
Submitted:
28 January 2026
Posted:
28 January 2026
You are already at the latest version
Abstract
Background and Objectives: Paraneoplastic hypercalcemia represents a rare but clinically significant complication of penile squamous cell carcinoma (PSCC), with limited evidence available. This systematic review aimed to comprehensively evaluate the pathophysiological mechanisms, clinical presentation, therapeutic strategies and prognostic outcomes of tumor-induced hypercalcemia in PSCC. Methods: A comprehensive literature search was conducted across PubMed/MEDLINE and Scopus databases from inception to December 2024. Cases were included if they documented histopathologically confirmed PSCC with biochemically verified hypercalcemia and objective evidence of paraneoplastic etiology. Data extraction encompassed tumor characteristics, hypercalcemia severity, mechanistic classification, therapeutic interventions and survival outcomes. Analysis followed PRISMA 2020 guidelines adapted for descriptive synthesis. Results: Twelve published cases spanning six decades (1965-2024) met inclusion criteria. The median age at presentation was 56 years, with 91.6% of patients presenting with advanced disease. Severe hypercalcemia (≥14 mg/dL) occurred in 66.7% of cases, with a median calcium level of 15.45 mg/dL. Three distinct pathophysiological mechanisms were identified: PTHrP-mediated humoral hypercalcemia, bone metastasis-associated hypercalcemia and tumor burden-mediated hypercalcemia. Despite biochemical correction, median overall survival was 9 weeks following hypercalcemia diagnosis. Conclusions: Paraneoplastic hypercalcemia in PSCC represents a rare metabolic emergency. While aggressive management can achieve biochemical correction, the occurrence of hypercalcemia uniformly indicates advanced tumor biology with limited survival benefit. Early recognition and prompt multidisciplinary intervention remain essential for symptomatic relief and quality of life preservation. Future prospective studies are needed to better characterize optimal management strategies and refine prognostic models.
Keywords:
penile cancer
; squamous cell carcinoma
; paraneoplastic syndrome
; hypercalcemia
; PTHrP
; bisphosphonates
1. Introduction
Penile cancer (PC) represents a rare malignancy, with incidence rates ranging from 0.86 to 1.3 per 100,000 population in Central and Eastern European countries and an estimated mortality rate of 0.4 per 100,000. The disease disproportionately affects populations with low socio-economic status, reflected in limited access to preventive health measures and high prevalence of human papillomavirus (HPV) infection (particularly types 16 and 18). Despite known associations with risk factors such as phimosis, chronic inflammatory conditions (lichen sclerosus - LS) or tobacco use, the molecular pathogenesis remains incompletely characterized and late-stage presentation continues to dominate in resource-limited settings [1].
Although localized penile squamous cell carcinoma (PSCC) is feasible to surgical treatment and demonstrates favourable response, disease progression to advanced stages is associated with significantly poor clinical outcomes. Paraneoplastic syndromes are uncommonly encountered and reported in PSCC.
Tumor-induced hypercalcemia is predominantly observed in squamous cell carcinomas of pulmonary, head and neck, and esophageal origin, with pathogenesis primarily attributed to humoral factors, notably parathyroid hormone-related peptide (PTHrP) [2,3]. This condition has been documented in association with a range of genitourinary tumors. Among these, prostate cancer and renal cell carcinoma (RCC) are frequently noted [4,5]. The syndrome may manifest even in localized RCC, occasionally representing the presenting feature prompting diagnostic evaluation [5]. When hypercalcemia occurs in advanced prostate cancer, it typically indicates osteolytic lesions or ectopic PTHrP production, both markers of particularly aggressive disease biology [4]. By comparison, the occurrence of hypercalcemia in PSCC is exceptionally rare [6,7], with documentation limited to sporadic case reports. The paucity of literature reflects both the rarity of PC itself and the infrequency of this paraneoplastic manifestation. Nevertheless, when hypercalcemia develops in the setting of PSCC, it universally indicates advanced disease and portends poor prognosis. Consequently, the clinical and pathophysiological mechanisms, therapeutic responses and prognostic implications of this entity require comprehensive characterization.
Hypercalcemia represents a significant paraneoplastic complication, accounting for more than 20% of cancer-associated morbidity, with mortality rates reaching 50% within 30 days of diagnosis. Malignancy-associated acute severe hypercalcemia represents an oncologic emergency requiring prompt recognition and interdisciplinary management [8]. Without timely recognition and intervention, this complication is associated with substantial morbidity and mortality [9,10,11,12].
The aim of this study was to perform a systematic review on the available evidence regarding tumor-induced hypercalcemia in PSCC, in order to synthesize existing evidence on clinical presentation, pathophysiological mechanisms, therapeutic strategies and outcomes. This could provide a structured framework to guide future clinical research.
2. Materials and Methods
A systematic literature search was conducted across PubMed/MEDLINE and Scopus databases from database inception to December 2024, employing the following search terms: “penile cancer”,” “squamous cell carcinoma,” “hypercalcemia,” and “paraneoplastic syndrome”, without filters for language. Supplementary manual searching of bibliographies from all included articles was performed to identify additional relevant studies (backward citation searching). The flow chart highlighting the selection process of eligible studies is presented in Figure 1.
Inclusion criteria: histopathologically confirmed PSCC; biochemically documented hypercalcemia (serum calcium >10.5 mg/dL or ionized calcium >1.3 mmol/L); objective evidence of paraneoplastic etiology (elevated PTHrP, bone metastases or exclusion of alternative causes); published case reports, case series, or cohort studies and no language restrictions.
