
Submitted:
23 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Objectives: The general objective of the study was to analyze the influence of sociodemographic factors and care and hygiene practices on the appearance of Incontinence-Associated Dermatitis (IAD). The specific objectives sought to identify the relationship between sociodemographic variables (age, sex, comorbidities) and incidence of IAD, to evaluate hygiene protocols (cleaning products and absorbent handling), and to compare the time of onset of IAD according to the input used. Methods: A multicenter, prospective cohort study was conducted across 10 social health centers. The study population consisted of older institutionalized patients with urinary and/or mixed incontinence who used absorbents continuously. The variables included risk assessment using validated scales, such as the Braden Scale and the Perianal Assessment Tool (PAT), as well as ad hoc questionnaires. Survival analysis to assess the time-to-event onset was performed using the Kaplan-Meier curve and the Log-Rank test. Results: A statistically significant relationship was found between the occurrence of IAD and the risk detected by the Braden scale (p=0.004) and the PAT scale (p=0.02). However, no statistically significant relationship was found with age, sex, or the Barthel Index. Regarding hygiene, soapy wipes were associated with the highest incidence of IAD, while dry wipes were the most effective method, with the lowest cumulative risk and the longest time-to-event (p=0.001). The absorbent brand had a significant influence (p=0.024), suggesting that the "B" brand prevented one injury per six patients compared with the "A" brand. The frequency of absorbent changes did not show a statistically significant association. Conclusions: The risk of developing IAD is strongly linked to the scores of the Braden and PAT scales, the brand of the absorbent ("B" being more effective), and the hygiene method, where dry wipes were found to be the most protective against soapy ones. On the other hand, factors such as age, sex, degree of dependence (Barthel), or frequency of change of the absorbent did not show a significant influence on the appearance of the lesion.
Keywords:
incontinence-associated dermatitis
; non-irritating barrier films
; zinc oxide
; effectiveness
; prevention
; incontinence
; skin protection
; hygiene
; cleanliness
; absorbents
1. Introduction
Incontinence-Associated Dermatitis (IAD) is the most common subcategory of Moisture-Associated Skin Damage (MASD). MASD is defined as inflammation and/or erosion of the skin caused by prolonged or excessive exposure to moisture, such as urine and feces. These injuries represent a problem of great relevance in health care, as they affect people in a situation of dependency (permanent or transitory), seriously compromising their quality of life and comfort[1,2,3,4].
Etiologically, IAD is a complex and multifactorial condition. Constant exposure to body effluents causes overhydration and maceration of the stratum corneum, the outermost layer of the skin, making it more vulnerable to damage. The key pathophysiology centers on inflammation, altered skin pH, and physical deterioration of the skin. Specifically, the breakdown of urea into ammonia alkalizes the skin’s pH, disrupting the protective dermolipid barrier and facilitating the proliferation of pathogenic microorganisms. In addition, liquid stools are particularly irritating due to digestive enzymes (proteases and lipases) that, in an alkaline environment, break down essential lipids and proteins from the stratum corneum[2,5,6,7,8,9]. The epidemiology of IAD shows prevalence rates ranging from 4.3% to 42% and incidence rates ranging from 3.4% to 50%, depending on the population and environment studied.
Numerous sociodemographic and clinical factors act as adjuvants or predisposing factors, increasing an individual's risk of suffering from IAD. Advanced age is a crucial factor, given that aging skin is more fragile and has a compromised barrier function, and the incidence of IAD is higher in older people. Other risk factors include chronic health problems (such as diabetes), malnutrition or hypoproteinemia, fever, impaired consciousness, and immobility[2,5,6,8,9,10,11].
The prevention and treatment of IAD focus on a structured skincare program based on Hygiene, Hydration, and Protection [9]. Regarding care and hygiene practices, gentle, careful cleansing is recommended using products with a pH close to the skin's physiological pH (4.0-6.8), such as specific leave-on cleansers, since traditional alkaline soaps can damage the skin barrier. The handling of absorbents is also a determining factor, as the use of occlusive or inappropriate devices can prevent the drying of the skin, increasing sweating and raising the skin's pH, which increases the risk of damage[5,6,7,9,10,12,13,14,15,16,17,18,19,20,21].
The lack of high-quality evidence has resulted in the implementation of care that is often based on personal experience or opinion, rather than standardized, science-based protocols. It is crucial to conduct studies that standardize care, optimize care time, and improve the effectiveness of treatments by comparing the most commonly used supplies.
Therefore, the present study aims to address this need for evidence by analyzing the influence of sociodemographic factors and care practices on the occurrence of IAD, focusing on the protective effects of the inputs used.
2. Objectives
General Objective
- -
- To analyze the influence of sociodemographic factors and care and hygiene practices on the appearance of IAD.
Specific objectives:
- -
- To identify the relationship between sociodemographic variables (age, sex, comorbidities) and the incidence of IAD in the population studied.
- -
- To evaluate the relationship between hygiene protocols (type of cleaning products and handling of absorbents) and the incidence of IAD.
- -
- To compare the time of onset of IAD according to the type of input used, identifying in which group the event occurs earlier.
3. Methodology
3.1. Type of Study
This research is part of a larger research project in which a multicenter prospective cohort study was carried out across 10 social health centers in several primary care districts in the provinces of Jaen and Cadiz, focused on the medical device used as prevention (zinc oxide and non-irritating barrier films) for moisture injuries associated with incontinence. In a previous article, the profile of institutionalized people with incontinence (urinary and/or mixed) included in this research project was presented[11], and in the present study, its influence on the appearance of an IAD is shown.
3.2. Study Overview
- •
- Study population. Patients treated in nursing homes in the Jaen-South Jaen, North Jaen and Cadiz health districts, which care for dependent older adults, accredited by the Autonomous Community (ORDER of 5 November 2007 regulating the procedure and requirements for the accreditation of centers for older adults in a situation of dependency in Andalusia), with their own doctor and 24-hour nursing care and who have urinary and/or mixed incontinence.
- •
- Sample: Patients from the study population who met the inclusion/exclusion criteria agreed to participate in the study and who remained admitted from the date of the start of the study in the participating centers.
- •
- Sample selection method: A non-probabilistic sampling of an intentional or convenience type was carried out, selecting all participants in the primary project from the beginning of the study until the sample size was completed.
- •
- Inclusion criteria
- o
- Be over 18 years of age and have a life expectancy of more than 6 months from the start of the study.
- o
- Have urinary incontinence and/or mixed incontinence.
- o
- Use of absorbents on a continuous basis and as the only method for managing incontinence.
- o
- Previous absence of moisture injury.
- o
- Use regularly and only one of the products under study: zinc oxide ointment or non-irritant barrier film.
- •
- Exclusion criteria:
- o
- Patients with allergies to some of the study products.
- o
- Patients in a situation of terminal illness.
- o
- Presence of LPP, multifactorial lesions or combined lesions prior to the start of the study in the gluteal, sacral, genital or perigenital area.
- •
- Sample size calculation: For the sample calculation in the cohort study, the hypothesis was taken into account that people treated with NIBPs have better prevention outcomes in incontinence-associated dermatitis (IAD) than those treated with ZnO ointments. Patients were included according to the estimates made in the cohort study of the main project, which assumed an α error of 0.05, a statistical power of 80%, and considering that the IAD associated with patients with incontinence was 36%[22], establishing a sample size of 110 patients (55 per cohort). 95% confidence intervals were used.
3.3. Variables Analyzed
The following variables were analyzed: age, sex, associated comorbidities, pharmacological treatment, nutritional degree using a validated scale such as the Mini Nutritional Assessment (MNA), type of incontinence, existence of urinary tract infection or gastroenteritis at the time of the intervention, degree of personal autonomy (Barthel), type of absorbent used, number of daily changes of absorbent performed, Perineal Injury Measurement Scale (Perianal Assessment Tool, PAT), Risk Scale for Dependence-Related Injuries (Braden Scale), method of hygiene used, bad habits, type of skin protection used after hygiene and percentage of ZnO in the case of using ZnO ointment as a protection measure, presence and categorization of MASD and presence and degree of erythema.
3.4. Methods and Instruments in Data Collection
Data collection was carried out through an ad hoc questionnaire and validated scales for those variables that had this option: Barthel Index, Perianal Assessment Tool, Braden Scale, Visual Erythema Scale, and Categorization of MASD proposed by the National Group for the Study and Counseling of Pressure Ulcers (GNEAUPP).
3.5. Data Analysis
A global descriptive analysis was carried out. The qualitative variables were described using frequencies and percentages, and the quantitative variables were reported as means and standard deviations when normally distributed and as medians and interquartile ranges when not. To analyze survival or time-to-event, the Kaplan-Meier curve and the Log-Rank test were used.
3.6. Ethical Aspects
The study was approved by the Coordinating Committee on Biomedical Research Ethics of Andalusia (CCEIBA). The verbal and written consent of patients and/or relatives was requested, in accordance with the Declaration of Helsinki, and identification data were coded and treated confidentially, as provided in Organic Law 3/2018, of 5 December, on Data Protection and ARCO Rights (Access, Rectification, Cancellation and Opposition). This study is also funded by the FIBAO (Foundation for Biomedical Research of Eastern Andalusia. Alejandro Otero) under Project code AP-0312-2022.
4. Results
4.1. On Whether Sociodemographic Variables Influence the Appearance of an IAD
To determine these relationships, in addition to age and sex, three scales have been used: Barthel for dependence, PAT for the risk of injury due to humidity, and Braden for the risk of LPP, all of which have been related to the appearance of an IAD.
All quantitative variables (age, Barthel, PAT, and Braden) do not have a normal distribution (Kolmogorov-Smirnov test with Lilliefors correction), so non-parametric means were used. This test was completed with the normal distribution charts. Figure 1, Figure 2 and Figure 3, and 4 show the distribution graphs of the sociodemographic variable of age, degree of dependence (Barthel Index), risk of developing IAD (PAT), and risk of pressure injuries (Braden), respectively. As can be seen from the graph, the curve is asymmetrical, positive and plastic.
Table 1 and Table 2 present the frequencies and mean values of each variable analyzed, distinguishing between the IAD and non-IAD groups, and the statistical significance of each, after the association between the variables has been analyzed.
The association between the Braden scale and the PAT scale and the occurrence of IAD shows a statistically significant relationship. The mean scores obtained on the Braden scale in those patients who developed lesions were 13.62 with an average error deviation of 0.373, and for the PAT scale, it was a mean score of 5.34 points with a deviation of 0.163.
Thus, the greater the risk detected in the appearance of LPP (Braden Scale) and the greater the risk of developing a risk of skin lesion due to incontinence in the perineal area (PAT Scale), the greater the appearance of lesions and this is shown by the study.
