Submitted:
20 January 2026
Posted:
23 January 2026
You are already at the latest version
Abstract
Objective: This systematic review aimed to evaluate the efficacy and safety of preoperative nutrition-based interventions on pre-, intra-, and postoperative outcomes in children undergoing cardiac surgical procedures. Methods: CENTRAL, MEDLINE, and EMBASE were systematically searched for interventional and observational studies comparing any nutritional preoperative intervention with a control or alternative strategy in pediatric patients undergoing cardiac surgery, up to July 2025. The main outcome was postoperative length of stay in the intensive care unit (ICU). The certainty of evidence was assessed using the GRADE approach. Results: Nineteen studies were included (8 randomized controlled trials [RCTs], 1 non-randomized trial, and 10 observational studies), evaluating heterogeneous interventions or exposures, including fatty acids, vitamin D supplementation, and structured preoperative nutritional protocols. Two RCTs demonstrated shorter ICU and hospital stays with extended preoperative nutritional support (2 weeks vs 1 week; n = 40; and 1 month vs no support; n = 80). Observational data indicated an association between preoperative nutritional support and reduced hospital length of stay (meta-analysis of 4 studies; n = 278) as well as fewer days to achieve full enteral feeding postoperatively (meta-analysis of 3 studies; n = 138). No significant difference in postoperative ICU stay was observed between groups (meta-analysis of 2 studies; n = 175). No intervention-related serious adverse events were reported. The overall certainty of evidence was very low. Conclusions: This systematic review provides very low–certainty evidence suggesting that preoperative nutrition-based interventions in children undergoing cardiac surgery are safe and may offer clinical benefits. Substantial heterogeneity across studies underscores the need for well-designed trials and standardized preoperative nutritional protocols.
Keywords:
preoperative nutrition
; congenital heart disease
; children
; malnutrition
; meta-analysis
1. Introduction
Despite the significant advances in pediatric cardiac surgeries for congenital heart defects (CHD), preoperative underweight remains common, affecting an estimated 27.4% of children with CHD (1). A 2019 systematic review reported that malnourished children undergoing surgery for CHD experienced significantly longer hospital and intensive care unit (ICU) stays, as well as mechanical ventilation, compared with well-nourished children (2). These findings highlight the need for early identification of malnutrition in children preparing for cardiac surgery and for individualized nutritional interventions to improve postoperative outcomes.
In adults, a multimodal, multidisciplinary, and evidence-based perioperative concept called Enhanced Recovery After Surgery (ERAS), is widely recognized, as it has been associated with fewer complications, shorter hospital stay, and faster recovery of gastrointestinal function (3, 4). While, in children undergoing abdominal surgery, ERAS protocols have been shown to reduce length of hospital stay, number of postoperative complications, and readmission rate (systematic review of 12 studies) (5), the overall evidence remains limited.
Several guidelines recommend avoiding prolonged fasting prior to surgery to support adequate preoperative nutrition (6-8). Moreover, current expert recommendations highlight the importance of adequate preoperative caloric intake and enteral nutrition in children undergoing cardiac surgeries (9, 10); however, evidence regarding their effect on perioperative outcomes remains limited, and no standardized preoperative nutritional protocol has been established (11).
The aim of this systematic review was to summarize the evidence on the efficacy and safety of preoperative nutrition-based interventions on pre-, intra-, and postoperative outcomes in children undergoing cardiac surgery.
2. Materials and Methods
The protocol of this systematic review was registered in PROSPERO (CRD420251085196). The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines (12) and the Cochrane Handbook for Systematic Review of Interventions, Version 6.4, were followed (13).
2.1. Eligibility Criteria
Type of studies. Interventional trials and observational studies (including cohort, case-control, and cross-sectional) were included, regardless of setting and country income level.
Type of population. The participants were children undergoing any cardiac surgery, regardless of diagnosis (e.g., congenital heart disease) or baseline nutritional status.
Type of intervention and comparators. Studies assessing any nutrition-based preoperative intervention, with or without other intervention components, were considered for this review (11). Although intra- and postoperative interventions were not considered, studies evaluating preoperative nutrition support continued in the postoperative period were included. For observational studies, the exposure of interest was defined as any preoperative nutrition-based intervention. Studies were included regardless of the comparator used (i.e., no intervention/exposure or an alternative intervention/exposure).
Outcomes. The main outcome was defined as total length of intensive care unit stay in the post-operative period, reported as the median/mean number of hours or days during the intervention/ observation period. Secondary outcomes are outlined in Suppl Table S1.
2.2. Search Strategy
The Cochrane Central Register of Controlled Trials (CENTRAL, the Cochrane Library), MEDLINE, and EMBASE were searched from inception to July 2025 using a pre-specified search strategy (for full search strategy, see PROSPERO CRD420251085196). No restrictions regarding language, publication date, geography, or duration of the study were imposed. Manual searches of relevant systematic review articles were also conducted. In addition, the International Clinical Trial Registry Platform (ICTRP, https://trialsearch.who.int/) was also searched manually to identify any ongoing trials.
2.3. Data Collection and Management
Data collection and management were prespecified in the protocol registered in PROSPERO (CRD420251085196). Briefly, three reviewers (AS, PH and MK) independently screened the titles, abstracts, and keywords of all studies identified through the search strategy using EndNote X9 (Version 9.3.3. Philadelphia, The Clarivate Analytics, 2020). Full texts of potentially relevant studies were then retrieved and independently assessed against the eligibility criteria by the reviewers, if required, another review author was consulted (MB, RP and AH).
Two reviewers (AS and PH), using a standardized form, independently extracted pre-specified data in accordance with the registered protocol. To facilitate extraction of study characteristics items, we used ChatGPT-5® Plus (OpenAI®, San Francisco, CA, USA) as a supportive tool. The software was applied solely for the initial drafting of study characteristics using a self-developed data extraction form. All outputs were subsequently verified, corrected, and supplemented by the authors to ensure accuracy and completeness. The authors retained full responsibility for data interpretation, synthesis, and final reporting. We contacted Jelveh-Moghaddam et al. to clarify methodological concern, however, no response was received.
2.4. Risk of Bias Assessment
The risk of bias for randomized controlled trial (RCTs) and the quality of observational studies were assessed independently by three reviewers (AS, PH and MK). For interventional trials, the risk of bias was assessed using the second version of the Cochrane Collaboration’s risk-of-bias tool for randomized trials (RoB 2) (14). The assessment was conducted at the study level and aimed to evaluate the ‘intention-to-treat’ effect. Domains 3 and 4 were evaluated for the main outcome or, if not reported, for change in the degree of malnutrition.
For cohort and case-control studies, study quality was assessed using the Newcastle–Ottawa Scale (NOS). Although key confounders should ideally be prespecified, two stars were assigned for multivariate analyses including multiple relevant factors and one star when only a single relevant confounder was controlled for. Given the predominantly retrospective design of the of the included studies, it was difficult to confirm that controls had no history of the outcome; moreover, in non-registry-based studies, we cannot exclude the possibility that it was known before study initiation.
2.5. Data Analysis
Whenever feasible, data were analyzed using the Review Manager (RevMan) (Version 5.4. The Cochrane Collaboration, 2020). For dichotomous outcomes, risk ratio (RR) or odds ratio (OR) comparing the intervention/exposure and control groups were calculated with 95% confidence intervals (Cls). For continuous outcomes, the mean difference (MD) between the intervention/exposure and control group was determined. All analyses were based on a random-effects model. For studies reporting only median values with ranges, the MD and standard deviation (SD) were estimated using the method proposed by Hozo et al. to (15). In one RCT (16), SD was estimated to be zero, therefore means and MD could not be calculated. Three trials (16-19) reported anthropometric measures not as z-scores, therefore, these data were not analyzed.
In cases of substantial heterogeneity in the analyzed populations, interventions, comparators and outcomes, trial results were not pooled and were instead described narratively. For meta-analysis, heterogeneity among trials was determined using the estimation of inconsistency (I², where ≥ 50% is defined as substantial heterogeneity) (13). Although several subgroup analyses were planned, they were not performed because of the small number of eligible studies per comparison.
The certainty of evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) methodology (20) independently by three authors (AS, MK and PH). We used GRADEpro software to prepare the ‘Summary of findings’ table (GRADEpro GDT, McMaster University and Evidence Prime, 2023).
3. Results
3.1. Study Selection
For the study selection process, see Suppl Figure 1. Nineteen studies were included (8 RCTs, one non-randomized trial [non-RCT], 9 cohort studies and 1 case-control study). For studies excluded with reasons, see Suppl Table S2. A search of the ICTRP identified two ongoing RCTs (NCT05457712 and ChiCTR2000031872), both of which are not yet recruiting.