Exclusion criteria: primary hyperparathyroidism or other non-malignant causes of hypercalcemia; insufficient clinical data to confirm diagnosis; duplicate or irrelevant publications.
Data Extraction
Data extraction was performed independently by two reviewers using a standardized extraction form. Extracted variables encompassed: (1) patient demographics; (2) tumor-specific variables (histological grade, clinical stage, presence and anatomical distribution of metastases); (3) biochemical parameters (serum calcium concentrations, corrected calcium values, PTHrP levels, serum PTH, alkaline phosphatase); (4) established etiology of hypercalcemia; (5) therapeutic strategies employed and (6) clinical outcomes (biochemical response, symptomatic improvement, survival data).
Due to the rarity of the condition and heterogeneity of reports, data were synthesized descriptively using: median and range for continuous variables, frequencies and proportions for categorical variables, narrative synthesis of mechanistic pathways and presentation of individual case characteristics. This review was conducted and reported in accordance with PRISMA 2020 recommendations, adapted to the descriptive nature of the available evidence.
3. Results
The systematic review identified 12 documented cases of hypercalcemia associated with PSCC published over a period of 6 decades of medical literature, between 1965 and 2024. The key characteristics of the studies are summarized in Table 1.
3.1. Clinical and Tumor Characteristics
The median age at presentation was 56 years (between 45 and 83 years). The majority of patients had advanced disease, 91.6% (11/12) presenting either locally extension of the primary tumor (at least T3) or systemically, at the time of diagnosis of hypercalcemia [6,9,13,14,15,16,17,18,19,20,21,22,23]. Five cases presented with primary tumor staged T1/T2, but complicated by hypercalcemia, as reported by Anderson and Glenn in 1965 [6].
Constitutional symptoms associated with hypercalcemia were varied and represented by anorexia, fatigue or fever in the context of tumor-associated infection. Neurological symptoms occurred in 7 cases and included altered mental status, confusion, somnolence or lethargy [9,14,15,19,20]. Belrhali et al. specifically documented bradylalia (slow speech) as a manifestation of severe hypercalcemia in their report [15].
Gastrointestinal symptoms were reported in 4 cases, with dysphagia documented as a rare, but notable manifestation. Ayyathurai et al. described dysphagia that improved concurrent with calcium normalization and recurred when calcium levels increased, suggesting a causal relationship [14]. Acute kidney injury (AKI) was reported in 4 cases, with serum creatinine elevations ranging from 1.7 to 6.25 mg/dL [9,15,19,21].
All 12 cases involved squamous cell carcinoma histology, but the tumor grade was specified in only 8 cases, the majority being represented by moderately differentiated (G2) tumors in 5 of cases (5/8) [9,13,17,19], subsequently well-differentiated (G1) tumors in 2 cases [6,22] and poorly differentiated (G3) tumors in 1 case [21].
3.2. Hypercalcemia Characteristics
Serum calcium levels at presentation had a median value of 15.45 mg/dL (12.6 – 18.6 mg/dL / 3.14 - 4.64 mmol/L). Severe hypercalcemia (≥14 mg/dL) was documented in 66.7% of cases [9,13,15,19,20,21], with the highest documented level of 18.6 mg/dL, reported by Ho et al. [26]. Moderate hypercalcemia (12.6 - 14 mg/dL) occurred in 4 cases [6,17,21,23].
Distant metastases were documented in 8 cases at the time of hypercalcemia diagnosis. The pattern of metastatic spread included: lymph node metastases - retroperitoneal (2 cases) [17,20], pulmonary metastases (4 cases) [9,14,15,19], bone metastases (2 cases) [13,26]. The presence of visceral metastases was strongly associated with poor outcomes.
3.3. Mechanistic Classification
To better characterize the three pathophysiological mechanisms, published cases were stratified by mechanism (Table 2):
3.3.1. PTHrP-Mediated Humoral Hypercalcemia
Humoral hypercalcemia of malignancy is mediated predominantly by PTHrP, which accounts for approximately 80% of cases, while less frequent mechanisms include ectopic PTH secretion and increased 1,25-dihydroxyvitamin D production, typically associated with neuroendocrine and lymphoproliferative tumors [27,28]. PTHrP increases serum calcium through bone resorption but has limited effects on renal 1,25-dihydroxyvitamin D synthesis and intestinal calcium absorption [29]. Its biological action is driven mainly by stimulation of osteoclastic activity and induces osteoblast expression of RANKL and suppresses osteoprotegerin, promoting osteoclast differentiation and activation [30].
Humoral hypercalcemia of malignancy can be sustained by a biochemical profile of elevated PTHrP with suppressed PTH [19]. PTHrP measurement was performed in 7 cases, with elevation documented in 6 cases [9,13,15,16,17,19] and borderline high in one case [21]. PTHrP levels ranged from 1.6 to 127 pmol/L (reference range typically <1.3-1.5 pmol/L). The highest PTHrP level was reported by Trejo-Rosales et al. at 127 pg/mL [9]. Concurrent PTH measurement was documented in 5 cases [9,15,17,19,21], highlighting suppressed levels in all instances, thus confirming the non-parathyroid-mediated mechanism of hypercalcemia.
