Submitted:
24 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Shock remains a major cause of morbidity and mortality in critical care despite substantial advances in monitoring and resuscitation. Persistent reliance on arterial pressure–centered assessment limits early detection of tissue hypoperfusion, as compensatory mechanisms may preserve macrocirculatory variables while cellular hypoxia and metabolic failure progress. This pressure–perfusion dissociation contributes to delayed diagnosis, late intervention, and unfavorable outcomes, highlighting the need for a pathophysiological coherent approach to shock evaluation. This article develops a theory-driven conceptual framework for integrative hemodynamic assessment grounded in pathophysiological reasoning rather than outcome-based metrics. Drawing on established evidence related to microcirculatory dysfunction, venous congestion, metabolic failure, and loss of hemodynamic coherence, shock is conceptualized as a dynamic, self-reinforcing system. The framework is organized around three interdependent hemodynamic domains—Perfusion, Flow, and Venous drainage—whose interaction defines the integrative hemodynamic state. The model is non-prescriptive and does not introduce numerical scores, clinical protocols, or therapeutic algorithms.The proposed framework enables phenotype-oriented interpretation of shock by identifying the dominant axis of circulatory failure, including impaired forward flow, pathological venous congestion, microcirculatory-metabolic decoupling, or mixed patterns. By shifting emphasis from arterial pressure toward restoration of perfusion coherence, this framework provides a structured foundation for mechanism-aware clinical reasoning and future perfusion-oriented research, while acknowledging the need for prospective validation.
Keywords:
shock
; hemodynamic assessment
; tissue perfusion
; microcirculation
; venous congestion
; hemodynamic coherence
; circulatory failure
; metabolic dysfunction
; critical care
; integrative framework
Introduction
Shock represents a final common pathway of diverse critical conditions and remains a leading cause of morbidity and mortality in intensive care settings.
Despite advances in monitoring technologies and resuscitation strategies, early recognition and accurate characterization of shock continue to pose significant clinical challenges.
A central limitation lies in the persistent reliance on arterial pressure–centered and isolated macrocirculatory parameters, which frequently fail to reflect the adequacy of tissue perfusion and cellular metabolism.
Hemodynamic instability in shock is not a unidimensional phenomenon but rather a dynamic interaction between cardiac pump function, vascular capacitance, venous return, and microcirculatory perfusion.
Compensatory mechanisms may preserve arterial pressure despite progressive impairment at the tissue level, creating a dissociation between apparent hemodynamic stability and ongoing cellular hypoxia. As a result, shock may remain clinically unrecognized until overt decompensation occurs, at which point therapeutic options become limited and outcomes worsen.
From a pathophysiological perspective, shock progression is characterized by self-reinforcing feedback loops linking impaired perfusion, metabolic derangement, inflammatory activation, and further circulatory dysfunction. These interdependent processes cannot be adequately captured by single-parameter assessment or pressure-targeted resuscitation strategies. Consequently, therapeutic interventions guided exclusively by conventional markers risk correcting secondary manifestations rather than addressing the dominant underlying mechanism.
Current clinical practice often prioritizes parameters that are readily accessible and easily quantifiable, such as mean arterial pressure, urine output, and basic laboratory markers. While indispensable for initial stabilization, these indicators predominantly represent late-stage or surface-level manifestations of circulatory failure. More subtle yet decisive disturbances—particularly those related to venous congestion, ineffective forward flow, and microcirculatory dysfunction—remain concealed without extended and integrative assessment.
These limitations highlight the need for a structured framework that moves beyond isolated measurements towards a multidimensional interpretation of hemodynamic instability.
Such a framework should account for the interaction between global flow, venous drainage, and tissue perfusion, allowing clinicians to identify the prevailing pathophysiological phenotype rather than treating shock as a uniform entity. In this context, the present article proposes a conceptual and methodological framework for integrative hemodynamic assessment in shock.
By combining pathophysiological reasoning, diagnostic hierarchy, and domain-based interpretation, the framework aims to support phenotype-oriented understanding of circulatory failure.
Rather than introducing a numerical score or outcome-driven validation, this work provides a theory-building foundation intended to inform future clinical studies and the development of perfusion-oriented, personalized resuscitation strategies.
Conceptual Pathophysiological Background
Classically, shock has been defined by a decrease in mean arterial pressure (MAP). Yet, studies demonstrate that this relationship is only relative. In some cases, even with preserved arterial pressure, severe microcirculatory failure and tissue hypoxia develop. This phenomenon—known as pressure–perfusion dissociation—highlights the discrepancy between macrocirculatory stability and microcirculatory distress.
Compensatory mechanisms such as sympathetic activation and peripheral vasoconstriction temporarily maintain central organ perfusion but at the expense of peripheral ischemia. Consequently, heterogeneity of capillary blood flow, impaired capillary recruitment, and endothelial dysfunction lead to the loss of perfusion coherence (De Backer et al., 2002), (Ince, 2015), (Trzeciak et al., 2008).
Even when MAP and cardiac output appear normal, profound cellular hypoxia may persist—forming the basis for “cryptic shock” or “occult hypoperfusion,” an early yet critical stage of circulatory failure.
