
Submitted:
23 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Background: The physiologic effects of vasoactive medications on the venous circulation remain incompletely understood. Contemporary bedside management often emphasizes the arterial circulation, whereas Guytonian physiology emphasizes the venous circulation and mean circulatory in determining steady-state cardiac output. The primary aim of this study was to characterize the effect of vasoactive medications on mean circulatory filling pressure and venous resistance. Methods: Demographic data and vasoactive data were collected from the electronic health record and collated with high-fidelity physiologic monitoring data. Mean circulatory filling pressure and venous resistance were calculated using clinically validated equations and then were modeled using a random forest regression incorporating postoperative time and infusion doses of epinephrine, norepinephrine, milrinone, vasopressin, phenylephrine, calcium, sodium nitroprusside, and nicardipine. Similar models were constructed for indexed systemic vascular resistance, cardiac index, cerebral oxygen extraction, and renal oxygen extraction. Results: Data from a total of 57 unique patients comprising 9,654,239 data points were analyzed. The model explained 91% of the variance in mean circulatory filling pressure and 58% of the variance in venous resistance. Vasopressin and norepinephrine were the most influential for mean circulatory filling pressure and venous resistance. Conclusion: Vasoactive medications modulate venous tone and impact mean circulatory filling pressure and venous resistance. High-fidelity physiologic data allow for characterizing these effects and guide titration of vasoactive medications at the bedside.
Keywords:
vasoactive medications
Introduction
Clinical management in the pediatric cardiac intensive care unit is often directed toward maintaining arterial pressure and cardiac output. Although oximetric indices such as venous oxyhemoglobin saturation are inherently important physiologic parameters, they are non-specific markers of the adequacy of the circulation; they may effectively indicate inadequate oxygen delivery but are ineffective in distinguishing its cause. They inform that something should be done, but not what should be done [1,2,3,4,5,6].
Arthur Guyton’s model of circulatory physiology emphasized the critical importance of venous return in determining cardiac performance. In this framework, the mean circulatory filling pressure represents the equilibrium pressure throughout the vasculature when cardiac output ceases and reflects the degree of vascular filling relative to compliance. Venous resistance determines how effectively this stored potential energy drives flow back to the right atrium. Together, mean circulatory filling pressure and venous resistance define the operating point at which venous return intersects cardiac output [7,8,9,10].
The venous system consists of a compliant splanchnic reservoir and a peripheral venous compartment, arranged in parallel and series. The splanchnic circulation serves as a dynamically regulated capacitance reservoir that is recruited through venoconstriction or sequestered through venodilation. Blood can flow from the peripheral venous system, through the splanchnic system, and back to the peripheral system which reflects its series circulation. Blood can also be circulated within the splanchnic system, using its reservoir functionality, which reflects is parallel circulation. Despite its physiologic importance, the venous circulation receives limited clinical attention, especially in pediatric populations [11]. Quantitative data describing the effects of vasoactive medications on venous tone, mean circulatory filling pressure, and venous resistance are sparse, and no prior studies have described these relationships in the setting of pediatric heart transplant recipients.
The primary aim of this study was to characterize the effects of commonly used vasoactive medications on mean circulatory filling pressure and venous resistance following pediatric heart transplantation. Secondary aims were to assess their effects on systemic vascular resistance, cardiac index, renal oxygen extraction, and cerebral oxygen extraction.
Methods
Study Design
This retrospective study included pediatric patients younger than 18 years of age who underwent heart transplant at a single institution. Eligible patients had continuous arterial blood pressure monitoring via an arterial catheter and central venous pressure monitoring via central venous catheter. Patients receiving mechanical circulatory support were excluded.
This study was reviewed and approved by the local institutional review board and conducted in accordance with the Helsinki declaration.
Variables of Interest
High frequency physiologic data were collected from the Sickbay platform (Medical Informatics Corporation, Houston, TX) for the first 48 postoperative hours. Heart rate was obtained from telemetry; systolic, mean, and diastolic blood pressures were obtained from the arterial catheter; respiratory rate and arterial saturation from pulse oximetry, and central venous pressure from the central venous catheter. Data were recorded at 1-second intervals.
Vasoactive infusion doses were recorded as follows: epinephrine, norepinephrine, milrinone, sodium nitroprusside, and nicardipine in mcg/kg/min, calcium chloride infusion in mg/kg/hr, and vasopressin in milliunits/kg/min. Data for vasoactive infusions were extracted from the medicine administration record in Epic (Epic Systems Corporation, Verona, Wisconsin).
Oxygen consumption was estimated using the equation outlined by Seckeler: 242.1 + (9.7 x ln age) – (34 x ln weight) – (9.6 x single ventricle)- (11.2 x critical illness). This equation was chosen for its superior performance across age groups [12].
Cardiac index was calculated by Fick equation using the estimated oxygen consumption and renal near infrared spectroscopy value as the surrogate for the venous oxygen saturation.
Indexed systemic vascular resistance was calculated using the following equation: (mean arterial pressure – central venous pressure) x 80 / cardiac index.
Mean circulatory filling pressure was calculated using the following equation: (0.96 x central venous pressure) + (0.04 x mean arterial pressure) + (0.2 x cardiac output). Venous resistance was calculated using the following equation: (mean circulatory filling pressure – central venous pressure)/venous return [13].
