Submitted:
28 January 2026
Posted:
28 January 2026
You are already at the latest version
Abstract
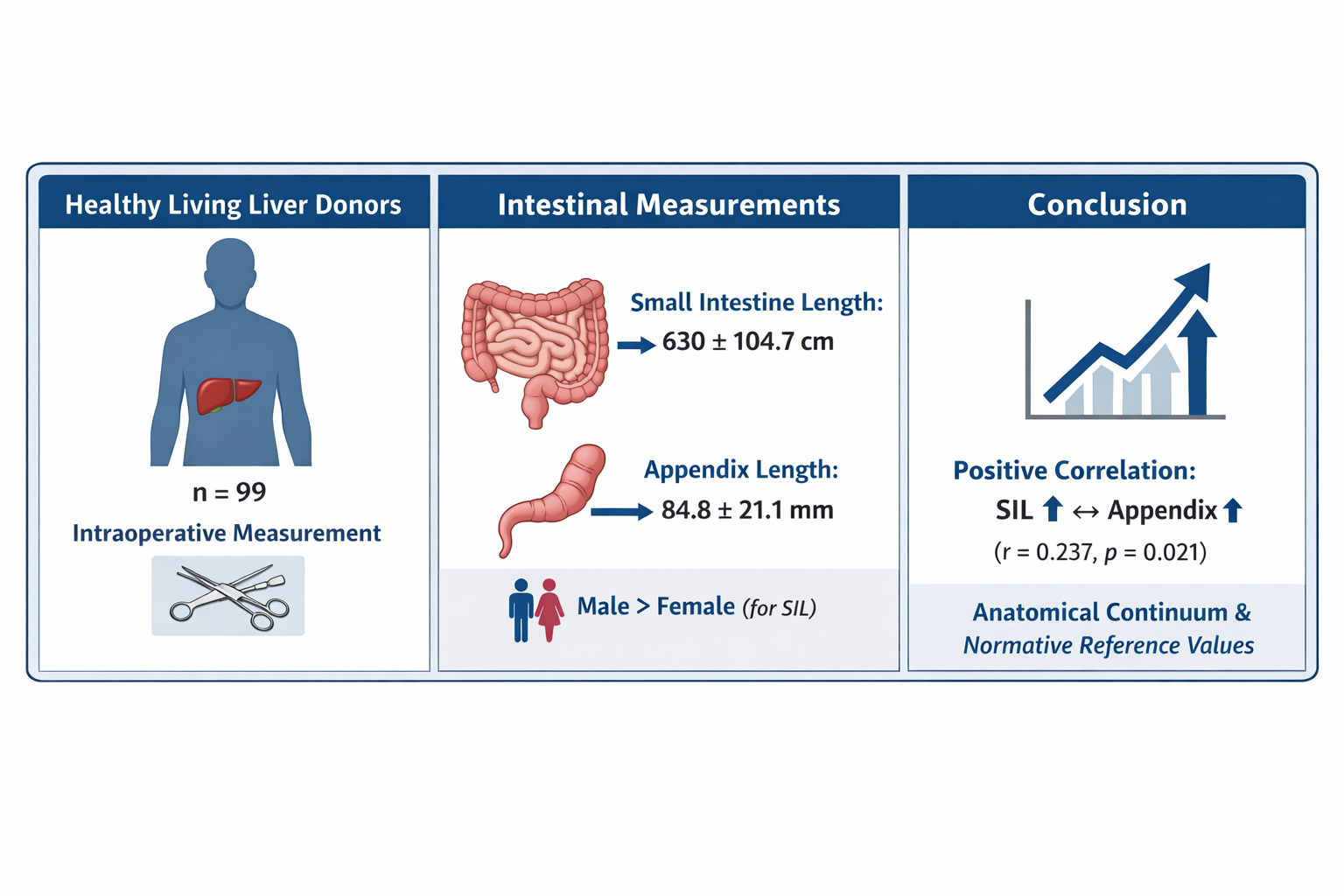
Background/Objectives: Small intestine and vermiform appendix lengths are critical anatomical parameters with significant implications for bariatric surgery, transplantation, and the management of short bowel syndrome. However, reliable normative data derived from direct in vivo measurements in healthy individuals remain limited. This study aimed to establish reference values in a homogeneous cohort of healthy living liver donors and to investigate the potential anatomical and functional correlation between these two structures based on their shared embryological origin and immunological roles.
Methods: Data from 99 healthy living liver donors representing a multi-ethnic population were analyzed. Intraoperative measurements were performed using a standardized surgical technique: small intestine length was measured from the ligament of Treitz to the ileocecal valve, and appendix length from the base to the tip. Relationships between morphometric measurements and anthropometric variables were evaluated.
Results: The mean small intestine length was 630 ± 104.7 cm, and the mean appendix length was 84.8 ± 21.1 mm. Small intestine length was significantly greater in males (p = 0.011), while appendix length showed no sex-based difference. A weak but statistically significant positive correlation was found between small intestine length and appendix length (r = 0.237; p = 0.021). Furthermore, an appendix length ≥8 cm was associated with a higher probability of having a small intestine length >600 cm. Notably, the retrocecal appendix position was observed in only 4.0% of donors, a prevalence substantially lower than that reported in appendicitis series, suggesting it may be a risk factor for inflammation.
Conclusions: This study provides normative reference values derived from healthy individuals, free from the bias of cadaveric changes or inflammation. The novel finding of a correlation between small intestine and appendix lengths supports the hypothesis of a functional "anatomical continuum" within the gut-associated lymphoid tissue (GALT) system. These data may offer practical guidance for surgical planning in procedures requiring precise bowel length estimation.
