
Submitted:
23 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Background: Lemierre’s syndrome, previously termed the “forgotten disease” after the introduction of modern antibiotics, is a rare and potentially fatal infection of the neck resulting in septic thrombophlebitis of the internal jugular and other neck veins. There has been an increased resurgence of this disease in more recent years and it remains an important diagnosis with life threatening potential to consider when presenting with multifocal cavitary pneumonia. Fusobacterium necrophorum, an obligate anaerobic gram-negative bacterium is the most isolated culprit organism involved in this condition, however often fastidious and difficult to culture. The use of gene sequencing using 16rRNA can aid in this diagnosis when uncertainty exists. Methods: This case report describes an otherwise healthy 17 year-old male with a history of vaping presenting with upper respiratory infectious symptoms who ultimately was diagnosed with multi-focal necrotizing pneumonia. There was significant diagnostic uncertainty throughout the case as traditional microbiologic culture mechanisms failed to identify a causative organism for tailored antimicrobial treatment. This was despite direct empyema fluid analysis and pulmonary-bronchial biopsy. Novel gene sequencing was performed using 16s rRNA typing, a promising new way to identify a catalog of host organisms, detecting F. necrophorum. This diagnosis prompted further diagnostic imaging of the neck, confirming a small internal jugular clot and diagnosis of Lemierre’s Disease. Results: This case highlights the need for suspicion of Lemierre’s disease in patients presenting with multi-focal pneumonia. Furthermore, it re-iterates the idea of culture-negative infection, whereby fastidious organisms or tissue samples do not readily provide a diagnosis. Lastly, it further introduces hypotheses regarding the use of vaping and associated significant infection and lung injury. Conclusions: The use of 16s rRNA sequencing for the detection of fastidious, opportunistic organisms is another tool for physicians to ensure adequate diagnostic clarity and appropriate treatment.
Keywords:
Lemierre's disease
; 16s rRNA sequencing
; acute respiratory distress syndrome
; ARDS
; necrotizing pneumonia
; Fusibacterium necrophorum
; vape-associated lung injury
; empyema
Introduction
Lemierre’s syndrome, previously termed the “forgotten disease” after the introduction of modern antibiotics, is a rare and potentially fatal infection of the neck resulting in septic thrombophlebitis of the internal jugular and other neck veins. There has been an increased resurgence of this disease in more recent years, likely in part due to changes in antibiotic prescription patterns with B-Lactams typically only prescribed for confirmed streptococcal pharyngitis and simply better testing to diagnose and report this condition. Additionally, with the increased usage of macrolides and fluoroquinolones for pneumonias, selection for organisms with broad antimicrobial resistance to these medications may occur [1]. While still rare, it remains an important diagnosis with life threatening potential to consider when presenting with multifocal cavitary pneumonia, as was seen in this case. It is classically recognized in younger patients by clinical signs of deep neck space infection or radiological imaging indicating jugular vein thrombosis with a recent history of oropharyngeal infection.
Fusobacterium necrophorum, an obligate anaerobic gram-negative bacterium is the most commonly isolated culprit organism involved in this condition [2,3,4]. This fastidious organism typically colonizes the human oropharynx, possibly contributing to routine non-streptococcal pharyngitis, gingival and odontogenic infections [5,6]. With mucosal breakdown, repeat inhalational exposure and immunocompromised states it behaves as an opportunistic pathogen resulting in necrotizing abscesses of the lungs, liver, heart, brain and other organ systems [5,6,7,8]. Lemierre’s disease caries an overall mortality of 4-9% increasing to upwards of 21% with F. necrophorum bacteremia and systemic infection [7]. Unfortunately, F. necrophorum remains a challenging organism to culture by traditional methods [9].
This manuscript reviews novel approaches to clinical identification of bacterial pathogens for Lemierre’s disease through the review of a complex patient case. It also reviews the associations of vaping, an increasing popular alternative to traditional smoking, with opportunistic oropharyngeal and pulmonary infections. The goal of this review is to improve clinical suspicion and highlight diagnostic opportunities for these types of infections, overall improving treatment and patient care.
