
Submitted:
28 January 2026
Posted:
28 January 2026
You are already at the latest version
Abstract
The ICD-11 release renewed interest in comparable traditional medicine data. The ICD-11 Traditional Medicine chapter, known as TM1, supports optional dual coding for morbidity but is not used for mortality reporting. TM1 includes two entity types: traditional medicine disorders and patterns. Coders may record a TM1 disorder, a TM1 pattern, or both, always paired with a primary diagnosis from Chapter 01 to 25.This roadmap coordinates TM1 with SNOMED CT and LOINC for clinical semantics, HL7 FHIR R5 for product and ingredient catalogs and prescribing workflows, and the OMOP Common Data Model for analytics. A clear boundary for FHIR has been drawn:FHIR Product-Definition resources represent catalog data, not care events. Clinical events use Medication, MedicationRequest, and MedicationDispense. This distinction is important in traditional medicine-authorized manufactured products fit the Product-Definition resources, while compounded prescriptions prepared in healthcare settings usually lack product master entries and should be captured as medication based care events with ingredient-level details. The OMOP handoff uses ETL mapping tables linking FHIR identifiers and ingredients to OMOP standard concepts, without assuming one-to-one equivalence. This roadmap proposes to add TM1 as an optional supplementary code in the next KCD revision. Also, the site checklist in this roadmap covers regulations, co-coding examples, EHR certification, terminology management, FHIR catalogues, and OMOP loading. This would improve international comparability and safety surveillance and support clinical research and AI applications more strongly. This is helpful as it will not interfere with current medical reimbursement or mortality management workflows.
Keywords:
ICD-11
; traditional medicine
; dual coding
; SNOMED CT
; LOINC
; HL7 FHIR R5
; OMOP CDM
; interoperability
; Korea
1. Introduction
Health systems increasingly need traditional medicine data that can be compared across countries and reused in analytics and research [1]. The 2025 ICD-11 release refreshed this framework and brought renewed attention to traditional medicine within an international classification used for health statistics [1,2].
The ICD-11 is designed for recording, reporting, and statistical analysis of mortality and morbidity. This is essential for comparability, but lacking the clinical detail needed for real-world evidence [2,3,4]. A practical approach layers complementary standard: SNOMED CT for procedures and clinical findings, LOINC for observations and measurements, HL7 FHIR for exchange and modeling, and OMOP CDM for large-scale analysis [5,6,7,8,9,10]. This aligns with current initiatives including the WHO–SNOMED collaboration, LOINC’s observation framework, HL7 Vulcan’s FHIR profiles for RWD, and OHDSI’s data standardization efforts [5,6,7,8,9,10].
Traditional medicine adds domain-specific requirements. TM1 in ICD-11 supports optional dual coding for morbidity only—not for mortality [11]. It includes two entity types: disorders and patterns. Coders can record either or both, always with a primary Chapter 01-25 diagnosis [6,11]. These rules let traditional medicine context appear in clinical records without disrupting existing indicators [2,3,4,11].
Moving from records to evidence requires clear handoffs. In FHIR R5, Product-Definition resources represent catalog data, not care events, while Medication, MedicationRequest, and MedicationDispense capture actual prescribing and dispensing [12,13]. For analytics, FHIR identifiers and ingredients connect to OMOP standard concepts through ETL mapping tables [7,8]. Making these boundaries explicit reduces confusion and supports quality monitoring and research.
This roadmap proposes a TM1-centric approach coordinating classification, semantics, exchange, and analytics, using Korea as an example. We aim for minimal disruption by treating TM1 as an optional secondary code and coordinating SNOMED CT, LOINC, FHIR, and OMOP accordingly. ICD-11 (TM1). Classification for morbidity aggregation. Add TM1 as a secondary code with a primary
2. Roles and Handoffs Across Standards
ICD-11 (TM1). Classification for morbidity aggregation. Add TM1 as a secondary code with a primary
SNOMED CT and LOINC. Clinical semantics. SNOMED CT covers procedures like acupuncture and moxibustion, plus clinical findings; LOINC handles laboratory tests and measurements [5,6].
