
Submitted:
21 January 2026
Posted:
22 January 2026
Read the latest preprint version here
Abstract
Congenital cytomegalovirus (CMV) infection is the most common congenital viral infection worldwide and a leading cause of neurodevelopmental abnormalities, including sensorineural hearing loss, microcephaly, and developmental delay in neonates. Transmission occurs primarily through vertical maternal–fetal infection during early pregnancy. Although most infected neonates are asymptomatic at birth, a significant proportion develop long-term neurological sequelae. In low- and middle-income countries, including Nigeria, routine screening for congenital CMV is rarely performed, and molecular epidemiological data remain limited. This study aimed to determine the molecular prevalence and characterize congenital CMV infection among neonates attending tertiary health institutions in Jos, Nigeria. A cross-sectional molecular study was conducted among neonates aged ≤21 days recruited from three tertiary hospitals in Jos between January 2021 and December 2022. Buccal swab samples were collected and tested for CMV DNA using standardized in-house polymerase chain reaction (PCR). Positive samples were subjected to Sanger sequencing, and phylogenetic analysis was performed. Data were analyzed descriptively, and molecular prevalence was reported with exact 95% confidence intervals. Out of 180 neonates enrolled, one tested positive for CMV DNA, giving a molecular prevalence of 0.6% (95% CI: 0.02–3.1%). BLAST analysis revealed 98.9% nucleotide sequence similarity to Human herpesvirus 5 strain HAN22, and the sequence was assigned the GenBank accession number PV668598. Phylogenetic analysis showed clustering with previously reported African isolates. The CMV-positive neonate presented with microcephaly and small-for-gestational-age status. Although congenital CMV infection was rare in this cohort, molecular detection and genomic characterization provide valuable baseline data on CMV epidemiology in Nigeria and underscore the importance of continued surveillance and early diagnosis.
Keywords:
cytomegalovirus
; congenital infection
; neonates
; molecular epidemiology
; PCR
; Sanger sequencing
; phylogenetics
; Nigeria
1. Introduction
The human cytomegalovirus (HCM) is a DNA virus belonging to the beta herpesviridae family and also known as human herpesvirus-5 (HHV-5) with humans as its only natural hosts. (Zenebe et al. 2021), Shedding of the virus in body fluids is responsible for transmission which correlate with periods of active replication.(Lawrence et al. 2024; van der Sande et al. 2007; Zenebe et al. 2021) CMV is transmitted via contact with body secretions such as saliva, breast milk, blood, urine, semen and cervical secretions, (Zenebe et al. 2021).
Perinatal/postnatal phase of infection can occur at the time of foetal passage through the birth canal or immediately after birth due to exposure to infected cervical secretions, breast milk, or contact with traumatized vagina secretions and or blood. Newborns are commonly affected prenatally (congenital) through trans-placental acquisition of the virus either as a consequence of primary or a recurrent maternal infection with the worst sequelae associated with primary maternal infections(Ebrahim et al. 2015; Ebrahimi-Rad et al. 2017). The incubation period of the infection is about 2–3 weeks, after which shedding of the virus and detection in secretions such as urine, vaginal secretions and breast milk is possible. Congenital cytomegalovirus is the most common cause of congenital infections worldwide (0.2 to 2.2%), with substantial variation in developing countries (6 to 14% ) (Ross et al. 2011) (Fernandez et al. 2022). Some factors have been associated with poor neurodevelopmental prognosis among which are the presence of microcephaly, chorioretinitis, or neurological abnormalities at birth (Manicklal et al. 2013; Noyola et al. 2001). Cytomegalovirus retinitis is the most frequent ocular complication and is the main cause of visual loss in patients with AIDS, the immunosuppressed are at increased risk of complications, disability and mortality.
The socioeconomic background has significant effects on the epidemiology and clinical outcome of the infection, however very few data are available from developing countries where the overall burden of infectious diseases is frequently high (Marsico, Kimberlin, David W, and Kimberlin 2017). Congenital cytomegalovirus infection often goes undetected at birth on account that majority of affected children are asymptomatic or present with trivial symptoms that do not attract clinicians attention. Hence behavioral practical guidance such as personal hygiene are aimed at reducing the transmission of CMV to pregnant women (Korver et al. 2009; Marsico et al. 2017).
The commencement of antiviral therapy such as gancyclovir among other antiviral on symptomatic children with CNS manifestation is effective at reducing the risk of long-term disabilities and should be offered to families with affected newborns.(Elizabeth C. Swanson, DO and Mark R. Schleiss 2013).