Immunohistochemical confirmation of PTHrP production by tumor cells was described by Akashi et al., specifically demonstrating strong brown immunohistochemical staining for PTHrP in PC tissue [13].
3.3.2. Bone Metastasis-Associated Hypercalcemia
Bone scan metastases associated with hypercalcemia were documented in 3 cases [13,19,26]. Bone involvement included lytic lesions of the pelvis, vertebrae and ribs. It is worth noting that in the case reported by Ho et al., pathological fracture of the humerus represented the clinical manifestation of metastatic disease [26].
3.3.3. Tumor Burden-Mediated Hypercalcemia
Another hypothesis supported in the literature is that definitive control of malignant hypercalcemia relies on tumor removal. In the presence of metastatic disease, resection of the primary tumor often fails to achieve sustained correction of hypercalcemia. In 3 cases, hypercalcemia occurred in the absence of documented bone metastases, but with large primary tumors or bulky nodal masses [6,18,22]. Even though PTHrP levels were not measured in all instances, a purely humoral mechanism driven by tumor burden was suggested.
3.4. Medical Management of Hypercalcemia (Table 3)
3.4.1. Intravenous Hydration and Diuretics
Aggressive intravenous hydration with normal saline was used in all cases as initial management (2,500 to 8,000 mL per 24 hours). Loop diuretics (furosemide) were administered in 10 cases, with doses ranging from 40 to 120 mg daily. This is regarded as first-line treatment [31], but the response was limited in all cases. The calcium levels either failed to normalize or demonstrated only temporary improvement lasting mostly 24-72 hours [6,9,13,14,15,17,18,19,20,21,22,23,26].
3.4.2. Bisphosphonate Therapy
Bisphosphonates, such as pamidronate [13,14,15], etidronate [23] or zoledronic acid [9,19,21,26], were administered in 10 cases, representing the most used specific calcium-lowering therapy [32]. The response was documented, with calcium normalization achieved in 6 cases and significant reduction the other 2 cases. The benefits were represented by the relatively fast impact (time to response - 2 to 7 days) and also by the sustained effect (2-6 weeks).
3.4.3. Corticosteroids
3.4.4. Tumor Targeted Therapies
Tumor mediators most often originate in tumor tissue, whether we are referring to the primary tumor, pathological lymph nodes or secondary distant metastases. Even though favorable effects in normalizing calcium levels through treatment of the primary tumor are reported [6,18], the significant impact of surgery is described especially in cases with large lymph node metastases.
Another way in which we can act directly on tumor tissue, with the idea of indirectly controlling hypercalcemia, is represented by radiotherapy. Although applied in several cases in the literature, an impact on the control of calcemia was described by Malakoff and Schmidt. They noted that when therapy was directed on metastases (external irradiation and bleomycin), there was sustained remission of hypercalcemia, suggesting the previously mentioned hypothesis [20].

Table 3.
Therapeutic Interventions and Response Rates in Paraneoplastic Hypercalcemia Associated with PSCC.
Table 3.
Therapeutic Interventions and Response Rates in Paraneoplastic Hypercalcemia Associated with PSCC.
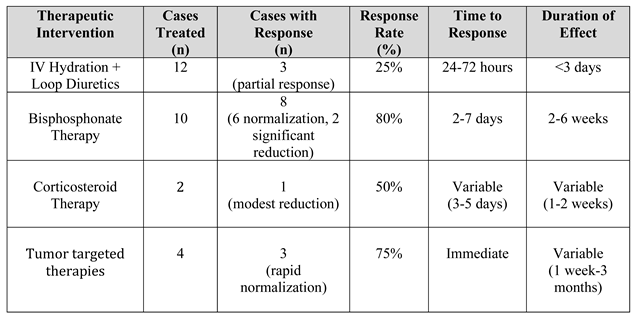 |
Abbreviations: IV - intravenous; h - hours. Response defined as normalization or significant reduction (≥2 mg/dL decrease) in serum calcium. Time to response measured from treatment initiation to documented calcium reduction. Duration represents sustained normocalcemia or calcium reduction period. Bisphosphonates included pamidronate, zoledronic acid and etidronate. Surgical debulking refers to cytoreductive surgery targeting primary tumor or bulky lymph node masses.
3.5. Survival Outcome
Hypercalcemia is a life-threatening emergency, the argument being represented by the unfavorable prognosis at the time of diagnosis. The median survival of reported cases is 9 weeks. The data varies from a 7 months survival, reported by Videtic et al., to a 9 days survival, reported by Belrhali et al., in an 82-year-old patient with refractory hypercalcemia despite bisphosphonate therapy [15,23].
Although the general clinical picture consisted of neurological disorders and altered general condition at the time of presentation in most cases, the direct cause of mortality is not specified, except in the case presented by Sekita et al. The death of the 57-year-old patient was due to renal and respiratory failure, consequences of hypercalcemia [22].
The factors with considerable impact on survival among these patients are represented by the peak of hypercalcemia (>17 mg/dL), its response to combined treatment and the presence of metastases [9,15,19]. Also, Ayyathurai et al. noted that PTHrP-related hypercalcemia seems to be a strong indicator of reduced life expectancy for PC, as for other neoplasms [14].