3.2. Study Characteristics
3.2.1. Interventional Studies
The characteristics of all included interventional studies are summarized in Suppl Table S3. A total of 402 children were randomized; one non-RCT included 60 participants. Four studies were conducted in North America (18, 21-23), four in Asia (17, 19, 24, 25), and one in Africa (16).
The majority of trials were single-center (7 RCTs and 1 non-RCT) (16-18, 21-25), except for one multi-center RCT (19). All included interventional trials had two parallel arms. Four studies were double-blinded (17, 21-23), one was single-blinded (18), two were open-label (16, 19) and two did not report blinding (24, 25).
Six trials included neonates and infants (16-19, 21, 22), whereas three also involved older children (up to 16-18 years of age) (23-25). Cardiac surgery definition varied across trials and included open-heart surgery with cardiopulmonary bypass (3 RCTs) (18, 22, 23), non-restricted ventricular septal defect (2 RCTs) (17, 19), Blalock–Taussig shunt or aortoplasty for cardiovascular malformations (1 RCT) (21), intracardiac repair with cardiopulmonary bypass for tetralogy of Fallot (1 RCT) (25), any cardiac surgery (1 non-RCT and 1 RCT), and surgery for non-restricted ventricular septal defect (2 RCTs) (16, 24).
Nutritional interventions ranged from supplementation with single nutrients (fatty, acids emulsion, vitamin D) to the use human milk fortifier and complex preoperative nutrition protocols. The effects of two fatty acids emulsions were assessed in two trials: enteral docosahexaenoic acid (DHA) in sunflower oil (75 mg/kg of baseline weight/day; in two daily doses) versus sunflower oil alone (21), and intravenous emulsion containing 50% medium-chain triglycerides (MCTs) and 40% long-chain triglycerides (LCTs) from soybean oil, and 10% of fish oil (0.02 g of eicosapentaenoic acid/DHA per ml of total fat; MCT/LCT/fish oil) versus a fully LCT emulsion (22). Both interventions were continued for 6 and 10 days after surgery, respectively (21, 22).
Three trials assessed the effect of high-dose cholecalciferol, however, the administration route, dose, and comparators varied: a single oral dose (10,000 IU/kg up to a maximum of 400,000 IU; one RCT) versus no intervention (25); enteral supplementation equivalent to 1600 IU/day for children <1 y or 2400 IU/day for those aged 1 to 17 y; one RCT) versus usual care (23); and a single intramuscular dose of 300,000 IU (one non-RCT) versus no intervention (24).
One trial in breastfed infants assessed the addition of a human milk fortifier (HMF) to breast milk versus placebo (17). In one trial, preoperative enteral trophic breast milk feeding (every 3 hours, with a total daily volume of 10 ml/kg/day) was compared with no feeding (18). Moreover, two RCTs assessed the efficacy of different preoperative nutrition protocols. The first trial (16) assessed the effects of a 2-week prehabilitation program using an oral nutrition supplement (ONS) compared with an identical 1-week prehabilitation program. The second trial evaluated the efficacy of an individualized nutritional support protocol initiated one month before surgery compared with no structured nutritional support plan (Suppl Table S3) (19).
3.2.2. Observational Studies
Eight retrospective cohort study (26-33), one prospective cohort study (34), and one case-control study (35) were included. The characteristics of included observational studies are summarized in Suppl Table S4. In total studies involved 3902 children. All studies were performed in the United States. Seven studies were single-center (27, 30-35), and three publications were based on two large multi-center studies (26, 28, 29).
Eight of included studies involved children with varied cardiac diagnoses (26-31, 33, 34), half of these studies involved patients with hypoplastic left heart syndrome (HLHS) or other single ventricle CHD (28, 29, 31, 34). In one study only children with HLHS were eligible for inclusion (32). Among these studies, five included infants who underwent stage 1 palliation (26, 28, 29, 32, 34), in two of these studies Norwood or Norwood variant procedure was performed (29, 32). In four other studies, any cardiac surgery were performed (27, 30, 31, 33). Additionally, one study included only children undergoing arterial switch operation for transposition of great arteries(35). In two of included studies only children who were discharged home after surgery were included (27, 29).
Exposures varied across included cohort studies, with most of them (six studies) (26, 27, 31-34) assessing any preoperative feeding compared with no feeding; in one of these studies, all children received additionally postoperative feeds (32). Moreover, two cohorts studies assessed impact of achieving center-recommended pre-operative caloric intake requirements (29), and receiving preoperatively fortified nutrition (≥22 kcal/oz) compared with unfortified nutrition (20 kcal/oz) (30). Additionally, one case-control study assessed an association between preoperative feeds intake and length of postoperative stay (shorter than 7 days vs longer than 14 days) (35). We also identified a propensity score matched cohort that assessed an association between exclusive human milk feeding and direct breastfeeding and varied intraoperative outcomes (28).
3.3. Risk of Bias
Interventional trials. The risk of bias is reported in Figure 1. The overall risk of bias was assessed as low in 4 RCTs (18, 21-23) and as having some concerns in 4 RCTs (16, 17, 19, 25). Two trials (16, 17) had an unclear risk of bias related to randomization process because allocation sequence concealment was not reported. In four RCTs (16, 17, 19, 25), some concern were identified regarding the selection of the reported results, mainly due to the lack of a registered or published study protocol. Although one trial (24) was reported as randomized, the allocation process was not clearly described, therefore, it was judged to be at high risk of non-random assignment. While some RCTs (16, 19) were open-label, we did not identify any major deviations from the intended intervention. A sample size calculation was reported in 5 trials (16, 17, 19, 21, 23).
Observational studies. The quality of the cohort studies is summarized in the Table 1 and Suppl Table S5. The NOS total score ranged from 5 (one study) to 9 (maximum score, four studies). The weakest item was cohort comparability based on study design or analysis: only 4 out of 9 studies received 2 stars (maximum score), whereas 3 studies did not adjust outcome for any confounding factors. The NOS total score for one case-control study was 5 (Suppl Table S6), downgraded by selection of control groups and lack of control for any confounders.
3.4. Effects of Any Modified Fatty Acids Emulsion
3.4.1. Enteral DHA in Sunflower Oil vs. Sunflower Oil Only
Data were reported in one small trial involving 34 children (21).
3.4.1.1. Efficacy
Length of ICU stay. We found a shorter mean duration of ICU stay in the group receiving an enteral DHA in sunflower oil compared with the group on sunflower oil alone (MD = -4.3 days, 95% CI, -5.71 to -2.89) (21).
3.4.1.2. Safety
Intraoperative adverse events. There was no significant difference between groups in the number of children with bleeding during surgery (RR=0.16; 95% CI, 0.01 to 2.87) (21).
Postoperative adverse events
Fewer children with at least one organ dysfunction were observed in the group receiving enteral DHA in sunflower oil compared with the sunflower oil only group in both the ITT analysis (RR=0.45, 95%CI 0.22-0.84, n=55) and in the PP analysis (RR=0.41, 95%CI 0.23-0.75, n=34) (21). Additionally, we found no difference between groups in the proportion of children with:
- postoperative sepsis and severe sepsis, in both the intention-to-treat (ITT; RR=0.67, 95%CI, 0.34 to 1.30; and RR=0.89. 95% CI, 0.51 to 1.56, respectively; n=55) and per-protocol (PP; RR=0.38, 95% CI, 0.12 to 1.15; RR=0.28, 95% CI, 0.03 to 2.26, respectively; n=34) analyses;
- any postoperative organ dysfunction, including: respiratory (RR=0.19; 95% CI, 0.03 to 1.4), cardiovascular (RR=0.28; 95% CI, 0.03 to 2.26), hematological (RR=0.16; 95% CI, 0.01 to 2.87), hepatic (RR=0.37; 95% CI, 0.02 to 8.55), and renal dysfunctions (RR=0.16; 95% CI, 0.01 to 2.87);
- vomiting events in the ICU (RR=1.13, 95% CI, 0.18 to 7.09; n=34);
- mortality in either the ITT analysis (RR=0.21; 0.03 to 1.66; n=55) or in the PP analysis (RR=0.37; 0.02 to 8.55; n=34); none of the deaths were related to DHA administration (21).
3.4.2. Intravenous 50% MCT and 40% LCT and 10% of Fish Oil Emulsion (MCT/LCT/fish oil) vs. Fully LCT Emulsion
Data were reported in one small study involving 32 subjects (22).
3.4.2.1. Efficacy
Compared with the fully LCT emulsion group, in the MCT/LCT/fish oil emulsion group we found a shorter:
- mean duration of the ICU stay (MD = -7.4 days, 95% CI, -10.86 to -3.94);
- mean duration of mechanical ventilation (MD=-2.1 days, 95% CI, -2.86 to -1.34);
- and mean length of hospital stay (MD=-5.1 days, 95% CI, -8.77 to -1.43) (22).