Despite the known burden of congenital CMV and its long-term complications, there is a paucity of data on its seroprevalence in Nigeria, particularly in northern region including Jos. This gap in surveillance data puts limitations on early diagnosis and targeted interventions. Moreover, the utility of cord blood samples for early CMV detection is not routinely explored in our setting. This study aimed to determine the molecular prevalence of congenital CMV infection among neonates in Jos, North-Central Nigeria, and to characterize detected CMV strains using sequencing and phylogenetic analysis..
2. Materials and Methods
2.1. Study Design and Setting
This cross-sectional molecular study was conducted between January 2021 and December 2022 among neonates attending the Special Care Baby Unit and immunization units of three tertiary health facilities in Jos metropolis, Plateau State, Nigeria: Jos University Teaching Hospital (JUTH), Plateau State Specialist Hospital (PSSH), and Bingham University Teaching Hospital (BhUTH).
2.2. Study Population and Sample Size
Neonates aged ≤21 days presenting to the selected health facilities were eligible for inclusion. Written informed consent was obtained from parents or guardians prior to enrolment. Neonates were consecutively recruited, and no samples were excluded from analysis.
The minimum sample size was calculated using the formula
N = (Z2 × p × q × D) / d2,
where Z = 1.96 (95% confidence level), p = 0.038 (prevalence of congenital CMV infection reported by Olusanya et al., 2015), q = 1 − p, d = 0.05 (margin of error), and D = 2 (design effect). This yielded a minimum sample size of 112 neonates. To improve statistical power, the final sample size was increased to 180 neonates.
2.3. Data Collection
Sociodemographic, clinical, and maternal data were collected using a structured data collection form. Information obtained included neonatal sex, age, anthropometric measurements, clinical features, maternal demographic characteristics, and ward of recruitment.
2.4. Sample Collection and DNA Extraction
Buccal swab samples were collected under aseptic conditions by brushing the inner cheek with a sterile flocked swab. Samples were transported under cold-chain conditions to the molecular laboratory and stored at −80 °C until DNA extraction.
Genomic DNA was extracted using the Zymo-Spin™ IIC column–based protocol (Zymo Research, USA) in accordance with the manufacturer’s instructions. DNA was eluted in ≥50 µL of elution buffer and stored at −20 °C until polymerase chain reaction (PCR) analysis.
2.5. PCR Detection of Human Cytomegalovirus
Human cytomegalovirus (HCMV) DNA was detected using an in-house nested PCR assay targeting the glycoprotein B (gB) gene, employing primers adopted from previously published studies (Choudhary et al., 2015). The outer primer pair (gB1138/gB1638) amplified a 661-bp fragment, while the inner primer pair (gB1276/gB1524) produced a 249-bp fragment (Table 1).
PCR amplification was performed for 35 cycles under standard conditions. HCMV strain AD169 was included as a positive control, and nuclease-free water served as a negative control. PCR products were resolved on 1.5% agarose gel and visualized under ultraviolet illumination using a molecular size ladder.
2.6. Sequencing and Phylogenetic Analysis
Purified PCR products were subjected to Sanger sequencing using the ABI Prism BigDye Terminator v3.1 Cycle Sequencing Kit and analyzed on an ABI 3730/3730xl DNA Analyzer, following the manufacturer’s instructions. Sequence similarity analysis was performed using the Basic Local Alignment Search Tool (BLAST). Phylogenetic analysis was conducted using MEGA version 11. The generated nucleotide sequence was deposited in the GenBank database.
2.7. Statistical Analysis
Data were analyzed using standard statistical software. Continuous variables were summarized as means and standard deviations, while categorical variables were presented as frequencies and percentages. The molecular prevalence of congenital CMV infection was calculated with exact 95% confidence intervals using the Clopper–Pearson method. Due to the low number of PCR-positive cases, inferential statistical analyses were not performed, and results were reported descriptively.
2.8. Ethical Approval
Ethical approval for the study was obtained from the institutional ethics committees of the participating hospitals. Written informed consent was obtained from parents or guardians prior to enrolment. All data were anonymized to ensure participant confidentiality.
3. Results
3.1. Study Population Characteristics
Between January 2021 and August 2022, a total of 180 neonates aged ≤21 days were enrolled from three healthcare facilities in Jos, Nigeria: Jos University Teaching Hospital, Plateau State Specialist Hospital, and Bingham University Teaching Hospital. Of the enrolled neonates, 102 (56.7%) were male and 78 (43.3%) were female.
