Submitted:
23 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Background/objectives: The prevalence of autistic spectrum disorder has been increasing rapidly in the world population and the cause of this increase is unknown. Autistic spectrum disorder is an important cause of social, communication and specific learning difficulties in children. Assortative mating may increase the genetic burden leading to manifestation of polygenic diseases affecting mental health in the offspring. Correlation of scores in the Social Responsiveness Scale (SRS), which is used to quantify autistic spectrum disorder features, between spouses, has been used as indicator of phenotypic assortative mating. We investigated whether assortative mating is involved in increased severity of autism spectrum disorder in the offspring. Methods: All studies reporting on investigation of assortative mating in relationship to autistic spectrum disorder were included. Information sources were Pubmed, EMBASE and the Cochrane Library. Results were synthesized by entering correlation analyses of results of the SRS conducted in spouses in a meta-analysis. A sub-group analysis was performed comparing spouses with offspring with diagnosed autistic spectrum disorder to spouses without. Prevalence of autistic spectrum disorders in children in countries with and without predominant assortative mating was compared. Results: 14 investigations of assortative mating including 9914 spouse pairs were included. 8 studies (4641spouse pairs) reported intra-class correlation (ICC) or Spearman’s correlation cofficients between spouses SRS Scores. There was a significant correlation of SRS scores in studies using ICC or Spearman’s correlation with a pooled co-efficient of = 0.37. Spouse pairs (n=401) with offspring diagnosed with autistic spectrum disorder had a pooled ICC coefficient which was with 0.278 (95% CI 0.08 to 0.46) significantly lower than spouse pairs without (n=1525): 0.40 (95% CI 0.35 to 0.46). Higher scores in SRS of both spouses were associated with higher scores and more autism diagnoses in offspring. Pooled prevalence of autistic spectrum disorder in children in countries where assortative mating is most common was 63.1 per 10000 of population and in countries without it was significantly lower with 14.1 per 10000 of population. Conclusions There is evidence of assortative mating according to Social Responsiveness Scale Score which correlates significantly in spouse pairs with and without children with autistic spectrum disorder. In countries where assortative mating is predominant a higher prevalence of autism spectrum disorder in children is found compared to countries without. Funding: There was no funding involved in the conduct of this research. Registration: The protocol for this systematic review was pre-registered in the International prospective register of systematic reviews PROSPERO registration number: CRD420251141431.
Keywords:
autism
; autistic spectrum disorder
; assortative mating
; protective allels
; non-random mating
Introduction:
Rationale:
Autism spectrum disorders (ASD) is an umbrella term for a group of neurocognitive phenotypes which have as core features social communication deficits and restricted or repetitive sensory-motor behaviours manifesting itself for example in repetitive hand or finger movements or handling of objects, and repetitive use of phrases, interests or activities which are different from the majority of the population. Up to 2.3% of children are currently affected by ASD [1,2]. According to a recent systematic review overall 33% of people with ASD have been reported as having learning difficulties [3]. The cause is unknown. It can’t be environmental factors because twin studies showed that 92% of monozygotic twin pairs were concordant for a broader spectrum of related cognitive or social abnormalities versus 10% of dizygotic twin pairs in a British study of forty-four sets of twins and triplets, which were available for genetic analysis and these contained 59 autistic individuals [4] demonstrating that this condition is inherited. The largest previous systematic review into environmental risk factors identified metabolic syndrome features in pregnancy, which are related to obesity, as the only convincingly associated factor, which may also explain the association with testosterone exposure [5]. This association is however simply due to the fact that undiagnosed masked autistic spectrum disorder gene expression in the pregnant women included caused obesity in pregnancy and at the same time autism spectrum disorder in the offspring. Autistic spectrum disorder is associated with increased BMI in 33% [3] and the largest systematic review on the association of obesity with autism revealed from the analysis of fifteen studies encompassing 49,937,078 participants and 1,045,538 individuals with ASD that the prevalence of obesity was significantly higher in individuals with ASD than in controls (OR = 1.84, 95% confidence interval [CI]: 1.37–2.48, P < 0.001) [6]. The global increase in obesity prevalence is therefore unlikely to be the cause of an increase in autism spectrum disorder prevalence. Global epidemiological studies have demonstrated that the prevalence of autism spectrum disorders is increasing world-wide [2] with a doubling of prevalence in the USA from 2008 to 2018 from 1.1 to 2.3%, in South Korea from 5.04 (per 100,000) in 2008, to 10.97 in 2015 [7], in Taiwan [8], Hong Kong [9], Thailand [10] and France with a significant increase between 1997 and 2003 [11]. The question therefore arises how an overwhelmingly genetic condition can increase rapidly in the general population without it being simply a reflection of increased awareness or diagnostic capability.
Assortative mating is a non-random mating system which occurs when there is a correlation (positive or negative) between male and female phenotypes or genotypes across mated pairs. Assortative mating can be measured as a correlation between the values of homologous phenotypic or genotypic traits across members of mated pairs. Assortative mating may be either positive, implying a tendency to mate with phenotypically similar individuals, or negative (also called dis-assortative), implying the converse [12]. When the trait has a genetic component and assortative mating occurs, both genetic and phenotypic assortative mating take place. Assortative mating can hereby increase the deviation of a phenotype from the average. This will then cause a phenotype with enough features to enable a diagnosis and hence increase the prevalence of a condition being diagnosed in the general population. Assortative mating has first been proposed as a mechanism for increase in autism spectrum disorder prevalence by Professor Sir Simon Baron-Cohen based on his observation of similarities in spousal cognitive phenotype amongst parents of children with autistic spectrum disorder [13,14].
This systematic review has as a goal to investigate whether assortative mating is involved in the increase in prevalence of autism spectrum disorders by parents who have chosen each other on the basis of a phenotype resulting from genes involved in the pathogenesis of autistic spectrum disorder increasing the overall genetic load of autism spectrum disorder causing genes in the offspring. This increased genetic load causes the phenotype to be more severe and above the threshold enabling a diagnosis hence increasing the prevalence of diagnosed cases. Assortative mating forms the basis of marriage in the United States of America, Mexico, South American countries, European countries, Israel, Lebanon, China, Taiwan and Australia [15]. Epidemiological investigations in Saudia Arabia, India, Bangladesh and Nepal revealed that the majority of marriages are arranged [16,17,18,19,20].
Objectives:
- To investigate whether assortative mating guided by features of autistic spectrum disorder occurs.
- To investigate whether, if assortative mating occurs, there are specific personal characteristics guiding the mating more than others.
- To investigate whether assortative mating is involved in increased severity of autism spectrum disorder in the offspring.
- To investigate if autistic spectrum disorder is less common in countries where mating is not assortative compared to countries where assortative mating can occur due to individual partner choice.
Methods
The review was structured and conducted following the PRISMA 2020 guidelines: See check list in appendix 1.
Eligibility criteria
Inclusion criteria
Included were all studies reporting on assortative mating of the following participants:
- Adults and children with a diagnosis of autistic spectrum disorder
- Adults and children with phenotypic traits of an autistic spectrum disorder
- Adults and children with genes associated with autistic spectrum disorder
- Adults and children without the above phenotypic features, diagnoses or genes of autistic spectrum disorder used as control groups for the above groups
For investigation of the influence of marriage practices based on assortative mating versus arranged marriages population based studies applying validated tools for diagnosis of autistic spectrum disorder to all participants were included. Only the most recent such investigation for each country was included. If there was more than one study from a country only those conducted on non-overlapping populations were included.
Exclusion criteria
Studies where the criteria for diagnosis of autistic spectrum disorder or traits of autistic spectrum disorder were not documented or assortative mating was not investigated.
Information sources
Search strategy: Both authors searched the data bases Pubmed, EMBASE and the Cochrane library were searched from inception to 08.09.2025 using the following keywords (autism OR autistic spectrum disorder OR autism spectrum disorder) AND (assortative mating OR random mating OR non-random mating OR protective allels). In addition literature quoted was retrieved and screened for eligibility. Data on prevalence of autistic spectrum disorders were taken from already existing recent systematic reviews [21,22,23].
Selection process: The selection process was documented following the PRISMA 2020 guidance [24] (see figure 1).
Data collection process was performed using an excel word spreadsheet
Data items extracted included: Characteristics of the population of each study, number of spouse pairs, tool used for ascertainment of features of autistic spectrum disorder, statistical tool used for ascertainment of assortative mating, result of correlation analyses.
Study risk of bias assessment
The included studies were checked for the following risks of bias: Publication bias (tested for by the Egger test), confirmation bias, halo/horn effect, primacy/recency bias, evaluative bias, cultural bias, social desirability bias, subjective judgement and lack of expertise related bias.
Effect measures: Pooled correlation co-efficients for psychometric scores related to assessment for autistic spectrum disorder between spouses were calculated where meta-analysis was appropriate and compared between spouses with offspring with and without a diagnosis of autistic spectrum disorder.
Synthesis methods
Because of the heterogeneity of studies the Hedges-Olkin random effects method was used for meta-analysis of intra-class correlation (ICC) and Spearman’s correlation coefficients.
The heterogeneity of studies was quantified and reported using Cochrane Q and I2 with values > 40% representing moderate heterogeneity, > 60% substantial heterogeneity, and > 80% considerable heterogeneity.
If in separate studies correlation of spousal’s mutual psychometric testing derived from the same cohort was investigated only the investigation with the larger number of participants was included in the meta-analysis to avoid duplication.
To compare the pooled ICCs the Fisher’s z-transformation was used to convert the ICC coefficients into Fisher’s Z-transformed values followed by use of the formula:
Z obs = Fisher’s Z-statistic for the comparison. Z1 and Z2 are the Fisher’s Z statistics of the ICC’s of the two groups compared and N1 and N2 are the number of participants in each group.
Reporting bias assessment: Both Begg-Mazumdar and Egger test were applied to studies included in the meta-analysis
Quality scores were compared between studies reporting on assortative mating of spouses with and without offspring with ASD using Mann-Whitney U test.
We compared incidence rates (per 10000 of population) of autism spectrum disorders in countries with generally predominant mating by individual choice as a more likely assortative mating strategy versus countries with other mating systems like guided by astrology and arrangement by parents using chi-square testing and calculated the relative risk.
Statistical software used for meta-analysis was: StatsDirect® (STATSDIRECT LIMITED 36 Barton Hey Drive, Wirral, England, CH48 1PZ). Chi-square testing and risk ratio calculation was conducted using EpiInfo® version 7.0 (CDC, Atlanta, USA).