When tissue perfusion declines, the balance between oxygen delivery (DO₂) and utilization (VO₂) becomes disrupted, forcing a shift toward anaerobic glycolysis. Anaerobic metabolism increases lactate production, which functions not only as a biomarker of hypoperfusion but also as a pathophysiological mediator.
Lactate accumulation correlates with impaired mitochondrial oxidative phosphorylation, redox imbalance, and altered NADH/NAD⁺ ratios (Levraut et al., 1998), (Garcia-Alvarez et al., 2014), (Walley, 2018).
The resulting intracellular acidosis inhibits metabolic enzymes, promotes oxidative stress, and reduces energy availability—thus amplifying circulatory collapse through self-perpetuating feedback.
Metabolic acidosis and ionic imbalance reduce vascular smooth muscle responsiveness to catecholamines, lowering the effectiveness of vasopressors such as norepinephrine.
Simultaneously, endothelial dysfunction enhances nitric oxide (NO) release and activates the guanylate cyclase pathway, leading to pathological vasodilation and refractory vasoplegia, characteristic of septic shock (Landry & Oliver, 2001), (Annane et al., 2005), (Russell, 2006).
Recent research emphasizes the importance of venous congestion in shock pathogenesis. Elevated central venous pressure (CVP) reduces capillary perfusion gradients and impairs microcirculatory drainage, while increased interstitial pressure hinders oxygen diffusion and metabolite clearance (Marik et al., 2008; Pinsky, 2016).This leads to passive hypoxia, where oxygen is present in the circulation but cannot effectively reach tissues due to diffusion limitations.
This vicious cycle is schematically illustrated by the Ouroboros model (Figure 1), which conceptualises shock progression as an internally sustained process rather than a series of isolated events
The Ouroboros Shock Model unifies these processes into one dynamic system. Perfusion failure induces metabolic imbalance; metabolic dysfunction promotes endothelial injury and vasoplegia; and vasoplegia further worsens perfusion.
This creates a self-reinforcing closed feedback loop, transforming shock from a simple hemodynamic event into a systems-level collapse (Vincent & De Backer, 2013), (Cecconi et al., 2014), (Ince, 2015).
The Ouroboros Shock Model presents shock as an integrative, dynamic, and system-oriented disorder in which hemodynamic and metabolic pathways are tightly coupled through self-perpetuating feedback loops.
It reframes shock not merely as hypotension but as a systemic energetic collapse involving mitochondrial dysfunction, endothelial failure, and microcirculatory breakdown—calling for resuscitation strategies that restore perfusion coherence and metabolic balance, rather than targeting pressure alone.
Within this loop, compensatory responses such as tachycardia and vasoconstriction may transiently preserve arterial pressure, yet simultaneously increase myocardial oxygen demand, worsen venous congestion, and accelerate metabolic exhaustion.
This conceptual framework highlights the inherent limitations of single-parameter assessment and pressure-targeted resuscitation strategies. Interventions aimed solely at restoring arterial pressure or correcting isolated abnormalities may address the downstream manifestations of shock while leaving the upstream drivers of tissue hypoxia and metabolic failure unaltered. Consequently, such approaches risk stabilizing surface-level indicators without interrupting the underlying pathophysiological cycle.
Understanding shock as a multidimensional, self-amplifying process provides the rationale for integrative assessment strategies that move beyond isolated measurements. By identifying the dominant mechanism within the pathophysiological feedback loop—whether impaired forward flow, pathological venous congestion, or primary microcirculatory dysfunction—clinicians may more effectively target interventions capable of disrupting shock progression rather than merely attenuating its late clinical signs.
Limitations of Conventional Shock Assessment
Despite decades of progress in critical care, conventional shock assessment remains largely anchored to arterial pressure–centered reasoning, with mean arterial pressure (MAP) commonly treated as the primary surrogate for circulatory adequacy. However, this MAP-based paradigm oversimplifies the complex and dynamic physiology of shock. As Vincent and De Backer (2013) emphasize, “circulatory shock is not simply arterial hypotension, but rather a state of inadequate tissue perfusion resulting in cellular dysoxia and metabolic failure” (Vincent & De Backer, 2013).
MAP reflects the interaction of cardiac output and systemic vascular resistance but provides no direct information about microcirculatory blood flow, capillary exchange, or oxygen utilization at the tissue level. This physiological decoupling has been described as “loss of hemodynamic coherence”—a condition where macrocirculatory variables are normalized while the microcirculation remains impaired (Ince, 2015). According to De Backer et al. (2002), “microvascular blood flow is altered in patients with sepsis,” even when systemic hemodynamic parameters are restored (De Backer et al., 2002). These microcirculatory disturbances result in inadequate tissue oxygen delivery and are closely linked to organ dysfunction and mortality (Sakr et al., 2018).