Keywords:
appendix
; intestine
; small
; living donors
; organ size
; reference values
; anatomy
1. Introduction
The length of the small intestine is a fundamental anatomical variable that plays a decisive role in digestive physiology and surgical outcomes. Although classical anatomical studies have attempted to define "normal" values, results have varied widely due to methodological differences, such as the use of cadavers affected by postmortem tissue relaxation [1,2]. Consequently, establishing reliable normative reference ranges based on living, healthy individuals remains a challenge in surgical literature.
From a clinical perspective, knowing the precise length of the small intestine is critical, particularly in the era of metabolic and transplant surgery. In short bowel syndrome, the residual intestinal length is the strongest predictor of nutritional independence; patients with less than 200 cm of functional bowel face a high risk of chronic malabsorption [3]. Similarly, in bariatric procedures such as Roux-en-Y gastric bypass, standardizing the length of the alimentary and biliopancreatic limbs assumes a relative uniformity in total bowel length [4]. However, if total length varies significantly among individuals, a fixed-length bypass could lead to insufficient weight loss in patients with long intestines or severe malnutrition in those with short intestines [5]. Therefore, preoperative estimation or reliable population norms are essential for tailoring surgical approaches.
The vermiform appendix, traditionally regarded as a vestigial organ, is now recognized as a specialized component of the gut-associated lymphoid tissue (GALT) system. It serves as a reservoir for commensal bacteria and plays a role in mucosal immunity. Its length, diameter, and anatomical variations may directly influence both the clinical presentation and the surgical approach [6,7]. Despite their distinct morphologies, the small intestine and the appendix share a common embryological origin from the midgut. Biologically, it is plausible to hypothesize a functional "anatomical continuum" between these structures; a longer small intestine, possessing a larger mucosal surface area and microbial load, might require a more developed lymphoid organ—i.e., a longer appendix—for adequate immunoregulatory support [8,9]. However, this potential morphometric relationship has not been systematically evaluated in healthy human populations.
Most existing data on these organs are derived from cadaveric studies or patient cohorts undergoing surgery for specific pathologies, which may introduce bias due to inflammation or anatomical distortion [10,11]. Intraoperative measurements performed in living patients typically involve heterogeneous groups. Therefore, reliable normative anatomical data derived from a homogeneous cohort of completely healthy individuals, obtained using direct intraoperative measurements—the accepted gold standard—are still needed [12].
The primary aim of this study was to establish normative reference values for small intestine and appendix lengths using direct intraoperative measurements in a multi-ethnic cohort of healthy living donors. Secondly, we aimed to test the hypothesis that appendix length is positively correlated with small intestine length, potentially serving as a surrogate marker in surgical planning.
2. Materials and Methods
2.1. Study Design and Ethical Approval
This single-center, descriptive, retrospective cohort study was conducted at the Department of General Surgery, Istanbul Aydın University. The study protocol adhered strictly to the ethical principles of the Declaration of Helsinki and received formal approval from the Istanbul Aydın University Non-Interventional Clinical Research Ethics Committee on 03 April 2024 (Approval No. 29/2024). To ensure patient confidentiality, all data were fully anonymized prior to analysis.
2.2. Participant Selection
The study population consisted of healthy individuals who underwent living-donor liver transplantation surgery between October 2023 and July 2025. A total of 103 consecutive donor candidates were initially assessed. Rigorous exclusion criteria were applied to ensure a homogeneous "healthy" cohort: individuals with a prior history of appendectomy (n=1), cases disqualified from donation due to intraoperative findings (n=1), and donors with incomplete morphometric data (n=2) were excluded. Consequently, the final analysis included 99 healthy living liver donors.
Inclusion criteria were defined as: age between 18 and 55 years, undergoing surgery as a living liver donor, no history of major abdominal surgery, and absence of known intestinal pathology. Candidates for living liver donation undergo an extensive preoperative screening process to confirm optimal physiological health, making this cohort a unique representation of the "normal" human population, free from the biases often found in cadaveric or symptomatic patient series.
2.3. Data Collection and Measurement Techniques
Demographic and anthropometric data, including age, sex, height (cm), weight (kg), and body mass index (BMI), were recorded. Standardized Intraoperative Measurement: All measurements were performed by a single surgeon within the same transplant team to eliminate inter-observer variability. Measurements were taken intraoperatively under general anesthesia, ensuring complete muscle relaxation.
• Small Intestine Length (SIL): The length was measured from the ligament of Treitz to the ileocecal valve along the antimesenteric border. To avoid the confounding effect of tissue elasticity, a standardized technique was used where the bowel was measured segment by segment using a 70 cm sterile nylon surgical tape, without applying excessive traction. This technique aligns with established methods recognized in the literature as the most accurate for in vivo assessment [12,13,14].
• Appendix Length: The vermiform appendix was measured from its base at the cecal wall to its distal tip. The free segment was gently extended to its physiological length without overstretching. Measurements were taken only when the organ was in a relaxed state, avoiding spasm.
• Ethical Consideration for Retrocecal Appendix: In cases where the appendix was located in a retrocecal position, it was measured in situ. Mobilization of a healthy retrocecal appendix solely for measurement purposes was avoided to prevent unnecessary tissue trauma and potential postoperative complications for the healthy donor.
Anatomical variations, such as Meckel's diverticulum, were also documented during the exploration.