A p-value of <0.05 was taken as indicator of evidence of significantly low probability of erroneously rejecting the null hypothesis of no difference.
Certainty assessment: We used the GRADE approach to certainty assessment, which included domains of Risk of bias, Inconsistency, imprecision, indirectness, publication bias and others [25].
Quality assessment: For critical appraisal we used the AXIS tool for assessment of the quality of cross-sectional studies using 20 items covering introduction, methods, results and discussion of findings [26].
Each item was attributed if fully addressed by the authors a scoring point with at least 70% of total equivalent to a high quality publication, between 60 and 69% fair quality and below 60% low quality [27].
Results
Study selection
For studies on assortative mating 14 investigations including 9914 spouse pairs were included (See PRISMA Flow chart in figure 1 for study selection and for content of studies table 1). A total of 10 articles reporting on investigations into phenotypical parental assortative mating in 13 study groups totalling 6705 spouse pairs (see table 1 and table 2) were identified. 10 studies (4641spouse pairs) reported intra-class correlation (ICC) or Spearman’s correlation coefficients between spouses SRS Scores. A meta-analysis could be conducted for 8 study groups reporting intra-class correlation (ICC) between Social Responsiveness Scale Scores (SRSS) (1927 spouse pairs) (see figure 2) and separately on 2 studies (2674 spouse pairs) reporting Spearman’s correlation coefficients for SRSS (See figure 3). A further three studies could not be included in a meta-analysis as one reported on Pearson’s correlation co-efficient of the Dutch Autism Spectrum Quotients (128 spouse pairs) and another on the Pearson’s correlation co-efficients for SRSS (121 spouse pairs) and a third on tetrachoric correlation of mating of spouses with a diagnosis of autism spectrum disorder (1855 spouse pairs). In 2 studies correlation of subdomains of SRSS was investigated. 3 articles reported on 4 study groups where genotypic assortative mating was investigated. Five studies detailed in table 1 investigated correlation of parental social responsiveness scale score with severity of autism spectrum disorder in offspring. There the influence of mating comparing the severity of autism spectrum disorder in the offspring from spouses with similar versus dissimilar ethnic or ancestry related back ground.
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources.
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources.
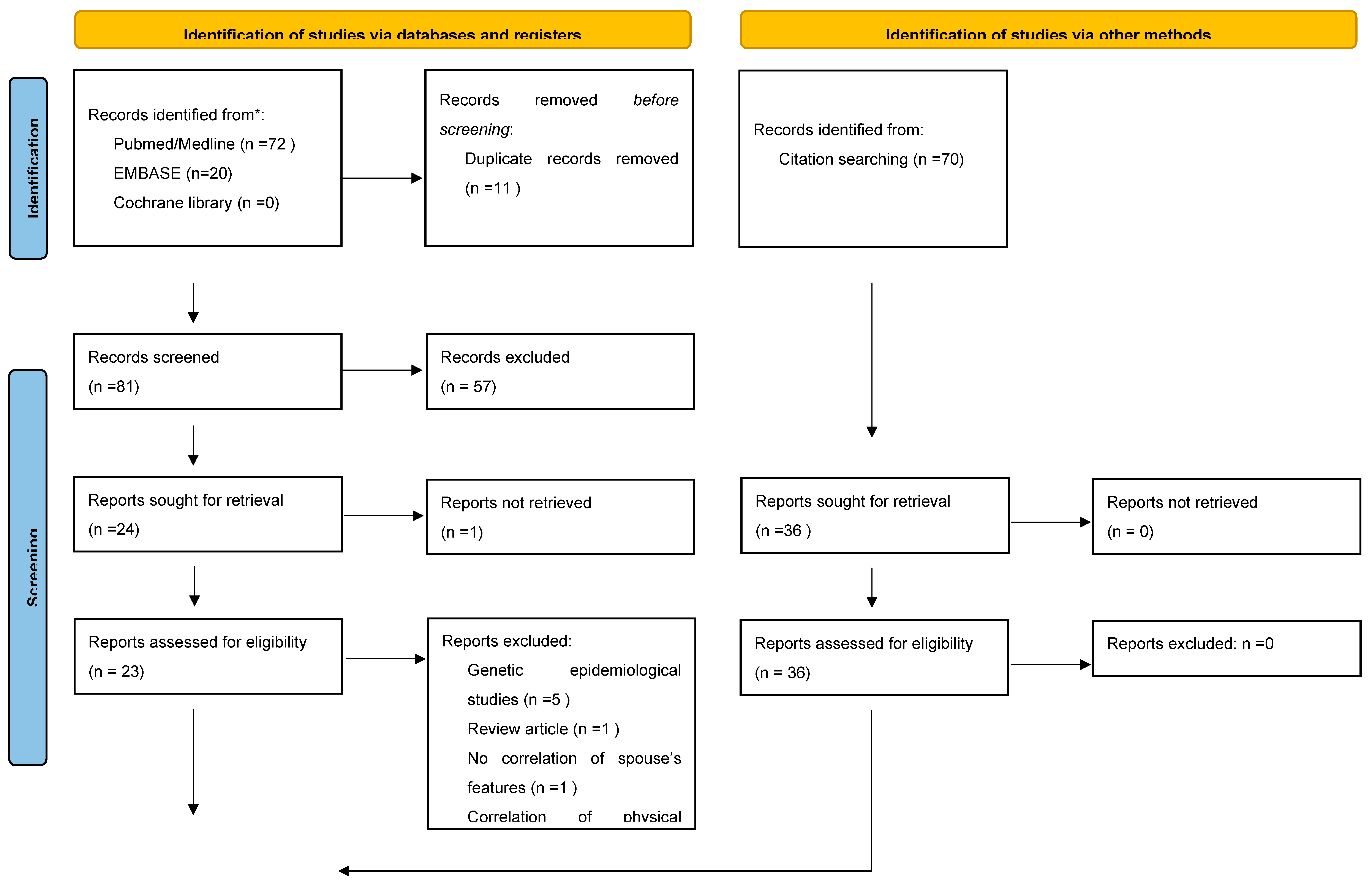


Table 1.
Characteristics of included studies regarding comparison of phenotype in parents of children with autistic spectrum disorder.
Table 1.
Characteristics of included studies regarding comparison of phenotype in parents of children with autistic spectrum disorder.
| First author and year | Study design | Population and sample | Comparison | Outcome measures | Key findings | Quality Assessment Score (AXIS tool) | Limitations |
| Constantino et al 2005 [28] | Observational study | 89 monozygotic female– female twin pairs and their parents, 69 dizygotic female–female twin pairs, 127 dizygotic male–female twin pairs and the parents of those twin pairs equivalent to 285 parent pairs. Age range from 8 to 17 years, with an average age of 12.5 years. European American, with 12.5% African American and<1% other ethnicity by self-report.The Missouri Twin Study population was the random sample from which study subjects were recruited. |
Social Responsiveness Scale score (SRSS) compared between parents and parents and their children. | Intraclass correlations of SRSS between parents and parents and their children. The mean SRS scores of the parents were compared to the mean SRS scores of the offspring | Intraclass correlations for pairings of family members: mother–daughter 0.41, mother– son 0.38, father–daughter 0.49, father–son 0.58. Intraclass correlation between mothers and fathers was 0.38, P<0.001 for all comparisons |
14 | Bias forms associated with lay assessment1 There was a restriction of spousal reports to biological parents who were still married. This may have biased against the inclusion of parents with extreme scores (but may have protected from artificially inflated scores from disgruntled divorced parents). |
| Forsen et al 2024 [29] |
Observational study | Quantitative autistic trait data of parents of epidemiologically ascertained toddler twins were collected in the Early Quantitative Characterization of Reciprocal Social Behavior Study in Missouri with 95 spousal pairs and California with 93 spousal pairs. Birth records were used to identify all twin pairs born between 2011 and 2013 in those respective States, and parents were selected at random from pools of self-identified English-speaking Hispanic families in California and Non-Hispanic White families in Missouri. | SRSS compared between parents | Intraclass correlation coefficients (ICCs) for square-root-transformed SRS-2 scores between spouses were calculated to index assortative mating. Quantile regressions tested the relationship between spousal SRS-2 scores based on estimates of regression coefficients at the 25th, 50th, and 75th quantile. | Missouri spousal pairs: intra class correlation (ICC) of 0.43 (95% CI: 0.25, 0.58); California spousal pairs: 0.44 (95% CI: 0.26, 0.59. Quantile regression analysis showed that stronger associations between spousal SRS scores at higher quantiles. Significant spousal associations were observed at each quantile. |
13 | Bias forms associated with lay assessment1 |
| Zhang et al. 2024 [30] | Observational study | Family based autism collection: Simons Simplex Collection (SSC) including data on 2246 spouse pairs of European ancestry with one child with autism. |
SRS obtained from an informant (mother reported on father and father reported on mother) 2246 spouse pairs, and the self-reported Broad Autism Phenotype Questionnaire (BAPQ) 2176 spouse pairs |
The correlations between spouses’ measures of quantitative autistic traits in SSC were evaluated using Spearman’s correlation coefficient with subgroup analysis for parents of children with and without learning difficulties Comparison of the pattern of AM of autism w/ and w/o CI/ID. |
There was moderate and significant correlation of total scores and similar for children with and without learning difficulties (r=0.32) for the SRS and weak with/ without learning difficulties in children assessed by BAPQ: 0.12/.0.15. | 15 | Bias forms associated with lay assessment1 Selection bias 2 |
| Smolen et al 2023 [31] | Observational study | Family based autism collection: Simons Simplex Collection (SSC) including data on 1822 spouse pairs of European ancestry with one child with autism. |
SRS obtained from an informant (mother reported on father and father reported on mother), and the self-reported BAPQ |
The correlations between spouses’ measures of quantitative autistic traits in SSC and were evaluated using Pearsons correlation coefficient |
There was moderate significant correlation of total scores: r=0.29 on SRS and 0.10 on BAPQ | 12 | Selection bias 2 |
| Connolly et al 2019 [32] | Observational study | Simons Simplex Collection (SSC) including data on 1953 spouse pairs of European ancestry with one child with autism. | SRS obtained from an informant (mother reported on father and father reported on mother) |
The correlations between spouses’ measures of quantitative autistic traits in SSC were evaluated using Spearman’s correlation coefficient |
There was moderate significant correlation of total scores: r=0.34 on SRS | 14 | Bias forms associated with lay assessment1 Selection bias 2 |