HL7 FHIR R5. Boundary between catalog definitions and care events. MedicinalProductDefinition and related resources serve as catalog or regulatory master data. Care events use Medication, MedicationRequest, and MedicationDispense, capturing ingredient details where needed [12,13].
OMOP CDM. Analytics layer. Load standard concepts for conditions, procedures, and measurements. Represent patterns, complex prescriptions, and procedure attributes initially in Observation or Notes with local vocabularies and relationships, then evolve through community extensions [7,8].
FHIR in Scope Beyond Medications
In this roadmap, FHIR is the exchange and modeling layer for the entire clinical record, not just for medicines. We highlighted product definitions because compounded prescriptions create a real boundary between catalog and care events. For the rest of the record, standard representations for problems, procedures, observations, orders, reports, and documents are used. TM1 is kept alongside the primary diagnosis either as a paired entry or through multiple coding in the same field. Local terminology services can supply value sets and simple maps between ICD-11 TM1, and SNOMED CT when needed. The OMOP handoff remains an ETL mapping step, not a one-to-one conversion [5,6,7,8,12,13,14].
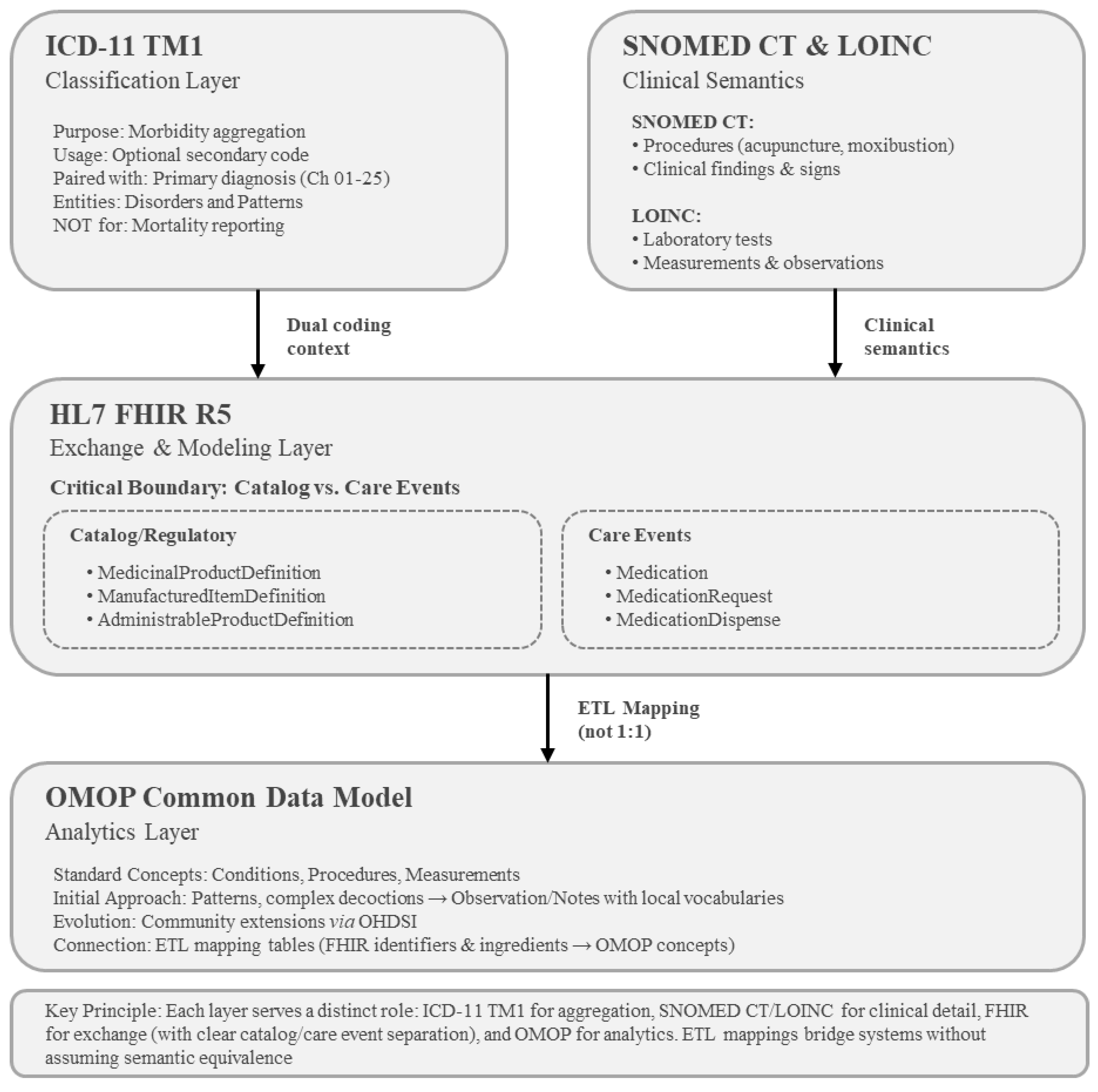
Figure 1.
Roles and handoffs among ICD-11 TM1, SNOMED CT and LOINC, HL7 FHIR R5, and OMOP CDM. The roadmap has four layers: ICD-11 TM1 for morbidity classification, SNOMED CT and LOINC for clinical semantics, HL7 FHIR R5 for exchange and modeling, and OMOP CDM for analytics. Within FHIR, a key boundary operates catalog/regulatory master dataset from clinical care events separately. The procedure of Figure 1 shows data transfer through ETL processes that bridge FHIR components to OMOP standard concepts. Mapping tables connect the systems without assuming one-to-one equivalence, preserving unmapped content for quality monitoring.
Figure 1.