2.4. Statistical Analysis
Data were entered into Microsoft Excel and analyzed using SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). The normality of continuous variables was assessed using the Kolmogorov–Smirnov test and visual inspection of histograms. Continuous variables with a normal distribution were presented as mean ± standard deviation (SD), while those with a non-normal distribution were expressed as median (minimum–maximum). Categorical variables were summarized as frequencies (n) and percentages (%).
For comparisons between two independent groups (e.g., male vs. female), the Student's t-test was used for normally distributed data, and the Mann–Whitney U test for non-normally distributed data. The relationships between morphometric measurements (SIL, appendix length) and anthropometric variables were evaluated using Pearson correlation analysis.
The sample size was not determined by an a priori power analysis; rather, it included all consecutive eligible cases within the study period. Therefore, the study was designed as a hypothesis-generating exploratory analysis. Cut-off values for appendix length and subsequent ROC (Receiver Operating Characteristic) analyses were conducted as part of this exploratory approach to investigate the predictive value of appendix length for intestinal length. A p-value of <0.05 was considered statistically significant.
3. Results
3.1. Demographic and Anthropometric Characteristics
The study cohort consisted of 99 healthy living liver donors, comprising 46 females (46.5%) and 53 males (53.5%). The mean age was 33.6 ± 9.6 years (range: 18–55 years). The participants represented a physically healthy population with a mean BMI of 24.0 ± 3.5 kg/m². Detailed baseline characteristics are presented in Table 1.
3.2. Small Intestine and Appendix Morphometry
The mean small intestine length (SIL) for the entire cohort was 630 ± 104.7 cm, with a wide range of variation from 432 cm to 910 cm. A statistically significant difference was observed between sexes; males had a longer mean SIL compared to females (654.8 ± 110.2 cm vs. 601.5 ± 91.1 cm; p = 0.011).
The mean appendix length was 84.8 ± 21.1 mm (range: 50–150 mm). Unlike the small intestine, appendix length did not differ significantly between males (86.5 ± 21.0 mm) and females (82.8 ± 21.4 mm) (p = 0.389). The distribution of measurements by sex is summarized in Table 2.
3.3. Geographical Distribution of the Cohort
A unique strength of this study is the multi-ethnic composition of the donor pool, representing 13 different countries. While the majority of donors were of Turkish origin (60.6%), a significant portion (39.4%) consisted of international donors, predominantly from North African and Middle Eastern regions. Subgroup analysis of nationalities with n ≥ 5 revealed that mean SIL values were relatively consistent across different ethnic groups, ranging from 622 cm (Iraq) to 643 cm (Algeria). The geographical distribution and corresponding SIL values are detailed in Table 3.
3.4. Anatomical Variations
Anatomical variations were meticulously documented during the surgical exploration. A retrocecal appendix position was identified in only 4 donors (4.0%). This prevalence is notably lower than rates frequently reported in acute appendicitis series. Additionally, Meckel's diverticulum was incidental detected in 2 donors (2.0%). No other significant intestinal anomalies were observed in this healthy cohort.
3.5. Correlation Analysis
Pearson correlation analysis demonstrated that SIL was positively correlated with both height (r = 0.256, p = 0.011) and weight (r = 0.261, p = 0.009). However, no significant correlation was found between SIL and age (p = 0.927), suggesting that intestinal length remains stable in adulthood. All correlation coefficients and significance levels are summarized in Table 4.
A key finding of this study was the statistically significant positive correlation between small intestine length and appendix length (r = 0.237; p = 0.021). As illustrated in Figure 1, individuals with longer appendices tended to have longer small intestines, supporting the hypothesis of an anatomical continuum.
The scatter plot demonstrates a statistically significant positive correlation (r = 0.237, p = 0.021), suggesting that individuals with longer appendices tend to have longer small intestines.
3.6. Predictive Value of Appendix Length
To evaluate the clinical utility of appendix length as a predictor for intestinal length, donors were stratified based on appendix length. Donors with an appendix length ≥8 cm had a significantly longer mean SIL compared to those with an appendix <8 cm (645.4 ± 107.6 cm vs. 595.6 ± 94.0 cm; p = 0.021). Detailed comparative statistics for these subgroups are provided in Table 5.
Further exploratory analysis using logistic regression indicated that for every 1 cm increase in appendix length, the likelihood of having a small intestine longer than 600 cm increased by a factor of 1.28 (OR = 1.28; 95% CI: 1.03–1.58; p = 0.025). The logistic regression model demonstrating this probability is shown in Figure 2.
The solid line represents the estimated probability, while the shaded area indicates the 95% confidence interval. The vertical dotted lines mark the 6 cm and 8 cm thresholds.
Finally, to define a practical cut-off value for surgical decision-making, a Receiver Operating Characteristic (ROC) curve analysis was performed. The analysis confirmed the discriminatory ability of appendix length in predicting a small intestine length ≥600 cm, yielding an Area Under the Curve (AUC) of 0.63 (95% CI: 0.51–0.74). While the overall predictive power was moderate, the analysis identified 8.0 cm as the optimal threshold. At this cut-off point, appendix length demonstrated a high sensitivity of 76%, suggesting that donors with an appendix shorter than 8 cm are less likely to have a long small intestine. The ROC curve illustrating this diagnostic performance is presented in Figure 3.
The Area Under the Curve (AUC) is 0.63 (95% CI: 0.51–0.74), indicating a moderate predictive value.
