Submitted:
23 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Background: The aim of the study was to determine if there is an association between catheter-based occlusion of an arterial duct in premature infants and the incidence of necrotizing enterocolitis. Methods: This was a single center retrospective observational case control study. Infants born between 7/2018 and 12/2022, who were either born prior to 32 weeks gestation or weighed less than 1500 grams and had a patent arterial duct that received medical management, device closure, or surgical ligation were included. Group 1 consisted of infants born prior to 2020 who received only medical therapy and group 2 consisted of those who were born after 2020 and received catheter-based intervention. Analyses were conducted to determine if the incidence of necrotizing enterocolitis had changed since the introduction of catheter-based intervention at the institution in 2020. Results: There were 101 infants which met the inclusion criteria. Group 1 (n = 24) was prior to 2020 with medical management only, and group 2 (n = 77), 2020 onward with introduction of catheter-based occlusion. There were no significant changes in patient characteristics or any management options other than the introduction of device closure between the two groups. Development of necrotizing enterocolitis was shown to be at a median of 31 days and device closure at 49 days. There was a decreasing trend in the institutional incidence of necrotizing enterocolitis (2.6% vs 1.7%). Conclusion: Although we were unable to demonstrate statistical significance in the reduction of necrotizing enterocolitis between the groups, this may be due to the demonstrated need to intervene earlier as well as a larger sample size.
Keywords:
necrotizing enterocolitis
; amplatzer piccolo occlude
; premature infant
; patent ductus arteriosus
; transcatheter closure
; arterial duct
1. Introduction
Patent arterial duct is one of the most common congenital heart defects accounting for between 5% to 10% of all anomalies. A persistent connection between the two great arteries, the arterial duct allows for shunting, typically left to right. This leads to over-circulation into the pulmonary arterial circulation and steal from the systemic arterial circulation. Persistence of an arterial duct in premature neonates has been associated with an increased risk of developing necrotizing enterocolitis, chronic respiratory disease, pulmonary hemorrhage, intraventricular hemorrhage, and death [1]. For these patients, surgical arterial duct ligation was previously the standard of care if attempts with failed attempts at medical closure, with medical management only being successful in approximately 50% of premature infants [2] Surgical ligation, although highly effective, is also associated with significant procedural and post-procedural complications and poor long-term outcomes [2,3]. Transcatheter device closure, although not entirely without complication, has been shown to be better tolerated and associated with improved post-procedural recovery [4].
In January 2019, the Amplatzer Piccolo Occluder received Food and Drug Administration approval and became the first device approved for arterial duct closure in patients ≥700 g [1]. The availability of such small devices as the Piccolo Occluder now allow for early and safe closure of the PDA, with the potential of reducing complications related to the left-right shunting of blood.
Necrotizing enterocolitis is an intestinal inflammatory condition which causes ulceration and necrosis of the intestines. Necrotizing enterocolitis can lead to several complications and is the most common cause of intestinal perforation in premature infants. It has an incidence of 0.3 to 2.4 per 1000 live births and a prevalence of 2% to 5% for premature infants admitted to neonatal intensive care units [5]. Among the known risk factors (Table 1), congenital heart disease can play a significant role in stealing vital blood flow away from the gastrointestinal system, resulting in a mismatch between supply and demand. An arterial duct can result in a reduction of blood flow and oxygen to the intestines, which in turn can lead to intestinal perforation.
Although prior studies have demonstrated improved hospital length of stay and number of ventilatory days [19], there are no data demonstrating the optimal timing for intervention, nor for a reduction in the incidence of necrotizing enterocolitis due to early device closure of the arterial duct. The primary aim of the study was to characterize the timing of development of necrotizing enterocolitis as compared to timing of catheter-based intervention in neonates. The secondary aim of this study was to determine if there was an institutional reduction in the incidence of necrotizing enterocolitis after the implementation of catheter based arterial duct occlusion.
2. Methods
2.1. Study Design
This was a single center retrospective observational case control study conducted at Children’s Hospital of New Orleans, in New Orleans, Louisiana. Patients for this study were cared for at the institution’s level IV neonatal intensive care unit. This study was approved by the institutional review board at Louisiana State University Health Sciences Center. The study was in concordance with the Helsinki Declaration.
The primary aim of the study was to characterize the timing of development of necrotizing enterocolitis as compared to timing of catheter-based intervention in neonates. The secondary aim of this study was to determine if there was an institutional reduction in the incidence of necrotizing enterocolitis after the implementation of catheter based arterial duct occlusion.
2.2. Patient Selection
Inclusion criteria were infants admitted to the unit of interest; 2) gestation age of less than 32 weeks or birthweight of less than 1,500 grams; 3) presence of a hemodynamically significant arterial duct; 4) admission between July 1, 2018 and December 31, 2022. Hemodynamic significance was defined by echocardiography and clinical criteria as outlined by Backes et al. [21] Infants with known congenital heart or chromosomal anomalies were excluded from the study.