3.6. Temporal Trends in Diagnosis and Management
Cases were categorized by publication decade to identify the resulting changes in therapeutic and diagnostic strategy, as a result of the increased level of knowledge and experience: between 1965-1989 (n=4 cases), the management was dictated by limited biochemical characterization, impossibility of PTHrP measurement or bisphosphonates use, basic therapy consisting only in primarily supportive care. During the following period, 1990-2009 (n=4 cases), the PTHrP measurement became available, with bisphosphonate therapy emerging, thus improving mechanistic understanding. In recent times 2010-2024 (n=4 cases), we identify the routine PTHrP measurement, standardized bisphosphonate protocols, Denosumab emerging as alternative and obviously better supportive care.
4. Discussion
This systematic review identified only 12 published cases of paraneoplastic hypercalcemia in PSCC over six decades, underscoring both the extreme rarity of this metabolic disorder and clinical significance. The paucity of literature highlights both the uncommon nature of PSCC itself and the infrequency with which this paraneoplastic syndrome manifests even in advanced disease. The evidence base consists exclusively of case reports and small case series, limiting the ability to perform meta-analysis or establish definitive treatment algorithms. The present review synthesizes these reports to illustrate the spectrum of clinical presentations, underlying mechanisms and therapeutic approaches described in this uncommon paraneoplastic syndrome.
Humoral hypercalcemia of malignancy mediated by PTHrP represents the most frequently reported pathway. Seven reports document elevated PTHrP levels in the setting of suppressed iPTH, supporting this mechanism [9,13,14,15,19,21,22]. The immunohistochemical detection of PTHrP from tumor cells was documented by Akashi et al. and Sardinas et al., providing definitive evidence of ectopic hormone secretion as the causative mechanism [13,21].
The relationship between bone metastases and hypercalcemia in PSCC appears less common than the purely humoral mechanism [35]. Published cases describing osteolytic hypercalcemia emphasize the contribution of diffuse bone metastases, with some authors suggesting a mixed mechanism involving both direct bone destruction and humoral factors. A similar case is that reported by Ho et al., also without a PTHrP dosage, its particularity being represented by the diagnosis of hypercalcemia, secondary to a pathological bone fracture [26].
The literature also indicates that surgical cytoreduction (debulking) may influence calcium homeostasis in selected patients. The hypothesis is supported by Anderson and Glenn, describing the spontaneous normalization of calcium values following surgical treatment of the primary tumor [6]. In contrast is the experience reported by Malakoff and Schmidt, where primary tumor ablation had minimal effect on hypercalcemia, but subsequent therapy directed at metastatic lesions achieved calcium control. These differences suggest different anatomical tumor sites of hormonal discharge, variable among patients [20].
Notably, the degree of hypercalcemia does not implicitly correlate with tumor volume or staging. Moderate biochemical changes have been described in patients with extensive loco-regional or metastatic disease, whereas severe hypercalcemia has also been reported in the absence of significant bone involvement. This observation reinforces the multifactorial nature of hypercalcemia in PSCC.
Clinical manifestations reported across published cases are complex, highlighting neurological symptoms (altered mental status, somnolence, bradylalia), gastrointestinal dynamic disorders (loss of appetite, dysphagia), renal dysfunction and constitutional manifestations (weight loss, anorexia). Dysphagia is a rarely documented manifestation of hypercalcemia, attributed to reduced gastrointestinal smooth muscle contractility. Ayyathurai et al. reported it as a prominent symptom of the clinical picture [14].
Diagnostic evaluation requires a systematic exclusion of alternative etiologies of hypercalcemia and characterization of the underlying mechanism. This should include measurement of intact PTH, lactate dehydrogenase (LDH) and alkaline phosphatase (AP), followed by PTHrP assay when initial studies suggested a paraneoplastic etiology [36].
The biochemical profile characteristic of PTHrP-mediated hypercalcemia implies suppressed PTH, hypophosphatemia and absence of significantly elevated values of AP, in the absence of bone metastases. The confirmation of PTHrP elevation, when available, provides definitive evidence of the humoral mechanism. Immunohistochemical detection of PTHrP is rarely performed in clinical practice, but represents the gold standard for establishing ectopic hormone production, as performed by Akashi et al. [13].
Staging imaging at the time of diagnosis to detect bone metastases is a critical component of the evaluation. Published cases consistently highlighted the importance of comprehensive imaging at diagnosis to guide both metabolic and oncological management.
Management strategies described in the literature reflect the complexity of malignancy-associated hypercalcemia. The choice between bisphosphonates and denosumab represents an evolving area in the management of malignancy-associated hypercalcemia but depends on institutional resources. While bisphosphonates have historically represented first-line therapy, denosumab, a RANKL inhibitor, has demonstrated superior efficacy in some studies, particularly in bisphosphonate-refractory cases [37]. These approaches align with contemporary management principles for severe hypercalcemia of malignancy [19,21].
The occurrence of paraneoplastic hypercalcemia in PSCC uniformly indicates a poor prognosis. The survival outcome following hypercalcemia diagnosis ranges from 9 days, reported by Belrhali et al. [15], following a rapid clinical deterioration after admission, despite pamidronate, to 7 months reported by Videtic et al. [23].
The prognostic significance of hypercalcemia likely reflects the advanced tumor biology, rather than the metabolic derangement itself. While aggressive management can achieve biochemical correction, this intervention rarely translates into meaningful survival prolongation, emphasizing the need for early detection and treatment of PSCC before the development of such complications [38].
Systematic reporting and collaborative data collection are needed to improve understanding of pathophysiology, optimize management strategies and refine prognostic assessment.