4. Discussion
This study contributes to the surgical literature by providing normative reference values for small intestine and vermiform appendix lengths obtained through direct intraoperative assessment in a strictly screened, healthy, and geographically diverse cohort of living liver donors. By focusing exclusively on healthy individuals, we aimed to eliminate the confounding biases often introduced by inflammation, chronic disease, or postmortem tissue changes that have limited the accuracy of previous anatomical studies.
The mean small intestine length observed in our cohort was 630.0 ± 104.7 cm. This value represents a physiological middle ground between the longer lengths frequently reported in cadaveric studies and the shorter lengths seen in some living patient series. These variations are likely attributable to differences in measurement standardization, as well as anthropometric and genetic differences among populations. A detailed comparison of our findings with previous cadaveric and in vivo studies is presented in Table 6.
For instance, [1] reported a mean length of roughly 690 cm in cadavers, a discrepancy likely attributable to the postmortem loss of smooth muscle tone leading to tissue elongation. Conversely, living patient cohorts often yield lower means, such as the ~460 cm reported by [15] or 506 cm by [16]. Our finding of 630 cm suggests that in a healthy individual under general anesthesia, where muscle tone is preserved but relaxed, the measurements reflect the most accurate "functional" anatomical length. Recent studies on bariatric populations have also highlighted the importance of these measurements for predicting malnutrition risks [17].
Regarding anthropometric variables, our data confirmed that males possess significantly longer small intestines than females (654.8 cm vs. 601.5 cm; p = 0.011), likely due to greater body surface area and metabolic mass. While some meta-analyses have suggested varying relationships between appendiceal morphometry and body dimensions [18], our findings align with studies indicating a positive correlation between organ size and height/weight [19]. The absence of a correlation with age supports the view that intestinal length remains anatomically stable in adulthood [2].
Beyond standard morphometry, this study offers novel insights into the biological relationship between the appendix and the small intestine. We identified a significant positive correlation between the lengths of these two organs (r = 0.237; p = 0.021), a finding that supports the hypothesis of a functional "anatomical continuum." Since both structures share a common embryological origin from the midgut and are integral components of the GALT system, this correlation is biologically plausible [7]. It is reasonable to postulate that a longer small intestine, which presents a larger mucosal surface area and sustains a higher microbial load, requires a more developed lymphoid reservoir for immune regulation [8,9]. This functional linkage is further supported by animal models where compensatory hypertrophy of the appendix—or cecal lymphoid patches—has been observed following massive small intestinal resection [20].
These anatomical variations have profound implications for modern surgical practice. Procedures such as Roux-en-Y gastric bypass often employ standardized limb lengths under the assumption of anatomical uniformity. However, our data reveal a massive range in total intestinal length (432–910 cm). Bypassing 150 cm in a patient with a 432 cm total length represents a critical reduction in absorptive capacity, whereas the same bypass in a patient with 910 cm constitutes a much smaller fraction [4,5]. Similarly, in the management of short bowel syndrome, where the residual length is the strongest predictor of nutritional autonomy [3], our predictive analysis suggests that appendix length could serve as a surrogate marker.
Perhaps the most striking incidental finding of our study was the remarkably low prevalence of the retrocecal appendix position (4.0%) in our healthy donors. This stands in stark contrast to the 25–79% prevalence frequently reported in acute appendicitis series [21,22]. Since our cohort consists of healthy individuals screened to exclude pathology, this discrepancy implies that the retrocecal position is not merely a random anatomical variant but a significant risk factor for appendicitis. The anatomical configuration may predispose the organ to kinking, impaired lymphatic drainage, or luminal stasis, thereby increasing susceptibility to inflammation [23]. Similarly, the 2.0% prevalence of incidental Meckel's diverticulum aligns with general population rates reported in systematic reviews [24,25], further supporting the representativeness of our cohort.
Author Contributions
Conceptualization, C.K., S.K. and E.S.; Methodology, E.S. and A.T.; Validation, S.K. and A.D.; Formal Analysis, E.S.; Investigation, B.U.; Data Curation, A.T.; Writing—Original Draft Preparation, E.S.; Writing—Review and Editing, C.K. and B.U.; Visualization, E.S.; Supervision, C.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Non-Interventional Clinical Research Ethics Committee of Istanbul Aydın University (Approval No. 29/2024, Date: 03 April 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hounnou, G.; Destrieux, C.; Desmé, J.; Bertrand, P.; Velut, S. Anatomical study of the length of the human intestine. Surg. Radiol. Anat. 2002, 24, 290–294. [Google Scholar] [CrossRef]
