
Submitted:
27 January 2026
Posted:
28 January 2026
You are already at the latest version
Abstract
Background/Objectives: The L5–S1 segment presents unique characteristics that make surgical access challenging in minimally invasive spine surgery (MISS) procedures. Variability in the spatial relationships of bony and neural structures may restrict some approaches. However, few studies have so far combined radiologic analysis with ca-daveric dissection to characterize the morphology relevant to transforaminal and extra-foraminal L5-S1 approaches. The purpose of the study is to characterize anatomical and radiological features of the lumbosacral region that influence planning and execution of MISS procedures. Methods: Twelve Thiel-embalmed donor bodies underwent CT im-aging (L4–S2) followed by posterior dissection. Bony landmarks were used to obtain bilateral anatomical measurements. Qualitative anatomical analysis included iliolumbar ligament morphology and extraforaminal access feasibility. CT-based morphometrics included L5 transverse process (TP) dimensions; maximal and minimal distances between L5 TP and sacral ala; extraforaminal area bounded by L5 TP, L5 facet (zygapophyseal) joint, and sacral ala; iliac crest–based approach angle to the L5-S1 disc; minimal distance between this approach vector and the ventral ramus of the L5 spinal nerve; facet an-gulation and iliac crest height. Results: No left–right asymmetry was detected. Except for L5 TP length, all anatomical measurements obtained in the donor bodies differed sig-nificantly between sexes. A direct disc access with a uniportal endoscopic working tube was feasible in 25% of cases. On CT analysis, the maximal and minimal distances between the TP and sacral ala were 11.1 (4.0)mm and 5.6±2.9mm, with a mean extraforaminal area of 202.0±45.9mm². Neither gender nor sacral dysmorphism significantly influenced these imaging parameters. The mean approach angle was 35.2±5.0°, and an extraforaminal corridor to L5–S1 disc was feasible in 75% of donated bodies. The median minimal distance between the approach vector and the ventral ramus of the L5 spinal nerve was 5.0 (7.1)mm, with frequent overlap. Conclusions: The L5–S1 segment shows substantial interindividual morphologic variability, compromising the feasibility of transforaminal and extraforaminal MISS approaches, and highlighting the need for individualized preoperative planning, neural identification and/or bony resection to create a safe working corridor.
Keywords:
L5–S1 segment
; lumbosacral anatomy
; extraforaminal
; transforaminal
; minimally inva-sive spine surgery
; endoscopic surgery
; iliolumbar ligament
1. Introduction
Commonly occurring degenerative spinal conditions such as disc herniation, disc degeneration and/or spondylolisthesis occur most frequently in the lower lumbar spine, particularly at the L4-L5 and L5-S1 levels [1,2]. The L5-S1 segment has distinct anatomical and biomechanical characteristics that may contribute to these degenerative diseases. Positioned at the transition between the mobile lumbar spine and the rigid sacrum, this segment is subject to substantial compressive and shear forces. It typically exhibits the greatest intervertebral disc height, more coronally oriented facet (zygapophyseal) joints, and stabilizing structures such as the iliolumbar ligament, contributing to its unique functional profile [1,2,3,4,5].
Surgical management of lumbar degenerative disease and spinal instability involves decompression and/or fusion. When surgery is required, the aforementioned features may influence the choice of surgical technique and approach [6,7]. For the L5-S1 level, posterior approaches remain widely used due to surgeon familiarity and versatility. The ongoing demand to maximize clinical outcomes while minimizing morbidity has driven rapid expansion of minimally invasive spine surgery (MISS), including tubular and endoscopic techniques, as they may reduce iatrogenic muscle injury, blood loss and post-operative pain, promoting faster recovery [8,9,10,11,12]. However, L5-S1 access can be particularly challenging due to lumbosacral and iliac morphologic variability. For instance, the iliac crest height, foraminal dimensions, and orientation of bony structures may restrict working angles and limit safe instrument trajectories, especially during transforaminal (TF) and extraforaminal (EF) approaches [13,14].
To the best of our knowledge, few studies have specifically analyzed the L5-S1 morphologic features in the surgical setting [14,15,16]. This study aims to characterize anatomical and radiological features of the L5–S1 segment and to identify factors relevant for planning and execution of MISS procedures.
2. Donor Information, Materials and Methods
This study was conducted at the Unit of Anatomy, Department of Biomedicine, Faculty of Medicine of the University of Porto (FMUP), Portugal. Ethical approval was granted by the Ethics Committee of FMUP/RISE Health in 23 September 2025 (365/CEFMUP-RISE Health/2025).
Twelve donor bodies preserved using Thiel’s embalming method were included in the present study [17]. All donor bodies derived from donation with informed consent, written and signed by the donor himself, in accordance with Portuguese Decree-Law number 271/99. Age and gender were retrieved from donation records. Donor bodies were excluded if they presented unexplained deformities or signs of previous dissection/surgery involving the lumbosacral region.
Previous to anatomical dissection, computed tomography (CT) scans of the lumbosacral spine (L4-S2) were obtained for all donor bodies. All predefined measurements were obtained bilaterally (totalizing 24 segments) and independently recorded by two observers.
2.1. Anatomical Dissection
A standard midline posterior approach to the lumbosacral spine was performed to expose the posterior elements from L4 to S2. Care was taken to preserve bony structures as well as the native position of ligamentous and neurovascular components. Four predefined anatomical landmarks (points A-D) were identified (Figure 1):
- Point A: base of the L5 transverse process (TP)
- Point B: tip of the L5 TP
- Point C: inferior tip of L5 inferior articular process
- Point D: medial margin of the iliac crest at the level of point C
Using these landmarks, four distances were measured (A-B, C-D, A-C and B-D) using a ruler graduated in millimeters.
Qualitative assessments included the characterization of the iliolumbar ligament anatomy from a posterior view, regarding its attachment points, number of bands and shape. Moreover, EF direct access to the L5-S1 disc using a uniportal endoscopic working tube (Joimax® Tessys, REF WTS176575; 170mm length; 6.5mm inner / 7.5mm outer diameter) was tested, to assess potential anatomical barriers.
2.2. Imaging Analysis
Using Sectra® IDS7 software, five morphometric parameters were defined and measured on CT scan images (Figure 2, Figure 3, Figure 4 and Figure 5):
- L5-TP: length of the L5 TP (axial plane; Figure 2)
- MaxTP-sacrum and minTP-sacrum: maximum and minimum distance from the inferior border of the L5 TP to the superior border of the sacral ala, respectively, (coronal plane intersecting the L5 TP center; Figure 3)
- EF-area: EF area bounded superiorly by the L5 TP, medially by the facet joint and inferiorly by the sacral ala (coronal plane; Figure 4)
- Approach angle (AA): angle between the midline and the vector (V) tangential to the iliac crest that crosses the most anterior point of the L5-S1 disc space (axial plane at IVD space; Figure 5)
- MinL5-V: minimum distance from the ventral ramus of the L5 spinal nerve to V (axial plane; Figure 5)
Further analysis included evaluation of facet joint angulation, measured as the angle between a sagittal line and a line crossing the L5-S1 zygapophyseal joint (Figure 6), assessment of iliac crest height (using coronal CT cuts and considering the classification described by Nagasse and colleagues [18]), and a qualitative assessment of sacral morphology (based on the characteristics described by Miller and Routt [19]).