Cerebral oxygen extraction was calculated using the following equation: (arterial oxygen saturation – cerebral near infrared spectroscopy) / arterial oxygen saturation. Renal oxygen extraction was calculated using the following equation: (arterial oxygen saturation – renal near infrared spectroscopy) / arterial oxygen saturation.
Prior to processing, all data were normalized to relative time, defined in seconds, with time 0 corresponding to admission to the cardiac intensive care unit following heart transplant. Missing data were imputed using the patient-specific median values.
Statistical Analyses
Machine learning methods were constructed for each independent variable: mean circulatory filling pressure, venous pressure, indexed systemic vascular resistance, cardiac index, renal oxygen extraction, and cerebral oxygen extraction. Independent predictors included relative time, patient identifier, age, weight, and vasoactive infusion doses. Separate random forest regression models were trained for each dependent variable. Each model consisted of 100 trees, a minimum leaf size of two, and bootstrap sampling. Data were split into training and testing subsets in an 80:20 ratio. Model performance was assessed by R2 and mean absolute error. Feature importance rankings and partial-dependence plots were generated to quantify and visualize predictor influence.
All statistical analyses were performed using Python (v3.12) on a local Jupyter environment using scikit-learn.
Results
Cohort Characteristics
Fifty-seven patients were included. Ten were under 1 year of age, 11 were between 1 and 5 years of age, 5 were between 6 and 10 years of age, and 20 were over 10 years of age. Median body surface area was 1.23 m2 (interquartile range [IQR] 0.57 to 1.86). Median waitlist time was 3.0 months (IQR 1.0-7.0). Median ischemic time was 252 minutes (IQR 228-279). Median donor age was 15 years (IQR 3-20) and the median donor-to-recipient weight ratio was 1.2 (IQR 1.0 to 1.4).
Mean Circulatory Filling Pressure
The model explained 57% of the variance in mean circulatory filling pressure (R² = 0.57; mean absolute error, 6.61). Feature importance from greatest to least was time, epinephrine, nicardipine, milrinone, vasopressin, calcium chloride, norepinephrine, and nitroprusside (Table 1). Mean circulatory filling pressure decreased with time, nitroprusside, and nicardipine and increased with epinephrine, norepinephrine, and vasopressin (Table 2).
Venous Resistance
The venous resistance model explained 59% of the variance (R2 =0.59; mean absolute error was 5.26). Feature importance ranked time, nicardipine, epinephrine, calcium chloride, milrinone, vasopressin, nitroprusside, and norepinephrine (Table 1). Venous resistance decreased with milrinone, nicardipine, nitroprusside, and calcium chloride and increased with time and epinephrine, norepinephrine, and vasopressin (Table 2).
Indexed Systemic Vascular Resistance
The model explained 90% of the variance in systemic vascular resistance (R2 =0.90; mean absolute error 15.8). Systemic vascular resistance decreased with time, epinephrine, milrinone, nicardipine, nitroprusside, and calcium chloride and increased with norepinephrine and vasopressin (Table 2).
Cardiac Index
The model for cardiac index explained 16% of the variance (R2 =0.16; mean absolute error 2.60). Cardiac index increased with time, epinephrine, milrinone, nitroprusside, and calcium chloride (Table 2).
Cerebral and Renal Oxygen Extraction
Models explained 90% (R2 =0.90; mean absolute error was 0.01) and 93% (R2 =0.93; mean absolute error 0.01) of the variance in cerebral and renal oxygen extraction, respectively. Both measures decreased with time, epinephrine, milrinone, nitroprusside, and nicardipine and increased with norepinephrine and vasopressin (Table 2).
In summary for each medication, epinephrine was a vasodilator (at the doses used) and venoconstrictor, norepinephrine was a vasoconstrictor and venoconstrictor, milrinone was a vasodilator and a venodilatory, calcium was essentially neutral on both sides of the circulation, nitroprusside was a vasodilator and venodilator, nicardipine was a vasodilator, and vasopressin was a vasoconstrictor and venodilator. Venous return, cardiac output curves for epinephrine, norepinephrine, milrinone, vasopressin, and calcium chloride are demonstrated in Figure 1, Figure 2, Figure 3, Figure 4 and Figure 5.
Discussion
High-fidelity physiologic data enable detailed characterization of both arterial and venous circulatory dynamics following pediatric heart transplantation. Approximately 60% of the variance in mean circulatory filing pressure and venous resistance was explained by postoperative time and vasoactive infusions, while systemic vascular resistance and regional oxygen extraction were explained by the model to a much greater extent. In contrast, cardiac index was only weakly predicted by these variables, suggesting that vasoactive infusions primarily modulate vascular tone rather than directly augmenting cardiac output.
Epinephrine was associated with increased mean circulatory filling pressure, venous resistance, and cardiac index alongside decreased systemic vascular resistance, and oxygen extraction. These findings are consistent with venoconstriction and (associated with, if not causing) enhanced contractility. The decrease in systemic vascular resistance occurred from a dose of 0.025 to 0.075 mcg/kg/min after which systemic vascular resistance increased with increasing epinephrine infusion dose. The rise in mean circulatory filling pressure suggests recruitment of unstressed into stressed volume (i.e. increased preload), and the decrement in systemic vascular resistance likely reflects b2 mediated arterial dilation [14,15,16,17]. The decrease in oxygen extraction suggests enhanced oxygen delivery despite higher venous tone [18]. These findings refine the typical mental model of post-transplant recipients in which arteriolar vasodilation is thought to be paramount to enhanced post-transplant cardiac output, by emphasizing the critical contribution of venous recruitment and preload augmentation. Norepinephrine increased mean circulatory filling pressure, venous resistance, and systemic vascular resistance without a corresponding increase in cardiac index, consistent with concurrent preload and afterload augmentation. Some of this has been demonstrated before [17,19]. The associated rise in oxygen extraction suggests reduced adequacy of oxygen delivery in a high-resistance state.