- Underhill, B.M. Intestinal length in man. Br. Med. J. 1955, 2, 1243–1246. [Google Scholar] [CrossRef]
- Parrish, C.R. The clinician’s guide to short bowel syndrome. Gut 2005, 54, iv1–iv12. [Google Scholar]
- Mahawar, K.K.; Kumar, P.; Parmar, C.; Graham, Y.; Carr, W.R.; Jennings, N.; Schroeder, N.; Small, P.K. Small bowel limb lengths and Roux-en-Y gastric bypass: a systematic review. Obes. Surg. 2016, 26, 660–671. [Google Scholar] [CrossRef]
- Felsenreich, D.M.; Langer, F.B.; Eichelter, J.; Jedamzik, J.; Kristo, I.; Prager, G. Bariatric surgery—how much malabsorption do we need? A review of various limb lengths in different gastric bypass procedures. J. Clin. Med. 2021, 10, 674. [Google Scholar] [CrossRef]
- Akbulut, S.; Tas, M.; Sogutcu, N.; Arikanoglu, Z.; Basbug, M.; Ulku, A.; Yagmur, Y. Unusual histopathological findings in appendectomy specimens: a retrospective analysis and literature review. World J. Gastroenterol. 2011, 17, 1961–1970. [Google Scholar] [CrossRef] [PubMed]
- Mowat, A.M.; Agace, W.W. Regional specialization within the intestinal immune system. Nat. Rev. Immunol. 2014, 14, 667–685. [Google Scholar] [CrossRef]
- Girard-Madoux, M.J.H.; Gómez de Agüero, M.; Ganal-Vonarburg, S.C.; Mooser, C.; Belz, G.T.; Macpherson, A.J.; Vivier, E. The immunological functions of the appendix: An example of redundancy? Semin. Immunol. 2018, 36, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Vitetta, L.; Chen, J.; Clarke, S. The vermiform appendix: an immunological organ sustaining a microbiome inoculum. Clin. Sci. 2019, 133, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gondolesi, G.; Ramisch, D.; Padin, J.; Rumbo, C.; Alvarez, G.; Pekolj, J. What is the normal small bowel length in humans? First donor-based cohort analysis. Am. J. Transplant. 2012, 12, S49–S54. [Google Scholar] [CrossRef]
- Shatari, T.; Clark, M.A.; Yamane, T.; Engel, A.F. Reliability of radiographic measurement of small intestinal length. Colorectal Dis. 2004, 6, 327–329. [Google Scholar] [CrossRef] [PubMed]
- Muise, E.D.; Tackett, J.J.; Callender, K.A.; et al. Accurate assessment of bowel length: the method of measurement matters. J. Surg. Res. 2016, 206, 146–150. [Google Scholar] [CrossRef]
- Karagül, S.; Kayaalp, C.; Kirmizi, S.; Tamer, D.; Ersan, V. Influence of repeated measurements on small bowel length. SpringerPlus 2016, 5, 1649. [Google Scholar] [CrossRef] [PubMed]
- Karagül, S.; Kayaalp, C. Repeated stretched or non-stretched small bowel length measurements in healthy individuals. Turk. J. Surg. 2019, 35, 1–5. [Google Scholar] [CrossRef]
- Hosseinpour, M.; Behdad, A. Evaluation of small bowel measurement in alive patients. Surg. Radiol. Anat. 2008, 30, 653–655. [Google Scholar] [CrossRef]
- Teitelbaum, E.N.; Vaziri, K.; Zettervall, S.; Amdur, R.L.; Orkin, B.A. Intraoperative small bowel length measurements and analysis of demographic predictors of increased length. Clin. Anat. 2013, 26, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Sayadishahraki, M.; Mahmoudieh, M.; Keleidari, B.; Jamshidi, K.; Shahraki, A.D. Using anthropometric and demographic factors to predict small bowel length to prevent malnutrition in bariatric surgery. Adv. Biomed. Res. 2023, 12, 209. [Google Scholar] [CrossRef]
- Kacprzyk, A.; Droś, J.; Stefura, T.; Krzysztofik, M.; Jasińska, K.; Pędzisz, P.; Mizia, E.; Major, P. Variations and morphometric features of the vermiform appendix: a systematic review and meta-analysis of 114,080 subjects with clinical implications. Clin. Anat. 2020, 33, 85–98. [Google Scholar] [CrossRef]
- Raschka, S.; Raschka, C. On the relationship between body dimensions and appendix length. Anthropol. Anz. 2008, 66, 67–72. [Google Scholar] [CrossRef]
- Sachdev, R.; Ackerman, N.B. Comparison of changes in intestinal length and circumference after 90 per cent bypass and 90 per cent resection. Am. J. Surg. 1979, 137, 208–212. [Google Scholar] [CrossRef]
- Wakeley, C.P.G. The position of the vermiform appendix as ascertained by an analysis of 10,000 cases. J. Anat. 1933, 67, 277–283. [Google Scholar]
- Ghorbani, A.; Forouzesh, M.; Kazemifar, A.M. Variation in anatomical position of vermiform appendix among Iranian population: an old issue which has not lost its importance. Anat. Res. Int. 2014, 2014, 313575. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Wang, Y.C.; Yang, H.R.; Chung, P.K.; Jeng, L.B.; Chen, R.J. Retroperitoneal abscess resulting from perforated acute appendicitis: analysis of its management and outcome. Surg. Today 2007, 37, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Sagar, J.; Kumar, V.; Shah, D.K. Meckel’s diverticulum: a systematic review. J. R. Soc. Med. 2006, 99, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Kuru, S.; Kismet, K. Meckel’s diverticulum: clinical features, diagnosis and management. Rev. Esp. Enferm. Dig. 2018, 110, 726–732. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Correlation between small intestine length (SIL) and appendix length.