2.3. Statistical Analysis
Statistical analyses were performed using IBM SPSS® Software, version 27. Results for continuous variables are expressed as medians (IQR [interquartile range]) or means (±SD [standard deviation]) for non-normal or normal variable distribution, respectively. Categorical variables were expressed as absolute and relative frequencies. Paired Student’s t-tests, Mann-Whitney U test and Spearman’s correlation coefficients were applied to analyse continuous variables. Interobserver reliability was assessed using intraclass correlation coefficients (ICC) and their 95% confidence intervals. ICC estimates were based on a mean rating (k = 2), absolute agreement, and two-way mixed-effects model [20]. P-values less than 0.05 were considered statistically significant.
3. Results
Twelve donor bodies were included (8 male, 4 female), all Caucasian and of Portuguese nationality, with a mean age at death of 75±9 years. Inter-rater reliability ranged from 0.816 to 0.995. No statistically significant left-right asymmetry was evident between measurements.
3.1. Anatomical Dissection Results
No statistically significant sex-related differences were observed for L5-TP (A-B distance). In contrast, all other measurements showed statistically significant differences between female and male donor bodies:
- -
- A-B distance: 16±6 mm (female) vs. 15±2 mm (male); p=0.702
- -
- C–D distance: 16±5 mm (female) vs. 10±3 mm (male); p=0.003
- -
- A–C distance: 18±4 mm (female) vs. 27±6 mm (male); p<0.001
- -
- B–D distance: 21±6 mm (female) vs. 29±7 mm (male); p=0.01
From a posterior view, the iliolumbar ligament originated from L5 bilaterally in all donor bodies. Morphologically, it consisted either of a single (n=18) or a double band (n=6), displaying a rectangular (n=16) or fan-shaped (n=8) configuration.
Direct access to the L5-S1 disc using an EF endoscopic approach was assessed with a uniportal endoscopic working tube. This access was feasible in 25% of attempts (n=6/24), with no gender difference (p=0.545).
3.2. Imaging Results
Imaging analysis showed an equal distribution of nondysmorphic (n=6) and dysmorphic (n=6) sacra
CT-based L5-TP (Figure 2) closely matched the anatomical A-B distance, with no significant differences (p=0.144). However, the values obtained in the CT analysis were slightly higher.
The maxTP-sacrum distance (Figure 3) was 11.1(4.0)mm, consistently located in the second quarter of the L5 TP (from its base). The mean minTP-sacrum distance (Figure 3) was 5.6±2.9mm, always near the L5 TP tip. No statistically significant differences were observed between nondysmorphic and dysmorphic upper sacral morphology (p=0.662 and p=0.498, respectively).
The mean CT-defined EF-area (Figure 4) was 202.0±45.9mm2. No statistically significant difference was found between nondysmorphic and dysmorphic sacral morphologies (p=0.540): 193.8±53.2 and 212.0±38.7mm2, respectively.
The mean AA (Figure 5) was 35.2±5.0°. An EF vector (V) tangential to the iliac crest that crosses the most anterior point of the L5-S1 disc space defined a workable corridor to the L5-S1 disc in 75% of the cases (18/24 sides). These cases had significantly greater AA (29.9±3° vs 37.2±4°; p=0.02) and despite not statistically significant, larger TP to sacrum distances, greater EF-areas, and increased minL5-V values were found. However, in 44% (8/18) of cases with a workable corridor on CT based on AA the distance to the ventral ramus of the L5 spinal nerve was inferior to 5mm.
The median minL5-V distance was 5.0(7.1) mm, with no statistically significant gender (p=0.788) or sacral morphology (p=0.429) variation. This parameter was zero in 8 out of 24 cases (33%), meaning direct overlap between the vector V and the ventral ramus of the L5 spinal nerve.
The mean L5-S1 facet joints angulation was 51.4±10.8º, with no statistically significant difference between cases in which EF access was feasible and those in which it was not (p=0.597). Iliac crest height was graded 3 to 7, with 58% of cases (7/12) grading 6 or 7. Further analysis evaluated the correlation between iliac crest height and AA – Spearman’s ρ = –0.465, p = 0.150.
4. Discussion
This study provides an integrated anatomical and radiological characterization of the lumbosacral junction relevant to posterior TF and EF access using MISS techniques. Although prior studies have highlighted the challenges of L5–S1 segment access due to iliac crest, sacral and facet morphology [13,14,21,22], few have combined cadaveric dissection and imaging analysis [23,24].
Regarding dissection data, there was considerable gender-related variation, with no side-to-side asymmetry. The C-D distance, which reflects the spatial relationship between the L5 inferior articular facet and the iliac crest, was greater in females (p=0.003), whereas the A-C and B-D vertical distances were greater in males. These differences may reflect sexual dimorphism in stature and pelvic morphology [25,26,27,28]. From a surgical standpoint, such variations may influence instrument trajectory and available working space.
Qualitative assessment of iliolumbar ligament and endoscopic access provides useful information. Regarding the iliolumbar ligament anatomy, our findings closely align with results from Dabrowski and Ciszek [29], and may help surgeons in preventing iatrogenic injury, which may compromise lumbosacral stability. The relatively low direct accessibility (25%) to the L5-S1 disc using a uniportal endoscopic working tube further underscores the need for detailed preoperative planning. The angulation of the intervertebral disc space, combined with local anatomical bony variations may condition this access and request bony gestures – such as L5 TP resection, sacral ala resection and/or foraminoplasty – or alternative approaches to access the disc space. To overcome some of the limitations imposed by the unique anatomy of L5-S1 segment, a transiliac approach has been described [23,24,30]. Notably, in a cadaveric study, Sousa and colleagues demonstrated that L5-S1 transiliac intraforaminal lumbar interbody fusion is a feasible surgical technique, which allows both a more centrally placed interbody cage in the coronal plane without compromising the anterior position in the lateral plane, and also the integrity of the major anatomic structures at risk [24]. In this context, Sousa and collaborators recently shown the outcomes of 5 patients submitted to a transiliac endoscopic-assisted L5-S1 intraforaminal lumbar interbody fusion with good clinical results as well as high fusion rates at 12 months [31]. However, they stated that this surgical technique may present some complications, such as late-onset dysesthesia of the ipsilateral lower limb (10 to 14 days after surgery) [31].
The CT-based component of the study adds further nuance to the anatomical data analysis. Neither gender nor sacral morphology statistically significantly influenced the measurements. Nonetheless, male donor bodies presented greater values for maxTP-sacrum, min-TP-sacrum, EF-area and minL5-V, while females had greater AA, which may reflect sexual dimorphism in stature and pelvic morphology, as previously suggested by the results from anatomical dissection analysis.
The EF-area, defined using bony landmarks easily identifiable during surgical procedures, is relevant for EF access and decompression procedures, and clinically relevant in scenarios such as far-out syndrome [32,33]. This area exhibited wide variability (123-287mm2), which may reflect interindividual anatomical variations and/or induced degenerative changes.