Case Presentation:
A previously healthy 17-year-old male presented to a peripheral tertiary emergency department acutely unwell with a preceding 5-7 day history of cough, fevers, chills, rigors, myalgias and shortness of breath. He was found to be hypotensive, tachycardic with rapid shallow breathing and relatively hypoxic with initial vitals as followed; HR 188, BP 102/51, RR 36, 02 saturation of 92%. Chest X-ray revealed multifocal consolidations (Figure 1). He was fluid resuscitated, placed on non-invasive pressure ventilation due to his work of breathing and elevated respiratory rate and given ceftriaxone, azithromycin, vancomycin and dexamethasone empirically with admission to hospital. The remainder of his clinical exam was unremarkable, specifically normal cardiac examination with no murmurs and a normal head and neck examination without any neck stiffness, tonsillar exudate, or lymphadenopathy. His past medical and social history only revealed significant e-cigarette and vape pen usage of both nicotine and cannabis products. Initial laboratory investigations of note included a leukocytosis, mild thrombocytopenia and anemia, as well as evidence of presumed acute kidney injury and elevated venous lactate (Table 1).
Despite aggressive resuscitation and sepsis management, the patient continued to decompensate, developing acute respiratory distress syndrome (ARDS) within 24 hours requiring intubation and ICU support. Initial blood cultures did not reveal a specific pathogen. On post-admission day three the patient was transferred to our center for consideration of Veno-venous Extracorporeal Membrane Oxygenation (VV-ECMO) due to profound ongoing hypoxemia. Computer Tomography imaging (CT) of the chest was performed upon arrival showing cavitating airspace disease with significant, presumed exudative, bilateral pleural effusions (Figure 2). A transesophageal echo was also performed which revealed stress cardiomyopathy and global dysfunction with an ejection fraction of 35%. No endocarditis was identified. Systemic immunoglobulin testing shows elevated levels of IgG, IgA and IgM, (Table 1) and further testing for HIV and other immunocompromising conditions were negative.
Bronchoscopy was performed with samples sent for both standard and immunocompromised infectious work-up. Targeted bronchoscopic biopsy was obtained from the right upper lobe, however, ultimately did not aid in the diagnosis of a specific pathogen, showing only inflammatory cells. Bilateral chest tubes were inserted to drain the pleural effusions. Samples were obtained from each lung, confirming exudative effusions based on Light’s criteria and were visibly purulent. Significantly elevated cell count and LDH were noted in the fluid sample (Table 1). These samples were sent for standard and fastidious cultures. Given the significantly elevated LDH, multifocal cavitating pneumonia, and septic shock without a causative organism isolated, 16s rRNA gene sequence analysis from the pleural fluid was ordered for further delineation of potential pathogen.
This novel gene sequence analysis proved critical to this patient’s diagnosis as it resulted positive for F. necrophorum. This positive result prompted CT imaging of the patient’s neck revealing a 3cm non-occlusive thrombus in the left internal jugular vein with mild phlegmonous inflammatory changes in the retropharyngeal space. No retropharyngeal, parapharyngeal, tonsillar or apical abscesses were identified to explain the origin of this infection. A diagnosis of Lemierre’s disease was presumed and the patient was started on a six-week course of meropenem in consultation with our Infectious Disease service. The patient had a complicated critical care stay, including tracheostomy placement, small areas of presumed septic emboli in the brain, loculated empyema requiring surgical drainage and severe ICU-acquired weakness and delirium. Ultimately, following a near two-month hospital stay, he was discharged neurologically intact with full recovery of cardiac and renal function. Outpatient follow-up appointments revealed no voiced complaints and continued improvement from the patient. As of one year follow-up formal pulmonary function tests had not been attained, however there was no mention of ongoing shortness of breath because of his complicated pneumonia.