The majority of neonates (145/180; 80.6%) were aged 1–5 days, while 21 (11.7%) were aged 6–10 days, and 14 (7.8%) were older than 10 days. The age and sex distribution of the study population is summarized in Table 2.
3.2. Detection of Congenital CMV Infection and Maternal Characteristics
Out of the 180 neonatal samples analyzed, one neonate (0.6%) tested positive for CMV DNA by PCR. Owing to the presence of only a single PCR-positive case, statistical comparisons between CMV-positive and CMV-negative groups were not performed.
Maternal demographic characteristics, including age group, marital status, parity, occupation, educational level, and ward of recruitment, are therefore presented descriptively according to neonatal CMV PCR status in Table 3. The CMV-positive neonate was born to a mother aged ≤25 years, in a monogamous marriage, with parity of 1–2, secondary education, and recruited from the Special Care Baby Unit (SCBU).
3.3. Molecular Detection of CMV
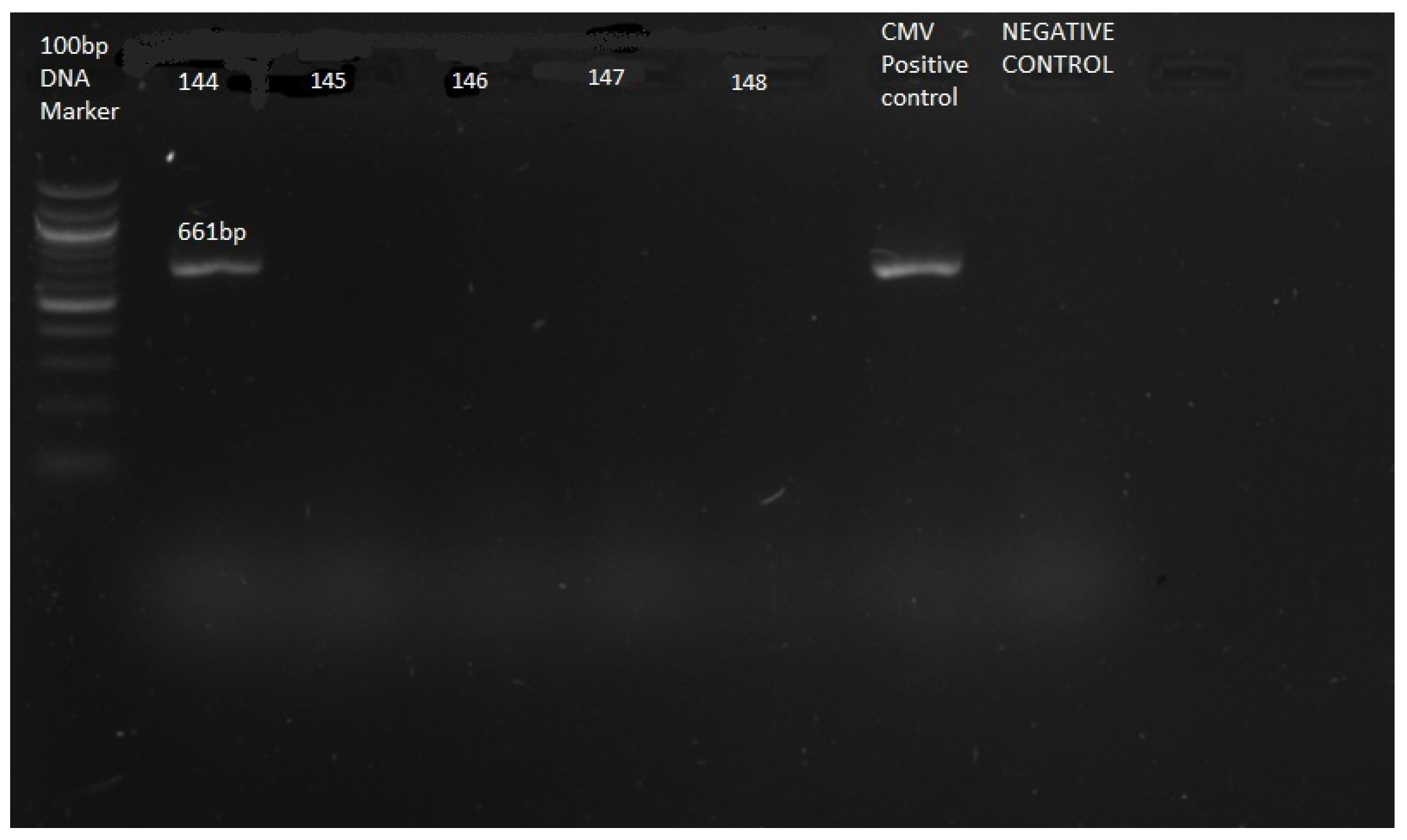
PCR amplification targeting the cytomegalovirus glycoprotein B (gB) gene yielded a positive result in one sample (Sample 144). Agarose gel electrophoresis demonstrated a distinct band at approximately 661 bp, corresponding to the expected size of the outer PCR amplicon. No amplification was observed in the remaining samples or in the negative control (Plate 1).
