Submitted:
22 January 2026
Posted:
23 January 2026
You are already at the latest version
Abstract
Systemic light-chain (AL) amyloidosis is a rare and incurable disease, classified under the category of plasma cell neoplasms and other diseases with paraproteins in the fifth edition of the World Health Organization classification of lymphoid tumors. This entity shares some similarities with multiple myeloma (MM), remarkably a bone marrow infiltration of clonal plasma cells. Moreover, one out of five newly diagnosed AL amyloidosis (NDAL) also fulfills the current diagnostic criteria for MM. A multidisciplinary therapy approach should be established, in which hematological therapy plays a crucial role. Anti-clonal therapy is the basis of hematological therapy, besides supportive therapy and emerging anti-fibrils therapy. In recent years, advances in the anti-clonal therapy of MM have progressively transferred to carefully selected patients with systemic AL amyloidosis, significantly improving outcomes in this rapidly changing field. This review aims to critically analyze the comparative evolution and evidence-based approach of anti-clonal therapy in NDAL vs. MM since the introduction of bortezomib. Participation in clinical trials remains the first option to consider in daily clinical practice.
Keywords:
systemic light-chain amyloidosis
; multiple myeloma
; treatment
; anti-clonal therapy
; immunotherapy
; autologous stem cell transplant
; anti-CD38 monoclonal antibodies
; conjugated monoclonal antibodies
; bispecific antibodies
; chimeric antigen receptor T-cell therapy
1. Introduction
Immunoglobulin (Ig)-related light chain (AL) amyloidosis is a challenging and heterogeneous entity included in the 5th edition of the World Health Organization (WHO) classification of lymphoid tumors [1] into the category of “Plasma cell neoplasms and other diseases with paraproteins”, and in the family of “Diseases with monoclonal Ig deposition”.
AL amyloidosis can be local, in about 5% of patients [2], or systemic, in most cases. Systemic involvement must always be excluded in cases of local disease at the time of diagnosis. The clinical behavior of true localized AL amyloidosis is commonly benign, with a very low risk of systemic transformation. Importantly, only systemic AL amyloidosis patients require systemic treatment.
Newly diagnosed (ND) systemic AL amyloidosis (NDAL) is characterized by the presence of a clonal population of Ig secreting bone marrow plasma cells (cBMPCs), that produces a light chain (LC) as either an intact Ig or as LC-only monoclonal protein. This protein misfolds and forms insoluble amyloid fibrils that deposit in different organs, causing organ failure [3]. The spectrum of monoclonal gammopathies (MGs) includes MG of uncertain significance (MGUS), MG of clinical significance (MGCS), multiple myeloma (MM), Waldenström macroglobulinemia (WM), and other entities [4]. The bone marrow aspirate and biopsy are crucial to characterize cBMPCs and confirm a timely and accurate diagnosis [5].
The prognostic impact of comorbidity in MM and systemic AL amyloidosis is well documented [6,7]. About 20% of patients with systemic AL amyloidosis fulfill the current diagnostic criteria for MM (AL/MM) [2], representing a peculiar form of comorbidity with negative prognostic impact. Nonetheless, AL amyloidosis may be associated with other MGs such as MGUS, MGCS, particularly MG of renal significance, WM, other types of non-Hodgkin lymphomas, and the full spectrum of MM ranging from smoldering MM (SMM) from plasma cell leukemia.
MM and systemic AL amyloidosis are both complex, incurable, and heterogeneous diseases. However, the epidemiology of these two entities [8,9] presents key differences, mainly in terms of incidence and prevalence, being considered systemic AL amyloidosis a rare disease. Consequently, the pace of research has been agile, thrilling, and dizzying in MM, while the rhythm in AL amyloidosis has been slow and challenging. Interestingly, AL/MM patients have been able to benefit from recent approved therapeutic advances in MM, showing deeper hematological (hem) and cardiac (car) responses. The response dynamics studies demonstrated that achieving an early and deep hem response was necessary in most cases to reach deep and long-lasting car response, which is the crucial endpoint in terms of overall survival (OS) [10,11]. This has been confirmed mainly in the setting of observational real-world (RW) studies. Unfortunately, patients with both diseases have usually been mutually excluded in specific clinical trials for one of the two entities.
The use of T-cell redirecting immunotherapy has transformed the treatment of relapsed/refractory (RR) MM (RRMM). Both chimeric antigen receptor (CAR) T cells and T-cell engagers have changed this clinical scenario, and they are being investigated in ND MM (NDMM). The prognostic relevance of achieving and maintaining measurable residual disease (MRD) negativity (MRD-) has been confirmed in both NDMM and RRMM [12,13], becoming a surrogate early endpoint of progression free survival (PFS) and OS. The growing evidence on the role of MRD in systemic AL amyloidosis seems to point in the same direction as in the case of MM [14].
The current therapeutic approach of systemic AL amyloidosis should be necessarily personalized, comprehensive, and multidisciplinary [15,16], involving a group of specialists integrated into a specific AL clinical unit. Hematological treatment should be addressed at three levels. First, supportive therapy [17]. Second, anti-clonal therapy [18,19]. Third, anti-fibrils therapy (currently, only available in clinical trials) [20].
Epidemiology can help to unveil clinical disparities and therefore, it could be considered the first level of heterogeneity. The incidence and prevalence of AL are much lower than those of MM, justifying slower research development.
Despite similarities between AL and MM (cBMPCs infiltration and similar anti-clonal therapy), a time-based comparative approach in [15,16the evolution of the anti-clonal therapies is lacking. This narrative review aims to comparatively explore the evolving bortezomib-based anti-clonal therapy in NDAL vs. MM, focusing on the respective accumulated evidence and the speed with which it was obtained.
2. The Evolution over Time of Anti-Clonal Therapy in Systemic-AL Amyloidosis
The history of anti-clonal therapy in systemic AL amyloidosis mirrors what happened in MM, with some peculiarities, nuances, and a certain delay. Overall, three periods could be pointed out.
2.1. Second Half of the 20th Century, the Chemotherapy Era
The history of systemic AL amyloidosis has been recently summarized [21]. Remarkably, more than a century passed from the first clinical use of the term “amyloid” by Rudolf Virchow (1854) and the first description of a patient with primary amyloidosis, attributed to Samuel Wilks (1856), to the use of alkylating agents in the 1960s. Melphalan (M) was first used in MM [22], and later in AL amyloidosis, when the close relationship between AL and MM was pointed out [23,24,25].
MF was the most frequently used during the past century in both NDAL and RRAL. However, a shift to cyclophosphamide (C) occurred over the past two decades due to its immunomodulatory effect and a better safety profile in comparison with MF [26]. Since 2005, Bendamustine (B) has been an option particularly for RRAL [27].
Alkylating agents are usually administered in combination with corticosteroids, mainly prednisone (p) or dexamethasone (d).
The seemingly outdated chemo era has reached the present day. C remains in use besides daratumumab (D), bortezomib (V) and d, as a quadruplet (DVCd), being the current standard of care (soc) for NDAL patients [18,19]. On the other hand, high dose M (HDM) is still the preferred conditioning regimen for autologous stem cell transplant (ASCT) in transplant eligible (TE) AL patients [28].
2.2. First Two Decades of the 21st Century, the Era of the New Agents
Immunomodulatory drugs (IMiDs) and proteasome inhibitors (PIs), the so-called new agents, have gained special prominence in the treatment of AL patients over the last two decades.
Regarding IMiDs [29], thalidomide (T) was the first-in-class drug used in this setting, followed by lenalidomide (R) and pomalidomide (P). IMiDs are mainly used in RRAL patients. These all-oral drugs should be used with caution, particularly in patients with cardiac involvement, due to their toxicity profile.
PIs [30] have been a cornerstone in the treatment of AL patients over the current century, following their success in MM. V is still the PI most frequently used, remaining involved in the present soc for NDAL. Intravenous carfilzomib and oral ixazomib are other less used PIs.
Both families of drugs can be eventually combined with each other, with alkylators, and corticosteroids, resulting in different and well-known combinations such as VCd [31].
2.3. Third Decade of the 21st Century, the Immunotherapy Era
The recognition of specific therapeutic targets in cBMPCs allowed the development of monoclonal antibodies (mAbs) [32] and Ab-drug-conjugates (ADC) [33], deeply changing the treatment paradigm of PC disorders, first in MM and then in AL.
The emergence of antiCD38 mAbs represented a revolution in the treatment of AL, being D the first antiCD38 used [34]. The addition of D to VCd in the phase 3 Andromeda trial [35] was the basis for the first FDA approved regimen for NDAL in 2021. Subsequently, other antiCD38 mAbs were developed. Isatuximab (Isa) as monotherapy has demonstrated similar results than D in the RRAL setting [36].
Elotuzumab (Elo) is a mAb targeting the signaling lymphocytic activation molecule family member F7 (SLAMF7). It has been mainly used in RRAL, in combination with IMiDs [37].
B-cell maturation antigen (BCMA) is a glycoprotein expressed on cBMPCs which has become a key therapeutic target for MM and AL. Several BCMA-targeting approaches have been developed [38,39]. First, belantamab mafodotin (belamab) is a BCMA-directed IgG1 conjugated to monomethyl auristatin F, a microtubule-disrupting agent. Curiously, the first report on the use of belamab as single agent in AL was also in 2021, involving six RR AL/MM patients [40]. Second, T-cell redirecting bispecific Abs (BsAbs). Several BCMA-CD3 BsAbs have been used in RRAL, mainly teclistamab [41] and elranatamab [42], whereas ABBV-383 (etentamig) [43], linvoseltamab, and others, are under development. Third, chimeric antigen receptor (CAR) T-cells [44]. Several anti-BCMA CAR-T cells have been used in AL: NXC201 (HBI0101) [45,46], idecabtagene vicleucel (Ide-cel, BB2121) [47], ciltacabtagene autoleucel (Cilta-cel) [48,49], and cesnicabtagene autoleucel (ARI0002h) [50]. Fourth, emerging anti-BCMA therapeutic approaches. Trispecific Abs (TsAbs) may potentially overcome acquired resistance to BsAbs. JNJ-5322 is a TsAb dually targeting BCMA and G protein-coupled receptor class C group 5 member D (GPRC5D), showing a 100% overall response rate (ORR) in a recent phase 1 study (NCT05652335) for RRMM patients [51].