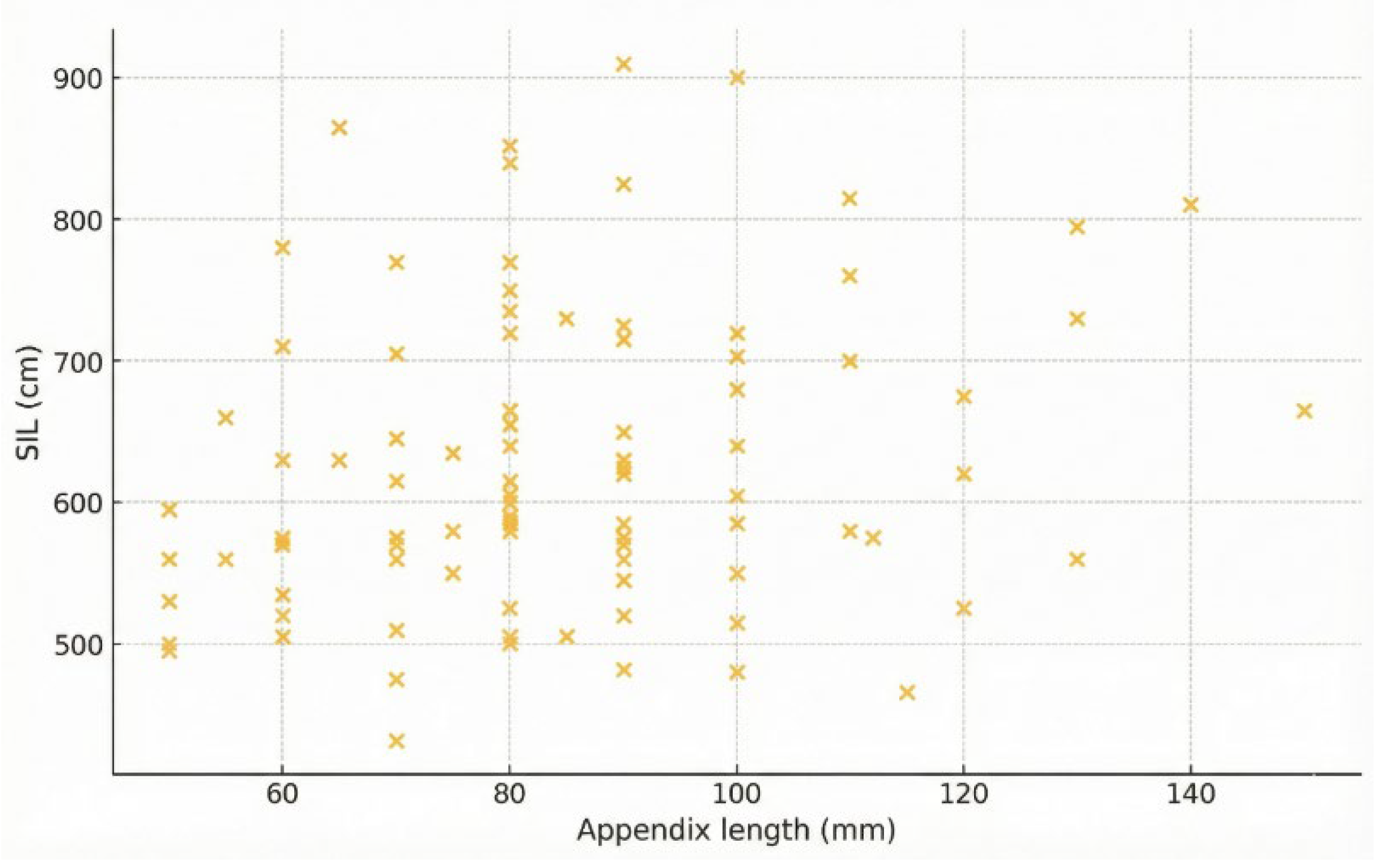
Figure 2.
Logistic regression curve showing the probability of having a small intestine length (SIL) ≥600 cm based on appendix length.
Figure 2.
Logistic regression curve showing the probability of having a small intestine length (SIL) ≥600 cm based on appendix length.
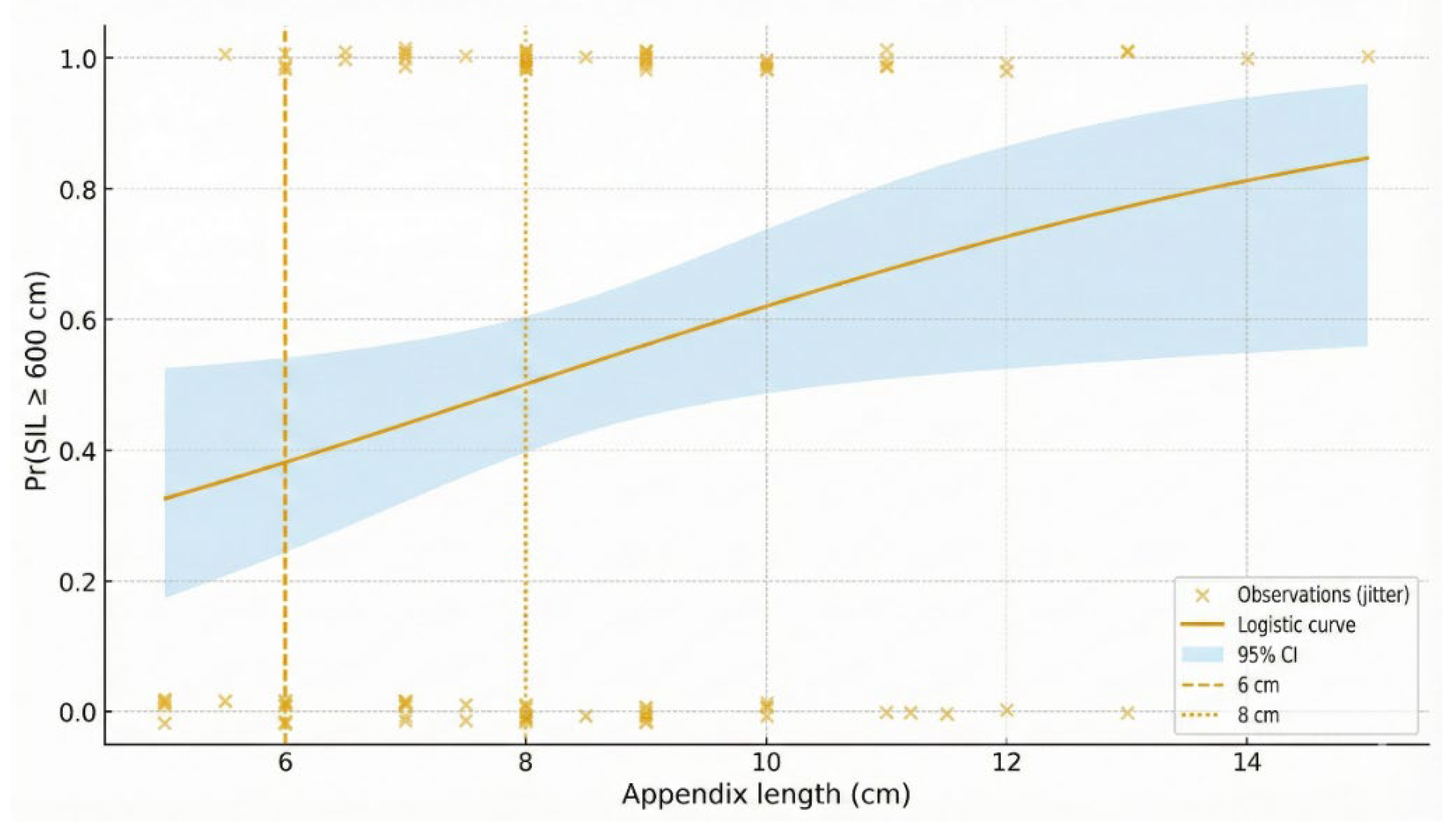
Figure 3.