2.3. Study Groups
Infants in our study were categorized into 2 groups. Group 1 included all infants meeting the inclusion criteria from 2018 to 2019 prior to institutional initiation of transcatheter arterial ductal device closures. Group 2 included all infants meeting the inclusion criteria from 202 to 2022 post initiation of transcatheter arterial ductal closure (Figure 1A and 1B). It is important to note that although we attempted to include any infants having surgical ligation, we found none, as the institutional preference of our neonatology group was to opt for only medical management in the prior era. The comparison of these 2 groups is therefore a clean one between medical management only versus medical management plus catheter-based device closure.
2.4. Operational Definitions
Gestational age was assessed using an early (less than 14 weeks) ultrasound. If the patient did not have an early ultrasound, then the gestational age was calculated from the last menstrual period. Chorioamnionitis was defined as presence of intrapartum fever of greater than 100 °F (37.8 °C) plus at least two additional clinical signs (maternal tachycardia with heart rate greater than 100 beats per minute, fetal tachycardia with fetal heart rate greater than 160 beats per minute, uterine tenderness, foul-smelling amniotic fluid, or leukocytosis white blood cell count greater than 15,000 cells/mm3) [6]. Necrotizing enterocolitis was defined as Bell stage 2 or more based on radiologic findings read by a pediatric radiologist. [7]. Bronchopulmonary dysplasia was defined as need for oxygen and/or positive pressure support at 36 weeks corrected gestation. [8]. Length of stay was defined as the total duration of hospital stay until date of discharge. Procedural success was defined as having the device positioned within the arterial duct by the end of the implant procedure. Arterial ductal closure was defined as the presence of either no or only trivial residual shunt, as assessed by an independent echocardiographer [9].
2.5. Statistical Analyses
Group comparisons for categorical variables between both groups were conducted using a chi square test and t-test for continuous variables. A two-sided p-value of 0.05 was used to denote statistical significance. Statistical analysis was performed with Statistical Package for the Social Sciences, version 25.0, (Armonk, NY: IBM Corp. 2019).
3. Results
There were 101 infants which met the inclusion criteria as demonstrated in Table 2. (Group 1 n=24 and Group 2 n= 77). There was no significant difference between the gestational age at time of birth between both groups 26.5 vs 25.8 weeks, respectively. Our data demonstrated that birthweight was lower in group 2 (826 grams) vs group 1 (970 grams) (p=0.045). When comparing all infants that underwent arterial ductal device closure with Piccolo device (n= 48) to all infants that developed necrotizing enterocolitis (n=19), regardless of device or no device (Table 3), there was a statistically significant difference in the age at which infants underwent device closure (49 days) as compared to when infants developed necrotizing enterocolitis (31 days), (p<0.001). Additionally, there is a statistically significant difference in median weight between the Piccolo group and the necrotizing enterocolitis group (p = 0.029). Individuals in the Piccolo group were noted to have a higher weight compared to those in the necrotizing enterocolitis group, which is consistent with their greater gestational age.
Additionally, there was no significant difference in resuscitation metrics such as APGAR scores at 1 or 5 minutes. Very importantly, from an antenatal standpoint, there has not been any notable institutional change between pre and post device era in any of the other known risk factors for development necrotizing enterocolitis, namely, the percentage of infants born to mothers receiving prenatal care, antenatal antibiotics, preterm premature rupture of membrane, artificial rupture of membrane, mode of delivery or chorioamnionitis. Finally, the percentage of infants receiving breast milk remained unchanged over the 2 time periods. When evaluating data for long term morbidity and mortality there was no significant difference between the incidence of bronchopulmonary dysplasia, necrotizing enterocolitis, or death prior to discharge. Group 2 did have a significantly increased hospital length of stay (134 days vs 95 days) when compared to group 1. Patients in Group 1 had a significantly increased incidence of a residual arterial duct at time of discharge when compared to Group 2 (50% vs 14.3%, P<0.001).
When focused solely on the subgroup of patients with necrotizing enterocolitis highlighted in Table 4, five patients developed necrotizing enterocolitis in group 1 (20.8%) and 14 in group 2 (18.2%). Based on the p-values there wasn’t any statistically significant differences between the two groups regarding all the other factors measured (gestational age at birth, gestational age when diagnosed with necrotizing enterocolitis, necrotizing enterocolitis age at diagnosis, and weight when diagnosed with necrotizing enterocolitis). This suggests that these factors are overall similar and therefore should not contribute significantly towards any differences we identify in our secondary endpoint of a possible reduction on the institutional incidence of necrotizing enterocolitis.
It is very important to note, all the infants in Group 2 who developed necrotizing enterocolitis did so prior to the catheterization. Only one infant in the device group developed necrotizing enterocolitis after device closure and that infant also had necrotizing enterocolitis prior to the device placement. We then compared the institutional incidence of necrotizing enterocolitis before and after the year 2020 when our institution began using the Piccolo device. Although there is a decreasing trend, there is no strong evidence to suggest a significant change in the incidence of necrotizing enterocolitis (2.6% vs 1.7%, p=0.294).
Table 5 provides procedural data for the 48 infants that underwent arterial ductal device closure using the piccolo device. Only 3 infants had evidence of any residual shunting on echocardiography 24 hours after the procedure, and no infants in this cohort had evidence of a residual arterial duct by time of discharge.