Figure 1.
Gel electrophoresis of CMV. Agarose gel electrophoresis of CMV gB gene PCR products. Lane M: molecular weight marker; Lane 144: CMV-positive sample showing a band at 661 bp; Lanes 145–148: CMV-negative samples.
Figure 1.
Gel electrophoresis of CMV. Agarose gel electrophoresis of CMV gB gene PCR products. Lane M: molecular weight marker; Lane 144: CMV-positive sample showing a band at 661 bp; Lanes 145–148: CMV-negative samples.
3.4. Sequence Analysis and Phylogenetic Characterization
The CMV-positive PCR product was successfully sequenced using the Sanger method. BLAST analysis of the nucleotide sequence showed 98.9% similarity to Human herpesvirus 5 strain HAN22. The sequence was deposited in GenBank under the accession number PV668598.
Phylogenetic analysis performed using MEGA version 11 revealed that the study isolate clustered within the HAN22 lineage, showing close genetic relatedness to CMV strains previously reported from southern Africa, including Zambia. In the phylogenetic tree, the study sequence is labeled “ISOLATE BELLO” to distinguish it from reference strains (Figure 1).
Figure 1.
Neighbor-joining phylogenetic tree based on CMV gB gene sequences showing the relationship between Isolate Bello and reference Human herpesvirus 5 strains.
Figure 1.
Neighbor-joining phylogenetic tree based on CMV gB gene sequences showing the relationship between Isolate Bello and reference Human herpesvirus 5 strains.

4. Discussion
This study provides molecular evidence of congenital CMV infection (Adrien et al. 2016) among neonates in Jos, Nigeria, with a low prevalence detected using PCR furthermore the observed prevalence is comparable to findings from other regions including the country of study with a low prevalence. Notably, the prevalence reported in this study is lower than that observed in a pilot study conducted in Lagos by Olusanya and colleagues, who reported a prevalence of 3.8% using PCR (Olusanya, Slusher, and Boppana 2015). However the value obtained in this study falls within the range obtained in a review by Lanzieri and colleagues from Africa, Asia, and Latin America were they found out that the prevalence using PCR varied from 0.6% in Panama to 6.1% in China (Lanzieri et al. 2014; van der Sande et al. 2007), and 0.2–2.0% most often reported for developed countries (Lanzieri et al. 2014).
Differences in maternal seroepidemiology, (Moglad et al. 2023) diagnostic approaches, and specimen types may partly explain this variability.(Ramchandar et al. 2020)
Importantly, this study demonstrates the feasibility of sentinel molecular surveillance for congenital CMV infection in resource-limited settings, aligning with previously identified priorities and opportunities for improving surveillance of congenital infections in such contexts.(Roilides, Ladhani, and Syrogiannopoulos 2023)
The strain identified in this study Human herpesvirus 5 strain HAN22, showed a high degree of genetic similarity (98.9% molecular identity) to previously reported CMV strains. Human cytomegalovirus is known to exhibit considerable genetic diversity, which may contribute to the emergence of variants with distinct genetic characteristics (Ross et al. 2020, Variation 2016). Available evidence suggests that common CMV strains can circulate within specific geographical regions over relatively short periods, while no single strain appears to be uniquely restricted to a particular region (Scarborough, Scarborough, and Sikes 2016; Variation 2016). The genetic relatedness of the detected strain to a Southern African lineage underscores the need for broader regional genomic surveillance (Charles 2023).
The absence of routine congenital CMV screening in most country including Nigeria likely contributes to underestimation of disease burden. (Payne and Barnabas 2024)These findings support the need for structured surveillance and targeted screening strategies, particularly for high-risk neonates.(Berkovitz 2024)
Future studies should adopt a multicenter design with larger sample sizes across different regions of Nigeria to better define the epidemiology, transmission dynamics, and genetic diversity of congenital CMV infection.
5. Conclusions
Congenital CMV infection was not common among neonates in this study from Jos, Nigeria. However, molecular detection and genomic characterization of CMV contribute important baseline data and highlight the need for continued surveillance and early diagnostic strategies in resource-limited settings.
