Submitted:
24 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Background: Mental health needs are rising globally, while workforce shortages constrain access to timely care. Israel launched formal training for Psychiatric–Mental Health Nurse Practitioners (PMHNPs) in 2023 as part of broader efforts to strengthen the public mental health system. This narrative review synthesizes international and Israeli evidence on PMHNP roles, models of practice, outcomes, and implementation considerations relevant to the Israeli context. Methods: A narrative literature review was conducted using PubMed/MEDLINE, CINAHL, PsycINFO, and Scopus (January 2000–December 2024), along with targeted policy and regulatory documents. Eligible sources addressed NP/PMHNP roles, scope of practice, clinical outcomes, implementation processes, workforce implications, or policy considerations in high-income health systems. Findings were synthesized thematically. Results: Across diverse settings, PMHNP-delivered care was generally comparable in quality and safety to psychiatrist-led or physician-led care, and was associated with improved accessibility, continuity, and high patient satisfaction. Successful implementation depended on regulatory clarity, organizational readiness, interprofessional collaboration, and the development of a clear professional identity. In Israel, the role is emerging within a cautious regulatory framework and may face early barriers related to role ambiguity, variable organizational support, and limited stakeholder awareness. Conclusions: Strategic, system-level implementation of the PMHNP role-aligned with regulation, training, and supportive organizational structures-may help expand access to mental health services and strengthen continuity of care in Israel amid growing demand.
Keywords:
psychiatric–mental health nurse practitioner
; advanced practice nursing
; mental health workforce
; scope of practice
; implementation
; narrative review
1. Introduction
Mental health is a fundamental component of individual well-being and social functioning. Nevertheless, the provision of mental healthcare, particularly within public healthcare systems, faces substantial and persistent challenges. Global epidemiological data indicates a continuous rise in the prevalence of mental disorders, accompanied by a growing social and economic burden on individuals, families, and healthcare systems [1]. Mental health conditions are now among the leading contributors to disability worldwide, with long-term consequences for quality of life and healthcare utilization [2].
International policy reports emphasize that mental health systems in many countries are struggling to respond adequately to increasing demand due to chronic workforce shortages, fragmented service delivery, and prolonged underinvestment. These reports consistently call for structural reforms, including the expansion and optimization of advanced clinical roles, in order to improve accessibility, continuity, and quality of care [3,4].
In Israel, these global challenges are particularly pronounced. The public mental health system has long been characterized by limited resources, shortages of trained professionals, and structural disparities compared with other high-income countries [5]. Long waiting times, insufficient community-based services, and uneven geographic distribution of mental health professionals have been persistent features of the system even prior to recent crises.
The psychological consequences of the events of October 7 and the subsequent “Iron Swords” war have further intensified the demand for mental health services. The need for psychological support has increased not only in terms of acute and immediate interventions but also in relation to long-term therapeutic care for trauma-related conditions, anxiety, depression, and complex psychosocial distress [3,5]. These developments have exposed existing structural gaps and underscored the urgent need to strengthen and expand responses within the public mental health system.
As part of strategies promoted by the Israeli Ministry of Health, formal training for Psychiatric–Mental Health Nurse Practitioners (PMHNPs) was launched in 2023. This role grants nurses selected medical authorities and is intended to support the mental health system in addressing growing population needs. The introduction of a new professional role particularly in a sensitive and complex field such as mental health is a dynamic and resource-intensive process that requires time, regulatory clarity, organizational readiness, and collaboration among multiple stakeholders.
Evidence from previous initiatives in Israel suggests that the implementation of advanced nursing roles is not without difficulty. Studies examining Nurse Practitioner (NP) roles in geriatrics and supportive care have identified challenges related to role ambiguity, professional boundaries, and organizational integration (Nissanholtz-Gannot & Cohen, 2023). These experiences highlight the importance of examining the PMHNP role not only in terms of clinical effectiveness, but also through a broader lens that considers implementation processes, system-level implications, and policy context.
2. Materials and Methods
2.1. Design
This study was conducted as a narrative literature review to provide an integrative and critical overview of the role, implementation, and contribution of Nurse Practitioners (NPs), with a specific focus on Psychiatric–Mental Health Nurse Practitioners (PMHNPs), within mental health systems internationally and in Israel. A narrative approach was selected to support conceptual synthesis and contextual interpretation of clinical, organizational, and policy dimensions that may be underrepresented in strictly effectiveness-focused systematic reviews.