4. Discussion
The presence of an arterial duct is associated with possible long-term morbidities related to either increased pulmonary blood flow or systemic steal. Although there are retrospective studies which describe possible relationships, it is difficult to prove an association between the presence of an arterial duct and increased mortality from any specific comorbidity [10,11]. To date there are no published data providing specific guidance of the proper timing of device closure of the arterial duct in premature infants, nor in demonstrating improved incidence of necrotizing enterocolitis due to early device closure of the arterial duct. Prior to 2020, our institutional preference was to not surgically ligate an arterial duct. With pre and post market approval studies having demonstrated safety and efficacy of the device in premature infants, our neonatology team was agreeable to begin a concerted effort to identify at risk neonates with significant arterial duct for device closure. Our aim in this study was to identify if the timing of our interventions had been appropriate as well as evaluate the institutional incidence of necrotizing enterocolitis comparing our pre and post device era.
The initial therapy at our institution has traditionally been medical therapy aimed at arterial ductal closure and is based on the administration of either non-steroidal anti-inflammatory drugs like indomethacin, ibuprofen, or Tylenol. All neonates in our population cohort (Group 1 and 2) underwent medical therapy as the initial course of treatment for their arterial duct. Medical therapy has been driven in the neonatology community largely by concerns of the complications associated with surgical ligation and no significant benefits aside from ductal closure itself being demonstrated [12]. Surgical ligation of the arterial duct has been the first alternative to failed pharmacological treatment, and it is usually performed through left thoracotomy. Surgical ligation has been reported to be associated with bleeding, infection, vocal paresis, with subsequent development of gastroesophageal reflux disease and need for prolonged intubation and mechanical ventilation [13]. The post-operative course of infants undergoing surgical ligation of an arterial duct is often complicated by post ligation cardiac syndrome with decreased cardiac output. It has also been associated with an increased incidence of bronchopulmonary dysplasia, retinopathy of prematurity, and neurodevelopmental impairment [14,15]. This method had largely fallen out of favor at our institution with only 1 patient having ligation over the duration of the study.
The use of transcatheter arterial ductal closure has gained favor among cardiologists and neonatologists alike as a less invasive alternative to surgical ligation and a more effective treatment option than medical therapy for preterm, premature infants [16]. Since the FDA approval of the Piccolo device for the occlusion of an arterial duct in preterm patients, this device has gained popularity at our institution with resultant performance of over 50 procedures at the time of writing this manuscript. The device has been specifically designed for fetal duct morphology and with reported implant success rate of greater than 99% in infants less than 2 kg [1]. Our experience has largely been similar with a near 100% implant success rate and a median procedure time of 36 minutes. Our procedure time may seem longer than what other institutions have reported, as we define this as the official intra-procedure time beginning with initiation of ultrasound evaluation of the access site and ending with hemostasis being achieved after sheath removal. There are few reported significant complications associated with the use of the device in the literature. Among them, implanters have reported rare cases of dissection of inferior vena cava, cardiac perforation, protrusion of the proximal disk at the pulmonary end causing left pulmonary artery stenosis, protrusion of the distal disk in aorta precipitating aortic coarctation, device embolization, vascular injury, and tricuspid regurgitation [20]. To date there have been 2 reported cases of severe left pulmonary artery stenosis which required surgical intervention at our institution as highlighted by Jaile et al. [17]. There have been no other significant complications associated with the use of this device at our institution. Perceptions regarding left pulmonary artery stenosis amongst implanters has been that it is commonly seen but should improve as the infant grows and the degree of stenosis lessens. The few reported cases of surgery to relieve severe stenosis of the left pulmonary artery post device are likely related to an early learning curve as this procedure is still in its relative infancy.
As previously mentioned, the aim of the study was to evaluate the timing of device closure of an arterial duct with the median age of when necrotizing enterocolitis typically developed as well as determine if the institutional incidence of necrotizing enterocolitis has changed with introduction of the device at our institution. In a meta-analysis by Su et al. factors associated with increased risk of developing necrotizing enterocolitis include low birth weight, premature rupture of membrane, prematurity amongst others. Factors that are protective and may reduce the incidence of necrotizing enterocolitis include the prenatal use of steroids and breast feeding [18]. Another important risk factor for the development of necrotizing enterocolitis includes whether an infant is breast fed or formula fed in addition to the feeding protocol that is being used. Given the multifactorial nature of necrotizing enterocolitis, and this information, we incorporated all these factors in collection of data between Group 1 and 2 and with our statistical analysis. There was no significant change in any other potentially confounding variables in our patient population between pre and post device era to account for any change in necrotizing enterocolitis incidence.
Having seen no significant difference between Group 1 and 2, we further evaluated the patients that had been diagnosed with necrotizing enterocolitis as demonstrated in Table 4. Overall, we were unable to demonstrate any significant changes to this patient population in terms of their gestational age at birth when they were diagnosed with necrotizing enterocolitis or the weight on the day at which the diagnosis was made.