However, the study does not indicate a relationship between the Barthel Index and the development of an IAD, and it cannot be established that the higher the degree of dependence, the greater the risk of developing an injury.
On the contrary, for the Barthel index, the mean score of patients who developed a lesion was 4 points lower than that of those who did not, but the high dispersion of the data with overlapping intervals indicates that this difference does not reach statistical significance.
Figure 1.
Distribution of the sociodemographic variable of age. Source: Authors.
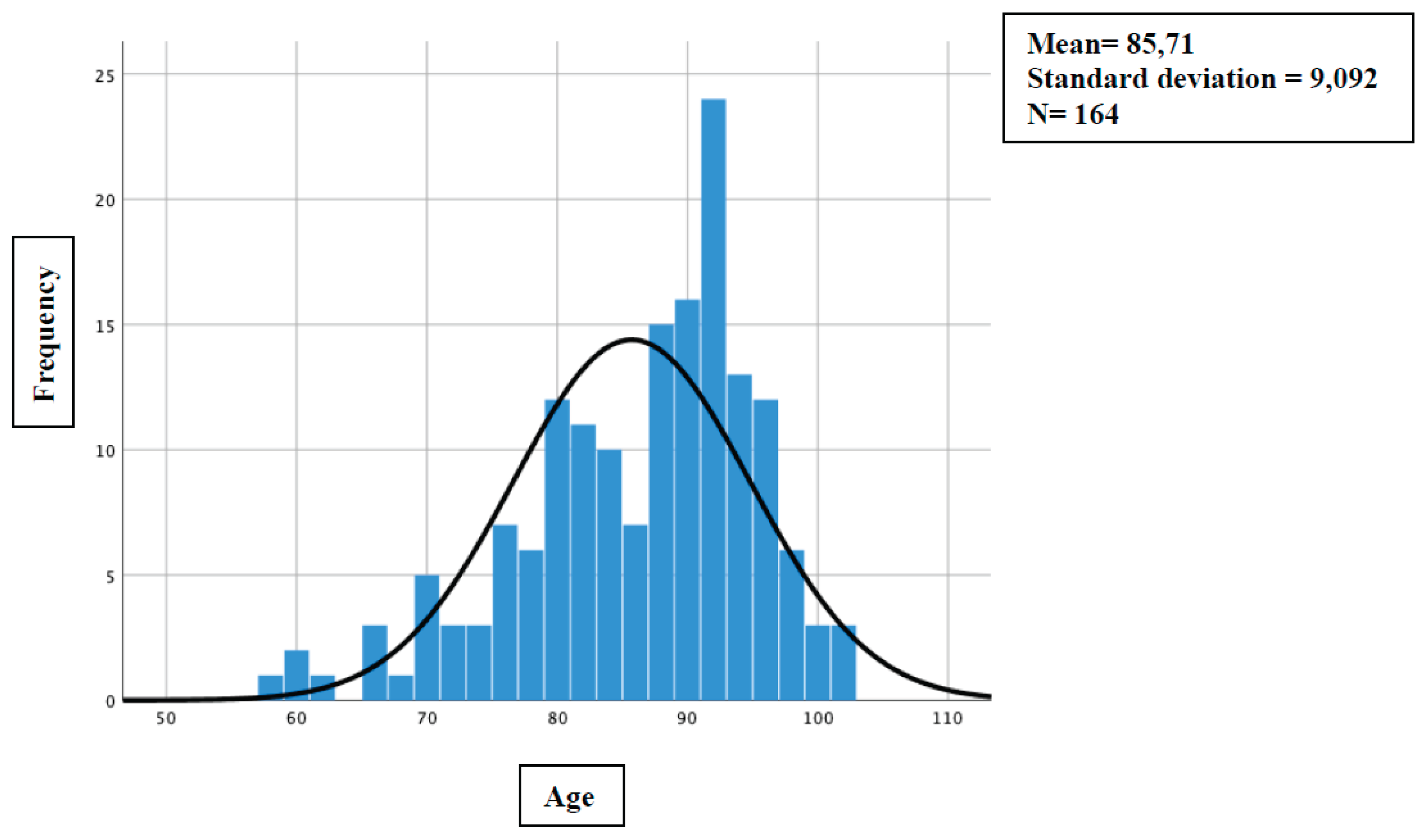
Figure 2.
Distribution of the sociodemographic variable of the degree of dependency (Barthel Index). Source: Authors.
Figure 2.
Distribution of the sociodemographic variable of the degree of dependency (Barthel Index). Source: Authors.
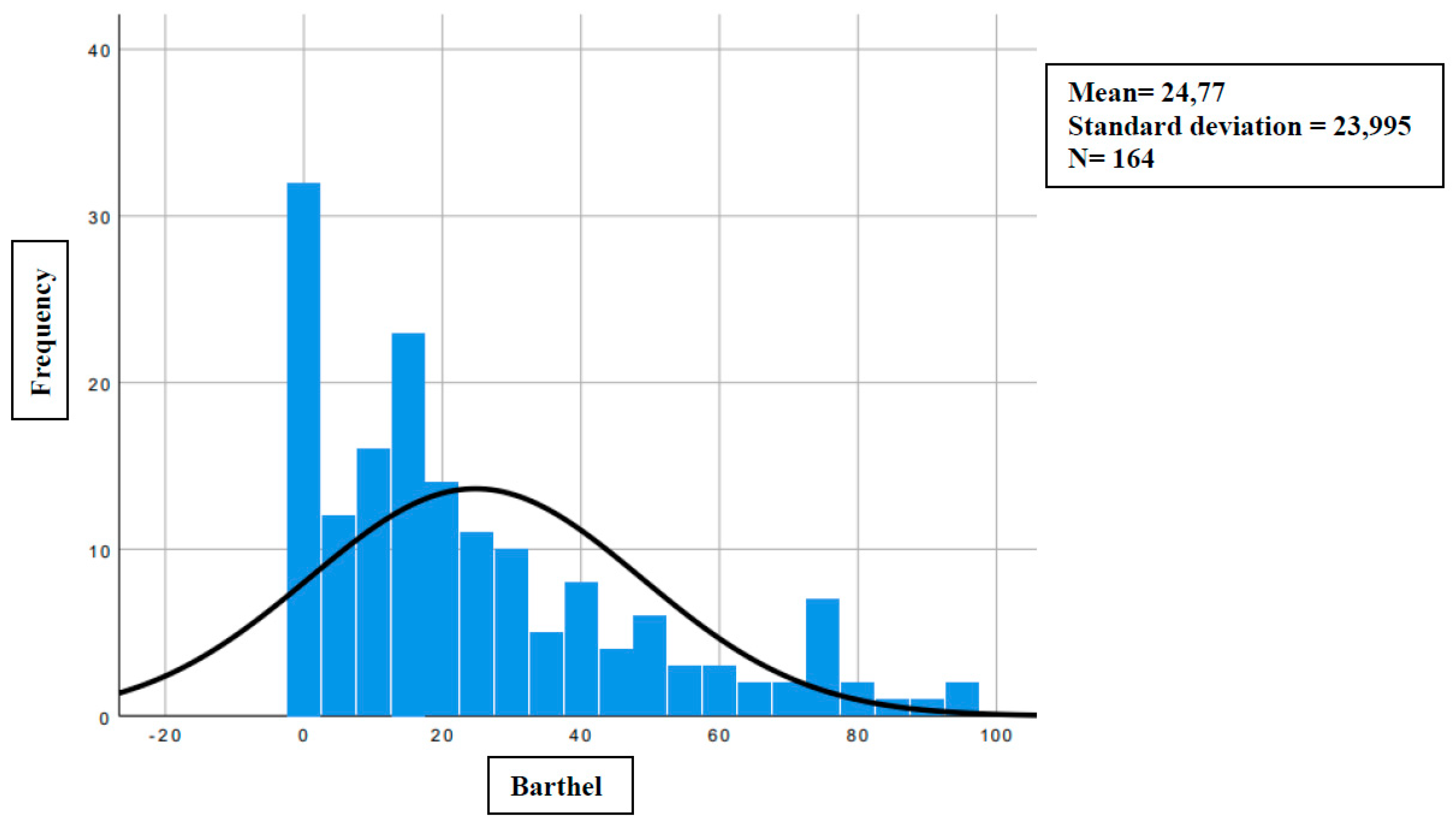
Figure 3.
Distribution of the sociodemographic variable of risk of developing IAD (PAT). Source: Authors.
Figure 3.
Distribution of the sociodemographic variable of risk of developing IAD (PAT). Source: Authors.
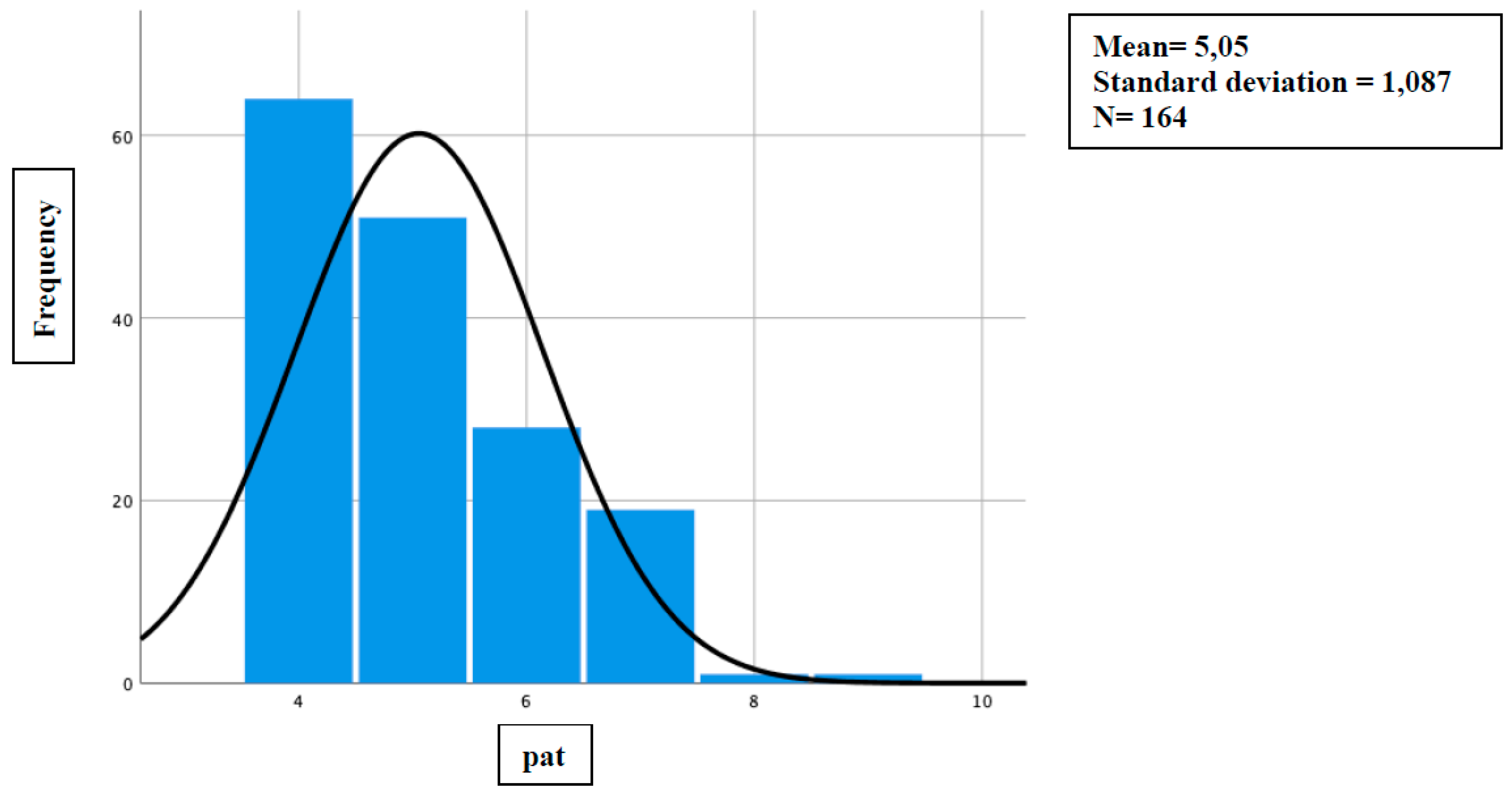
Figure 4.