2.2. Literature Search Strategy
A structured literature search was conducted across PubMed/MEDLINE, CINAHL, PsycINFO, and Scopus to identify relevant peer-reviewed publications. The search covered the period from January 2000 to December 2024, reflecting the timeframe during which advanced practice nursing roles—and particularly the PMHNP role—expanded substantially in policy, practice, and research. To capture implementation and policy context, we also screened reference lists of key review articles and conducted targeted searches for regulatory and policy documents from recognized organizations (e.g., World Health Organization, OECD) and Israeli Ministry of Health circulars.
Search terms were combined using Boolean operators and included:
“Nurse Practitioner”, “Psychiatric–Mental Health Nurse Practitioner”, “PMHNP”, “mental health care”, “psychiatric care”, “scope of practice”, “role implementation”, “advanced nursing practice”, “primary care”, “community mental health”, and “health systems”. Reference lists of key articles and reviews were also manually screened to identify additional relevant sources.
Study Selection
Eligible sources included peer-reviewed articles published in English that addressed NP or PMHNP roles in mental health care, clinical and service outcomes, implementation processes, workforce implications, or policy and regulatory considerations. Both empirical studies and review articles were included, alongside relevant policy and regulatory analyses from recognized international and Israeli organizations. Sources focused exclusively on educational curricula without practice implications, opinion pieces without empirical or policy grounding, and non-healthcare settings were excluded.
Findings were synthesized thematically rather than quantitatively, emphasizing conceptual integration and relevance to implementation and health-system decision-making. Given the heterogeneity of evidence and settings, the review prioritized convergence across sources and identification of contextual determinants that may influence successful PMHNP integration, particularly in the Israeli mental health system.
Data were charted using a structured extraction framework capturing publication year, country/setting, study design, population and clinical context, described PMHNP scope of practice, and reported outcomes (e.g., access, continuity, safety, patient satisfaction, utilization). Findings were synthesized thematically through iterative comparison across sources, focusing on recurring domains including models of care, regulatory variation, interprofessional dynamics, and organizational readiness. Reporting was guided by established quality principles for narrative reviews, including those reflected in the SANRA framework.
3. Results
3.1. Nurse Practitioners: Role Development and Evidence Base
Challenges related to workforce shortages, demographic change, and the increasing burden of chronic illness are shared by healthcare systems worldwide. In response, many countries have redefined professional roles to optimize the use of available human resources and enhance service delivery [6]. One of the most prominent roles developed in this context is that of the Nurse Practitioner (NP).
The International Council of Nurses defines the Nurse Practitioner as a registered nurse who has acquired advanced clinical expertise, complex decision-making skills, and expanded professional competencies, with a master’s degree recommended for entry-level preparation [7]. Admission requirements for NP training typically include advanced academic education, formal clinical specialization, and extensive professional experience in assessment and management of defined health conditions.
The NP role originated in the United States in 1965, with the establishment of the first academic training program at the University of Colorado. Since then, the role has expanded globally and is now formally recognized and regulated in countries such as the United States, Canada, Australia, and several European nations. Despite this shared foundation, there is considerable international variation in scope of practice, level of autonomy, prescribing authority, and regulatory frameworks [7,8].
A growing body of evidence supports the quality, safety, and effectiveness of NP-led care across diverse healthcare settings. An overview of systematic reviews conducted across 38 countries demonstrated that care provided by Nurse Practitioners was equivalent or superior to physician-led care across multiple quality indicators, including patient safety, clinical outcomes, and patient satisfaction [9]. Importantly, these findings were consistent across a wide range of clinical domains and population groups.
In primary care settings, NP-led models have been shown to be particularly effective for patients with complex and chronic conditions. A systematic review focusing on individuals with multimorbidity found that NP-led care was associated with comparable or reduced healthcare costs, similar or improved quality of care, and reduced utilization of emergency and inpatient services [10]. These findings highlight the potential contribution of NPs to healthcare system efficiency, particularly in publicly funded systems facing increasing demand and limited physician availability.