Milrinone demonstrated venodilation and arterial vasodilation with preserved cardiac index and reduced oxygen extraction, likely reflecting improved ventricular compliance and redistribution of venous blood [20,21,22]. Nitroprusside produced balanced arterial and venous dilation, whereas nicardipine primarily affected arterial tone [23,24,25,26,27]. Calcium chloride appeared largely neutral with modest improvements in cardiac index and oxygen delivery [28].
With high-fidelity physiologic data, there are some special nuances that must be considered. First, the sample size in such a study ,is the number of data points, not the number of patients, that powers the statistical analyses. Second, “conventional” statistics cannot be practically used for such analyses. While readers may be unfamiliar with the statistical analyses used herein, all are encouraged to use electronic and print resources to familiarize themselves with such methods. As such data becomes more available such analyses will become more prevalent, particularly since there is ample compute for such methods in the current era. Machine learning methods such as random forest have already been increasingly employed and are particularly helpful when the dataframe is large as is the case with the current study in which there were over 9 million datapoints worth of data. Such physiologic studies can also be prone to mathematical coupling. This phenomenon occurs when the dependent variable is a calculated variable and the components of it are included as independent variables in the model used to predict it. As the calculated physiologic variables were only used as the dependent variables and not entered as the independent variables in the current study the risk of mathematical coupling was greatly reduced. The fact that for the same vasoactives there were divergent effects on mean arterial pressure, systemic vascular resistance, and mean circulating filling pressure demonstrate the absence of significant mathematical coupling.
While the current study offers novel insight into the effects of vasoactive medications on the venous and arterial circulations after pediatric heart transplant using high fidelity physiologic data, it is not without its limitations. First, oxygen consumption relied on an equation that is imperfect. This formula was selected for its overall performance in children of all ages with and without congenital heart disease but that does not mean it is perfect. Even if the oxygen consumption estimates are not perfect, the hierarchy, direction, and relative strength of associations between variables should be preserved. Consequently, while the exact numerical scale of derived parameters such as cardiac index or systemic vascular resistance may differ depending on the chosen oxygen consumption equation, the overall physiologic relationships and model effects remain valid. Secondly, other variables such as fluid balance were purposely not included in the model. The aim of the study was to focus on vasoactive effect. For the dependent variables except cardiac index, the model performance was quite good. Adding additional independent variables could have helped increase the variability that could be accounted for in cardiac index, but it would not alter the direction of effect of the vasoactive medications which was the aim of the study. Additionally, the dataframe was already quite large and adding additional variables could have significantly increased the required compute and time for model creation.
Conclusion
After pediatric heart transplant, vasoactive medications primarily influence vascular tone rather than directly augmenting cardiac output. By shifting mean circulatory pressure and venous resistance, these agents modulate venous return, systemic vascular resistance, and oxygen extraction.
References
- Loomba, R.S. The Oximetric Approach to Clinical Care. Pediatr. Cardiol. 2023, 44, 960–961. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.S.; Flores, S. Oximetry Titrated Care: This Is the Way. Paediatr. Anaesth. 2022, 32, 485. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.S. Venous Saturation Guided Postoperative Care for Pediatric Cardiac Surgical Patients: The Body Wants Oxygen! Braz. J. Anesthesiol. Engl. Ed. 2025, 75, 844641. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.M.; Araujo, D.D.; Dantas, G.M.; Cunha, L.C.C.; Zeferino, S.P.; Galas, F.B. Goal-Directed Therapy with Continuous SvcO2 Monitoring in Pediatric Cardiac Surgery: The PediaSat Single-Center Randomized Trial. Braz. J. Anesthesiol. Engl. Ed. 2025, 844614. [Google Scholar] [CrossRef]
- Scott, J.P.; Hoffman, G.M. Near-Infrared Spectroscopy: Exposing the Dark (Venous) Side of the Circulation. Paediatr. Anaesth. 2014, 24, 74–88. [Google Scholar] [CrossRef]
- Tweddell, J.S.; Ghanayem, N.S.; Mussatto, K.A.; Mitchell, M.E.; Lamers, L.J.; Musa, N.L.; Berger, S.; Litwin, S.B.; Hoffman, G.M. Mixed Venous Oxygen Saturation Monitoring after Stage 1 Palliation for Hypoplastic Left Heart Syndrome. Ann. Thorac. Surg. 2007, 84, 1301–1310; discussion 1310-1311. [Google Scholar] [CrossRef]