Discussion:
In this case report, this patient presented relatively atypically without a sore throat, neck mass, or neck pain – the typical features of Lemierre’s disease. He instead had a relative rapid respiratory decompensation and septic shock necessitating broad initial management and early transfer to quaternary care facilities. All efforts to identify a causative organism through traditional methods; blood cultures, bronchoscopy evaluation, empyema sampling and even direct biopsy, yielded no causative pathogen. Low culture sensitivity and specificity from pleural fluid is a problem encountered frequently, with up to 40%-56% of parapneumonic effusions and empyema ultimately being cultured negative [10,11]. This may be further exacerbated by empiric antimicrobial therapy in critically ill patients. Given the strong suspicion for culture negative infection, further pleural fluid testing with bacteria gene sequence analysis became critical to furthering this patient’s medical care and identifying F. necrophorum as the culprit organism.
16s rRNA gene sequence is a novel way in which to identify bacterial isolates, specifically useful in bacteria with ambiguous profiles. This method uses gene sequencing to look at the 16s rRNA gene, one that is present in nearly all bacteria, remains stable throughout time with respect to random sequence changes and is often preserved within the same bacterial families [12]. It has been shown that 16S rRNA gene sequence analysis can be used to identify nonculture bacteria or organisms that are rarely isolated by traditional methods [9]. Identification rates for the genus of the organism are greater than 90%, with a range from 62-85% for specific bacterial species identification [5]. In a recent retrospective review, this type of gene sequencing of pleural fluid has been shown to add to diagnosis in 63% of patients [13]. More specifically, 16s rRNA gene sequencing has been utilized in small case reports to increase diagnostic yield for Fusobacterium sp. within pleural fluid, broncho-alveolar lavage samples and from direct abscess aspiration [6,8,10]. This techniques usage remains novel and rare, with our case being one of the first to utilize this technique to find a causative organism in culture-negative septic shock and ultimately led to the diagnosis of Lemierre’s disease when no other clinically apparent features of the disease were present. Clinically, the test characteristics of 16s gene sequencing make it ideal in cases when traditional methods of culture and identification of organisms have not worked, or in this case, when the organisms are challenging to identify by traditional means.
The route of infection with F. necrophorum in this patient remains in question. While the patient had radiographic evidence of Lemierre’s disease, his clinical complaints and presentation did not identify typical risk factors. One possible theory would be this patient’s noted heavy use of e-cigarettes and vaping. While evidence linking the use of e-cigarettes and F. necrophorum or other necrotizing pneumonias is sparse, we do know that e-cigarettes compromise the integrity of the mouth, oropharynx and trachea-bronchial tree causing persistent inflammatory states [14]. The typical route of infection of F. necrophorum is through mucosal membrane breakdown [15], making it plausible that in patients with this constellation of mucosal injury from vaping, may be at higher risk. Other emerging case reports have identified F. necrophorum cavitary multifocal pneumonia with or without internal jugular clot in young patients who use e-cigarettes, further questioning whether there is a relationship between vaping and F. necrophorum infection [16,17]. El Chebib and colleagues further describe the literature in this regard, commenting on the links between compounds found within e-cigarettes and impaired host defence mechanisms [16]. More specifically, animal models have shown that common components of e-cigarette liquid such as nicotine, propylene glycol and flavouring substances such as cinnamaldehyde impair mucociliary clearance and phagocytic function, while animal models exposed to vaping liquid show impaired innate immunity and an increased virulence in colonizing bacteria [16,18,19,20]. With medical knowledge surrounding the complications of e-cigarette usage continuing to grow, its reasonable to hypothesize that a heightened suspicion for opportunistic anaerobic necrotizing infections is warranted in individuals with significant usage.
Conclusion:
Lemierre’s disease is an oft overlooked diagnosis and should be considered in patients presenting with necrotizing multi-lobal pneumonia. As illustrated by this case report, Gene sequencing of the 16s rRNA sequence is a novel way in which to improve diagnostic yield for specific bacteria pathogens in ambiguous or culture negative patients where infection is still the most likely condition. As gene sequencing becomes more readily available, there may be a more routine role for this type of testing to further support antimicrobial identification and stewardship. Lastly, though un-established, there is a growing body of literature suggesting e-cigarettes may reduce host immunity and allow for opportunistic infections of the oropharynx and lungs. Ongoing suspicion for these types of infections in patients who vape when there is diagnostic ambiguity is warranted.