Roles and handoffs among ICD-11 TM1, SNOMED CT and LOINC, HL7 FHIR R5, and OMOP CDM. The roadmap has four layers: ICD-11 TM1 for morbidity classification, SNOMED CT and LOINC for clinical semantics, HL7 FHIR R5 for exchange and modeling, and OMOP CDM for analytics. Within FHIR, a key boundary operates catalog/regulatory master dataset from clinical care events separately. The procedure of Figure 1 shows data transfer through ETL processes that bridge FHIR components to OMOP standard concepts. Mapping tables connect the systems without assuming one-to-one equivalence, preserving unmapped content for quality monitoring.
3. TM1 Entity Choices: Disorder and Pattern
4. Manufactured Products and Extemporaneous Prescriptions: Scope and Limits in FHIR
Authorized manufactured herbal products map well to FHIR Product-Definition resources [12]. Compounded prescriptions prepared in clinical settings usually have no national product master entry; therefore, they should be modeled as Medication-based care events with explicit ingredients and strengths. When codes don’t exist, record the text with provenance. For analysis, ETL mapping tables that link FHIR identifiers and ingredients to OMOP standard concepts and drug-strength entries should be maintained. Keep a local formulary for traceability over time [7,13,14].
5. A Korea-Based Case: Why and When
Why. Improved international comparability with minimal disruption, stratified quality and safety signals, stronger RWE and AI readiness through alignment with SNOMED CT, LOINC, FHIR, and OMOP, and lower transition cost by building co-coding literacy early.When. Consider TM1 as an optional secondary code during the next KCD revision. Enforce EHR validation that blocks TM1-only saves. Mortality coding remains unchanged.
6. Site-Level Preparation Checklist
Policy and controls. Primary equals Chapters 01 to 25. Secondary equals TM1. Include the phrase “morbidity only, not for mortality.” Block TM1-only saves.Exemplar library. Provide recommended co-coding examples for common scenarios, such as low back pain and insomnia.