- Guyton, A.C.; Lindsey, A.W.; Abernathy, B.; Richardson, T. Venous Return at Various Right Atrial Pressures and the Normal Venous Return Curve. Am. J. Physiol. 1957, 189, 609–615. [Google Scholar] [CrossRef]
- Guyton, A.C. Determination of Cardiac Output by Equating Venous Return Curves with Cardiac Response Curves. Physiol. Rev. 1955, 35, 123–129. [Google Scholar] [CrossRef]
- Guyton, A.C.; Polizo, D.; Armstrong, G.G. Mean Circulatory Filling Pressure Measured Immediately after Cessation of Heart Pumping. Am. J. Physiol. 1954, 179, 261–267. [Google Scholar] [CrossRef]
- Rothe, C.F. Mean Circulatory Filling Pressure: Its Meaning and Measurement. J. Appl. Physiol. 1993, 74, 499–509. [Google Scholar] [CrossRef]
- Greenway, C.V.; Lister, G.E. Capacitance Effects and Blood Reservoir Function in the Splanchnic Vascular Bed during Non-Hypotensive Haemorrhage and Blood Volume Expansion in Anaesthetized Cats. J. Physiol. 1974, 237, 279–294. [Google Scholar] [CrossRef] [PubMed]
- Seckeler, M.D.; Hirsch, R.; Beekman, R.H.; Goldstein, B.H. A New Predictive Equation for Oxygen Consumption in Children and Adults with Congenital and Acquired Heart Disease. Heart Br. Card. Soc. 2015, 101, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Parkin, W.G.; Leaning, M.S. Therapeutic Control of the Circulation. J. Clin. Monit. Comput. 2008, 22, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Stratton, J.R.; Pfeifer, M.A.; Ritchie, J.L.; Halter, J.B. Hemodynamic Effects of Epinephrine: Concentration-Effect Study in Humans. J. Appl. Physiol. Bethesda Md 1985, 58, 1199–1206. [Google Scholar] [CrossRef]
- Hiatt, W.R.; Wolfel, E.E.; Stoll, S.; Nies, A.S.; Zerbe, G.O.; Brammell, H.L.; Horwitz, L.D. Beta-2 Adrenergic Blockade Evaluated with Epinephrine after Placebo, Atenolol, and Nadolol. Clin. Pharmacol. Ther. 1985, 37, 2–6. [Google Scholar] [CrossRef]
- Jacobsohn, E.; Chorn, R.; O’Connor, M. The Role of the Vasculature in Regulating Venous Return and Cardiac Output: Historical and Graphical Approach. Can. J. Anaesth. J. Can. Anesth. 1997, 44, 849–867. [Google Scholar] [CrossRef]
- Rothe, C.F. Reflex Control of Veins and Vascular Capacitance. Physiol. Rev. 1983, 63, 1281–1342. [Google Scholar] [CrossRef]
- Loomba, R.S.; Villarreal, E.G.; Farias, J.S.; Flores, S.; Wong, J. Factors Associated with Renal Oxygen Extraction in Mechanically Ventilated Children after the Norwood Operation: Insights from High Fidelity Haemodynamic Data. Cardiol. Young 2024, 1–6. [Google Scholar] [CrossRef]
- Imai, Y.; Satoh, K.; Taira, N. Role of the Peripheral Vasculature in Changes in Venous Return Caused by Isoproterenol, Norepinephrine, and Methoxamine in Anesthetized Dogs. Circ. Res. 1978, 43, 553–561. [Google Scholar] [CrossRef]
- Hirakawa, S.; Ito, H.; Sahashi, T.; Takai, K.; Wada, H. Effects of Milrinone on Systemic Capacitance Vessels in Relation to Venous Return and Right Ventricular Pump Function. J. Cardiovasc. Pharmacol. 1992, 19, 96–101. [Google Scholar] [CrossRef]
- Colucci, W.S. Observations on the Intracoronary Administration of Milrinone and Dobutamine to Patients with Congestive Heart Failure. Am. J. Cardiol. 1989, 63, 17A–22A. [Google Scholar] [CrossRef]
- Remme, W.J.; van Hoogenhuyze, D.C.; Kruijssen, H.A.; Pieper, P.G.; Bruggeling, W.A. Preload-Dependent Hemodynamic Effects of Milrinone in Moderate Heart Failure. Cardiology 1992, 80, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, S.; Natsuyama, T.; Shigemi, K.; Chihara, E.; Kinoshita, T.; Tanaka, Y.; Miyazaki, M. Effect of Nicardipine Hydrochloride on Circulating Blood Volume and Vascular Compliance in Dogs. Jpn. Circ. J. 1990, 54, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Risöe, C.; Simonsen, S.; Rootwelt, K.; Sire, S.; Smiseth, O.A. Nitroprusside and Regional Vascular Capacitance in Patients with Severe Congestive Heart Failure. Circulation 1992, 85, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.R.; Vismara, L.A.; Zelis, R.; Amsterdam, E.A.; Mason, D.T. Clinical Use of Sodium Nitroprusside in Chronic Ischemic Heart Disease. Effects on Peripheral Vascular Resistance and Venous Tone and on Ventricular Volume, Pump and Mechanical Performance. Circulation 1975, 51, 328–336. [Google Scholar] [CrossRef]
- Wang, S.Y.; Scott-Douglas, N.W.; Manyari, D.E.; Tyberg, J.V. Arterial versus Venous Changes in Vascular Capacitance during Nitroprusside Infusion: A Vascular Modelling Study. Can. J. Physiol. Pharmacol. 1999, 77, 131–137. [Google Scholar] [CrossRef]
- Sohn, J.T.; Hoka, S.; Yamaura, K.; Takahashi, S. Effect of Nicardipine on Vascular Capacitance: Comparison with Sodium Nitroprusside during Induced Hypotension. J. Anesth. 1996, 10, 199–203. [Google Scholar] [CrossRef]
- Gallagher, J.D.; Geller, E.A.; Moore, R.A.; Botros, S.B.; Jose, A.B.; Clark, D.L. Hemodynamic Effects of Calcium Chloride in Adults with Regurgitant Valve Lesions. Anesth. Analg. 1984, 63, 723–728. [Google Scholar] [CrossRef]
Figure 1.