Distribution of the sociodemographic variable of pressure injury risk (Braden). Source: Authors.
Figure 4.
Distribution of the sociodemographic variable of pressure injury risk (Braden). Source: Authors.
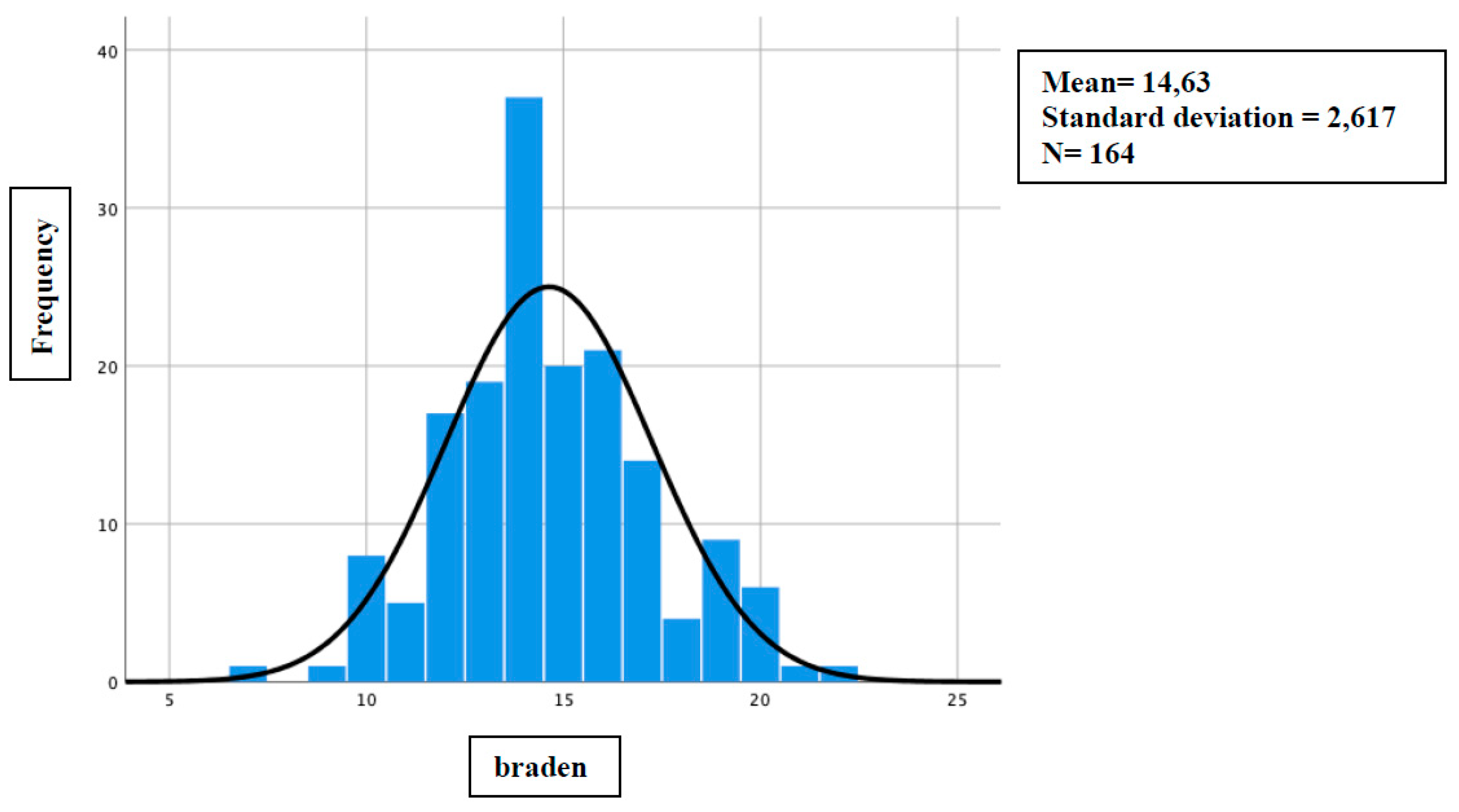

Table 1.
Frequency of qualitative sociodemographic variables (sex). Chi-square statistical test with Fisher's correction.
Table 1.
Frequency of qualitative sociodemographic variables (sex). Chi-square statistical test with Fisher's correction.
| Injury | Men | Women | P-Value | |
| No injury | 30 | 84 | 0.21(NS) | |
| With injury | 17 | 33 |
Source: Authors. (NS)= Not significant.
Table 2.
Mean values of sociodemographic variables. Mann-Whitney U test.
| Injury (No N=114) Yes (N=50) |
Average value | Average Range | U de Mann-Whitney | P-Value | |
| Age | No | 85.65(±)9,5 | 83.09 | 2783.0 | 0.81 (NS) |
| Yes | 85.86(±)8,1 | 81.19 | |||
| Braden | No | 15.08(±)2,5 | 89.47 | 2055.0 | 0.004* |
| Yes | 13.62(±)2,6 | 66.60 | |||
| Barthel | No | 26.10(±)24,8 | 85.01 | 2563.5 | 0.30 (NS) |
| Yes | 21.74(±)22,0 | 76.77 | |||
| PAT | No | 4.93(±)1,0 | 77.23 | 2249.5 | 0.02* |
| Yes | 5.34(±)1,2 | 94.51 |
Source: Authors. (NS)= Not significant; (*)= Statistical significance.
4.2. On Whether Cleaning and Moisture Control Products (Absorbents and Their Frequency of Changes) Influence the Appearance of an IAD
When assessing hygiene, the following cleaning options were analyzed: dry wipes, 3-in-1 wipes and soap (specific for cleaning the genital area), standard soap-and-water, and soapy wipes. The brands and models did differ from one social health center to another, so this bias could not be avoided (as it was an observational study), but it has been taken into account and measured independently.
Using the Chi-square test with statistically significant results (p=0.001), it was observed that soapy wipes have a statistically significant greater association with the appearance of an IAD, with a lesion having appeared in 57.6% of the patients where they used it, in other words, 1 in 1.7 patients develops a lesion when their hygiene has been with soapy wipes.
The second-highest hygiene method in terms of IAD incidence was dry wipes. They presented with a lesion in 1 out of 2 patients who used these (50% of the total sample who used this type of hygiene).
The standard soap-and-water hygiene accounted for 25% of IAD incidents. And the hygiene that turned out to be the most protective for the incidence of lesions were 3-in-1 wipes and soap, products designed not to need rinsing and specific for genital hygiene, with a representation of lesions out of the total of 16%, that is, only 1 person in 6 who used this cleaning method developed an IAD (Figure 5).
Regarding humidity control, this study considered only the continuous use of absorbents, without specifying a specific frequency of changes; however, this was taken into account and analyzed separately, as we will explain below.
As it was an observational study, it was not possible to interfere with the brand and model of the absorbents, but as all the residences were supplied with absorbents by agreement through the Andalusian Health Service, the brand supplied was the same without the possibility of any change, with the exception of a single social health center that used another brand in all its patients. but with a representative sample of the total to be able to analyze it independently, as explained above.
The absorbent brand: "A" was present in 35.2% of patients who developed an IAD, and the absorbent brand: "B" was present in 16.7% of IAD cases. Analyzing this data with the Chi-square test yielded a statistically significant association (p=0.024). This data corroborates when analyzed using Relative Risk, with a difference in risks between groups of 18.5% (95% CI 4.5% - 32.7%), or with the Newcombe test of differences in independent proportions, with 17.76% (CI 1.77-29.88), even more robust data. This leads us to the observation that, with a 95% CI of 4-23, for every 6 patients (NNT) who use the "B" brand, an injury is avoided among those who use the "A" brand.
Finally, with respect to the frequency of changing absorbents and the appearance of an IAD, the statistical association, as measured by Student's T, was not significant (p=0.6). However, patients with an injury showed a higher mean frequency of change (3.94) than those without an injury, with a mean number of changes in absorbents of 3.62.
When performing an analysis using the Kaplan-Meier curve to assess the cumulative survival in relation to the time to onset in days or rather "One minus survival", i.e., the cumulative probability of occurrence of an event (in this case the appearance of a lesion), with respect to the different hygiene methods, we obtain the following results (Figure 6):
Dry wipes have the lowest event accumulation, indicating that, in this group, it took longer to develop; thus, it seems associated with a lower cumulative event rate (IAD) or a delay in their onset.
3-in-1 wipes and soap show an accumulation of early events, suggesting that this option could be associated with a faster onset of the event. They show a greater accumulation of events in less time, suggesting that they may be associated with an earlier onset of the event, just like soap-and-water and soapy wipes.
Soap-and-water also show an early accumulation of events, similar to 3-in-1 soap and dry wipes. However, soap-and-water were associated with adverse events throughout follow-up, unlike the rest. We could say that, if the incontinence is due to an acute process that will last a short time, the hygiene method could be indistinct, but if a long period of time is foreseen or already in a chronic process, the hygiene method is very influential, with clear differences in the long term.