- Comparison with Other Squamous Cell Carcinomas
The oncological management of PSCC has been adapted from approaches to other types of squamous cell carcinomas (SCC), based on similarities generated by the histological subtype rather than the tumor site. Paraneoplastic hypercalcemia is also an argument, sharing remarkable similarities between PSCC and squamous cell carcinomas of other anatomical sites, particularly head and neck (HNSCC) or lung (LSCC). Epidemiologically, hypercalcemia complicates 3.6-51% of advanced HNSCC and 2.5-10% of lung cancer cases, predominantly affecting patients with advanced disease, similar to the patterns observed in PSCC. The PTHrP-mediated humoral hypercalcemia is the universal mechanism across all SCC, accounting for approximately 80% of cancer-associated hypercalcemia cases [3,39,40]. All SCC types present predominantly severe hypercalcemia, with median calcium levels remarkably similar (13.5-15.5 mg/dL) [41].
Common clinical manifestations are predominant neurological (confusion, altered mental status, lethargy), the clinical picture being completed by constitutional symptoms (fatigue, weakness, weight loss), renal impairment (AKI), gastrointestinal signs (anorexia, nausea) and rare, but documented dysphagia [14,24]. Regarding the impact on treatment, bisphosphonate response rates are remarkably similar (75-85%) across all three SCC types, towards time course and duration of effect [42,43]. Treatment algorithms are essentially identical across all SCC types, with bisphosphonates as first-line approach, denosumab for refractory cases and tumor-directed therapy for long-term control [34,37]. Surgical debulking can be an important tool in controlling hypercalcemia in all types of SCC when feasible, with immediate calcium reduction following removal of PTHrP-producing tumor tissue [6,44]. The similarities are also reflected in terms of survival, with hypercalcemia universally indicating terminal disease biology regardless of anatomical site [15,45]. The data suggests that the propensity for PTHrP production and subsequent hypercalcemia represents an inherent characteristic of squamous cell differentiation rather than a site-specific phenomenon.
- Study Limitations
The systematic review has several inherent limitations. First, the retrospective nature of case collection limits generalizability and preclude meta-analysis. Publication bias exists, with severe cases more likely to be reported than typical presentations.
Second, the measurement of PTHrP was inconsistently performed across published cases (in only 58% of cases) and management approaches varied substantially. The lack of standardization of diagnostic and treatment protocols among cases reported to date limits direct comparison of outcomes. This heterogeneity limits the ability to definitively categorize pathophysiological mechanisms in all cases.
Third, the rarity of this metabolic disorder limits a statistical analysis and the conclusions can only be advisory. The survival outcomes were incompletely reported in several cases, with variable follow-up duration and inconsistent documentation of cause of death.
Finally, this review was limited to published English-language literature indexed in PubMed/MEDLINE and Scopus. Additional cases may exist in other databases or unpublished institutional experiences. A truly comprehensive understanding of this rare entity would require international registry collaboration.
Despite these limitations, this review provides the most comprehensive synthesis to date of paraneoplastic hypercalcemia in PSCC and offers a framework for future prospective studies.
- Future Research Perspectives
There are several critical knowledge gaps requiring future research: in terms of molecular status - genomic profiling of PTHrP-secreting PSCC to identify the drivers of the ectopic production, investigations of PTHrP promoter regulation and correlation of PTHrP expression patterns with tumor characteristics. Regarding the clear definition of the role of PTHrP, investigation of this biomarker as surrogate endpoint in clinical trials is needed, in order to develop predictive models incorporating PTHrP with staging parameters. The clinical practice may be optimized through development of evidence-based clinical practice guidelines and QoL studies comparing aggressive versus conservative management.
5. Conclusions
Paraneoplastic hypercalcemia represents a rare but clinically significant complication of advanced PSCC. The pathophysiological mechanisms include PTHrP-mediated humoral hypercalcemia, bone metastasis-driven osteolysis and tumor burden-mediated calcium dysregulation. Management strategies range from medical therapy with bisphosphonates or denosumab to surgical cytoreduction, with individualized approaches based on tumor characteristics and patient factors. Despite aggressive supportive care and metabolic correction, prognosis remains poor, with hypercalcemia serving as a marker of advanced disease biology. Future prospective studies are needed to better characterize the incidence, optimal management strategies and prognostic implications of this life-threatening clinical entity.
Author Contributions
Conceptualization, A.A and C.G; methodology, A.A, B.M.S and M.R.O; literature search and screening, A.A and M.A.D; data extraction and validation, A.A, M.R.O, B.O and B.M.S; formal analysis, A.A, M.R.O, and B.M.S; writing—original draft preparation, A.A; writing—review and editing, A.A, C.G, M.R.O, B.O, B.M.S, D.E.G and I.S; visualization, A.A, M.R.O, M.E and D.E.G; supervision, C.G and I.S; project administration, A.A, C.G and I.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. This systematic review analyzed only previously published data from the peer-reviewed literature and did not involve human participants.