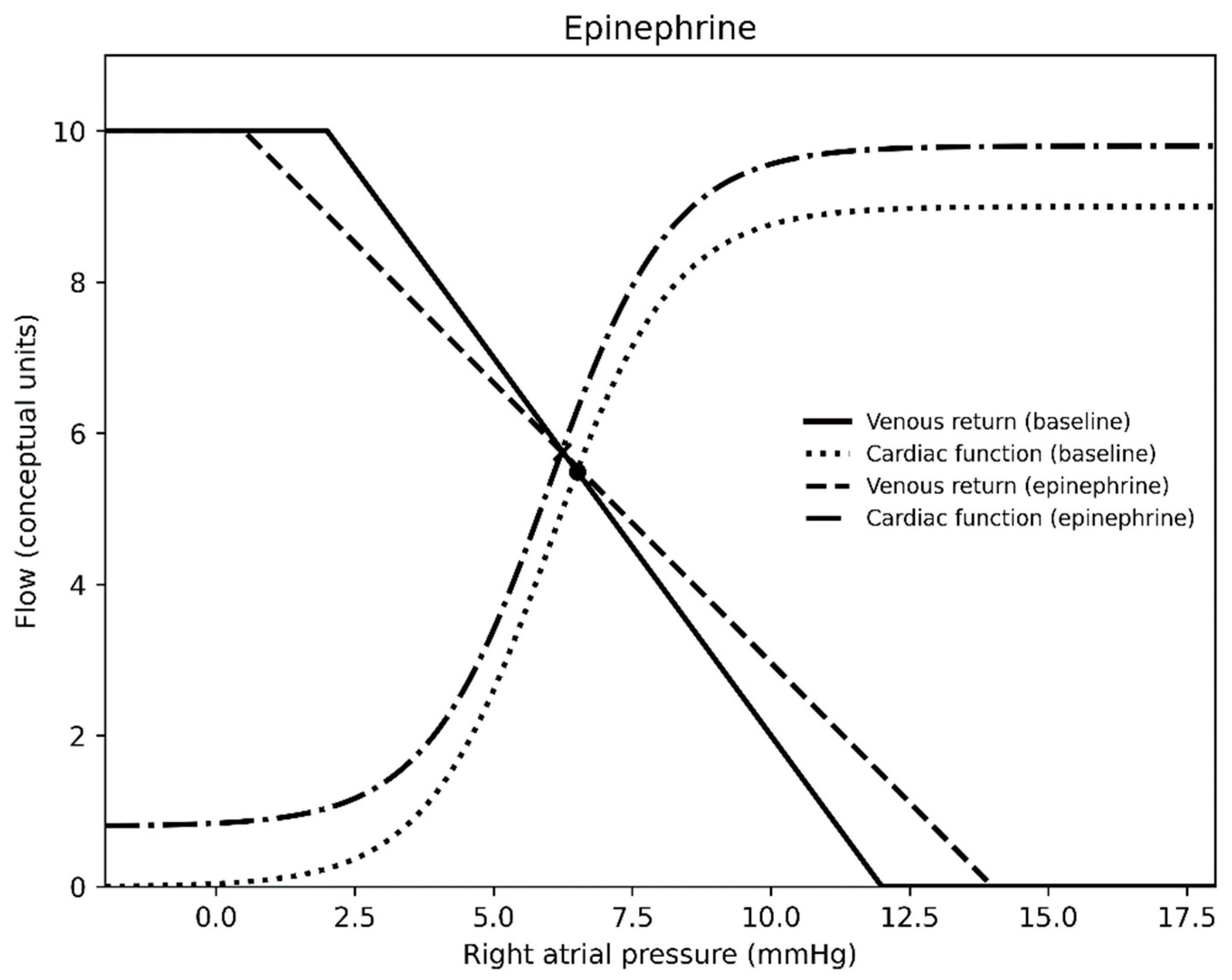
Figure 2.