These differences were statistically significant, as determined by the log-rank test (p=0.001).
Similarly, in Figure 7, which corresponds to the Kaplan-Meier curve for cumulative survival, we observe that dry wipes are the method with the longest time to the onset of the event (IAD injury).
The dry wipes group (blue) clearly stands out. Cumulative survival remains constant at 0.5 (50%) over an extended period, up to approximately 42 units of time, at which point it drops to 0.0 by study completion. The remaining methods (3-in-1 soap and wipes, soap-and-water, and soapy wipes) show a much earlier and faster onset of the event.
In Figure 8, the direct counterpart of Figure 7, we see the Kaplan-Meier Curve analyzing its risk function.
This risk curve reinforces and complements the interpretation of the Kaplan-Meier survival curve. We observed that dry wipes clearly proved to be the most effective method, as it presented the lowest cumulative risk (zero) and the longest time of occurrence of the event, and the methods of three-in-one plus wipes, soap and water, and soapy wipes accumulated the highest risk in the study period, indicating a much earlier occurrence of the event. The superiority of dry wipes suggests that this method of hygiene best prevents or delays the onset of the event of interest in this study.
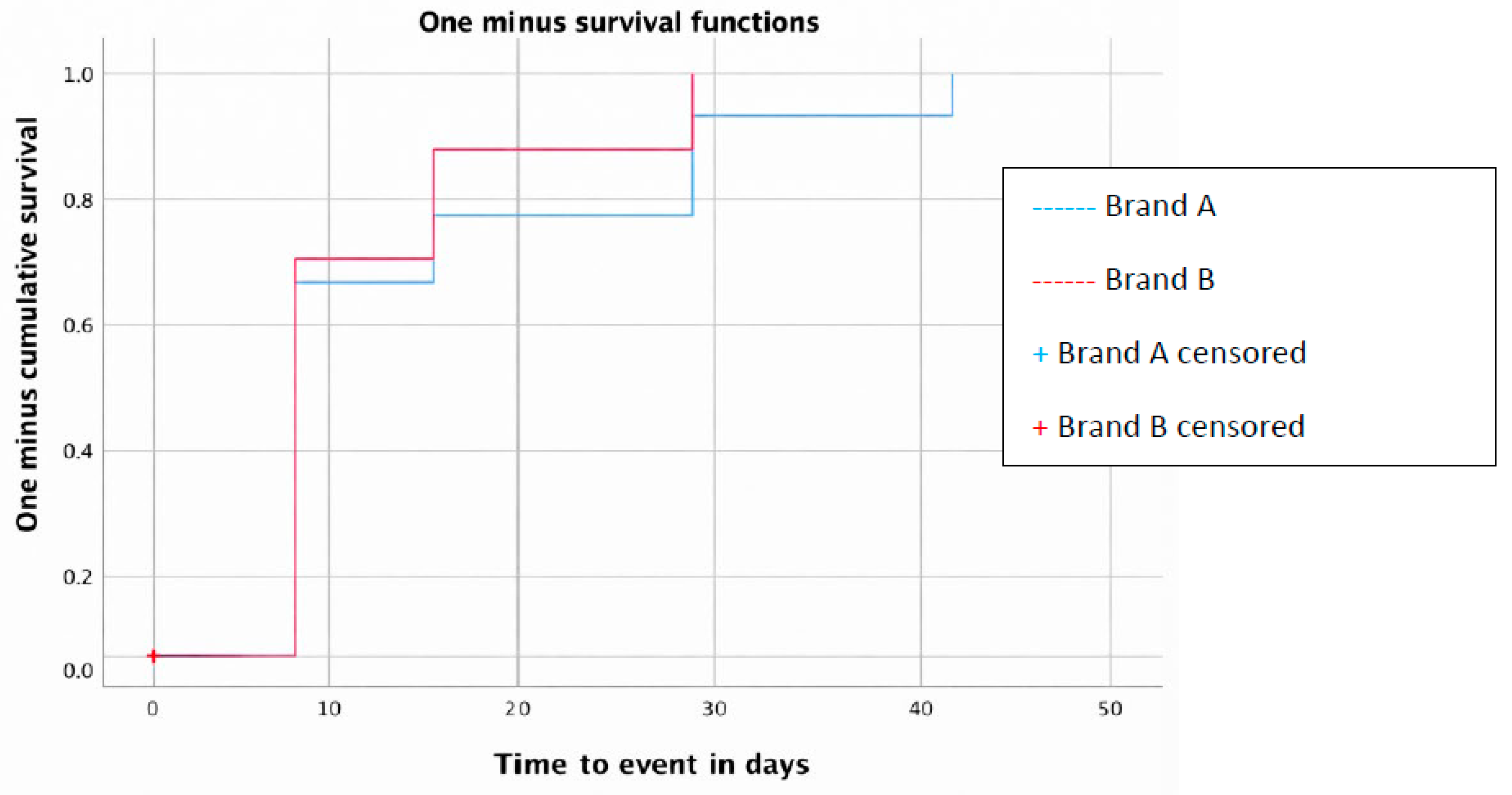
The absorbent brand was also analyzed using the Kaplan-Meier curve to assess the incidence over time (Figure 9).
The proportion of individuals who have experienced IAD onset and the time of onset are shown. The "B" brand has a slightly earlier accumulation of events (IAD) compared to the "A" brand, suggesting that the event occurs more quickly
Although the difference between the two groups does not seem very significant, when performing the log-rank test, we do obtain such a difference (p=0.022).
5. Discussion
5.1. Preventive Measures Used in Patients with Incontinence and Their Influence on the Appearance of an IAD
- - Hygiene method
Skin hygiene is a fundamental aspect of clinical nursing practice, with a substantial impact on the prevention and treatment of various skin conditions, especially MASD and IAD [23]. The effectiveness of the hygiene method in preventing moisture-related injuries can be assessed by comparing traditional practices with more modern, structured approaches. Our study determined that the IAD was influenced not only by the protective product but also by the previous hygiene method used. Traditional soap-and-water is associated with a 25% incidence of registered IADs, compared with 16% for wipes and specific soap for intimate hygiene without subsequent rinsing. The literature shows similar results as detailed below:
5.1.1. Traditional Hygiene Method: Classic Soap-and-Water
Traditionally, pH-neutral soap-and-water have been used for grooming and skin hygiene[24]. However, several studies and reviews suggest that skincare programs that use classic soap-and-water are less preferred or less effective in maintaining skin integrity and preventing IAD and xerosis cutis[23,25].
Frequent and repeated use of conventional soaps is considered an aggressive technique for skin exposed to moisture and for fragile skin [24]. This is because many common soaps are too alkaline (pH 9-10), which disrupts the skin's acid mantle or damages its structural proteins[21]. When the skin becomes more alkaline, its ability to inhibit bacterial growth is compromised[12]. Traditional soap, combined with towel drying, can disrupt the skin's barrier function. The soap-and-water formula often requires excessive rubbing or friction to remove urine and fecal residue, which can cause micro-damage and abrasion to vulnerable skin [21,26,27,28]. In cases where the skin is already vulnerable, soap-and-water may not be the best option, as the friction of washing can worsen the damage[30]. In addition, the surfactants present in soap can cause contact dermatitis, dehydrate the skin, and damage keratinocytes, since although they promote cleansing, they can remove the lipid content of the stratum corneum, which weakens the protective function of the skin[26,29].
Although cleaning with soap-and-water can be effective in reducing microorganisms in the groin and perineum area[30], current evidence suggests that it represents too aggressive a technique for vulnerable skin exposed to moisture[23,24,31].
From a cost perspective, while soap-and-water are economic resources, a no-rinse cleaner can be less expensive in terms of labor[24].
5.1.2. Other, More Current Hygiene Methods: Rinse-Free Cleansers and Wipes with Added Properties
In contrast to soap-and-water, various reviews indicate that leave-on cleansers and wipes with moisturizing and protective properties are beneficial and often preferable [9,23,24,25,28,32].
These products often contain low-irritation surfactants, dimethicone, and emollients, and are formulated with a balanced pH similar to that of healthy skin (between 5.4 and 5.9), helping to minimize disruption of the skin's barrier function[9,23].
Studies have shown that "three-in-one" cleansing wipes (with cleanser, moisturizer, and barrier) can result in a lower prevalence and incidence of IAD compared to using pH-neutral soap-and-water or aerosol cleaners and barrier creams[9,24,32,33].
Cleaning with this type of product should be done with a gentle, careful technique, using minimal friction and avoiding rubbing or scrubbing the skin [9,21,26,34]. The use of soft materials, such as disposable nonwoven towels, is recommended to minimize friction damage and prevent cross-infection [9,26,34]. These methods can reduce nursing time and associated labor costs[9,24,33,35,36].
If we compare the incidence or prevalence data of our study with those of the scientific literature, we find similarities. A systematic review[31] found that a skincare protocol using wipes with three-in-one cleansing, moisturizing, and protective properties resulted in a lower incidence of IAD. Specifically, 80 cases of IAD per 1,000 participants were reported among those who used three-in-one wipes, compared with 259 cases per 1,000 participants among those who used pH-neutral soap-and-water. This finding was based on one RCT with 121 participants, and we judged the evidence to be of moderate quality.
In a 2022 review by Rumbo Prieto[24], aimed to establish the efficacy of topical skin products in reducing the occurrence or severity of IAD, including the use of three-in-one wipes, No-Sting Barrier Film, foam cleansers, leave-in cleansing lotion, and a long-lasting protective cream and concluded the following:
- - Three-in-one wipes as a more robust option: The use of three-in-one cleansing wipes (cleanser, moisturizer, and barrier) consistently demonstrates a lower incidence and prevalence of IAD compared to soap-and-water or separate two-step products (cleaner + ZnO barrier). This positions them as an effective option for the standardization of perineal care, although their effect on the severity of skin deterioration was not significant.
- - Both foam cleansers (especially those with dimethicone) and leave-in cleansing lotions are shown to be more effective at preventing or treating IAD than standard soap-and-water care, offering improvement, albeit sometimes marginal.
- - No-Sting Barrier Films were shown to be significantly more effective in protecting the skin or slowing its degradation than ZnO, although their effectiveness was comparable to that of 3-in-1 wipes. In addition, the long-lasting barrier cream exhibited high effectiveness in treating and resolving IAD within 14 days.
Evidence suggests the need to replace traditional soap-and-water perineal care with protocols that incorporate specialized products that combine cleansing, hydration, and skin barrier protection [24].
Another review by Bohnenkamp showed that at 120 days, the prevalence of IAD in the group treated with three-in-one wipes was 8.1%, while in the soap-and-water group it was 27.1% [32].