Ince (2005) further described that “microcirculatory dysfunction persisting for extended periods can act as a motor driving the pathogenic effects of sepsis by fueling cellular hypoxia and eventual organ failure” (Ince, 2005). This concept redefines shock as a disorder of perfusion coherence rather than arterial pressure alone. Even when MAP and cardiac output are maintained within “acceptable” ranges, severe regional hypoxia, metabolic stress, and cellular energy failure may progress silently (De Backer et al., 2002). The recognition of this phenomenon has led to the development of advanced monitoring techniques aimed at evaluating microcirculatory parameters such as the proportion of perfused vessels (PPV) and perfused vessel density (PVD), which provide more accurate prognostic information than systemic variables alone (Sakr et al., 2018).
Microcirculatory dysfunction contributes to the heterogeneity of capillary perfusion observed in distributive and septic shock. As summarized in Distributive Shock (2023), “abnormal distribution of microvascular blood flow, with some capillaries underperfused and others with normal or high flow, reflects impaired microcirculation.” This heterogeneity leads to inefficient oxygen extraction, accumulation of metabolites, and tissue-level hypoxia even under normal systemic pressure (Distributive Shock, 2023). Persistent microvascular alterations have been directly associated with multiple organ failure and increased mortality, whereas early recovery of microcirculatory perfusion predicts improved outcomes (Sakr et al., 2018).
Traditional MAP-centered approaches to shock assessment provide an incomplete picture of circulatory adequacy. The dissociation between systemic and microcirculatory hemodynamics—the loss of hemodynamic coherence—explains why tissue hypoxia and organ failure may develop despite apparently stable systemic parameters. Recognizing this limitation necessitates a paradigm shift in shock management: from pressure-targeted resuscitation toward strategies that aim to restore microvascular perfusion, cellular oxygen utilization, and metabolic balance.
Collectively, these limitations demonstrate that conventional shock assessment is not merely incomplete but structurally biased towards late recognition and partial correction. By prioritising arterial pressure over perfusion integrity, it encourages a reactive rather than anticipatory approach to circulatory failure.
This realisation provides the conceptual justification for transitioning towards integrative, perfusion-oriented frameworks capable of revealing the true pathophysiological state of shock before irreversible decompensation occurs.
Proposed Framework: Integrative Haemodynamic Assessment
The limitations of traditional, pressure-centred shock assessment necessitate a structured alternative capable of capturing the multidimensional nature of circulatory failure. In response, we propose an Integrative Haemodynamic Assessment (IHA) framework that links macrocirculatory, microcirculatory, and metabolic domains into a unified interpretative model.
This framework is not a numerical scoring system but a conceptual structure designed to ensure pathophysiological coherence between observable haemodynamic parameters and their underlying tissue-level consequences. As Ince (2015) described, the “loss of hemodynamic coherence” underscores how normalized systemic variables can coexist with impaired microcirculation, necessitating integrative evaluation rather than isolated measurements (Ince, 2015).
Within this approach, haemodynamic evaluation shifts away from reliance on isolated macrocirculatory targets (e.g., mean arterial pressure) towards a tissue-oriented interpretative logic. Instead of merely questioning whether arterial pressure is “adequate,” clinicians must consider how blood flow is generated, how it is distributed, and how effectively it is converted into tissue perfusion (Vincent & De Backer, 2013). As De Backer et al. (2002) demonstrated, microvascular blood flow alterations can persist even when systemic hemodynamics appear restored, showing that identical macrocirculatory profiles may mask distinct microcirculatory states (De Backer et al., 2002).
The IHA framework is organized along three interdependent haemodynamic axes: Perfusion (P), Flow (F), and Venous drainage (V).
- Flow (F) reflects the heart’s capacity to generate effective forward blood flow, encompassing cardiac output, stroke volume, and ventricular–arterial coupling.
- Venous drainage (V) represents the efficiency of venous return and systemic capacitance, including venous congestion, right heart loading conditions, and the pressure gradient that governs capillary outflow (Ince, 2005).
- Perfusion (P) denotes the tissue-level outcome of circulatory function, integrating oxygen delivery, microvascular coherence, and metabolic adequacy (Sakr et al., 2004).
Crucially, these axes are interdependent—their combined interaction defines the overall integrative haemodynamic state. Disruption in any axis can destabilize the entire system, leading to tissue hypoxia or organ dysfunction. Importantly, similar clinical presentations (e.g., hypotension) may arise from distinct underlying mechanisms—such as impaired flow, venous congestion, or primary microcirculatory failure—each demanding a different therapeutic approach (Vincent & De Backer, 2013).
This visualisation reinforces the principle that restoring one axis in isolation—such as augmenting arterial pressure—may fail to normalise the integrative state if discordance persists in the remaining domains.
Within this framework, shock is conceptualised as a phenotype-dependent disturbance of the integrative state, rather than a uniform entity defined by threshold values.
Phenotypes emerge based on the dominant axis of failure: flow-limited states, congestion-dominated states, perfusion-decoupled states, or mixed configurations. Importantly, these phenotypes are not static categories but dynamic patterns that may evolve over time as compensatory mechanisms fail or therapeutic interventions alter system balance.
Integrative haemodynamic assessment serves as a conceptual foundation linking pathophysiological reasoning to clinical interpretation.
This approach is not intended to generate numerical indices or scoring systems, but rather to represent a synthesised understanding of how disturbances across perfusion (P), flow (F), and venous drainage (V) converge at the tissue level.