| Connolly et al 2019 [32] | Observational study | Autism genome project data base where data from 428 spouse pairs with 62% multiplex families (more than one child with autism) | SRS obtained from an informant (mother reported on father and father reported on mother) |
The correlations between spouses’ measures of quantitative autistic traits in SSC were evaluated using Spearman’s correlation coefficient |
There was a significant correlation of 0.44 for total scores observed. | 14 | Bias forms associated with lay assessment1 Selection bias 2 |
| Page et al. 2016 [33] | Observational study | 151 Hispanic families recruited from the University of Miami Department of Psychology, categorized into two groups by index subject: ASD diagnosis (n = 85) and controls (n = 66) and their parents and siblings. The controls were families recruited from South Florida, including the University of Miami student community. In 79% of families both parents were Hispanic. | Spanish version of SRS (see above) version 2 obtained from parents assessing each other. SRS-2 scores were obtained from children by parents and teacher report. All ASD subjects were diagnosed by expert clinicians at the University of Miami site; in addition to the SRS-2. |
An intraclass correlation co-efficient between parental SRS scores was calculated. Concordant elevation in parental scores of ASD subjects were analysed comparing families with and without children with ASD by dividing the raw spouse-report SRS-2 data into four quartiles based on parental severity. |
There was a significant correlation coefficient of 0.48 between parents of ASD families (62 spouse pairs) in ASD families and 0.60 in non-ASD families (60 spouse pairs) | 16 | Bias forms associated with lay assessment1 Selection bias 2一 The recruitment from a predominantly Hispanic background may have increased intraclass correlation due to common ancestors. |
| Lyall et al 2014 [34] | Observational study | 240 spouse pairs of children with autism spectrum disorder (maternal report of diagnosis) from the Nurses’Health Study (NHS) II, a prospective cohort of 116 430 female nurses in the USA, with 92.2% with Caucasian ethnic origin. There were 993 control spouse pairs, which were parents with a child without a diagnosis of autistic spectrum disorder. |
SRS-A was used and parents assessed each other. All index child were completed by the index child’s mother. |
An intraclass correlation co-efficient between parental SRS scores was calculated. The percentage of concordantly elevated parent score in offspring with ASD versus no ASD was reported. | Correlation of SRS-A scores between parents of children with ASD had a non-significant correlation coefficient of 0.14 and in the control group 0.39. | 17 | Bias forms associated with lay assessment1 Selection bias 2 |
| Van Steijn et al. 2012 [35] | Observational study | 121 spouse pairs were recruited as part of the Biological Origins of Autism (BOA) project in the Netherlands which aims to examine the genetic, biochemical and cognitive origins of ASD and all children had a diagnosis of ASD. |
Adult version of the autism spectrum quotient (AQ) |
Correlation of the autism spectrum quotient using Pierson’s correlation co-efficient | Both fathers and mothers scored above population average with respect to self-reported ASD symptoms but the correlation of symptom scores of the autism quotient was not significant. | 16 | The sample size calculation was small and the autism spectrum quotient data were from parental report therefore they could not rule out outcome misclassification, inclusion of milder cases, or other diagnoses. |
| Virkud et al. 2009 [36] | Observational study | Multiplex ASD families, n=58, recruited from the Autism Genetic Resource Exchange and 2) 41 conservatively-defined simplex ASD families recruited for a longitudinal study of male sibling pairs at Washington University. |
SRS-A was used and parents assessed each other. SRS scoring by one parent (in most cases mother) and one teacher was completed. |
An intraclass correlation co-efficient between parental SRS scores was calculated. To compare spousal ICC correlation between families with one to families with more than one family member with ASD. To investigate whether concordantly elevated SRS scores in spouses are different in children of families with one compared to more than one member with ASD |
Correlation of SRS-A scores between parents of children with ASD had a significant (p<0.01) correlation coefficient of 0.26 (99 spouse pairs). | 14 | Bias forms associated with lay assessment1 Selection bias 2 |
| Hoekstra et al 2007 [37] | Observational study | Netherlands Twin Register kept by the Department of Biological Psychology at the VU University in Amsterdam. 128 mother/father pairs were included. Participation rate for this data collection was 54%. Participating families did not significantly differ from nonparticipating families in socioeconomic status, but parental education level was slightly higher in participating families. No information about ASD diagnoses was available. | The parents completed the Dutch Autism-spectrum quotient (AQ) about each other. | The Pearson correlation co-efficient between scores of spouses was calculated. | The partner correlation for AQ score was r=0.05 (p=0.59) | 16 | Participants were recruited on an informational day for parents of multiples. Individuals who dislike being confronted with large crowds may have been unlikely to attend this event. |
| Nordsletten et al 2016 [38] | Observational study | Population-based cohort using Swedish population registers. Participants were all Swedish residents with a psychiatric diagnosis of interest along with their mates. 880 men and their spouses and 975 women and their spouses were included |
Diagnosis (as determined by the treating physician). These diagnoses are documented using the World Health Organization’s International Statistical Classification of Diseases and Related Health Problems. | Tetrachoric correlation coefficient | ASD diagnosis correlated with a tetrachoric correlation coefficient of 0.48 for men and 0.45 for women which was highly significant (p<0.01) and the highest for any psychiatric diagnosis and higher than the highest correlation coefficient for the control group with organic diagnoses. | 16 | The authors quoted detection bias as diagnosis in one spouse may have resulted in diagnosis in the spouse. |
1 Confirmation bias, halo/horn effect, primacy/recency bias, evaluative bias, cultural bias, social desirability bias, subjective judgement and lack of expertise. 2Inclusion of only families with an autistic child will lead to an increased probability of both patients to have autistic traits as it is an inherited condition
Results of syntheses
Pooled correlation of SRSS in spouses
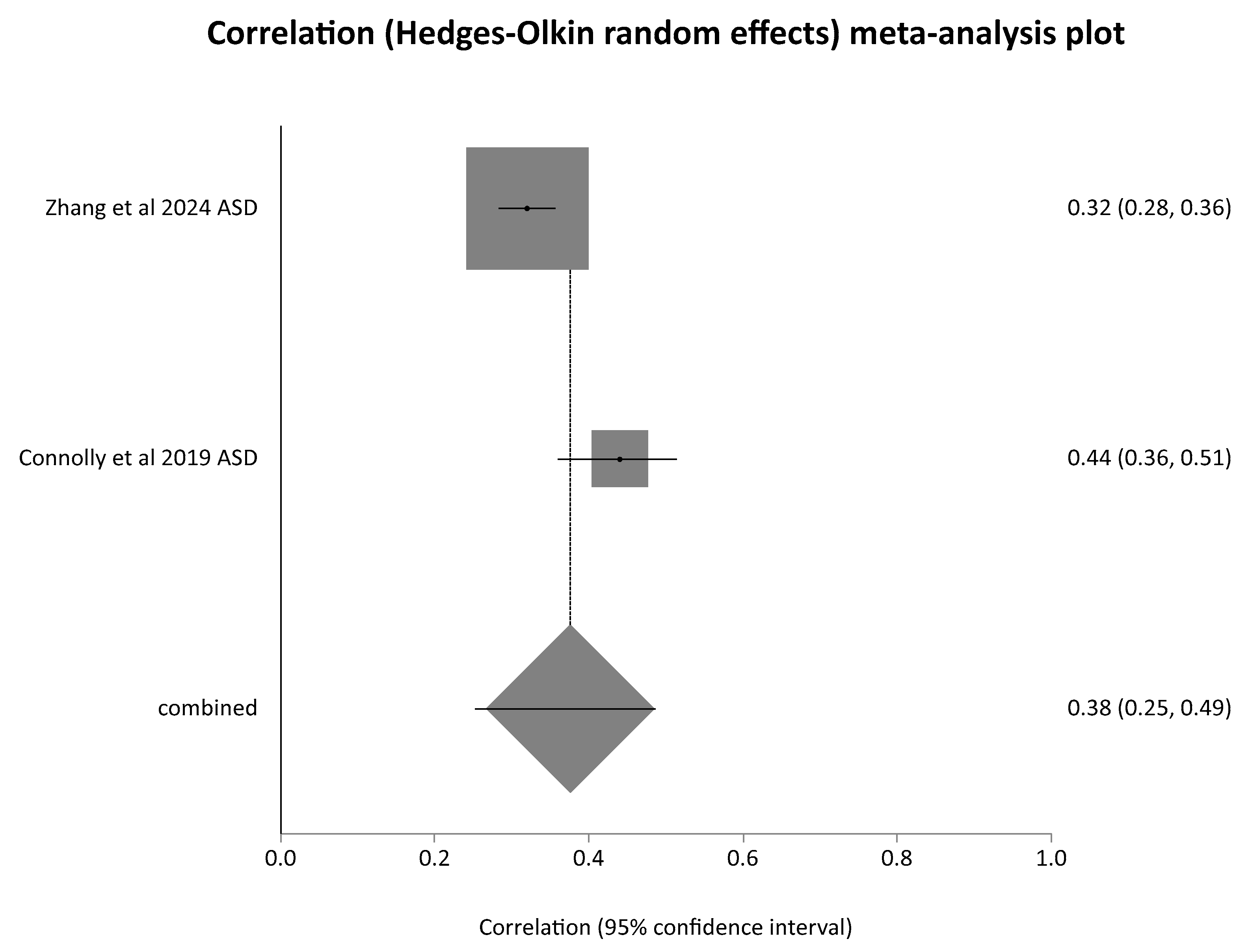
Meta-analysis of ICC of SRSS scores revealed a pooled correlation = 0.378 (95% CI = 0.289 to 0.461) which was statistically significant with a Z (test correlation differs from 0) = 7.76, p < 0.0001. This meta-analysis included both studies of families without an offspring with autistic spectrum disorder (ASD) (in figure 1 designated as “no ASD” behind the year of publication) and those with an offspring with ASD (designated in the forest plot of figure 1 as “ASD” behind the year of publication). This may account for some of the substantial heterogeneity detected which was reflected in a Cochran Q = 23.985 (df = 7) P = 0.0011, I² (inconsistency) = 70.8% (95% CI = 23.3% to 84.2%). In a separate meta-analysis of studies reporting a Spearman’s correlation co-efficient (both studies for families with offspring with ASD) a pooled correlation coefficient of 0.375 (95% CI = 0.252 to 0.487) was noted with a Z (test correlation differs from 0) = 5.648006 P < 0.0001. The heterogeneity of study results was considerable with a-Cochran Q = 7.061587 (df = 1) P = 0.0079 and an I² (inconsistency) = 85.8% .