The incidence of necrotizing enterocolitis at our institution was 2.6% for preterm infants less than 32 weeks prior to 2020 and dropped to 1.7% thereafter. We did additionally observe that there were 2 sets of twins in Group 2 where one twin had expired due to septic shock secondary to necrotizing enterocolitis and the second infant had undergone arterial ductal device closure with a Piccolo and did not develop necrotizing enterocolitis.
Lastly, we aimed to compare the weight and age of neonate undergoing arterial ductal device closure and compare that to the weight and age at which a neonate develops necrotizing enterocolitis at our institution. Interestingly we found that among neonates that develop necrotizing enterocolitis this tended to occur at a younger age and lower weight, both of which were statistically significant, thus perhaps there may be even further benefit of performing this procedure at a younger age or weight to prevent necrotizing enterocolitis in this population, which ultimately may prove to be a statistically significant reduction in the incidence of necrotizing enterocolitis. There are currently no prospective studies evaluating such, but this may be an area of interest for future studies. Although we were unable to demonstrate statistical significance in the reduction of necrotizing enterocolitis, there was a favorable trend and could be shown to be significant with a larger sample size. Furthermore, the data shown in Table 3 is suggestive that we could potentially have made an even larger impact on reducing necrotizing enterocolitis incidence had we intervened earlier.
Interestingly we were also able to demonstrate that in Group 2 there was a trend towards caring for smaller and younger infants compared to the previous era, thus likely explaining the increased length of hospital stay compared to Group 1 or to those reported in previous studies. As our institutional experience stabilizes with having achieved success in the smallest of neonates, the length of stay should stabilize. Therefore, even a mere trend in the reduction of necrotizing enterocolitis, coupled with a population that is of smaller size and younger gestational age, could in fact be significant and requires additional investigation.
We would point out that our median ages of 31 days versus 49 days between development of necrotizing enterocolitis and intervention are mere targets for our institution. Moving forward, we will attempt to narrow this gap to hopefully have a greater impact on the reduction of developing necrotizing enterocolitis. For other institutions, these targets would only be applicable if all the other confounding variables for development of necrotizing enterocolitis (Table 1) are similar to ours.
The limitations of the study are as follows. This is a retrospective study conducted at a single center. The overall sample size was somewhat limited, thereby hindering our ability to establish statistical significance. Necrotizing enterocolitis is a multifactorial condition, making it challenging to assess the specific contributions of various variables within this fragile heterogamous patient population. Additionally at our institution there is no standardized protocol for referring patients for arterial ductal device closure, thus this might introduce a selection bias in our Piccolo population or Group 2. The development of a specific protocol would aid with sooner referral for intervention.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by WS, MS, MJ, SB. The first draft of the manuscript was written by WS and SB. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
No funding was required for this original research.
Conflicts of Interest
The authors have no disclosures.
References
- Sathanandam, S.K.; Gutfinger, D.; O'BRien, L.; Forbes, T.J.; Gillespie, M.J.; Berman, D.P.; Armstrong, A.K.; Shahanavaz, S.; Jones, T.K.; Morray, B.H.; et al. Amplatzer Piccolo Occluder clinical trial for percutaneous closure of the patent ductus arteriosus in patients ≥700 grams. Catheter Cardiovasc Interv. 2020, 96(6), 1266–1276. [Google Scholar] [CrossRef]
- Koehne, PS; Bein, G; Alexi-Meskhishvili, V; Weng, Y; Bührer, C; Obladen, M. Patent ductus arteriosus in very low birthweight infants: complications of pharmacological and surgical treatment. J Perinat Med. 2001, 29(4), 327–334. [Google Scholar] [CrossRef] [PubMed]
- Zbar, RI; Chen, AH; Behrendt, DM; Bell, EF; Smith, RJ. Incidence of vocal fold paralysis in infants undergoing ligation of patent ductus arteriosus. Ann Thorac Surg. 1996, 61(3), 814–816, Google Scholar. [Google Scholar] [CrossRef] [PubMed]
- Serrano, R.M.; Madison, M.; Lorant, D.; et al. Comparison of ‘post-patent ductus arteriosus ligation syndrome’ in premature infants after surgical ligation vs. percutaneous closure. J Perinatol 2020, 40, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Ginglen, JG; Butki, N. Necrotizing enterocolitisrotizing Enterocolitis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island (FL), 8 Aug 2023; Available online: https://www.ncbi.nlm.nih.gov/books/NBK513357/.