Semantics and catalogs. Apply SNOMED CT and LOINC to procedures, findings, and tests, and maintain change logs. Build FHIR R5 product catalogs. Use Medication for prescribing and dispensing.
Analytics. Start with minimal OMOP loading. Track unmapped rates and the data quality. Plan community contributions for botanicals and related content.Community pathway. Engage OHDSI and SNOMED International for extension requests and content development.

Table 1.
Ten-point checklist for preparing TM1 co-coding and cross-standard mapping at healthcare sites.
Table 1.
Ten-point checklist for preparing TM1 co-coding and cross-standard mapping at healthcare sites.
| No. | Category | Action Item | Details |
| 1 | Policy framework | Establish dual-coding policy | Define TM1 as optional secondary code for morbidity only; primary diagnosis must be from ICD-11 Chapters 01–25 |
| 2 | Regulatory compliance | Document mortality exclusion | Include explicit policy text: “TM1 for morbidity only, not for mortality reporting” |
| 3 | EHR validation | Implement technical controls | Configure EHR system to block saves with TM1 code only; require paired primary diagnosis |
| 4 | Clinical guidance | Create exemplar co-coding library | Develop and distribute recommended coding examples for common scenarios (e.g., low back pain with TM1 disorder/pattern, insomnia with sleep-wake disorder) |
| 5 | Semantic interoperability | Map to SNOMED CT and LOINC | Apply SNOMED CT for TM procedures (acupuncture, moxibustion) and clinical findings; use LOINC for laboratory tests and measurements |
| 6 | Product cataloging | Build FHIR R5 product catalogs | Implement MedicinalProductDefinition for authorized manufactured herbal products; maintain change logs |
| 7 | Prescribing workflow | Use Medication resources for care events | Model compounded prescriptions as Medication-based events with ingredient-level detail; avoid Product-Definition resources for non-cataloged items |
| 8 | Analytics preparation | Establish minimal OMOP CDM loading plan | Develop mapping tables to connect FHIR identifiers and components to OMOP concepts; begin loading conditions, procedures, and measurements |
| 9 | Data quality monitoring | Trace vocabulary gaps and unmapped rates | Trace vocabulary gaps (patterns, prescriptions, procedure attributes) initially stored in Observation or Notes; document local terms used |
| 10 | Community engagement | Participate in standards development | Cooperate with OHDSI on OMOP extensions, SNOMED International on content requests, and national terminology bodies on botanical and TM vocabularies |
Note: Implementation depends on governance approval and EHR readiness. In case of Korea, adoption timing aligns with the next KCD revision cycle.
7. Risks and Limitations, and How to Handle Them
TM1 implementation faces several practical challenges. The biggest risk is that it can be misused as primary diagnoses, which could not follow WHO guidelines and distort mortality statistics. To prevent this risk, EHR verification rules enforcing dual coding as well as clear institutional policies are essential. Second, vocabulary gaps for patterns and procedure attributes induce another problem. Observation or Notes with local vocabularies and proposed extensions can be used to solve this problem on a limited basis. These workarounds should be documented and proposed to terminology communities for future standardization. Third, compounded prescriptions complicate medication tracking because these individualized preparations do not match conventional pharmaceutical databases. Recording them as Medication events with local formulary support provides a practical solution, particularly when paired with published OMOP CDM mapping tables that enable multi-site research. Finally, updating TM modules like TM2 and ASU (Ayurveda, Siddha, Unani) cause uncertainty. Proper application for TM1 should be the first challenge and keeping documentation in accordance with WHO updates and national guidelines would help manage this change up to date.
8. Outlook and Scope
This paper addressed TM1 adoption rationale, stakeholder roles, coding boundaries between traditional and conventional medicine, and preparation requirements. Technical details—code lists, FHIR specifications, OMOP mappings, quality metrics—report in separate documentation
9. Conclusion
This roadmap demonstrates how TM1 dual coding can work alongside SNOMED CT, FHIR, and OMOP using real clinical data. Adding TM1 as an optional secondary code for morbidity—timed to a future KCD revision—offers a practical path toward strong clinical context and better international comparability without disrupting current reimbursement or mortality workflows. The distinction between FHIR catalog/regulatory data and Medication care events, combined with ETL-based mapping to OMOP, enables effective progress on research and AI applications for traditional medicine.