By integrating information across the macro-, meso-, and microcirculatory domains, integrative haemodynamic assessment supports a phenotype-oriented evaluation strategy that prioritises mechanisms over measurements and causal relationships over the correction of superficial haemodynamic abnormalities.
In contrast to conventional assessment paradigms, the proposed framework does not prescribe uniform targets or stepwise algorithms. Its purpose is to guide mechanism-aware clinical reasoning, enabling clinicians to identify which component of the circulatory system primarily sustains shock at a given moment. Such an approach provides the conceptual foundation for perfusion-oriented, personalised resuscitation, in which interventions are selected to restore coherence of the integrative state rather than merely normalise isolated haemodynamic variables.
Clinical and Methodological Implications
The proposed Integrative Haemodynamic Assessment framework is intended to inform clinical reasoning rather than dictate predefined therapeutic actions. Its primary value lies in supporting decision-making under conditions of haemodynamic uncertainty, where conventional pressure-based indicators provide incomplete or potentially misleading information. By shifting the analytical focus from isolated variables to mechanism-oriented interpretation, the framework may assist clinicians in contextualising haemodynamic data within an underlying pathophysiological structure.
From a clinical perspective, the framework is particularly relevant in scenarios characterised by discordance between arterial pressure and tissue perfusion. In such settings, reliance on MAP alone may obscure dominant mechanisms sustaining shock, whereas an integrative P–F–V interpretation may help clarify whether circulatory instability is primarily driven by impaired forward flow, pathological venous congestion, or decoupling at the microcirculatory level.
This distinction may support more deliberate prioritisation of diagnostic and therapeutic considerations without presupposing specific interventions.
Importantly, the framework may influence how clinical decisions are approached rather than which decisions are made. For example, instead of reflexively escalating vasopressor support in response to hypotension, clinicians may be encouraged to reassess the integrative state and reconsider whether pressure augmentation aligns with the dominant pathophysiological pattern.
In this way, the framework may help reframe decision thresholds and reduce overreliance on single-parameter triggers. Methodologically, the proposed approach offers a flexible structure adaptable to varying levels of monitoring availability. It does not require uniform instrumentation, fixed parameter sets, or proprietary technologies. Rather, it provides an interpretative framework into which locally available data—ranging from basic bedside observations to advanced haemodynamic measurements—may be coherently integrated. This adaptability supports applicability across heterogeneous clinical environments without enforcing standardisation that exceeds practical constraints.
The phenotype-oriented nature of the framework also carries methodological implications for clinical research and education. By emphasising dominant mechanisms over diagnostic labels, it may facilitate more precise stratification of haemodynamic states in observational studies and hypothesis-generating research.
Furthermore, it offers a conceptual language for teaching circulatory physiology that aligns macrocirculatory observations with tissue-level consequences, potentially reducing cognitive fragmentation between monitoring domains.
Crucially, this framework does not propose a new score, protocol, or outcome-driven algorithm. It does not claim to optimise resuscitation endpoints or predict prognosis.
Instead, it functions as a cognitive tool designed to enhance coherence between observed haemodynamics and inferred pathophysiology. As such, its contribution is methodological rather than prescriptive, supporting reflective clinical judgement in complex and evolving shock states.
In summary, the integrative framework may support clinical and methodological decision-making by clarifying mechanistic context, highlighting concealed domains of circulatory dysfunction, and promoting adaptive interpretation over rigid target adherence.
Its role is to assist, not replace, clinician expertise—providing a structured way of seeing shock differently rather than asserting how it must be treated.
Limitations
The present work has several important limitations that should be explicitly acknowledged. First and foremost, the proposed framework is conceptual and theoretical in nature. It is not derived from prospective clinical cohorts, randomised trials, or outcome-based validation studies. As such, it does not provide empirical evidence regarding clinical effectiveness, prognostic value, or superiority over existing assessment strategies. Second, the framework has not undergone formal clinical validation. No predefined endpoints, diagnostic accuracy metrics, or interventional comparisons are presented.
Consequently, the model should not be interpreted as a clinical protocol, decision algorithm, or performance benchmark. Its purpose is to structure reasoning rather than to prescribe practice. Third, the absence of a numerical index or standardised parameter set, while intentional, introduces inherent subjectivity. Interpretation of the integrative state depends on clinical judgement and the quality of available haemodynamic data. This may limit reproducibility across operators and institutions, particularly in environments with heterogeneous monitoring capabilities or variable expertise.
Additionally, the framework does not account for all contextual modifiers of shock physiology, such as chronic cardiovascular disease, pre-existing microvascular pathology, or pharmacological influences. These factors may alter the relationship between macrocirculatory parameters and tissue perfusion, potentially affecting the applicability of the proposed constructs in specific patient populations.
Finally, this work does not address implementation feasibility, educational requirements, or workflow integration.
The cognitive demands of integrative, phenotype-oriented reasoning may represent a barrier to adoption without structured training or decision-support tools. Importantly, these limitations are intrinsic to the conceptual scope of the article rather than oversights.