3. The Evolving Landscape of Bortezomib-Based Therapies in NDAL vs. NDMM
New drugs for MM and AL are usually first tested in the RR setting and then in ND patients. V has demonstrated a crucial role in both entities since its accelerated approval by FDA in 2003 for its use in RRMM, based on the phase II SUMMIT trial [52]. Five years passed before its approval for NDMM in 2008.
From the beginning, V was commonly used in combination with d (Vd), due to a well demonstrated synergism. Step by step, different Vd-based combinations that were used in NDMM were also tested in NDAL, except for those associated with an unacceptable toxicity profile, particularly in terms of cardiotoxicity, such as Adriamycin (A) in VAd. Progressively, different alkylating agents were associated with the Vd backbone, mainly M, C, and B, as well as IMiDs (T, R, P), and mAbs (D, Isa, Elo), in diverse triplets or quadruplets.
AL is a rare entity and therefore the evidence in the evolving landscape of the treatment in NDAL patients comes maily from case reports and small single-center series of real-world retrospective studies. To avoid potential bias in the comparison between the respective evolution of NDMM and NDAL anti-clonal therapy, only chronologically ordered, V-based, phase II and III clinical trials for both clinical scenarios were analyzed in Table 1, after an intensive English PubMed search including the following terms: “multiple myeloma, systemic AL amyloidosis, clinical trials, induction, therapy, treatment, bortezomib, and newly diagnosed”.
Several phase II and two phase III trials [53,54,55,56,57,58] assessed Vd in NDMM (2005-2015) whereas in the NDAL setting, a small observational study [59] including 18 consecutive AL patients (11 NDAL and 7 RRAL) treated with Vd pointed out an excellent 94% ORR. Shortly after a phase III tested direct ASCT vs. two cycles of Vd as induction followed by ASCT [60], showing a better outcome for patients treated with Vd induction. The corresponding phase II studies for NDAL [61,62,63] presented an evident delay (2015-2020) with respect to those for NDMM.
VAd was utilized as induction in NDMM mainly during the first decade of the current century [64,65,66], but this triplet was not applied to NDAL due to the A-associated cardiotoxicity risk.
Until the advent of D, the soc for NDAL patients was a combination of Vd and an alkylating agent, M (VMd or VMp) or C (VCd). Again, a huge difference in the time frame and the associated supporting evidence was obvious between both clinical scenarios. Regarding VMp, several phase II and III trials (2008-2025) demonstrated excellent outcomes in TI NDMM [67,68,69,70,71]. Remarkably, 682 patients were recruited in the phase III VISTA trial (2008) over less than two years [67]. In contrast, only one relatively recent (2020) phase III trial established VMd as soc in NDAL [72]. This study included 109 patients, and the recruitment took place over five years.
The clinical impact of VCd was also extensively analyzed in phase II and III trials (2009-2019) for NDMM patients [73,74,75,76,77,78,79] whereas most studies investigating the role of this triplet in NDAL patients were retrospective. Only one recent trial [80] demonstrated a lack of clinical benefit when doxycycline was added to VCd compared with VCd alone in cardiac NDAL patients. The most relevant retrospective study using VCd in NDAL enrolled 230 patients during more than six years [81].
Frontline BVp was explored in NDMM [82,83], but no trials were identified on the use of this triplet in NDAL patients.
Regarding combinations of V with IMiDs, several trials were identified for NDMM patients with the following triplets: VTd [84,85,86], VRd [87,88,89,90], and PVd [91]. However, no trials with these triplets were tested in NDAL patients.
As expected, all the previously commented anti-clonal combinations were challenged with the progressive introduction of different mAbs directed against specific therapeutic targets such as anti-SLAMF7 (Elo), anti-CD38 (D, Isa) and anti-BCMA (Belamaf). Overall, VRd has been the most widely used regimen to combine with the new mAbs in NDMM. This way, EloVRd revealed excellent results in NDMM [92,93,94], but trials are lacking in NDAL.
Following thrilling clinical development schedules, first D and then Isa-based anti-clonal therapies have highlighted the key role of targeted anti-CD38 therapy in NDMM and NDAL. D was the first anti-CD38 used in association with the full range of previous V-based regimens in NDMM. Interestingly, two phase II trials on the use of DVd in MM [95] and in AL [96] were published almost simultaneously. The DVMp regimen was successfully applied to transplant ineligible (TI) NDMM [97], but no trials were developed for NDAL. Remarkably, DVCd was also tested earlier in NDMM [98] than in NDAL [35], and other recent trials have confirmed good outcomes in both settings [99,100,101,102]. Regarding D-based combinations with IMiDs, DVTd [103], and mainly DVRd [104,105,106,107], which is the current soc, have been extensively employed in NDMM, but no trials with these combinations have been tested in NDAL, probably due to the toxicity profile of IMiDs.
Alternatively, Isa-based combinations, mostly IsaVRd [108,109,110,111], have also been developed in NDMM with excellent results, but no completed trials are still available for NDAL.
Early assessment of new immunotherapy approaches in NDAL are being evaluated in ongoing clinical trials, but they are beyond the scope of this review, as well as anti-clonal therapy in the RRAL setting.
3. Discussion
The global landscape of V-based phase II/III trials focused on NDMM and NDAL over the last two decades is summarized in Table 2.
58 trials (27 of them were phase III) were included in the analysis, and only 10 of them (17.2%) were performed in the setting of NDAL.
23 (85.2%) out of 27 phase III trials were performed in NDMM, and only 4 in NDAL [35,60,72,102], associated with Vd, VMd, and DVCd.
16 combinations, including doublets, triplets, and quads, were compared in both scenarios. There was at least one NDAL study to compare in 5 (31.2%) of these regimens (Vd, VMp, VCd, DVd, and DVCd), highlighting the real evolution of anti-clonal therapy in NDAL in which V and D appear as the crucial drugs, along with an increasingly cautious use of corticosteroids.
Regarding the long-lasting debate about the use of alkylators in both scenarios, HDM conditioning with ASCT remains in use for TE NDMM and NDAL patients. On the other hand, C is the preferred alkylator for induction in NDAL (DVCd).
Figure 1 shows graphically the important delay in phase II and III trials between NDMM and NDAL regarding four common V-based regimens.
5. Conclusions
The implementation of V-based phase II and III trials in NDAL shows a significant delay when compared with NDMM over the last two decades. Moreover, the number of trials, particularly phase III trials, is significantly lower in the NDAL setting. This is mainly attributed to differences in the epidemiological background of both entities, underlining the difficulty of performing clinical trials in the context of very rare diseases. Despite this, large collaborative research platforms led by referral centers increasingly allow studies to be carried out.
At the present time, two quads (DVRd and DVCd), only changing one drug, are the soc for NDMM and NDAL, respectively. Remarkably, since its introduction two decades ago, V remains a cornerstone in the induction of both entities. On the other hand, anti-CD38 mAbs have also demonstrated a crucial role in the induction therapy of these two scenarios, also in the event of the coexistence of both diseases (AL/MM).
