
Submitted:
23 January 2026
Posted:
27 January 2026
You are already at the latest version
Abstract
Background: This retrospective study compared the safety and efficacy of phacoemulsification performed with topical Cyclopentolate (Cykloftyal) versus a standard intracameral mydriatic and anesthetic combination (Mydrane) in patients undergoing RayOne EMV intraocular lens implantation.
Materials and Methods: Medical records of 60 eyes (30 patients per group) were analyzed. Group A received topical Cyclopentolate and intracameral lidocaine, whereas Group B received intracameral Mydrane alone for mydriasis and anesthesia. Data on pupil diameter (at the start and end of surgery), procedure duration, and postoperative visual acuity at various distances were extracted and compared.
Results: There was no statistically significant difference in surgical duration between Group A (7.05 min) and Group B (6.70 min; p=0.35), nor in postoperative visual acuity at any distance. However, the initial pupil diameter was significantly larger in the topical group (7.31±1.12 mm) than in the intracameral group (6.19±0.92 mm; p=0.04). Two months postoperatively, approximately 67% of patients in both groups reported spectacle independence for daily activities.
Conclusions: Topical Cyclopentolate is a safe and effective alternative to intracameral mydriasis, providing significantly wider initial pupil dilation while maintaining comparable surgical efficiency. Additionally, the RayOne EMV lens demonstrated favorable outcomes in functional spectacle independence.
Keywords:
cataract surgery
; mydriasis
; intracameral
; cyclopentolate
; enhanced monofocal IOL
; phacoemulsification
Background
Visual function is essential for independent daily functioning and decision-making. Due to its complex anatomy and high metabolic activity, the visual system is particularly vulnerable to degenerative and pathological processes that may impair vision. The most common reversible cause of visual impairment in individuals over 60 years of age is lens opacification, known as cataract [1]. In adults, cataracts most commonly develop as a result of age-related degenerative processes [2]. Based on the location of the predominant lens opacity, age-related cataract can be classified into several subtypes, with nuclear cataract being the most prevalent. Less frequently, opacities are located in the cortex or the posterior lens capsule, which are seen mainly in patients taking steroids long-term [3].
Following a cataract diagnosis and determination of the need for surgical treatment, patients are eligible for phacoemulsification. This process involves several tests, including an individual calculation of the implanted lens power. A critical stage is the appropriate preparation of the patient to ensure the safe and efficient performance of the procedure. One of the key factors determining the safety and ease of the surgery is a sufficiently wide pupil in the operated eye, which provides convenient access to the cloudy lens and insight into the deeper structures of the eyeball [4]. To achieve sufficient mydriasis, a number of preparations are used in the form of ophthalmic drops and intracameral solutions containing substances with anesthetic and pupil-dilating effects. The concept of intracameral mydriasis, first introduced to streamline the preoperative process, has become an established alternative to traditional topical regimens [4]. Currently, various methods are available in clinical practice to ensure stable pupil dilation in the operated eye. In addition to the above-mentioned chemical substances, if necessary, mechanical devices such as retractors or a Malyugin ring may be used to widen access to the lens [5]. Despite the constant development and application of new methods, there are cases in which the operating conditions are very demanding and the safe performance of the procedure requires great skill and experience of the surgeon.
Phacoemulsification, a surgical procedure for cataracts that involves removing the cloudy lens with ultrasound and implanting an artificial lens in its place, is the most commonly performed procedure worldwide [3]. It is widely performed in most ophthalmology departments, does not require long-term hospitalization, and patients are usually discharged the same day with recommendations for regular check-ups and the use of several eye drops. Cataract remains the leading cause of reversible blindness globally. According to the IAPB (International Agency for the Prevention of Blindness) Vision Atlas, developed in partnership with the World Health Organization, over 20 million cataract surgeries are performed annually worldwide [6]. Ophthalmological societies precisely define the algorithms for pre-, intra-, and postoperative procedures and the appropriate use of drugs to ensure pupil dilation and protect patients from postoperative complications. One of the mydriatic drugs approved for use is Cyclopentolate (Cykloftyal 10 mg/ml; 5 ml, Verco, Warsaw, Poland) at a concentration of 10 mg/ml in the form of eye drops, while standardized intracameral combinations (Mydrane) have demonstrated proven efficacy in large-scale clinical trials [7].