Dry wipes or no rinsing afterwards are the methods our study showed yielded the best results. As we have seen above, the Kaplan-Meier curve visually points to this method of hygiene being superior (Figures 13-15); however, it is essential to interpret this finding with caution due to the low number of events (only 4 cases) that defined the estimates of the Kaplan-Meier curve in the dry wipe hygiene group of a total of 164 participants in the study. While the direction of the result is clear, extrapolation of this potential benefit to a wider population should be the subject of more powered studies with a higher number of events. For the rest of the products, the curve falls quickly and lower, so the results are worse. Specifically, with the rest, it indicates that most individuals develop the event more quickly and more frequently (Figures 10,12). These results align with the literature, which positions this method as an advantage over more conventional methods, such as soap-and-water. They are defined as specialized cleansers with a slightly acidic pH (close to 5.5), designed to be gentle, that do not require rinsing, and that often contain surfactants and emollient or moisturizing ingredients[28,33,37]. A randomized controlled trial compared the use of a 3-in-1 disposable wipes (impregnated with a cleansing agent, a moisture barrier enhancer, and a dimethicone-based skin protectant) with standard care (cleaning with pH-neutral soap-and-water) in nursing home patients and participants who used the 3-in-1 wipes had a significantly lower incidence of IAD (8.1%) compared to the group who received standard care (27.1%) (p=0.003)[38]; however, our study shows better value than dry wipes.
A doctoral thesis with some similarity to this one, but using the ECA methodology [26], compared a ZnO ointment and a No-Sting Barrier Film with basic soap-and-water hygiene and found no statistically significant difference between the intervention groups and the control group in the prevention of IAD. The specific results showed a relative risk of 0.54 for No-Sting Barrier Film compared with the control, but the p-value of 0.183 indicated that the difference was not statistically significant.
Overall, soap-and-water performed poorly in preventing and treating IAD[25]. Sources suggest that hygiene methods that go beyond the simple use of soap-and-water, such as three-in-one wipes or foam cleansers, may be more effective in reducing the incidence and prevalence of IAD. Soap-and-water, while inexpensive, are considered less effective and potentially more aggressive to vulnerable skin.
- - Absorbent. Brand or composition and frequency of changes
The quality and efficacy of absorbent products directly influence the prevention and treatment of IAD. Aspects such as design, absorbency, retention and breathability are crucial[16,26,39]. Its use without clinical justification, without an adequate assessment of clinical needs or in the absence of incontinence can cause unintentional harm to the patient such as skin damage, risk of falls or psychological dependence[40].
An improved diaper design, including breathable materials, can reduce skin occlusion and overhydration, thereby decreasing the risk of IAD[9,36,40,41]. Some diapers incorporate cellulose fibers that help lower the pH on the skin's surface or superabsorbent polymers that turn urine into gel, reducing exposure to air and helping to mitigate odor[9,40] and the size, logically, must be appropriate for the patient, as one that does not fit well around the legs and waist can increase the risk of IAD, as well as leaks.
The different brands of absorbents available differ in their composition and, as we have seen in our study, this influences the appearance of an IAD. There are no quality studies in the literature that directly compare one brand to another, but the composition of absorbents and their efficacy are studied. The composition of absorbents considered best for the prevention of IAD focuses on maintaining an acidic surface pH and reducing occlusion and excess moisture from the skin[42,43]. The spiral curly fiber cellulose allows to buffer the pH of the alkaline fluid (such as urine) and maintain a more acidic environment close to the skin. This design by interposing a special type of acidic, curly or spiral fiber cellulose between the top layer (in contact with the skin) and the absorption core (containing superabsorbent polyacrylate) allows to achieve a surface pH of 4.6 that remained stable even after repeated wetting over a period of 5 hours in contrast to the conventional composition that can reach values of 7.1[42,44]. On the other hand, the introduction of polyacrylate superabsorbent polymers into the absorption core is critical; they compartmentalize liquids and prevent rewetting even under pressure, resulting in a drier skin microenvironment[42,43]. The addition of absorbents of water vapour permeable and breathable outer sheets reduce skin occlusion and are also considered a breakthrough point in the design of absorbents for incontinence control[42,43]. These compounds are present in the B brand of absorbents used in our study and obtained the best prevention results (Annex 13).
These same compounds could be present in brand A, although we do not know this because the data are sensitive and have not been provided by the manufacturers, and we can only access product information online [45].
But even if present in both, perhaps other additives or differences in the concentration and type of the superabsorbent polymer influenced the absorption capacity and/or the rate of superficial drying, thereby preventing IAD. In addition, it is important to point out, as a limiting and influential point, the degree of absorption of each scheduled absorbent: day, night, or supernight; since the number of changes of absorbents was taken into account, but not the degree of absorption that each one had.
In a 2018 RCT [26], the frequency of absorbent changes was similar to our study, with 3 absorbents per day, a minimum of 2.84 and a maximum of 3.03; thus, identifying a higher global incidence of IAD, which we will discuss in the next section.
The frequency of change of absorbent products is a key aspect in the prevention of IAD, although evidence on optimal technique and frequency is limited[24]. Interestingly, some sources indicate that the possibility of skin damage may increase with the frequency of soap-and-water cleaning, suggesting that routine washing after each episode of urinary incontinence might need re-evaluation and frequency reduction where possible[9].
The effects of different change frequency regimes (less frequent, every eight hours, vs. frequent, every four hours) in institutionalized women have been studied [9,46], finding no significant differences in the incidence or severity of erythema/dermatitis between the groups. However, the less frequent change regimen did result in significantly wetter skin. The authors hypothesized that this increase in humidity did not translate into an increased occurrence of IADs due to the absence of stool during the night, underscoring the critical role of fecal enzymes in the development of dermatitis, since, in the absence of stool, increased skin moisture alone might not be the determining factor for IAD. However, they acknowledge that it makes the skin more vulnerable to friction and abrasion[9,12,46]. Even so, the absorbent's protective effect decreases or disappears when the device is saturated, allowing moisture to remain in direct contact with the skin and preventing its evaporation. Clinical experience also suggests that the risk of IAD is related to occlusion and prolonged contact with urine or feces when the absorbent is saturated[9].
5.2. Sociodemographic Variables and Their Influence on the Appearance of IAD
- - In relation to age.
Our study found no statistical significance (p= 0.81) in the association between the age of an incontinent patient and the occurrence of an IAD.
The prevalence and incidence of IAD tend to be higher in older people, and this is attributed to the fact that aging is a factor associated with incontinence and skin changes in older people, which make it more fragile and vulnerable[9,25,26]. However, there is research that goes along the same lines as ours that suggests that age does not seem to be an isolated risk factor for IAD, that there are no significant differences in the appearance or manifestation of IAD according to age[9].
- In relation to gender.
The prevalence of urinary incontinence is higher in women, regardless of age, mainly due to anatomical causes, and therefore the frequency of IAD[9,24]. Nonetheless, the scientific literature is not entirely clear, as there are also studies where significant differences are found in the appearance or manifestations of IAD according to sex[9]. The present results are not consistent with those reported in this research, in which we did not find a statistical relationship (p=0.21).
- - In relation to the degree of dependency according to the Barthel Index.
The Barthel Index is used to measure the level of functional dependence and activities of daily living in patients. Our study did not conclude statistically significant relationships between patients' level of dependence and the development of IAD. Nor has any direct or explicit relationship between the Barthel Index score and the appearance of IAD been found in the scientific literature. However, it has been identified that patients with higher degrees of functional and mental impairment have a higher probability of suffering from IAD[9,47]. This implies that greater dependence, measured by scales such as the Barthel, could be indirectly associated.
- - In relation to the risk detected for MASD according to the PAT scale.
The PAT is a scale designed to assess the risk of developing IAD. It assesses risk based on four subscales that rank the intensity of the irritant (liquid, soft, urine stools), duration of contact, perineal skin condition, and the presence of other contributing factors (such as antibiotic use or Clostridium difficile diarrhea), with a total score range between 4 and 12 points. It has been suggested that a score of between 7 and 8 points could be a threshold for distinguishing between low and high risk, although its predictive validity has not been formally measured[9].
Our results do show a statistical significance between the risk measured with the PAT scale and the incidence of IAD (p=0.02). In fact, there are already preventive algorithms for IAD that use the PAT scale score to guide absorbent change frequency, for example, every 2 hours for high scores [8,9,10,11,12] and every 4 hours for medium scores [4,5,6,7] [48].
- - In relation to the risk detected for pressure injuries according to the Braden scale.
Traditionally, the original Braden scale was specifically designed to assess the risk of developing pressure injuries. But a doctoral thesis defended in 2016[49] entitled "Predictive Capacity of Risk Assessment Scales for Pressure Ulcers and Other Dependence-Related Injuries in the Critically Ill Patient" and a subsequent article published in the Journal of Wound Care[50] focused on Braden's predictive capacity and other scales (such as EMINA and EVARUCI) primarily for pressure injuries and dependence-related skin lesions (DRSLs)s in general. In the thesis, the author determined the cut-off points that offer the best balance between validity and predictive capacity for each scale. For example, the cut-off point that offered the best balance between validity and predictive capacity for the Braden Scale, in the context of Alba Roca Biosca's doctoral thesis, referred to above, was 10.
Traditionally, humidity has been linked to the development of pressure injuries[36] and the Braden scale includes humidity as an extrinsic factor[51]. Braden scale factors, such as constant or frequent skin moisture and friction and shear problems during repositioning or mobilization, increase the likelihood of having IAD[9,47]. The Braden friction/shear subscale was associated with a 1.87-fold increase in the odds of IAD at admission for every one-point decrease in the score[52]. Altered sensory perception was also associated with IAD[52].
Therefore, a priori, the results of our research are not surprising, where a statistically significant association (p=0.004) has been found between high scores on the Braden scale and the development of an IAD. The mean Braden score of patients who developed an IAD was 13.62.
Although the literature confirms an association between IAD and pressure injury formation, where IAD may be associated with a higher incidence of LPP than established by the Braden risk scale score alone. This suggests that while Braden is useful for LPP, the presence of an IAD may alter its predictability for pressure injury[21] and in some reviews no predictive utility for IAD has been found at all[9].
That is why it has been suggested that pressure injury risk assessment scales, such as the Braden scale, may not be adequate to predict skin changes specifically related to incontinence [9], and that there are specific risk alternatives for moisture injuries, such as the PAT Scale.
6. Conclusions
- The study found a statistically significant relationship between the Braden and PAT scales and the occurrence of IAD. This means that the greater the risk detected by these scales, the more lesions develop.