3.4.2.2. Safety
There was no difference between groups in the proportion of children with postoperative sepsis (RR = 1.0, 95% CI, 0.41 to 2.45) (22).
3.4.3. High-Dose Cholecalciferol vs Usual Care/No Intervention
Data were reported in 2 RCTs (n=101) and 1 non-randomized trial (n=60).
3.4.3.1. Efficacy
Length of ICU stay. A meta-analysis of 2 RCTs showed no difference in the mean length of ICU stay between the high-dose cholecalciferol group and any control group (usual care or no supplementation) (MD=-2.25 hours, 95% CI, -5.83 to 1.32; I2=97%; n=101; Suppl Fig S2) (23, 25). However, this evidence should be interpreted with caution due to differences in dosing between the two trials and the very low certainty of evidence.
Length of mechanical ventilation. In a meta-analysis of 2 RCTs (23, 25), no difference was found in the mean length of mechanical ventilation between the high-dose cholecalciferol group and any control group (MD=-22.02 hours, 95% CI, -58.86 to 14.82; I2=92%; n=101; Suppl Fig S3), however the certainty of evidence was very low. Moreover, in one of these trials (23), a shorter mean length of initial mechanical ventilation was reported in the enteral high-dose cholecalciferol group compared with the usual care group (MD=-34.0 hours; 95% CI, -38.87 to -29.13; n=41).
Additionally, in one non-RCT (24), we found a longer duration of mechanical ventilation in children who received a single intramuscular injection of cholecalciferol (300 000 IU) three days before the surgery, compared with the no intervention group (MD = -6.75 hours, 95% CI, -11.2 to -2.3; n=60). However, these findings are limited by a high risk of bias.
Length of hospital stay. In one RCT (23), a shorter mean length of hospital stay was observed in the enteral high-dose cholecalciferol group compared with the usual care group (MD=-4.75 days, 95%CI, -6.47 to -3.03, n=41).
Administration of inotropes. This outcome was reported in one RCT (23), with no difference in the proportion of children receiving catecholamines between the enteral high-dose cholecalciferol group and the usual care group (RR=0.7, 95% CI, 0.43 to 1.13; n=41).
3.4.3.2. Safety
Adverse events. Data were reported in two RCTs. In one trial (23), there was no difference between the enteral high-dose cholecalciferol group and the usual care group in any of the reported adverse events: hypocalcemia; post-operative, acute renal failure requiring dialysis; intraoperative and post-operative day 1 hypercalciuria; transient (< 24h) hypercalcemia during pediatric ICU admission and positive post-operative cultures (data not shown; n=41). In the other RCT (25), there was no difference in the proportion of the participants with low cardiac output syndrome (RR=0.67, 95% CI, 0.21 to 2.13) or junctional ectopic tachycardia (RR=1.5, 95% CI, 0.27 to 8.34) between the oral high-dose cholecalciferol group and the no intervention group (n=60). Additionally, no neurological deficit was identified in any of participants.
Mortality. This outcome was reported in two RCTs (23, 25), with no deaths observed (n=101).
3.4.3.3. Compliance
Compliance was reported in one RCT (23), with a high median compliance rate (94%, IQR 77 to 100, n=41). There was no difference between the enteral high-dose cholecalciferol group and the usual care group in mean compliance rate (MD=− 8.6%, 95% CI − 21.7 to 4.5) or in the number of doses received by participants (MD= – 2 doses, 95% CI − 26 to 24 doses).
3.4.4. Effect of human milk fortifier vs. placebo in breastfed infants
Data were reported in one trial (n=58) (17). All preoperative outcomes were reported one month after nutritional intervention.
3.4.4.1. Efficacy
Preoperative laboratory markers of malnutrition. Higher preoperative levels of albumin (MD = 5.70 g/l, 95% CI, 3.25, 8.15) and prealbumin (MD = 49.4 mg/l, 95% CI, 34.57 to 64.23) were observed one month after the intervention in the HMF group compared with the placebo group; with no difference in preoperative hemoglobin levels between groups (MD=3.3 g/l, 95% CI, -5.77 to 12.37) (17).
Preoperative validated malnutrition risk score. A lower mean preoperative STRONG Kids Score was observed in the HMF group compared with the placebo group (MD=-1.9, 95% CI, -2.29 to -1.51) (17).
3.4.4.2. Safety
We found no difference between the study groups in the number of children with preoperative pneumonia (RR = 0.75, 95% CI, 0.18 to 3.06), liver insufficiency (RR = 0.5, 95% CI, 0.05 to 5.21), jaundice (RR = 0.5, 95% CI, 0.05 to 5.21), or feeding intolerance (RR = 3.0, 95% CI, 0.33 to 27.18) (17). Preoperative necrotizing enterocolitis (NEC), gastrointestinal bleeding, and death were not reported in any child.
3.4.5. Effects of Preoperative Nutrition-Based Protocols
3.4.5.1. Efficacy of Preoperative Trophic Breast Milk Feeds
Data were reported in one small trial (n=27) (18).
3.4.5.1.1. Efficacy
Postoperative feeding tolerance. We found no difference between groups in the number of children who postoperatively required a formula change due to feeding intolerance (RR = 1.39, 95% CI 0.69 to 2.82), were dependent on a nasogastric tube at hospital discharge (RR = 1.06, 95% CI, 0.54 to 2.09), or received exclusive breast milk feeds at discharge (RR = 0.93, 95% CI, 0.29 to 2.97) (18).
3.4.5.1.2. Safety
One trial found no preoperative adverse events associated with preoperative trophic breast milk feeds (18). Moreover, no differences between groups were observed in the proportion of children with postoperative NEC (RR = 1.86, 95% CI, 0.19 to 18.13); in those who required gastroesophageal reflux medication at discharge (RR = 1.24, 95% CI, 0.81 to 1.89); and in postoperative mortality rate (RR = 4.67, 95% CI, 0.24 to 88.96), with no deaths reported in the preoperative trophic breast milk feeds group (18).
3.4.5.2. A 2-week vs. 1-week preoperative nutrition support
Data were reported only in one small trial (n-40) (16).
3.4.5.2.1. Efficacy of the 2-week vs. 1-week preoperative nutrition support
Compared with the 1-week prehabilitation group, in the 2-week prehabilitation group we found:
- a shorter mean length of ICU stay (MD=36.5 hours, 95% CI, -44.61 to -28.39) (16);
- a shorter mean hospital length of stay (MD=-40.9 days, 95%CI, -65.26 to -16.54) (16);
- a shorter mean duration of postoperative mechanical ventilation was found (MD=-14.0 hours, 95% CI, -17.95 to -10.05) (16);
- and higher mean postoperative feeding volume intake, measured before discharge (MD = 7.53 ml/feed, 95%CI, 0.99 to 14.07) (16).
However, no difference between groups was found for:
- other feeding-related outcomes, including: day of enteral feeding initiation (RR = 1.33, 95% CI, 0.88 to 2.03, and RR=1.00, 95% CI, 0.34 to 2.93, for day 1 and 2 respectively), route of feeding (oral: RR = 1.42, 95% CI, 0.95 to 2.12, vs oral and nasogastric tube: RR = 0.38, 95% CI, 0.12 to 1.21), and feeding frequency (every 2 hours: RR = 1.19, 95% CI, 0.93 to 1.51, vs every 3 hours: RR = 0.25, 95% CI, 0.03 to 2.05) (16);
- and the proportion of children with successful extubation (RR=1.05, 95% CI, 0.92 to 1.2), early extubation (≤48 h) (RR=1.2, 95% CI, 0.9 to 1.61), late extubation (>48 h) (RR=0.33, 95% CI, 0.04 to 2.94), and reintubation (RR=0.5, 95%CI, 0.05 to 5.08) (16).
Change in degree of malnutrition
Preoperative anthropometric measures. The authors reported a higher median weight-for-age z-score in the 2-week prehabilitation group compared with the 1-week prehabilitation group based on the p-value (p = 0.001); with no difference in height-for age-z-score between groups (p = 0.16).
Postoperative anthropometric measures. A higher mean weight-for-age and height-for-age z-scores were observed in the 2-week prehabilitation group compared with the 1-week prehabilitation group (MD = 2.50, 95% CI, 2.15 to 2.85; and MD = 1.00, 95% CI, 0.69 to 1.31, respectively).
Laboratory markers of malnutrition. No difference between study groups were observed in albumin and hemoglobin levels measured at discharge (MD = 0.00 gm, 95% CI, -0.16 to 0.16; MD = -0.08 g/dl, 95% CI, -0.92 to 0.76; respectively) (16).