The mean AA value and L5-S1 facet joints angulation are comparable to values from other anatomical series [14]. According to CT-based planning, the EF corridor to the L5-S1 disc was feasible in 75% of donor bodies segments. This value widely differs from the cadaveric findings for a direct EF endoscopic access (feasible in only 25% of cases), which may highlight the need for multiplanar CT analysis to understand the local morphology. Potential barriers to L5-S1 EF approach might include iliac crest and facet joint morphology, and L5 TP to sacrum distances. The moderate negative correlation between iliac crest height and AA, reinforces the iliac crest as a frequent limiting factor when planning EF trajectories, similar to previous works [21,22]. Contrarily, facet joint orientation showed no statistically significant differences between donor segments in which EF access was feasible and those in which it was not. Authors believe facet degeneration, with osteophytosis and hypertrophy, may impede access more than facet angulation. Therefore, partial resection of the isthmus, partial facetectomy and/or foraminoplasty may improve access during EF approaches.
The MinL5-vector distance was generally short, with median values around 5.0(7.1)mm. In 33% of the cases the projected vector directly collided with the ventral ramus of the L5 spinal nerve. This finding reinforces the need for meticulous neural identification and protection. Considering that most interbody cages measure close to 10mm in width, even minor deviations between planned and real trajectories may place the spinal nerve at risk.
Collectively, this work provides quantitative insight into the geometric constraints of the L5–S1 surgical corridor for TF and EF approaches, which may be useful for the management of foraminal and EF disc herniations, foraminal stenosis and far-out syndrome, revision cases (to avoid scar tissue) and/or lumbar interbody fusion procedures. Considerable interindividual variability in parameters that define the L5–S1 surgical working corridor, together with the close proximity of the L5 spinal nerve, reinforce the need for individualized preoperative analysis, customized approaches and real-time neuromonitoring (when applicable). Combining the values of maxTP-sacrum, minTP-sacrum and AA, and the dimensions of commonly used MISS (including endoscopic) working tubes, these findings suggest that bony gestures, or even the choice for alternative approaches, will frequently be necessary to optimize procedures and minimize iatrogeny.
We acknowledge some limitations and strengths to the present study. As with all cadaveric studies, tissues may not accurately replicate the physiological and biomechanical properties of living specimens, as death and/or embalming procedures can alter tissue consistency, potentially affecting dissection and measurement accuracy (as suggested by non-significant differences in L5 TP measurements between cadaveric and imaging analysis). However, our measurements were based in fixed bony landmarks which may barely be affected by death and/or preservation methods. Moreover, examiners were trained in the local anatomy and independent measurements were performed, with a good to excellent inter-rater reliability. Furthermore, we measured some parameters previously reported in the literature, and the results obtained were similar to this data, which unequivocally provides robustness to our results. Another limitation concerns the small sample of Portuguese Caucasian and older donor bodies, limiting generalizability and statistical power to detect subtle differences. Finally, the absence of accurate donor height and weight prevented reliable correlation of morphological variability with these anthropometric parameters. A major strength of this study is the combined use of CT imaging and direct anatomical measurements, allowing validation of imaging-based assumptions with high-fidelity Thiel-preserved tissue. Bilateral measurements and independent observers further reinforced reliability, a fact corroborated by ICC values in the good–excellent range. Future studies should expand sample size, incorporate three-dimensional reconstructions and navigation tools, and correlate anatomical features with clinical outcomes of L5–S1 segment MISS procedures.
5. Conclusions
In conclusion, the lumbosacral junction exhibits considerable variability in bony and neural morphology, yet consistent anatomical relationships can be defined using reproducible landmarks. The integration of imaging and cadaveric findings, and the recognition of segment specificities, enhances understanding of the L5–S1 surgical corridor and may assist surgeons in planning safer, more effective minimally invasive access routes.
Author Contributions
Conceptualization, MRS, ARP, PAP; Methodology, MRS, PAP; Validation, VV, MDM; Formal analysis, MRS, ARP, HA, PAP; Investigation, MRS, DMD, APR; Data curation, MRS, DMD; Writing—original draft preparation, MRS; Writing—review and editing, ARP, HA, MDM, PAP; Supervision, VV, MDM. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by National Funds through FCT—Fundação para a Ciência e a Tecnologia, I.P., within CINTESIS, R&D Unit (reference UIDB/4255/2020) and within the scope of the project RISE, Associated Laboratory (reference LA/P/0053/2020).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and was approved by the Ethics Committee of the FMUP/RISE Health in 23 September 2025 (approval 365/CEFMUP-RISE-Health/2025).
Informed Consent Statement
All donor bodies derived from body donation with informed consent, written and signed by the donor (Portuguese Decree-Law number 271/99).
Acknowledgments
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Results from such research can potentially increase mankind’s overall knowledge and contribute to the improvement in patient care. Therefore, these donors and their families deserve our highest gratitude. The authors also wish to thank the Unit of Anatomy Technicians Filipe Silva and Rui Garcez for their technical assistance.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AA | Approach angle |
| CT | Computer tomography |
| EF | Extraforaminal |
| EF-area | EF area bounded superiorly by the L5 TP, medially by the facet joint and inferiorly by the sacral ala |
| MaxTP-sacrum | Maximum distance from the inferior border of the L5 TP to the superior border of the sacral ala |
| MinL5-V | minimum distance from the ventral ramus of the L5 spinal nerve to V |
| MinTP-sacrum | Minimum distance from the inferior border of the L5 TP to the superior border of the sacral ala |
| MISS | Minimally invasive spine surgery |
| TF | Transforaminal |
| TP | Transverse process |
| V | Vector tangential to the iliac crest that crosses the most anterior point of the L5-S1 disc space |
References
- Saleem, S.; Aslam, H.M.; Rehmani, M.A.; Raees, A.; Alvi, A.A.; Ashraf, J. Lumbar disc degenerative disease: disc degeneration symptoms and magnetic resonance image findings. Asian Spine J 2013, 7, 322–334. [Google Scholar] [CrossRef]
- Sabnis, A.B.; Chamoli, U.; Diwan, A.D. Is L5-S1 motion segment different from the rest? A radiographic kinematic assessment of 72 patients with chronic low back pain. Eur Spine J 2018, 27, 1127–1135. [Google Scholar] [CrossRef]
- Mahato, N.K. Facet dimensions, orientation, and symmetry at L5-S1 junction in lumbosacral transitional States. Spine (Phila Pa 1976) 2011, 36, E569–E573. [Google Scholar] [CrossRef]
