K.A.; Norton, B.L.; Pericot-Valverde, I.; Muench, S.; Heo, M.; Litwin, A.H. Changes in Health-related Quality of Life for Hepatitis C Virus-Infected People Who Inject Drugs While on Opioid Agonist Treatment Following Sustained Virologic Response. Clin Infect Dis 2022, 74, 1586–1593. [Google Scholar] [CrossRef]
- Dalgard, O.; Litwin, A.H.; Shibolet, O.; Grebely, J.; Nahass, R.; Altice, F.L.; Conway, B.; Gane, E.J.; Luetkemeyer, A.F.; Peng, C.Y.; et al. Health-related quality of life in people receiving opioid agonist treatment and treatment for hepatitis C virus infection. J Addict Dis 2023, 41, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Stepanova, M.; Thompson, A.; Doyle, J.; Younossi, I.; de Avila, L.; Younossi, Z.M. Hepatitis C Virus–Infected Patients Receiving Opioid Substitution Therapy Experience Improvement in Patient-Reported Outcomes Following Treatment With Interferon-Free Regimens. The Journal of Infectious Diseases 2017, 217, 1033–1043. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Q.; Cunningham, E.B.; Shih, S.; Amin, J.; Bruneau, J.; Artenie, A.A.; Powis, J.; Litwin, A.H.; Cooper, C.; Dalgard, O.; et al. Patient-Reported Outcomes During and After Hepatitis C Virus Direct-Acting Antiviral Treatment Among People Who Inject Drugs. Value Health 2023, 26, 883–892. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