Informed Consent Statement
Not applicable. This systematic review did not involve direct patient participation.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
This study is part of the doctoral research of Andrei Andreșanu, student at the Doctoral School of Medicine of IOSUD “Carol Davila” University of Medicine and Pharmacy in Bucharest, with Ioanel Sinescu as the scientific coordinator. The authors acknowledge the librarians at “Carol Davila” University of Medicine and Pharmacy for assistance with literature retrieval. Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila, through the institutional program Publish not Perish.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PSCC | Penile squamous cell carcinoma |
| PC | Penile cancer |
| PTH | Parathyroid hormone |
| PTHrP | Parathyroid hormone-related peptide |
| AKI | Acute kidney injury |
| RANKL | Receptor Activator of Nuclear factor Kappa-B Ligand |
| RT | Radiation therapy |
| CHT | Chemotherapy |
| ECE | Extracapsular extension |
| LVI | Lymphovascular invasion |
| LDH | Lactate dehydrogenase |
| AP | Alkaline Phosphatase |
| LS | Lichen sclerosus |
References
- Fu, L., et al., Global Pattern and Trends in Penile Cancer Incidence: Population-Based Study. JMIR Public Health Surveill 2022, 8(7), e34874. [CrossRef] [PubMed]
- Stewart, A.F. Clinical practice. Hypercalcemia associated with cancer. N Engl J Med 2005, 352(4), 373–9. [Google Scholar] [CrossRef] [PubMed]
- Mirrakhimov, A.E. Hypercalcemia of Malignancy: An Update on Pathogenesis and Management. N Am J Med Sci 2015, 7(11), 483–93. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, T.E. Mithramycin for hypercalcemia of malignant disease. Calif Med 1971, 115(4), 1–4. [Google Scholar]
- Cooper Worobey, C.; Magee, C.C. Humoral hypercalcemia of malignancy presenting after oncologic surgery. Kidney Int 2006, 70(1), 225–9. [Google Scholar] [CrossRef]
- Anderson, E.E.; Glenn, J.F. Penile Malignancy and Hypercalcemia. JAMA 1965, 192(4), 328–329. [Google Scholar] [CrossRef]
- Rudd, F.V., et al., Tumor-induced hypercalcemia. J Urol 1972, 107(6), 986–9. [CrossRef]
- Lumachi, F., et al., Medical treatment of malignancy-associated hypercalcemia. Curr Med Chem 2008, 15(4), 415–21. [CrossRef]
- Trejo-Rosales, R., et al., Rare association between penile squamous cell carcinoma and parathyroid related peptide (PTH-rP) secretion. Arq Bras Endocrinol Metabol 2014, 58(6), 646–9. [CrossRef]
- Jibrin, I.M., G.D. Lawrence, and C.B. Miller, MD, FACP Hypercalcemia of Malignancy in Hospitalized Patients. 2006.
- Spinazzé, S.; Schrijvers, D. Metabolic emergencies. Crit Rev Oncol Hematol 2006, 58(1), 79–89. [Google Scholar] [CrossRef]
- Ralston, S.H., et al., Cancer-associated hypercalcemia: morbidity and mortality. Clinical experience in 126 treated patients. Ann Intern Med 1990, 112(7), 499–504. [CrossRef]
- Akashi, T., et al., Parathyroid hormone related protein producing penile cancer. J Urol 2002, 167(1), p. 249. [CrossRef]
- Ayyathurai, R., et al., Humoral hypercalcemia of penile carcinoma. Urology 2007, 69(1), 184 e9–10. [CrossRef]
- Belrhali, I., et al., Severe Hypercalcemia in Penile Squamous Cell Carcinoma: Case Report. International Journal of Innovative Science and Research Technology (IJISRT) 2024.
- Dexeus, F.H., et al., Combination chemotherapy with methotrexate, bleomycin and cisplatin for advanced squamous cell carcinoma of the male genital tract. J Urol 1991, 146(5), 1284–7. [CrossRef] [PubMed]
- Dorfinger, K.; Maier, U.; Base, W. Parathyroid hormone related protein and carcinoma of the penis: paraneoplastic hypercalcemia. J Urol 1999, 161(5), p. 1570. [Google Scholar] [CrossRef]
- Glenn, J.F. Hypercalcemia and urologic malignancies. Urology 1995, 45(1), 139–41. [Google Scholar] [CrossRef]
- Kanta, R., et al., SAT-120 Humoral Hypercalcemia of Malignancy Caused by Squamous Cell Carcinoma of the Penis. Journal of the Endocrine Society 2020, 4 (Supplement_1).
- Malakoff, A.F.; Schmidt, J.D. Metastatic carcinoma of penis complicated by hypercalcemia. Urology 1975, 5(4), 510–3. [Google Scholar] [CrossRef]
- Sardiñas, Z., et al., Ectopic Parathyroid Hormone Secretion by A Penile Squamous Cell Carcinoma. AACE Clinical Case Reports 2018, 4(1), 9–12. [CrossRef]
- Sekita, N. Penile carcinoma with humoral hypercalcemia of malignancy (HHM): a case report. Hinyokika Kiyo 1999, 45(7), 497–9. [Google Scholar]
- Videtic, G.M.; Ago, C.T.; Winquist, E.W. Hypercalcemia and carcinoma of the penis. Med Pediatr Oncol 1997, 29(6), 576–7. [Google Scholar] [CrossRef]
- Balcombe, N.R. Dysphagia and hypercalcaemia. Postgrad Med J 1999, 75(884), 373–4. [Google Scholar] [CrossRef] [PubMed]
- Grieve, R.J.; Dixon, P.F. Dysphagia: a further symptom of hypercalcaemia? Br Med J (Clin Res Ed) 1983, 286(6382), 1935–6. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.C., et al., Metastatic penile cancer presenting as hypercalcemia and pathological fracture of the humerus: a rare event. Med J Malaysia 2006, 61(4), 503–5.