The gradual aging of society and the simultaneous extension of the period of seniors’ activity create a need for continuous improvement of surgical techniques and materials. Patients’ expectations regarding postoperative visual acuity, rehabilitation time, and the possibility of independence from glasses have contributed to the development of intraocular implants. Standard lenses used in cataract surgery include the most popular monofocal implants. They provide sharp vision at one distance, are free from most of the shortcomings of multifocal lenses, but are associated with the need to use glasses for distance or near vision [8,9,10]. Considering the economic aspect and the possibility of ensuring patients’ independence from glasses during most activities of everyday life, i.e., good functional vision, lenses with extended depth of focus, referred to as monofocal-plus, are gaining increasing recognition in the public healthcare sector. The leader in the group of implants with extended depth of focus is the RayOne EMV (Rayner, Worthing, United Kingdom) lens, introduced in 2020 as the result of collaboration between Professor Graham Barrett and Rayner. By using positive spherical aberrations, they increase optical abilities toward hyperopia, which seems to be important for maintaining stereopsis and thereby affects the level of postoperative patient satisfaction [11].
Material and Methods
Study Design and Ethics: Medical records of patients who underwent cataract surgery were reviewed. All procedures were performed in accordance with the Helsinki Declaration on Human Medical Research and its subsequent amendments, or with comparable ethical standards. All methods were carried out in accordance with applicable guidelines and regulations. Prior to surgery, all patients or their legal guardians provided informed, written consent for cataract phacoemulsification with artificial lens implantation. Our retrospective analysis of patients’ medical records was exempt from Institutional Review Board (IRB) approval.
Surgical Protocol and Grouping: In this retrospective analysis, patients were divided into two groups based on the mydriatic protocol used. In Group A (30 patients, 60 eyes), the protocol involved local administration of 2 drops of Cykloftyal into the conjunctival sac, with a 5-minute interval, approximately 30 minutes before the procedure. To ensure patient comfort and a painless procedure, after measuring pupil width, 0.1 mL of 2% lidocaine solution (Lidocainum Hydrochloricum WZF 2%, Polfa Warsaw, Warsaw, Poland) was administered intracamerally. Group B included 30 patients (60 eyes) who underwent cataract surgery in both eyes using the RayOne EMV lens, with intracameral administration of 0.2 mL of Mydrane (Mydrane 0.2 mg tropicamide + 3.1 mg phenylephrine hydrochloride + 10.0 mg lidocaine hydrochloride, Thea, Clermont-Ferrand, France), without preoperative local application of a mydriatic agent.
Immediately before disinfection of the surgical site and application of the eyelid dilator, all patients received 1 drop (0.05 ml) of Alcaine (proxymetacaine hydrochloride, 5 mg/ml, Alcon, Geneva, Switzerland) topically. During phacoemulsification, a cohesive viscoelastic with a density of 1.4% was used in all patients. To ensure postoperative emmetropia, RayOne EMV intraocular implants were selected to achieve a postoperative refraction as close as possible to zero in all eyes. All calculations for selecting the appropriate intraocular lenses were performed using the Carl Zeiss IOL Master 500. The formulas used were in accordance with the manufacturer’s recommendations: Holladay 1 for axial lengths between 22 and 25 mm. For axial lengths below 22 mm, Hoffer Q was used, and for axial lengths above 25 mm, SRK/T.