Figure 2.
Meta-analysis of studies reporting intra-class correlation co-efficients of spouse pairs Social Responsiveness Scale Scores for adults.
Figure 2.
Meta-analysis of studies reporting intra-class correlation co-efficients of spouse pairs Social Responsiveness Scale Scores for adults.
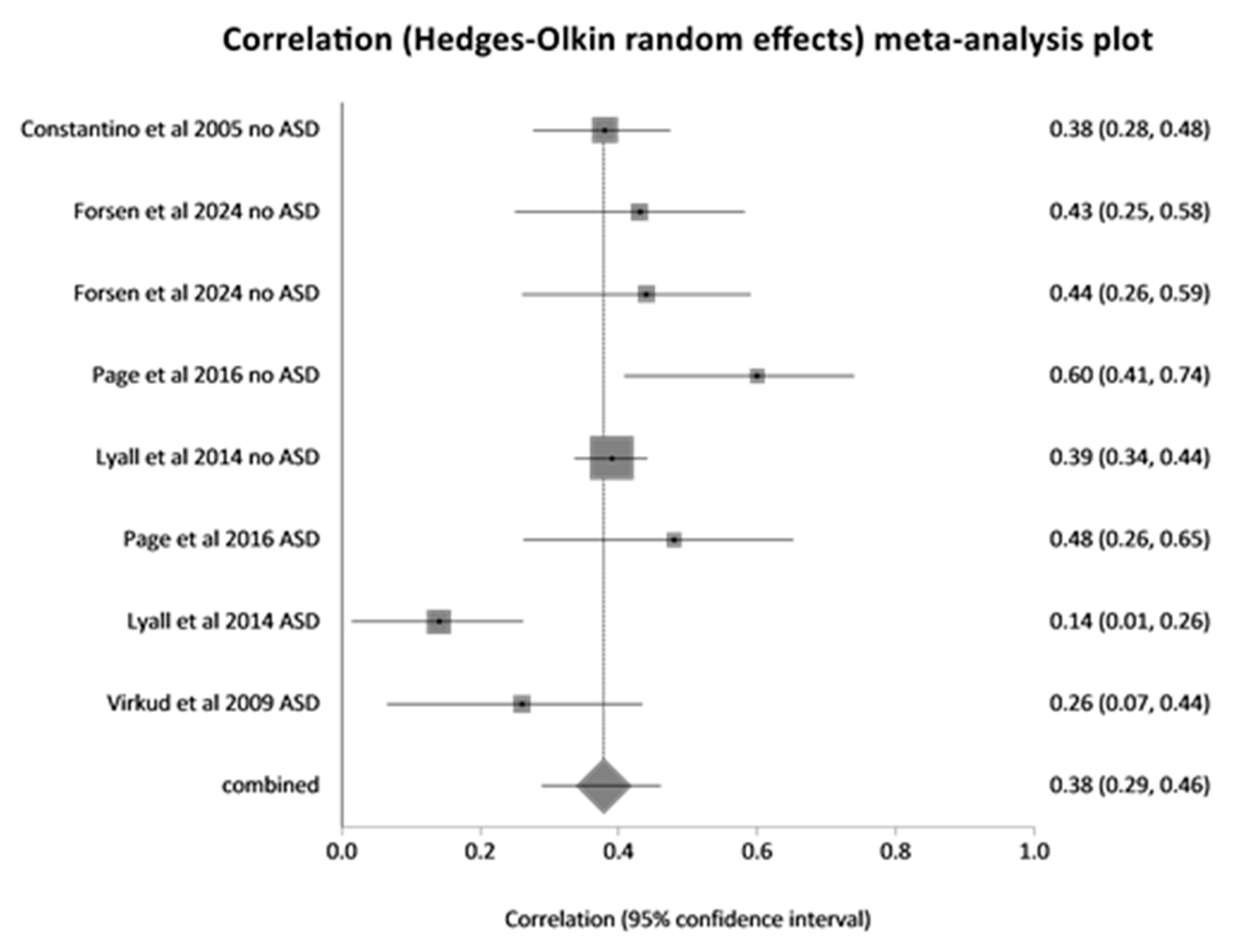
Figure 3.
Meta-analysis of Spearman’s correlation cofficients of Social Responsiveness Scale scores of spouses.
Figure 3.
Meta-analysis of Spearman’s correlation cofficients of Social Responsiveness Scale scores of spouses.
Correlation ofphenotype subgroups of the Social Responsiveness Scales
In the two studies reporting on correlation of subdomains of the social responsiveness scales [30,32] there was no evidence for any of the subdomains for the SRS being differently correlated to others between spouse pairs.
Correlation of genotype data in parents of children with autistic spectrum disorder
Table 2 lists the results of studies detailing attempts at investigating evidence for correlation of genotypic characteristics of spouses of children with autistic spectrum disorder. Using polygenic risk scores for ASD derived from differences in single-nucleotide polymorphisms no genetic evidence of assortative mating was found in 3 studies including 7067 spouse pairs with one autistic child [30,32,39]. One study group of 1092 spouse pairs of the Autism Genome project [32] demonstrated a significant spousal correlation between the principal components using genome-wide single nucleotide polymorphism data. The spouse pairs of this study had in 62% more than one offspring with ASD as opposed to all the other study likely accounting for an increased burden of ASD associated gene polymorphism in both spouses resulting in a significant correlation.
Reporting biases
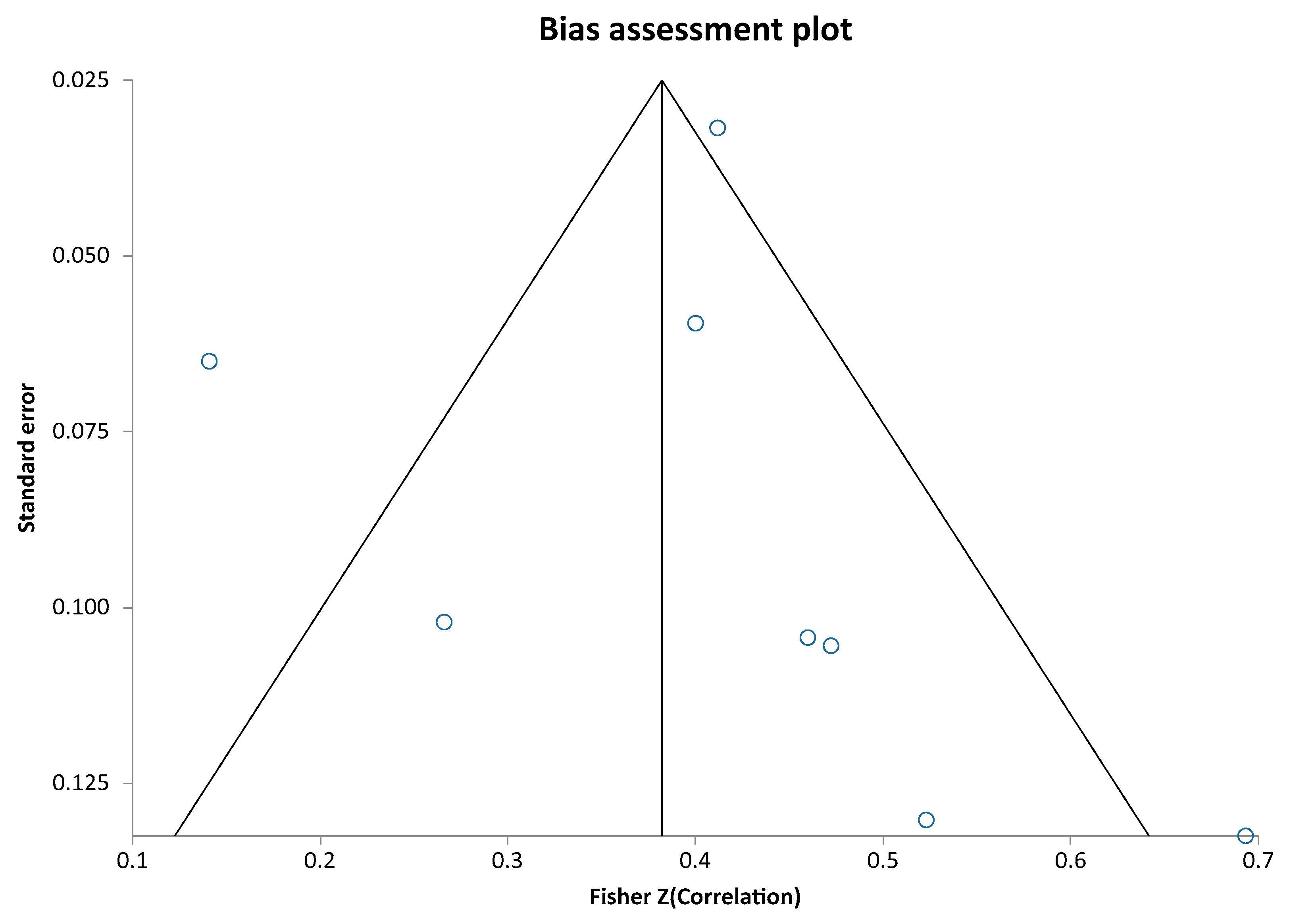
For the meta-analysis of the intra-class correlation coefficients analysis of reporting biases revealed a Begg-Mazumdar test: Kendall's tau= 0.428571, P = 0.1789 and a non-significant Egger test result with a bias = 0.5240655053464733 (95% CI = -2.9882532201752032 to 4.0363842308681495) P = 0.7276 (see Bias assessment plot of figure 3) indicating that there was no evidence of reporting bias.
Figure 4.
Fisher Z correlation score plotted against the respective standard error value Subgroup analysis:.
Figure 4.
Fisher Z correlation score plotted against the respective standard error value Subgroup analysis:.
Meta-analysis of intraclass correlation co-efficients for social responsiveness scale scores (SRSS) for study groups without known autistic spectrum disorders in parents or offspring (1526 spouse pairs) showed a pooled ICC of 0.40 (95% CI 0.35 to 0.46) with a Z-statistic of 13.42: p<0.001. And for study groups with known autistic spectrum disorder in offspring (401 spouse pairs) a pooled ICC of 0.278 (95% CI 0.08 to 0.46) with a Z-statistic of 2.723: p=0.006.Comparison of ICC coefficients for SRSS between groups with and without ASD as offspring revealed a Z score of 190 indicating a highly significant difference: P<0.0001 indicating a lower correlation of SRSS between parents of one or more children with autistic spectrum disorder compared to parents not chosen for having offspring with this disorder.