3.4.5.2.2. Safety of the 2-week vs 1-week preoperative nutrition support
Adverse events. Only proportion of children with nosocomial sepsis was reported, however, no difference between the study groups was observed (RR=0.2, 95% CI, 0.01 to 3.92) (16).
Feeding-related adverse events. We found no difference between the study groups in the proportion of children with any feeding-related adverse events, including abdominal distension (RR = 0.43, 95% CI, 0.13 to 1.43), increased gastric residue (RR = 0.14, 95% CI, 0.01 to 2.6), vomiting (RR = 0.33, 95% CI, 0.01 to 7.72), diarrhea (RR = 0.33, 95% CI, 0.01 to 7.72), and hematemesis (RR = 0.2, 95% CI, 0.01 to 3.92) (16).
3.4.5.3. Efficacy of a 1-month preoperative nutrition support vs no support
One trial involving 80 children was identified (19).
Length of ICU and hospital stay. A shorter mean length of ICU stay and time to discharge were observed in the 1-month preoperative nutrition support group compared with the no support group (MD = -1.40 days, 95% CI, -1.93 to -0.87; and MD = -3.30 days, 95% CI, -5.09 to -1.51, respectively) (19).
Preoperative degree of malnutrition
Validated malnutrition risk score. We found a significantly lower mean preoperative STRONG Kids Score in the 1-month preoperative nutrition support group compared with the no support group (MD = -0.50, 95% CI, -0.72 to -0.28) (19).
Laboratory markers of malnutrition. We found a higher level of preoperative albumin, prealbumin and hemoglobin levels in the month preoperative nutrition support group compared with the no support group (MD = 2.60 g/l, 95% CI, 1.45, 3.75; MD = 10.30 mg/l, 95% CI, 1.03 to 19.57; and MD = 4.20 g/l, 95% CI, 1.14 to 7.26, respectively) (19).
3.4.5.4. Effects of any preoperative feeding vs. no feeding
Data were reported in 6 cohort studies and 1 case-control study.
3.4.5.4.1. Effectiveness
Length of ICU. In a meta-analysis of 2 cohort studies (31, 32), we found no difference in the mean postoperative length of ICU stay between the group receiving any preoperative feeding and the no feeding group (MD = -3.56 days, 95% CI, -7.22 to 0.11, I2=23%, n=175; Suppl Fig S4), however the certainty of evidence is very low. Moreover, in one cohort study (33), the mean length of ICU stay did not differ between the standardized preoperative feeding protocol group and the no feeding protocol group, based on the reported p-value (p=0.14; n=51).
Length of hospital stay. A meta-analysis of four cohort studies (31-34) found a shorter mean length of hospital stay in the group receiving any preoperative feeding compared with the no feeding group (MD=-7.23 days, 95% CI, -14.07-0.4, I2=58%, n=278; Figure 2), however the certainty of evidence is very low.
Duration of mechanical ventilation. In one cohort study (31), no difference in the mean duration of mechanical ventilation was observed between the group receiving any preoperative feeding and the no feeding group (MD=-2.0 days, 95% CI, -7.6 to 3.6, n=130). In another cohort study (32), a lower mean duration of mechanical ventilation was observed in the group receiving preoperative trophic feeds compared with no feeds (MD = -2.78 days, 95% CI, -3.84 to -1.71, n=45).
Change in degree of malnutrition
Anthropometric measures at discharge. In one cohort study (31), no difference in the mean change in weight-for age z-score from hospital admission to discharge was observed between the group receiving any preoperative feeding and the no feeding group (MD=-0.04, 95% CI, -0.73 to 0.65, n=130). In another cohort study (33), no difference were reported in median weight-for-age, length-for-age, and head circumference-for-age at discharge between the standardized preoperative feeding protocol group and the no feeding protocol group (p=0.52, 0.92 and 0.93, respectively; n=51).
Postoperative laboratory markers. In one study (32) the lowest albumin level in the first 72 h after surgery was higher in the group receiving preoperative trophic feeds compared with no feeds (MD = 0.23, 95% CI, 0.16 to 0.29, n=45).
Mean number of days to achieve full feeds postoperatively. A meta-analysis of three cohort studies (32-34) showed a lower mean number of days required to achieve full postoperative feeds in the group receiving any preoperative feeding compared with the no feeding group (MD = -3.29, 95% CI, -4.23 to -2.34, n=138, I2=21%; Figure 3). However, the certainty of evidence is very low. One of these studies (32) also reported a shorter time to the first postoperative feed in the group receiving preoperative trophic feeds compared with the nothing by mouth group (MD = -0.75 day, 95% CI, -1.28 to -0.22, n=45). Additionally, one study (34) found no association between preoperative feeding and the need for G-tube placement within the first postoperative year (OR=0.29, 95% CI, 0.08 to 1.07, n=52).
Moreover, one study (27) reported a higher proportion of children with full post-operative feeding at discharge in the group receiving any preoperative feeding (OR 2.78, 95% CI 1.48–5.24, n=235), including those receiving > 20 ml/kg/day (adjusted OR = 2.92, 95% CI, 1.28 to 6.69) and ≤ 20 ml/kg/day (adjusted OR = 2.25, 95% CI, 1.06 to 4.79), compared with the group without any preoperative oral feeding.
In one case-control study (35), a higher proportion of children fed preoperatively (the majority receiving ad libitum oral feeds accounting for full caloric intake) was observed in the short-stay group (<7 days) compared with the long stay group (<14 days) (OR=8.8, 95% CI, 2.57 to 30.18, n=57; Suppl Fig S5).
3.4.5.4.2. Safety
Severe cardiac surgery-associated acute kidney injury. In a secondary analysis of the NEPHRON multicenter cohort (26), the authors reported 52% lower odds of severe cardiac surgery-associated acute kidney injury in the group receiving preoperative feeding (adjusted OR=0.48; 95% CI, 0.27 to 0.86, n=347).
NEC. In a meta-analysis of three cohort studies (31, 33, 34), we found no association between the proportion of children with NEC and previous exposure to preoperative feeding (OR=0.69, 95%CI, 0.26 to 1.82, n=232; Figure 4). However, the certainty of evidence is very low. Additionally, in one of these studies (31), no association was observed between preoperative enteral feeding and NEC (OR=0.62, CI 0.19–2.0, n=130). Moreover, no association was found between intake of feeding volumes exceeding >20 ml/kg/day and an increased risk of NEC (OR=4.04, 95% CI, 0.49 to 33.3) (31). One study (34) also reported no difference in the risk of preoperative, stage 1 or stage 2 NEC between children fed and non-fed preoperatively (data not shown, n=42).
Postoperative infection rate. One cohort study (32) found no association between postoperative infections rate and receipt of preoperative trophic feeds compared with nothing by mouth (OR = 1.07, 95% CI, 0.23; 4.94, n=45).
Mortality. A meta-analysis of two cohort studies (32, 34), showed no difference in the number of deaths between the group receiving any preoperative feeding and the no feeding group (OR=0.65, 95% CI, 0.25 to 1.69, n=97, I2=0%; Suppl Fig S6), but the certainty of evidence is very low.
3.4.5.5. Effectiveness of Meeting Versus Not Meeting Center-Recommended Preoperative Caloric Intake Requirements (Cohort Study)
In one cohort study (29), failure to achieve center-recommended preoperative caloric intake requirements at the last visit before bidirectional Glenn procedure was associated with a longer post-BDG hospital length of stay (adjusted HR=1.81, 95% CI, 1.13 to 2.87, n=160).
3.4.5.6. Preoperative Fortified vs. Unfortified Nutrition
Data were reported in one retrospective cohort study (n=84) (30).
3.4.5.6.1. Effectiveness
Length of ICU and hospital stay. The authors reported shorter length of ICU stay (MD=1.00 days, 95% CI, 0.76 to 1.24) and hospital stay (MD=0.38 day, 95% CI 0.09 to 0.66) in children receiving unfortified nutrition (20 kcal/oz) compared with infants receiving fortified nutrition (≥22 kcal/oz) (30).
Duration of mechanical ventilation. No difference in the duration of mechanical intubation was observed between groups (30).
Postoperative anthropometric measures. Based on p values only, the authors reported lower postoperative weight-for-age percentiles in the group receiving fortified nutrition at 2, 5 and 10 years of age, but not at first 30 and 31-60 days after surgery, compared with children receiving unfortified nutrition (30). BMI-for-age percentiles were also higher at 5 and 10 years of age (p=0.04 [n=52] and 0.02 [n=41], respectively) in the group receiving unfortified nutrition compared with fortified group (p=0.045 and 0.02, respectively), but not at 2 years of age. However, no difference between groups was observed in the change in weight-for-age after repair at 30 days (n=23) or 60 days after surgery.