- Lumachi, F., et al., Cancer-induced hypercalcemia. Anticancer Res 2009, 29(5), 1551–5.
- Donovan, P.J., et al., PTHrP-mediated hypercalcemia: causes and survival in 138 patients. J Clin Endocrinol Metab 2015, 100(5), 2024–9. [CrossRef]
- Holick, M.F. Vitamin D deficiency. N Engl J Med 2007, 357(3), 266–81. [Google Scholar] [CrossRef]
- Reagan, P.; Pani, A.; Rosner, M.H. Approach to diagnosis and treatment of hypercalcemia in a patient with malignancy. Am J Kidney Dis 2014, 63(1), 141–7. [Google Scholar] [CrossRef]
- Rosner, M.H.; Dalkin, A.C. Onco-nephrology: the pathophysiology and treatment of malignancy-associated hypercalcemia. Clin J Am Soc Nephrol 2012, 7(10), 1722–9. [Google Scholar] [CrossRef]
- Papapoulos, S.E.; Hamdy, N.A.T.; van der Pluijm, G. Bisphosphonates in the management of prostate carcinoma metastatic to the skeleton. Cancer 2000, 88(S12), 3047–3053. [Google Scholar] [CrossRef] [PubMed]
- Kessinger, A.; Lemon, H.M.; Foley, J.F. Hypercalcemia of malignancy. Geriatrics 1972, 27(9), 97–106. [Google Scholar] [PubMed]
- Goldner, W. Cancer-Related Hypercalcemia. J Oncol Pract 2016, 12(5), 426–32. [Google Scholar] [CrossRef] [PubMed]
- Grill, V.; Martin, T.J. Hypercalcemia of malignancy. Rev Endocr Metab Disord 2000, 1(4), 253–63. [Google Scholar] [CrossRef]
- Clines, G.A. Mechanisms and treatment of hypercalcemia of malignancy. Curr Opin Endocrinol Diabetes Obes 2011, 18(6), 339–46. [Google Scholar] [CrossRef]
- Hu, M.I., et al., Denosumab for treatment of hypercalcemia of malignancy. J Clin Endocrinol Metab 2014, 99(9), 3144–52. [CrossRef]
- Asonitis, N., et al., Diagnosis, Pathophysiology and Management of Hypercalcemia in Malignancy: A Review of the Literature. Horm Metab Res 2019, 51(12), 770–778. [CrossRef]
- Brawner, J.T.; Zitsch, R.P. Parathyroid hormone-related peptide as a cause of hypercalcemia in squamous cell carcinoma of the head and neck: a case presentation and subject review. Head Neck 2004, 26(4), 382–4. [Google Scholar] [CrossRef]
- Takai, E., et al., Tumor-induced hypercalcemia and parathyroid hormone-related protein in lung carcinoma. Cancer 1996, 78(7), 1384–7. [CrossRef]
- Ramos, R.E.O., et al., Malignancy-Related Hypercalcemia in Advanced Solid Tumors: Survival Outcomes. J Glob Oncol 2017, 3(6), 728–733. [CrossRef]
- Le Tinier, F., et al., Cancer-associated hypercalcaemia in squamous-cell malignancies: a survival and prognostic factor analysis. Int J Oral Maxillofac Surg 2011, 40(9), 938–42. [CrossRef]
- Mamou, E., et al., Prognosis and Phenotypes of Advanced Head and Neck Carcinoma Associated With Hypercalcemia. Head Neck 2025, 47(8), 2174–2182. [CrossRef]
- Lazutkin, A., et al., Head and neck non-metastatic cancer associated hypercalcemia. International Surgery Journal 2019, 6(6), 2183–2186. [CrossRef]
- Penel, N., et al., Prognosis of hypercalcemia in aerodigestive tract cancers: study of 136 recent cases. Oral Oncol 2005, 41(9), 884–9. [CrossRef]
Figure 1.
Flowchart of paper selection process.