- Pinho, A.R.; Pereira, P.A.; Leite, M.J.; Santos, C.C.; Vaz, R.P.; Dulce Madeira, M. The Surgical Vascular Anatomy of the Lower Lumbar Arteries and Its Implications in Minimally Invasive Spine Surgery: A Cadaveric Study. Int J Spine Surg 2022, 16, 631–637. [Google Scholar] [CrossRef]
- Relvas-Silva, M.; Matos Sousa, J.M.; Dias, D.; Pinto, B.S.; Sousa, A.; Fonseca, J.; Loureiro, M.; Pinho, A.R.; Veludo, V.; Serdoura, A.; et al. Prone Position for Preoperative Planning in Lumbar Endoscopic and Minimally Invasive Fusion Procedures: Insights From a Magnetic Resonance Imaging Study. Int J Spine Surg 2025, 19, 179–187. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Phan, K.; Malham, G.; Seex, K.; Rao, P.J. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg 2015, 1, 2–18. [Google Scholar] [CrossRef]
- Reid, P.C.; Morr, S.; Kaiser, M.G. State of the union: a review of lumbar fusion indications and techniques for degenerative spine disease. J Neurosurg Spine 2019, 31, 1–14. [Google Scholar] [CrossRef]
- Chan, A.K.; Bydon, M.; Bisson, E.F.; Glassman, S.D.; Foley, K.T.; Shaffrey, C.I.; Potts, E.A.; Shaffrey, M.E.; Coric, D.; Knightly, J.J.; et al. Minimally invasive versus open transforaminal lumbar interbody fusion for grade I lumbar spondylolisthesis: 5-year follow-up from the prospective multicenter Quality Outcomes Database registry. Neurosurg Focus 2023, 54, E2. [Google Scholar] [CrossRef]
- Hu, X.; Yan, L.; Jin, X.; Liu, H.; Chai, J.; Zhao, B. Endoscopic Lumbar Interbody Fusion, Minimally Invasive Transforaminal Lumbar Interbody Fusion, and Open Transforaminal Lumbar Interbody Fusion for the Treatment of Lumbar Degenerative Diseases: A Systematic Review and Network Meta-Analysis. Global Spine J 2024, 14, 295–305. [Google Scholar] [CrossRef]
- Kou, Y.; Chang, J.; Guan, X.; Chang, Q.; Feng, H. Endoscopic Lumbar Interbody Fusion and Minimally Invasive Transforaminal Lumbar Interbody Fusion for the Treatment of Lumbar Degenerative Diseases: A Systematic Review and Meta-Analysis. World Neurosurg 2021, 152, e352–e368. [Google Scholar] [CrossRef]
- Morgenstern, C.; Morgenstern, R. Full-Percutaneous Trans-Kambin Lumbar Interbody Fusion With a Large-Footprint Interbody Cage. Global Spine J 2025, 15, 3101–3112. [Google Scholar] [CrossRef]
- Pholprajug, P.; Kotheeranurak, V.; Liu, Y.; Kim, J.S. The Endoscopic Lumbar Interbody Fusion: A Narrative Review, and Future Perspective. Neurospine 2023, 20, 1224–1245. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.T.; Wei, S.T.; Tseng, C.; Ou, S.W.; Sun, L.W.; Chen, C.M. Transforaminal Endoscopic Lumbar Discectomy for L5-S1 Disc Herniation With High Iliac Crest: Technical Note and Preliminary Series. Neurospine 2020, 17, S81–S87. [Google Scholar] [CrossRef]
- Sousa, J.M.; Serrano, A.; Nave, A.; Mascarenhas, V.; Nogueira, P.; Gamelas, J.; Guimaraes Consciencia, J. Transforaminal Endoscopic Approach to L5S1: Imaging Characterization of the Lower Lumbar Spine and Pelvis for Surgical Planning. World Neurosurg 2023, 175, e809–e817. [Google Scholar] [CrossRef]
- Ju, C.I.; Kim, P.; Seo, J.H. Full-Endoscopic J-Shaped Transforaminal L5 Nerve Decompression in Bertolotti Syndrome. Neurospine 2024, 21, 1131–1136. [Google Scholar] [CrossRef]
- Shen, S.C.; Chen, H.C.; Tsou, H.K.; Lin, R.H.; Shih, Y.T.; Huang, C.W.; Tang, C.L.; Chen, H.T.; Chang, C.C.; Tzeng, C.Y. Percutaneous endoscopic lumbar discectomy for L5-S1 disc herniation based on image analysis and clinical findings: A retrospective review of 345 cases. Medicine (Baltimore) 2023, 102, e32832. [Google Scholar] [CrossRef]
- Eisma, R.; Lamb, C.; Soames, R.W. From formalin to Thiel embalming: What changes? One anatomy department’s experiences. Clin Anat 2013, 26, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Nagasse, Y.; Lima, C.J.; Ferreira, J.P.A.; Utino, E.T.; Bergamaschi, J.P.; Defino, H.L.A. Radiographic Study of L5-S1 Transforaminal Endoscopic Access in a Sample from the Brazilian Population. Rev Bras Ortop (Sao Paulo) 2024, 59, e847–e853. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.N.; Routt, M.L., Jr. Variations in sacral morphology and implications for iliosacral screw fixation. J Am Acad Orthop Surg 2012, 20, 8–16. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr Med 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.C.; Park, C.K. Percutaneous Endoscopic Lumbar Discectomy for L5-S1 Disc Herniation: Consideration of the Relation between the Iliac Crest and L5-S1 Disc. Pain Physician 2016, 19, E301–E308. [Google Scholar] [CrossRef] [PubMed]
- Patgaonkar, P.; Datar, G.; Agrawal, U.; Palanikumar, C.; Agrawal, A.; Goyal, V.; Patel, V. Suprailiac versus transiliac approach in transforaminal endoscopic discectomy at L5-S1: a new surgical classification of L5-iliac crest relationship and guidelines for approach. J Spine Surg 2020, 6, S145–S154. [Google Scholar] [CrossRef]
- Osman, S.G.; Marsolais, E.B. Endoscopic transiliac approach to L5-S1 disc and foramen. A cadaver study. Spine (Phila Pa 1976) 1997, 22, 1259–1263. [Google Scholar] [CrossRef]
- Sousa, JM; Ribeiro, H; Gamelas, J; Consciencia, JG. Transiliac endoscopic assisted iLIF: a cadaveric study. Coluna/Columna 2023, 22, e268180. [Google Scholar] [CrossRef]
- Fischer, B.; Mitteroecker, P. Covariation between human pelvis shape, stature, and head size alleviates the obstetric dilemma. Proc Natl Acad Sci U S A 2015, 112, 5655–5660. [Google Scholar] [CrossRef]
- Saluja, S.; Tigga, S.R.; Das, S.S.; Thakur, A. Determination of Sexual Dimorphism of the Human Sacrum Based on Receiver Operating Characteristic Curve Analysis of Morphometric Parameters. Cureus 2023, 15, e38629. [Google Scholar] [CrossRef]
- Standring, S.E.-i.-C., Gray’s Anatomy—The Anatomical Basis of Clinical Practice. 42nd ed. 2021.
- Vleeming, A.; Schuenke, M.D.; Masi, A.T.; Carreiro, J.E.; Danneels, L.; Willard, F.H. The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat 2012, 221, 537–567. [Google Scholar] [CrossRef] [PubMed]
- Dabrowski, K.; Ciszek, B. Anatomy and morphology of iliolumbar ligament. Surg Radiol Anat 2023, 45, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Osman, S.G.; Sherlekar, S.; Malik, A.; Winters, C.; Grewal, P.K.; Narayanan, M.; Gemechu, N. Endoscopic trans-iliac approach to L5-S1 disc and foramen - a report on clinical experience. Int J Spine Surg 2014, 8. [Google Scholar] [CrossRef]
- Sousa, J.M.; Silva, J.L.; Gamelas, J.; Guimaraes Consciencia, J. Transiliac Endoscopic-Assisted L5S1 Intraforaminal Lumbar Interbody Fusion: Technical Considerations and Potential Complications. World Neurosurg 2023, 178, e741–e749. [Google Scholar] [CrossRef]
- Ha, J.S.; Sakhrekar, R.; Han, H.D.; Kim, D.H.; Kim, C.W.; Kulkarni, S. Unilateral Biportal Endoscopy for L5-S1 Extraforaminal Stenosis (Far Out Syndrome) - Technical Note with Literature Review. J Orthop Case Rep 2024, 14, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Heo, D.H.; Sharma, S.; Park, C.K. Endoscopic Treatment of Extraforaminal Entrapment of L5 Nerve Root (Far Out Syndrome) by Unilateral Biportal Endoscopic Approach: Technical Report and Preliminary Clinical Results. Neurospine 2019, 16, 130–137. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Lumbosacral region dissection (posterior view). For demonstration purposes the zygapophyseal joint was opened on the left side. A: base of the L5 transverse process (TP); B: tip of the L5 TP; C: tip of L5 inferior articular process; D: medial margin of the iliac crest at the level of point C.