Studies investigating the relationship of correlation of parental social responsiveness scale scores with autistic spectrum severity in offspring
Five studies detailed in table 1 (28, 30, 33, 34, 36] investigated correlation of parental social responsiveness scale score with severity of autism spectrum disorder in offspring. The key finding in the study of Lyall et al [34] was that 12% of offspring with ASD versus 6% of controls had concordantly elevated parent scores (p<0.001) ; liability to ASD was increased by approximately 90% among children with concordantly elevated parent scores (OR=1.85, 95% CI 1.08, 3.16) and by approximately 50% when either parent’s score was elevated (OR=1.52, 95% CI 1.11, 2.06). This finding was reproducible in the study by Constantino et al [28] where the mean SRS scores for the offspring (n =64 twins) of parents whose SRS scores both fell in the top quartile of their respective distributions (for parents in this sample) and were substantially higher (by approximately 1.5 standard deviations) than those whose parents fell in any other SRS profile. Of these 64 children, 4 (from 4 different families) had SRS scores at or above 80 (i.e., within or above 1 standard deviation of the mean SRS score for children with PDD-NOS, in comparison to 3 such children (from 3 different families) in the entire remainder of the sample (n = 506 twins; Fisher’s exact p <0.004). Only 3 of the parents of these clinical-level-affected offspring had SRS scores at or above 80. In another study [33] concordant elevations of mothers and fathers (i.e., both parents in upper quartile of the sample distribution) were observed more among ASD families than among non-ASD families (16.1 vs. 3.3 %, Fisher’s exact, p = 0.03), and the former substantially exceeded the proportion expected by chance, which was 6.25 %. These results were unchanged when restricting the analysis to data from one or the other specific language versions of the SRS-2 (Spanish vs. English). In the study by Virkud et al. [36] there was no significant difference in spousal correlations between families with a single child with ASD (SA) and families with multiple members affected by ASD (MA). Concordantly-elevated (upper quartile) spousal pairs were not significantly more common in MA versus SA families. In the study by Zhang et al. [30] there were no significant differences in the degree of spousal correlations for the quantitative autistic traits between groups with offspring with autism with versus without intellectual disability.
Autism prevalence in countries with assortative mating leading to marriages versus in countries with arranged marriages
Table 3 lists studies of prevalence of autism spectrum disorder separate for countries known to have arranged marriages in the majority and countries with assortative mating determining marriages. Population based studies on autism spectrum disorder prevalence were identified for the following countries with predominantly assortative mating determining marriage for the United States of America, Mexico, Venezuela, Aruba, The United Kingdom, France, Spain, Denmark, Poland, Sweden, Norway, Finland, Greece, Israel, Lebanon, Qatar, Oman, China, Taiwan, Australia and Faroe Islands including data on 7072330 participants with 44660 identified with autistic spectrum disorder between the years 2008 and 2022 giving a pooled prevalence rate for autism spectrum disorder of 63.1 per 10000 of population in these countries.
Studies in countries with predominantly arranged marriages included data from India, Bangladesh, Sri Lanka, Nepal, and Saudi Arabia from 111297 participants with 157 diagnosed with autistic spectrum disorder resulting in a pooled prevalence rate for autistic spectrum disorder of 14.1 per 10000 in those countries. The difference in prevalence rates was highly significant giving a risk ratio of autism with a culture of assortative mating versus one without of 4.4 (95% CI 3.8 to 5.2) (p<0.0001).
Certainty of evidence
Regarding the certainty of the evidence for assortative mating we came to the following conclusion: Across different populations in and outside the USA and using different analysis methods there was evidence of significant assortative mating. The significant heterogeneity of study results indicates a degree of inconsistency and there were concerns about risk of bias as studies were based on self and spouses instead of expert report regarding Social Responsiveness Scoring. Regarding phenotypical assortative mating we judged the certainty of evidence therefore as low. Regarding genotypical assortative mating we rated the certainty that there is no genetic assortative mating as very low because there is inconsistency, imprecision and indirectness of the evidence.
Quality assessment
Using the AXIS tool for assessment of all studies (n=14) reporting on phenotypic assortative mating 11were of high, 2 of fair and one of low quality. Of the studies reporting on genotypic assortative mating 3 were of high and one of low quality. Comparison of AXIS tool scores between studies included in the meta analyses and with versus without offspring with ASD revealed a high median AXIS tool score of 14 for both types of studies without difference between groups (p=0.643).
Discussion
General interpretation
This systematic review demonstrated that there is assortative mating following social responsiveness score scale scores in spouses with and without offspring with autistic spectrum disorder. The fact that the pooled correlation of scores with and without offspring with autistic spectrum was significantly different may reflect that in families without offspring with autistic spectrum disorder there may have been a higher percentage of spouses who both scored their partner with low scores for autism related items as they both had no features of autistic spectrum disorder while spouses with offspring with autistic spectrum disorder may have both had increased scores consistent with autistic spectrum disorder in different domains of the scoring system reducing correlation. The genetic load causing autistic spectrum disorder will increase in the offspring if spouses have different domains affected adding to the overall phenotypic severity in the offspring. Three studies which investigated the risk of increased SRS scores in offspring of both parents with correlating high SRS scores found higher SRS scores in offspring if both parents had more and significantly correlating autistic features. This illustrates that genetic load from both parents is additive in the offspring but was as one study showed not necessarily associated with more learning difficulties. The few data on subdomain correlation in social responsiveness scales between spouses did not show any particular domain correlating more than others but the number of studies was small.
Our results of a lower prevalence of autistic spectrum disorder in counties with a lower prevalence of assortative mating due to a dominance of arranged marriages was confirmed in the Global Burden of Disease study from 2021 on bigger data sets: In the subset comprising the largest data collections from countries with arranged marriages represented by the countries of South Asia which include Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka the prevalence of autistic spectrum disorder was 68.6 per 10000 (uncertainty interval 57.6 to 80.2) while in Western Europe and North America it was 89.6 (uncertainty interval 75.1 to 105.4) and 109.7 (uncertainty interval 91.9 to 129.6) respectively [22]. The lack of denominators for the pooled prevalence data from the Global Burden of Disease Study made a statistical comparison of data impossible. The higher prevalence rates reported in the Global Burden of Disease Study compared to this systematic review may have been due to the fact that we included only carefully designed population based studies using stringent criteria with validated tools in all participants.
Limitations
The Social Responsiveness Scale most studies on assortative mating used as a tool is heavily weighted toward social impairments and most of the data in previous studies were generated among samples with IQ >70. The SRS has not been evaluated systematically among populations with an intellectual disability [72]. The significant heterogeneity of study results may reflect bias as studies were based on self and spouses instead of expert report regarding Social Responsiveness Scoring. Investigations into genotypical assortative mating were characterized by inconsistency, imprecision and indirectness of the evidence and there was a lack of ranking of genes according to degree of association with ASD and a lack of focus on investigating association of common high impact genetic polymorphisms and guidance by a sample size calculation providing adequate statistical power to detect significant correlations between spouses.
Implications for practice, policy and future research
Despite assortative mating offering an explanation for the increase in prevalence of autistic spectrum disorder the rapid increase is difficult to understand in view of the fact that autism in the offspring reduces the number of further offspring within a family [73]. Future studies need to explore the dynamics of an increase in assortative mating promoted by information technology (e.g. internet facilitated dating), which enables distant people with “matching” personal characteristics to find each other. The impact of this assortative mating across distances needs to be investigated: For evolutionary survival of the genes generating a less reproductive phenotype we hypothesize that there needs to be a protective gene constellation mitigating phenotypical features impairing reproduction which has co-evolved with genes encoding autistic spectrum disorder features within a specific group of people, which has co-evolved of a long period of history. This implies that offspring of spouses with a similar and elevated SRS score but different genetic (for example ethnic) background should have a higher risk of a SRS score above both parents SRS score compared to offspring of spouses of the same genetic (ethnic) background. This is because the process of meiosis of the parental genes would entail a higher risk of losing one of the protective allels evolved within a specific genetically more similar (e.g. ethnic) group. This hypothesis could be tested in future epidemiological and genetic studies. Investigations could hereby clarify whether assortative mating within a family or within a group of ethnically similar ancestry is associated with less severe autism in offspring compared to assortative mating between genetically less related families. Such research needs to correct for consanguineous unions (e.g. first cousins) which by themselves could lead to an increased risk of autosomal recessive gene mutations producing neurodevelopmental disorders with an autistic spectrum phenotype. There is an urgent need to investigate mating of which phenotypical features and which genes contributing to an autistic spectrum disorder phenotype are associated with learning difficulties in the offspring. Future research needs to investigate whether the findings of Nordsletten et al [38] that people with clinically obvious autistic spectrum disorder are attracted to each other more than people with any other neurocognitive condition are reproducible in other ethnic groups without obstacles to assortative mating. If reproducible the features guiding this attraction need to be defined. Preference for “sameness” and anxiety triggered by unpredictability of behaviour are candidates to be explored.
Spousal assortment can occur on autistic spectrum disorder features without the persons having them being aware. To avoid severe autism in the offspring partners could be guided by improved informed choice provided through SRS scores which could be used to assess a future spouse similar to screening taking already place for conditions like thalassemia and others before starting a family.
Registration and protocol
The protocol for this systematic review was pre-registered in the International prospective register of systematic reviews PROSPERO registration number: CRD420251141431
Author’s contribution
Michael Eisenhut has devised the study, contributed to the literature search, done all data analysis and interpretation and written the manuscript. Anjana Jeevan has participated in the protocol generation, performed literature search and selection of included articles and critically appraised the manuscript.
Funding
Financial or non-financial support was not involved in the conduct of this study.
Informed Consent Statement
Not applicable as only already published data were included in this systematic review.
Data availability Statement
Availability of data, code and other materials: The data used for this systematic review are documented in the publications reviewed.