Contributions: MH; Primary author. Responsible for all written sections. KB; Responsible for background research, literature synthesis and editing. AG; Responsible for background research, primary editing and final formatting for submission AFR; Oversaw project development, completion, editing and final formatting.
Ethical Statement: Verbal and written consent for education-related dissemination of this case and publication were obtained from patient and legal guardian at time of discharge from hospital.
References
- Sen, Lee W; Jean, SS; Chen, FL; Hsieh, SM; Hsueh, PR. Lemierre’s syndrome: A forgotten and re-emerging infection. In Journal of Microbiology, Immunology and Infection; Elsevier Ltd, 2020; Vol. 53, pp. 513–7. [Google Scholar]
- Eilbert, W; Singla, N. Lemierre's syndrome. Int J Emerg Med 2013, 6(1), 40. [Google Scholar] [CrossRef]
- Karkos, PD; Asrani, S; Karkos, CD; Leong, SC; Theochari, EG; Alexopoulou, TD; et al. Lemierre’s syndrome: A systematic review. Laryngoscope 2009, 119(8), 1552–9. [Google Scholar] [CrossRef]
- Valerio, L; Corsi, G; Sebastian, T; Barco, S. Lemierre syndrome: Current evidence and rationale of the Bacteria-Associated Thrombosis, Thrombophlebitis and LEmierre syndrome (BATTLE) registry. In Thrombosis Research; Elsevier Ltd, 2020; Vol. 196, pp. 494–9. [Google Scholar]
- Huggan, PJ; Murdoch, DR. Fusobacterial infections: Clinical spectrum and incidence of invasive disease. Journal of Infection 2008, 57(4), 283–9. [Google Scholar] [CrossRef] [PubMed]
- Saar, M; Vaikjärv, R; Parm, Ü; Kasenõmm, P; Kõljalg, S; Sepp, E; et al. Unveiling the etiology of peritonsillar abscess using next generation sequencing. Ann Clin Microbiol Antimicrob 2023, 22(1). [Google Scholar] [CrossRef] [PubMed]