3.4.5.6.2. Safety
No difference in risk of surgical site infection was observed between groups (30).
3.4.6. Preoperative Exclusive Human Milk and Direct Breastfeeding
In one propensity score matched cohort (28), involving 2491 participants, the association between preoperative human milk feeding and direct breastfeeding, and several outcomes of interest was assessed. Some evidence suggested that exclusive human milk feeding and any direct breastfeeding were associated with a shorter hospital length of stay was observed (data not shown due to complexity of comparisons, Suppl Table S7).
3.5. Quality of Evidence
In all meta-analyses, the certainty of evidence was very low (Suppl Table S8).
4. Discussion
4.1. Summary
This systematic review summarized evidence from 9 interventional and 10 observational studies on the efficacy/effectiveness and safety of preoperative nutrition intervention on pre-, intra- and postoperative outcomes in children undergoing cardiac surgery. Half of the included trials had some methodological concerns. The quality of observational studies ranged from moderate to high.
An overall summary of findings is presented in Table 2. The intervention/exposures across studies were heterogenous and included parenteral fatty acids emulsions, enteral high-dose vitamin D, HMF, trophic breast milk feeds and various preoperative nutrition support protocols. The main finding of this systematic review is the provision of evidence from a limited number of RCTs and observational studies suggesting overall safety of different preoperative nutrition interventions in children undergoing cardiac surgery. While the magnitude and type of benefits varied across interventions, most preoperative nutrition strategies were associated with some favorable outcomes . Enteral DHA in sunflower oil and intravenous MCT/LCT/fish oil emulsion were associated with shorter ICU length of stay in two small trials. Similarly, shorter ICU and hospital stays were observed with 2-week and 1-month preoperative nutrition support in two RCTs. Observational studies demonstrated an association between any preoperative nutrition support and shorter hospital length of stay (meta-analysis of 4 studies), as well as fewer days required to achieve full postoperative feeding (meta-analysis of 3 studies). However, the findings of this systematic review are limited by the very low certainty of the available evidence.
Intraoperative outcomes and changes in the degree of malnutrition were rarely and poorly reported. Compliance was reported in only 1 RCT. Postoperative health-related quality of life and readmission rate were not reported in any of the included trials.
4.2. Comparison with Other Systematic Reviews
A 2019 systematic review of five cohort studies focused on ductal-dependent lesions (36), reported insufficient evidence for the benefit of preoperative feeding on postoperative outcomes, highlighting small samples sizes and variable protocols. Similarly, Bell et al. (2022) (37) conducted a PRISMA-guided systematic review in neonates and infants awaiting cardiac surgery and found no association between preoperative enteral feeding and NEC; nor with any secondary outcomes such as length of hospital stay and tube-assisted feeding at discharge. However, their dataset was based mainly on observational studies (8 of 9 studies), which limits robustness of these findings.
Additionally, in 2022, the Neonatal Cardiac Care Collaborative (NeoC3) synthesized available evidence across six domains (energy and protein needs, enteral nutrition, feeding practices, parenteral nutrition, and outcomes) and developed consensus statements for infants <6 months of age with CHD (38). This document highlighted wide practice variation, frequent reliance on low-level evidence, and the absence of adequately powered RCTs—particularly regarding standardized preoperative feeding advancement and the role of lipid formulations—underscoring the need for multicenter trials and quality-improvement frameworks.
Recently, a non-systematic review on perioperative nutrition support in children with congenital heart disease and heart failure emphasized the need for implementation of pragmatic, institution-level pathways (39). Proposed nutrition protocols included standardized preoperative feeding algorithms, liberalization of fasting within ERAS-consistent care, coordinated escalation of enteral versus parenteral strategies, and integration of macronutrient and protein targets and lipid considerations alongside micronutrient supplementation. Although complementary in scope to our work, this review does not provide quantitative pooling or CHD-only stratification and therefore could not estimate effect sizes for preoperative interventions; nevertheless, it aligns with our conclusions regarding the paucity of high-quality trials and the need for standardized preoperative nutritional protocols.
Consistent with our findings, Szentirmay et al. (40) in a recent nonsystematic review, highlighted feasibility and safety signals alongside substantial heterogeneity and limited-quality evidence for preoperative enteral nutrition in neonates with CHD. However, their scope did not address broader preoperative nutrition strategies (e.g., fortification, structured nutrition support, or parenteral approaches) or older infants, which were evaluated in our systematic review.
In contrast to these previous works, our review summarizes a broader spectrum of preoperative nutrition-based interventions, including structured nutrition support programs, feed fortification, lipid emulsions, and short-term prehabilitation elements, and quantitatively explores postoperative endpoints such as length of stay and time to full feeds. While our pooled estimates suggest potential benefits without major safety signals, the certainty of evidence was very low and substantial heterogeneity across populations, interventions, and outcome definitions were observed. Overall, our findings remain consistent with limitations identified by previous reviews (37, 38) and reinforce the need for standardized, multicenter trials.
4.3. Strengths and Limitations
A key strength of this review is its rigorous methodology, with clearly defined eligibility criteria and clinically relevant outcome measures, and the use of recommended tools for assessing risk of bias for RCTs and the quality of observational studies. This strengthens the reliability and robustness of these findings. Moreover, the inclusion of both, interventional trial and observational studies regardless of any language or settings restrictions allows for a broader synthesis and assessment of the impact of different nutritional interventions. We are confident that this systematic review summarizes all currently available evidence on preoperative nutrition interventions on perioperative outcomes.
Additionally, the inclusion of a large number of children undergoing various cardiac surgeries for different cardiac conditions and from different regions enhance the generalizability of the results. However, due to limited sample sizes for individual comparison, we did not perform subgroup analyses, which limits the applicability of the findings to specific diseases or types of surgery.
Nonetheless, several methodological limitations should be considered. A major limitation of this systematic review is the heterogeneity of reported interventions/exposures and outcome measures, which complicates comparison and data pooling and reduces the ability to draw firm conclusions across studies . Many studies reported only within-group differences and statistical significance based solely on p-values, without presenting preferred effect measures. To improve the interpretability of the results, between group differences were calculated whenever feasible.
Although, the overall quality of the included studies was moderate or high, most evidence regarding preoperative nutrition support protocols was derived from observational studies, which limits the strength of the conclusions. For all conducted meta-analyses, the certainty of evidence is very low, and it was downgraded mainly because of substantial inconsistency, and indirectness, and for observational studies methodological limitations. A key limitation of the included observational studies was lack of adjustment for potential confounders. Confounding may lead to spurious associations when a true causal relationship does not exist (41). Therefore, potential factors affecting outcome or exposure should be carefully considered during study design.
Another important limitation of most included studies is the small sample size, with evidence largely derived from single-center cohorts. Only two registry-based observational studies included substantial number of participants (ranging from 347 to 2491 participants) (26, 28). Although limited by their observational design, multi-center patient registries represent a promising approach to achieving adequate sample size, particularly for the assessment of long-term efficacy and safety outcomes (42).
5. Conclusions
This systematic review provides very low–certainty evidence suggesting that preoperative nutrition-based interventions may be safe and potentially beneficial in children undergoing cardiac surgery. The main limitations are the variability of included interventions and outcomes, and the limited certainty of evidence, both of which hinder the formulation of consistent conclusions regarding the effectiveness of preoperative nutrition strategies. Further research is required to establish standardized preoperative nutrition protocol with confirmed efficacy and safety in well-designed, adequately powered trials.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, A.S., M.K., A.H., M. B., and R.P.; methodology, A.S., M.K., A.H., M. B., and R.P.; formal analysis, A.S., M.K., and P.H.; writing—original draft preparation, A.S., M.K., and P.H.; writing—review and editing, A.H., M. B., and R.P.; visualization, A.S., M.K., and P.H.; supervision, A.S., M.K., and A.H.; funding acquisition, R.P. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
During the preparation of this manuscript/study, the author(s) used ChatGPT-5® Plus (OpenAI®, San Francisco, CA, USA) in order to facilitate the extraction of study characteristics items. The software was applied only for the initial drafting of study characteristics using the self-developed data extraction form. After using this tool, the authors independently reviewed and edited the content as needed and take(s) full responsibility for the content of the publication. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BDG | Bidirectional Glenn |
| BMI | Body mass index |
| CHD | Congenital heart disease |
| CI | Confidence interval |
| CS-AKI | Cardiac surgery–associated acute kidney injury |
| DHA | Docosahexaenoic acid |
| ERAS | Enhanced Recovery After Surgery |
| GER | Gastroesophageal reflux |
| GRADE | Grading of Recommendations, Assessment, Development, and Evaluation |
| HMF | Human milk fortifier |
| HR | Hazard ratio |
| ICU | Intensive care unit |
| ITT | Intention-to-treat |
| IV | Intravenous |
| LCT | Long-chain triglycerides |
| MD | Mean difference |
| MCT | Medium-chain triglycerides |
| MV | Mechanical ventilation |
| n | Number of participants |
| ND | No difference |
| NEC | Necrotizing enterocolitis |
| NeoC3 | Neonatal Cardiac Care Collaborative |
| NOS | Newcastle–Ottawa Scale |
| OR | Odds ratio |
| PP | Per-protocol |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RCT | Randomized controlled trial |
| RoB 2 | Revised Cochrane risk-of-bias tool for randomized trials |
| RR | Risk ratio |
| SD | Standard deviation |
| STRONG | Screening Tool for Risk on Nutritional Status and Growth |
References
- Diao J, Chen L, Wei J, Shu J, Li Y, Li J, et al. Prevalence of Malnutrition in Children with Congenital Heart Disease: A Systematic Review and Meta-Analysis. The Journal of pediatrics. 2022;242:39-47.e4.