Hopefully, the research background for the introduction of new therapeutic advances in NDAL will be shortened in the coming years and will resemble what happens in NDMM, a model of highly efficient dynamic research.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ADC | Antibody-drug-conjugates |
| AL | Light-chain amyloidosis |
| AL/MM | Light-chain amyloidosis and multiple myeloma |
| ASCT | Autologous stem cell transplant |
| B | Bendamustine |
| BCMA | B-cell maturation antigen |
| BsAbs | Bispecific antibodies |
| C | Cyclophosphamide |
| CAR | Chimeric antigen receptor |
| cBMPCs | Clonal bone marrow plasma cells |
| d | Dexamethasone |
| D | Daratumumab |
| Elo | Elotuzumab |
| HDM | High dose melphalan |
| Ig | Immunoglobulin |
| IMiDs | Immunomodulatory drugs |
| Isa | Isatuximab |
| LC | Light chain |
| M | Melphalan |
| mAbs | Monoclonal antibodies |
| MGs | Monoclonal gammopathies |
| MGCS | Monoclonal gammopathy of clinical significance |
| MGUS | Monoclonal gammopathy of uncertain significance |
| MM | Multiple Myeloma |
| MRD | Measurable residual disease |
| ND | Newly diagnosed |
| NDAL | Newly diagnosed systemic AL amyloidosis |
| NDMM | Newly diagnosed multiple myeloma |
| ORR | Overall response rate |
| OS | Overall survival |
| p | Prednisone |
| P | Pomalidomide |
| PIs | Proteasome inhibitors |
| R | Lenalidomide |
| RR | Relapsed/refractory |
| SMM | Smoldering multiple myeloma |
| T | Thalidomide |
| TE | Transplant eligible |
| TI | Transplant ineligible |
| TsAbs | Trispecific antibodies |
| V | Bortezomib |
| WM | Waldenström macroglobulinemia |
References
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, A.D.; Araujo, I.B.d.O.; Berti, E.; Bhagat, G.; Borges, A.M.; Boyer, D.; Calaminici, M.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022, 36, 1720–1748. [Google Scholar] [CrossRef]
- Ríos-Tamayo, R.; Krsnik, I.; Gómez-Bueno, M.; Garcia-Pavia, P.; Segovia-Cubero, J.; Huerta, A.; Salas, C.; Silvestre, R.; Sánchez, A.; Manso, M.; et al. AL Amyloidosis and Multiple Myeloma: A Complex Scenario in Which Cardiac Involvement Remains the Key Prognostic Factor. Life 2023, 13, 1518. [Google Scholar] [CrossRef]
- Ríos-Tamayo, R. Monoclonal Gammopathies. In Comprehensive Hematology and Stem Cell Research, 1st Edition; Editor Nima Rezaei; Elsevier: Amsterdam, Netherlands, 2024; pp. 358–374. [Google Scholar] [CrossRef]
- Ríos-Tamayo, R.; Paiva, B; Lahuerta, J.J.; Martínez López, J.; Duarte, R.F. Monoclonal Gammopathies of Clinical Significance: A Critical Appraisal. Cancers 2022, 14, 5247. [Google Scholar] [CrossRef]
- Ríos-Tamayo, R.; Sánchez, M.J.; Gómez-Rojas, S.; Rodríguez-Barranco, M.; Segura, G.P.; Redondo-Sánchez, D.; Gómez-Tarragona, G.; Nicolás, A.R.; Ruiz-Cabello, F.; Jiménez, P.; et al. Cell Count Differentials by Cytomorphology and Next-Generation Flow Cytometry in Bone Marrow Aspirate: An Evidence-Based Approach. Diagnostics 2023, 13, 1071. [Google Scholar] [CrossRef]
- Ríos-Tamayo, R.; Sainz, J.; Martínez-López, J.; Puerta, J.M.; Chang, D.Y.L.; Rodríguez, T.; Lahuerta, J.J. Early mortality in multiple myeloma: The time-dependent impact of comorbidity. A population-based study in 621 real-life patients. Am. J. Hematol. 2016, 91, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Ríos-Tamayo, R.; Lecumberri, R.; Cibeira, M.T.; González-Calle, V.; Alonso, R.; Domingo-González, A.; Landete, E.; Encinas, C.; Iñigo, B.; Blanchard, M.J.; et al. A Simple Frailty Score Predicts Survival and Early Mortality in Systemic AL Amyloidosis. Cancers 2024, 16, 1689. [Google Scholar] [CrossRef]
- Ríos-Tamayo, R.; Sánchez Rodríguez, D.; Chang-Chan, D.-Y.-L.; Sánchez Pérez, M.J. Epidemiology of Multiple Myeloma. In Update on Multiple Myeloma; Editor Khalid Ahmed Al-Anazi; Intech: London, UK, 2019; pp. 13–33. [Google Scholar] [CrossRef]
- Ríos-Tamayo, R. Epidemiology of systemic light-chain (AL) amyloidosis. Lymphatics 2025, 3, 25. [Google Scholar] [CrossRef]
- Muchtar, E; Dispenzieri, A.; Leung, N.; Lacy, M.Q.; Buadi, F.K.; Dingli, D.; Grogan, M.; Hayman, S.R.; Kapoor, P.; Hwa, Y.L.; et al. Depth of organ response in AL amyloidosis is associated with improved survival: grading the organ response criteria. Leukemia 2018, 32, 2240–2249. [Google Scholar] [CrossRef] [PubMed]
- Muchtar, E.; Geyer, S.; Merlini, G.; Gertz, M.A. Patients with a cardiac complete response in AL amyloidosis have survival rates similar to those of a matched general population. Blood 2024, 144, 790–793. [Google Scholar] [CrossRef] [PubMed]
- Zabaleta, A.; Puig, N.; Cedena, M.T.; Oliver-Caldes, A.; Pérez, J.J.; Moreno, C.; Tamariz-Amador, L.E.; Rodriguez-Otero, P.; Prosper, F.; Gonzalez-Calle, V.; et al. Clinical significance of complete remission and measurable residual disease in relapsed/refractory multiple myeloma patients treated with T-cell redirecting immunotherapy. Am. J. Hematol. 2025, 100, 93–102. [Google Scholar] [CrossRef]
- Ntanasis-Stathopoulos, I.; Filippatos, C.; Ntanasis-Stathopoulos, A.; Malandrakis, P.; Kastritis, E.; Tsitsilonis, O.E.; Dimopoulos, M.A.; Terpos, E.; Gavriatopoulou, M. Evaluating Minimal Residual Disease Negativity as a Surrogate Endpoint for Treatment Efficacy in Multiple Myeloma: A Meta-Analysis of Randomized Controlled Trials. Am. J. Hematol. 2025, 100, 427–438. [Google Scholar] [CrossRef]
- Lasa, M.; Nuvolone, M.; Kostopoulos, I.V.; Jelinek, T.; Basset, M.; Milani, P.; Massa, M.; Theodorakakou, F.; Wechalekar, A.D.; Zherniakova, A.; et al. Clinical Significance of Measurable Residual Disease (MRD) in Light-Chain (AL) Amyloidosis. Blood 2024, 144, 889–891. [Google Scholar] [CrossRef]
- Sarubbi, C.; Abowali, H.; Varga, C.; Landau, H. Treatment of AL amyloidosis in the era of novel immune and cellular therapies. Front. Oncol. 2024, 14, 1425521. [Google Scholar] [CrossRef]
- O’Sullivan, M.; Osman, W.; Krisnagopal, A.; Parry, M.; Davis, M.; Chu, C.H. Integrated specialty care for amyloidosis: a scoping review using the Consolidated Framework for Implementation Research. BMC Health Serv. Res. 25, 415. [CrossRef] [PubMed]
- Muchtar, E.; Grogan, M.; aus dem Siepen, F.; Waddington-Cruz, M.; Misumi, Y.; Carroll, A.S.; Clarke, J.O.; Sanchorawala, V.; Milani, P.; Caccialanza, R.; et al. Supportive care for systemic amyloidosis: International Society of Amyloidosis (ISA) expert panel guidelines. Amyloid 2025, 32, 93–116. [Google Scholar] [CrossRef] [PubMed]
- Palladini, G.; Milani, P. Individualized Approach to Management of Light Chain Amyloidosis. J. Natl. Compr. Canc. Netw. 2023, 21, 91–98. [Google Scholar] [CrossRef]
- Gertz, M.A. Immunoglobulin light chain amyloidosis: 2024 update on diagnosis, prognosis, and treatment. Am. J. Hematol. 2024, 99, 309–324. [Google Scholar] [CrossRef]
- Wang, J.; Li, J.; Zhong, L. Current status and prospect of anti-amyloid fibril therapy in AL amyloidosis. Blood Rev. 2024, 66, 101207. [Google Scholar] [CrossRef]
- Giorgetti, A.; Pucci, A.; Aimo, A. A Brief history of amyloidosis. In Cardiac Amyloidosis; Emdin, M., Vergaro, G., Aimo, A., Fontana, M., Eds.; Springer: Cham, Switzerland, 2024; pp. 13–22. [Google Scholar] [CrossRef]
- Blokhin, N.; Larionov, L.F.; Perevod-chikova, N.I.; Chebotreva, L.; Merkulova, N. Clinical experiences with sarcolysin in neoplastic diseases. Ann. N.Y. Acad. Sci. 1958, 68, 1128. [Google Scholar] [CrossRef] [PubMed]
- Kyle, R.A.; Bayrd, E.D. Primary" Systemic Amyloidosis and Myeloma Discussion of Relationship and Review of 81 Cases. Arch Intern Med 1961, 107, 344–353. [Google Scholar] [CrossRef]