Data Collection and Exclusion Criteria: Pupil width was recorded at the start of cataract surgery (at the onset of capsulorhexis) and at completion (during administration of 0.1 mL of Cefuroxime; Aprokam, Thea, Clermont-Ferrand, France). The analysis also included procedure duration and uncorrected visual acuity for distance (UDVA), intermediate (UIVA, 60 cm), and near (UNVA, 40 cm), measured at follow-up visits 2 weeks, 2 months, and 6 months after the procedure. Pupil diameter was calculated as the mean of two perpendicular measurements (horizontal and vertical).
Exclusion criteria included a history of glaucoma, pseudoexfoliative syndrome (PEX), retinal or optic nerve diseases, and allergy to any ingredient in the substances used during standard procedures. The presence of posterior or anterior synechiae or prior ophthalmic surgery (other than cataract surgery in the other eye) also excluded patients from the study groups. The absence of mydriasis after topical preparations at previous visits, which could suggest intraoperative floppy iris syndrome (IFIS) or lens subluxation, was also an exclusion criterion. Although the frequency of IFIS may increase from the population level of about 1-2% to 90% after Tamsulosin use for prostatic hyperplasia, no pharmacological method of achieving stable mydriasis guarantees success.
Statistical Analysis: A descriptive analysis was performed to characterize the study population and verify the collected data. A 95% confidence interval (CI) was used, and the distribution of quantitative variables was assessed. Because the variables followed a normal distribution, they were reported as means and standard deviations (SD). Comparative analysis was performed to evaluate differences between the study groups. The following factors were considered: patient age, preoperative distance visual acuity (pre-opUDVA), duration of surgery, pupil diameter at the beginning and end of the procedure, and visual acuity at individual distances tested at follow-up visits.
Quantitative variables were analyzed with Student’s t-test for independent samples. To assess the clinical relevance of the observed differences, Effect Size was calculated using Cohen’s d. Effect sizes were interpreted using standard criteria: 0.2 indicates a small effect, 0.5 a medium effect, and 0.8 a large effect. Homogeneity of variance was assessed with Levene’s test, and statistical significance was set at p<0.05. All calculations and statistical analyses were performed using IBM SPSS Statistics 26 (Armonk, New York, USA).
Results
The study included 60 patients (120 eyes), comprising 39 males and 21 females, with a mean age of 51.6 (±5.2) years. Baseline characteristics were comparable between the groups; preoperative visual acuity was 0.98±0.57 logMAR in the topical group (Cyclopentolate) and 0.94±0.50 logMAR in the intracameral group (mean difference: 0.04; p=0.71), indicating homogeneity of the study population despite the retrospective design. Descriptive statistics for both groups are presented in Table 1 and Table 2.
Surgical Outcomes: A statistically significant difference in pupil diameter was observed at the onset of capsulorhexis. Patients in the Cyclopentolate group had a significantly larger mean pupil diameter (7.31 ± 1.12 mm) than those in the intracameral group (6.19 ± 0.92 mm). The mean difference was 1.12 mm (p=0.04, 95% CI: -1.43 to -0.81). Notably, the calculated effect size for this parameter was very large (Cohen’s d = 1.09), indicating a strong clinical benefit of the topical preparation (Figure 1).
No statistically significant difference was found in pupil size at the end of the procedure (6.89 ± 0.89 mm vs. 6.78 ± 0.85 mm; p=0.42; Cohen’s d = 0.13) or in surgical duration (7.05 min vs. 6.70 min; p=0.35), with a negligible effect size (Cohen’s d = 0.17). This suggests that although Cyclopentolate provides better initial dilation, both methods enable efficient surgery without prolonging operative time. The comparative analysis is summarized in Table 3.
Visual Acuity: Postoperative visual acuity outcomes were comparable between the two groups at all follow-up intervals (2 weeks, 2 months, and 6 months). Notably, the rate of functional vision was high: at 2 months, 66.4% of patients in Group A and 66.9% in Group B reported complete spectacle independence, requiring no corrective eyewear for daily activities.