Competing interests
There are no competing interests
Appendix 1. PRISMA 2020 Checklist
| Section and Topic | Item # | Checklist item | Location where item is reported |
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | Page 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | Page 2 and 3 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | Page 4 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | Page 6 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Page 7 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | Page 8 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Page 8 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | Page 8 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | Page 8 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g. for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | Page 8 |
| 10b | List and define all other variables for which data were sought (e.g. participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | Page 8 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | Page 8 and 9 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g. risk ratio, mean difference) used in the synthesis or presentation of results. | Page 9 |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g. tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | Page 9 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | Page 9 | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | Page 9 | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | Page 9 | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g. subgroup analysis, meta-regression). | Page 9 | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | Not applicable | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | Page 9 and 10 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | Page 11 |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Page 11, 13 and 31 to 41 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | Not applicable | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Page 13 to 19 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | Page 13 to 20 and 33 to 41 |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g. confidence/credible interval), ideally using structured tables or plots. | Page 13 to 20 |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | Page 13 to 23, 27 and 28 |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g. confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | Page 21 and 23 | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | Page 30 | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | Not applicable | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | Not applicable |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | Page 41 |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | Page 42 |
| 23b | Discuss any limitations of the evidence included in the review. | Page 44 | |
| 23c | Discuss any limitations of the review processes used. | Page 44 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | Page 44 and 45 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | Page 46 |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | Page 46 | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | Not applicable | |
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | Not applicable |
| Competing interests | 26 | Declare any competing interests of review authors. | Not applicable |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | Not applicable |
| From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/ | |||
References
- Lord, C.; Elsabbagh, M.; Baird, G.; Veenstra-Vanderweele, J. Autism spectrum disorder. Lancet 2018, 392(10146), 508–520. [Google Scholar] [CrossRef]
- Hirota, T.; King, B.H. Autism Spectrum Disorder: A Review. JAMA 2023, 329(2), 157–168. [Google Scholar] [CrossRef] [PubMed]
- Micai, M.; Fatta, L.M.; Gila, L.; Caruso, A.; Salvitti, T.; Fulceri, F.; Ciaramella, A.; D'Amico, R.; Del Giovane, C.; Bertelli, M.; Romano, G.; Schünemann, H.J.; Scattoni, M.L. Prevalence of co-occurring conditions in children and adults with autism spectrum disorder: A systematic review and meta-analysis. Neurosci Biobehav Rev 2023, 155, 105436. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.; Le Couteur, A.; Gottesman, I.; Bolton, P.; Simonoff, E.; Yuzda, E.; Rutter, M. Autism as a strongly genetic disorder: evidence from a British twin study. Psychol Med 1995, 25(1), 63–77. [Google Scholar] [CrossRef]
- Kim, J.Y.; Son, M.J.; Son, C.Y.; Radua, J.; Eisenhut, M.; Gressier, F.; Koyanagi, A.; Carvalho, A.F.; Stubbs, B.; Solmi, M.; Rais, T.B.; Lee, K.H.; Kronbichler, A.; Dragioti, E.; Shin, J.I.; Fusar-Poli, P. Environmental risk factors and biomarkers for autism spectrum disorder: an umbrella review of the evidence. Lancet Psychiatry 2019, 6(7), 590–600. [Google Scholar] [CrossRef]
- Zheng, Z.; Zhang, L.; Li, S.; et al. Association among obesity, overweight and autism spectrum disorder: a systematic review and meta-analysis. Sci Rep 2017, 7, 11697. [Google Scholar] [CrossRef]
- Hong, M.; Lee, S.M.; Park, S.; Yoon, S.J.; Kim, Y.E.; Oh, I.H. Prevalence and Economic Burden of Autism Spectrum Disorder in South Korea Using National Health Insurance Data from 2008 to 2015. J Autism Dev Disord 2020, 50(1), 333–339. [Google Scholar] [CrossRef] [PubMed]
- Lai, D.C.; Tseng, Y.C.; Hou, Y.M.; Guo, H.R. Gender and geographic differences in the prevalence of autism spectrum disorders in children: analysis of data from the national disability registry of Taiwan. Res Dev Disabil 2012, 33(3), 909–915. [Google Scholar] [CrossRef]
- Wong, V.C.; Hui, S.L. Epidemiological study of autism spectrum disorder in China. J Child Neurol 2008, 23(1), 67–72. [Google Scholar] [CrossRef]
- Plubrukarn, R.; Piyasil, V.; Moungnoi, P.; Tanprasert, S.; Chutchawalitsakul, V. Trend study of autistic spectrum disorders at Queen Sirikit National Institute of Child Health. J Med Assoc Thai 2005, 88, 891–897. [Google Scholar]
- van Bakel, M.M.; Delobel-Ayoub, M.; Cans, C.; Assouline, B.; Jouk, P.S.; Raynaud, J.P.; Arnaud, C. Low but increasing prevalence of autism spectrum disorders in a French area from register-based data. J Autism Dev Disord 2015, 45(10), 3255–3261. [Google Scholar] [CrossRef]
- Jiang, Y.; Bolnick, D.I.; Kirkpatrick, M. Assortative mating in animals. Am Nat 2013, 181(6), E125-138. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Hammer, J. Parents of children with Asperger syndrome: what is the cognitive phenotype? J Cogn Neurosci 1997, 9, 548–554. [Google Scholar] [CrossRef]
- Baron-Cohen, S. The hyper-systemizing, assortative mating theory of autism. Prog Neuropsychopharmacol Biol Psychiatry. 2006, 30(5), 865–872. [Google Scholar] [CrossRef]
- Available online: https://en.wikipedia.org/wiki/Arranged_marriage (accessed on 20.11.2025).
- Islam, M.K.; Haque, M.R.; Hossain, M.B. Regional variations in child marriage in Bangladesh. J Biosoc Sci 2016, 48(5), 694–708. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M. Determinates of early marriage in Bangladesh: an evidence of the nationally representative survey. Int J Sociol Anthropol 2017, 9(1), 1–7. [Google Scholar]
- Manandhar, N.; Joshi, S.K. Health co-morbidities and early marriage in women of a rural area of nepal: A descriptive cross-sectional study. J Nepal Med Assoc 2020, 58(230), 780–783. [Google Scholar] [CrossRef] [PubMed]
- Raj, A.; Saggurti, N.; Balaiah, D.; Silverman, J.G. Prevalence of child marriage and its effect on fertility and fertility-control outcomes of young women in India: a cross-sectional, observational study. Lancet (London, England). 2009, 373(9678), 1883–1889. [Google Scholar] [CrossRef]
- Available online: https://culturalatlas.sbs.com.au/saudi-arabian-culture/saudi-arabian-culture-family (accessed on 20.11.2025).
- Issac, A.; Halemani, K.; Shetty, A.; Thimmappa, L.; Vijay, V.R.; Koni, K.; Mishra, P.; Kapoor, V. The global prevalence of autism spectrum disorder in children: a systematic review and meta-analysis. Osong Public Health Res Perspect. 2025, 16(1), 3–27. [Google Scholar] [CrossRef]
- Global Burden of Disease Study 2021 Autism Spectrum Collaborators. The global epidemiology and health burden of the autism spectrum: findings from the Global Burden of Disease Study 2021. Lancet Psychiatry 2025, 12(2), 111–121.
- Yang, F; Chen, R; Xiong, J; Liu, B. Disease Burden of Autism Spectrum Disorder and Attention - Deficit/Hyperactivity Disorder in the 0-14 Age Group across 204 Countries and Regions from 1990 To 2021. Child Psychiatry Hum Dev 2025. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; Chou, R.; Glanville, J.; Grimshaw, J.M.; Hróbjartsson, A.; Lalu, M.M.; Li, T.; Loder, E.W.; Mayo-Wilson, E.; McDonald, S.; McGuinness, L.A.; Stewart, L.A.; Thomas, J.; Tricco, A.C.; Welch, V.A.; Whiting, P.; Moher, D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Brignardello-Petersen, R.; Guyatt, G.H. Assessing the certainty of the evidence in systematic reviews: importance, process, and use. Am J Epidemiol. 2025, 194(6), 1681–1686. [Google Scholar] [CrossRef]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; et al. Development of a critical appraisal tool to assess the quality of crosssectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef]
- Rovito, M.J.; Bruzzone, A.; Lee, E.; López Castillo, H.; Talton, W.; Taliaferro, L.; Falk, D. Assessing Health-Related Quality of Life Among Survivors of Testicular Cancer: A Systematic Review. Am J Mens Health 2021, 15(1), 1557988320982184. [Google Scholar] [CrossRef]
- Constantino, J.N.; Todd, R.D. Intergenerational transmission of subthreshold autistic traits in the general population. Biol Psychiatry 2005, 57(6), 655–660. [Google Scholar] [CrossRef]
- Forsen, E.; Marrus, N.; Joyce, J.; Zhang, Y.; Constantino, J.N. Mate selection and current trends in the prevalence of autism. Mol Autism 2024, 15(1), 29. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J., Weissenkampen, J.D., Kember, R.L.; iPSYCH Consortium; Grove, J., Børglum, A.D., Robinson, E.B., Brodkin, E.S., Almasy, L., Bucan, M., Sebro, R. Phenotypic and ancestry-related assortative mating in autism. Mol Autism, 2024, 15(1), 27. [CrossRef]
- Smolen, C.; Jensen, M.; Dyer, L.; Pizzo, L.; Tyryshkina, A.; Banerjee, D.; Rohan, L.; Huber, E.; El Khattabi, L.; Prontera, P.; Caberg, J.H.; Van Dijck, A.; Schwartz, C.; Faivre, L.; Callier, P.; Mosca-Boidron, A.L.; Lefebvre, M.; Pope, K.; Snell, P.; Lockhart, P.J.; Castiglia, L.; Galesi, O.; Avola, E.; Mattina, T.; Fichera, M.; Luana Mandarà, G.M.; Bruccheri, M.G.; Pichon, O.; Le Caignec, C.; Stoeva, R.; Cuinat, S.; Mercier, S.; Bénéteau, C.; Blesson, S.; Nordsletten, A.; Martin-Coignard, D.; Sistermans, E.; Kooy, R.F.; Amor, D.J.; Romano, C.; Isidor, B.; Juusola, J.; Girirajan, S. Assortative mating and parental genetic relatedness contribute to the pathogenicity of variably expressive variants. Am J Hum Genet 2023, 110(12), 2015–2028. [Google Scholar] [CrossRef]
- Connolly, S.; Anney, R.; Gallagher, L.; Heron, E.A. Evidence of Assortative Mating in Autism Spectrum Disorder. Biol Psychiatry 2019, 86(4), 286–293. [Google Scholar] [CrossRef] [PubMed]
- Page, J.; Constantino, J.N.; Zambrana, K.; Martin, E.; Tunc, I.; Zhang, Y.; Abbacchi, A.; Messinger, D. Quantitative autistic trait measurements index background genetic risk for ASD in Hispanic families. Mol Autism 2016, 7(1), 39. [Google Scholar] [CrossRef] [PubMed]
- Lyall, K.; Constantino, J.N.; Weisskopf, M.G.; Roberts, A.L.; Ascherio, A.; Santangelo, S.L. Parental social responsiveness and risk of autism spectrum disorder in offspring. JAMA Psychiatry 2014, 71(8), 936–942. [Google Scholar] [CrossRef] [PubMed]
- van Steijn, D.J.; Richards, J.S.; Oerlemans, A.M.; de Ruiter, S.W.; van Aken, M.A.; Franke, B.; Buitelaar, J.K.; Rommelse, N.N. The co-occurrence of autism spectrum disorder and attention-deficit/hyperactivity disorder symptoms in parents of children with ASD or ASD with ADHD. J Child Psychol Psychiatry 2012, 53(9), 954–963. [Google Scholar] [CrossRef] [PubMed]
- Virkud, Y.V.; Todd, R.D.; Abbacchi, A.M.; Zhang, Y.; Constantino, J.N. Familial aggregation of quantitative autistic traits in multiplex versus simplex autism. Am J Med Genet B Neuropsychiatr Genet 2009, 150B(3), 328–334. [Google Scholar] [CrossRef]
- Hoekstra, R.A.; Bartels, M.; Verweij, C.J.; Boomsma, D.I. Heritability of autistic traits in the general population. Arch Pediatr Adolesc Med 2007, 161(4), 372–377. [Google Scholar] [CrossRef] [PubMed]
- Nordsletten, A.E.; Larsson, H.; Crowley, J.J.; Almqvist, C.; Lichtenstein, P.; Mataix-Cols, D. Patterns of Nonrandom Mating Within and Across 11 Major Psychiatric Disorders. JAMA Psychiatry 2016, 73(4), 354–361. [Google Scholar] [CrossRef]
- Weiner, D.J., Wigdor, E.M., Ripke, S., Walters, R.K., Kosmicki, J.A., Grove, J., Samocha, K.E., Goldstein, J.I., Okbay, A., Bybjerg-Grauholm, J., Werge, T., Hougaard, D.M., Taylor, J.; iPSYCH-Broad Autism Group; Psychiatric Genomics Consortium Autism Group; Skuse, D., Devlin, B., Anney, R., Sanders, S.J., Bishop, S., Mortensen, P.B., Børglum, A.D., Smith, G.D., Daly, M.J., Robinson, E.B. Polygenic transmission disequilibrium confirms that common and rare variation act additively to create risk for autism spectrum disorders. Nat Genet, 2017 49(7),978-985.