Figure 1.
Lumbosacral region dissection (posterior view). For demonstration purposes the zygapophyseal joint was opened on the left side. A: base of the L5 transverse process (TP); B: tip of the L5 TP; C: tip of L5 inferior articular process; D: medial margin of the iliac crest at the level of point C.
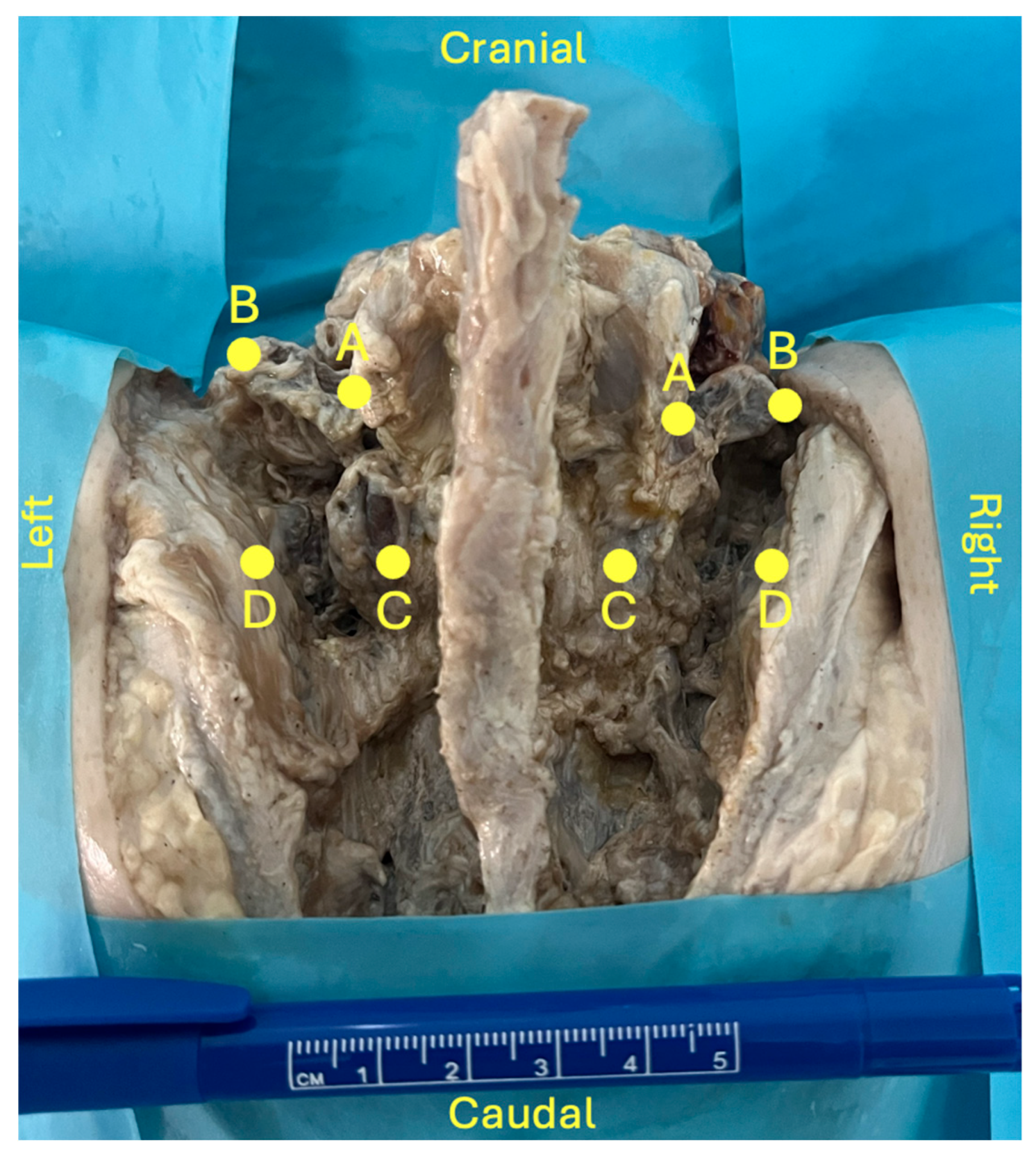
Figure 2.
Lumbar spine CT – axial plane; *: L5 transverse process; yellow line: L5 transverse process length.
Figure 2.
Lumbar spine CT – axial plane; *: L5 transverse process; yellow line: L5 transverse process length.
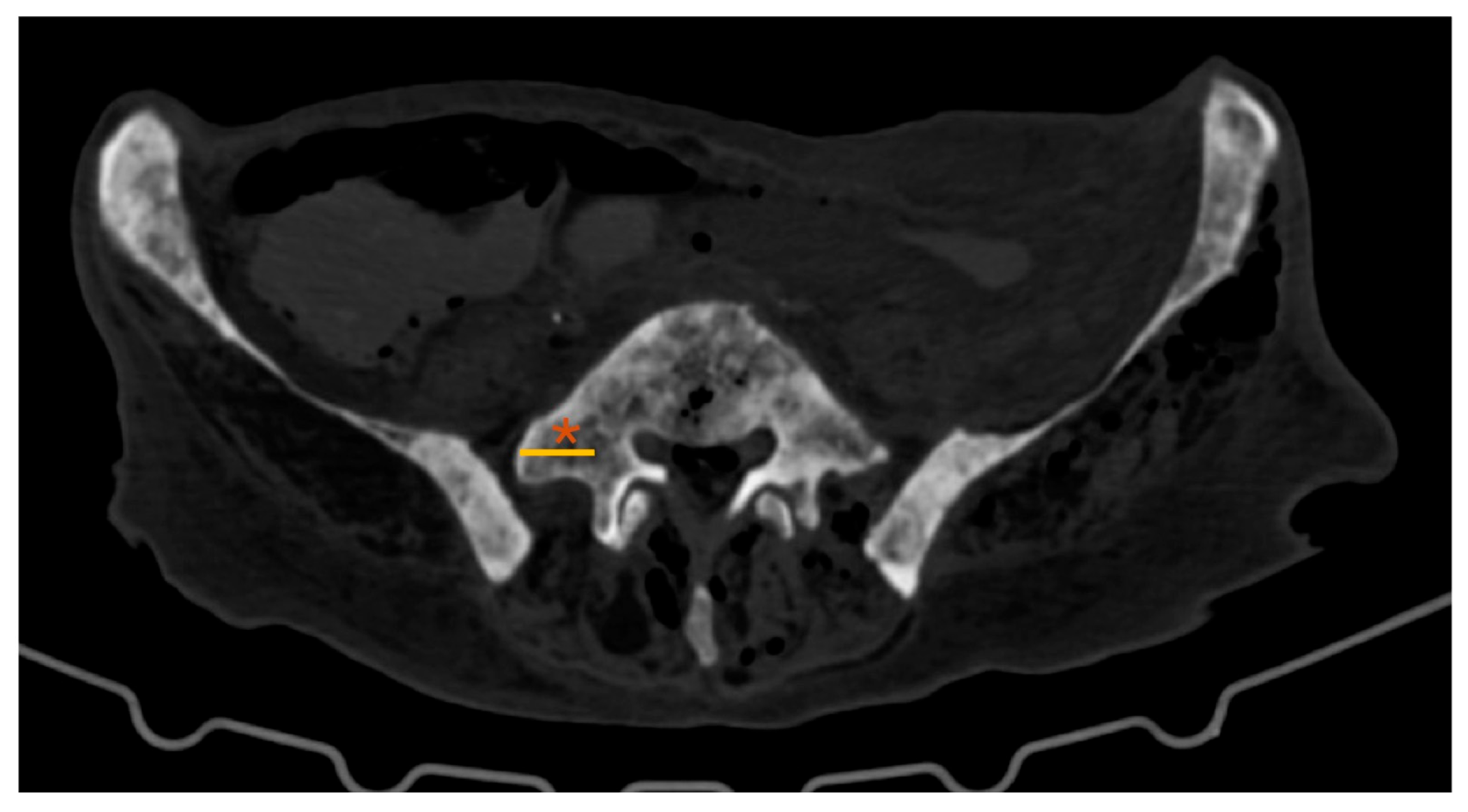
Figure 3.