Safe and comfortable performance of the procedures for both patients and the surgeon was achieved in all cases in both groups. The level of pupillary dilatation was sufficient to perform an appropriately wide capsulorhexis and to proceed with the subsequent stages of the procedure. In group A, additional viscoelastic was used to stabilize the anterior chamber in 4 cases, and in group B in 3 cases. Both methods of pharmacological mydriasis proved very effective; patients receiving Mydrane, as well as those treated with Cykloftyal, achieved appropriate pupil sizes for surgery. No complaints were reported during the procedures, and pupil dilation was maintained throughout the surgery.
Discussion
Our findings indicate that topical Cyclopentolate provides significantly greater pupil dilation at the onset of capsulorhexis than the intracameral Mydrane regimen (mean difference: 1.12 mm; Cohen’s d = 1.09, p=0.04). This aligns with the meta-analysis by Iftikhar et al. [12], which found that topical regimens generally yielded wider pupils than intracameral protocols alone. However, unlike some previous studies suggesting that wider pupils significantly shorten surgical time, we did not observe a significant difference in procedure duration (p=0.35). This suggests that although Mydrane yields a more constricted pupil, it remains sufficient for experienced surgeons to perform phacoemulsification safely and efficiently without prolonging the operation.
From a clinical workflow perspective, the choice between these two methods involves a trade-off between logistical efficiency and maximal dilation. Intracameral mydriasis (Mydrane) eliminates the need for preoperative drop instillation, potentially streamlining patient flow in high-volume cataract centers and reducing nursing workload, as emphasized by Rouland et al. in their budget impact analysis [13]. Furthermore, intracameral administration significantly reduces systemic exposure to mydriatic agents, thereby minimizing the risk of cardiovascular side effects such as tachycardia or hypertension, which is particularly beneficial in elderly patients with comorbidities [14].
However, our study shows that when maximal mydriasis is prioritized—for example, in eyes with pseudoexfoliation or dense cataracts requiring extensive manipulation—topical Cyclopentolate remains the superior choice for efficacy. Therefore, surgeons might consider a hybrid approach: using intracameral agents for routine cases and reserving topical protocols for complex cases where wider exposure is critical. Long-term follow-up studies confirm that intracameral protocols are safe for the corneal endothelium [15], supporting their routine use.
Regarding visual outcomes, our results confirm the effectiveness of the enhanced monofocal RayOne EMV lens. The high rate of spectacle independence in our cohort is consistent with the optical principles described by Schmid and Borkenstein [11] and aligns with recent clinical data from García-Bella et al., who reported excellent refractive stability and patient satisfaction with this IOL model [16].
Because Mydrane contains 3 active substances, the patient may be statistically more likely to experience intolerance to individual components of the preparation. In such cases, the use of Cyclopentolate may be an effective alternative, allowing the surgeon to safely perform the procedure. At the same time, we must consider the potential side effects of Cycloftyal and exercise special caution when using it in the elderly, who are more susceptible to systemic anticholinergic toxicity. Potential adverse reactions include central nervous system disturbances such as disorientation, ataxia, hallucinations, and behavioral changes, as well as urinary retention or tachycardia.
In 2021, a meta-analysis was published, covering 14 randomized clinical trials that examined the benefits of various methods and drugs to ensure adequate pupil width for cataract surgery [12]. The comparison of intracameral administration of mydriatic substances with local application of drops included an analysis of 8 randomized clinical trials. In 4 studies (739 patients, 757 eyes), where pupil width was assessed at the initiation of capsulorhexis, all authors reported better results with local than intracameral application; however, the mean difference was small (1.06 mm), making it difficult to draw clear conclusions [12]. In an analysis of 5 studies, where pupil width was assessed after the procedure (799 patients, 817 eyes), the results were inconsistent, not providing a clear answer as to which application method would be more effective. The authors reached the same conclusions by analyzing the average procedure time, without clearly indicating a better method [12]. Currently, there are many studies in the scientific literature comparing the efficacy of different methods of achieving mydriasis while maintaining patient comfort [4,7,12].