- Gibbs, R; Blanco, J; St. Clair, P; Castaneda, Y. Quantitative Bacteriology of Amniotic Fluid from Women with Clinical Intraamniotic Infection at Term. Journal of Infectious Diseases 1982, 145(1), 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bell, M; Ternberg, J; Feigin, R; Keating, J; Marshall, R; Barton, L; et al. Neonatal Necrotizing enterocolitisrotizing Enterocolitis. Annals of Surgery 1978, 187(1), 1–7. [Google Scholar] [CrossRef] [PubMed]
- Fajardo, C; Alshaikh, B; Harabor, A. Prolonged use of antibiotics after birth is associated with increased morbidity in preterm infants with negative cultures. The Journal of Maternal-Fetal & Neonatal Medicine 2018, 32(24), 4060–4066. [Google Scholar] [CrossRef] [PubMed]
- Baspinar, O; Sahin, DA; Sulu, A; Irdem, A; Gokaslan, G; Sivasli, E; et al. Transcatheter closure of patent ductus arteriosus in under 6 kg and premature infants. J Interv Cardiol. 2015, 28, 180–9. [Google Scholar] [CrossRef] [PubMed]
- Schena, F; Francescato, G; Cappelleri, A; et al. Association between hemodynamically significant patent ductus arteriosus and bronchopulmonary dysplasia. J Pediatr. 2015, 166(6), 1488–92. [Google Scholar] [CrossRef] [PubMed]
- Mayer, A; Francescato, G; Pesenti, N; Schena, F; Mosca, F. Patent ductus arteriosus and spontaneous intestinal perforation in a cohort of preterm infants. J Perinatol. 2022, 42(12), 1649–53. [Google Scholar] [CrossRef] [PubMed]
- Hundscheid, T; Onland, W; Kooi, EMW; et al. Expectant manage-ment or early ibuprofen for patent ductus arteriosus. N Engl J Med. 2023, 388(11), 980–90. [Google Scholar] [CrossRef] [PubMed]
- Fraisse, A; Bautista-Rodriguez, C; Burmester, M; Lane, M; Singh, Y. Transcath-eter closure of patent ductus arteriosus in infants with weight under 1,500 Grams. Front Pediatr. 2020, 8, 558256. [Google Scholar] [CrossRef] [PubMed]
- Weisz, DE; Mirea, L; Rosenberg, E; et al. Association of patent ductus arte- riosus ligation with death or neurodevelopmental impairment among extremely preterm infants. JAMA Pediatr. 2017, 171(5), 443. [Google Scholar] [CrossRef] [PubMed]
- Weisz, DE; Giesinger, RE. Surgical management of a patent ductus arterio- sus: Is this still an option? Semin Fetal Neonatal Med. 2018, 23(4), 255–66. [Google Scholar] [CrossRef] [PubMed]
- Sathanandam, S; Agrawal, H; Chilakala, S; et al. Can transcatheter PDA clo- sure be performed in neonates ≤1000 grams? The Memphis experience: XXXX. Congenit Heart Dis. 2019, 14(1), 79–84. [Google Scholar] [CrossRef] [PubMed]
- Jaile, J. C.; Siwik, E.; Bartakian, S. Left pulmonary artery occlusion following device closure of patent ductus arteriosus in premature infants. Journal of the Society for Cardiovascular Angiography & Interventions 2023, 101194. [Google Scholar] [CrossRef] [PubMed]
- Su, Yan; Xu, Rui-Hong; Guo, Li-Yan; Chen, Xin-Qing; Han, Wen-Xiao; Ma, Jin-Jin; Liang, Jiao-Jiao; Hao, Ling; Ren, Chang-Jun. Risk factors for necrotizing enterocolitisrotizing enterocolitis in neonates: A meta-analysis. Frontiers in pediatrics 2023, 10, 1079894. [Google Scholar] [CrossRef] [PubMed]
- Baruteau, Alban-Elouen; Regan, W.; Benbrik, Nadir; Sharma, S.; Auriau, J.; Romefort, Bénédicte; Prigent, Solène; Le Gloan, Laurianne; Bautista-Rodriguez, Carles; Sirico, D.; Guérin, P.; Rozé, Jean-Christophe; Di Salvo, Giovanni; Foldvari, Sandrine; Fraisse, Alain. Improved ventilation and hospital stay in premature babies after transcatheter closure of patent ductus arteriosus as compared to surgical ligation: A multi-center comparative study. Archives of Cardiovascular Diseases Supplements 2019, 11(4), e380–e380. [Google Scholar] [CrossRef]
- Francescato, G.; Doni, D.; Annoni, G.; et al. Transcatheter closure in preterm infants with patent ductus arteriosus: feasibility, results, hemodynamic monitoring and future prospectives. Ital J Pediatr 2023, 49, 147. [Google Scholar] [CrossRef] [PubMed]
- Backes, CH; Hill, KD; Shelton, EL; Slaughter, JL; Lewis, TR; Weisz, DE; Mah, ML; Bhombal, S; Smith, CV; McNamara, PJ; Benitz, WE; Garg, V. Patent Ductus Arteriosus: A Contemporary Perspective for the Pediatric and Adult Cardiac Care Provider. J Am Heart Assoc. 2022, 11(17), e025784. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
A—Infants were categorized into 2 groups. Group 1 included all infants meeting the inclusion criteria from 2018–2019 prior to institutional initiation of transcatheter arterial ductal device closures. B—Group 2 included all infants meeting the inclusion criteria from 2020-2022 post initiation of transcatheter arterial ductal closure.
Figure 1.
A—Infants were categorized into 2 groups. Group 1 included all infants meeting the inclusion criteria from 2018–2019 prior to institutional initiation of transcatheter arterial ductal device closures. B—Group 2 included all infants meeting the inclusion criteria from 2020-2022 post initiation of transcatheter arterial ductal closure.