- Abbas Q, Ali H, Ahuja AK, Bhatti OA, Ladak S, Khan I, et al. Preoperative nutrition status in children with congenital heart disease and its impact on postoperative outcomes: a systematic review and meta-analysis. Sci Rep. 2025;15(1):25738.
- Ljungqvist O, Scott M, Fearon KC. Enhanced Recovery After Surgery: A Review. JAMA Surg. 2017;152(3):292-8.
- Lau CS, Chamberlain RS. Enhanced Recovery After Surgery Programs Improve Patient Outcomes and Recovery: A Meta-analysis. World J Surg. 2017;41(4):899-913.
- Hidayah BA, Toh ZA, Cheng LJ, Syahzarin BD, Zhu Y, Pölkki T, et al. Enhanced recovery after surgery in children undergoing abdominal surgery: meta-analysis. BJS Open. 2023;7(1).
- Anesthesiology 2017, 126(3), 376–93.
- Frykholm P, Disma N, Andersson H, Beck C, Bouvet L, Cercueil E, et al. Pre-operative fasting in children: A guideline from the European Society of Anaesthesiology and Intensive Care. Eur J Anaesthesiol. 2022;39(1):4-25.
- Mehta NM, Skillman HE, Irving SY, Coss-Bu JA, Vermilyea S, Farrington EA, et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition. JPEN J Parenter Enteral Nutr. 2017;41(5):706-42.
- Kołodziej M, Skulimowska J. A Systematic Review of Clinical Practice Guidelines on the Management of Malnutrition in Children with Congenital Heart Disease. Nutrients. 2024;16(16).
- Raval MV, Brockel MA, Kolaček S, Simpson KE, Spoede E, Starr KNP, et al. Key Strategies for Optimizing Pediatric Perioperative Nutrition-Insight from a Multidisciplinary Expert Panel. Nutrients. 2023;15(5).
- Weimann A, Bezmarevic M, Braga M, Correia M, Funk-Debleds P, Gianotti L, et al. ESPEN guideline on clinical nutrition in surgery - Update 2025. Clin Nutr. 2025;53:222-61.
- Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160.
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane, 2023. Available from www.training.cochrane.org/handbook. 2023.
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. Bmj. 2019;366:l4898.
- Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Medical Research Methodology. 2005;5(1):13.
- El-Ganzoury MM, El-Farrash RA, Ahmed GF, Hassan SI, Barakat NM. Perioperative nutritional prehabilitation in malnourished children with congenital heart disease: a randomized controlled trial. Nutrition (Burbank, Los Angeles County, Calif). 2021;84:111027.
- Lin YF, Lin WH, Lin SH, Zhang QL, Chen Q, Zheng YR. Using Human Milk Fortifiers to Improve the Preoperative Nutritional Status of Infants With Non-restricted Ventricular Septal Defect. Frontiers in Pediatrics. 2022;10.
- Zyblewski SC, Nietert PJ, Graham EM, Taylor SN, Atz AM, Wagner CL. Randomized Clinical Trial of Preoperative Feeding to Evaluate Intestinal Barrier Function in Neonates Requiring Cardiac Surgery. Journal of pediatrics. 2015;167(1):47-51.e1.
- Xu LP, Lin SH, Zhang QL, Zheng Y, Lin G. Short-Term Nutritional Support Improves The Preoperative Nutritional Status of Infants With Non-Restrictive Ventricular Septal Defect: A Prospective Controlled Study. Heart Surg Forum. 2022;25(5):E745-e9.
- In GRADE handbook for grading quality of evidence and strength of recommendations; Schünemann H, Brożek J, Guyatt G, Oxman A, editors. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from guidelinedevelopment.org/handbook.
- Bernabe-Garcia M, Lopez-Alarcon M, Villegas-Silva R, Mancilla-Ramirez J, Rodriguez-Cruz M, Maldonado-Hernandez J, et al. Beneficial Effects of Enteral Docosahexaenoic Acid on the Markers of Inflammation and Clinical Outcomes of Neonates Undergoing Cardiovascular Surgery: an Intervention Study. Annals of nutrition & metabolism. 2016;69(1):15-23.
- Larsen BM, Goonewardene LA, Joffe AR, Van Aerde JE, Field CJ, Olstad DL, et al. Pre-treatment with an intravenous lipid emulsion containing fish oil (eicosapentaenoic and docosahexaenoic acid) decreases inflammatory markers after open-heart surgery in infants: a randomized, controlled trial. Clinical nutrition (Edinburgh, Scotland). 2012;31(3):322-9.
- McNally JD, O’Hearn K, Fergusson DA, Lougheed J, Doherty DR, Maharajh G, et al. Prevention of post-cardiac surgery vitamin D deficiency in children with congenital heart disease: a pilot feasibility dose evaluation randomized controlled trial. Pilot and Feasibility Studies. 2020;6(1).
- Jelveh-Moghaddam H, Fani K, Hekmat M, Azari AA. The effects of Vitamin D3 in pediatric patients undergoing congenital heart surgery. Journal of cellular and molecular anesthesia. 2020;5(2):66-73.
- Sahu MK, Bipin C, Niraghatam HV, Karanjkar A, Singh SP, Rajashekar P, et al. Vitamin D Deficiency and Its Response to Supplementation as Stoss Therapy in Children with Cyanotic Congenital Heart Disease Undergoing Open Heart Surgery. Journal of Cardiac Critical Care. 2019;3(1):17-23.
- Bertrandt RA, Gist K, Hasson D, Zang H, Reichle G, Krawczeski C, et al. Cardiac Surgery-Associated Acute Kidney Injury in Neonates Undergoing the Norwood Operation: Retrospective Analysis of the Multicenter Neonatal and Pediatric Heart and Renal Outcomes Network Dataset, 2015-2018. Pediatr Crit Care Med. 2024;25(5):e246-e57.
- Dabbagh A, Miller S, McCulloch M, Rosenthal G, Conaway M, White S. Preoperative Oral Feeding in Infants with Congenital Heart Disease Within the First Month of Life is Associated with a Higher Likelihood of Freedom From Tube Feeding at Time of Postoperative Discharge. Pediatric cardiology. 2025.
- Elgersma KM, Wolfson J, Fulkerson JA, Georgieff MK, Looman WS, Spatz DL, et al. Human Milk Feeding and Direct Breastfeeding Improve Outcomes for Infants With Single Ventricle Congenital Heart Disease: Propensity Score-Matched Analysis of the NPC-QIC Registry. Journal of the American Heart Association. 2023;12(17):e030756.
- Menon SC, McCandless RT, Mack GK, Lambert LM, McFadden M, Williams RV, et al. Clinical outcomes and resource use for infants with hypoplastic left heart syndrome during bidirectional Glenn: summary from the Joint Council for Congenital Heart Disease National Pediatric Cardiology Quality Improvement Collaborative registry. Pediatr Cardiol. 2013;34(1):143-8.
- Murray SE, Zimmerman D, Patel SS. Preoperative Feeding Fortification Among Infants with Congenital Heart Disease is Associated with Higher Growth Velocity in the First 30 Days Post-repair and Lower BMI Percentile for Age at 10 Years: A Retrospective Cohort Study. Pediatric cardiology. 2025;46(2):394-400.
- Scahill CJ, Graham EM, Atz AM, Bradley SM, Kavarana MN, Zyblewski SC. Preoperative Feeding Neonates With Cardiac Disease. World J Pediatr Congenit Heart Surg. 2017;8(1):62-8.
- Toms R, Jackson KW, Dabal RJ, Reebals CH, Alten JA. Preoperative trophic feeds in neonates with hypoplastic left heart syndrome. Congenit Heart Dis. 2015;10(1):36-42.