Some authors note that patient satisfaction after cataract surgery is more closely tied to functional vision and spectacle independence in everyday activities than to maximal near visual acuity measured under test conditions [10].
Limitations of the Study: The present study has several limitations inherent to its retrospective design. First, the sample size (n=60) is relatively small, although the large effect size observed for pupil diameter strengthens the statistical validity of the findings. Second, the study was conducted at a single center, which may limit the generalizability of the results to other surgical settings with different preoperative protocols. Additionally, the analysis was performed at the eye level, which may introduce intra-patient correlation when both eyes from the same individual are included, potentially affecting the independence of observations. Future prospective, randomized studies with larger cohorts are warranted to confirm these findings.
Conclusion
In conclusion, this retrospective analysis shows that although both intracameral (Mydrane) and topical (Cyclopentolate) regimens enable safe and efficient phacoemulsification, topical Cyclopentolate provides significantly greater initial mydriasis. Importantly, the smaller pupil diameter with the intracameral protocol did not result in prolonged operative times or higher complication rates in the hands of an experienced surgeon. Both groups achieved excellent, comparable postoperative visual outcomes, with a high level of reported spectacle independence provided by the enhanced monofocal RayOne EMV intraocular lens. Therefore, topical Cyclopentolate remains a valuable option, particularly for complex cases requiring maximal pupil dilation, whereas intracameral Mydrane offers a streamlined workflow suitable for routine procedures. The choice of mydriatic strategy should be tailored to the specific clinical scenario and logistical needs of the surgical center.
Conflicts of Interest
The authors report no conflicts of interest in this work.
References
- Hashemi H, Hatef E, Fotouhi A, Feizzadeh A, Mohammed K. The prevalence of lens opacities in Tehran: the Tehran Eye Study. Ophthalmic Epidemiol. 2009;16(3):187–192.
- Chen SP, Woreta F, Chang DF. Cataracts: A Review. JAMA. 2025;333(23):2093-2103.
- Moshirfar M, Milner D, Patel BC. Cataract Surgery. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
- Lundberg B, Behndig A. Intracameral mydriatics in phacoemulsification cataract surgery. J Cataract Refract Surg. 2003;29(12):2366–2371.
- Malyugin B. Cataract surgery in small pupils. Indian J Ophthalmol. 2017;65(12):1323-1328.
- International Agency for the Prevention of Blindness. Vision Atlas. Published 2025. Accessed January 5, 2026. https://visionatlas.iapb.org/.
- Labetoulle M, Findl O, Malecaze F, et al. Evaluation of the efficacy and safety of a standardised intracameral combination of mydriatics and anaesthetics for cataract surgery. Br J Ophthalmol. 2016;100(7):976–985.
- Böhm M, Petermann K, Hemkeppler E, Kohnen T. Defocus curves of 4 presbyopia-correcting IOL designs: diffractive panfocal, diffractive trifocal, segmental refractive, and extended-depth-of-focus. J Cataract Refract Surg. 2019;45(11):1625–1636.
- Tandogan T, Son HS, Choi CY, Knorz M, Auffarth G, Knoramnia R. Laboratory evaluation of the influence of decentration and pupil size on the optical performance of a monofocal, bifocal, and trifocal intraocular lens. J Refract Surg. 2017;33(12):808–812.
- Tran DB, Owyang A, Hwang J, Potvin R. Visual acuity, quality of vision, and patient-reported outcomes after bilateral implantation with a trifocal or extended depth of focus intraocular lens. Clin Ophthalmol. 2021;15:403–412.
- Schmid R, Borkenstein AF. Analysis of higher order aberrations in recently developed wavefront-shaped IOLs. Graefes Arch Clin Exp Ophthalmol. 2022;260(2):609–620.