- Shaw, K.A.; Williams, S.; Patrick, M.E; et al. Prevalence and Early Identification of Autism Spectrum Disorder Among Children Aged 4 and 8 Years — Autism and Developmental Disabilities Monitoring Network, 16 Sites, United States, 2022. MMWR Surveill Summ 2025, 74(No. SS-2), 1–22. [Google Scholar] [CrossRef]
- van Balkom, I.D.; Bresnahan, M.; Vogtländer, M.F.; van Hoeken, D.; Minderaa, R.B.; Susser, E.; Hoek, H.W. Prevalence of treated autism spectrum disorders in Aruba. J Neurodev Disord 2009, 1(3), 197–204. [Google Scholar] [CrossRef]
- Chaaya, M.; Saab, D.; Maalouf, F.T.; et al. Prevalence of Autism Spectrum Disorder in Nurseries in Lebanon: A Cross Sectional Study. J Autism Dev Disord 2016, 46, 514–522. [Google Scholar] [CrossRef]
- Raz, R.; Weisskopf, M.G.; Davidovitch, M.; et al. Differences in Autism Spectrum Disorders Incidence by Sub-Populations in Israel 1992–2009: A Total Population Study. J Autism Dev Disord. 2015, 45, 1062–1069. [Google Scholar] [CrossRef]
- Chien, I-C.; Lin, C-H.; Chou, Y-J.; Chou, P. Prevalence and Incidence of Autism Spectrum Disorders Among National Health Insurance Enrollees in Taiwan from 1996 to 2005. Journal of Child Neurology 2011, 26(7), 830–834. [Google Scholar] [CrossRef]
- Sun, X.; Allison, C.; Wei, L.; et al. Autism prevalence in China is comparable to Western prevalence. Mol Autism 2019, 10, 7. [Google Scholar] [CrossRef]
- Zhou, H.; Xu, X.; Yan, W.; et al. Prevalence of autism spectrum disorder in China: a nationwide multi-center population-based study among children aged 6 to 12 years. Neurosci Bull 2020, 36, 961–971. [Google Scholar] [CrossRef]
- Fombonne, E.; Marcin, C.; Manero, A.C.; et al. Prevalence of Autism Spectrum Disorders in Guanajuato, Mexico: The Leon survey. J Autism Dev Disord 2016, 46, 1669–1685. [Google Scholar] [CrossRef]
- Montiel-Nava, C.; Peña, J. A. Epidemiological findings of pervasive developmental disorders in a Venezuelan study. Autism 2008, 12(2), 191–202. [Google Scholar] [CrossRef] [PubMed]
- Alshaban, F.; Aldosari, M.; Al-Shammari, H; et al. Prevalence and correlates of autism spectrum disorder in Qatar: a national study. J Child Psychol Psychiatry 2019, 60, 1254–1268. [Google Scholar] [CrossRef]
- Al-Mamri, W.; Idris, A.B.; Dakak, S.; et al. Revisiting the prevalence of autism spectrum disorder among Omani children: a multicentre study. Sultan Qaboos Univ Med J 2019, 19, e305–309. [Google Scholar] [CrossRef]
- Nygren, G.; Cederlund, M.; Sandberg, E.; et al. The Prevalence of Autism Spectrum Disorders in Toddlers: A Population Study of 2-Year-Old Swedish Children. J Autism Dev Disord 2012, 42, 1491–1497. [Google Scholar] [CrossRef] [PubMed]
- Idring, S.; Lundberg, M.; Sturm, H.; et al. Changes in prevalence of autism spectrum disorders in 2001-2011: findings from the Stockholm youth cohort. J Autism Dev Disord 2015, 45, 1766–1773. [Google Scholar] [CrossRef] [PubMed]
- Morales-Hidalgo, P.; Roigé-Castellví, J.; Hernández-Martínez, C.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Spanish School-Age Children. J Autism Dev Disord 2018, 48, 3176–3190. [Google Scholar] [CrossRef]
- Fuentes, J.; Basurko, A.; Isasa, I.; et al. The ASDEU autism prevalence study in northern Spain. Eur Child Adolesc Psychiatry 2021, 30, 579–589. [Google Scholar] [CrossRef]
- Skonieczna-Zydecka, K; Gorzkowska, I; Pierzak-Sominka, J; et al. The prevalence of autism spectrum disorders in West Pomeranian and Pomeranian Regions of Poland. J Appl Res Intellect Disabil 2017, 30, 283–289. [Google Scholar] [CrossRef]
- Hansen, S.N.; Schendel, D.E.; Parner, E.T. Explaining the Increase in the Prevalence of Autism Spectrum Disorders: The Proportion Attributable to Changes in Reporting Practices. JAMA Pediatr 2015, 169(1), 56–62. [Google Scholar] [CrossRef]
- Posserud, M.; Lundervold, A.J.; Lie, S.A.; et al. The prevalence of autism spectrum disorders: impact of diagnostic instrument and non-response bias. Soc Psychiatry Psychiatr Epidemiol 2010, 45, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Mattila, M.L.; Kielinen, M.; Linna, S.L.; Jussila, K.; Ebeling, H.; Bloigu, R.; Joseph, R.M.; Moilanen, I. Autism spectrum disorders according to DSM-IV-TR and comparison with DSM-5 draft criteria: an epidemiological study. J Am Acad Child Adolesc Psychiatry 2011, 50(6), 583–592. [Google Scholar] [CrossRef] [PubMed]
- van Bakel, M.M.E.; Delobel-Ayoub, M.; Cans, C.; et al. Low but Increasing Prevalence of Autism Spectrum Disorders in a French Area from Register-Based Data. J Autism Dev Disord 2015, 45, 3255–3261. [Google Scholar] [CrossRef]
- Thomaidis, L.; Mavroeidi, N.; Richardson, C.; Choleva, A.; Damianos, G.; Bolias, K.; Tsolia, M. Autism Spectrum Disorders in Greece: Nationwide Prevalence in 10–11 Year-Old Children and Regional Disparities. Journal of Clinical Medicine 2020, 9(7), 2163. [Google Scholar] [CrossRef]
- Williams, E.; Thomas, K.; Sidebotham, H.; et al. Prevalence and characteristics of autistic spectrum disorders in the ALSPAC cohort. Dev Med Child Neurol 2008, 50, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Randall, M.; Sciberras, E.; Brignell, A; et al. Autism spectrum disorder: Presentation and prevalence in a nationally representative Australian sample. Australian & New Zealand Journal of Psychiatry 2015, 50(3), 243–253. [Google Scholar]
- Kočovská, E.; Biskupstø, R.; Carina Gillberg, I.; et al. The Rising Prevalence of Autism: A Prospective Longitudinal Study in the Faroe Islands. J Autism Dev Disord 2012, 42, 1959–1966. [Google Scholar] [CrossRef]
- Al-Zahrani, A. Prevalence and clinical characteristics of autism spectrum disorders in school-age children in Taif-KSA. Int J Med Sci Public Health 2013, 2, 578–582. [Google Scholar] [CrossRef]
- Akhter, S.; Hussain, A.H.; Shefa, J.; et al. Prevalence of autism spectrum disorder (ASD) among the children aged 18-36 months in a rural community of Bangladesh: a cross sectional study. F1000Res 2018, 7, 424. [Google Scholar] [CrossRef] [PubMed]
- Raina, S.K.; Chander, V.; Bhardwaj, A.K.; et al. Prevalence of autism spectrum disorder among rural, urban, and tribal children (1-10 years of age). J Neurosci Rural Pract 2017, 8, 368–374. [Google Scholar] [CrossRef]
- Rudra, A.; Belmonte, M.K.; Soni, P.K.; et al. Prevalence of autism spectrum disorder and autistic symptoms in a school-based cohort of children in Kolkata, India. Autism Res 2017, 10, 1597–1605. [Google Scholar] [CrossRef]
- Poovathinal, S.A.; Anitha, A.; Thomas, R.; et al. Prevalence of autism spectrum disorders in a semiurban community in south India. Ann Epidemiol 2016, 26, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Nair, K.S., George, R.L., Remya, V.R., P A R, Saji, C.V., Mullasseril. R.R., Shenoi, R.A., Nair, J., Krishna, R., K N K, Thomas, A., Varughese, D., Chandra, G., Mohanakumar, K.P., Rajamma, U. Prevalence Estimates of Neurodevelopmental Disorders (NDD) in a South Indian Population. Ann Neurosci 2025 Jul 11:09727531251348188. [CrossRef]
- Perera, H.; Wijewardena, K.; Aluthwelage, R. Screening of 18–24-Month-Old Children for Autism in a Semi-Urban Community in Sri Lanka. Journal of Tropical Pediatrics 2009, 55, 402–405. [Google Scholar] [CrossRef]
- Heys, M.; Gibbons, F.; Haworth, E.; et al. The estimated prevalence of autism in school-aged children living in rural Nepal using a population-based screening tool. J Autism Dev Disord 2018, 48, 3483–3498. [Google Scholar] [CrossRef]
- Norris, M.; Lecavalier, L. Screening accuracy of Level 2 autism spectrum disorder rating scales. A review of selected instruments. Autism 2010, 14(4), 263–284. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.J.; Windham, G.C.; Anderson, M.; Croen, L.A.; Grether, J.K.; Risch, N. Evidence of reproductive stoppage in families with autism spectrum disorder: a large, population-based cohort study. JAMA Psychiatry 2014, 71(8), 943–951. [Google Scholar] [CrossRef]
Table 2.