- Zacharias P, Blinci J, Shenoy R, Lee J, Singh Y. Impact of the Pre-Operative Standardized Nutritional Protocol in Infants with Congenital Heart Disease (CHD). J Cardiovasc Dev Dis. 2025;12(5).
- Venna A, Reid K, Davis S, Gai J, d’Udekem Y, Clauss S. Preoperative Feeding in Single Ventricle Neonates is Predictive of Shorter Time to Goal Feed. Congenital Heart Disease. 2022;17(5):505-18.
- Iliopoulos I, Burke R, Hannan R, Bolivar J, Cooper DS, Zafar F, et al. Preoperative Intubation and Lack of Enteral Nutrition are Associated with Prolonged Stay After Arterial Switch Operation. Pediatric cardiology. 2016;37(6):1078-84.
- Kataria-Hale J, Osborne SW, Hair A, Hagan J, Pammi M. Preoperative Feeds in Ductal-Dependent Cardiac Disease: A Systematic Review and Meta-analysis. Hosp Pediatr. 2019;9(12):998-1006.
- Bell D, Suna J, Marathe SP, Perumal G, Betts KS, Venugopal P, et al. Feeding Neonates and Infants Prior to Surgery for Congenital Heart Defects: Systematic Review and Meta-Analysis. Children (Basel). 2022;9(12).
- Mills KI, Kim JH, Fogg K, Goldshtrom N, Graham EM, Kataria-Hale J, et al. Nutritional Considerations for the Neonate With Congenital Heart Disease. Pediatrics. 2022;150(Suppl 2).
- Silva-Gburek J, May K, Walvoord B, Lozano C, Coss-Bu JA. Perioperative Nutrition in Pediatric Patients with Congenital Heart Disease and Heart Failure. Nutrients. 2025;17(22).
- Szentirmay LS, Heywood A, James-Nunez K, Trivedi A, Dalrymple H. Preoperative enteral nutrition in neonates with congenital heart disease: A review of literature. Journal of Neonatal Nursing. 2025;31(3):101667.
- Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Int J Surg. 2014;12(12):1500-24.
- European Medicines Agency (EMA). Guideline on registry-based studies. EMA/426390/2021 (22 October 2021). .
Figure 1.
Assessment of risk of bias in randomized controlled trials using the revised Cochrane risk-of-bias tool for RCTs (RoB 2).
Figure 1.
Assessment of risk of bias in randomized controlled trials using the revised Cochrane risk-of-bias tool for RCTs (RoB 2).
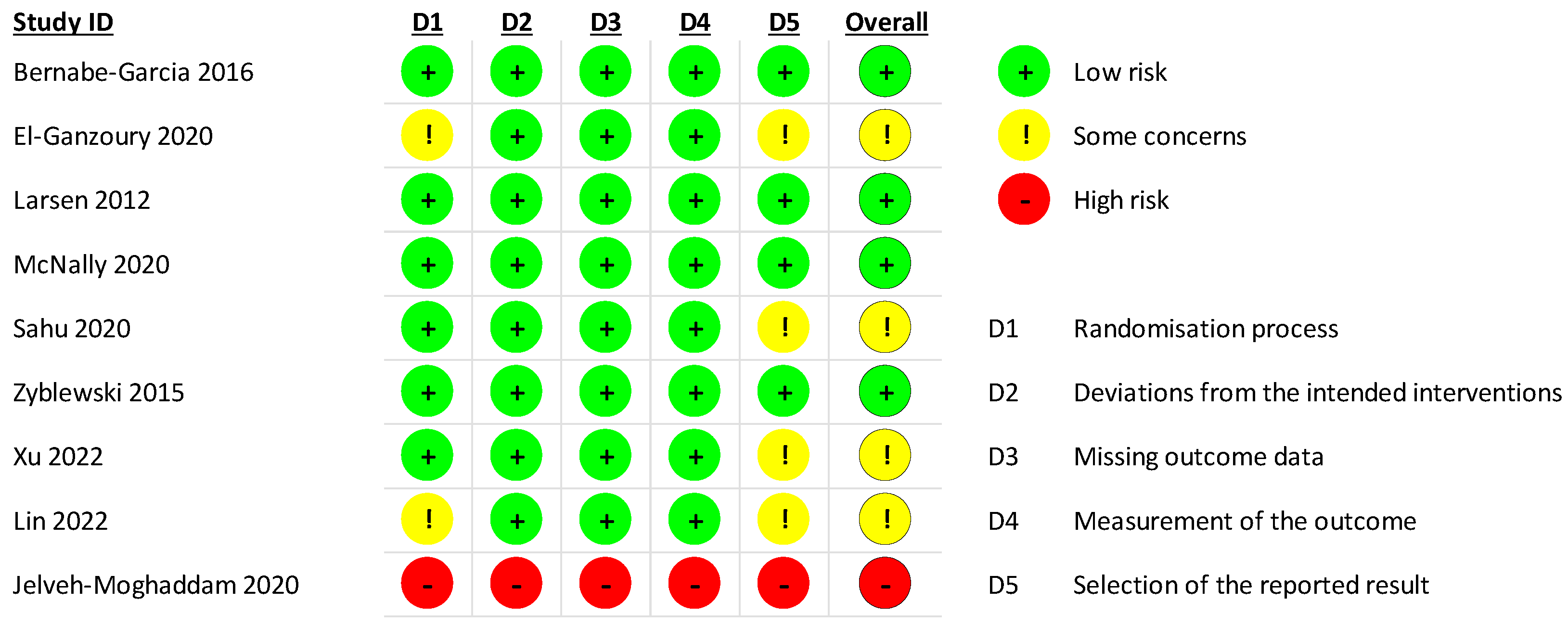
Figure 2.
Association between any preoperative feeding and length of hospital stay.
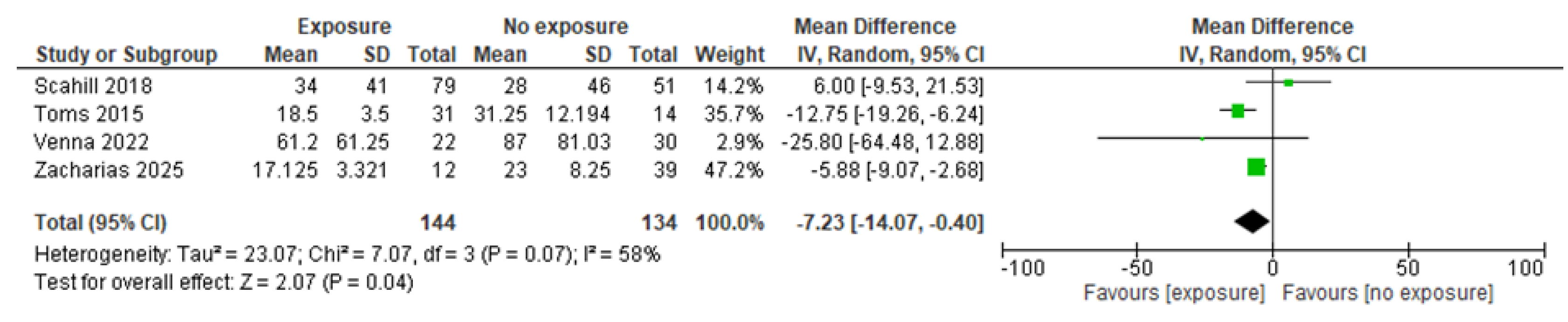
Figure 3.
Association between any preoperative feeding and mean number of days to achieve full feeds postoperatively.
Figure 3.
Association between any preoperative feeding and mean number of days to achieve full feeds postoperatively.

Figure 4.
Association between any preoperative feeding and risk of necrotizing enterocolitis.
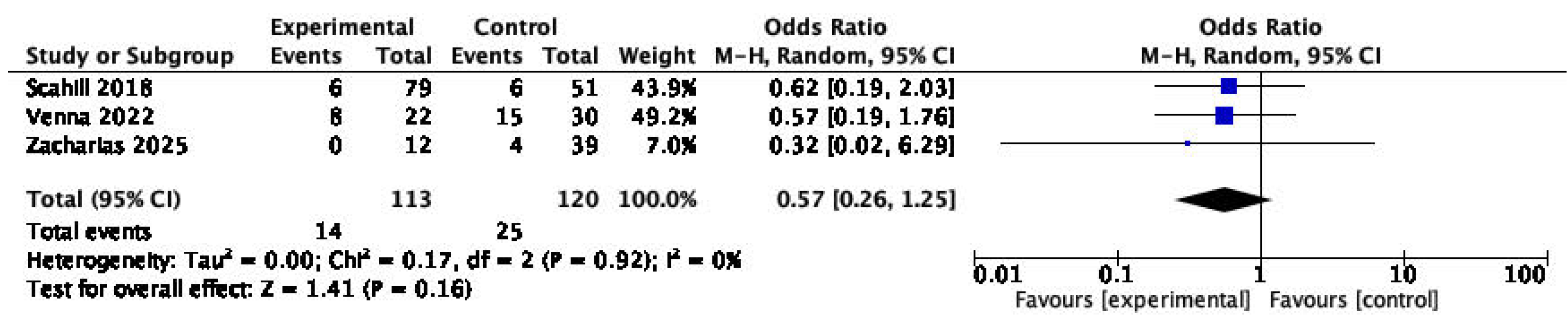

Table 1.