Receiver Operating Characteristic (ROC) curve illustrating the discriminatory ability of appendix length in predicting a small intestine length ≥600 cm.
Figure 3.
Receiver Operating Characteristic (ROC) curve illustrating the discriminatory ability of appendix length in predicting a small intestine length ≥600 cm.
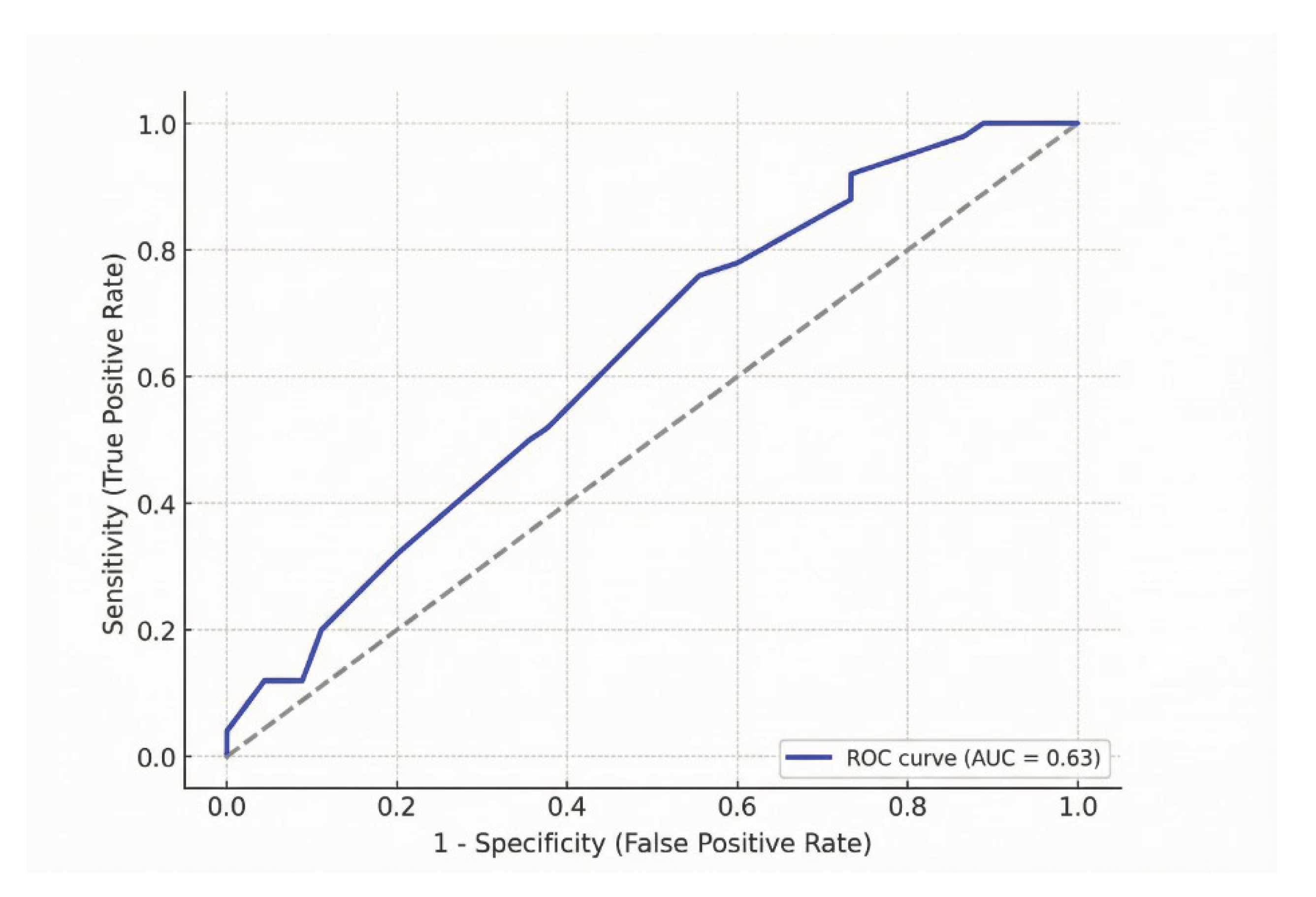

Table 1.