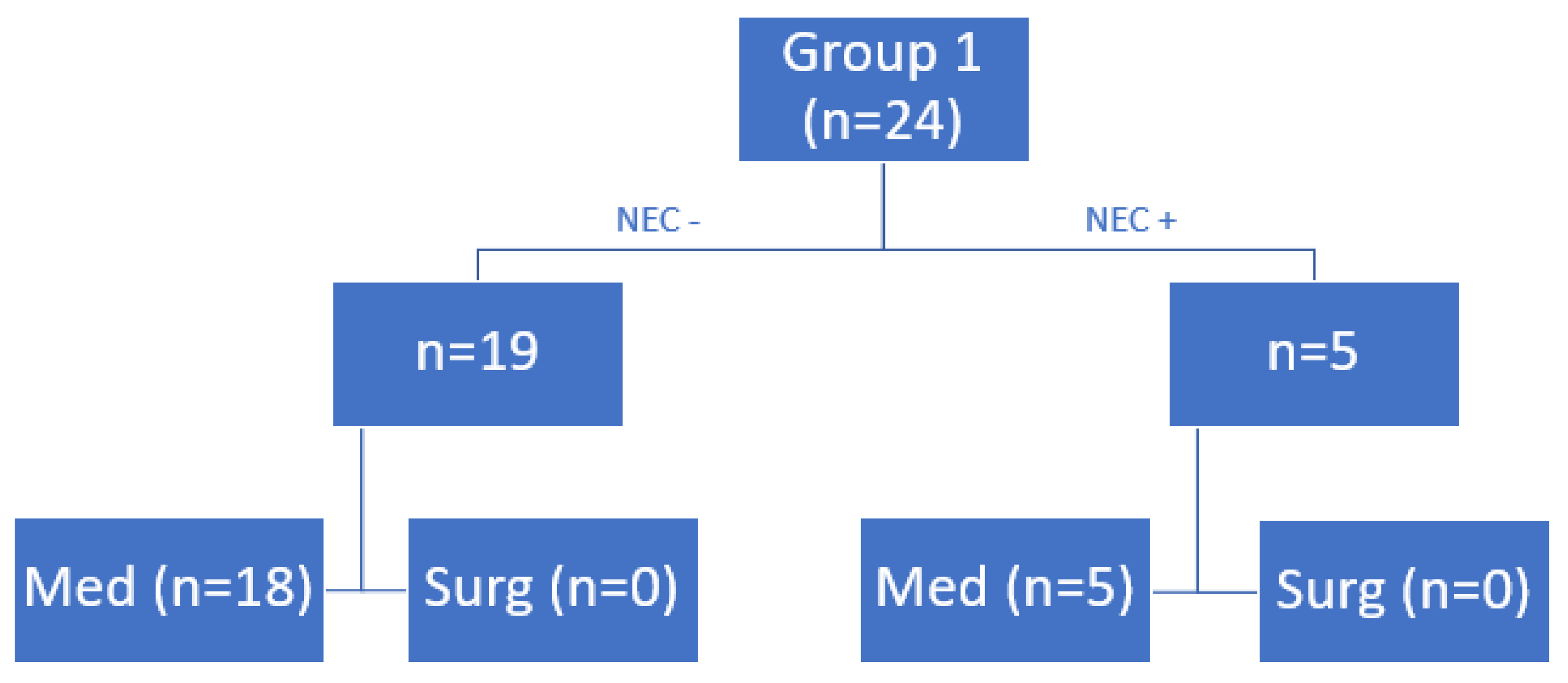
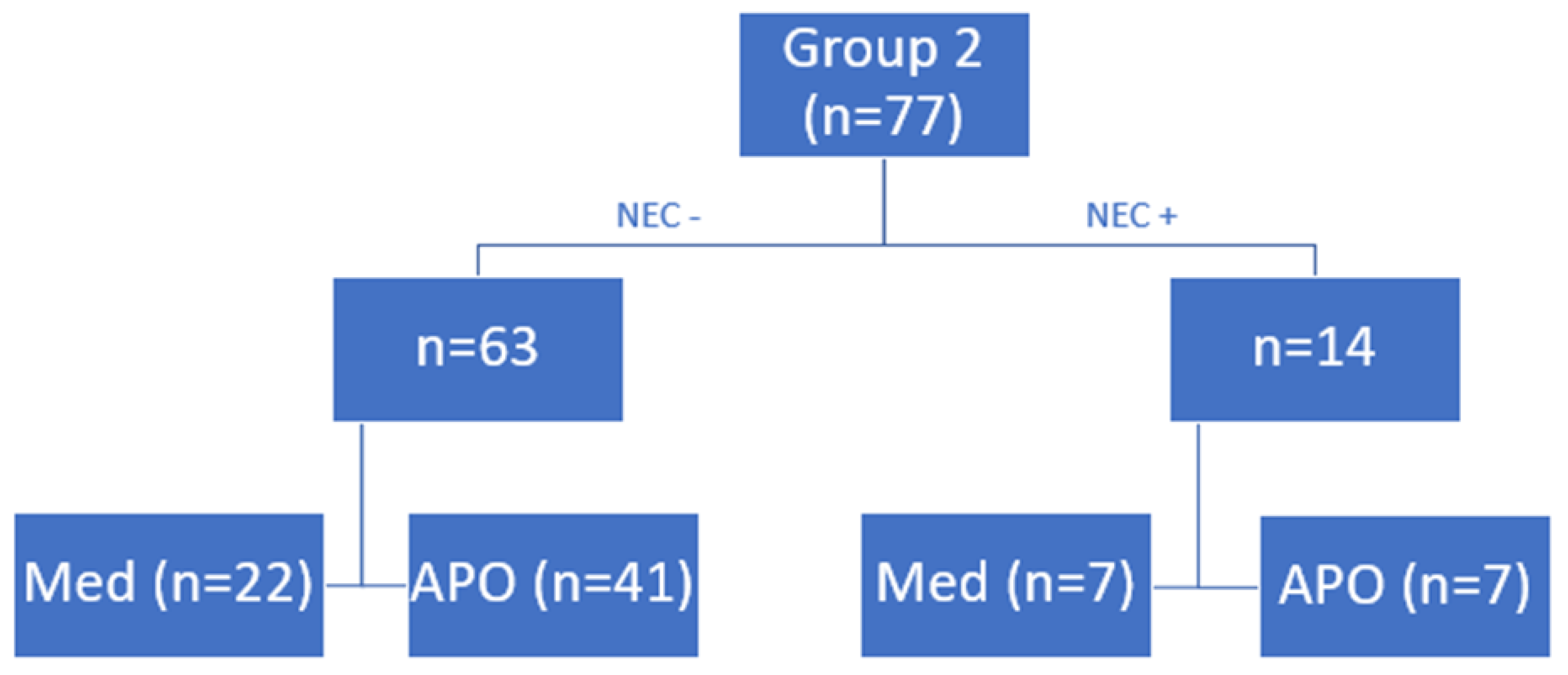

Table 1.
Risk factors for