- Iftikhar M, Abariga SA, Hawkins BS, et al. Pharmacologic interventions for mydriasis in cataract surgery. Cochrane Database Syst Rev. 2021;5(5):CD012830.
- Rouland JF, Korobelnik JF, Daien V, et al. Budget impact model of Mydrane®, a new intracameral injectable used for intra-operative mydriasis, from a UK hospital perspective. BMC Ophthalmol. 2018;18(1):104.
- Davey K, Chang B. Systemic exposure to intracameral vs topical mydriatic agents: in cataract surgery. Clin Ophthalmol. 2019;13:811–819.
- Behndig A, Lundberg B. Intracameral mydriatics in phacoemulsification cataract surgery – a 6-year follow-up. Acta Ophthalmol. 2013;91(3):243–246.
- García-Bella J, Burgos-Blasco B, Vidal-Villegas B, Garzón N, Villanueva C, García-Feijoo J. Visual and refractive outcomes after bilateral implantation of an enhanced monofocal intraocular lens: prospective study. J Cataract Refract Surg. 2024;50(6):585-590.
Figure 1.
Comparison of pupil diameter at the onset of capsulorhexis between the Topical (Cykloftyal) and Intracameral (Mydrane) groups. The topical group demonstrated significantly better mydriasis (p=0.04; Cohen’s d = 1.09). The box represents the interquartile range, the horizontal line indicates the median, and the whiskers show the range.
Figure 1.
Comparison of pupil diameter at the onset of capsulorhexis between the Topical (Cykloftyal) and Intracameral (Mydrane) groups. The topical group demonstrated significantly better mydriasis (p=0.04; Cohen’s d = 1.09). The box represents the interquartile range, the horizontal line indicates the median, and the whiskers show the range.