Demographic and anthropometric characteristics of the donors (n=99).
| Parameter | Mean ± SD / n (%) | Range (min-max) |
|---|---|---|
| Age (years) | 33.6 ± 9.6 | 18–55 |
| Sex | Female 46 (46.5%) Male 53 (53.5%) |
– |
| Height (cm) | 170.7 ± 9.6 | 147–192 |
| Weight (kg) | 70.1 ± 12.8 | 46–106 |
| BMI (kg/m²) | 24.0 ± 3.5 | 16.5–34.4 |
Note: Data are reported as mean ± standard deviation and range (minimum–maximum). Abbreviation: BMI: Body Mass Index.
Table 2.
Small intestine and appendix length measurements by sex.
| Parameter | Entire Cohort | Female | Male | p value* |
|---|---|---|---|---|
| SIL (cm) | 630.0 ± 104.7 | 601.5 ± 91.1 | 654.8 ± 110.2 | 0.011 |
| Appendix (mm) | 84.8 ± 21.1 | 82.8 ± 21.4 | 86.5 ± 21.0 | 0.389 |
Note: Data are presented as mean ± standard deviation. * Differences between groups were evaluated using Student’s t-test. Abbreviation: SIL: Small Intestine Length.
Table 3.
Distribution of Small Intestine Length (SIL) by Nationality (Groups with n ≥ 5).
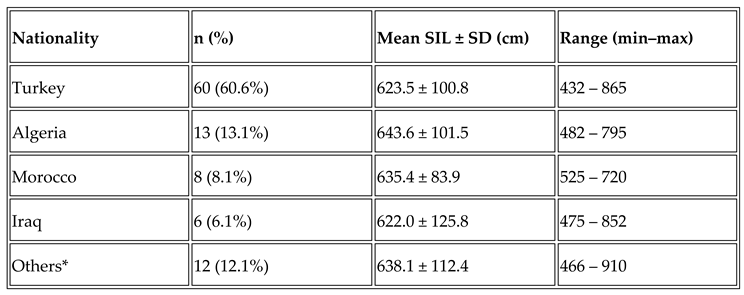 |
Note: * Includes donors from 9 other countries with n < 5. Data are presented as mean ± standard deviation and range (minimum–maximum). This distribution highlights the multi-ethnic composition of the study cohort. Abbreviation: SIL: Small Intestine Length.
Table 4.
Correlation coefficients between morphometric and anthropometric variables.
| Parameter | Height | BMI | Age |
|---|---|---|---|
| SIL | 0.256 (p=0.011) | 0.261 (p=0.009) | -0.009 (p=0.927) |
| Appendix | 0.214 (p=0.037) | 0.292 (p=0.004) | -0.072 (p=0.486) |
Note: Data represent Pearson correlation coefficients (r) and corresponding p-values. Abbreviations: SIL: Small Intestine Length; BMI: Body Mass Index.
Table 5.
Comparison of Small Intestine Length According to Appendix Length Subgroups.
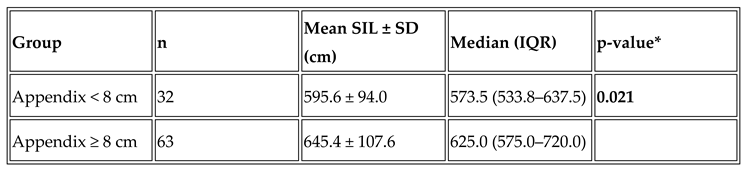 |
Note: Donors with an appendix length ≥ 8 cm had significantly longer small intestines. * Statistical comparison was performed using the Mann–Whitney U test. Abbreviations: SIL: Small Intestine Length; SD: Standard Deviation; IQR: Interquartile Range (q1–q3).
Table 6.
Comparison of mean small intestine length (SIL) reported in selected studies versus the current study.
Table 6.
Comparison of mean small intestine length (SIL) reported in selected studies versus the current study.
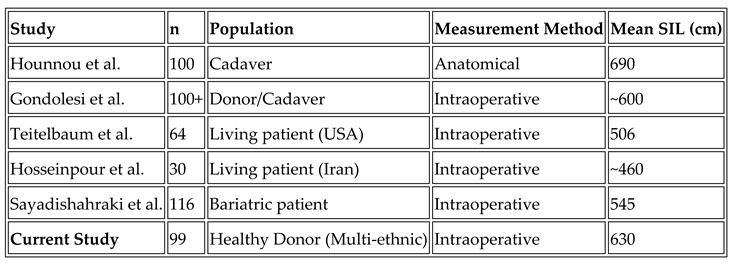 |
Note: This table highlights the variability in reported intestinal lengths based on the population type (cadaver vs. living) and measurement technique. Abbreviation: SIL: Small Intestine Length.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