- Jones, N.F.; Hilton, P.J.; Tighe, J.R.; Hobbs, J.R. Treatment of “primary” renal amyloidosis with melphalan. The Lancet 1972, 300, 616–619. [Google Scholar] [CrossRef]
- Kyle, R.A.; Bayrd, E.D. Amyloidosis: Review of 236 cases. Medicine (Baltimore) 1975, 54, 271–99. [Google Scholar] [CrossRef]
- Swan, D.; Gurney, M.; Krawczyk, J.; Ryan, A.E.; O’Dwyer, M. Beyond DNA Damage: Exploring the Immunomodulatory Effects of Cyclophosphamide in Multiple Myeloma. HemaSphere 2020, 4, 2. [Google Scholar] [CrossRef] [PubMed]
- Milani, P.; Schönland, S.; Merlini, G.; Kimmich, C.; Foli, A.; Dittrich, T.; Basset, M.; Müller-Tidow, C.; Bochtler, T.; Palladini, G.; et al. Treatment of AL amyloidosis with bendamustine: a study of 122 patients. Blood 2018, 132, 1988–1991. [Google Scholar] [CrossRef]
- Chakraborty, R.; Milani, P.; Palladini, G.; Gertz, M. Role of autologous haematopoietic cell transplantation in the treatment of systemic light chain amyloidosis in the era of anti-CD38 monoclonal antibodies. Lancet Haematol. 2023, 10, e936–940. [Google Scholar] [CrossRef]
- Jelinek, T.; Kufova, Z.; Hajek, R. Immunomodulatory drugs in AL amyloidosis. Crit. Rev. Oncol. Hematol. 2016, 99, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Javed, S.; Iqtidar, T.; Fatima, H.; Hashim, S.; Rehan, T.; Maaz, S.; Musa, M.; Zaka, M.; Neupane, K.; Khawar, M.; et al. Efficacy and Safety Profile of Proteasome Inhibitor Based Drug Regimens for Treatment of NewlyDiagnosed AL Amyloidosis: A Systematic Review. Blood 2020, 136 (Suppl.1), 31. [Google Scholar] [CrossRef]
- Mikhael, J.R.; Schuster, S.R.; Jimenez-Zepeda, V.H.; Bello, N.; Spong, J.; Reeder, C.B.; Stewart, A.K.; Bergsagel, P.L.; Fonseca, R. Cyclophosphamide-bortezomib-dexamethasone (CyBorD) produces rapid and complete hematologic response in patients with AL amyloidosis. Blood 2012, 119, 4391–4394. [Google Scholar] [CrossRef]
- Godara, A.; Palladini, G. Monoclonal Antibody Therapies in Systemic Light-Chain Amyloidosis. Hematol. Oncol. Clin. N. Am. 2020, 34, 1145–1159. [Google Scholar] [CrossRef]
- Leong, S.; Pui, H.; Kirkham, Z.; Popat, R. Antibody drug conjugates for the treatment of multiple myeloma. Am. J. Hematol. 2022, 98, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Wechalekar, A.D.; Sanchorawala, V. Daratumumab in AL amyloidosis. Blood 2022, 140, 2317–2322. [Google Scholar] [CrossRef]
- Kastritis, E.; Palladini, G.; Minnema, M.C.; Wechalekar, A.D.; Jaccard, A.; Lee, H.C.; Sanchorawala, V.; Gibbs, S.; Mollee, P.; Venner, C.P.; et al. Daratumumab-Based Treatment for Immunoglobulin Light-Chain Amyloidosis. N. Engl. J. Med. 2021, 385, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Parker, T.L.; Rosenthal, A; Sanchorawala, V.; Landau, H.J.; Campagnaro, E.L.; Kapoor, P.; Neparidze, N.; Girnius, S.; 7 Hagen, P.; Scott, E.C.; et al. Isatuximab for relapsed and/or refractory AL amyloidosis: results of a prospective phase 2 trial (SWOG S1702). Blood 2025, 146, 2507–2516. [Google Scholar] [CrossRef]
- Dittrich, T.; Hansen, T; Kimmich, C.R.; Veelken, K.; Jauch, A.; Raab, M.S.; Müller-Tidow, C.; Hegenbart, U.; Schönland, S.O. Elotuzumab in Combination With Dose Reduced IMiDs and Dexamethasone for AL Amyloidosis Patients With Relapsed/Refractory Plasma Cell Dyscrasia and Advanced Organ Involvement. Am. J. Hematol. 2025, 100, 1098–1101. [Google Scholar] [CrossRef]
- Kastritis, E. BCMA: BeCoMing a new hope for AL amyloidosis. Blood 2025, 146, 1874–1875. [Google Scholar] [CrossRef] [PubMed]
- Jamroziak, K.; Zielonka, K.; Khwaja, J.; Wechalekar, A.D. Update on B-cell maturation antigen-directed therapies in AL amyloidosis. Br. J. Haematol. 2025, 206, 817–831. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Godara, A.; Pan, S.; Toskic, D.; Fogaren, T.; Sborov, D.W.; Comenzo, R.; Kansagra, A. Belantamab Mafadotin in Patients with Relapsed/Refractory AL Amyloidosis with Myeloma. Blood 2021, 138, 1670–1672. [Google Scholar] [CrossRef]
- Leung, N.; Chapman, J.A.; Bhatia, S. First report of teclistamab in a patient with relapsed AL amyloidosis and multiple mieloma. e. J. Haem. 2023, 4, 1157–1159. [Google Scholar] [CrossRef]
- Vianna, P.; Chakraborty, R.; Hossain, S.; Bhutani, D.; Miller, S.; Rossi, A.; Cuddy, S.A.M.; Falk, R.H.; Lentzsch, S.; Laubach, J.; et al. Safety and efficacy of elranatamab in patients with daratumumab relapsed and/or refractory immunoglobulin light-chain amyloidosis. Blood 2025, 146, 1929–1935. [Google Scholar] [CrossRef]
- Chakraborty, R.; Kastritis, E.; Huart, A.; Jaccard, A.; Landau, H.; Iida, S.; Motorna, O.; Mollee, P.; Ishida, T.; Kawano, Y.; et al. Phase 1/2 dose escalation and expansion study of etentamig in patients with relapsed or refractory light chain. Blood 2025, 146, 692–693. [Google Scholar] [CrossRef]
- Lewis, E; Jimenez-Zepeda, V.H. BCMA CAR-T: From Multiple Myeloma to Light-Chain Amyloidosis. Curr. Oncol. 2025, 32, 418. [Google Scholar] [CrossRef]
- Lebel, L; Asherie, N.; Kfir-Erenfeld, S.; Grisariu, S.; Avni, B.; Elias, S.; Assayag, M.; Dubnikov-Sharon, T.; Pick, M.; Alexander-Shani, R.; et al. Efficacy and Safety of Anti–B-Cell Maturation Antigen Chimeric Antigen Receptor T-Cell for the Treatment of Relapsed and Refractory AL Amyloidosis. J. Clin. Oncol. 2024, 43, 2007–2016. [Google Scholar] [CrossRef]
- Landau, H.J.; Hughes, C.; Rosenberg, A.S.; Abedi, M.; Raza, S.; Zonder, J.A.; Brailovski, E.; Liu, J. Safety and efficacy data from Nexicart-2, the first US trial of CAR-T in R/R light chain (AL) amyloidosis, NXC-201. J. Clin. Oncol. 2025, 43, 7508. [Google Scholar] [CrossRef]
- Tan, M.S.Y.; Warsame, R.; Parrondo, R.; Muchtar, E.; Kourelis, T.; Buadi, F.; Gonsalves, W.; Cook, J.; Kapoor, P.; Hayman, S.; et al. AL Amyloidosis: A Real-World Experience with CAR-T Cell Therapy. Blood Adv. 2025. [Google Scholar] [CrossRef]
- Goel, U.; Dima, D.; Davis, J.; Ahmed, N.; Shaikh, H.; Lochner, J.; Abdallah, A.O.; Khouri, J.; Hashmi, H.; Anwer, F. Safety and efficacy of B cell maturation antigen-directed CAR T-cell therapy in patients with relapsed/refractory multiple myeloma and concurrent light chain amyloidosis. Eur. J. Haematol. 2024, 113, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Rees, M.; Cassano, R.; Tan, M.; Zolotov, E; Sidana, S.; Dima, D.; Kort, J.; Afrough, A.; Gaballa, M.; Pasvolsky, O.; et al. The real-world safety and efficacy of BCMA-directed chimeric antigen receptor T-cell therapy in systemic AL amyloidosis. Blood 2025, 146, 2181–2182. [Google Scholar] [CrossRef]
- Oliver-Caldes, A.; Jiménez, R.; Español-Rego, M.; Cibeira, M.T.; Ortiz-Maldonado, V.; Quintana, L.F.; Castillo, P.; Guijarro, F.; Tovar, N.; Montoro, M.; et al. First report of CAR-T therapy in AL amyloidosis and relapsed/refractory multiple myeloma. J. Immunother. Cancer 2021, 9, e003783. [Google Scholar] [CrossRef]
- van de Donk, N.W.C.J.; Vega, G.; Perrot, A.; Anguille, S.; Oriol, A.; Minnema, M.; Kaiser, M.F.; Lee, H.C.; Garfall, A.; Matous, J.V.; et al. First-in-human study of JNJ-79635322 (JNJ-5322), a novel, next-generation trispecific antibody (TsAb), in patients (pts) with relapsed/refractory multiple myeloma (RRMM): Initial phase 1 results. J. Clin. Oncol. 2025, 43, 7505. [Google Scholar] [CrossRef]
- Richardson, P.G.; Barlogie, B.; Berenson, J.; Singhal, S.; Jagannath, S.; Irwin, D.; Rajkumar, S.V.; Srkalovic, G.; Alsina, M.; Alexanian, R.; et al. A Phase 2 Study of Bortezomib in Relapsed, Refractory Myeloma. N. Engl. J. Med. 2003, 348, 2609–261. [Google Scholar] [CrossRef]