Lumbar spine CT – coronal plane; *: L5 transverse process; arrow: sacral ala; dotted yellow line: maxTP-sacrum (maximum distance from the inferior border of the L5 transverse process to the superior border of the sacral ala); solid yellow line: minTP-sacrum (minimum distance from the inferior border of the L5 transverse process to the superior border of the sacral ala).
Figure 3.
Lumbar spine CT – coronal plane; *: L5 transverse process; arrow: sacral ala; dotted yellow line: maxTP-sacrum (maximum distance from the inferior border of the L5 transverse process to the superior border of the sacral ala); solid yellow line: minTP-sacrum (minimum distance from the inferior border of the L5 transverse process to the superior border of the sacral ala).
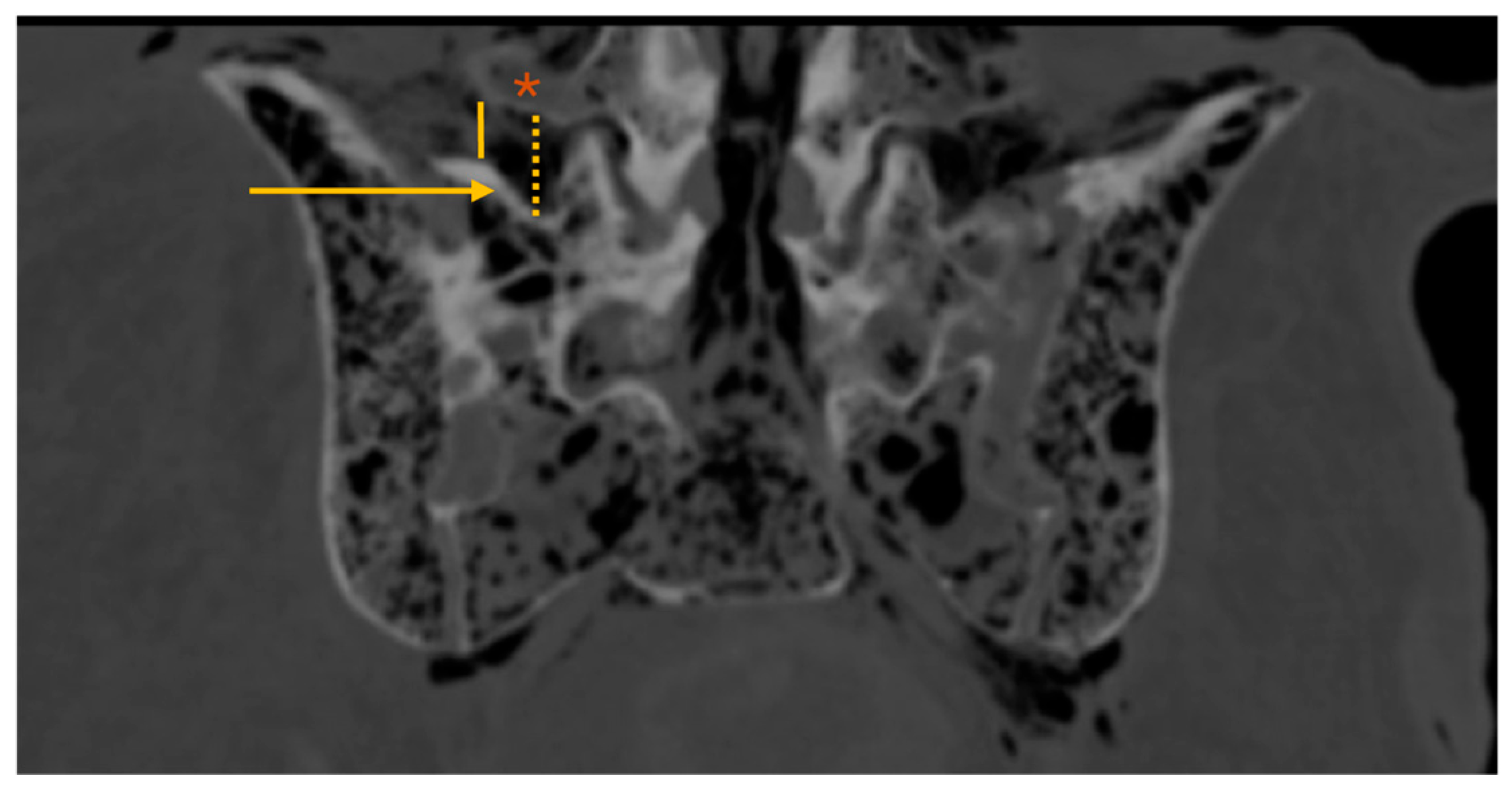
Figure 4.
Lumbar spine CT – coronal plane; *: L5 transverse process; #facet joint; arrow: sacral ala; blue area: EF-area (extraforaminal area bounded superiorly by the L5 transverse process, medially by the facet joint and inferiorly by the sacral ala).
Figure 4.
Lumbar spine CT – coronal plane; *: L5 transverse process; #facet joint; arrow: sacral ala; blue area: EF-area (extraforaminal area bounded superiorly by the L5 transverse process, medially by the facet joint and inferiorly by the sacral ala).