Beyond clinical outcomes, studies have consistently reported high levels of patient satisfaction with NP-provided care, as well as positive effects on care continuity and access [11,12]. Evidence also suggests that NP integration does not result in increased referrals or unnecessary utilization of additional services, further supporting the role’s contribution to sustainable healthcare delivery [12,13,14]
Psychiatric–Mental Health Nurse Practitioners: International Evidence and Models of Practice
Mental health systems worldwide have increasingly turned to Psychiatric–Mental Health Nurse Practitioners (PMHNPs) as a response to growing service demand, workforce shortages, and the need for accessible, community-based care. The PMHNP role is typically characterized by advanced clinical training in psychiatric assessment, diagnosis, psychotherapy, psychopharmacology, and care coordination, enabling practitioners to function with a high degree of clinical responsibility [3,15].
3.2. PMHNPs in Primary Care and Community Settings
One of the most extensively studied areas of PMHNP practice is primary care and community mental health services, where early identification and intervention are critical. In these settings, PMHNPs often serve as first-line providers for individuals presenting with common mental health conditions such as depression, anxiety disorders, and substance use disorders. Their integration into primary care teams has been associated with improved access to mental health services, reduced waiting times, and enhanced continuity of care [9,16,17].
Empirical studies and reviews consistently demonstrate that PMHNP-led care in community settings achieves clinical outcomes comparable to those of psychiatrist-led models. A systematic review examining NP-delivered care for individuals with depression, anxiety, and substance use disorders found no significant differences in symptom reduction, safety outcomes, or rates of hospitalization compared with physician-led care, while highlighting improved accessibility and patient satisfaction (Alexander & Schnell, 2019). Similar findings were reported in later analyses focusing specifically on PMHNP roles within integrated care models [16].
In addition to direct clinical outcomes, PMHNPs in community settings frequently play a central role in care coordination and case management, particularly for individuals with complex psychosocial needs. This includes collaboration with primary care physicians, social workers, psychologists, and community services, contributing to a more holistic and patient-centered approach. Such models are particularly relevant in public health systems, where fragmentation of care has been identified as a major barrier to effective mental health service delivery [17].
3.3. PMHNPs in Inpatient and Specialized Services
Beyond community-based care, PMHNPs are increasingly integrated into inpatient psychiatric units and specialized mental health services. In these settings, their roles often include comprehensive psychiatric assessments, medication management, participation in multidisciplinary treatment planning, and follow-up care planning. Studies examining inpatient PMHNP practice suggest that their involvement contributes to improved continuity between inpatient and community services, as well as more efficient use of psychiatric resources.
Workforce data from several high-income countries indicate a substantial expansion of the PMHNP workforce over the past decade, coinciding with a relative decline in the number of practicing psychiatrists in public systems [18]. This trend has intensified interest in optimizing the utilization of PMHNPs across care settings, particularly in regions experiencing acute shortages of psychiatric physicians.
3.4. Scope of Practice and Regulatory Variation
Despite shared core competencies, the scope of PMHNP practice varies considerably across countries and jurisdictions. In some systems, PMHNPs are granted full practice authority, including independent prescribing and autonomous clinical decision-making. In others, practice authority remains conditional upon physician supervision or collaborative agreements. Comparative analyses suggest that broader scopes of practice are associated with improved service accessibility and workforce stability, without compromising quality or safety (Maier & Aiken, 2016).
Nevertheless, regulatory expansion alone does not guarantee effective role implementation. Organizational culture, interprofessional relationships, and clarity of role definition have been identified as critical determinants of successful PMHNP integration. These factors underscore the importance of examining PMHNP practice not only through a clinical lens, but also in relation to system-level and organizational contexts.
Psychiatric–Mental Health Nurse Practitioners in Israel: Context, Regulation, and Implementation
The introduction of the PMHNP role in Israel represents a significant development within the national mental health system. Historically, advanced nursing roles in Israel have been implemented gradually and unevenly, often accompanied by professional and organizational challenges. Understanding this context is essential for evaluating the potential contribution of PMHNPs and anticipating barriers to effective integration.
3.5. Development of Advanced Nursing Roles in Israel
Advanced nursing practice in Israel has evolved primarily through targeted initiatives addressing specific system needs, such as geriatrics, palliative care, and community health. While these initiatives have demonstrated the potential of Nurse Practitioners to enhance service delivery, research has also documented challenges related to role ambiguity, limited professional autonomy, and resistance from medical staff (Nissanholtz-Gannot & Cohen, 2023).
These experiences provide an important backdrop for the implementation of the PMHNP role. Unlike some countries where NP roles were introduced alongside broad regulatory reforms, Israel’s approach has often involved incremental delegation of authority, with significant discretion retained by supervising physicians and healthcare organizations.
3.6. Regulatory Framework for PMHNPs in Israel
According to the Ministry of Health Director-General Circular (No. 4/2023), PMHNPs are formally recognized as part of multidisciplinary mental healthcare teams and are authorized to perform a defined set of clinical activities. These include psychiatric assessment, referral for diagnostic testing, management of acute and chronic psychiatric conditions, and renewal of pharmacological treatment in accordance with clinical guidelines.
Eligibility criteria for PMHNP training include completion of post-basic psychiatric nursing certification and a minimum of two years of professional experience in mental health settings. The training program comprises approximately 726 academic and clinical hours and culminates in a comprehensive examination. PMHNPs operate under dual supervision: professional supervision by a specialist physician and administrative supervision by nursing management. Importantly, the exercise of medical authority is subject to physician approval, and implementation of granted powers is not mandatory across settings. This regulatory structure reflects a cautious approach to role expansion, aimed at balancing innovation with professional oversight.
3.7. Early Implementation Challenges
While empirical data on PMHNP practice in Israel remain limited due to the recency of the role, evidence from other NP specialties suggests that similar challenges are likely to emerge. These include uncertainty regarding role boundaries, variability in organizational support, and limited awareness of NP competencies among physicians and managers [19,20].
In the context of mental health, such challenges may be further compounded by high workload, staff shortages, and the emotional demands of psychiatric care [3]. Without clear implementation strategies and organizational commitment, there is a risk that PMHNPs will be underutilized, with their roles confined to functions already performed by post-basic psychiatric nurses rather than fully leveraging their advanced training.
As the PMHNP role in Israel was introduced only recently, empirical outcome data are not yet available, and evaluation of its impact will require longitudinal and mixed-methods research [Insert Figure 1 here].
4. Discussion
This narrative review highlights the growing importance of Psychiatric–Mental Health Nurse Practitioners as a strategic response to escalating mental health needs in both international and Israeli contexts. The reviewed literature indicates that PMHNPs provide care that is comparable in quality and safety to psychiatrist-led models across a range of mental health conditions, while offering additional benefits related to accessibility, continuity, and system efficiency [11,12,18].
Professional Identity and Role Implementation
From a theoretical perspective, the challenges associated with PMHNP integration can be understood through the lens of Role Theory, which emphasizes the impact of role expectations, role ambiguity, and role conflict on professional practice. When expectations regarding authority, responsibility, and autonomy are unclear or contested, role strain may occur, potentially limiting the effective utilization of professional competencies. Evidence from both international and Israeli contexts suggests that successful PMHNP implementation depends on the establishment of a clear professional identity within multidisciplinary teams. This includes explicit role definitions, alignment between training and practice, and recognition of PMHNP competencies by physicians and organizational leaders [20].
Interprofessional Dynamics and Organizational Readiness
Interprofessional collaboration is a central component of mental healthcare delivery. While PMHNPs are trained to function within multidisciplinary teams, their integration may challenge traditional professional hierarchies. Studies examining NP implementation consistently identify physician resistance and organizational inertia as key barriers, particularly in systems where medical authority has historically been centralized [21]. Organizational readiness, including leadership support, clear protocols, and opportunities for collaborative practice has been shown to facilitate successful role integration. In the absence of such conditions, PMHNPs may experience limited autonomy and reduced job satisfaction, potentially undermining workforce retention and system benefits [9,20].
Policy Implications
International policy documents underscore the urgency of addressing mental health workforce shortages through innovative role expansion. Both the World Health Organization and the OECD explicitly recommend optimizing the use of advanced nursing roles as part of comprehensive mental health system reform [3,4]. These recommendations are highly relevant to Israel, where rising demand, limited psychiatric workforce capacity, and recent national crises have intensified pressure on public mental health services. Strategic implementation of the PMHNP role in Israel will require more than regulatory authorization. Policy efforts should focus on aligning training, regulation, and organizational practice; promoting awareness of PMHNP competencies; and establishing evaluation mechanisms to monitor outcomes and guide ongoing development.
Limitations
This review has several limitations. As a narrative review, it does not aim to provide quantitative estimates of effectiveness or causal inference. Although a structured search strategy was employed, the potential for selection bias cannot be fully excluded. In addition, empirical evidence regarding PMHNP implementation in Israel is still emerging, and conclusions related to the Israeli context should therefore be interpreted with caution.
Beyond the settings described above, international literature highlights variation in how PMHNP roles are operationalized across healthcare systems. In countries with well-established advanced nursing regulation, PMHNPs are increasingly embedded within stepped-care and collaborative care models. These models emphasize early identification of mental health conditions, continuity across levels of care, and integration between physical and mental health services. Within such frameworks, PMHNPs frequently assume responsibility for longitudinal follow-up, medication management, and coordination between primary care and specialist services, thereby reducing fragmentation of care.
Evidence from publicly funded health systems suggests that PMHNPs may be particularly valuable in underserved or peripheral regions, where access to psychiatrists is limited. In these contexts, PMHNPs often function as stable, long-term providers who maintain continuity of therapeutic relationships. This continuity has been associated with improved adherence to treatment plans and enhanced patient engagement, particularly among individuals with chronic and recurrent mental health conditions. Comparative analyses also indicate that systems granting broader professional autonomy to PMHNPs tend to demonstrate more efficient utilization of psychiatric resources. While psychiatrists in these systems often focus on complex diagnostic cases and treatment-resistant conditions, PMHNPs manage a substantial proportion of routine and moderate-severity cases. This complementary distribution of roles appears to support system sustainability without compromising clinical quality [9].
Implications for Service Organization
From a service organization perspective, the integration of PMHNPs may contribute to reconfiguration of mental health service delivery. Rather than functioning solely as substitutes for psychiatrists, PMHNPs often introduce distinct professional perspectives grounded in nursing frameworks that emphasize holistic assessment, patient education, and psychosocial support. These contributions may be particularly relevant in community mental health settings, where social determinants of health play a central role in patient outcomes [3]. The literature also suggests that PMHNPs may enhance system responsiveness during periods of crisis. During times of increased demand, such as public health emergencies or armed conflict, flexible deployment of PMHNPs across settings may help mitigate service disruptions. Their broad clinical training enables adaptation to diverse roles, including triage, short-term interventions, and coordination of follow-up care.
Future Directions in the Israeli Context
In Israel, the gradual implementation of the PMHNP role provides an opportunity to proactively address known barriers identified in previous advanced nursing initiatives. Early investment in structured role definition, interprofessional education, and organizational support may reduce resistance and facilitate smoother integration. Establishing clear expectations regarding scope of practice and decision-making authority may also support professional confidence and retention among PMHNPs. Future evaluation of the PMHNP role in Israel should extend beyond clinical outcomes to include organizational and system-level indicators. These may include waiting times for mental health services, continuity of care following hospitalization, patient satisfaction, and workforce stability. Qualitative research exploring the experiences of PMHNPs, psychiatrists, and service users may further illuminate facilitators and barriers to effective implementation.
5. Conclusions
The evidence reviewed suggests that Psychiatric–Mental Health Nurse Practitioners are well positioned to play a pivotal role in addressing current and future mental health challenges. When effectively integrated into mental health systems, PMHNPs can enhance access to care, support continuity of treatment, and maintain high-quality clinical outcomes, while contributing to more efficient and sustainable service delivery.
This review contributes to the literature by integrating clinical, organizational, and policy perspectives on PMHNPs and by situating their potential role within the unique challenges currently facing the Israeli mental health system. In a context of growing unmet need and workforce constraints, timely and strategic implementation of the PMHNP role—supported by clear regulation, organizational alignment, and interprofessional collaboration—may represent a critical opportunity to strengthen public mental health services and improve population well-being.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Y.S. and K.G.; methodology, Y.S. and K.G.; writing original draft preparation, Y.S.; writing-review and editing, Y.S., K.G., and R.N.-G.; supervision, K.G. and R.N.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
During the preparation of this manuscript, the author(s) used Chat GPT (OpenAI) for language editing and stylistic refinement. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three letter acronym |
| LD | Linear dichroism |
References
- Xu, J.-J.; Ding, L.-Y.; Sun, C.-C.; Qiao, Y.; Wang, M.-T.; Zheng, J.-X.; et al. The burden of mental disorders, substance use disorders, and self-harm among youths globally: Findings from the 2021 Global Burden of Disease study. Transl. Psychiatry 2025, 15, 346. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Mental Disorders Collaborators. Global prevalence and burden of mental disorders in 204 countries and territories in 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Mental Health Report: Transforming Mental Health for All; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- OECD. A New Benchmark for Mental Health Systems: Tackling the Social and Economic Costs of Mental Ill-Health; OECD Publishing: Paris, France, 2023. [Google Scholar]
- Rosenthal, G.; Tzur, R.; Hadas, H.; Tashler-Lazovik, S. The Economics of Mental Health in Israel: Current Status, International Comparison, Optimal Scope and Composition, Challenges, and Policy Recommendations. Position Paper. Mental Health Organizations Coalition: Israel, 2023. (In Hebrew) [Google Scholar]
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- International Council of Nurses. Guidelines on Advanced Practice Nursing; International Council of Nurses: Geneva, Switzerland, 2018. [Google Scholar]
- American Association of Nurse Practitioners. Historical Timeline of the Nurse Practitioner Role. Available online: https://www.aanp.org/about/about-the-american-association-of-nurse-practitioners-aanp/np-history (accessed on 19 January 2026).
- Kilpatrick, K.; Savard, I.; Audet, L.A.; Costanzo, G.; Khanassov, V.; Caspar, C.; et al. A global perspective of advanced practice nursing research: A review of systematic reviews protocol. PLoS ONE 2023, 18, e0280726. [Google Scholar] [CrossRef] [PubMed]
- McMenamin, A.; Turi, E.; Schlak, A.; Poghosyan, L. Outcomes related to nurse practitioner-delivered primary care for multiple chronic conditions: A systematic review. Med. Care Res. Rev. 2023, 80, 563–581. [Google Scholar] [CrossRef] [PubMed]
- DesRoches, C.M.; Clarke, S.; Perloff, J.; O’Reilly-Jacob, M.; Buerhaus, P. The quality of primary care provided by nurse practitioners to vulnerable Medicare beneficiaries. Nurs. Outlook 2017, 65, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Laurant, M.; van der Biezen, M.; Wijers, N.; Watananirun, K.; Kontopantelis, E.; van Vught, A.J. Nurses as substitutes for doctors in primary care. Cochrane Database Syst. Rev. 2018, 7, CD001271. [Google Scholar] [CrossRef] [PubMed]
- Christianson-Silva, P.; Russell-Kibble, A.; Shaver, J. Advanced practice palliative care nursing in Israel: A review. J. Hosp. Palliat. Nurs. 2021, 23, 21–27. [Google Scholar] [CrossRef]
- Hing, E.; Hooker, R.; Ashman, J. Primary health care in community health centers and comparison with office-based practice. J. Community Health 2011, 36, 406–413. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Nurses Association. Psychiatric–Mental Health Nursing: Scope and Standards of Practice, 3rd ed.; American Psychiatric Nurses Association: Chicago, IL, USA, 2022. [Google Scholar]
- Turi, E.; McMenamin, A.; Kueakomoldej, S.; Kurtzman, E.; Poghosyan, L. The effectiveness of nurse practitioner care for patients with mental health conditions in primary care settings: A systematic review. Nurs. Outlook 2023, 71, 101995. [Google Scholar] [CrossRef] [PubMed]