the development of necrotizing enterocolitis in neonates.
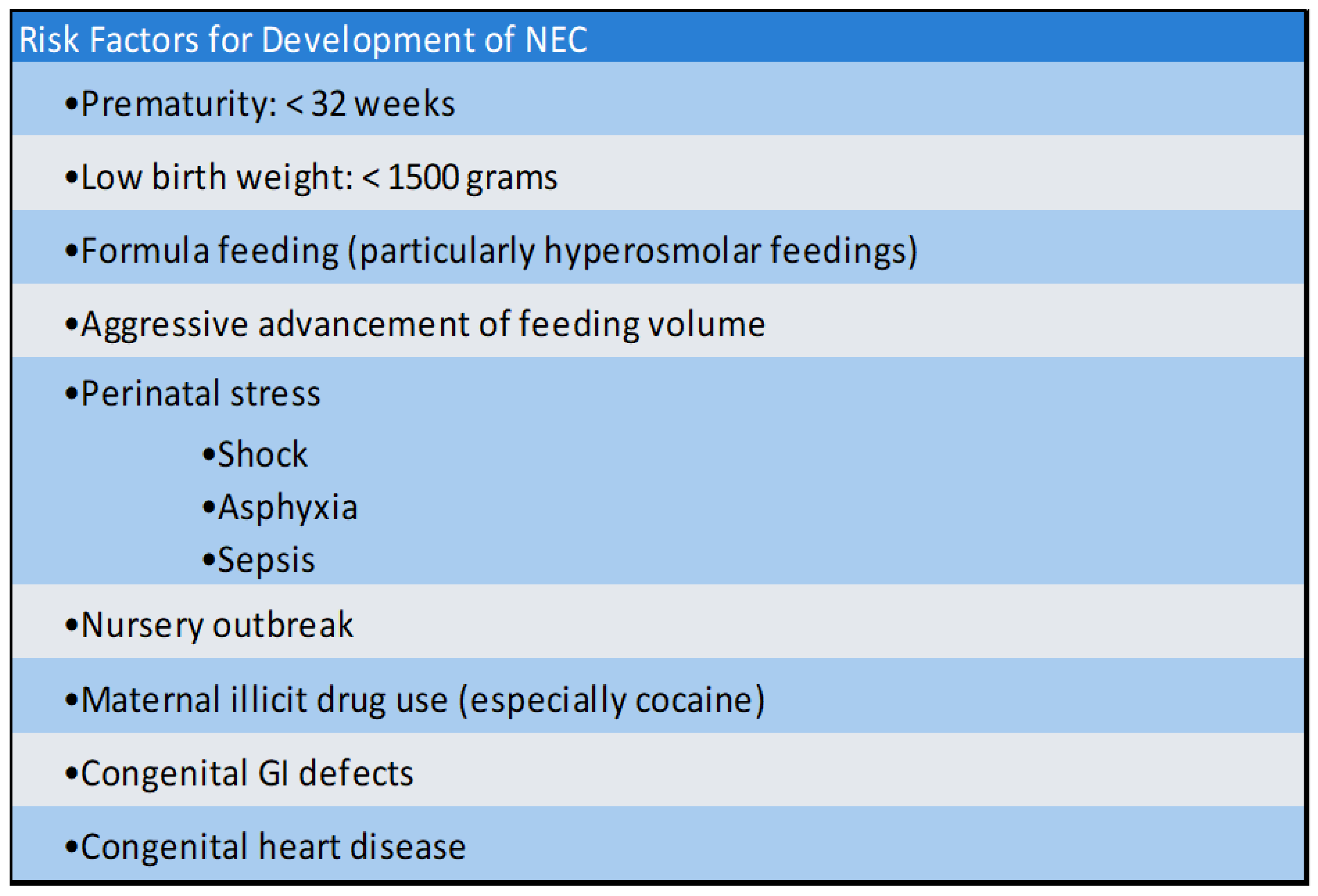 |
Table 2.