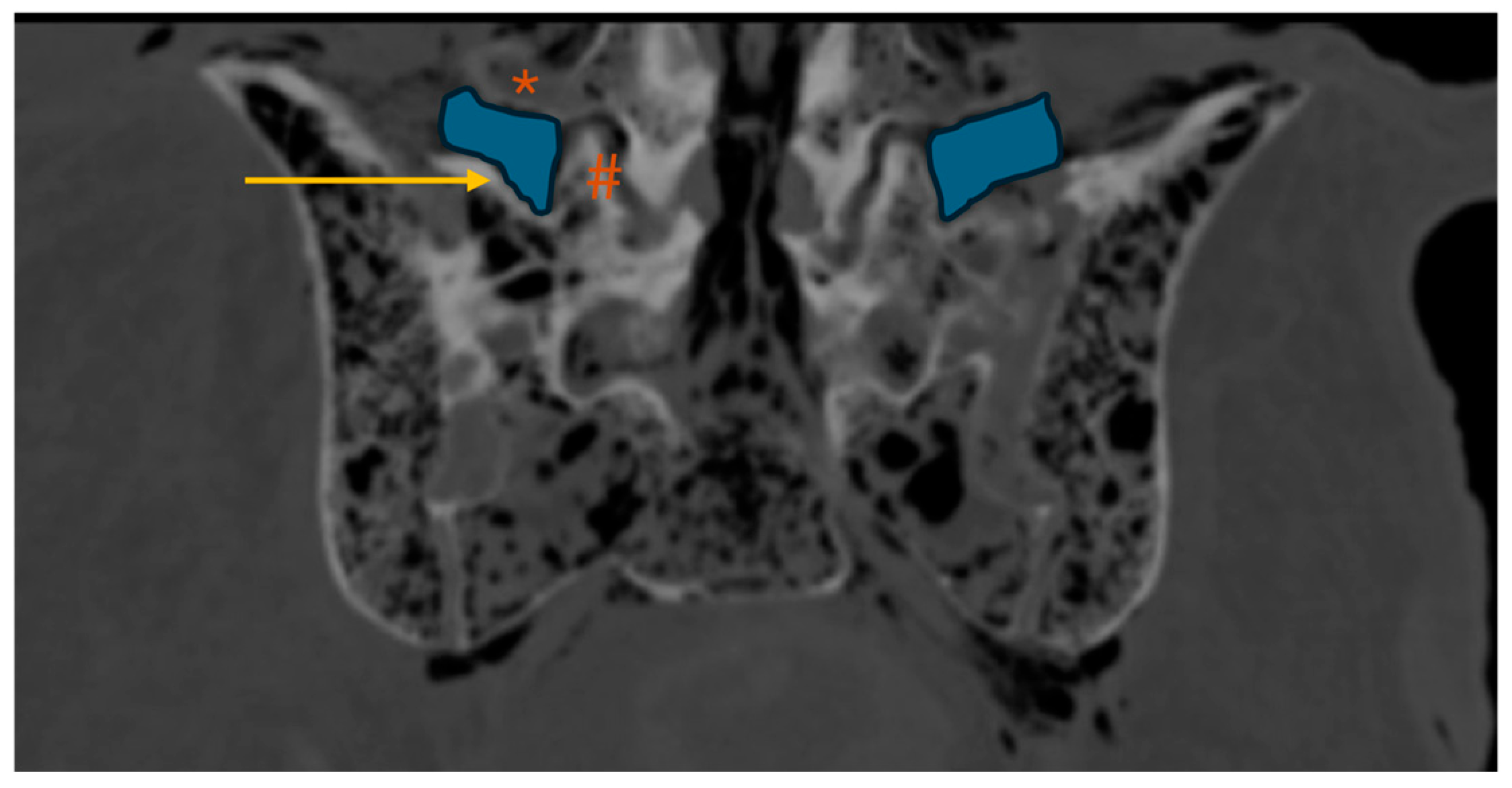
Figure 5.
Lumbar spine CT – axial plane; *: ventral ramus of the L5 spinal nerve; dotted yellow lines: marking of the approach angle (AA; angle between the midline and the vector (V) tangential to the iliac crest that crosses the most anterior point of the L5-S1 disc space; solid orange line: minL5-V (minimum distance from the ventral ramus of the L5 spinal nerve to vector line).
Figure 5.
Lumbar spine CT – axial plane; *: ventral ramus of the L5 spinal nerve; dotted yellow lines: marking of the approach angle (AA; angle between the midline and the vector (V) tangential to the iliac crest that crosses the most anterior point of the L5-S1 disc space; solid orange line: minL5-V (minimum distance from the ventral ramus of the L5 spinal nerve to vector line).
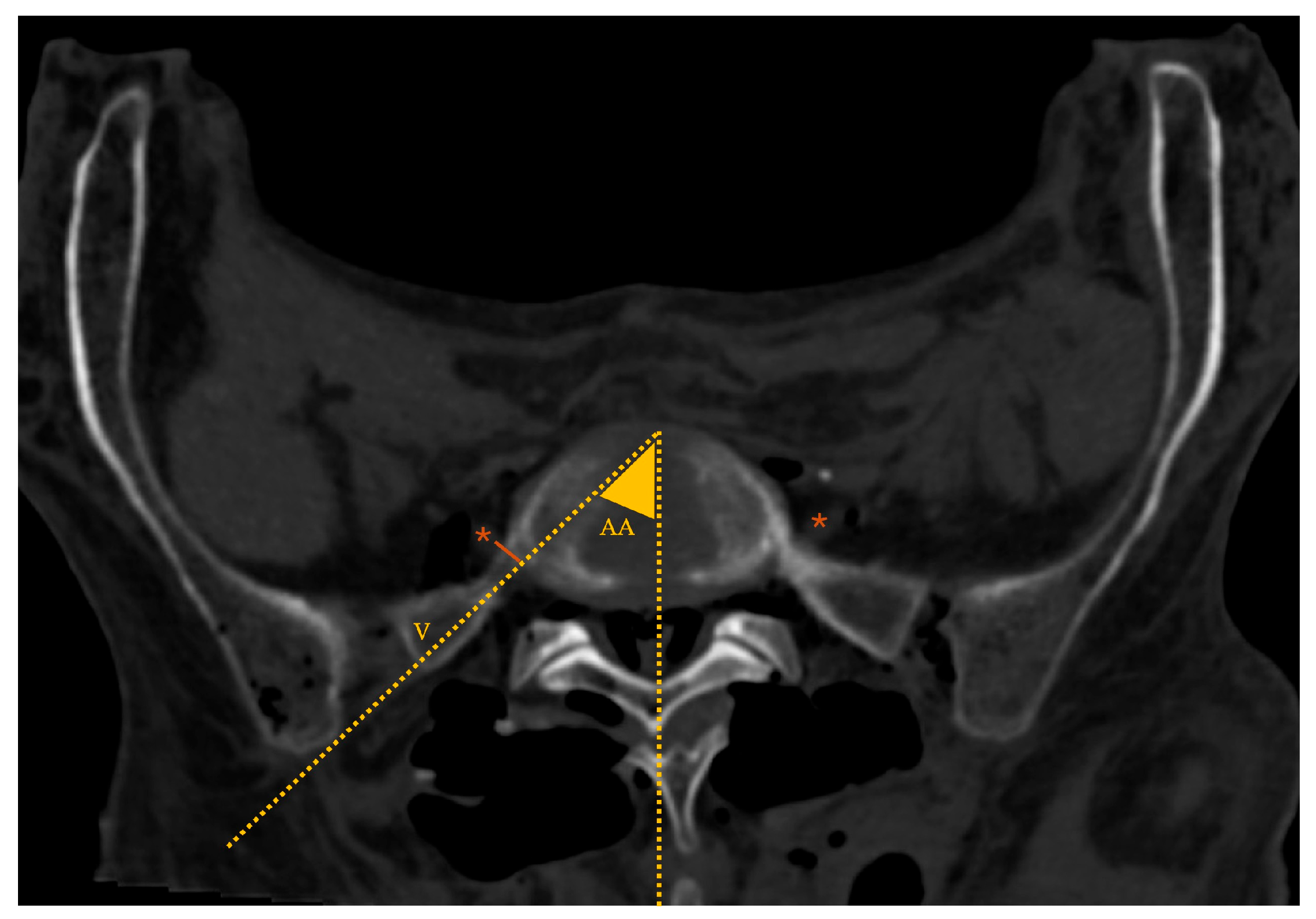
Figure 6.