- Jagannath, S.; Durie, B.G.M.; Wolf, J.; Camacho, E.; Irwin, D.; Lutzky, J.; McKinley, M.; Gabayan, E.; Mazumder, A.; Schenkein, D.; et al. Bortezomib therapy alone and in combination with dexamethasone for previously untreated symptomatic multiple mieloma. Br. J. Haematol. 2005, 129, 776–783. [Google Scholar] [CrossRef]
- Harousseau, J.L.; Attal, M.; Leleu, X.; Troncy, J.; Pegourie, B.; Stoppa, A.M.; Hulin, C.; Benboubker, L.; Fuzibet, J.G.; Renaud, M.; et al. Bortezomib plus dexamethasone as induction treatment prior to autologous stem cell transplantation in patients with newly diagnosed multiple myeloma: results of an IFM phase II study. Haematologica 2006, 91, 1498–1505. [Google Scholar]
- Rosiñol, L.; Oriol, A.; Mateos, M.V.; Sureda, A.; García-Sánchez, P.; Gutiérrez, N.; Alegre, A.; Lahuerta, J.J.; de la Rubia, J.; Herrero, C.; et al. Phase II Pethema Trial of Alternating Bortezomib and Dexamethasone As Induction Regimen Before Autologous Stem-Cell Transplantation in Younger Patients With Multiple Myeloma: Efficacy and Clinical Implications of Tumor Response Kinetics. J. Clin. Oncol. 2007, 25, 4452–4458. [Google Scholar] [CrossRef]
- Harousseau, J.L.; Attal, M.; Avet-Loiseau, H.; Marit, G.; Caillot, D.; Mohty, M.; Lenain, P.; Hulin, C.; Facon, T.; Casassus, P.; et al. Bortezomib Plus Dexamethasone Is Superior to Vincristine Plus Doxorubicin Plus Dexamethasone As InductionTreatment Prior to Autologous Stem-Cell Transplantation in Newly Diagnosed Multiple Myeloma: Results of the IFM 2005-01 Phase III Trial. J. Clin. Oncol. 2010, 28, 4621–4629. [Google Scholar] [CrossRef]
- Girnius, S.K.; Lee, S.; Kambhampati, S.; Rose, M.G.; Mohiuddin, A.; Houranieh, A.; Zimelman, A.; Grady, T.; Mehta, P.; Behler, C.; et al. A Phase II trial of weekly bortezomib and dexamethasone in veterans with newly diagnosed multiple myeloma not eligible for or who deferred autologous stem cell transplantation. Br. J. Haematol. 2015, 169, 36–43. [Google Scholar] [CrossRef]
- Niesvizky, R.; Flinn, I.W.; Rifkin, R.; Gabrail, N.; Charu, V.; Clowney, B.; Essell, J.; Gaffar, Y.; Warr, T.; Neuwirth, R.; et al. Community-Based Phase IIIB Trial of Three UPFRONT Bortezomib-Based Myeloma Regimens. J. Clin. Oncol. 2015, 33, 3921–3929. [Google Scholar] [CrossRef] [PubMed]
- Kastritis, E.; Anagnostopoulos, A.; Roussou, M.; Toumanidis, S.; Pamboukas, C.; Migkou, M.; Tassidou, A.; Xilouri, I.; Delibasi, S.; Psimenou, E.; et al. Treatment of light chain (AL) amyloidosis with the combination of bortezomib and dexamethasone. Haematologica 2007, 92, 1351–1358. [Google Scholar] [CrossRef]
- Huang, X.; Wang, Q.; Chen, W.; Zeng, C.; Chen, Z.; Gong, D.; Zhang, H.; Liu, Z. Induction therapy with bortezomib andexamethasone followed by autologous stem cell transplantation versus autologous stem cell transplantation alone in the treatment of renal AL amyloidosis: a randomized controlled trial. BMC Med. 2014, 12, 2. Available online: http://www.biomedcentral.com/1741-7015/12/2. [CrossRef]
- Sanchorawala, V.; Brauneis, D.; Shelton, A.C.; Lo, S.; Sun, F.; Sloan, J.M.; Quillen, K.; Seldin, D.C. Induction Therapy with Bortezomib Followed by Bortezomib-High Dose Melphalan and Stem Cell Transplantation for Light Chain Amyloidosis: Results of a Prospective Clinical Trial. Biol. Blood Marrow Transplant. 2015, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- Minnema, M.C.; Nasserinejad, K.; Hazenberg, B.; Hegenbart, U.; Vlummens, P.; Ypma, P.F.; Kröger, N.; Wu, K.L.; Kersten, M.J.; Schaafsma, M.R.; et al. Bortezomib-based induction followed by stem cell transplantation in light chain amyloidosis: results of the multicenter HOVON 104 trial. Haematologica 2019, 104, 2274–2282. [Google Scholar] [CrossRef] [PubMed]
- Landau, H.; Lahoud, O.; Devlin, S.; Lendvai, N.; Chung, D.J.; Dogan, A.; Landgren, C.O.; Giralt, S.; Hassoun, H. Pilot Study of Bortezomib and Dexamethasone Pre- and Post-Risk-Adapted Autologous Stem Cell Transplantation in AL Amyloidosis. Biol. Blood Marrow Transplant. 2020, 204–208. [Google Scholar] [CrossRef]
- Jakubowiak, A.J.; Kendall, T.; Al-Zoubi, A.; Khaled, Y.; Mineishi, S.; Ahmed, A.; Campagnaro, E.; Brozo, C.; Braun, T.; Talpaz, M.; Kaminski, M.S. Phase II Trial of Combination Therapy With Bortezomib, Pegylated Liposomal Doxorubicin, and Dexamethasone in Patients With Newly Diagnosed Myeloma. J. Clin. Oncol. 2009, 27, 5015–5022. [Google Scholar] [CrossRef]
- Palumbo, A.; Gay, F.; Falco, P.; Crippa, C.; Montefusco, V.; Patriarca, F.; Rossini, F.; Caltagirone, S.; Benevolo, G.; Norbert Pescosta, N.; et al. Bortezomib As Induction Before Autologous Transplantation, Followed by Lenalidomide As Consolidation-Maintenance in Untreated Multiple Myeloma Patients. J. Clin. Oncol. 2010, 28, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Sonneveld, P.; Schmidt-Wolf, I.G.H.; van der Holt, B.; el Jarari, L.; Bertsch, U.; Salwender, H.; Zweegman, S.; Vellenga, E.; Broyl, A.; Blau, I.W.; et al. Bortezomib Induction and Maintenance Treatment in Patients With Newly Diagnosed Multiple Myeloma: Results of the Randomized Phase III HOVON-65/GMMG-HD4 Trial. J. Clin. Oncol. 2012, 30, 2946–2955. [Google Scholar] [CrossRef]
- San Miguel, J.F.; Schlag, R.; Khuageva, N.K.; Dimopoulos, M. A.; Shpilberg, O.; Kropff, M.; Spicka, I.; Petrucci, M.T.; Palumbo, A.; Samoilova, O.S.; et al. Bortezomib plus Melphalan and Prednisone for Initial Treatment of Multiple Myeloma. N. Engl. J. Med. 2008, 359, 906–917. [Google Scholar] [CrossRef] [PubMed]
- Mateos, M.V.; Oriol, A.; Martínez-López, J.; Gutiérrez, N.; Teruel, A.I.; de Paz, R.; García-Laraña, J.; Bengoechea, B.; Martín, A.; Díaz Mediavilla, J.; et al. Bortezomib, melphalan, and prednisone versus bortezomib, thalidomide, and prednisone as induction therapy followed by maintenance treatment with bortezomib and thalidomide versus bortezomib and prednisone in elderly patients with untreated multiple myeloma: a randomised trial. Lancet Oncol. 2010, 11, 934–941. [Google Scholar] [CrossRef]
- Palumbo, A.; Bringhen, S.; Rossi, D.; Cavalli, M.; Larocca, A.; Ria, R.; Offidani, M.; Patriarca, F.; Nozzoli, C.; Guglielmelli, T.; et al. Bortezomib-Melphalan-Prednisone-Thalidomide Followed by Maintenance With Bortezomib-Thalidomide Compared With Bortezomib-Melphalan-Prednisone for Initial Treatment of Multiple Myeloma: A Randomized Controlled Trial. J. Clin. Oncol. 2010, 28, 5101–5109. [Google Scholar] [CrossRef]
- Mateos, M.V.; Martínez-López, J.; Hernández, M-T.; Ocio, E.M.; Rosiñol, L.; Martínez, R.; Teruel, A.-I.; Gutiérrez, N.C.; Martín Ramos, M.L.; Oriol, A.; et al. Sequential vs alternating administration of VMP and Rd in elderly patients with newly diagnosed MM. Blood 2016, 127, 420–425. [Google Scholar] [CrossRef]
- Mateos, M.V.; Paiva, B.; Cedena, M.T.; Puig, N.; Sureda-Balari, A.M.; González de la Calle, V.; Oriol, A.; Ocio, E.M.; Rosiñol, L.; González Montes, Y.; et al. Induction therapy with bortezomib, melphalan, and prednisone followed by lenalidomide and dexamethasone versus carfilzomib, lenalidomide, and dexamethasone with or without daratumumab in older, fit patients with newly diagnosed multiple myeloma (GEM-2017FIT): a phase 3, open-label, multicentre, randomised clinical trial. Lancet Haematol. 2025, 12, e588–e598. [Google Scholar] [CrossRef]
- Kastritis, E.; Leleu, X.; Arnulf, B.; Zamagni, E.; Cibeira, M.T.; Kwok, F.; Mollee, P.; Hájek, R.; Moreau, P.; Jaccard, A.; et al. Bortezomib, Melphalan, and Dexamethasone for Light-Chain Amyloidosis. J. Clin. Oncol. 2020, 38, 3252–3260. [Google Scholar] [CrossRef] [PubMed]