Characteristics of included studies regarding comparison of genotype in parents of children with autistic spectrum disorder.
Table 2.
Characteristics of included studies regarding comparison of genotype in parents of children with autistic spectrum disorder.
| First author and year | Study design | Population and sample | Comparison | Outcome measures | Key findings | Quality Assessment | Limitations |
| Zhang et al. 2024 [30] | Observational study | Family-based autism collections: the Simons Foundation Powering Autism Research for Knowledge (SPARK) (1575 families) and the Simons Simplex Collection (SSC) (2283 families). The reference ancestry population was a multi-ethnic population from the 1000 Genomes project. Autosomal SNPs only. |
Polygenic risk scores (PGS) based on single nucleotide polymorphisms comparing both parents and compared to a reference ancestry population . |
Correlation between PGS of spouses | No correlation of PGS | 16 | The restriction to autosomal SNP’s may have missed important allels on the x-chromosome. Only the top and bottom 200 SNPs were analysed. |
| Connolly et al. 2019 [32] | Observational study | 1092 spouse pairs of the Autism Genome Project | Kinship coefficients and spousal correlation between the principal components using genome-wide single nucleotide polymorphism data on trio families. |
Correlation between the principal components with comparison of the distribution of the kinship coefficients for spouses (mother/ father pairings) with the distribution of all other possible nonspouse pairings restricted to male/female pairings from the same ancestral background. The quantiles (from 0.001 to 0.999 in increments of 0.001) for the spouse pairs’ kinship coefficients were calculated and then mapped to the kinship coefficients for the nonspouse pairs; with the area under the deviation from a perfect correlation regression line (45 degrees indicating the degree of assortative mating |
Area under the curve 0.025 (95% CI 0.0110, 0.0389 indicating significant evidence of positive genetic assortative mating as spouses are more genetically similar than all possible nonspouse pairs | 14 | Only spouse pairs from the same ancestral population were included with similar proportions of ancestry to each other and to others in their population: The fact that this data base included families with more than one member s with autism may have increase the apparent assortative mating as parents who had both increased genetic burden would be over represented. The fact that all offspring had autism also increased apparent assortative mating for the same reason. |
| Connolly et al. 2019 [32] | Observational study | 1221 spouse pairs of the Simons Simplex Collection data | Kinship coefficients and spousal correlation between the principal components using genome-wide single nucleotide polymorphism data on trio families |
See above from the same first author | Area under the curve was equal to -0.0062 (95% CI = -0.0187, 0.0065) indicating that there was no evidence of genetic assortative mating in the SSC data set.. | 14 | The fact that all offspring had autism also increased apparent assortative mating for the same reason. |
| Weiner et al 2017[39] | Observational study | 3209 spouse pairs of European ancestry from the Psychiatric Genomics Consortium Autism Group (PGC ASD) sample Autism Group from California, Montreal and Boston and Philadelpia, USA | Polygenic Risk Score base on common variant genotype data from the largest available independent Genome-Wide Association Study including effect sizes and p-values for each single nucleotide polymorphism (SNP) in the imputed GWAS analysis, typically using a P-value for SNP inclusion in PRS of 0.1 | Pearson correlation co-efficient between maternal and paternal PRS | No correlation of PRS: r=0.00050 with p-value of 0.78 | 5 | An inappropriate high p-value for indication of significant SNPs was chosen reducing the power of detection of a significant inter-spouse correlation |
Table 3.
Characteristics of cross-sectional studies on autistic spectrum disorder prevalence with grouping into countries with and without mating of spouses by individual choice (assortative mating).
Table 3.
Characteristics of cross-sectional studies on autistic spectrum disorder prevalence with grouping into countries with and without mating of spouses by individual choice (assortative mating).
| First author and year | Year of publication | Country | Age of screened population (years) | Diagnostic tool | Incidence of autism spectrum disorder per 10000 of population (number of children assessed) |
| Countries with majority of mating by choice . Shaw et al 2025 [40] Van Balkom et al. 2009 [41] Chaaya et al. 2016 [42] Raz et al. 2015 [43] Chien et al 2011 [44] Sun et al. 2019 [45] Zhou et al 2020 [46] Fombonne et al 2016 [47] Montiel-Nava et al 2008 [48] Alshaban et al. 2019 [49] . Al-Mamri et al. 2019 [50] Nygren et al 2012 [51] Idring et al 2015 [52] Morales-Hidalgo et al. 2018 [53] Fuentes J et al. 2021 et al 2021 [54] Skonieczna-Zydecka et al. 2017 [55] Hansen et al. 2015 [56] Posserud et al. 2010 [57] Mattila et al. 2011 [58] Van Bakel et al. 2015 [59] Thomaidis et al. 2020 [60] Williams et al. 2008 [61] Randall et al. 2015 [62] Kočovská et a. 2012 [63] |
2025 2009 2016 2015 2011 2019 2020 2016 2008 2019 2019 2012 2015 2018 2021 2017 2015 2010 2011 2015 2020 2008 2015 2012 |
USA Aruba Lebanon Israel Taiwan China China Mexico Venezuela Qatar Oman Sweden Sweden Spain Spain Poland Denmark Norway Finland France Greece United Kingdom Australia Faroe Island |
8 0 to 9 1 to 10 8 17 6-10 6 to 12 8 3-9 5 to 12 0 to 14 2 0-27 4-11 7-9 0-16 0-20 7-9 8 7 10-11 11 6-7 15-24 |
Diagnosis as recorded in health and education data bases Overall, 66.5% of children aged 8 years with ASD had any documented autism test: ADOS1(39.6% overall), ASRS2 (30.2% overall;), CARS 3 (24.1% ), Gilliam Autism Rating Scale (12.2%), SRS4 (12.0 %) and ADI-R5 (2.7%) DSM6-IV DSM6-IV M-CHAT7 DSM6 DSM6 IVTR CAST8, ADOS1, ADI-R5 SRS4 ADOS1 DSM6-IV TR QSS-SCQ9 DSM6-5 M-CHAT7 ADOS1, ADI-R5 ICD10-8 and ICD10-10 ADOS1, ADI-R5, SCQ11 ADOS1, Q-CHA12 ICD10 and DSM6-IV ASSQ13, DAWBA14, DISCO15 ASSQ13, ADOS1, ADI-R5, FSIQ16 ICD10-10 ICD10 DSM6-IV DSM6-4 DSM6-5 ASSQ13, ADOS1 |
322 (274857) 19 (13109) 153 (998) 37 (2431649) 28.7 (372642) 97 (72697) 29 (125806) 87 (4195) 17 (254905) 930 (9074) 20.35 (837655) 80 (5007) 154 (735096) 150 (2765) 59 (14734) 35 (707975) 59.2 (677915) 87 (6609) 84 (4422) 36.5 (307751) 115 (182879) 61.9 (14062) 196 (8400) 94 (7128) |
| Countries with majority of mating determined by arrangement by parents or astrology Al-Zahrani et al 2013 [64] Akhter et al 2018 [65] . Raina et al 2017 [66] Rudra et al. 2017 [67] Poovathinal et al. 2016 [68] Nair et al. 2025 [69] . Perera et al 2009 [70] Heys et al 2018 [71] |
2013 2018 2017 2017 2016 2025 2009 2018 |
Saudi Arabia Bangladesh India India India India Sri Lanka Nepal |
7 to 12 1.5 to 3 1 to 10 3 to 8 1 to 3 0 to 108 1.5 to 2 9-13 |
DSM6, ASSQ13 CHAT7 Indian scale for assessment of autism Social and communication disorders checklist, ADOS 1, SCQ10 DSM 6 CARS3-2 M-CHAT7 Autism quotient 10 |
3.5 (22950) 7.5 (5286) 15 (28070) 23 (5947) 23.3 (18480) 1.5 (26092) 740 (374) 34 (4098) |
1 Autism Diagnostic Observation Schedule,2 Autism Spectrum Rating Scales, 3 Childhood Autism Rating Scale,4 Social Responsiveness Scale, 5 Autism Diagnostic Interview-Revised,6 Diagnostic and Statistical Manual of Mental Disorders of the American Psychiatric Association, 7 Modified Check list for autism in toddlers, 8Childhood Autism Spectrum Test, 9Qatar School survey-social communication questionnaire,10 International Classification of Diseases, 11 Social communication questionnaire, 12 Quantitative checklist for autism, 13 Autism spectrum screening questionnaire,14 Development and wellbeing assessment, 15 diagnostic interview for social and communication disorders, 16 Full scale IQ. .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