The framework is intended as a hypothesis-generating and theory-building construct, designed to inform future research rather than replace evidence-based practice. Prospective studies, observational validation, and translational investigations are required to explore how integrative, perfusion-orientated reasoning may be operationalised, tested, and refined in clinical settings.
Future Directions
Future work should focus on translating the proposed conceptual framework into empirically testable formats while preserving its mechanistic intent. Initial efforts may include pilot studies designed to explore the feasibility and interpretability of integrative, phenotype-oriented haemodynamic assessment in controlled clinical settings.
Such studies would primarily assess usability, internal coherence, and interobserver consistency rather than clinical efficacy.
Subsequent research may involve prospective observational validation, aimed at examining how integrative interpretation of Perfusion, Flow, and Venous drainage domains corresponds to established physiological markers and evolving shock states over time.
These investigations would help clarify the reproducibility of the integrative state concept and identify conditions under which the framework provides added explanatory value beyond conventional assessment.
Further development may also explore integration with existing monitoring tools, including bedside ultrasound, advanced haemodynamic monitors, and microcirculatory assessment technologies.
Rather than introducing new devices, this approach would evaluate how currently available data streams can be structured within the proposed framework to support coherent interpretation.
Collectively, these directions outline a stepwise research pathway from conceptual formulation towards methodological refinement, providing a foundation for future studies aimed at operationalising integrative, perfusion-oriented haemodynamic assessment in shock.
Conclusion
Conventional shock assessment remains constrained by arterial pressure–centred reasoning, which often fails to capture early and mechanistically decisive disturbances in tissue perfusion.
We propose a conceptual framework for integrative haemodynamic assessment that reorients evaluation towards tissue-resolved interpretation through coordinated analysis of Perfusion, Flow, and Venous drainage domains.
By framing shock as a phenotype-dependent disturbance of an integrative haemodynamic state rather than a uniform pressure-defined condition, the framework offers a coherent pathophysiological perspective.
While theoretical and unvalidated, this approach establishes a foundation for future research focused on perfusion-orientated, mechanism-aware evaluation of circulatory failure.
Figures and Figure Legends
Figure 1: Conceptual pathophysiological feedback loop underlying shock progression (Ouroboros model)
This figure illustrates the self-reinforcing pathophysiological loop that characterises shock progression. Impaired tissue perfusion initiates metabolic derangement and inflammatory activation, leading to endothelial dysfunction, altered vascular tone, and microcirculatory disorganisation.
These changes further deteriorate effective forward flow and venous drainage, thereby amplifying perfusion failure.
Compensatory responses may transiently preserve arterial pressure while intensifying myocardial workload and venous congestion. The Ouroboros configuration emphasises that shock evolves as an internally sustained process rather than a linear sequence of isolated events.
Figure 2: Limitations of arterial pressure–centered shock assessment and the concept of clinical blindness
This figure contrasts surface-level macrocirculatory indicators with hidden areas of circulatory dysfunction. Mean arterial pressure and related conventional parameters represent visible and continuously monitored signals, yet they remain physiologically separate from tissue perfusion and microcirculatory integrity.
The figure highlights how compensatory mechanisms may maintain arterial pressure despite progressive impairment in effective flow, venous drainage, and cellular oxygen utilisation.