Axial CT of the lumbar spine; circle: zygapophyseal joint; FA: facet (zygapophyseal) joint angulation, as defined by the yellow solid lines.
Figure 6.
Axial CT of the lumbar spine; circle: zygapophyseal joint; FA: facet (zygapophyseal) joint angulation, as defined by the yellow solid lines.
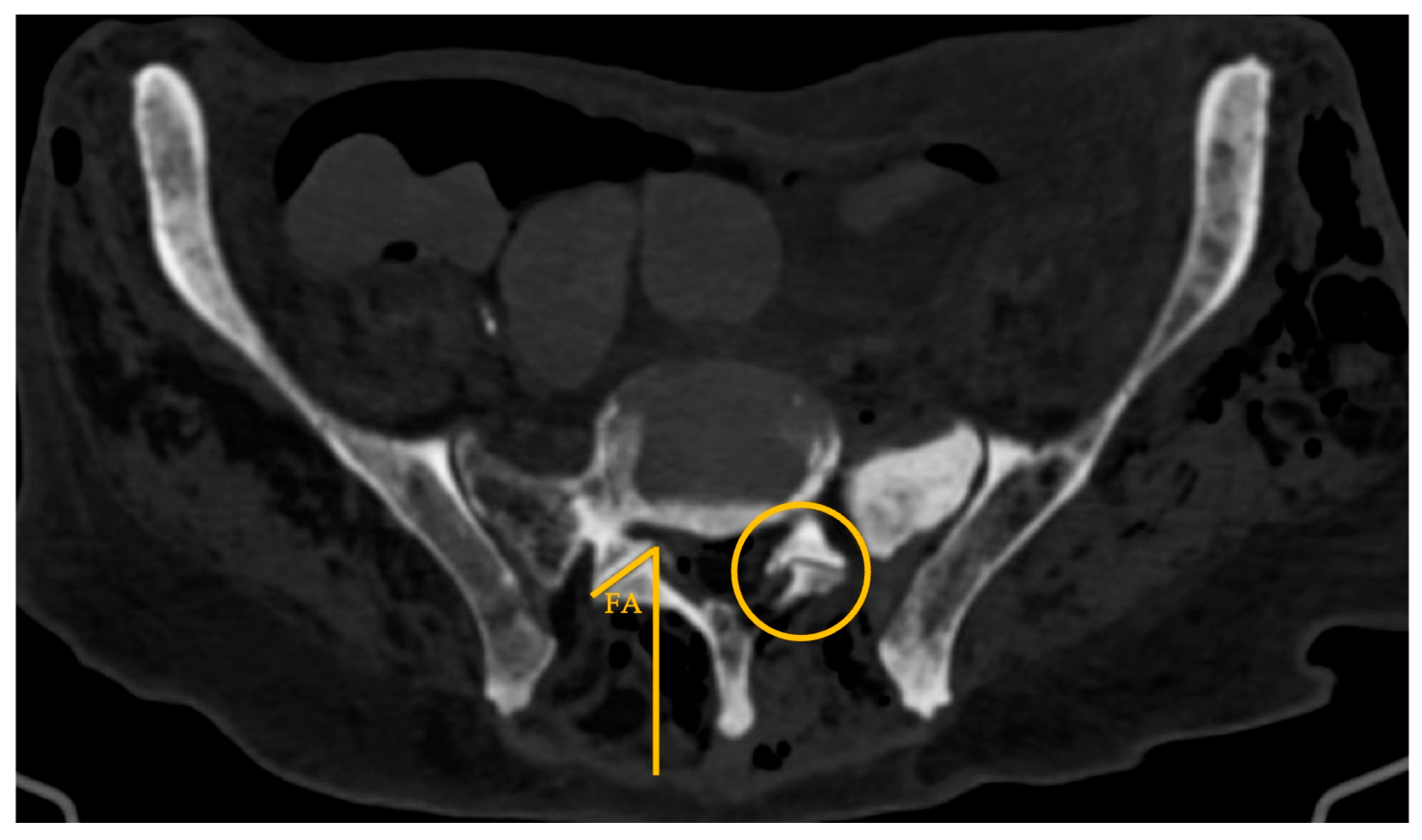

Table 1.
Analysis of CT scan parameters (global results and by gender).
| Total | Female | Male | P-value Female vs Male |
|
|---|---|---|---|---|
| L5-TP (mm; mean ± SD) | 17.8±3.1 | 19.4±3.1 | 16.8±2.8 | 0.197 |
| MaxTP-sacrum (mm; median (IQR)) | 11.1 (4.0) | 9.9 (3.9) | 11.4 (4.6) | 0.315 |
| MinTP-sacrum (mm; mean ± SD) | 5.6±2.9 | 4.8±1.2 | 6.0±3.6 | 0.498 |
| EF-area (mm2; mean ± SD) | 202.0+45.9 | 180.0±9.8 | 214.8±54.2 | 0.540 |
| AA (º; mean ± SD) | 35.2±5.0 | 38.8±4.8 | 33.2±4.0 | 0.563 |
| MinL5-V (mm; median (IQR)) | 5.0 (7.1) | 2.7 (9.3) | 5.0 (7.2) | 0.788 |
Detailed variables characterization is available in the “Donor Information, Materials and Methods” section. AA – approach angle; EF – extraforaminal; Max – maximum; Min – minimum; SD – standard deviation; TP – transverse process; V – vector.
Table 2.
Analysis of CT scan parameters regarding sacral morphology.
| Nondysmorphic | Dysmorphic | p-value | |
|---|---|---|---|
| L5-TP (mm; mean ± SD) | 16.0±3.0 | 15.3±2.4 | 0.673 |
| MaxTP-sacrum (mm; median (IQR)) | 11.0 (4.6) | 11.1 (5.5) | 0.662 |
| MinTP-sacrum (mm; mean ± SD) | 5.0±3.1 | 6.2±2.8 | 0.498 |
| EF-area (mm2; mean ± SD) | 193.8±53.2 | 212.0±38.7 | 0.540 |
| AA (º; mean ± SD) | 34.4±4.5 | 36.2±5.8 | 0.563 |
| MinL5-V (mm; median (IQR)) | 6.0 (10.9) | 2.6 (6.1) | 0.429 |
Detailed variables characterization is available in the “Donor Information, Materials and Methods” section. AA – approach angle; EF – extraforaminal; Max – maximum; Min – minimum; SD – standard deviation; TP – transverse process; V – vector.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