- No statistically significant relationship was found between age, sex, or Barthel Index and the development of IAD.
- The hygiene method significantly influenced the occurrence of IAD, showing that soapy wipes had the highest association with the occurrence of IAD, while dry wipes appear to be the most protective.
- In addition, the dry wipes hygiene method proved to be the most effective, as it presented the lowest cumulative risk and the longest time of onset of the event in contrast to soap-and-water where there was an earlier onset of IAD and were appearing throughout the follow-up.
- The brand of the absorbent was also significantly associated with the occurrence of IAD. The "B" brand prevented one injury for every 6 patients compared to the "A" brand.
- The frequency of absorbent changes did not show a statistically significant association with the occurrence of IAD.
References
- Defloor T, Schoonhoven L, Fletcher J, Furtado K, Heyman H, Lubbers M, et al. Statement of the European Pressure Ulcer Advisroy Panel—pressure ulcer classification: differentiation between pressure ulcers and moisture lesiones. J Wound Ostomy Continence Nurs. 2005 Sep-Oct; 32(5):302-6.
- García-Fernández FP, Soldevilla-Ágreda JJ, Pancorbo-Hidalgo PL, Verdú Soriano J, López-Casanova P, Rodríguez-Palma M, et al. Classification-categorization of skin lesions related to dependence. GNEAUPP Technical Document Series No II. 3rd Edition. National Group for the Study and Advice on Pressure Ulcers and Chronic Wounds. Logroño. 2021.
- Gray M, Bohacek L, Weir D, Zdanuk J. Moisture vs pressure: making sense out of perineal wounds. J Wound Ostomy Continence Nurs.2007 Mar-Apr; 34(2):134-42.
- Torra i Bou JE, Rodríguez Palma M, Soldevilla Agreda J, García Fernández FP, Sarabia Lavin R, Zabala Blanco J, et al. Redefining the concept and approach to damp lesions: A conceptual and methodological proposal to improve the care of damp-associated skin lesions (LESCAH). Gerokomos.2013; 24(2):90-4.
- Rumbo-Prieto JM, Arantón-Areosa L, López-de los Reyes R, Vives-Rodríguez E. Practical Guide to Skin Lesions Associated with Moisture [Practical Guide no. 7]. In: Rumbo-Prieto JM, Raña-Lama CD, Cimadevila-Álvarez MB, Calvo-Pérez AI, Fernández-Segade J, editors. Collection of practical wound guides of the Galician Health Service. Santiago de Compostela (A Coruña): Xunta de Galicia. Ministry of Health. Galician Health Service; 2016.
- Fletcher J, Beeckman D, Boyles A, et al. International Best Practice Recommendations: Prevention and management of moisture-associated skin damage (MASD) [Internet]. Londres: Wounds International; 2020 [consultado 11 jun 2025]. Disponible en: www.woundsinternational.com.
- García-Fernández FP, López-Casanova P, Rodríguez-Palma M, Segovia-Gómez T, Soldevilla-Agreda JJ. Skin care in patients with incontinence and prevention of moisture-associated injuries [Internet]. Logroño: GNEAUPP; 2021 [accessed 21 Jun 2025]. Available at: https://gneaupp.info/cuidados-de-la-piel-en-pacientes-con-incontinencia-y-prevencion-de-lesiones-asociadas-a-la-humedad/.
- Paniagua-Asensio ML. Dependency-Related Injuries: Prevention, Classification and Categorization. Clinical Document [Internet]. Logroño: GNEAUPP; 2020 [accessed 21 Jun 2025]. Available at: https://gneaupp.info/lesiones-relacionadas-con-la-dependencia-prevencion-clasificacion-y-categorizacion-documento-clinico-2020/.
- Rodriguez-Palma M. Systematic review of factors related to incontinence-associated dermatitis. Proposal of a new theoretical model [doctoral thesis]. Alicante: University of Alicante; 2015.
- Santiyán González AM, Caminero Ocaña B, González Galán B, Sánchez Carretero C, Bernardino Camacho E, Flores López-Ibarra JM, et al. Dependence-related injuries. In: Collection of Guides for the Care of Wounds. Ciudad Real: Health Service of Castilla-La Mancha (SESCAM). Integrated Care Management of Ciudad Real; 2020.
- García-Ruiz María Piedad, Torres-Bautista Rosa María, López-Franco María Dolores, Orozco-Cuadrado Agustina, Alarcon-Juárez Araceli, Nava-Anguis Vicenta et al . Skin lesions associated with humidity in institutionalized incontinent patients. Gerokomos [Internet]. 2025 [cited 2025 Dec 20] ; 36( 1 ): 43-49. Available at: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1134-928X2025000100008&lng=es. Epub 05-May-2025. https://dx.doi.org/10.4321/s1134-928x2025000100008.
- Banharak S, Panpanit L, Subindee S, Narongsanoi P, Sanun-Aur P, Kulwong W, Songtin P, Khemphimai W. Prevention and Care for Incontinence-Associated Dermatitis Among Older Adults: A Systematic Review. J Multidiscip Healthc. 2021 Oct 26;14:2983-3004.
- McNichol LL, Ayello EA, Phearman LA, Pezzella PA, Culver EA. Incontinence-Associated Dermatitis: State of the Science and Knowledge Translation. Adv Skin Wound Care. 2018 Nov; 31(11):502-513.
- General Council of Nursing; Spanish Institute of Nursing Research. Guide to practical recommendations in nursing: from disease-centred care to incontinence-centred care [Internet]. Madrid: General Council of Nursing; 2021 [accessed 17 Dec 2024]. Available at: https://www.consejogeneralenfermeria.org/profesion/guias-clinicas.
- Ferreira M, Abbade L, Bocchi SCM, Miot HA, Boas PV, Guimaraes HQCP. Incontinence-associated dermatitis in elderly patients: prevalence and risk factors. Rev Bras Enferm. 2020; 73 Suppl 3:e20180475. [CrossRef]
- Dissemond J, Assenheimer B, Gerber V, Hintner M, Puntigam MJ, Kolbig N, et al. Moisture-associated skin damage (MASD): A best practice recommendation from Wund-D.A.CH. J Dtsch Dermatol Ges. 2021 Jun; 19(6):815-25.
- Owen EJ, Heylen RA, Stewart K, Winyard PG, Jenkins ATA. Detecting and monitoring incontinence associated dermatitis: Does impedance spectroscopy have a part to play? Proc Inst Mech Eng H. 2024 Jun; 238(6):655-666.
- Jiang T, Zhang X, Wu J, Gao L, Tung TH. Risk Factors for Incontinence-Associated Dermatitis in Adults: A Systematic Review and Meta-Analysis. J Wound Ostomy Continence Nurs. 2025 Jan-Feb 01; 52(1):66-75.
- Graham T, Beeckman D, Kottner J, Fader M, Fiorentino F, Fitzpatrick JM, et al. Skin cleansers and leave-on product interventions for preventing incontinence-associated dermatitis in adults. Cochrane Database Syst Rev. 2025 Jul 11; 7(7):CD011627.
- Raepsaet C, Fourie A, Van Hecke A, Verhaeghe S, Beeckman D. Management of incontinence-associated dermatitis: A systematic review of monetary data. Int Wound J. 2021 Feb; 18(1):79-94.
- Smart H, Sibbald RG. Skin care for the protection and treatment of incontinence associated dermatitis (IAD) to minimise susceptibility for pressure injury (PI) development. WCET® Journal. 2020; 40(4):40-4.
- Bliss DZ, Savik K, Thorson MA, Ehman SJ, Lebak K, Beilman G. Incontinence-associated dermatitis in critically ill adults: time to development, severity, and risk factors. J Wound Ostomy Continence Nurs. 2011 Jul-Aug; 38(4):433-45. PMID: 21747261. [CrossRef]
- Fastner A, Hauss A, Kottner J. Skin assessments and interventions for maintaining skin integrity in nursing practice: An umbrella review. Int J Nurs Stud. 2023 Jul;143:104495.
- Rumbo-Prieto JM. Efficacy of topical skin products in the treatment and prevention of incontinence-associated dermatitis: a systematic review. Jan [Internet]. 2021 [accessed 17 Jun 2025]; 15(3):1338. Available at: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1988-348X2021000300014&lng=es.
- García-Ruiz MP. Effectiveness of non-irritating barrier films and zinc oxide ointment: exploratory review. Gerokomos. 2022; 33(1):45-52.
- Goulart Constant Alcoforado CL. Effect of zinc oxide ointment and non-irritating barrier film on the prevention of incontinence-associated dermatitis in hospitalized elderly: a randomized controlled trial [tesis doctoral]. Belo Horizonte: Universidade Federal de Minas Gerais. School of Nursing; 2018.
- Groven FM, Zwakhalen SM, Odekerken-Schröder G, Joosten EJ, Hamers JP. How does washing without water perform compared to the traditional bed bath: a systematic review. BMC Geriatr. 2017 Jan 25; 17(1):31. PMID: 28118815; PMCID: PMC5264342. [CrossRef]
- Glass GF Jr, Goh CCK, Cheong RQ, Ong ZL, Khong PCB, Chan EY. Effectiveness of skin cleanser and protectant regimen on incontinence-associated dermatitis outcomes in acute care patients: A cluster randomised trial. Int Wound J. 2021 Dec; 18(6):862-73.
- Castanedo-Cázares JP, Cortés-García JD, Cornejo-Guerrero MF, Torres-Álvarez B, Hernández-Blanco. Study of the cytotoxic and irritative effect of soaps for skin cleansing. Gac. Dr. Méx [online journal]. 2020 Oct; 156(5):426-431.
- Veje PL, Chen M, Jensen CS, Sørensen J, Primdahl J. Effectiveness of two bed bath methods in removing microorganisms from hospitalized patients: A prospective randomized crossover study. Am J Infect Control. 2020 Jun; 48(6):638-643. Epub 2019 Dec 6. PMID: 31813632. [CrossRef]
- Beeckman D, Van Damme N, Schoonhoven L, Van Lancker A, Kottner J, Beele H, et al. Interventions for preventing and treating incontinence-associated dermatitis in adults. Cochrane Database Syst Rev. 2016 Nov 10; 11(11):CD011627. PMID: 27841440; PMCID: PMC6464993. [CrossRef]
- Pather P, Hines S, Kynoch K, Coyer F. Effectiveness of topical skin products in the treatment and prevention of incontinence-associated dermatitis: a systematic review. JBI Database Syst Rev Implement Rep. 2017 May; 15(5):1473-96. PMID: 28498177. [CrossRef]
- Doughty D, Junkin J, Kurz P, Selekof J, Gray M, Fader M, et al. Incontinence-associated dermatitis: consensus statements, evidence-based guidelines for prevention and treatment, and current challenges. J Wound Ostomy Continence Nurs. 2012 May-Jun; 39(3):303-15; quiz 316-7. PMID: 22572899. [CrossRef]
- Wei HH, Huang CL, Huang WP, Chen HC. Development of an incontinence-associated dermatitis prevention bundle using an evidence-based framework. WCET® Journal. 2020; 40(3):37-42.