Funding
This research was supported by the Regional Innovation System & Education (RISE) program through the Gangwon RISE Center, funded by the Ministry of Education (MOE) and the Gangwon State (G.S.), Republic of Korea. (2025-RISE-10-005).
Data Availability Statement
No primary data were generated or analyzed in this study. All information supporting the roadmap framework is available within the paper.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. International Classification of Diseases 11th Revision (ICD-11): 2025 update and Traditional Medicine Chapter (TM1); WHO: Geneva, 2025; Available online: https://icd.who.int/browse/2025-01/mms/en (accessed on 2025 Nov 11).
- Harrison, JE; Weber, S; Jakob, R; Chute, CG. ICD-11: an international classification of diseases for the twenty-first century. BMC Med Inform Decis Mak 2021, 21 (Suppl 6), 206. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. ICD-11 Reference Guide; WHO: Geneva, 2022; Available online: https://icdcdn.who.int/icd11referenceguide/en/html/index.html (accessed on 2025 Jan 27).
- Bai, X; Guo, J; Zhang, M; Wang, Y; Li, N. Quantifying coding integrity and reliability of ICD-11 MMS for rare disease registration: a case study of the Chinese rare disease catalogue. BMC Med Inform Decis Mak. 2025, 25(1), 440. [Google Scholar] [CrossRef] [PubMed]
- Fung, KW; Xu, J; Brear, H; Lane, A; Lau, M; Wong, A; et al. Promoting interoperability between SNOMED CT and ICD-11: lessons learned from the pilot project mapping between SNOMED CT and the ICD-11 Foundation. J Am Med Inform Assoc. 2024, 31(8), 1631–7. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K; Dou, D; Hoshino, T; Saito, M. Development and implementation of ICD-11 traditional medicine chapter “1st International Symposium on Kampo Medicine”. Tradit Kampo Med. 2022, 9(2), 132–3. [Google Scholar] [CrossRef]
- Observational Health Data Sciences and Informatics. OMOP Common Data Model v5.4 specifications. Available online: https://ohdsi.github.io/CommonDataModel/ (accessed on 2025 Nov 15).
- Hripcsak, G; Duke, JD; Shah, NH; et al. Observational Health Data Sciences and Informatics (OHDSI): Opportunities for Observational Researchers. Stud Health Technol Inform. 2015, 216, 574–578. [Google Scholar] [PubMed]
- Vorisek, CN; Lehne, M; Klopfenstein, SAI; et al. Fast healthcare interoperability resources (FHIR) for interoperability in health research: systematic review. JMIR Med Inform. 2022, 10(7), e35724. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, JM; Robinson, D; Della Mea, V; et al. Semantic alignment between ICD-11 and SNOMED CT. Stud Health Technol Inform. 2015, 216, 790–794. [Google Scholar] [PubMed]
- World Health Organization. ICD-11 Reference Guide; WHO: Geneva, 2022; Available online: https://icdcdn.who.int/icd11referenceguide/en/html/index.html (accessed on 2025 Nov 11).
- Health Level Seven International. HL7 FHIR Release 5 (R5): MedicinalProductDefinition resource. Available online: https://hl7.org/fhir/R5/medicinalproductdefinition.html (accessed on 2025 Dec 10).
- Health Level Seven International. HL7 FHIR Release 5 (R5): Medication module. Available online: https://hl7.org/fhir/R5/medications-module.html (accessed on 2025 Dec 20).
- McDonald, CJ; Huff, SM; Suico, JG; Hill, G; et al. LOINC, a universal standard for identifying laboratory observations: a 5-year update. Clin Chem. 2003, 49(4), 624–633. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