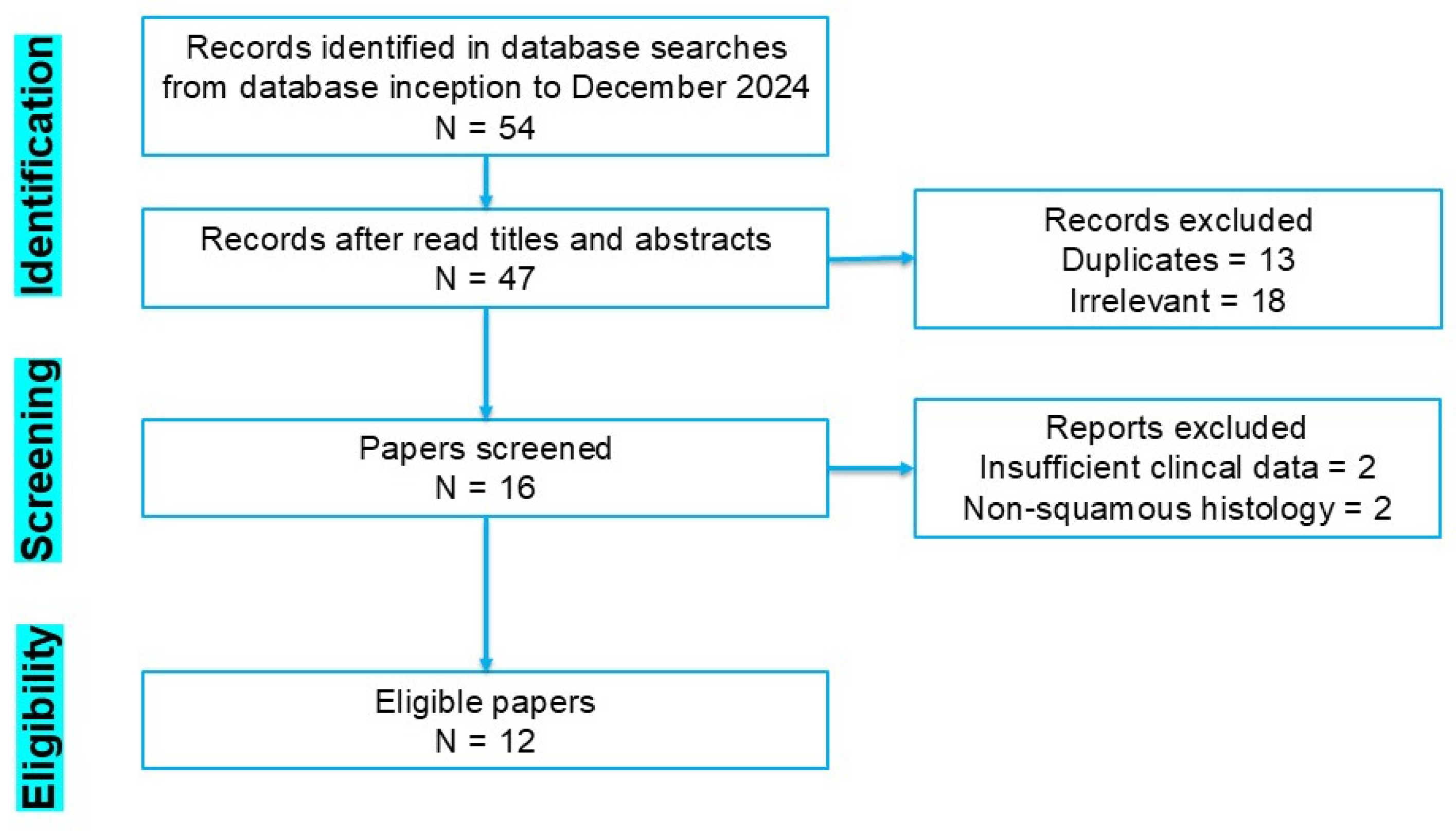
Table 1.
Summary of Published Cases of Hypercalcemia Associated with PSCC.
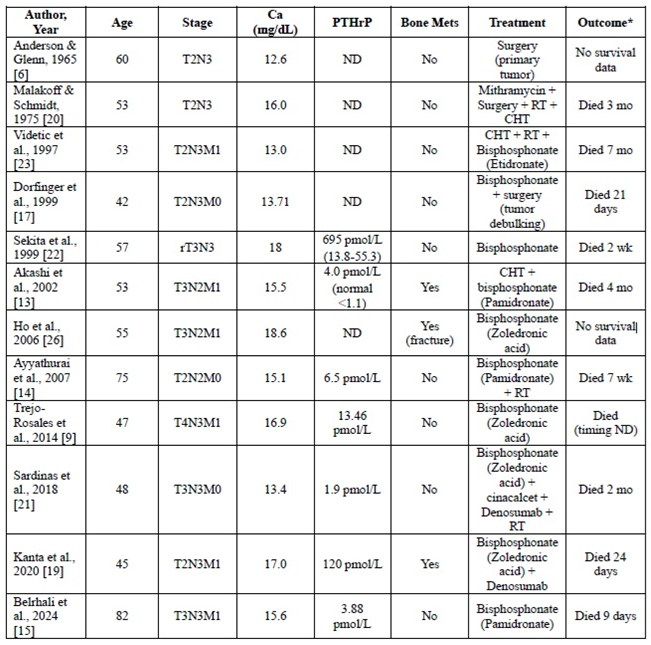 |
Abbreviations: Ca - calcium; PTHrP - parathyroid hormone-related peptide; ND - not documented; Mets - metastases; RT - radiation therapy; CHT - chemotherapy; wk – weeks; mo – months; *Calculated after hypercalcemia diagnosis
Table 2.
Biochemical Characteristics and Clinical Features by Mechanistic Subtype of Paraneoplastic Hypercalcemia in PSCC.
Table 2.
Biochemical Characteristics and Clinical Features by Mechanistic Subtype of Paraneoplastic Hypercalcemia in PSCC.
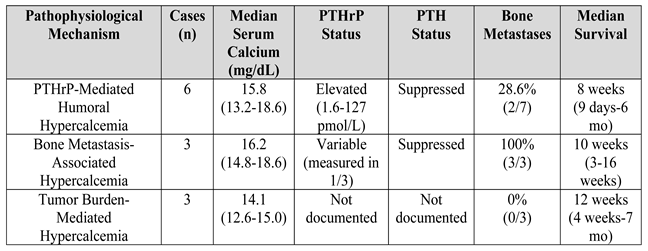 |
Abbreviations: PTHrP - parathyroid hormone-related peptide; PTH - parathyroid hormone; Ca - calcium; Mets - metastases.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