- Afra, K; Laupland, K; Leal, J; Lloyd, T; Gregson, D. Incidence, risk factors, and outcomes of Fusobacterium species bacteremia. BMC Infect Dis 2013, 13(1). [Google Scholar] [CrossRef] [PubMed]
- Liu, Y; Li, Z; Fu, H; Ruan, W; Wang, H; Ding, Y; et al. The first case report: diagnosis and management of necrotizing fusobacterium lung abscess via BALF next-generation sequencing. BMC Infect Dis 2024, 24(1). [Google Scholar] [CrossRef] [PubMed]
- Bank, S; Nielsen, HM; Hoyer Mathiasen, B; Christiansen Leth, D; Hagelskjær Kristensen, L; Prag, J. Fusobacterium necrophorum- detection and identification on a selective agar. APMIS 2010, 118(12), 994–9. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, Y; Kryukov, K; Tomomatsu, K; Sakamaki, F; Inoue, S; Nakagawa, S; et al. Diagnosis of pleural empyema/parapneumonic effusion by next-generation sequencing. Infect Dis. 2021, 53(6), 450–9. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M; Patel, S; Sadaka, AS; Bedawi, EO; Corcoran, JP; Porcel, JM. Recent insights into the management of pleural infection. In International Journal of General Medicine; Dove Medical Press Ltd, 2021; Vol. 14, pp. 3415–29. [Google Scholar]
- Janda, JM; Abbott, SL. 16S rRNA gene sequencing for bacterial identification in the diagnostic laboratory: Pluses, perils, and pitfalls. Journal of Clinical Microbiology 2007, Vol. 45, 2761–4. [Google Scholar] [CrossRef]
- Hjertman, J; Bläckberg, J; Ljungquist, O. 16S rRNA is a valuable tool in finding bacterial aetiology of community-acquired pleural empyema–a population-based observational study in South Sweden. Infect Dis. 2022, 54(3), 163–9. [Google Scholar] [CrossRef]
- Seiler-Ramadas, R; Sandner, I; Haider, S; Grabovac, I; Dorner, TE. Health effects of electronic cigarette (e-cigarette) use on organ systems and its implications for public health. In Wiener Klinische Wochenschrift; Springer, 2021; Vol. 133, pp. 1020–7. [Google Scholar]