This dissociation underlies delayed shock recognition and illustrates the concept of clinical blindness inherent to pressure-centred assessment paradigms.
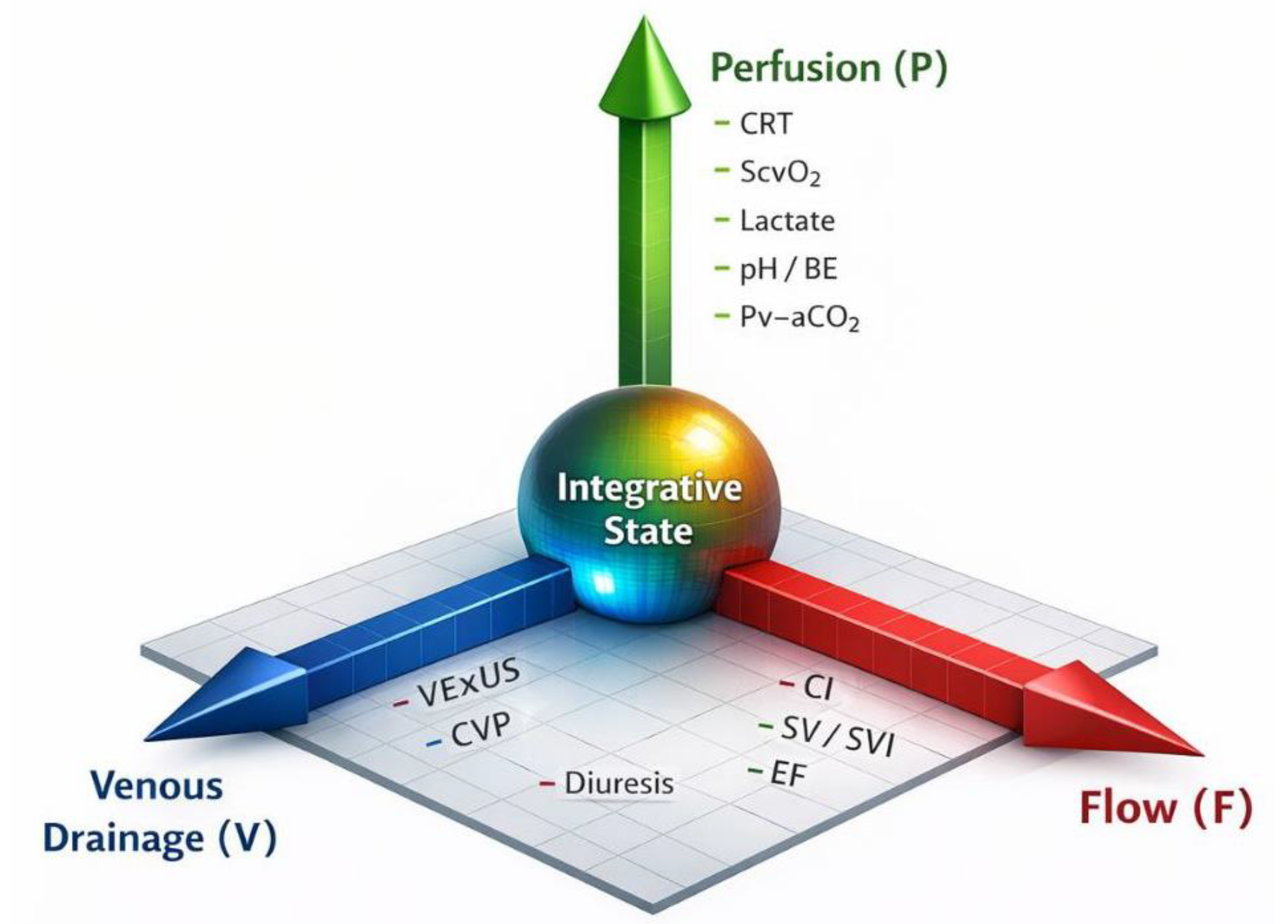
Figure 3: Proposed integrative hemodynamic assessment framework based on P–F–V axes and the integrative state
This figure schematically presents the proposed Integrative Haemodynamic Assessment framework. Three interdependent axes—Perfusion (P), Flow (F), and Venous drainage (V)—define the multidimensional domains of circulatory function. Their interaction determines an integrative haemodynamic state reflecting the coherence between global haemodynamics and tissue-level consequences.
Shock is conceptualised as a phenotype-dependent disturbance of this state, arising from dominant imbalance along one or more axes. The framework emphasises mechanism-oriented interpretation over isolated parameter normalisation.
References
- Annane, D.; Bellissant, E.; Cavaillon, J. M. Septic shock . The Lancet 2005, 365(9453), 63–78. [Google Scholar] [CrossRef] [PubMed]
- Cecconi, M.; De Backer, D.; Antonelli, M.; Beale, R.; Bakker, J.; Hofer, C.; Jaeschke, R.; Mebazaa, A.; Pinsky, M. R.; Teboul, J. L.; Vincent, J. L.; Rhodes, A.; ESICM Task Force. Consensus on circulatory shock and hemodynamic monitoring . Intensive Care Medicine 2014, 40(12), 1795–1815. [Google Scholar] [CrossRef] [PubMed]
- De Backer, D.; Creteur, J.; Preiser, J. C.; Dubois, M. J.; Vincent, J. L. Microvascular blood flow is altered in patients with sepsis . American Journal of Respiratory and Critical Care Medicine 2002, 166(1), 98–104. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Alvarez, M.; Marik, P. E.; Bellomo, R. Stress hyperlactatemia: Present understanding and controversy . Shock 2014, 41(4), 288–296. [Google Scholar] [CrossRef]
- Ince, C. The microcirculation is the motor of sepsis . Critical Care 2005, 9 (Suppl 4), S13–S19. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC3226164/. [CrossRef] [PubMed]
- Ince, C. Hemodynamic coherence and the rationale for monitoring the microcirculation . Critical Care 2015, 19 (Suppl 3), S8. [Google Scholar] [CrossRef] [PubMed]
- Landry, D. W.; Oliver, J. A. The pathogenesis of vasodilatory shock . The New England Journal of Medicine 2001, 345(8), 588–595. [Google Scholar] [CrossRef] [PubMed]
- Levraut, J.; Ciebiera, J. P.; Jambou, P.; Ichai, C.; Grimaud, D. Effect of sodium bicarbonate on intracellular pH under different buffering conditions . Shock 1998, 9(2), 119–124. [Google Scholar] [CrossRef] [PubMed]
- Levy, B. Lactate and shock state: The metabolic view . Current Opinion in Critical Care 2006, 12(4), 315–321. [Google Scholar] [CrossRef] [PubMed]
- Marik, P. E.; Baram, M.; Vahid, B. Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest 2008, 134(1), 172–178. [Google Scholar] [CrossRef] [PubMed]
- Pinsky, M. R. Hemodynamic evaluation and monitoring in the ICU . Chest 2007, 132(6), 2020–2029. [Google Scholar] [CrossRef] [PubMed]
- Russell, J. A.; Walley, K. R.; Singer, J.; et al. Vasopressin versus norepinephrine infusion in patients with septic shock . The New England Journal of Medicine 2008, 358(9), 877–887. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Dubois, M. J.; De Backer, D.; Creteur, J.; Vincent, J. L. Persistent microcirculatory alterations are associated with organ failure and death in patients with septic shock . Intensive Care Medicine 2004, 30(7), 1326–1333. [Google Scholar] [CrossRef] [PubMed]
- Trzeciak, S.; McCoy, J. V.; Dellinger, R. P.; Arnold, R. C.; Rizzuto, M.; Abate, N. L.; Shapiro, N. I.; Parrillo, J. E.; Hollenberg, S. M.; Microcirculatory Flow Consortium. Early increases in microcirculatory perfusion are associated with reduced organ failure and mortality in septic shock . Intensive Care Medicine 2008, 34(12), 2210–2217. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J. L.; De Backer, D. Circulatory shock . The New England Journal of Medicine 2013, 369(18), 1726–1734. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Ouroboros model.