- Reeder, C.B.; Reece, D.E.; Kukreti, V.; Chen, C.; Trudel, S.; Hentz, J.; Noble, B.; Pirooz, N.A.; Spong, J.E.; Piza, J.G.; et al. Cyclophosphamide, bortezomib and dexamethasone induction for newly diagnosed multiple myeloma: high response rates in a phase II clinical trial. Leukemia 2009, 23, 1337–1341. [Google Scholar] [CrossRef]
- Bensinger, W.I.; Jagannath, S.; Vescio, R.; Camacho, E.; Wolf, J.; Irwin, D.; Capo, G.; McKinley, M.; Potts, P.; Vesole, D.H.; et al. Phase 2 study of two sequential three-drug combinations containing bortezomib, cyclophosphamide and dexamethasone, followed by bortezomib, thalidomide and dexamethasone as frontline therapy for multiple myeloma. Br. J. Haematol. 2010, 148, 562–568. [Google Scholar] [CrossRef]
- Kumar, S.; Flinn, I.; Richardson, P.G.; Hari, P.; Callander, N.; Noga, S.J.; Stewart, A.K.; Turturro, F.; Rifkin, R.; Wolf, J.; et al. Randomized, multicenter, phase 2 study (EVOLUTION) of combinations of bortezomib, dexamethasone, cyclophosphamide, and lenalidomide in previously untreated multiple myeloma. Blood 2012, 119, 4375–4382. [Google Scholar] [CrossRef]
- Mai, E.K.; Bertsch, U.; Dürig, J.; Kunz, C.; Haenel, M.; Blau, I.W.; Munder, M.; Jauch, A.; Schurich, B.; Hielscher, T.; et al. Phase III trial of bortezomib, cyclophosphamide and dexamethasone (VCD) versus bortezomib, doxorubicin and dexamethasone (PAd) in newly diagnosed myeloma. Leukemia 2015, 1721–1729. [Google Scholar] [CrossRef]
- Moreau, P.; Hulin, C.; Macro, M.; Caillot, D.; Chaleteix, C.; Roussel, M.; Garderet, L.; Royer, B.; Brechignac, S.; Tiab, M.; et al. VTD is superior to VCD prior to intensive therapy in multiple myeloma: results of the prospective IFM2013-04 trial. Blood 2016, 127(21), 2569–2574. [Google Scholar] [CrossRef]
- Einsele, H.; Engelhardt, M.; Tapprich, C.; Müller, J.; Liebisch, P.; Langer, C.; Kropff, M.; Mügge, L.O.; Jung, W.; Wolf, H.H.; et al. Phase II study of bortezomib, cyclophosphamide and dexamethasone as induction therapy in multiple myeloma: DSMM XI trial. Br. J. Haematol. 2017, 179, 586–597. [Google Scholar] [CrossRef]
- Tanaka, K.; Toyota, S.; Akiyama, M.; Wakimoto, N.; Nakamura, Y.; Najima, Y.; Doki, N.; Kakihana, K.; Igarashi, A.; Kobayashi, T.; et al. Efficacy and Safety of a Weekly Cyclophosphamide-Bortezomib-Dexamethasone Regimen as Induction Therapy Prior to Autologous Stem Cell Transplantation in Japanese Patients with Newly Diagnosed Multiple Myeloma: A Phase 2 Multicenter Trial. Acta Haematol. 2019, 141, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Shen, K.-n.; Fu, W.-j.; Wu, Y.; Dong, Y.-j.; Huang, Z.-x.; Wei, Y.-q.; Li, C.r.; Sun, C.-y.; Chen, Y.; Miao, H.-l.; et al. Doxycycline Combined With Bortezomib-Cyclophosphamide-Dexamethasone Chemotherapy for Newly Diagnosed Cardiac Light-Chain Amyloidosis: A Multicenter Randomized Controlled Trial. Circulation 2022, 145, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Palladini, G.; Sachchithanantham, S.; Milani, P.; Gillmore, J.; Foli, A.; Lachmann, H.; Basset, M.; Hawkins, P.; Merlini, G.; Wechalekar, A.D. A European collaborative study of cyclophosphamide, bortezomib, and dexamethasone in upfront treatment of systemic AL amyloidosis. Blood 2015, 126, 612–615. [Google Scholar] [CrossRef]
- Berdeja, J.; Savona, M.; Chu, L.; Essell, J.; Murphy, P.; Bauer, T.; Raefsky, E.; Boccia, R.V.; Flinn, I. Bendamustine, Bortezomib and Dexamethasone (BBD) As First-Line Treatment Of Patients (Pts) With Multiple Myeloma Who Are Not Candidates For High Dose Chemotherapy. Blood 2013, 122, 3193. [Google Scholar] [CrossRef]
- Mateos, M.V.; Oriol, A.; Rosiñol, L.; de Arriba, F.; Puig, N.; Martín, J.; Martínez-López, J.; Echeveste, M.A.; Sarrá, J.; Ocio, E.; et al. Bendamustine, bortezomib and prednisone for the treatment of patients with newly diagnosed multiple myeloma: results of a prospective phase 2 Spanish/PETHEMA trial. Haematologica 2013, 100, 1096–1102. [Google Scholar] [CrossRef] [PubMed]
- Cavo, M.; Tacchetti, P.; Patriarca, F.; Petrucci, M.T.; Pantani, L.; Galli, M.; Di, R.F.; Crippa, C.; Zamagni, E.; Palumbo, A.; et al. Bortezomib with thalidomide plus dexamethasone compared with thalidomide plus dexamethasone as induction therapy before, and consolidation therapy after, double autologous stem-cell transplantation in newly diagnosed multiple myeloma: a randomised phase 3 study. The Lancet 2010, 376, 2075–2085. [Google Scholar] [CrossRef]
- Rosiñol, L.; Oriol, A.; Teruel, A.I.; de la Guía, A.L.; Blanchard, M.J.; de la Rubia, J.; Granell, M.; Sampol, M.A.; Palomera, L.; González, Y.; et al. Bortezomib and thalidomide maintenance after stem cell transplantation for multiple myeloma: a PETHEMA/GEM trial. Leukemia 2017, 31, 1922–1927. [Google Scholar] [CrossRef]
- Ludwig, H.; Greil, R.; Masszi, T.; Spicka, I.; Shpilberg, O.; Hajek, R.; Dmoszynska, A.; Paiva, B.; Vidriales, M.B.; Esteves, G.; et al. Bortezomib, thalidomide and dexamethasone, with or without cyclophosphamide, for patients with previously untreated multiple myeloma: 5-year follow-up. Br. J. Haematol. 2015, 171, 344–354. [Google Scholar] [CrossRef]
- Durie, B.G.M.; Hoering, A.; Abidi, M.H.; Rajkumar, S.V.; Epstein, J.; Kahanic, S.P.; Thakuri, M.; Reu, F.; Reynolds, C.M.; Sexton, R.; et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): a randomised, open-label, phase 3 trial. The Lancet 2017, 389, 519–527. [Google Scholar] [CrossRef]
- Rosiñol, L.; Oriol, A.; Ríos, R.; Sureda, A.; Blanchard, M.J.; Hernández, M.T.; Martínez-Martínez, R.; Moraleda, J.M.; Jarque, I.; Bargay, J.; et al. Bortezomib, lenalidomide, and dexamethasone as induction therapy prior to autologous transplant in multiple myeloma. Blood 2019, 134, 1337–1345. [Google Scholar] [CrossRef]
- Kumar, S.K.; Jacobus, S.J.; Cohen, A.D.; Weiss, M.; Callander, N.; Singh, A.K.; Parker, T.L.; Menter, A.; Yang, X.; Parsons, B.; et al. Carfilzomib or bortezomib in combination with lenalidomide and dexamethasone for patients with newly diagnosed multiple myeloma without intention for immediate autologous stem-cell transplantation (ENDURANCE): a multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol. 2020, 21, 1317–1330. [Google Scholar] [CrossRef]
- Ailawadhi, S.; Hoering, A.; J Ye, C.; Lipe, B.; Chauncey, T.R.; Gowin, K.; Calverley, D.; Holstein, S.A.; Campagnaro, E.L.; Rosenthal, A.; et al. A Phase III Randomized Trial for Frail Newly Diagnosed Multiple Myeloma Patients Comparing Bortezomib- Lenalidomide-Dexamethasone (VRd-Lite followed by Len maintenance) with Daratumumab-Lenalidomide- Dexamethasone (DRd followed by Len+/- Dara Maintenance): SWOG S2209. Blood 2024, 144, 3381–3383. [Google Scholar] [CrossRef]
- Saj, F.; Nisha, Y.; Ganesan, P.; Kayal, S.; Kar, R.; Halanaik, D.; Dubashi, B. Efficacy and safety of pomalidomide, bortezomib, and dexamethasone combination chemotherapy for newly diagnosed multiple myeloma: POMACE Phase II Study. Blood Cancer J. 2023, 13, 45. [Google Scholar] [CrossRef]
- Laubach, J.; Nooka, A.K.; Cole, C.; O'Donnell, E.; Vij, R.; Usmani, S.Z.; Orloff, G.J.; Richter, J.R.; Redd, R.; DiPietro, H.; et al. An open-label, single arm, phase IIa study of bortezomib, lenalidomide, dexamethasone, and elotuzumab in newly diagnosed multiple myeloma. J. Clin. Oncol. 2017, 35, 8002. [Google Scholar] [CrossRef]
- Usmani, S.Z.; Hoering, A.; Ailawadhi, S.; Sexton, R.; Lipe, B.; Hita, S.F.; Valent, J.; Rosenzweig, M.; Zonder, J.A.; Dhodapkar, M.; et al. Bortezomib, lenalidomide, and dexamethasone with or without elotuzumab in patients with untreated, high-risk multiple myeloma (SWOG-1211): primary analysis of a randomised, phase 2 trial. Lancet Hematol. 2021, 8, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Mai, E.K.; Goldschmidt, H.; Miah, K.; Bertsch, U.; Besemer, B.; Hänel, M.; Krzykalla, J.; Fenk, R.; Schlenzka, J.; Munder, M.; et al. Elotuzumab, lenalidomide, bortezomib, dexamethasone, and autologous haematopoietic stem-cell transplantation for newly diagnosed multiple myeloma (GMMG-HD6): results from a randomised, phase 3 trial. Lancet Haematol. 2024, 11, 101–113. [Google Scholar] [CrossRef]