- Rueda-López J, Guerrero-Palmero A, Segovia-Gómez T, Muñoz-Bueno AM, Bermejo-Martínez M, Rosell-Moreno C. Irritant diaper dermatitis: local treatment with barrier products and quality of life. Gerokomos [Internet]. 2012 [accessed 17 Jul 2025]; 23(1):35-41. Available at: https://dx.doi.org/10.4321/S1134-928X2012000100007.
- García-Fernández FP, Pancorbo-Hidalgo PL, Verdú-Soriano J. Effectiveness of the Non-Irritating Barrier Film in the prevention of skin lesions: Systematic review. Gerokomos. 2009; 20(1):29-40.
- Groven FMV, Zwakhalen SMG, Odekerken-Schröder G, Tan F, Hamers JPH. Comfort during the bed bath-A randomised crossover trial on the effect of washing without water versus water and soap in nursing students. J Clin Nurs. 2021 Aug; 30(15-16):2234-2245. Epub 2021 May 6. PMID: 33352004; PMCID: PMC8360161. [CrossRef]
- Kon Y, Ichikawa-Shigeta Y, Iuchi T, Nakajima Y, Nakagami G, Tabata K, et al. Effects of a Skin Barrier Cream on Management of Incontinence-Associated Dermatitis in Older Women: A Cluster Randomized Controlled Trial. J Wound Ostomy Continence Nurs. 2017; 44(5):481-6.
- Fader M, Cottenden AM, Getliffe K. Absorbent products for moderate-heavy urinary and/or faecal incontinence in women and men. Cochrane Database Syst Rev. 2008 Oct 8; 2008(4):CD007408. PMID: 18843748; PMCID: PMC12131696. [CrossRef]
- Evans T. To pad or not to pad? The use of containment products in healthcare. British Journal of Community Nursing. 2025 Apr; (The Continence Supplement):S26-S32. [CrossRef]
- Estarlich-Corominas J, Alexandre-Lozano S, Rosell-Moreno C. Effectiveness of acrylate polymer transparent film in the prevention and treatment of skin lesions. Bibliographic review. Gerokomos.2019; 30(3):147-56.
- Beguin AM, Malaquin-Pavan E, Guihaire C, Hallet-Lezy AM, Souchon S, Homann V, Zöllner P, Swerev M, Kesselmeier R, Hornung F, Smola H. Improving diaper design to address incontinence associated dermatitis. BMC Geriatr. 2010 Nov 22;10:86. PMID: 21092161; PMCID: PMC3000399. [CrossRef]
- Runeman B. Skin interaction with absorbent hygiene products. Clin Dermatol. 2008 Jan-Feb; 26(1):45-51. PMID: 18280904. [CrossRef]
- Bliss DZ, Bland P, Wiltzen K, Gannon A, Wilhems A, Mathiason MA, et al. Incontinence Briefs Containing Spiral-Shaped Fiber Acidify Skin pH of Older Nursing Home Residents at Risk for Incontinence-Associated Dermatitis. J Wound Ostomy Continence Nurs. 2017 Sep/Oct; 44(5):475-480. PMID: 28877114. [CrossRef]
- Severe incontinence [Internet]. Indas; n.d. [cited 14 Dec 2025]. Available at: https://www.indas.com/product-categories/incontinencia-grave.
- Fader M, Clarke-O’Neill S, Cook D, Dean G, Brooks R, Cottenden A, et al. Management of night-time urinary incontinence in residential settings for older people: an investigation into the effects of different pad changing regimes on skin health. J Clin Nurs. 2003 May; 12(3):374-86.
- Kottner J, Blume-Peytavi U, Lohrmann C, Halfens R. Associations between individual characteristics and incontinence-associated dermatitis: a secondary data analysis of a multi-centre prevalence study. Int J Nurs Stud. 2014 Oct; 51(10):1373-80. Epub 2014 Feb 23. PMID: 24636666. [CrossRef]
- Salomé GM, Da Rocha CA, Miranda FD, Alves JR, Dutra RAA, Tenório AG. Algorithms for prevention and treatment of incontinence-associated dermatitis. ESTIMA. 2020; 18:e1320. Disponible en: https://www.revistaestima.com.br/estima/article/view/837.
- Roca-Biosca MA. Predictive capacity of the risk assessment scales for pressure ulcers and other dependence-related injuries in the critically ill patient [Internet] [doctoral thesis]. Tarragona: Universitat Rovira i Virgili; 2016 [accessed 12 Dec 2024]. Available at: http://hdl.handle.net/10803/399144.
- Roca-Biosca A,Rubio-Rico L, de Molina Fernández MI, García Grau N, Tuset Garijo G,García Fernández FP. Predictive validity of the Braden scale for assessing risk of developing pressure ulcers and dependence-related lesions. Journal of Wound Care 2017; 26(9): 528-536.
- Braden B, Bergstrom N. A conceptual schema for the study of the etiology of pressure sores. Rehabil Nurs. 1987; 12(1):8-12.
- Long MA, Reed LA, Dunning K, Ying J. Incontinence-associated dermatitis in a long-term acute care facility. J Wound Ostomy Continence Nurs. 2012 May-Jun; 39(3):318-27. PMID: 22552105. [CrossRef]
Figure 5.
Hygiene method and percentage of occurrence of IAD. Source: Authors.
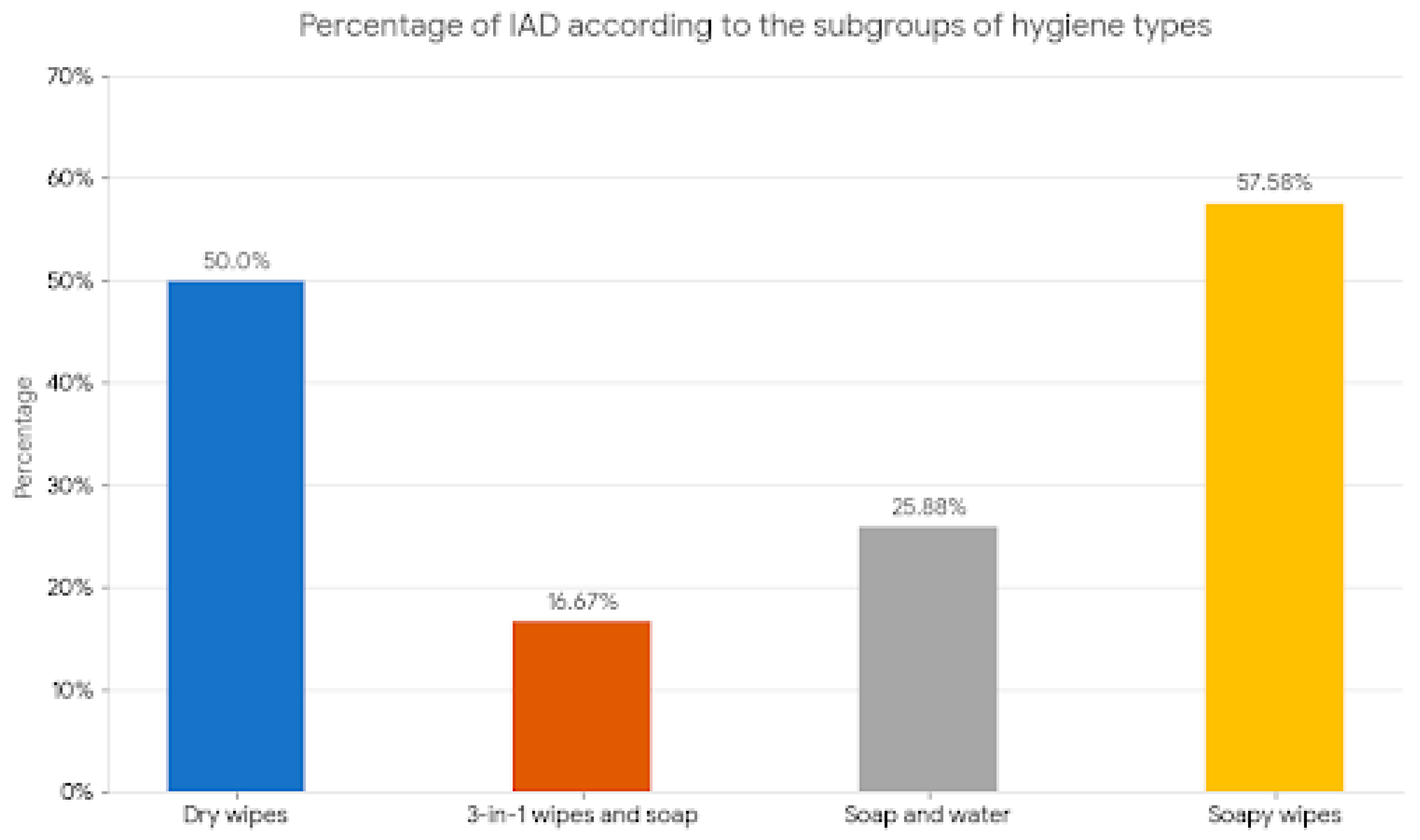
Figure 6.
Kaplan-Meier curve for hygiene methods. Source: Authors.