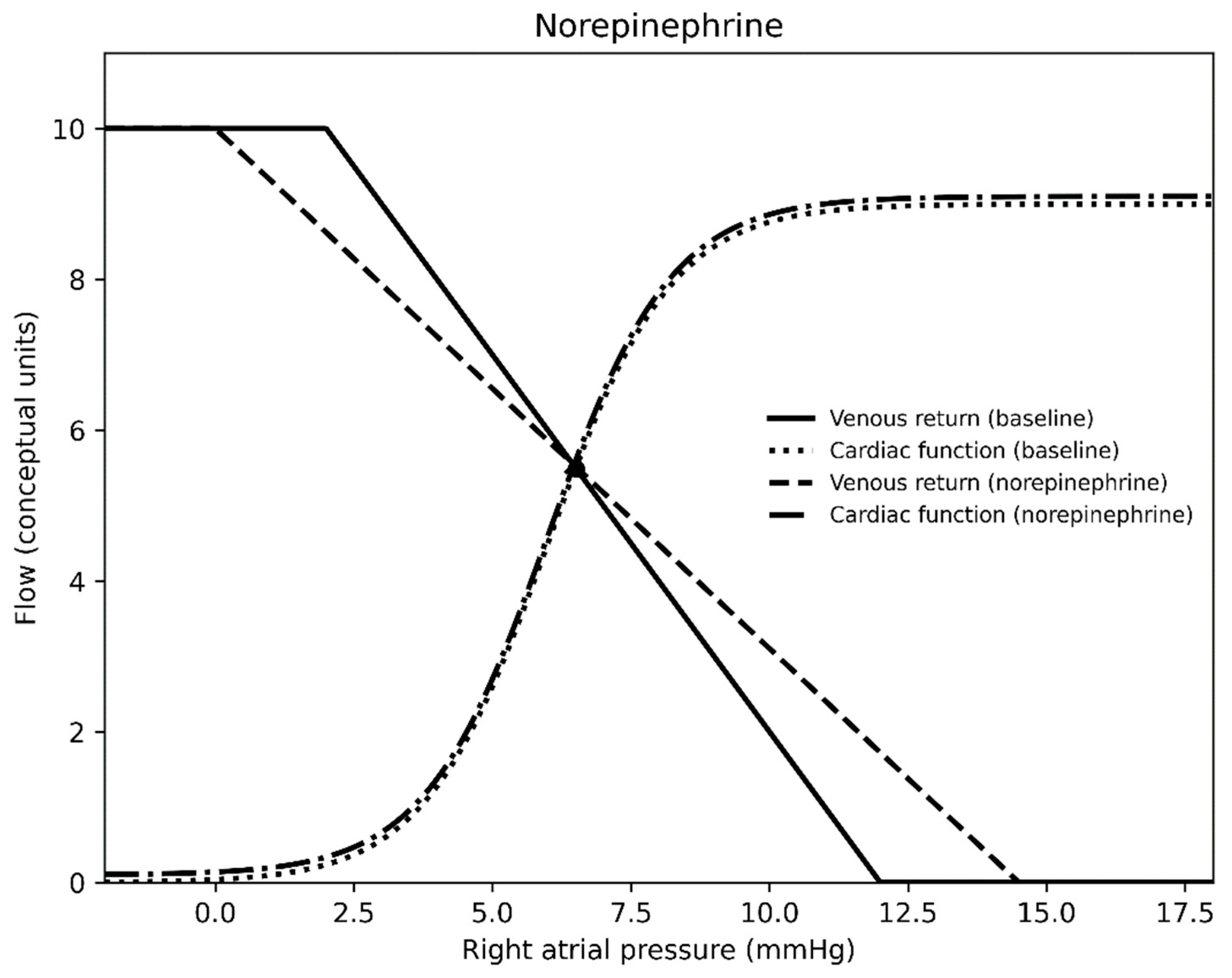
Figure 3.
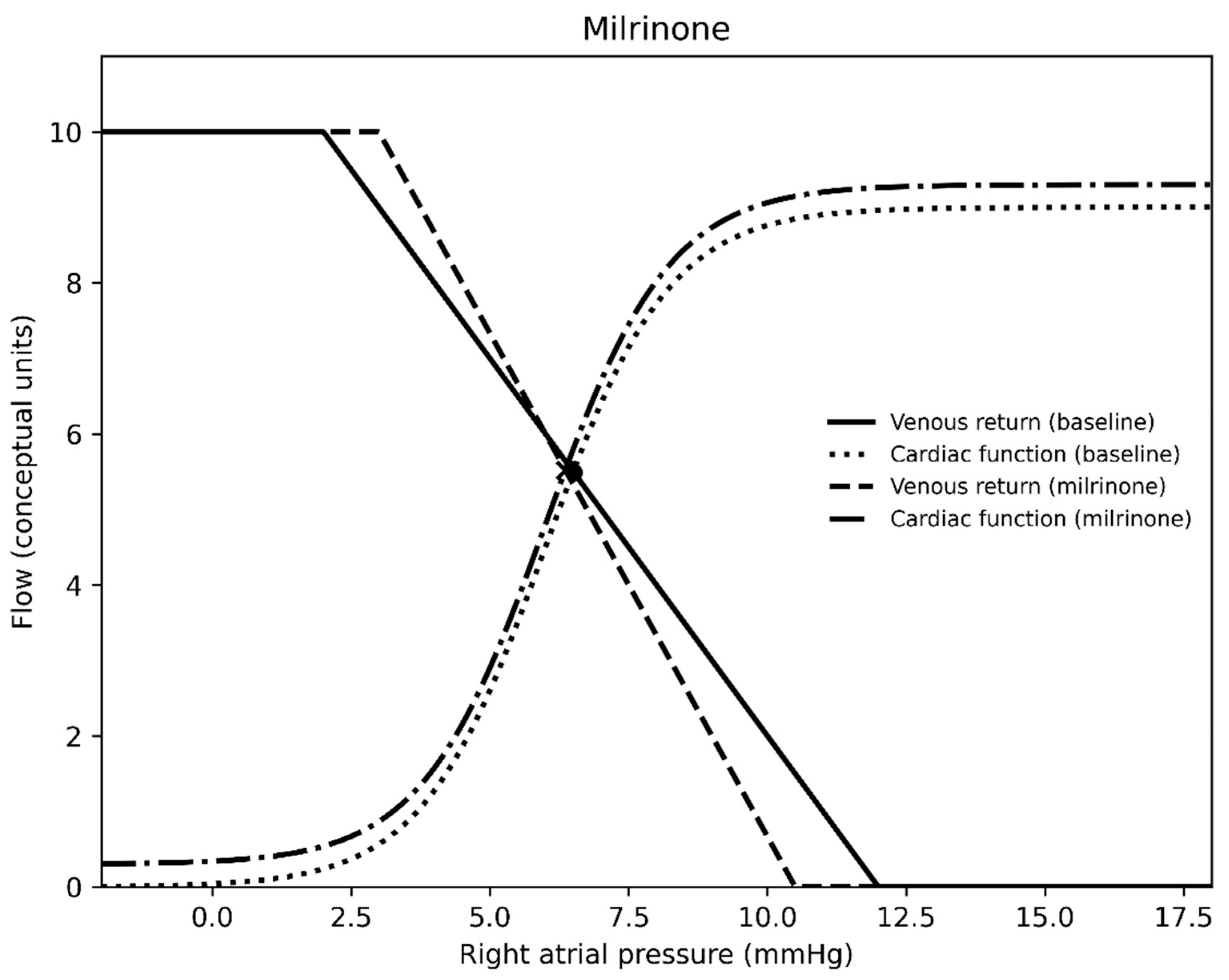
Figure 4.