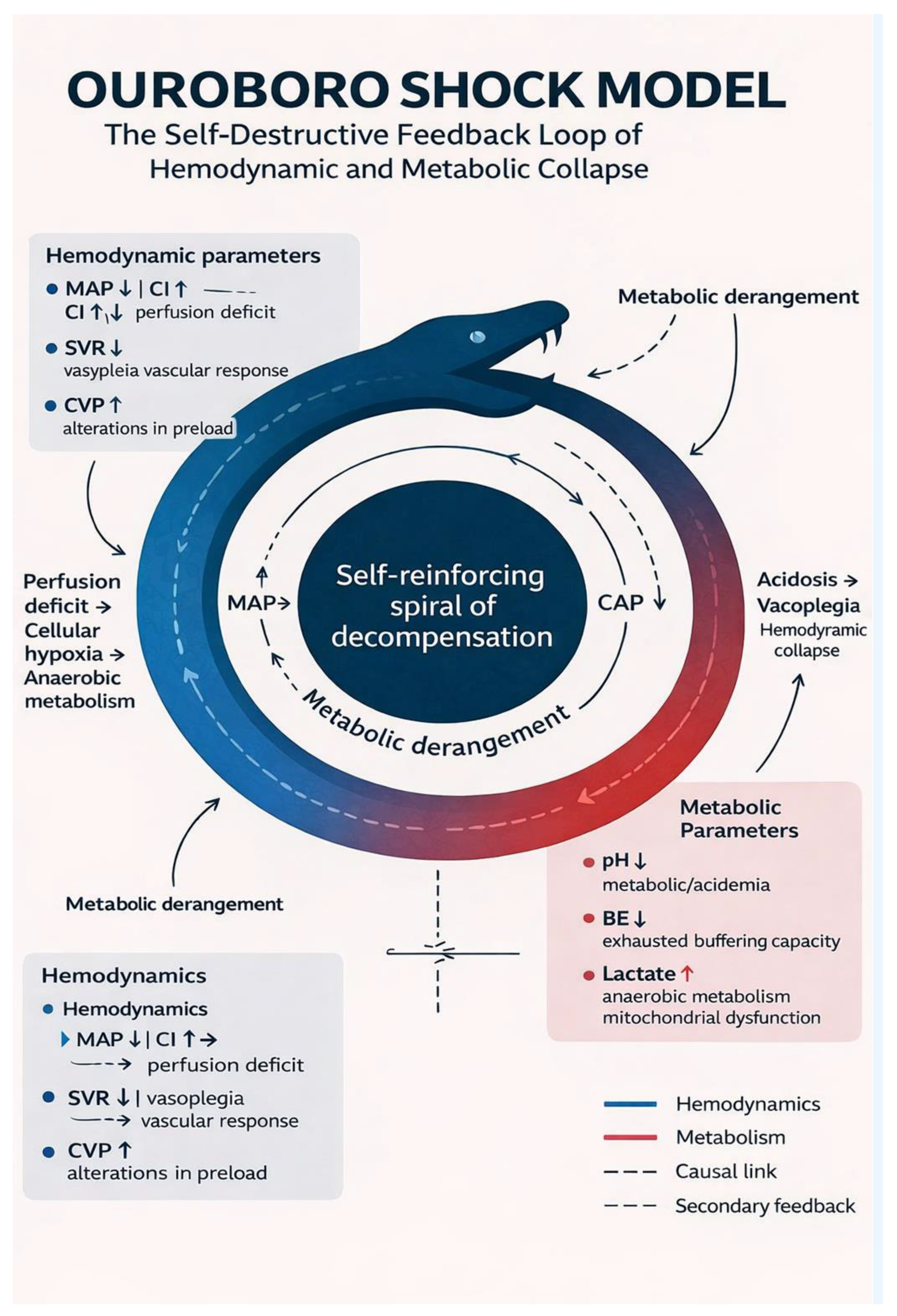
Figure 2.