Summary of assessment of observational studies quality using the Newcastle-Ottawa Scale (NOS).Table 2. Summary of findings.
Table 1.
Summary of assessment of observational studies quality using the Newcastle-Ottawa Scale (NOS).Table 2. Summary of findings.
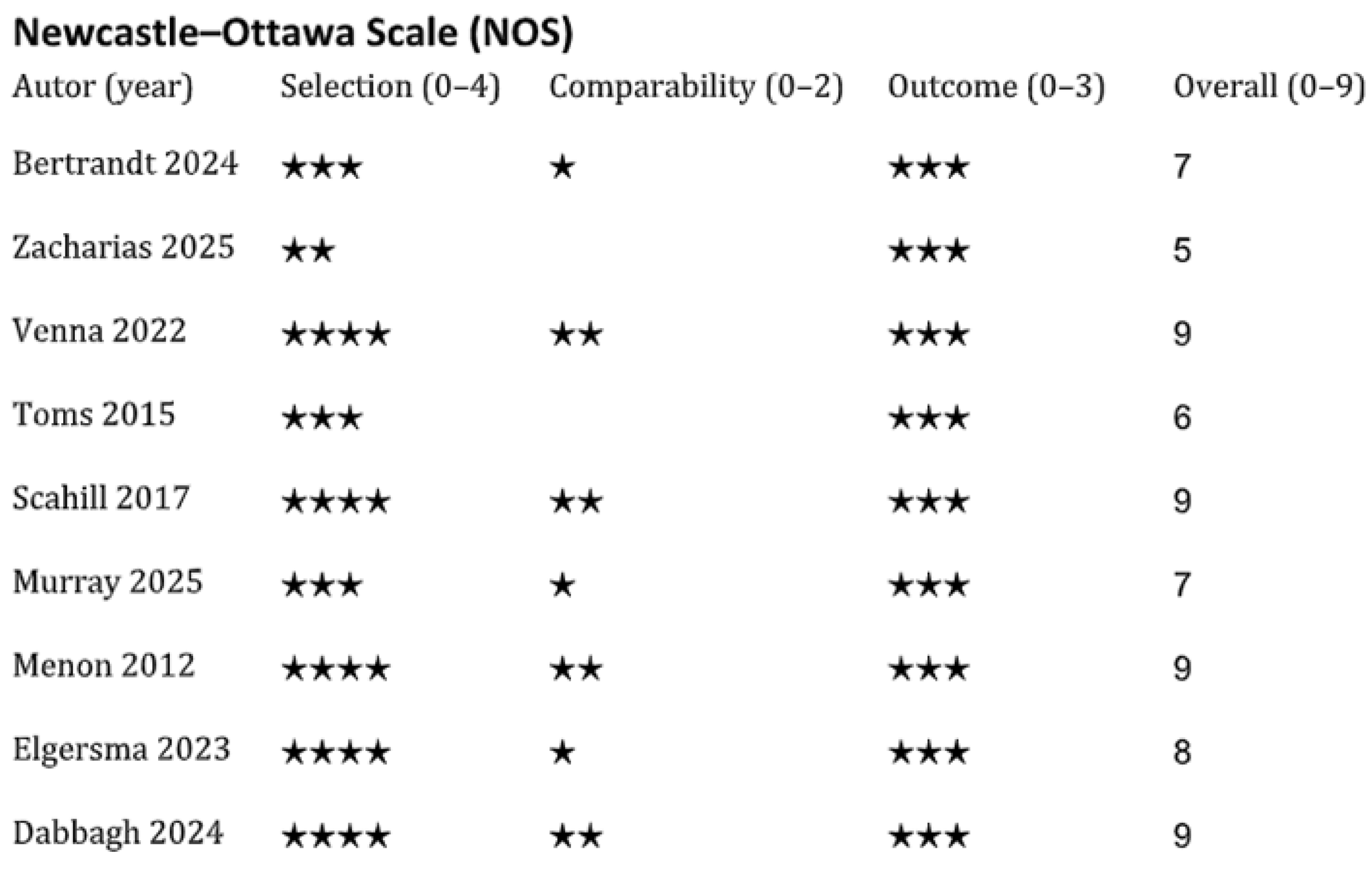 |
Table 2.
Summary of assessment of observational studies quality using the Newcastle-Ottawa Scale (NOS).Table 2. Summary of findings.
Table 2.
Summary of assessment of observational studies quality using the Newcastle-Ottawa Scale (NOS).Table 2. Summary of findings.
| Intervention/Exposure vs comparator |
Number of studies and participants (n) |
Efficacy/Effectiveness | Safety |
|---|---|---|---|
| Intravenous 50% MCT and 40% LCT and 10% of fish oil vs fully LCT emulsion |
1 RCT, n=32 | ↓ ICU stay ↓ hospital stay ↓ MV |
Sepsis – ND |
| Enteral DHA in sunflower oil vs sunflower oil only |
1 RCT, n=34 | ↓ ICU stay | Intraoperative bleeding – ND( Postoperative sepsis – ND Bleeding – ND Severe sepsis – ND Organ dysfunctions – ND Vomiting at ICU – ND Mortality – ND |
| High-dose vitamin D vs usual care/no intervention |
2 RCTs, n=101 | ICU stay – ND (2 RCTs, n=101) MV – ND (2 RCTs, n=101) ↓ hospital stay (1 RCT, n=41) ↑ MV (1 non-RCT, n=60) |
Adverse events – ND (2 RCT, n=101) Mortality ND (2 RCT, n=101) Need for inotropes ND (1 RCT, n=41) |
| Human milk fortifier vs placebo |
1 RCT, n=58 | ↑ Albumins and Prealbumins ↑ STRONG Kids score Hemoglobin ND |
Preoperative adverse events – ND No NEC No death |
| Preoperative trophic breast milk feeding vs no enteral feeding |
1 RCT, n=27 | Postoperative feeding intolerance ND Nasogastric tube dependence |
Postoperative NEC – ND GER medication – ND Mortality – ND |
| Preoperative nutrition support 2-weeks vs 1-week |
1 RCT, n=40 | ↓ ICU stay ↓ hospital stay ↓ MV ↑ postoperative feeding intake other feeding related outcomes – ND ↑ weight z-score pre- and postoperatively height z-score – inconsistent Albumins – ND Hemoglobulin – ND |
Sepsis – ND Successful extubation – ND Feeding-related adverse events ND |
| 1-month preoperative nutrition support vs no support |
1 RCT, n=80 | ↓ ICU and hospital stay ↓ preoperative STRONG Kids Score ↑ Albumins, Prealbumins and Hemoglobulin |
Not reported |
| Any preoperative feeding vs no feeding |
7 studies, n=917 | ICU stay – ND (3 studies, n=226) ↓ hospital stay (4 studies, n=278) ↓ days to achieve full feeds postoperatively (3 studies, n=138) MV duration – inconsistent results (2 studies, n=175) postoperative weight z-score – ND (2 studies, n=181) ↑ Albumins (1 study, n=45) ↑ children on full feeding (1 study, n=235) |
↓ CS-AKI (1 study, n=347) NEC – ND (3 studies, n=232), postoperative infection rate – ND (1 study, n=45) mortality risk – ND (2 studies, n=97) |
| Achieved vs not achieved center-recommended pre-operative caloric intake requirements |
1 study, n=160 | ↑ postoperative hospital stay ( | Not reported |
| Preoperative fortified nutrition (≥22 kcal/oz) vs unfortified nutrition (20 kcal/oz) |
1 study, n=84 | ↑ ICU stay ↑ hospital stay ↓ postoperative weight MV duration – ND BMI-for-age percentiles at 5 and 10 years |
Surgical site infection risk – ND |
DHA, docosahexaenoic acid; CS-AKI, cardiac surgery–associated acute kidney injury; GER, gastroesophageal reflux; ICU, intensive care unit; IV, intravenous; LCT, long-chain triglycerides; MCT, medium-chain triglycerides; MV, mechanical ventilation; n, number of participants; ND, no difference; NEC, necrotizing enterocolitis; STRONG, Screening Tool for Risk on Nutritional status and Growth (pediatric nutritional risk screening tool); RCT, randomized controlled trial.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