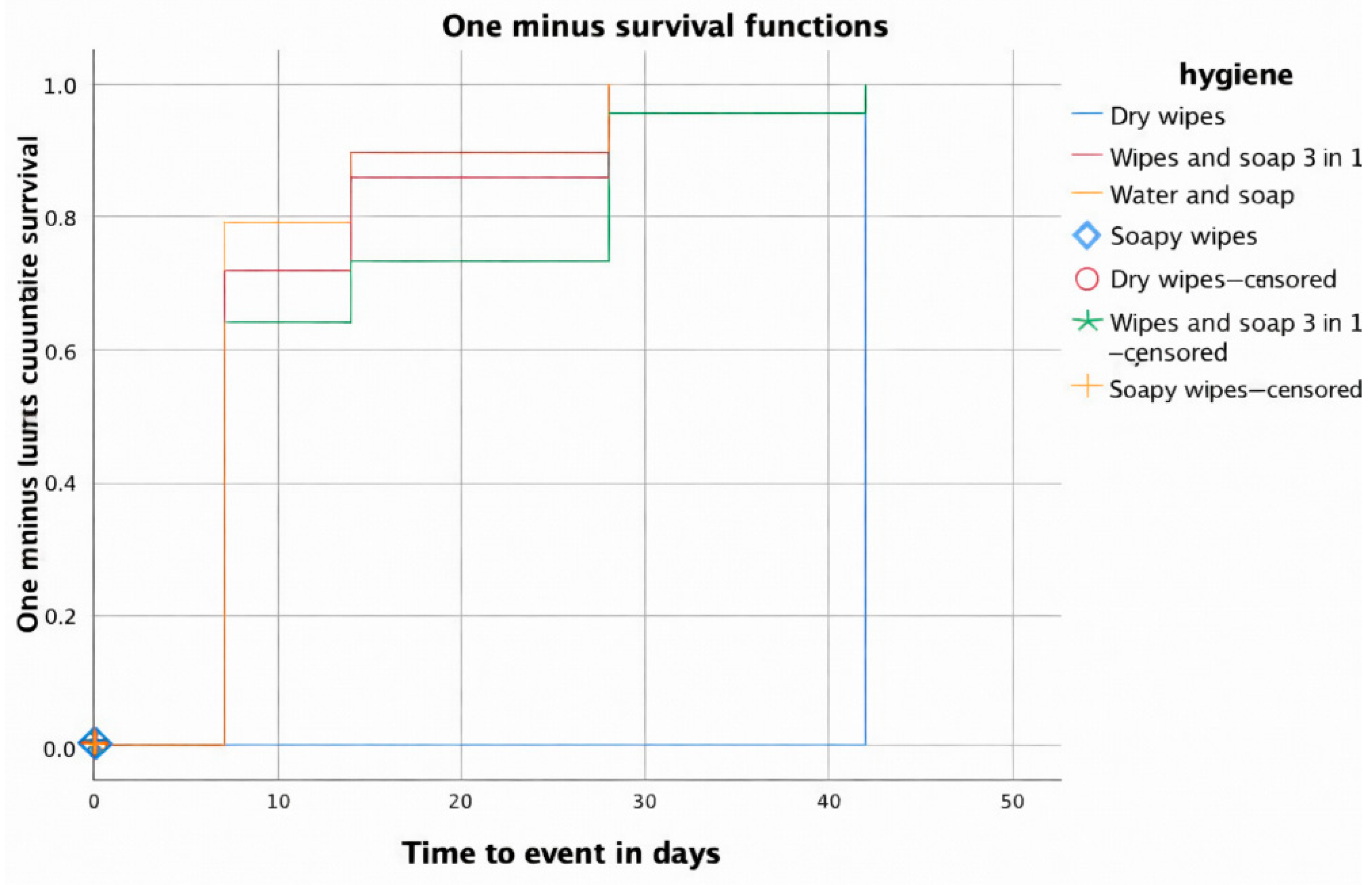
Figure 7.
Kaplan-Meier curve for hygiene methods, according to survival. Source: Authors.
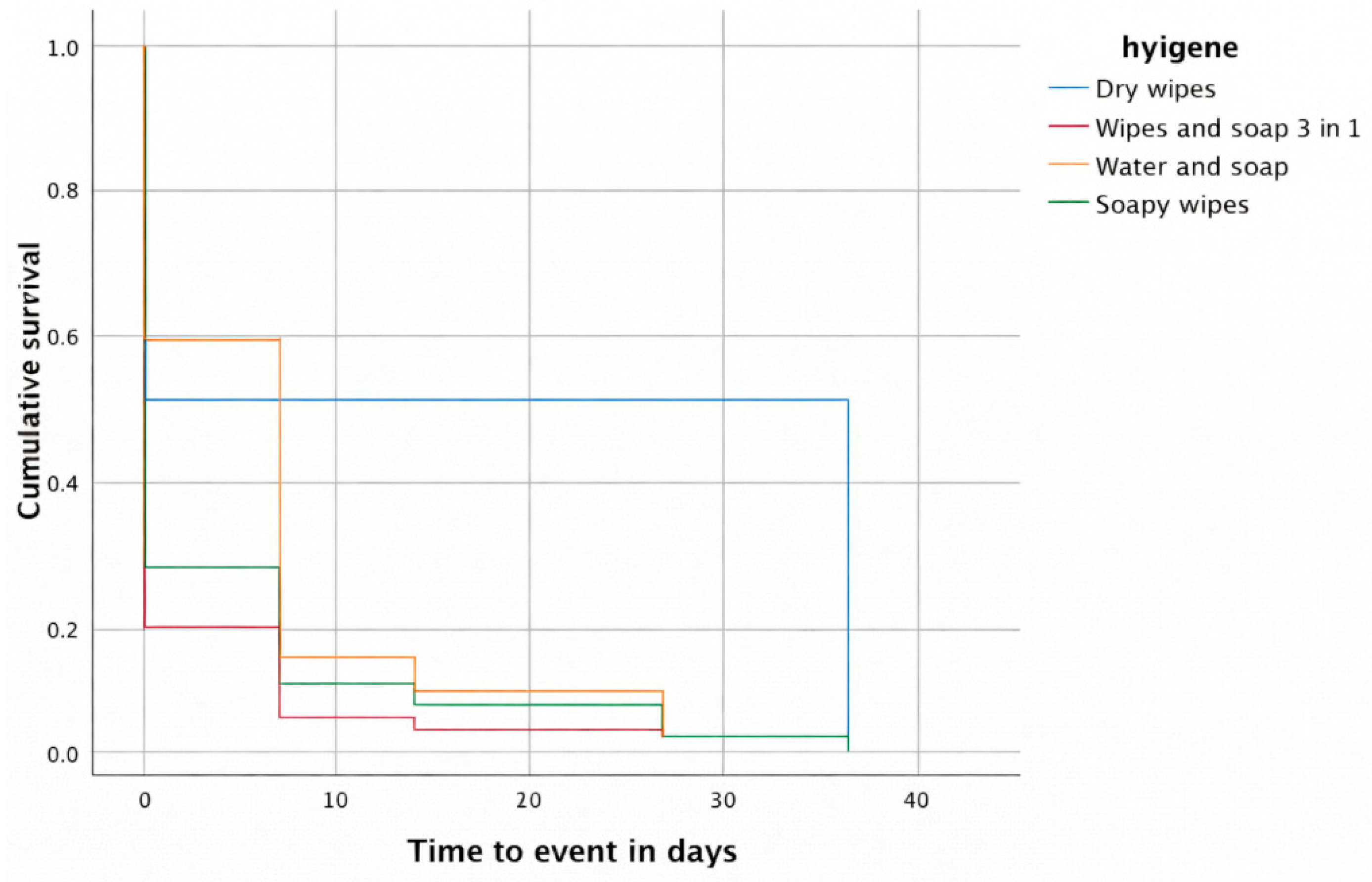
Figure 8.
Kaplan-Meier curve for hygiene methods, according to risk function. Source: Authors.
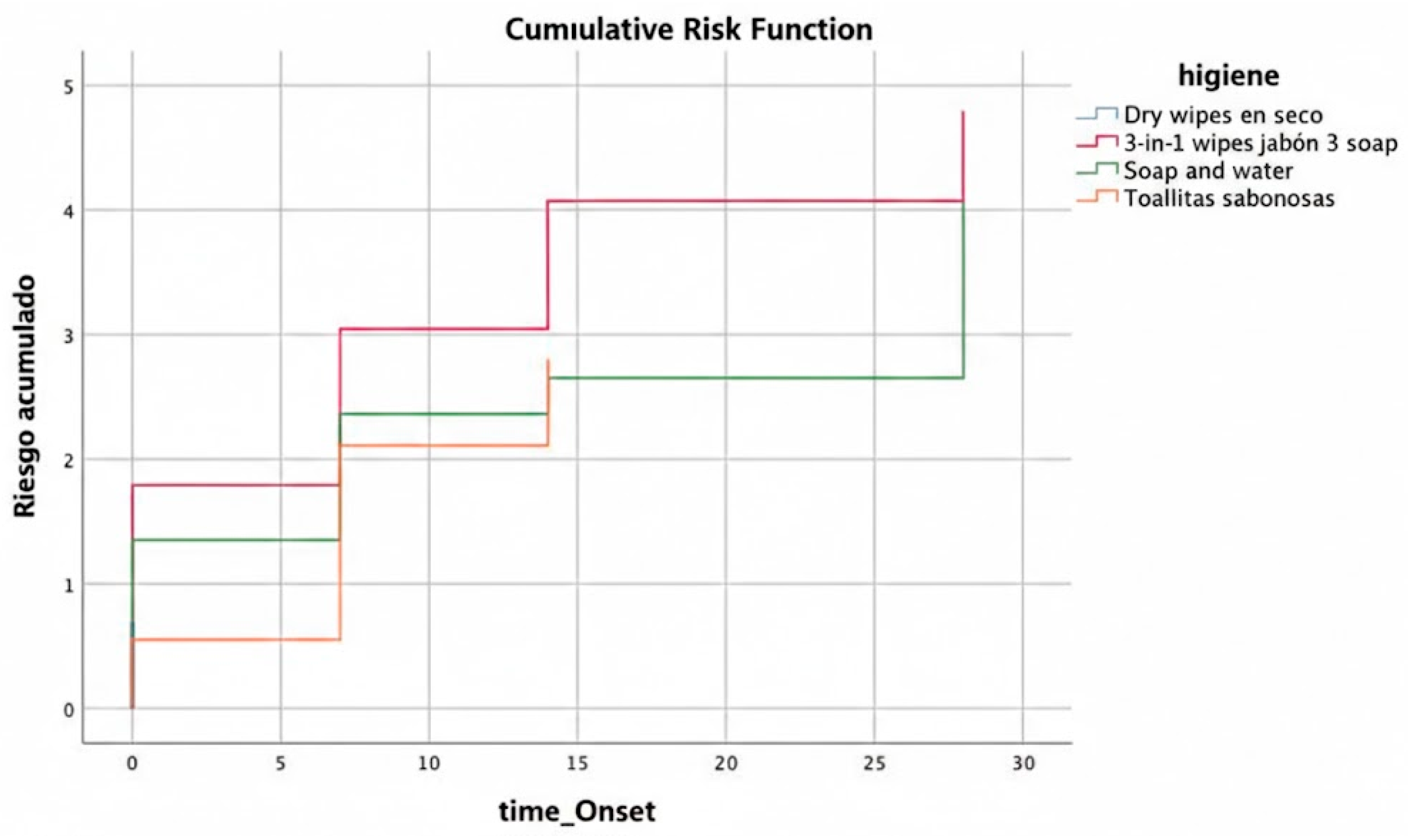
Figure 9.
Kaplan-Meier curve for absorbent brand. Source: Authors.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