Limitations and Strengths
The low number of CMV-positive cases limited inferential statistical analysis. The use of buccal swab specimens may have reduced diagnostic sensitivity compared with urine or saliva samples. Nevertheless, the strengths of this study include molecular confirmation of infection, sequencing with phylogenetic analysis, focus on early neonatal life, and the study contributed to a Nigerian CMV sequence in public databases.
Institutional Review Board Statement
The Ethical approval was obtained from the institutional ethics committees of the three participating hospitals (Jos university teaching Hospital, plateau state specialist hospital and Bingham University Teaching Hospital with ethical numbers JUTH/DCS/IREC/1274/XXXI/2374, NHREC/09/23/2010b and NHREC/21/05/2005/00875 respectively). A written informed consent was obtained from parents or guardians prior to enrolment. Confidentiality and anonymity of participants were strictly maintained.
Acknowledgments
We sincerely thank Dr. D.Z. Egah and Dr. E.B. Banwat for their unwavering support, motivation, and invaluable contributions. We also appreciate the guidance of Dr. M. Okolo, Head of the Department of Medical Microbiology at the time the study was conducted, for granting us access to the JUTH laboratory.
Conflicts of Interest
The authors declare no conflict of interest in this article.
Abbreviations
The following abbreviations are used in this manuscript:
| HCMV | Human Cytomegalovirus |
| BLAST | Basic Local Alignment Search Tool |
| BUTH | Bingham University Teaching Hospital |
| CMV | Cytomegalovirus |
| DNA | Deoxyribonucleic Acid |
| gB | Glycoprotein B |
| HHV-5 | Human Herpesvirus 5 |
| JUTH | Jos University Teaching Hospital |
| MEGA | Molecular Evolutionary Genetics Analysis |
| PCR | Polymerase Chain Reaction |
| PSSH | Plateau State Specialist Hospital |
| SCBU | Special Care Baby Uni |
References
- Adrien, Paul, Paul Jacques Boncy, Jean Frantz Lemoine, Alexandre Existe, Stanley Juin, Sénou Amouzou, Gabriel Thimoté, Lesly Liverdieu Andrécy, Samson Marseille, Patrick Dély, Wilnique Pierre, Robert Barais, Corvil Salomon, Mentor Lucien, Lottie Mondésir, Khulood Rizvi, Dana M Parke, and Marcus J Zervos. Malaria Elimination in Haiti: Challenges, Progress and Solutions. Clinical Microbiology and Infectious Diseases 2016, 1(2), 67–69. [CrossRef]
- Berkovitz, Shahar. 2024. “Congenital CMV Screening Strategies.” 1–10.
- Binder, Thomas, Wolfgang Siegert, Anja Kruse, and Helmut Oettle. 1999. “Identification of Human Cytomegalovirus Variants by Analysis of Single Strand Conformation Polymorphism and DNA Sequencing of the Envelope Glycoprotein B Gene Region-Distribution Frequency in Liver Transplant Recipients.” 78:153–62.
- Charles, Oscar J. 2023. “Genomic and Geographical Structure of Human Cytomegalovirus.” 1–11. [CrossRef]
- Choudhary, A., S. K. Pati, R. K. Patro, A. K. Deorari, and L. Dar. Comparison of Conventional, Immunological and Molecular Techniques for the Diagnosis of Symptomatic Congenital Human Cytomegalovirus Infection in Neonates and Infants. Indian Journal of Medical Microbiology 2015, 33, S15–S19. [CrossRef] [PubMed]
- Ebrahim, Maha G., Aisha S. Ali, Mohamed O. Mustafa, Dalal F. Musa, Abdel Rahim M. El Hussein, Isam M. Elkhidir, and Khalid A. Enan. Molecular Detection of Human Cytomegalovirus (HCMV) Among Infants with Congenital Anomalies in Khartoum State, Sudan. The Open Virology Journal 2015, 9(1), 38–41. [CrossRef] [PubMed]
- Ebrahimi-Rad, Mina, Talayeh Seyed Shakeri, Fariba Shirvani, Kiana Shahrokhi, and Nader Shahrokhi. Prevalence of Congenital Cytomegalovirus Infection in Symptomatic Newborns under 3 Weeks in Tehran, Iran. BMC Infectious Diseases 2017, 17(1), 1–7. [CrossRef]
- Elizabeth C. Swanson, DO and Mark R. Schleiss, Md. 2013. “Congenital Cytomegalovirus Infection: New Prospects for Prevention and Therapy. Congenital Cytomegalovirus Infection: Current Strategies and Future Perspectives. