Submitted:
25 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
High blood pressure, a silent killer as it is often called, represents a major public health concern. A number of treatments are available, yet a large number of individuals fail to maintain proper blood pressure control. This highlights the need to find more effective ways for the prevention and supplementary approaches to the conventional therapeutic opions we have. This narrative review provides an overview of the available human evidence assessing various nutraceuticals showing potential in blood pressure control. A number fo essential elements, polyphenols, omega-3 fatty acids, probiotics and bioactive compounds including coenzyme Q10 and L-Arginine show promising results. A summary of their physiologic effects and research evidence behind blood control is given for every component.
Keywords:
blood pressure control
; nutraceuticals
; essential elements
; polyphenols
; omega-3 fatty acids
; bioactive compounds
; public health
1. Introduction
High blood pressure is an adjustable risk factor for cardiovascular illness and death globally impacting around 1.3 billion adults as reported by World Heath Organisation (WHO)and possibly increasing [1]. Despite the availability of effective treatments for hypertension, a large number of individuals still fail to maintain proper control, over their blood pressure. This persistent issue arises due to various elements, including patients failing to adhere to their medication regimen consistently encountering adverse effects from the treatments and the reality that relying on a single medication frequently falls short of fully lowering the residual risk of cardiovascular disease [2]. These challenges have heightened enthusiasm, for preventive and supplementary approaches that can be combined with conventional hypertension care.
Present clinical recommendations highlight lifestyle changes—specifically eating habits and physical exercise—as the approach to managing blood pressure [3,4]. While adopting a lifestyle is beneficial it frequently falls short on its own—particularly for individuals, with metabolic disorders or vascular lining injury. In these cases nutraceuticals (substances obtained from foods that provide health benefits beyond basic nourishment) are viewed as supportive complementary therapies [5]. Growing data suggest that certain nutraceuticals may affect biological mechanisms associated with the control of blood pressure, such, as endothelial NO availability, vascular tone, inflammatory signaling and the renin–angiotensin system (RAS) thus enhancing standard pharmacological treatment [6].
This analysis evaluates the existing data backing strategies, for controlling blood pressure within a comprehensive systems-oriented model. Unlike reviews that mainly focus on single compounds separately, it integrates findings across five mechanistically related groups: (1) minerals (magnesium, potassium, iodine, calcium); (2) polyphenols derived from tea, cocoa and berries; (3) omega-3 fatty acids; (4) probiotics influencing the gut–vascular axis; and (5) isolated bioactive substances, like coenzyme Q10 and L-arginine [6,7]. By clearly connecting how nutraceuticals work at the biological (molecular) level with evidence from human clinical trials—and by emphasizing how different nutrients interact with each other—this review takes a practical, clinical approach. It shows that nutraceuticals may (or may not) help reduce cardiovascular risk when used together with standard treatments, but they should not replace blood pressure medications.
Methods and Literature Search Strategy
A structured narrative review approach was used. PubMed, Google Scholar, Food Science and Technology Abstracts (FSTA), Web of Science, and Scopus databases were searched for peer-reviewed articles published between 1990 and December 2025. Search terms included combinations of: “hypertension”, “blood pressure”, “nutraceuticals”, “minerals”, “potassium”, “magnesium”, “calcium”, “iodine”, “polyphenols”, “omega-3 fatty acids”, “probiotics”, and “dietary supplements”.
Priority was given to all systematic reviews and meta-analyses, randomized controlled trials and major epidemiological studies. Mechanistic studies were included when they provided clear insight into biological pathways relevant to blood pressure regulation.
International clinical guidelines were used to contextualize clinical relevance. Studies not published in English or Croatian, animal-only studies without clear translational relevance, and reports with insufficient methodological detail were excluded.
A summary of identified nutraceuticals with positive effect on blood pressure in is provided in Table 1.
2. Essential Minerals and Blood Pressure Regulation
Minerals are crucial in strategies for controlling high blood pressure. Beyond preserving electrolyte balance essential minerals assist in managing blood vessel activity promote signaling within the endothelium affect kidney sodium processing and modulate hormonal mechanisms related to blood pressure. These minerals work synergistically—their overall interaction is particularly significant. Notably the ratio of sodium to potassium in the diet is a reliable indicator of cardiovascular mortality, than sodium consumption alone [8].
Mechanistically, potassium, magnesium, calcium, and iodine influence blood pressure regulation through modulation of the renin–angiotensin–aldosterone system (RAAS), regulation of the Na⁺/K⁺-ATPase pump, effects on intracellular calcium signaling, and endocrine pathways affecting vascular function (Figure 1) [9,10]. Correction of mineral insufficiency therefore represents a generally low-risk strategy with potential population-level benefits for foundational blood pressure management. The principal biological pathways through which these minerals may influence blood pressure regulation are illustrated in Figure 1.
2.1. Potassium: A Central Dietary Determinant of Blood Pressure
Potassium ranks as an important dietary factor influencing blood pressure. Epidemiological research reliably shows that groups consuming levels of potassium—mainly sourced from fruits, vegetables, legumes and whole grains—experience lower blood pressure, throughout their lives and a decreased chance of stroke and cardiovascular incidents [11,12].
Multiple complementary processes play a role in the blood pressure-lowering effects of potassium. Within the kidneys higher potassium consumption encourages natriuresis by decreasing the activity of the sensitive sodium–chloride cotransporter in the distal convoluted tubule thus opposing sodium-driven volume expansion [13]. In the physiological system, potassium boosts Na⁺/K⁺-ATPase activity and triggers ATP-sensitive potassium (K_ATP) channels, in vascular smooth muscle cells. These effects promote membrane hyperpolarization and reduce intracellular calcium concentrations, resulting in vasodilation and a subsequent decrease in peripheral vascular resistance [14].
Clinical studies and systematic reviews validate the effectiveness of potassium supplementation in lowering blood pressure. An extensive meta-analysis revealed decreases in both systolic and diastolic blood pressure particularly in subjects, with hypertension and elevated initial sodium consumption [15]. This dose-related association highlights the role of potassium in reestablishing the sodium–potassium equilibrium instead of functioning as a standalone treatment [16].
Dietary potassium intake is safe and recommended for the vast majority of individuals. However, potassium supplementation should be used cautiously in patients with advanced chronic kidney disease or those receiving potassium-sparing diuretics (e.g., spironolactone) due to the risk of hyperkalemia [17].
2.2. Magnesium: A Physiological Calcium Antagonist
Magnesium is an intracellular ion that participates in more than 300 enzymatic processes, such, as those regulating vascular smooth muscle tone, endothelial activity and electrolyte balance [18]. Inadequate magnesium consumption is common worldwide. Magnesium has been closely linked to hypertension, insulin resistance and metabolic syndrome [19,20].
Magnesium acts as an antagonist to calcium by vying with calcium at voltage-gated calcium channels thus preventing calcium from entering vascular smooth muscle cells. This mechanism diminishes smooth muscle contraction. Decreases peripheral vascular resistance [21,22]. Furthermore intracellular magnesium enhances Na⁺/K⁺-ATPase function aiding in the preservation of gradients essential for vasodilation [23]. Apart from its vascular impacts, magnesium enhances endothelial function by decreasing oxidative stress boosting NO availability and diminishing systemic inflammation evidenced by decreased levels of C-reactive protein [24,25].
Evidence from randomized controlled trials indicates that magnesium supplementation produces modest but clinically meaningful reductions in blood pressure. Meta-analyses report average reductions in systolic blood pressure of approximately 2–4 mmHg, particularly in individuals with hypertension or low baseline magnesium status [26,27]. The antihypertensive response is influenced by magnesium formulation, with organic salts (e.g., magnesium citrate, glycinate, or lactate) demonstrating superior bioavailability compared with inorganic forms such as magnesium oxide, which is poorly absorbed and frequently associated with gastrointestinal side effects [28].
2.3. Calcium: The Dietary Calcium Paradox
Calcium has a function in cardiovascular physiology. Although intracellular calcium facilitates contraction of smooth muscle and vasoconstriction sufficient dietary calcium consumption has been reliably linked to reduced blood pressure in both observational and intervention studies [29]. This negative correlation is believed to result from calcium’s influence, on hormone (PTH) secretion and the renin–angiotensin system. Insufficient dietary calcium triggers PTH release, which raises calcium levels in vascular smooth muscle cells leading to vasoconstriction and high blood pressure [30,31].
Extensive dietary studies, such as the DASH (Dietary Approaches to Stop Hypertension) trial have shown that diets high, in calcium considerably lower blood pressure [11]. Meta-analyses of trials involving calcium supplements also indicate statistically meaningful, yet moderate decrease in blood pressure [33].
Nonetheless a controversial “calcium paradox” is present regarding supplementation. Although dietary calcium seems to offer protection, high-dose calcium supplements—especially when taken without vitamin D or magnesium—have been linked to heightened vascular calcification and cardiovascular risk [34]. As a result, current evidence favors achieving recommended calcium intakes (approximately 1,000–1,200 mg/day) through dietary sources such as dairy products, leafy green vegetables, and fortified foods, rather than through isolated high-dose supplements [35].
2.4. Iodine: Thyroid-Mediated Blood Pressure Regulation
In contrast to potassium and magnesium, iodine does not have a vasodilatory action. Rather its effect on blood pressure occurs via its function, in the production of thyroid hormones. Thyroid hormones (T₃ and thyroxine T₄) control metabolic rate, heart output, systemic vascular resistance and endothelial performance [36].
Both insufficient and excessive iodine levels interfere with thyroid balance and may negatively impact blood pressure control.Hypothyroidism, commonly linked to iodine scarcity, raises vascular resistance and arterial rigidity mainly leading to diastolic hypertension. In contrast, hyperthyroidism—possibly caused by much iodine consumption—increases cardiac output and can cause systolic hypertension [37,38]. Thyroid hormones also directly affect tissues with T₃ encouraging endothelial NO synthesis and aiding vasodilation [39].
Although iodine is not a primary antihypertensive agent, maintaining euthyroid status is a prerequisite for optimal cardiovascular and blood pressure regulation. Epidemiological studies demonstrate a U-shaped association between iodine intake and hypertension, with both insufficient and excessive intake linked to adverse effect on blood pressure [40]. Clinically, the emphasis remains on ensuring adequate iodine intake through dietary sources such as iodized salt and seafood, while avoiding high-dose supplementation that may precipitate thyroid dysfunction [41,42].
3. Polyphenols and Blood Pressure Regulation
Polyphenols are diverse group of bioactive compounds that can be find in foods and drinks that come from plants. Polyphenols are important topic because they might have m positive impact for heart and blood vessels which will be reviewed in this paper. Many studies have shown that some foods that are rich in polyphenols can help lower blood pressure, which is especially important for people who already have problems with their blood vessels or are at risk for heart disease. Polyphenols may help make NO more available in the body. They also may reduce the effects of oxidative stress and inflammation.
In this section, the evidence on polyphenols is presented across three major dietary sources with the strongest human data: (1) cocoa flavanols, (2) tea catechins and theaflavins, and (3) berry-derived anthocyanins. For each subgroup, mechanistic pathways, results from randomized controlled trials and meta-analyses, and relevant clinical considerations are summarized in order to contextualize their potential role as adjunctive nutraceutical strategies in blood pressure management.
3.1. General Mechanisms of Polyphenol Action in Blood Pressure Regulation
Dietary polyphenols constitute an structurally varied class of plant-derived secondary metabolites that have garnered growing interest for their possible advantages in cardiovascular health. These substances are commonly found in plant-origin foods and drinks such, as cocoa, tea, berries, fruits, vegetables and red wine. An increasing amount of epidemiological and clinical research indicates that dietary polyphenols might aid in controlling blood pressure via several interconnected mechanisms related to endothelial function, oxidative stress, inflammation and vascular architecture [43,44].
A major pathway through which polyphenols affect tone and blood pressure is by boosting the availability of endothelial NO. NO plays a role in maintaining vascular balance and disrupted NO signaling is a hallmark of endothelial dysfunction, in hypertension. Multiple polyphenols have demonstrated the ability to activate nitric oxide synthase (eNOS) via phosphorylation-related signaling routes, leading to greater NO availability and enhanced endothelium-dependent vasodilation [45,46]. These outcomes might lower vascular resistance and help in slightly decreasing systolic and diastolic blood pressure.
Polyphenols can also impact stress by regulating reactive oxygen species (ROS) generation and antioxidant defense mechanisms; rather than functioning mainly as direct radical scavengers, they appear to diminish oxidative stress by inhibiting ROS-producing enzymes such as NADPH oxidase and by protecting nitric oxide (NO) from oxidative degradation. [47]. By curbing stress, polyphenols contribute to preserving endothelial function and may reduce vascular stiffening linked to hypertension and atherosclerosis [48].
Furthermore polyphenols have demonstrated the ability to regulate signaling cascades associated with vascular impairment. Research findings suggest that polyphenols can affect agents, particularly pathways involving nuclear factor κB (NF-κB) which leads to decreased activation and vascular inflammation [49]. Additional processes that might indirectly aid in managing blood pressure encompass the suppression of angiotensin-converting enzyme (ACE) activity, adjustment of endothelin-1 synthesis and enhancement of insulin sensitivity [50,51]. Taken together, these measures indicate that polyphenols exert significant effects on vascular health, with important implications for both the prevention and management of hypertension.
3.2. Cocoa and Flavanols
Flavanols obtained from cocoa are some of the thoroughly researched polyphenols when it comes to effects on vascular health and blood pressure control. The main active components in cocoa comprise (–)-epicatechin, catechin and oligomeric procyanidins, all of which have been regularly linked to enhancements, in performance and arterial flexibility (see Figure 2 for catechin structure) [52,53].
Mechanistic research suggests that cocoa flavanols boost NO availability by stimulating eNOS activity and decreasing breakdown of NO [54]. Both short-term and prolonged intake of flavanol-rich cocoa items have been demonstrated to enhance flow-mediated dilation (FMD) a common non-invasive indicator of endothelial function indicating improved vasodilatory ability [55]. Additionally cocoa flavanols have been found to lower stiffness and wave reflection leading to beneficial impacts, on central hemodynamics [56].
Findings from controlled trials and meta-analyses show that consistent intake of flavanol-rich cocoa or dark chocolate corresponds with small yet statistically significant decreases in both systolic and diastolic blood pressure especially in people with hypertension or compromised endothelial function [57,58]. Meta-analytical evidence indicates reductions in systolic blood pressure of, around 3–5 mmHg, which could have clinical importance from a population perspective [59].
The impact of cocoa products on health is largely influenced by the flavanol levels and the techniques used in processing. Numerous chocolate items on the market possess low flavanol amounts alongside elevated sugar and saturated fat content potentially diminishing their beneficial effects [60]. Hence, using cocoa products high in flavanols is more suitable, for assessing therapeutic outcomes.
3.3. Tea Polyphenols: Green and Black Tea
Tea is among the most widely consumed beverages worldwide and represents a major dietary source of polyphenols. Green tea is particularly rich in catechins, especially epigallocatechin gallate (EGCG), whereas black tea contains theaflavins and thearubigins formed through enzymatic oxidation.Although their polyphenol profiles differ, both green and black tea have been linked to impacts, on vascular health and the control of blood pressure [61,62].
Catechins found in tea have demonstrated the ability to enhance endothelial function by increasing NO availability lowering oxidative stress and boosting insulin sensitivity [63]. EGCG is known to stimulate eNOS and influence inflammatory signaling pathways aiding in vascular responsiveness [64]. Polyphenols in tea produce comparable vascular benefits though variations, in their bioavailability and metabolism could affect their physiological effects [65].
Observational research, randomized controlled trials and meta-analyses suggest that consistent tea drinking is linked to decreases in both systolic and diastolic blood pressure [66]. A meta-analysis of intervention studies found that continuous intake of black tea for a minimum of 12 weeks led to an average systolic blood pressure drop of about 2–3 mmHg [67]. While these reductions are modest for individuals they could have public health consequences due, to the extensive consumption of tea.
3.4. Berries and Anthocyanins
Berries are a rich dietary source of anthocyanins, a class of flavonoids responsible for the red, blue, and purple pigmentation of fruits such as blueberries, strawberries, blackberries, and cherries. The vascular protective effects of anthocyanins, along with their potential role in blood pressure regulation, have been the focus of increasing research interest [68,69].
Anthocyanins have demonstrated the ability to enhance function via several mechanisms, such as increasing NO bioavailability lowering oxidative stress and regulating inflammatory pathways [70]. Beyond impacts there is some evidence indicating that anthocyanins could affect vascular structure, including decreases in arterial stiffness and enhancements, in microvascular function [71].
Clinical trials evaluating whole-berry consumption or anthocyanin supplementation have reported modest reductions in blood pressure, particularly in individuals with hypertension or elevated cardiovascular risk [72]. Meta-analyses indicate that anthocyanin-rich interventions may reduce systolic blood pressure by approximately 2–4 mmHg, with variability depending on dose, duration, and berry source [73]. Overall, current evidence supports the inclusion of anthocyanin-rich foods as part of a polyphenol-rich dietary pattern aimed at improving vascular health and supporting blood pressure control.
4. Omega-3 Fatty Acids
Omega-3 polyunsaturated fatty acids (PUFAs) are dietary fats that play an important role in cardiovascular health and have been extensively studied for their effects on blood pressure regulation.The main omega-3 fatty acids pertinent to biology are eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) mostly obtained from marine origins along with α-linolenic acid (ALA), from plant-based sources [90]. Of these EPA and DHA have shown the reliable blood pressure-lowering benefits, in both laboratory and clinical studies [75,91].
4.1. Mechanisms Underlying the Antihypertensive Effects of Omega-3 Fatty Acids
Omega-3 fatty acids influence blood pressure through synergistic mechanisms that target vascular health, inflammation, and neurohormonal regulation. A key pathway involves enhancement of endothelial function by increasing nitric oxide (NO) availability.EPA and DHA integrate into cell membranes enhancing membrane flexibility and stimulating endothelial nitric oxide synthase (eNOS) activity, which leads to better vasodilation [74,75].
Furthermore omega-3 fatty acids demonstrate anti-inflammatory properties by altering eicosanoid synthesis and generating specialized pro-resolving lipid mediators, including resolvins and protectins [79]. These substances diminish inflammation and endothelial activation, which are strongly associated with higher vascular resistance and hypertension [80]. Additionally omega-3 fatty acids decrease oxidative stress, by suppressing NADPH oxidase activity and boosting defense mechanisms thus maintaining NO bioavailability [76].
Omega-3 fatty acids also aid in controlling blood pressure by decreasing rigidity and enhancing arterial flexibility especially in major elastic arteries [81,82]. Other processes involve adjusting nervous system function marked by lowered sympathetic activity and slight suppression of the renin–angiotensin–aldosterone system (RAS) which together help reduce blood pressure [74,75].
4.2. Clinical Evidence for Blood Pressure Reduction
The blood pressure-lowering properties of omega-3 fatty acids have been investigated in randomized controlled trials and meta-analyses. Initial clinical research showed that supplementation with doses of fish oil led to notable decreases in systolic and diastolic blood pressure especially in patients with untreated hypertension [84]. Subsequent meta-analyses have validated these results showing dose-related declines in blood pressure, in groups [86].
A comprehensive meta-analysis of controlled trials found that omega-3 fatty acid supplementation lowered systolic blood pressure by around 4–5 mmHg and diastolic blood pressure by 2–3 mmHg in people with hypertension with lesser yet still meaningful effects seen in individuals with normal blood pressure [85]. Importantly DHA seems to have a potent blood pressure–reducing effect compared to EPA possibly because of its more pronounced influence, on arterial stiffness and endothelial function [82,87].
Regular consumption of fatty fish providing omega-3 fatty acids has been linked to decreased blood pressure and a lower risk of hypertension in observational research [88]. Nonetheless the human conversion of ALA, into EPA and DHA is restricted, which could account for the more inconsistent antihypertensive outcomes seen with plant-derived omega-3 sources [89].
4.3. Safety, Dosage, and Clinical Considerations
Omega-3 fatty acid supplements are generally safe and well tolerated when taken within recommended limits. Reported side effects are usually mild, including digestive discomfort and a fishy aftertaste, while higher doses may slightly increase bleeding risk in susceptible individuals [75,91]. Existing data indicate that daily consumption of 2–3 g of combined EPA and DHA works best for lowering blood pressure although smaller doses can still offer advantages if taken regularly [91].
Interindividual variability in response to omega-3 supplementation may be influenced by baseline blood pressure, habitual diet, genetic factors, and the EPA:DHA ratio of the supplement [74,75]. Consequently, omega-3 fatty acids should be considered an adjunctive nutraceutical strategy rather than a replacement for pharmacological therapy in individuals with established hypertension.
5. Probiotics and the Gut–Vascular Axis
The gut microbiome is progressively acknowledged as a modulator of cardiovascular well-being affecting blood pressure via intricate interactions between microbial metabolites, host metabolism, immune functions and vascular health. Increasing research evidence backs the idea of a gut– axis, in which changes, in gut microbial makeup and metabolic processes play a role in the onset and advancement of hypertension [93,94]. In this context probiotics—described as living microbes that provide health advantages when given in quantities—have appeared as possible nutraceutical options, for controlling blood pressure [99].
5.1. Gut Microbiota Dysbiosis and Hypertension
Hypertension has consistently been linked to gut microbiota imbalance, marked by reduced microbial diversity and shifts in the relative abundance of key bacterial taxa, including a depletion of short-chain fatty acid–producing genera such as Faecalibacterium, Roseburia, and Bifidobacterium, alongside an increased abundance of potentially pro-inflammatory taxa such as Prevotella, Desulfovibrio, and members of the Enterobacteriaceae family. [93]. Findings from models and human observational research show that people with hypertension have different gut microbial compositions compared to normotensive individuals, especially concerning bacteria associated with short-chain fatty acid (SCFA) synthesis and inflammation control [94]. Experimental data back up a role of the gut microbiota in managing blood pressure. In animal studies transferring microbiota from hypertensive donors to normotensive recipients has demonstrated an elevation in blood pressure while transplantation from normotensive donors provides protective benefits [99]. These results emphasize the importance of metabolites and host–microbe interactions, in maintaining vascular homeostasis.
5.2. Mechanisms Linking Probiotics to Blood Pressure Regulation
A key way probiotics might affect blood pressure is by generating short-chain fatty acids, like acetate, propionate and butyrate via the fermentation of fibers. These SCFAs engage with host receptors, including G protein–coupled receptors (GPR41 and GPR43) found in vascular, kidney and immune system tissues resulting in vasodilation and alteration of nervous system function [94].
Probiotics can additionally influence blood pressure by modulating the gut system and reducing inflammation, as dysbiosis-induced increases in intestinal permeability allow pro-inflammatory microbial components such as lipopolysaccharides to enter circulation, triggering systemic inflammation and endothelial dysfunction [94]. Adding probiotics has been demonstrated to strengthen the gut barrier, inflammatory markers, in the bloodstream and enhance endothelial performance—mechanisms strongly associated with the development of hypertension [99].
Other mechanisms involve altering the angiotensin system (RAS). Some probiotic strains produce peptides that inhibit angiotensin-converting enzyme (ACE) thus producing effects similar, to pharmacological ACE inhibitors but through a nutraceutical approach [95]. Additionally probiotics can impact bile acid metabolism, stress and insulin sensitivity which may indirectly influence vascular health and the control of blood pressure [96].
5.3. Clinical Evidence for Probiotic Interventions
Clinical studies assessing supplementation have found small yet statistically meaningful decreases in blood pressure. Meta-analyses of controlled trials suggest that probiotics can lower systolic blood pressure by around 2–4 mmHg and diastolic blood pressure by 1–2 mmHg with stronger effects seen in those, with hypertension or metabolic disorders [97,98].
The blood pressure-lowering effectiveness of probiotics seems to rely on aspects, such as the choice of strain the amount administered length of treatment and initial blood pressure levels. Formulations with strains and treatment periods of 8–12 weeks or longer generally show more reliable reductions in blood pressure compared to short-term or single-strain research [99]. The majority of trials have concentrated on strains, from the Lactobacillus and Bifidobacterium genera though new data indicates that next-generation probiotics might provide further cardiovascular advantages [100].
5.4. Limitations and Future Perspectives
Although the results are promising multiple limitations must be taken into account when evaluating the blood pressure-lowering effects of probiotics. Significant variation in strains, dosing schedules, study participants and measured outcomes restricts direct study comparisons and prevents conclusive statements [101]. Additionally differences in gut microbiota among individuals might affect how they respond to treatment underscoring the possible need, for personalized strategies [102].
Future studies should focus on identifying the specific probiotic strains and microbial metabolites most relevant to blood pressure regulation, as well as clarifying the interactions between probiotics, diet, and host factors. Well-designed, long-term randomized controlled trials are needed to determine optimal formulations and to establish the role of probiotics as adjunctive therapies for managing hypertension.5.5. Summary
In summary, probiotics represent a mechanistically plausible nutraceutical approach to blood pressure management through modulation of the gut–vascular axis. By influencing microbial metabolite production, inflammatory signaling, endothelial function, and neurohormonal pathways, probiotics may confer modest but clinically relevant benefits, particularly when incorporated into comprehensive dietary and lifestyle interventions.
6. Coenzyme Q10 and L-Arginine
Coenzyme Q10 (CoQ10) and L-arginine are biological substances that affect blood pressure control mainly by impacting mitochondrial activity oxidative stress levels and NO availability. Unlike minerals or polyphenols, these substances exert a more direct influence on cellular energy metabolism and the signaling mechanisms of the endothelium rendering them especially pertinent, in medical situations marked by endothelial impairment and heightened oxidative stress, including hypertension [106,107].
6.1. Coenzyme Q10
Coenzyme Q10, also known as ubiquinone, is a lipid-soluble molecule essential for mitochondrial electron transport and the production of adenosine triphosphate (ATP). In addition to its role in energy generation, CoQ10 functions as a natural antioxidant, protecting cell membranes and lipoproteins from oxidative damage [108,109].
Lower circulating and tissue concentrations of CoQ10 have been observed in patients with hypertension and various cardiovascular diseases indicating a link to blood pressure imbalance [107]. The blood pressure-lowering properties of CoQ10 are believed to result from enhancing endothelial function and maintaining redox equilibrium. CoQ10 reduces oxidative stress by neutralizing reactive oxygen species and regenerating other antioxidants, including vitamin E, thereby supporting the maintenance of nitric oxide availability [104,109]. Improved induced vasodilation correlates with decreases, in peripheral vascular resistance and blood pressure [111,112]. Moreover CoQ10 has demonstrated the ability to enhance function in both vascular and cardiac tissues potentially aiding vascular tone and heart function [108].
Clinical research examining CoQ10 supplementation has found clinically meaningful declines in blood pressure especially among those with uncontrolled or resistant hypertension. Randomized controlled trials and meta-analyses have shown drops in systolic and diastolic blood pressure with average decreases typically between about 5 to 17 mmHg for systolic and 3 to 10 mmHg, for diastolic readings [113,114]. Meta-analyses indicate that CoQ10 can reduce blood pressure; however significant variability, in study design, dosage and sample size requires consideration when interpreting these results [113].
CoQ10 supplementation is usually well accepted, exhibiting a safety profile with minimal side effects noted at typical doses (generally 100–300 mg/day) [115,116]. However, variations in formulation, absorption, and study design, along with a lack of long-term trials, underscore the need for more rigorous research to establish standardized dosing guidelines and clarify the long-term cardiovascular effects [117].
6.2. L-Arginine
L-arginine is an essential amino acid acting as the main substrate for endothelial nitric oxide synthase (eNOS) and thus plays a crucial role in NO generation and vascular health [105]. A decrease in L-arginine levels and compromised NO production are traits of endothelial dysfunction and high blood pressure supporting the mechanistic basis, for using L-arginine supplements in controlling blood pressure [105].
L-arginine supplementation boosts NO generation resulting in endothelium- vasodilation, better arterial flexibility and lowered peripheral vascular resistance [119]. Beyond its role, in NO production L-arginine is reported to affect oxidative stress and inflammation pathways thus promoting endothelial function [120]. Research also indicates L-arginine might affect insulin sensitivity and autonomic nervous system regulation potentially aiding in blood pressure management indirectly [120].
Clinical data on the blood pressure-lowering effects of L-arginine are varied but mostly favorable. Multiple randomized controlled studies have observed decreases in blood pressure after oral L-arginine intake especially among patients with hypertension, metabolic syndrome or compromised endothelial function [119]. Meta-analyses of these trials show drops of about 4–5 mmHg in systolic and 2–3 mmHg, in diastolic blood pressure [121,122].
The extent of response to L-arginine supplementation seems to be influenced by NO levels amount administered length of treatment and existing comorbidities [122]. High doses may cause complications, so caution is advised for patients with severe cardiovascular conditions or those taking medications that could interact. [123]. Evidence on long-term effectiveness is still scarce and other approaches focusing on the NO pathway—, like L-citrulline supplementation potentially providing better bioavailability—have been suggested [124].
6.3. Summary
In summary, Coenzyme Q10 and L-arginine represent mechanistically distinct nutraceutical strategies for blood pressure management. CoQ10 primarily acts by enhancing mitochondrial function and reducing oxidative stress, whereas L-arginine directly promotes nitric oxide synthesis and endothelium-dependent vasodilation. Both compounds have shown modest antihypertensive effects in clinical studies, particularly in populations with endothelial dysfunction. Nevertheless, large-scale, long-term randomized trials are needed to confirm their sustained efficacy and to establish their optimal role in clinical practice.
7. Nutrients Influencing Endothelial Function and the Renin–Angiotensin System (RAS)
Impaired function and dysregulation of the renin–angiotensin system (RAS) are key pathophysiological features of hypertension, contributing significantly to increased vascular resistance, arterial stiffness, and elevated cardiovascular risk. The vascular endothelium plays a central role in regulating vascular tone, inflammation, thrombosis, and oxidative balance, while the RAS is a critical hormonal system that controls blood pressure through effects on vasoconstriction, sodium homeostasis, and sympathetic nervous system activation [125,126]. Increasing data suggests that certain nutrients and nutraceuticals can affect performance and RAS function thus offering additional approaches, for controlling blood pressure.
7.1. Endothelial Function as a Target for Nutraceutical Intervention
Dysfunctional endothelial activity, frequently marked by lowered oxide (NO) availability and heightened oxidative stress is a key feature of hypertension and frequently occurs before obvious cardiovascular disease manifests [127]. Multiple nutrients highlighted in this review—such as polyphenols, omega-3 fatty acids, magnesium, L-arginine and coenzyme Q10—have shown impacts, on endothelial function via somewhat overlapping pathways [128,129]. Polyphenols, flavanols boost endothelial NO synthesis by activating endothelial nitric oxide synthase (eNOS) and by decreasing oxidative degradation of NO [130]. Omega-3 fatty acids enhance performance, by exerting anti-inflammatory actions modifying membrane composition and regulating eNOS signaling pathways [131]. Magnesium maintains health by affecting calcium balance lessening oxidative stress and lowering low-grade inflammation [22]. L-arginine acts as the substrate for eNOS and may increase NO production when availability is compromised whereas coenzyme Q10 maintains NO bioavailability mainly via its antioxidant effects and support of mitochondrial function [109,133]. Collectively these actions correlate with endothelium-dependent vasodilation and diminished vascular impairment, in hypertension [135].
7.2. Nutritional Modulation of the Renin–Angiotensin System
The RAS regulates blood pressure and extracellular fluid balance, with angiotensin II acting as a potent vasoconstrictor and pro-inflammatory mediator; prolonged activation of this system can lead to structural vascular changes and sustained hypertension. [136]. Various nutrients and bioactive substances affect RAS function at regulatory points. Increased dietary potassium reduces release and lessens angiotensin II–induced vasoconstriction thus opposing the blood pressure-raising impact of too much sodium consumption [137]. Magnesium might indirectly influence RAS signaling by impacting stress and insulin sensitivity, which in turn affect renin and aldosterone function [138]. Some polyphenols, such, as flavanols and catechins show angiotensin-converting enzyme (ACE) effects resulting in decreased angiotensin II production and improved vasodilation [50]. Moreover certain bioactive peptides derived from probiotics possess ACE- capabilities connecting gut microbiota-related pathways to RAS control [95]. Omega-3 fatty acids additionally reduce RAS-associated impairment, by inhibiting angiotensin II–triggered inflammation and oxidative damage [80].
7.3. Integrated Effects on Vascular Remodeling and Blood Pressure
Apart from the impact on vascular tone, long-term adjustment of endothelial function and RAS activity can affect vascular remodeling, which entails structural alterations, in the arterial wall contributing to chronic hypertension [142]. Nutrients that diminish stress, inflammation and angiotensin II pathways might aid in preventing harmful remodeling and enhance arterial flexibility gradually [143]. These combined effects underscore the importance of overall dietary patterns rather than focusing solely on individual nutrients. Diets rich in fruits, vegetables, whole grains, fatty fish, and fermented foods—such as the DASH and Mediterranean diets—naturally provide many of these bioactive compounds and have consistently demonstrated blood pressure-lowering effects in controlled clinical trials [11,145].
7.4. Clinical and Translational Implications
From a standpoint nutraceuticals affecting endothelial performance and RAS function could be especially significant for patients with early hypertension, endothelial impairment or ongoing cardiovascular risk despite drug treatments [146]. Although these interventions cannot replace drugs in high-risk groups they might act as helpful complementary approaches to enhance vascular function and aid in managing blood pressure [4]. Nonetheless, interindividual variability, inconsistent nutraceutical formulations, and limited long-term outcome data remain significant challenges. Future research should prioritize well-designed randomized controlled trials with clinically meaningful endpoints and identify the patient populations most likely to benefit from targeted nutraceutical interventions [148].
7.5. Summary
In summary, current evidence supports a role for selected nutrients and nutraceuticals in modulating endothelial function and the renin–angiotensin system—two fundamental mechanisms in blood pressure regulation. Through complementary actions on NO bioavailability, oxidative stress, inflammation, and hormonal signaling pathways, these compounds represent biologically plausible and clinically relevant components of dietary strategies for the prevention and management of hypertension.
8. Conclusions
Hypertension continues to be the primary cause of cardiovascular illness and death worldwide. Despite effective drug treatments exist, blood pressure control is often unattained. The data compiled in this narrative review show that nutraceuticals can serve as a supplementary option in managing blood pressure by addressing crucial pathophysiological factors, such as endothelial dysfunction, oxidative damage, inflammation, vascular rigidity, gut–vascular communication and disturbances in the renin–angiotensin system. Key minerals, foods abundant in polyphenols, omega-3 fatty acids, probiotics and particular bioactive agents like coenzyme Q10 and L-arginine demonstrate clinically significant decrease in blood pressure, especially among hypertensive individuals, metabolic issues or endothelial dysfunction. Notably, these impacts seem to be cumulative and synergistic when nutraceuticals are taken as part of dietary regimens rather than, as standalone high-dose supplements.
When we look at the public health picture, these findings tell us that using nutraceuticals might be a good strategy to help manage high blood pressure. Nutraceuticals are not meant to take the place of the medicines that doctors prescribe or the changes we make to our lifestyle. Instead nutraceuticals can work together with these things to help keep our blood pressure under control. The goal is to manage hypertension and nutraceuticals can be an addition, to the other things we are already doing to manage hypertension.
The change in blood pressure for each person is usually not that big. When you look at the whole population even small changes in average blood pressure can make a big difference. This means that fewer people will have heart problems and die from them. So even if a treatment only lowers blood pressure a bit it can still have a big impact on the health of the population. This is especially true if the treatment is safe and lots of people can get it. Blood pressure reduction can have an effect on public health. Even small reductions, in blood pressure can be very important.
There are still problems when it comes to using nutraceutical research to help people. One of the issues is that all the studies are very different. They use designs and different supplements and the dosage and how long people take them varies a lot. People also react to these supplements in ways. This makes it really hard to come up with rules for doctors to follow.
To fix these problems we need to do research. We should do studies that last a long time and compare different groups of people. We need to make sure everyone in the study is taking the supplement and that we are measuring the right things to see if it is working. We also need to look at the types of people in the study to see who is most likely to get better from taking nutraceuticals. This way we can give doctors advice, on how to use nutraceuticals to help their patients.
Within this context, the targeted integration of evidence-based nutraceuticals into personalized dietary and therapeutic frameworks represents a pragmatic, low-risk strategy for improving vascular health and supporting blood pressure control across the continuum of cardiovascular risk.
List of Abbreviations
| ACE | Angiotensin-converting enzyme |
| BP | Blood pressure |
| CoQ10 | Coenzyme Q10 |
| DASH | Dietary Approaches to Stop Hypertension |
| DHA | Docosahexaenoic acid |
| eNOS | Endothelial nitric oxide synthase |
| EPA | Eicosapentaenoic acid |
| NO | Nitric oxide |
| PUFA | Polyunsaturated fatty acid |
| RAAS | Renin–angiotensin–aldosterone system |
| RAS | Renin–angiotensin system |
| RCT | Randomized controlled trial |
| ROS | Reactive oxygen species |
| SCFA | Short-chain fatty acid |
| WHO | World Health Organization |
References
- World Health Organization. Global Report on Hypertension: The Race Against a Silent Killer; World Health Organization: Geneva, 2023; Available online: https://www.who.int/publications/i/item/9789240081062 (accessed on 14 December 2025).
- Burnier, M.; Egan, B.M. Adherence in hypertension. Circ. Res. 2019, 124, 1124–1140. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; et al. 2017 ACC/AHA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef]
- Kalra, E.K. Nutraceutical—Definition and introduction. AAPS PharmSci 2003, 5, 27–28. [Google Scholar] [CrossRef]
- Huang, L.; Trieu, K.; Yoshimura, S.; et al. Effect of nutraceuticals on blood pressure: A systematic review and meta-analysis. J. Clin. Hypertens. 2020, 22, 327–336. [Google Scholar] [CrossRef]
- He, F.J.; MacGregor, G.A. Dietary minerals and blood pressure. Curr. Opin. Nephrol. Hypertens. 2008, 17, 224–229. [Google Scholar]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. BMJ 2013, 346, f1378. [Google Scholar] [CrossRef]
- Houston, M.C. The role of magnesium in hypertension and cardiovascular disease. Journal of Clinical Hypertension 2011, 13(11), 843–847. [Google Scholar] [CrossRef]
- Weaver, C.M.; Heaney, R.P. Calcium in Human Health; Humana Press: Totowa, NJ, USA, 2006. [Google Scholar]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; et al. A clinical trial of the effects of dietary patterns on blood pressure (DASH). N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef]
- Mente, A.; O’Donnell, M.J.; Rangarajan, S.; et al. Association of urinary sodium and potassium excretion with blood pressure. N. Engl. J. Med. 2014, 371, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.E. The kidney, hypertension, and obesity. Hypertension 2003, 41, 625–633. [Google Scholar] [CrossRef]
- Haddy, F.J.; Vanhoutte, P.M.; Feletou, M. Role of potassium in regulating blood flow and blood pressure. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 290, R546–R552. [Google Scholar] [CrossRef] [PubMed]
- Filippini, T.; Violi, F.; D’Amico, R.; Vinceti, M. The effect of potassium supplementation on blood pressure in hypertensive and normotensive subjects: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 230, 127–135. [Google Scholar] [CrossRef]
- Aaron, K.J.; Sanders, P.W. Role of dietary salt and potassium intake in cardiovascular health and disease: A review of the evidence. Mayo Clin. Proc. 2013, 88, 987–995. [Google Scholar] [CrossRef]
- Palmer, B.F.; Clegg, D.J. Physiology and pathophysiology of potassium homeostasis. Adv. Physiol. Educ. 2016, 40, 480–490. [Google Scholar] [CrossRef] [PubMed]
- de Baaij, J.H.F.; Hoenderop, J.G.J.; Bindels, R.J.M. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef]
- Rosanoff, A.; Weaver, C.M.; Rude, R.K. Suboptimal magnesium status in the United States: Are the health consequences underestimated? Nutr. Rev. 2012, 70, 153–164. [Google Scholar] [CrossRef]
- Del Gobbo, L.C.; Imamura, F.; Wu, J.H.Y.; et al. Circulating and dietary magnesium and risk of cardiovascular disease: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 160–173. [Google Scholar] [CrossRef]
- Touyz, R.M. Role of magnesium in the pathogenesis of hypertension. Mol. Aspects Med. 2003, 24, 107–136. [Google Scholar] [CrossRef] [PubMed]
- Sontia, B.; Touyz, R.M. Role of magnesium in hypertension. Arch. Biochem. Biophys. 2007, 458, 33–39. [Google Scholar] [CrossRef]
- Altura, B.M.; Altura, B.T. Role of magnesium in patho-physiological processes and the clinical utility of magnesium ion selective electrodes. Scand. J. Clin. Lab. Invest. 1996, 56, 211–234. [Google Scholar] [CrossRef]
- Maier, J.A.M. Low magnesium and atherosclerosis: An evidence-based link. Mol. Aspects Med. 2003, 24, 137–146. [Google Scholar] [CrossRef]
- Dibaba, D.T.; Xun, P.; He, K. Dietary magnesium intake is inversely associated with serum C-reactive protein levels: Meta-analysis and systematic review. Eur. J. Clin. Nutr. 2014, 68, 510–516. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Y.; Del Gobbo, L.C.; et al. Effects of magnesium supplementation on blood pressure: A meta-analysis of randomized controlled trials. Hypertension 2016, 68, 324–333. [Google Scholar] [CrossRef]
- Kass, L.; Weekes, J.; Carpenter, L. Effect of magnesium supplementation on blood pressure: A meta-analysis. Eur. J. Clin. Nutr. 2012, 66, 411–418. [Google Scholar] [CrossRef]
- Ranade, V.V.; Somberg, J.C. Bioavailability and pharmacokinetics of magnesium after administration of magnesium salts to humans. Am. J. Ther. 2001, 8, 345–357. [Google Scholar] [CrossRef] [PubMed]
- McCarron, D.A.; Morris, C.D.; Cole, C. Dietary calcium in human hypertension. Science 1982, 217, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Blaustein, M.P.; Lederer, W.J. Sodium/calcium exchange: Its physiological implications. Physiol. Rev. 1999, 79, 763–854. [Google Scholar] [CrossRef]
- Resnick, L.M. Calcium metabolism in hypertension and allied metabolic disorders. Diabetes Care 1991, 14, 505–520. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, J.R.; McCarron, D.A. Calcium metabolism and blood pressure. Journal of Clinical Endocrinology & Metabolism 1984, 59, 1129–1134. [Google Scholar] [CrossRef]
- van Mierlo, L.A.J.; Arends, L.R.; Streppel, M.T.; Zeegers, M.P.A.; Kok, F.J.; Grobbee, D.E. Blood pressure response to calcium supplementation: A meta-analysis of randomized controlled trials. J. Hum. Hypertens. 2006, 20, 571–580. [Google Scholar] [CrossRef]
- Bolland, M.J.; Grey, A.; Avenell, A.; Gamble, G.D.; Reid, I.R. Calcium supplements with or without vitamin D and risk of cardiovascular events. BMJ 2011, 342, d2040. [Google Scholar] [CrossRef]
- Dickinson, H.O.; Nicolson, D.J.; Cook, J.V.; et al. Calcium supplementation for the management of primary hypertension in adults. Cochrane Database Syst. Rev. 2006, CD004639. [Google Scholar] [CrossRef]
- Laurberg, P.; Cerqueira, C.; Ovesen, L.; et al. Iodine intake as a determinant of thyroid disorders in populations. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 13–27. [Google Scholar] [CrossRef]
- Danzi, S.; Klein, I. Thyroid hormone and the cardiovascular system. Med. Clin. N. Am. 2012, 96, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Biondi, B.; Cooper, D.S. The clinical significance of subclinical thyroid dysfunction. Endocr. Rev. 2008, 29, 76–131. [Google Scholar] [CrossRef]
- Napoli, R.; Guardasole, V.; Angelini, V.; et al. Acute effects of triiodothyronine on endothelial function in human subjects. J. Clin. Endocrinol. Metab. 2007, 92, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.N.; Albrecht, D.; Scholz, A.; et al. Global epidemiology of hyperthyroidism and hypothyroidism. Nat. Rev. Endocrinol. 2018, 14, 301–316. [Google Scholar] [CrossRef]
- Leung, A.M.; Braverman, L.E. Consequences of excess iodine. Nat. Rev. Endocrinol. 2014, 10, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Boelaert, K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol. 2015, 3, 286–295. [Google Scholar] [CrossRef]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef]
- Del Rio, D.; Rodriguez-Mateos, A.; Spencer, J.P.E.; Tognolini, M.; Borges, G.; Crozier, A. Dietary polyphenolics in human health: Structures, bioavailability, and evidence of protective effects. Antioxid. Redox Signal. 2013, 18, 1818–1892. [Google Scholar] [CrossRef]
- Schroeter, H.; Heiss, C.; Balzer, J.; et al. (–)-Epicatechin mediates beneficial effects of flavanol-rich cocoa on vascular function. Proc. Natl. Acad. Sci. USA 2006, 103, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- Heiss, C.; Kleinbongard, P.; Dejam, A.; et al. Acute consumption of flavanol-rich cocoa improves endothelial function. J. Am. Coll. Cardiol. 2005, 46, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Halliwell, B. Dietary polyphenols: Good, bad, or indifferent for your health? Cardiovasc. Res. 2007, 73, 341–347. [Google Scholar] [CrossRef]
- Förstermann, U.; Xia, N.; Li, H. Roles of vascular oxidative stress and nitric oxide in the pathogenesis of atherosclerosis. Circ. Res. 2017, 120, 713–735. [Google Scholar] [CrossRef]
- González-Gallego, J.; García-Mediavilla, M.V.; Sánchez-Campos, S.; Tuñón, M.J. Fruit polyphenols, immunity and inflammation. Br. J. Nutr. 2010, 104, S15–S27. [Google Scholar] [CrossRef] [PubMed]
- Actis-Goretta, L.; Ottaviani, J.I.; Fraga, C.G. Inhibition of angiotensin-converting enzyme activity by flavanol-rich foods. J. Agric. Food Chem. 2006, 54, 229–234. [Google Scholar] [CrossRef]
- Williamson, G.; Clifford, M.N. Role of the small intestine, colon and microbiota in determining the metabolic fate of polyphenols. Biochem. Pharmacol. 2017, 139, 24–39. [Google Scholar] [CrossRef]
- Katz, D.L.; Doughty, K.; Ali, A. Cocoa and chocolate in human health and disease. Antioxid. Redox Signal. 2011, 15, 2779–2811. [Google Scholar] [CrossRef]
- Fraga, C.G.; Oteiza, P.I. Dietary flavonoids: Role of (–)-epicatechin and related procyanidins in cardiovascular health. Free Radic. Biol. Med. 2011, 51, 813–823. [Google Scholar] [CrossRef]
- Heiss, C.; Dejam, A.; Kleinbongard, P.; et al. Vascular effects of cocoa rich in flavan-3-ols. JAMA 2003, 290, 1030–1031. [Google Scholar] [CrossRef]
- Grassi, D.; Desideri, G.; Necozione, S.; et al. Blood pressure is reduced and insulin sensitivity increased by dark chocolate. Hypertension 2005, 46, 398–405. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Alexopoulos, N.; et al. Effect of dark chocolate on arterial stiffness. Am. J. Hypertens. 2005, 18, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Ried, K.; Fakler, P.; Stocks, N.P. Effect of cocoa on blood pressure. BMC Med. 2009, 7, 22. [Google Scholar] [CrossRef]
- Hooper, L.; Kay, C.; Abdelhamid, A.; et al. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health. Am. J. Clin. Nutr. 2012, 95, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Ried, K.; Sullivan, T.; Fakler, P.; Frank, O.R.; Stocks, N.P. Does chocolate reduce blood pressure? BMC Med. 2010, 8, 39. [Google Scholar] [CrossRef] [PubMed]
- Cooper, K.A.; Donovan, J.L.; Waterhouse, A.L.; Williamson, G. Cocoa and health: A decade of research. Br. J. Nutr. 2008, 99, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, C.; Artacho, R.; Giménez, R. Beneficial effects of green tea: A review. J. Am. Coll. Nutr. 2006, 25, 79–99. [Google Scholar] [CrossRef]
- Deka, A.; Vita, J.A. Tea and cardiovascular disease. Pharmacol. Res. 2011, 64, 136–145. [Google Scholar] [CrossRef]
- Lorenz, M.; Urban, J.; Engelhardt, U.; Baumann, G.; Stangl, K.; Stangl, V. Green tea polyphenols and cardiovascular protection. Eur. Heart J. 2009, 30, 2024–2032. [Google Scholar] [CrossRef]
- Kim, W.; Jeong, M.H.; Cho, S.H.; et al. Effect of green tea catechins on endothelial function. Circ. J. 2006, 70, 153–159. [Google Scholar] [CrossRef]
- Hodgson, J.M.; Croft, K.D. Tea flavonoids and cardiovascular health. Mol. Aspects Med. 2010, 31, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Lu, F.; Wu, J.S.; Wu, C.H.; Chang, C.J. The protective effect of habitual tea consumption on hypertension. Arch. Intern. Med. 2004, 164, 1534–1540. [Google Scholar] [CrossRef]
- Liu, G.; Mi, X.; Zheng, X.; et al. Effects of tea intake on blood pressure: A meta-analysis. Br. J. Nutr. 2014, 112, 1043–1054. [Google Scholar] [CrossRef]
- He, J.; Giusti, M.M. Anthocyanins: Natural colorants with health-promoting properties. Annu. Rev. Food Sci. Technol. 2010, 1, 163–187. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.C. Anthocyanins in cardiovascular disease. Adv. Nutr. 2011, 2, 1–7. [Google Scholar] [CrossRef]
- Khan, F.; Ray, S.; Craigie, A.M.; et al. Lowering of blood pressure by berry-derived polyphenols. Am. J. Clin. Nutr. 2014, 100, 1385–1393. [Google Scholar] [CrossRef]
- Rodriguez-Mateos, A.; Del Pino-García, R.; George, T.W.; et al. Impact of anthocyanins on vascular function. Am. J. Clin. Nutr. 2014, 99, 1280–1290. [Google Scholar] [CrossRef]
- Curtis, P.J.; van der Velpen, V.; Berends, L.; et al. Blueberry anthocyanins improve vascular function. Am. J. Clin. Nutr. 2019, 109, 1535–1545. [Google Scholar] [CrossRef]
- Huang, H.; Chen, G.; Liao, D.; Zhu, Y.; Xue, X. Effects of anthocyanin supplementation on blood pressure: A meta-analysis. Nutrients 2016, 8, 198. [Google Scholar] [CrossRef]
- Calder, P.C. Omega-3 fatty acids and cardiovascular disease: Evidence explained and mechanisms explored. Clin. Sci. 2004, 107, 1–11. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Wu, J.H.Y. Omega-3 fatty acids and cardiovascular disease: Effects on risk factors, molecular pathways, and clinical events. J. Am. Coll. Cardiol. 2011, 58, 2047–2067. [Google Scholar] [CrossRef]
- Harris, W.S.; Miller, M.; Tighe, A.P.; Davidson, M.H.; Schaefer, E.J. Omega-3 fatty acids and coronary heart disease risk. J. Cardiovasc. Risk 2008, 15, 4–11. [Google Scholar] [CrossRef]
- Dangardt, F.; Chen, Y.; Gronowitz, E.; Dahlgren, J.; Friberg, P.; Strandvik, B. High physiological omega-3 fatty acid supplementation affects endothelial function. 78. Circulation 2010, 121, 252–258. [Google Scholar] [CrossRef]
- Harris, W.S.; Miller, M. Omega-3 fatty acids and cardiovascular disease: New developments and applications. Postgraduate Medicine 2012, 124, 100–113. [Google Scholar] [CrossRef]
- Serhan, C.N.; Chiang, N.; Van Dyke, T.E. Resolving inflammation: Dual anti-inflammatory and pro-resolution lipid mediators. Nat. Rev. Immunol. 2008, 8, 349–361. [Google Scholar] [CrossRef]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes. Nutrients 2010, 2, 355–374. [Google Scholar] [CrossRef] [PubMed]
- Yates, C.M.; Calder, P.C.; Ed Rainger, G. Pharmacology and therapeutics of omega-3 polyunsaturated fatty acids in chronic inflammatory disease. Pharmacol. Ther. 2014, 141, 272–282. [Google Scholar] [CrossRef]
- Nestel, P.J.; Shige, H.; Pomeroy, S.; et al. The n−3 fatty acids eicosapentaenoic acid and docosahexaenoic acid increase arterial compliance. Am. J. Clin. Nutr. 2002, 76, 326–330. [Google Scholar] [CrossRef]
- Mori, T.A.; Bao, D.Q.; Burke, V.; et al. Differential effects of omega-3 fatty acids on blood pressure. Hypertension 1999, 34, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Geleijnse, J.M.; Giltay, E.J.; Grobbee, D.E.; Donders, A.R.T.; Kok, F.J. Blood pressure response to fish oil supplementation. J. Hypertens. 2002, 20, 1493–1499. [Google Scholar] [CrossRef]
- Knapp, H.R.; FitzGerald, G.A. The antihypertensive effects of fish oil. N. Engl. J. Med. 1989, 320, 1037–1043. [Google Scholar] [CrossRef]
- Miller, P.E.; Van Elswyk, M.; Alexander, D.D. Long-chain omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid and blood pressure. Am. J. Hypertens. 2014, 27, 885–896. [Google Scholar] [CrossRef]
- Zhang, X.; Ritonja, J.A.; Zhou, N.; et al. Omega-3 fatty acids and blood pressure: A meta-analysis of randomized controlled trials. J. Am. Heart Assoc. 2022, 11, e025070. [Google Scholar] [CrossRef]
- Mori, T.A.; Woodman, R.J. The independent effects of EPA and DHA on cardiovascular risk factors. J. Nutr. 2006, 136, 300S–304S. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Lemaitre, R.N.; Kuller, L.H.; et al. Cardiac benefits of fish consumption. Circulation 2003, 107, 1372–1377. [Google Scholar] [CrossRef]
- Burdge, G.C.; Calder, P.C. Conversion of α-linolenic acid to longer-chain polyunsaturated fatty acids in humans. Reprod. Nutr. Dev. 2005, 45, 581–597. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M.; Harris, W.S.; Appel, L.J. Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Circulation 2002, 106, 2747–2757. [Google Scholar] [CrossRef]
- Skulas-Ray, A.C.; Wilson, P.W.F.; Harris, W.S.; et al. Omega-3 fatty acids for the management of hypertension. Circulation 2019, 140, e673–e691. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.C.; Hoffmann, C.; Mota, J.F. The human gut microbiota: Metabolism and perspective in obesity. Gut Microbes 2018, 9, 308–325. [Google Scholar] [CrossRef]
- Tilg, H.; Zmora, N.; Adolph, T.E.; Elinav, E. The intestinal microbiota fuelling metabolic inflammation. Nat. Rev. Immunol. 2020, 20, 40–54. [Google Scholar] [CrossRef] [PubMed]
- Ahtesh, F.B.; Stojanovska, L.; Apostolopoulos, V. Anti-hypertensive peptides derived from milk proteins. Nutrients 2018, 10, 1779. [Google Scholar] [CrossRef]
- Joyce, S.A.; Gahan, C.G.M. Bile acid modifications at the microbe–host interface. Gut Microbes 2016, 7, 381–392. [Google Scholar] [CrossRef]
- Khalesi, S.; Sun, J.; Buys, N.; Jayasinghe, R. Effect of probiotics on blood pressure: A systematic review and meta-analysis. Hypertension 2014, 64, 897–903. [Google Scholar] [CrossRef]
- Qi, D.; Nie, X.; Sun, J.; et al. Probiotics supplementation improves blood pressure: A meta-analysis. Lipids Health Dis. 2020, 19, 146. [Google Scholar] [CrossRef]
- Khalesi, S.; Bellissimo, N.; Vandelanotte, C.; Williams, S.; Stanley, D.; Irwin, C. A review of probiotic supplementation in blood pressure regulation. Nutrients 2019, 11, 2539. [Google Scholar] [CrossRef]
- O’Toole, P.W.; Marchesi, J.R.; Hill, C. Next-generation probiotics: From probiotics to live biotherapeutics. Nat. Microbiol. 2017, 2, 17057. [Google Scholar] [CrossRef]
- Didari, T.; Solki, S.; Mozaffari, S.; Nikfar, S.; Abdollahi, M. A systematic review of the safety of probiotics. Expert Opin. Drug Saf. 2014, 13, 227–239. [Google Scholar] [CrossRef]
- Zmora, N.; Suez, J.; Elinav, E. Diet, health, and the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 35–56. [Google Scholar] [CrossRef]
- Tiano, L.; Belardinelli, R.; Carnevali, P.; et al. Effect of coenzyme Q10 administration on endothelial function and inflammatory markers. Mol. Aspects Med. 2007, 28, 168–176. [Google Scholar] [CrossRef]
- Böger, R.H. The pharmacodynamics of L-arginine. J. Nutr. 2007, 137, 1650S–1655S. [Google Scholar] [CrossRef] [PubMed]
- Crane, F.L. Biochemical functions of coenzyme Q10. J. Am. Coll. Nutr. 2001, 20, 591–598. [Google Scholar] [CrossRef]
- Langsjoen, P.H.; Langsjoen, A.M. The clinical use of HMG-CoA reductase inhibitors and the associated depletion of coenzyme Q10. J. Am. Coll. Cardiol. 2003, 41, 122–124. [Google Scholar] [CrossRef]
- Ernster, L.; Dallner, G. Biochemical, physiological and medical aspects of ubiquinone function. Biochim. Biophys. Acta 1995, 1271, 195–204. [Google Scholar] [CrossRef]
- Littarru, G.P.; Tiano, L. Bioenergetic and antioxidant properties of coenzyme Q10. Mol. Aspects Med. 2007, 28, 137–148. [Google Scholar] [CrossRef]
- Zhao, D.; et al. Dose-response effect of Coenzyme Q10 supplementation on blood pressure in patients with cardiometabolic diseases: A meta-analysis. Nutrition, Metabolism & Cardiovascular Diseases. This study reported modest but significant reductions in systolic BP with higher circulating CoQ10 following supplementation 2022.
- Hodgson, J.M.; et al. Coenzyme Q10 improves blood pressure and endothelial function. Am. J. Hypertens. 2002, 15, 686–690. [Google Scholar] [CrossRef]
- Singh, R.B.; et al. Effect of coenzyme Q10 on risk of atherosclerosis in patients with hypertension. Mol. Cell. Biochem. 1999, 196, 179–187. [Google Scholar] [CrossRef]
- Rosenfeldt, F.L.; et al. Coenzyme Q10 in the treatment of hypertension: A meta-analysis. J. Hum. Hypertens. 2007, 21, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.J.; Bellusci, M.; Wright, J.M. Blood pressure lowering efficacy of coenzyme Q10. Cochrane Database Syst. Rev. 2009, CD007435. [Google Scholar] [CrossRef]
- Hidaka, T.; et al. Safety assessment of coenzyme Q10. Biofactors 2008, 32, 199–208. [Google Scholar] [CrossRef]
- Bhagavan, H.N.; Chopra, R.K. Coenzyme Q10 pharmacokinetics. Free Radic. Res. 2006, 40, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Maraver, J.; et al. Coenzyme Q10 therapy. Mol. Syndromol. 2014, 5, 187–197. [Google Scholar] [CrossRef]
- Karimi, M.; Rahmani, J.; Varkaneh, H.K.; Clark, C.C.T.; Salehi-Sahlabadi, A.; Day, A.S.; Mirmiran, P.; Hekmatdoost, A. Effects of coenzyme Q10 supplementation on blood pressure: A systematic review and meta-analysis of randomized controlled trials. Int. J. Cardiol. Cardiovasc. Risk Prev. 2025, 24, 100301. [Google Scholar] [CrossRef]
- Gambardella, J.; et al. Arginine and endothelial function. Biomedicines 2020, 8, 277. [Google Scholar] [CrossRef]
- McRae, M.P. Therapeutic benefits of L-arginine: Umbrella review. J. Chiropr. Med. 2016, 15, 184–189. [Google Scholar] [CrossRef]
- Dong, J.Y.; et al. Effect of oral L-arginine on blood pressure. Am. Heart J. 2011, 162, 959–965. [Google Scholar] [CrossRef]
- Shiraseb, F.; et al. Dose–response meta-analysis of L-arginine and blood pressure. Adv. Nutr. 2022, 13, 1226–1242. [Google Scholar] [CrossRef] [PubMed]
- Grimble, G.K. Adverse gastrointestinal effects of arginine. J. Nutr. 2007, 137, 1693S–1701S. [Google Scholar] [CrossRef]
- Allerton, T.D.; et al. L-citrulline supplementation and cardiometabolic health. Nutrients 2018, 10, 921. [Google Scholar] [CrossRef]
- Vanhoutte, P.M.; Shimokawa, H.; Tang, E.H.C.; Feletou, M. Endothelial dysfunction and vascular disease. Acta Physiol. 2009, 196, 193–222. [Google Scholar] [CrossRef]
- Atlas, S.A. The renin–angiotensin aldosterone system: Pathophysiological role and pharmacologic inhibition. J. Manag. Care Pharm. 2007, 13, S9–S20. [Google Scholar] [CrossRef] [PubMed]
- Lüscher, T.F.; Barton, M. Biology of the endothelium. Clin. Cardiol. 1997, 20, II-3–II-10. [Google Scholar] [CrossRef]
- Förstermann, U.; Sessa, W.C. Nitric oxide synthases: Regulation and function. Eur. Heart J. 2012, 33, 829–837. [Google Scholar] [CrossRef]
- Higashi, Y.; Noma, K.; Yoshizumi, M.; Kihara, Y. Endothelial function and oxidative stress in cardiovascular diseases. Circ. J. 2009, 73, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Heiss, C.; Keen, C.L.; Kelm, M. Flavanols and cardiovascular health. J. Cardiovasc. Pharmacol. 2010, 56, 2–6. [Google Scholar] [CrossRef]
- Mori, T.A. Dietary omega-3 fatty acids, endothelial function, and cardiovascular risk. Lipids 2014, 49, 301–309. [Google Scholar] [CrossRef]
- Vanhoutte, P.M.; Shimokawa, H.; Feletou, M.; Tang, E.H.C. Endothelial dysfunction and vascular disease. Acta Physiol. 2017, 219, 22–35. [Google Scholar] [CrossRef]
- Tousoulis, D.; Kampoli, A.M.; Tentolouris, C.; Papageorgiou, N.; Stefanadis, C. The role of nitric oxide on endothelial function. Curr. Vasc. Pharmacol. 2012, 10, 4–18. [Google Scholar] [CrossRef]
- Zuchi, C. Nutraceuticals and endothelial function: clinical evidence and cardiovascular implications. Clin. Cardiol. 2010, 33, 375–384. [Google Scholar] [CrossRef]
- Gimbrone, M.A.; García-Cardeña, G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef]
- Carey, R.M.; Padia, S.H. Role of the renin–angiotensin–aldosterone system in hypertension. Circ. Res. 2008, 102, 127–137. [Google Scholar] [CrossRef]
- He, F.J.; MacGregor, G.A. Beneficial effects of potassium on human health. Physiol. Plant. 2008, 133, 725–735. [Google Scholar] [CrossRef]
- Touyz, R.M.; Campbell, N.; Logan, A.; Gledhill, N.; Petrella, R. The role of magnesium in hypertension. J. Clin. Hypertens. 2018, 20, 150–159. [Google Scholar] [CrossRef]
- Burnier, M.; Egan, B.M. Adherence in hypertension. Circ. Res. 2019, 124, 1124–1140. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M.; Petersen, K.S.; Hibbeln, J.R.; et al. Nutrition and behavioral health disorders: Depression and anxiety. Nutrients 2021, 13, 213. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; et al. 2017 ACC/AHA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef] [PubMed]
- Schiffrin, E.L. Vascular remodeling in hypertension: Mechanisms and treatment. Hypertension 2012, 59, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Montezano, A.C.; Touyz, R.M. Reactive oxygen species, vascular Noxs, and hypertension: Focus on translational and clinical research. Antioxid. Redox Signal. 2014, 20, 164–182. [Google Scholar] [CrossRef]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; et al. A clinical trial of the effects of dietary patterns on blood pressure. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Gimbrone, M.A.; García-Cardeña, G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef]
- Ordovás, J.M.; Ferguson, L.R.; Tai, E.S.; Mathers, J.C. Personalized nutrition and health. BMJ 2018, 361, k2173. [Google Scholar] [CrossRef]
- Zeevi, D.; Korem, T.; Zmora, N.; et al. Personalized nutrition by prediction of glycemic responses. Cell 2015, 163, 1079–1094. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Conceptual overview of mineral-related pathways potentially involved in blood pressure regulation.