- Nagarajan, C.; Tan, M.; Chen, Y.; Ooi, M.; De Mel, S.; Tso, A.; Ng, L.; Than, H.; Goh, Y.T.; Brian, GM; Durie, B.G.M.; et al. Daratumumab Bortezomib and Dexamethasone in Transplant Ineligible Newly Diagnosed Elderly Myeloma Patients - a Trial By Asian Myeloma Network. Blood 2023, 142, 6721–6723. [Google Scholar] [CrossRef]
- Shen, K.-n.; Gao, Y.-j.; Chang, L.; Zhang, L.; Cao, X.-x.; Tian, Z.; Wang, Y.-n.; Zhou, D.-b.; Li, J. Efficacy and safety of daratumumab plus bortezomib and dexamethasone in newly diagnosed Mayo 2004 stage IIIA or IIIB light-chain amyloidosis: a prospective phase II study. Haematologica 2024, 109, 2355–2358. [Google Scholar] [CrossRef]
- Mateos, M.V.; Dimopoulos, M.A.; Cavo, M.; Suzuki, K.; Jakubowiak, A.; Knop, S.; Doyen, C.; Lucio, P.; Nagy, Z.; Kaplan, P; et al. Daratumumab plus Bortezomib, Melphalan, and Prednisone for Untreated Myeloma. N. Engl. J. Med. 2018, 378, 518–528. [Google Scholar] [CrossRef]
- Yimer, H.; Melear, J.; Faber, E.; Bensinger, W.I.; Burke, J.M.; Narang, M.; Stevens, D.; Gunawardena, S.; Lutska, Y.; Qi, K.; et al. Daratumumab, bortezomib, cyclophosphamide and dexamethasone in newly diagnosed and relapsed multiple myeloma: LYRA study. Br. J. Haematol. 2019, 185, 492–502. [Google Scholar] [CrossRef]
- Beksac, M.; Tuglular, T.; Gay, F.; Mina, R.; Katodritou, E.; Unal, A.; Cavo, M.; Ozsan, G.H.; Van Der Velden, V.H.J.; Beverloo, H.B.; et al. Treatment with Daratumumab Plus Bortezomib, Cyclophosphamide, and Dexamethasone May Result in Both Hematologic and Metabolic Complete Response to Achieve Long-Term Progression Free Survival Among Patients Presenting with Extra-Medullary Disease: A European Myeloma Network Study (EMN19). Blood 2023, 142, 1956–1958. [Google Scholar] [CrossRef]
- Mollee, P.; Reynolds, J.; Janowski, W.; Quach, H.; Campbell, P.; Gibbs, S.; Lee, S.; Lee, E.; Taylor, K.; Cochrane, T.; et al. Daratumumab, cyclophosphamide, bortezomib, and dexamethasone for transplant-ineligible myeloma: AMaRC 03-16. Blood Adv. 2024, 8, 3721–3730. [Google Scholar] [CrossRef] [PubMed]
- Rosenzweig, M.; Efebera, Y.; Kastritis, E.; Blue, B.; Jamal, F.; Minnema, M.C.; Pericone, C.; Vasey, S.; Chen, Y.; Kotoulek, S.; et al. Phase 2 Study of Daratumumab (DARA) Plus Bortezomib, Cyclophosphamide, and Dexamethasone (D-VCd) in a Diverse Patient Population with Newly Diagnosed Amyloid Light Chain (AL) Amyloidosis: Aquarius. Blood 2023, 142, 4785–4787. [Google Scholar] [CrossRef]
- Hagen, P.; Sidana, S.; Parker, T.L.; Walker, B.A.; Sanchorawala, V.; Zonder, J.A.; Kourelis, T.; D’Souza, A.; Landau, H.J.; Rosenthal, A.; et al. A Phase III, Randomized Study of Daratumumab, Cyclophosphamide, Bortezomib and Dexamethasone (DARA-VCD) Induction Followed By Autologous Stem Cell Transplant or Dara-VCD Consolidation and Daratumumab Maintenance in Patients with Newly Diagnosed AL Amyloidosis. Blood 2024, 144, 3309.1–3309.2. [Google Scholar] [CrossRef]
- Roussel, M.; Moreau, P.; Hebraud, B.; Laribi, K.; Jaccard, A.; Dib, M.; Slama, B.; Dorvaux, V.; Royer, B.; Frenzel, L.; et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab for transplantation-eligible patients with newly diagnosed multiple myeloma (CASSIOPEIA): health-related quality of life outcomes of a randomised, open-label, phase 3 trial. Lancet Haematol. 2020, 7, e874-883. [Google Scholar] [CrossRef] [PubMed]
- Voorhees, P.M.; Sborov, D.W.; Laubach, J.; Kaufman, J.L.; Reeves, B.; Rodriguez, C.; Chari, A.; Silbermann, R.; Costa, L.J.; Anderson, L.D., Jr.; et al. Addition of daratumumab to lenalidomide, bortezomib, and dexamethasone for transplantation-eligible patients with newly diagnosed multiple myeloma (GRIFFIN): final analysis of an open-label, randomised, phase 2 trial. Lancet Haematol. 2023, 10, e825-837. [Google Scholar] [CrossRef] [PubMed]
- Sonneveld, P.; Dimopoulos, M.A.; Boccadoro, M.; Quach, H.; Ho, P.J.; Beksac, M.; Hulin, C.; Antonioli, E.; Leleu, X.; Mangiacavalli, S.; et al. Daratumumab, Bortezomib, Lenalidomide, and Dexamethasone for Multiple Myeloma. N. Engl. J. Med. 2024, 390, 301–313. [Google Scholar] [CrossRef]
- Usmani, S.Z.; Facon, T.; Hungria, V.; Bahlis, N.J.; Venner, C.P.; Marc Braunstein, M.; Ludek Pour, L.; Martí, J.M.; Basu, S.; Cohen, Y.C.; et al. Daratumumab plus bortezomib, lenalidomide and dexamethasone for transplant-ineligible or transplant-deferred newly diagnosed multiple myeloma: the randomized phase 3 CEPHEUS trial. Nat. Med. 2025, 31, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.F.; Hall, A.; Walker, K.; Sherborne, A.; De Tute, R.M.; Newnham, N.; Roberts, S.; Ingleson, E.; Bowles, K.; Garg, M.; et al. Daratumumab, Cyclophosphamide, Bortezomib, Lenalidomide, and Dexamethasone as Induction and Extended Consolidation Improves Outcome in Ultra-High-Risk Multiple Myeloma. J. Clin. Oncol. 2023, 41, 3945–3955. [Google Scholar] [CrossRef]
- Goldschmidt, H.; Mai, E.K.; Bertsch, U.; Fenk, R.; Nievergall, E.; Tichy, D.; Besemer, B.; Dürig, J.; Schroers, R.; von Metzler, I.; et al. Addition of isatuximab to lenalidomide, bortezomib, and dexamethasone as induction therapy for newly diagnosed, transplantation-eligible patients with multiple myeloma (GMMG-HD7): part 1 of an open-label, multicentre, randomised, active-controlled, phase 3 trial. Lancet Haematol. 2022, 9, e810-821. [Google Scholar] [CrossRef]
- Facon, T.; Dimopoulos, M.A.; Leleu, X.P.; Beksac, M.; Pour, L.; Hájek, R.; Liu, Z.; Jiri Minarik, J.; Moreau, P.; Romejko-Jarosinska, J.; et al. Isatuximab, Bortezomib, Lenalidomide, and Dexamethasone for Multiple Myeloma. N. Engl. J. Med. 2024, 391, 1597–1609. [Google Scholar] [CrossRef] [PubMed]
- Leleu, X.; Hulin, C.; Lambert, J.; Bobin, A.; Perrot, A.; Karlin, L.; Roussel, M.; Montes, L.; Cherel, B.; Chalopin, T.; et al. Isatuximab, lenalidomide, dexamethasone and bortezomib in transplant-ineligible multiple myeloma: the randomized phase 3 BENEFIT trial. Nat. Med. 2024, 30, 2235–2241. [Google Scholar] [CrossRef]
- Askeland, F.B.; Haukås, E.; Slørdahl, T.S.; Klostergaard, A.; Alexandersen, T.; Osnes, L.; Lysén, A.; Abdollahi, P.; Nielsen, L.K.; Hermansen, E.; et al. Isatuximab, bortezomib, lenalidomide, and limited dexamethasone in patients with transplant-ineligible multiple myeloma (REST): a multicentre, single-arm, phase 2 trial. Lancet Haematol. 2025, 12, e120-127. [Google Scholar] [CrossRef]
Figure 1.
Comparative delay in key bortezomib-based phase II and III trials in newly diagnosed multiple myeloma vs. newly diagnosed systemic light-chain (AL)-amyloidosis. C: cyclophosphamide, D: daratumumab, d: dexamethasone, IT: immunotherapy era, M: melphalan, NA: new agents' era. QT: chemotherapy era, V: bortezomib.
Figure 1.
Comparative delay in key bortezomib-based phase II and III trials in newly diagnosed multiple myeloma vs. newly diagnosed systemic light-chain (AL)-amyloidosis. C: cyclophosphamide, D: daratumumab, d: dexamethasone, IT: immunotherapy era, M: melphalan, NA: new agents' era. QT: chemotherapy era, V: bortezomib.
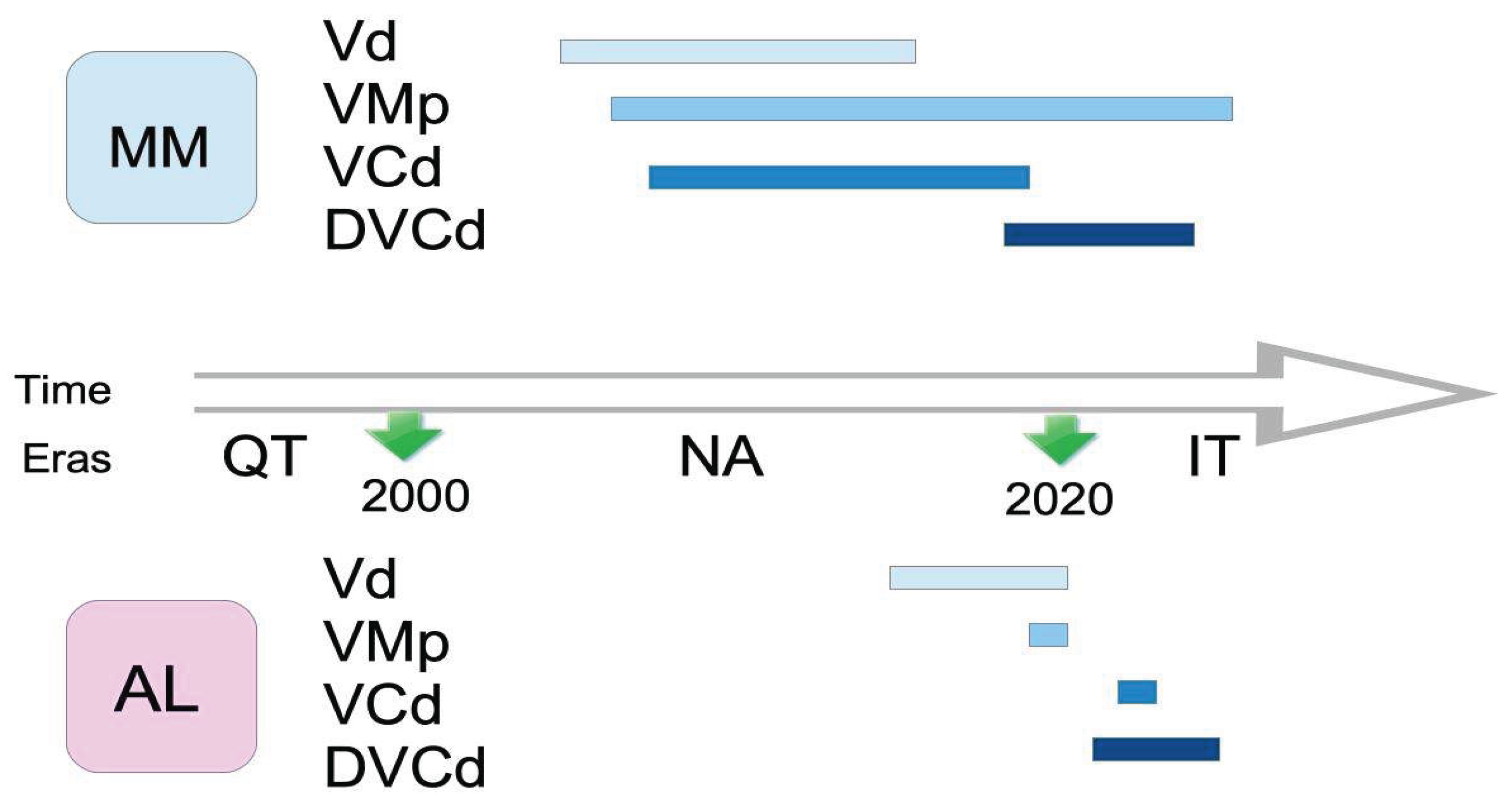

Table 1.
Comparative evolution of bortezomib-based phase II/III trials in newly diagnosed multiple myeloma vs. newly diagnosed light-chain (AL) amyloidosis.
Table 1.