- Goldberg, EA; Venkat-Ramani, T; Hewit, M; Bonilla, HF. Epidemiology and clinical outcomes of patients with Fusobacterium bacteraemia. Epidemiol Infect. 2013, 141(2), 325–9. [Google Scholar] [CrossRef]
- El Chebib, H; McArthur, K; Gorbonosov, M; Domachowske, JB. Anaerobic necrotizing pneumonia: Another Potential Life-threatening Complication of Vaping? Pediatrics 2020, 145(4). [Google Scholar] [CrossRef] [PubMed]
- Venditto, L; Ferrante, G; Caccin, A; Franchini, G; Zaffanello, M; Tenero, L; et al. Lung abscess as a complication of Lemierre Syndrome in adolescents: a single center case reports and review of the literature. Ital J Pediatr 2023, 49(1). [Google Scholar] [CrossRef] [PubMed]
- Sussan, TE; Gajghate, S; Thimmulappa, RK; Ma, J; Kim, JH; Sudini, K; et al. Exposure to electronic cigarettes impairs pulmonary anti-bacterial and anti-viral defenses in a mouse model. PLoS One 2015, 10(2). [Google Scholar] [CrossRef] [PubMed]
- Laube, BL; Afshar-Mohajer, N; Koehler, K; Chen, G; Lazarus, P; Collaco, JM; et al. Acute and chronic in vivo effects of exposure to nicotine and propylene glycol from an E-cigarette on mucociliary clearance in a murine model. Inhal Toxicol 2017, 29(5), 197–205. [Google Scholar] [CrossRef] [PubMed]
- Hwang, JH; Lyes, M; Sladewski, K; Enany, S; McEachern, E; Mathew, DP; et al. Electronic cigarette inhalation alters innate immunity and airway cytokines while increasing the virulence of colonizing bacteria. J Mol Med. 2016, 94(6), 667–79. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Initial X-ray revealing bilateral, multi-lobar airspace disease.
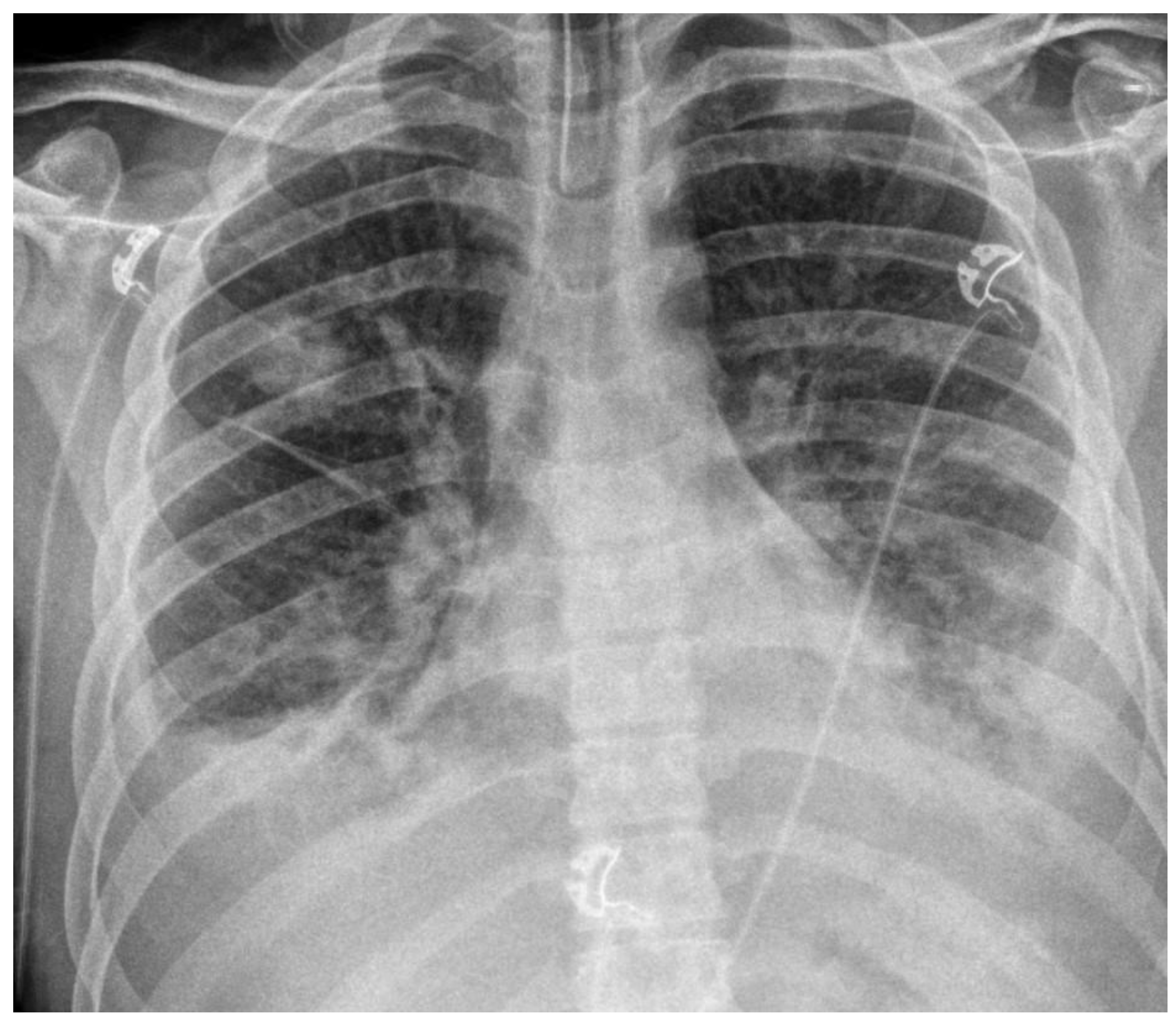