- Delaney, K.R.; Drew, B.L.; Rushton, C.H. Psychiatric mental health advanced practice registered nurse workforce and practice roles in the United States. J. Am. Psychiatr. Nurses Assoc. 2019, 25, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; McDowell, A.; Benson, N.M.; Cook, B.L.; Fung, V. Trends in participation in Medicare among psychiatrists and psychiatric mental health nurse practitioners, 2013–2019. JAMA Netw. Open 2022, 5, e2224368. [Google Scholar] [CrossRef] [PubMed]
- Haron, Y.; Romem, A.; Greenberger, C. The role and function of the palliative care nurse practitioner in Israel. Int. J. Palliat. Nurs. 2019, 25, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Porat-Dahlerbruch, J.; Ratz, S.; Aaron, E.; Ellen, M. Understanding factors affecting the integration of geriatric nurse practitioners into health systems. J. Am. Assoc. Nurse Pract. 2023, 35, 813–825. [Google Scholar] [CrossRef] [PubMed]
- Delaney, K.R.; Naegle, M.A.; Valentine, N.M.; Antai-Otong, D.; Groh, C.J.; Brennaman, L. The effective use of psychiatric mental health nurses in integrated care: Policy implications for increasing quality and access to care. J. Behav. Health Serv. Res. 2018, 45, 300–309. [Google Scholar] [CrossRef]
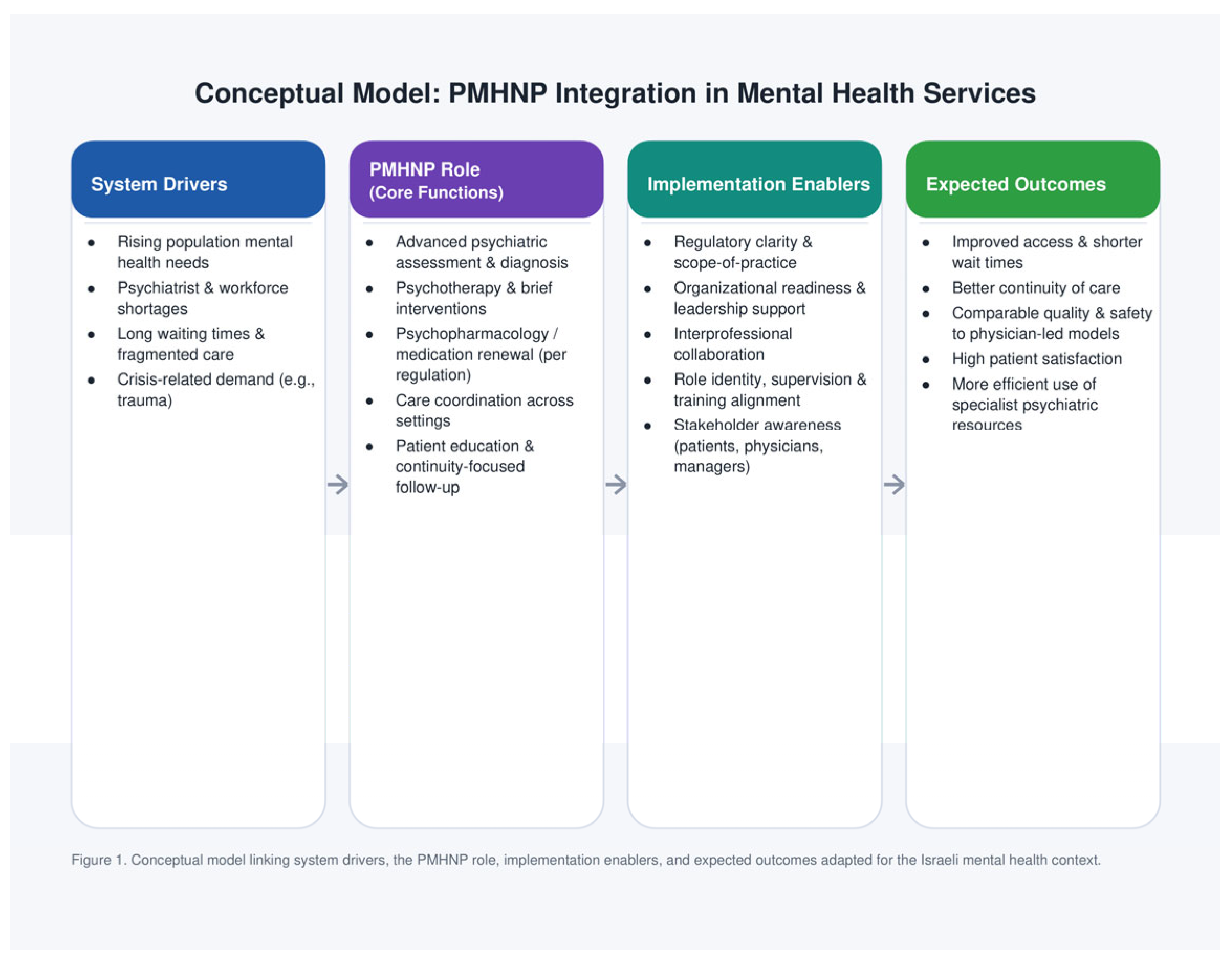
Figure 1.
Conceptual model linking system drivers, the PMHNP role, implementation enablers, and expected outcomes adapted for the Israeli mental health context.
Figure 1.
Conceptual model linking system drivers, the PMHNP role, implementation enablers, and expected outcomes adapted for the Israeli mental health context.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