Infant baseline characteristics, maternal and prenatal information, delivery room resuscitation and mode of delivery. * denotes statistical significance.
Table 2.
Infant baseline characteristics, maternal and prenatal information, delivery room resuscitation and mode of delivery. * denotes statistical significance.
| Group | |||
|---|---|---|---|
| 1 (n=24) | 2 (n=77) | p-value | |
| Weight (grams) | 970.0 | 826.0 | 0.04* |
| GA (weeks) | 26.5 | 25.8 | 0.25 |
| APGAR (1 min) | 4.0 | 4.3 | 0.58 |
| APGAR (5 min) | 7.0 | 6.6 | 0.29 |
| Length hospital stay (days) | 95.7 | 134.1 | 0.02* |
| Gender (% Male) | 15 (62.5%) | 38 (49.4%) | 0.26 |
| Prenatal care (Yes) | 21 (87.5%) | 71 (92.2%) | 0.44 |
| Antenatal AB (Yes) | 8 (33.3%) | 35 (45.4%) | 0.29 |
| Prenatal steroids (Yes) | 19 (79.2%) | 52 (67.5%) | 0.28 |
| PPROM (Yes) | 10 (41.7%) | 40 (51.9%) | 0.38 |
| AROM (Yes) | 0 (0%) | 2 (2.6%) | 1 |
| Chorioamnionitis (Yes) | 3 (12.5%) | 6 (7.8%) | 0.44 |
| Surfactant (Yes) | 19 (78.5%) | 77 (100%) | 0.01* |
| Type of Delivery (Vaginal) | 5 (20.8%) | 28 (36.4%) | 0.16 |
| BPD (Yes) | 11 (45.8%) | 39 (50.6%) | 0.68 |
| Breast Milk (%) | 6 (25%) | 21 (27.3%) | 0.83 |
| NECROTIZING ENTEROCOLITIS (Yes) | 5 (20.8%) | 14 (18.2%) | 0.77 |
| PDA at Time of DC (Yes) | 12 (50%) | 11 (14.3%) | <0.001* |
| Death Prior to DC (Yes) | 4 (16.7%) | 8 (10.4%) | 0.47 |
Table 3.
Patient characteristic comparison of infants that underwent PDA device closure to all infants that developed NECROTIZING ENTEROCOLITIS across both cohorts. *denotes statistical significance. .
Table 3.
Patient characteristic comparison of infants that underwent PDA device closure to all infants that developed NECROTIZING ENTEROCOLITIS across both cohorts. *denotes statistical significance. .
| Piccolo (n=48) | NECROTIZING ENTEROCOLITIS (n=19) | ||
|---|---|---|---|
| Mean | Mean | p-value | |
| DOL (days) | 49 | 31 | <0.001* |
| Weight (grams) | 1686 | 1312 | 0.029* |
Abbreviations: Day of Life (DOL).
Table 4.
Comparison of infants diagnosed with necrotizing enterocolitis between both groups. Specifically evaluating factors such age at birth as well as age and weight at time of diagnosis.
Table 4.
Comparison of infants diagnosed with necrotizing enterocolitis between both groups. Specifically evaluating factors such age at birth as well as age and weight at time of diagnosis.
| Group | ||||
|---|---|---|---|---|
| 1 (n=5) | 2 (n=14) | p-value | ||
| GA at Birth (weeks) | 27.79 | 27.53 | 0.85 | |
| GA at necrotizing enterocolitis diagnosis (weeks) | 31.56 | 29.92 | 0.24 | |
| DOL at necrotizing enterocolitis diagnosis (days) | 32.25 | 20.56 | 0.14 | |
| Weight at necrotizing enterocolitis diagnosis (grams) | 1447.81 | 1224.56 | 0.29 | |
Table 5.
Procedural data for all 48 infants that underwent arterial ductal device closure using the Piccolo. Including the median arterial duct diameter, length, duration of the procedure and the fluoroscopy time.
Table 5.
Procedural data for all 48 infants that underwent arterial ductal device closure using the Piccolo. Including the median arterial duct diameter, length, duration of the procedure and the fluoroscopy time.
| PDA Diameter (mm) | PDA Length (mm) | Duration of Procedure (min) | Fluoroscopy Time (min) |
|---|---|---|---|
| 3 (1.1-5.2) | 9.3 (4.3-14) | 36 (19-157) | 7.1 (3.2-80.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