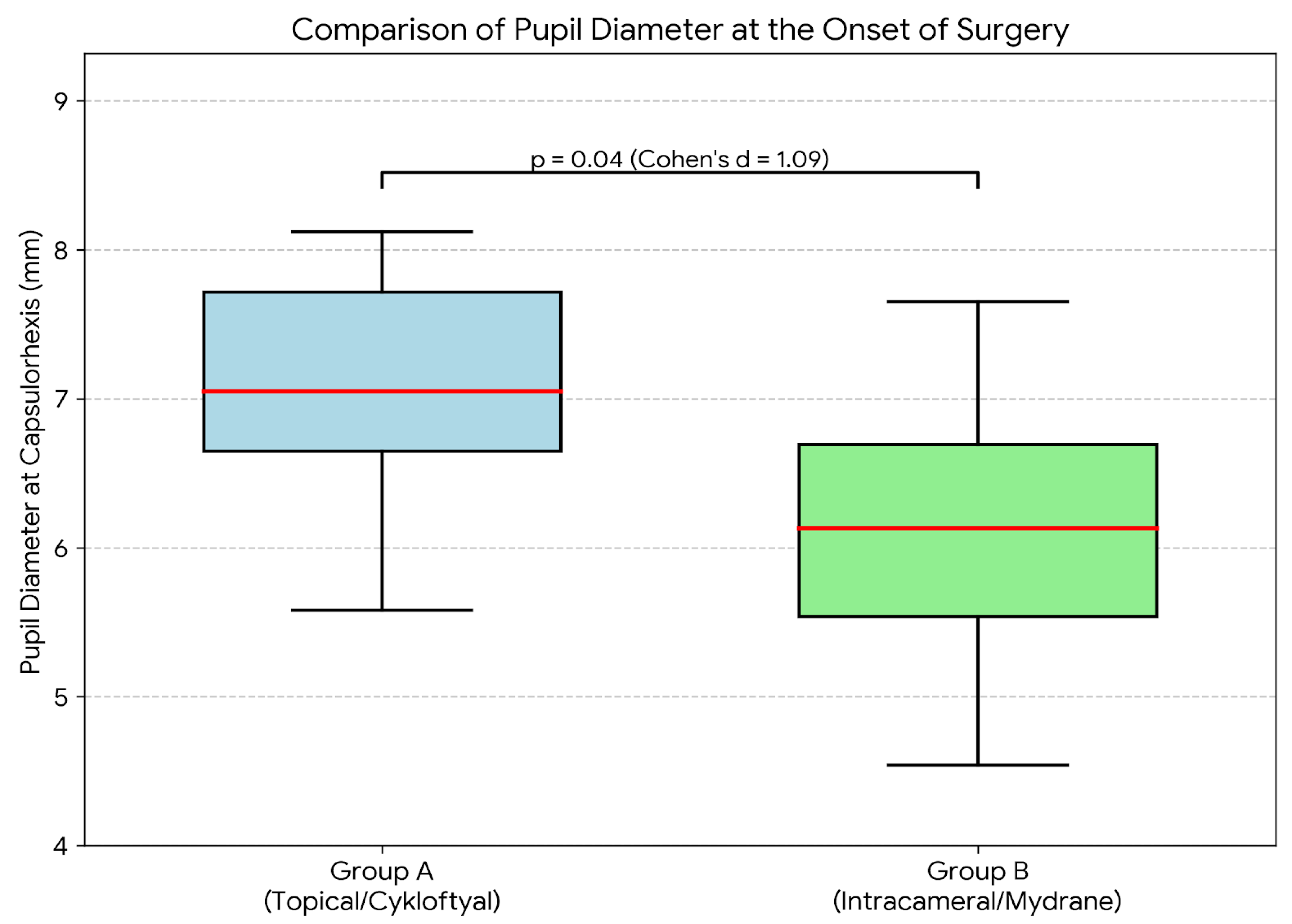

Table 1.
Descriptive statistics of group A.
| Parameter | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|
| Pre-op UDVA (logMAR) | 0.30 | 2.30 | 0.98 | 0.57 |
| Surgical Duration [min] | 4.00 | 10.00 | 07.05 | 2.00 |
| Pupil diameter at the beginning [mm] | 4.54 | 7.65 | 6.19 | 0.92 |
| Pupil diameter at the end [mm] | 4.10 | 7.95 | 6.89 | 0.89 |
Abbreviations: UDVA, Uncorrected Distance Visual Acuity; logMAR, Logarithm of the Minimum Angle of Resolution; Pre-op, Preoperative; SD, Standard Deviation.
Table 2.
Descriptive statistics of group B.
| Parameter | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|
| Pre-op UDVA (logMAR) | 0.20 | 2.30 | 0.94 | 0.50 |
| Surgical duration [min] | 4.00 | 10.00 | 6.70 | 2.12 |
| Pupil diameter at the beginning [mm] | 5.58 | 8.12 | 7.31 | 1.12 |
| Pupil diameter at the end [mm] | 5.11 | 7.78 | 6.78 | 0.85 |
Abbreviations: UDVA, Uncorrected Distance Visual Acuity; logMAR, Logarithm of the Minimum Angle of Resolution; Pre-op, Preoperative; SD, Standard Deviation.
Table 3.
Comparison of the significance of differences between groups.
| Parameter | Mean Difference | 95% CI of Difference (Lower - Upper) | P-value |
|---|---|---|---|
| Pre-op UDVA | 0.04 | -0.16 to 0.23 | 0.71 |
| Surgical duration [min] | 0.35 | -0.40 to 1.01 | 0.35 |
| Pupil diameter at the beginning [mm] | -1.12 | -1.43 to -0.81 | 0.04 |
| Pupil diameter at the end [mm] | 0.11 | -0.22 to 0.41 | 0.42 |
Abbreviations: CI, Confidence Interval; UDVA, Uncorrected Distance Visual Acuity; Pre-op, Preoperative.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