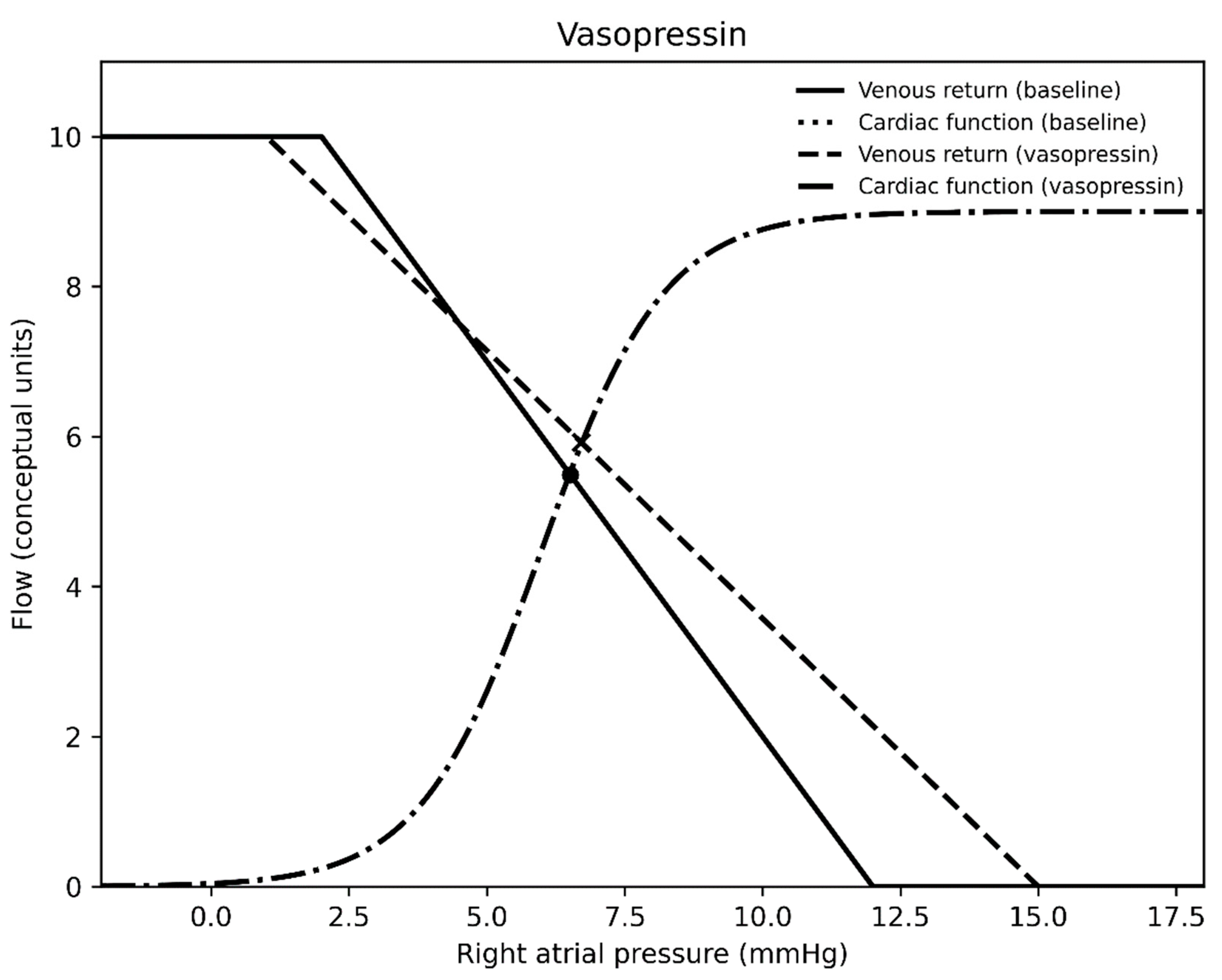
Figure 5.