Comparative evolution of bortezomib-based phase II/III trials in newly diagnosed multiple myeloma vs. newly diagnosed light-chain (AL) amyloidosis.
| Anti-clonal therapy |
NDMM |
NDAL |
||||||
| Year/ Authors |
Study | n | Name | Year/ Author |
Study | n | Name | |
| Vd | 2005 Jagannath S et al. [53] |
Phase II |
32 | - | 2014 Huang X et al. [60] |
Phase III Vdx2 & ASCT/ASCT |
28/28 | NCT01998503 |
| 2006 Harousseau JL et al. [54] |
Phase II |
48 | - | 2015 Sanchorawala V et al. [61] |
Phase II | 25 | NCT01083316 | |
| 2007 Rosiñol L et al. [55] |
Phase II |
40 | - | 2019 Minnema MC et al. [62] |
Phase II | 50 | HOVON 104 NTR3220 |
|
| 2010 Harousseau JL et al. [56] |
Phase III Vd/vAd |
121/121 | IFM 2005-01 | 2020 Landau H et al. [63] |
Phase II | 19 | NCT01383759 | |
| 2015 Girnius SK et al. [57] |
Phase II | 50 | NCT01090921 | - | ||||
| 2015 Niesvizky R et al. [58] |
Phase III Vd/VTd/VMp |
168/167/167 | UPFRONT NCT00507416 |
- | ||||
| VAd | 2009 Jakubowiak AJ et al. [64] |
Phase II | 40 | - | - | |||
| 2010 Palumbo A et al. [65] |
Phase II | 102 | - | - | ||||
| 2012 Sonneveld P et al. [66] |
Phase III VAd/vAd |
413/414 | HOVON-65/ GMMG-HD4 |
- | ||||
| VMp/VMd | 2008 San Miguel JF et al. [67] |
Phase III VMp/Mp |
344/338 | VISTA NCT00111319 |
2020 Kastritis E et al. [72] |
Phase III VMd/Md |
53/56 | EMN-03 NCT01277016 |
| 2010 Mateos MV et al. [68] |
Phase III VMp/VTp |
130/130 | GEM05 NCT00443235 |
- | ||||
| 2010 Palumbo A et al. [69] |
Phase III VMp/VMpT |
257/254 | GIMEMA-MM-03-05 NCT01063179 |
- | ||||
| 2016 Mateos MV et al. [70] |
Phase II VMp/Rd seq vs alt |
118/115 | GEM2010 NCT01237249 |
- | ||||
| 2025 Mateos MV et al. [71] |
Phase III VMp-Rd/KRd/ DKRd |
154/154/153 | GEM-2017FIT NCT03742297 |
- | ||||
| VCd | 2009 Reeder CB et al. [73] |
Phase II |
33 | - | 2022 Shen K-n et al. [80] |
NR VCd/VCddox |
55/56 | NCT03401372 |
| 2010 Bensinger WI et al. [74] |
Phase II VCd /VTd seq |
44 | - | - | ||||
| 2012 Kumar S et al. [75] |
Phase II VCd/VCd mod /VRd/VRCd |
33/17/42/48 | EVOLUTION NCT00507442 |
- | ||||
| 2015 Mai EK et al. [76] |
Phase III VCd/VAd |
251/251 | MM5-GMMG | - | ||||
| 2016 Moreau P et al. [77] |
Phase III VCd/VTd |
170/170 | IFM 2013-14 NCT01564537 |
- | ||||
| 2017 Einsele H et al. [78] |
Phase II |
414 | DSMM XI NCT00833560 |
- | ||||
| 2019 Tanaka et al. [79] | Phase II |
38 | - | - | ||||
| BVp | 2013 Berdeja J et al. [82] |
Phase II |
43 | - | - | |||
| 2015 Mateos MV et al. [83] |
Phase II |
60 | NCT01376401 | - | ||||
| VTd | 2010 Cavo M et al. [84] |
Phase III VTd/Td |
241/239 | NCT01134484 | - | |||
| 2012 Rosiñol L et al. [85] |
Phase III VTd/Td/QT+V |
56/56/57 | NCT00461747 | - | ||||
| 2015 Ludwig H et al. [86] |
Phase II VTd/VTCd |
49/49 | NCT00531453 | - | ||||
| VRd | 2017 Durie BGM et al. [87] |
Phase III VRd/Rd |
235/225 | SWOG S0777 NCT00644228 |
- | |||
| 2019 Rosiñol L et al. [88] |
Phase III |
458 | GEM2012 NCT01916252 |
- | ||||
| 2020 Kumar S et al. [89] |
Phase III VRd/KRd |
542/545 | ENDURANCE NCT01863550 |
- | ||||
| 2024 Ailawadhi S et al. [90] |
Phase III VRd/DRd |
459 | SWOG S2209 NCT05561387 |
- | ||||
| PVd | 2023 Saj F et al. [91] |
Phase II |
34 | POMACE | - | |||
| EloVRd | 2017 Laubach J et al. [92] |
Phase II |
41 | NCT02375555 | - | |||
| 2021 Usmani SZ et al. [93] |
Phase II EloVRd/VRd |
48/52 | SWOG-1211 NCT01668719 |
- | ||||
| 2024 Mai EK et al. [94] |
Phase III EloVRd/VRd |
279/280 | GMMG-HD6 NCT02495922 |
- | ||||
| DVd | 2023 Nagarajan C et al. [95] |
Phase II |
27 | AMN006 NCT03695744 |
2024 Shen K-n et al. [96] |
Phase II |
40 | NCT04474938 |
| DVMp | 2018 Mateos MV et al. [97] |
Phase III DVMp/VMp |
350/356 | ALCYONE NCT02195479 |
- | |||
| DVCd | 2019 Yimer et al. [98] |
Phase II |
86 | LYRA NCT02951819 |
2021 Kastritis E et al. [35] |
Phase III DVCd/VCd |
195/193 | ANDROMEDA NCT03201965 |
| 2023 Beksac M et al. [99] |
Phase II |
29 | EMN19 NCT04166565 |
2023 Rosenzweig M et al. [101] |
Phase II DVCd |
75 | AQUARIUS NCT05250973 | |
| 2024 Mollee P et al. [100] |
Phase II DVCd/VCd |
64/57 | AMaRC 03-16 ACTRN12617000202369 | 2024 Hagen P et al. [102] |
Phase III DVCd/DVCd-ASCT |
143/143 | SWOG S2213 NCT06022939 | |
| DVTd | 2020 Roussel M et al. [103] |
Phase III DVTd/VTd |
543/542 | CASSIOPEIA NCT02541383 |
- | |||
| DVRd | 2023 Voorhees PM et al. [104] |
Phase II DVRd/VRd |
104/103 | GRIFFIN NCT02874742 |
- | |||
| 2024 Sonneveld P et al. [105] |
Phase III DVRd/VRd |
355/354 | PERSEUS NCT03710603 |
- | ||||
| 2025 Usmani SZ et al. [106] |
Phase III DVRd/VRd |
197/198 | CEPHEUS NCT03652064 |
- | ||||
| DCVRd | 2023 Kaiser MT et al. [107] |
Phase II |
107 | OPTIMUM (MUKnine) NCT03188172 |
- | |||
| IsaVRd | 2022 Goldschmidt H et al. [108] |
Phase III IsaVRd/VRd |
331/329 | GMMG-HD7 NCT03617731 |
- | |||
| 2024 Facon T et al. [109] |
Phase III IsaVRd/VRd |
265/181 | IMROZ NCT03319667 |
- | ||||
| 2024 Leleu X et al. [110] |
Phase III IsaVRd/IsaRd |
135/135 | BENEFIT NCT04751877 |
- | ||||
| 2025 Askeland FB et al. [111] |
Phase II IsaVRd |
51 | REST NCT04939844 |
- | ||||
A: pegylated liposomal doxorubicin (adriamycin), alt: alternating, B: bendamustine, C: cyclophosphamide, D: daratumumab, d: dexamethasone, dox: doxycycline, Elo: elotuzumab, Isa: istuximab, K: carfilzomib, M: melphalan, mod: modified, NR: not reported, P: pomalidomide, p: prednisone, QT: chemotherapy, R: lenalidomide, seq: sequential, T: thalidomide, V: bortezomib, v: vincristine.
Table 2.
Summary of bortezomib-based phase II/III trials on newly diagnosed multiple myeloma vs. systemic light-chain (AL) amyloidosis.
Table 2.
Summary of bortezomib-based phase II/III trials on newly diagnosed multiple myeloma vs. systemic light-chain (AL) amyloidosis.
| Regimen | n (MM /AL) | Period MM | Period AL |
|---|---|---|---|
| Vd | 6/4 | 2005-2015 | 2014-2020 |
| VAd | 3/0 | 2009-2012 | - |
| VMp/VMd | 5/1 | 2008-2025 | 2020 |
| VCd | 7/1 | 2009-2019 | 2022 |
| BVp | 2/0 | 2013-2015 | - |
| VTd | 3/0 | 2010-2015 | - |
| VRd | 4/0 | 2017-2024 | - |
| PVd | 1/0 | 2023 | - |
| EloVRd | 3/0 | 2017-2024 | - |
| DVd | 1/1 | 2023 | 2024 |
| DVMp | 1/0 | 2018 | - |
| DVCd | 3/3 | 2019-2024 | 2021-2024 |
| DVTd | 1/0 | 2020 | - |
| DVRd | 3/0 | 2023-2025 | - |
| DCVRd | 1/0 | 2023 | - |
| IsaVRd | 4/0 | 2022-2025 | - |
| Total | 48/10 | 2005-2025 | 2014-2024 |
A: pegylated liposomal doxorubicin (adriamycin), alt: alternating, B: bendamustine, C: cyclophosphamide, D: daratumumab, d: dexamethasone, dox: doxycycline, Elo: elotuzumab, Isa: istuximab, K: carfilzomib, M: melphalan, mod: modified, NR: not reported, P: pomalidomide, p: prednisone, QT: chemotherapy, R: lenalidomide, seq: sequential, T: thalidomide, V: bortezomib, v: vincristine.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