Figure 1.
Conceptual overview of mineral-related pathways potentially involved in blood pressure regulation.
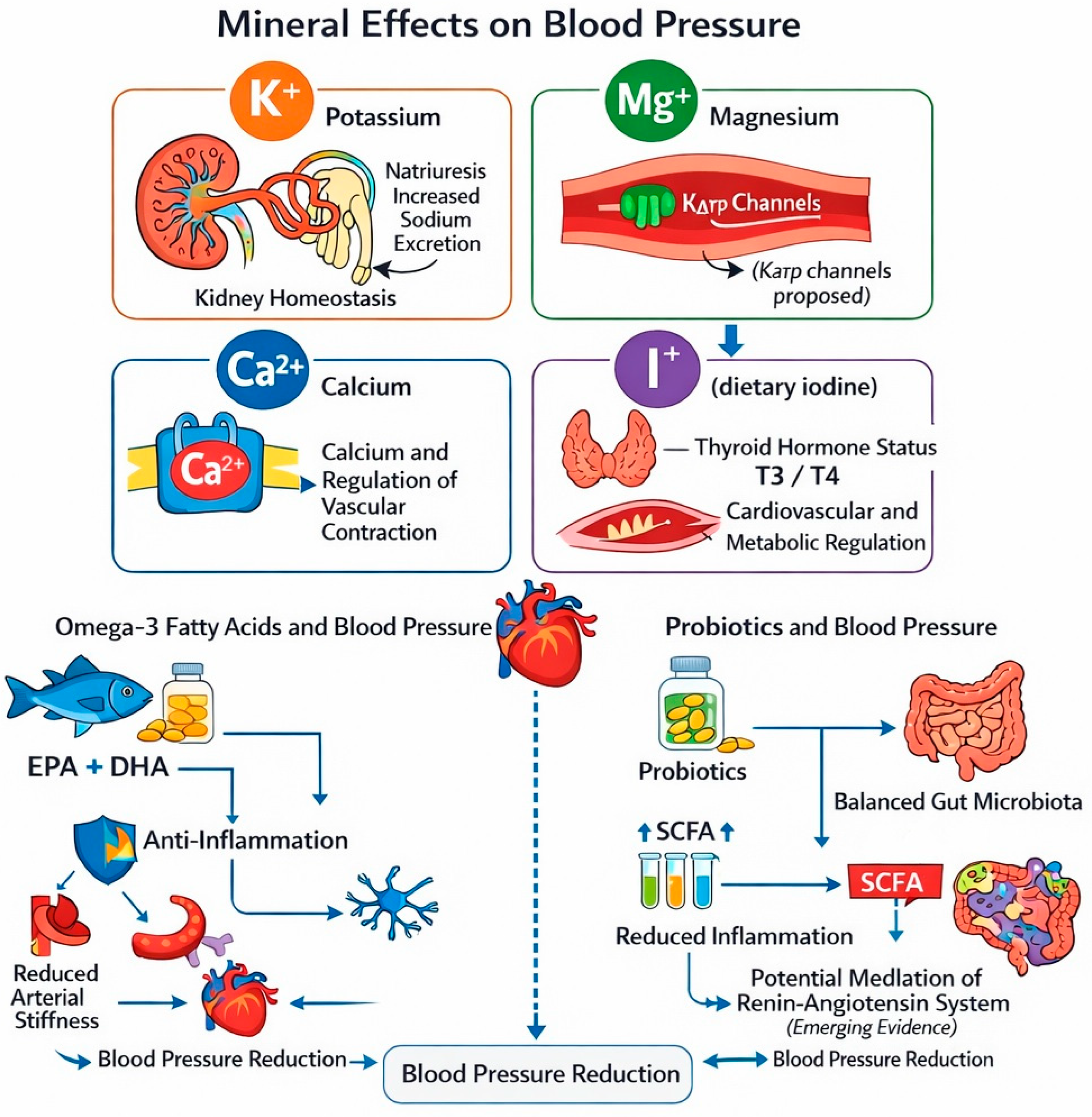
Figure 2.
Chemical structure of (-)-catechin (a flavan-3-ol polyphenol found in cocoa and tea). Source: Catechin.png, public domain, Wikimedia Commons.
Figure 2.
Chemical structure of (-)-catechin (a flavan-3-ol polyphenol found in cocoa and tea). Source: Catechin.png, public domain, Wikimedia Commons.

Table 1.
Nutraceuticals identified to have a potential positive impact on blood pressure control in human studies.
Table 1.
Nutraceuticals identified to have a potential positive impact on blood pressure control in human studies.
| Nutraceutical category | Key compounds / examples | Main mechanisms relevant to blood pressure | Evidence from human studies | Typical effect on blood pressure | Key clinical considerations |
| Essential minerals | Potassium | Increased natriuresis, reduced sodium retention, vascular smooth muscle hyperpolarization, partial RAAS suppression | Strong evidence (RCTs, meta-analyses) | ↓ SBP ~3–5 mmHg; ↓ DBP ~2–3 mmHg | Avoid supplementation in advanced CKD or with potassium-sparing diuretics |
| Magnesium | Calcium antagonism, improved endothelial function, reduced oxidative stress and inflammation | Moderate–strong evidence | ↓ SBP ~2–4 mmHg | Organic salts show better bioavailability; high doses may cause GI effects | |
| Calcium | Modulation of parathyroid hormone and RAAS activity | Moderate evidence (dietary intake strongest) | ↓ SBP ~2–3 mmHg | Prefer dietary sources; caution with high-dose supplements | |
| Iodine | Indirect effects via thyroid hormone regulation | Epidemiological evidence | Indirect / variable | Both deficiency and excess may adversely affect BP | |
| Polyphenols | Cocoa flavanols (epicatechin) | Increased eNOS activity, improved nitric oxide bioavailability, reduced arterial stiffness | Strong evidence | ↓ SBP ~3–5 mmHg | Effects depend on flavanol content; sugar-rich products not recommended |
| Tea polyphenols (catechins, theaflavins) | Improved endothelial function, reduced oxidative stress | Moderate evidence | ↓ SBP ~2–3 mmHg | Benefits accumulate with habitual intake | |
| Berry anthocyanins | Improved endothelial function, reduced inflammation and arterial stiffness | Moderate evidence | ↓ SBP ~2–4 mmHg | Whole berries preferred over isolated supplements | |
| Omega-3 fatty acids | EPA, DHA | Improved endothelial function, anti-inflammatory effects, reduced arterial stiffness, lower sympathetic activity | Strong evidence | ↓ SBP ~4–5 mmHg; ↓ DBP ~2–3 mmHg | DHA may be more potent; caution at high doses in bleeding risk |
| Probiotics | Lactobacillus, Bifidobacterium spp. | SCFA production, reduced inflammation, ACE inhibition, improved gut barrier integrity | Emerging–moderate evidence | ↓ SBP ~2–4 mmHg | Effects depend on strain, dose, and duration |
| Bioactive compounds | Coenzyme Q10 | Reduced oxidative stress, improved mitochondrial and endothelial function | Moderate evidence | ↓ SBP ~5–17 mmHg | Generally well tolerated; formulation affects bioavailability |
| L-Arginine | Substrate for nitric oxide synthesis, improved endothelium-dependent vasodilation | Moderate evidence | ↓ SBP ~4–5 mmHg | Limited long-term data; caution in severe cardiovascular disease |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