Conceptually illustrates this limitation by contrasting visible, pressure-based indicators of shock with concealed domains of circulatory dysfunction. The figure emphasises that conventional assessment captures only the most superficial layer of haemodynamic instability, while the dominant drivers of tissue hypoxia and metabolic failure remain hidden without integrative evaluation. This mismatch explains why treatment guided exclusively by conventional markers may stabilise numerical targets without altering the trajectory of shock.
Figure 2.
Conceptually illustrates this limitation by contrasting visible, pressure-based indicators of shock with concealed domains of circulatory dysfunction. The figure emphasises that conventional assessment captures only the most superficial layer of haemodynamic instability, while the dominant drivers of tissue hypoxia and metabolic failure remain hidden without integrative evaluation. This mismatch explains why treatment guided exclusively by conventional markers may stabilise numerical targets without altering the trajectory of shock.
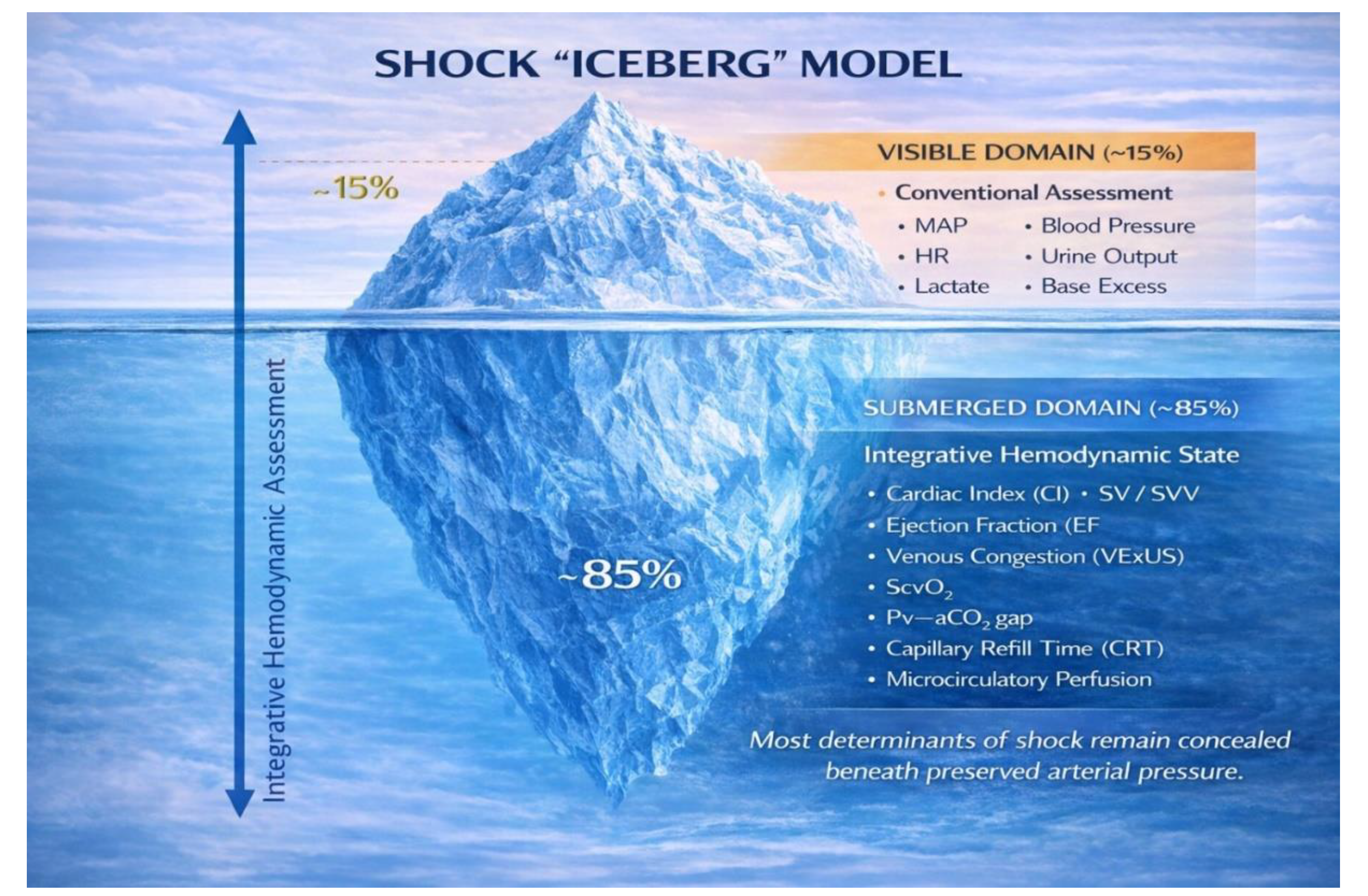
Figure 3.
Schematically represents this framework by positioning the integrative state at the intersection of the P–F–V axes. Rather than depicting shock as a linear progression, the figure emphasises multidirectional imbalance and compensatory trade-offs between domains.
Figure 3.
Schematically represents this framework by positioning the integrative state at the intersection of the P–F–V axes. Rather than depicting shock as a linear progression, the figure emphasises multidirectional imbalance and compensatory trade-offs between domains.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