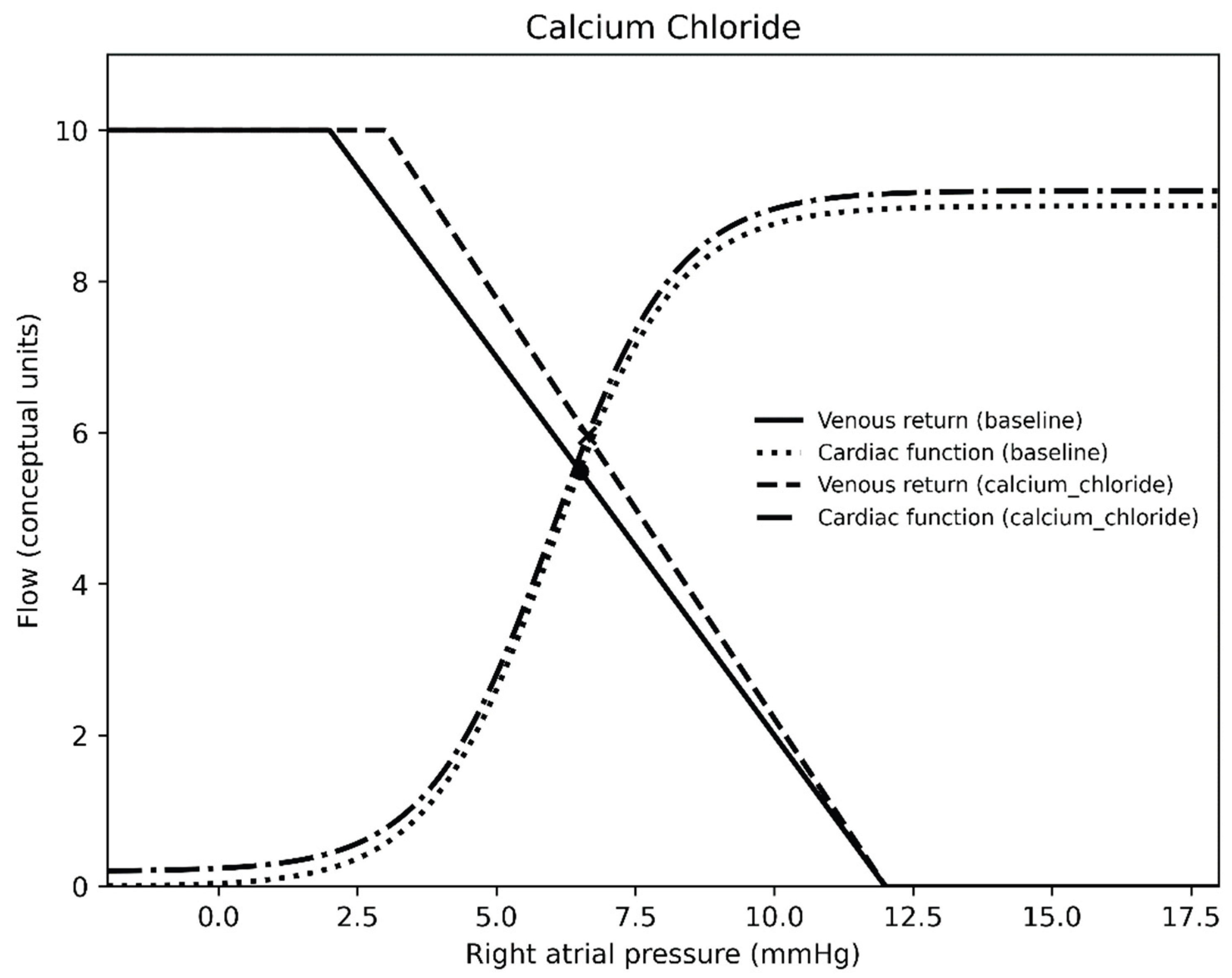

Table 1.
Feature importance from most important at top and least important at bottom for each dependent variable.
Table 1.
Feature importance from most important at top and least important at bottom for each dependent variable.
| Mean circulatory filling pressure | Venous resistance | Indexed systemic vascular resistance | Cardiac index | Cerebral oxygen extraction | Renal oxygen extraction |
|---|---|---|---|---|---|
| Time | Time | Time | Time | Time | Norepinephrine |
| Epinephrine | Nicardipine | Milrinone | Epinephrine | Milrinone | Time |
| Nicardipine | Epinephrine | Epinephrine | Nicardipine | Epinephrine | Epinephrine |
| Milrinone | Calcium chloride | Vasopressin | Milrinone | Nicardipine | Milrinone |
| Vasopressin | Milrinone | Nicardipine | Vasopressin | Vasopressin | Vasopressin |
| Calcium chloride | Vasopressin | Norepinephrine | Calcium chloride | Calcium chloride | Calcium chloride |
| Norepinephrine | Nitroprusside | Calcium Chloride | Nitroprusside | Norepinephrine | Nicardipine |
| Nitroprusside | Norepinephrine | Nitroprusside | Norepinephrine | Nitroprusside | Nitroprusside |
Table 2.
Overview of direction of effect of vasoactive medications on physiologic variables.
| Mean circulatory filling pressure | Venous resistance | Indexed systemic vascular resistance | Cardiac index | Cerebral oxygen extraction | Renal oxygen extraction | |
|---|---|---|---|---|---|---|
| Epinephrine | ↑ | ↑ | ↓ | ↑ | ↓ |
↓ |
| Norepinephrine | ↑ | ↑ | ↑ | ↑ | ↑ | |
| Milrinone | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ |
| Calcium chloride | ↓ | ↓ | ↑ | ↓ | ||
| Nitroprusside | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ |
| Nicardipine | ↓ | ↓ | ↓ | ↓ | ||
| Vasopressin | ↑ | ↑ | ↑ | ↑ | ↑ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