Figure 2.
Representative axial Computed Tomography (CT) of patient’s lungs. Demonstrates bilateral multi-focal airspace disease with corresponding bilateral empyemas.
Figure 2.
Representative axial Computed Tomography (CT) of patient’s lungs. Demonstrates bilateral multi-focal airspace disease with corresponding bilateral empyemas.
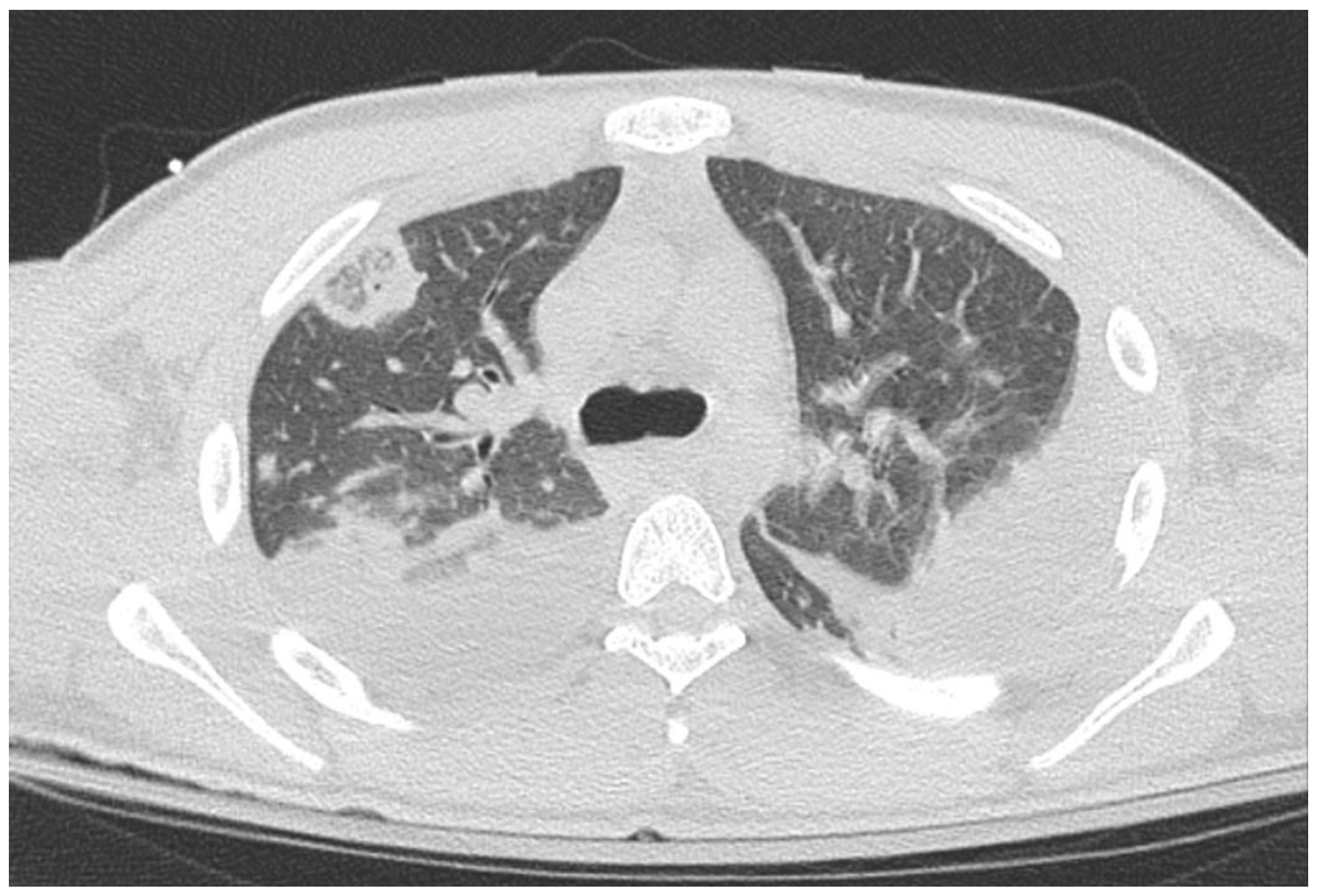

Table 1.
Select Laboratory Results from patient investigations.
| Test | Patient Result (reference range) |
| Serology | |
| Initial Leukocytes | 26 x109/L |
| Initial Platelet | 104 x109/L |
| Initial Hemoglobin | 102 x109/L |
| Initial Creatinine | 180 mmol/L |
| Initial Venous Lactate | 3.0 mmol/L |
| Immunoglobulins | |
| IgG | 19.4g/L (6.35-16.65g/L) |
| IgA | 4.97g/L (0.7-3.5g/L) |
| IgM | 2.33g/L (0.41-2.07g/L) |
| Pleural Analysis (exudative) | |
| Cell Count | 118,760 x106/L |
| Leukocytes | 117,760 x106/L |
| LDH | >10,000 u/L (upper limit of assay detection) |
| Protein | 44g/L |
| Gram Stain + Culture | No Growth |
| Tuberculosis Culture | No Growth |
| Fungal Culture | No Growth |
| 16s PCR | Positive – presence of Fusibacterium Necrophorum |
| Bronchoscopy | |
| Bacterial Culture | Negative |
| Fungal | No fungal elements |
| Aspergillus Galactomannan Antigen | 0.49 (<0.5) |
| Pneumocystis DFA | Not Detected |
| Brucella AB | Non Reactive (<1:20) |
| Viral Panel* | Negative |
| Tuberculosis Culture | Negative |
| Myobacterium PCR | Not Detected |
| Legionella DNA | Not Detected |
| Histoplasmosis AB | Negative |
| Right Upper Lobe Biopsy | Inflammatory Cells, No microorganisms |
*viral panel includes: Influenza A&B, Covid-19, Para-influenza, RSV, adenovirus, metopneumo virus, rhino/entero virus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



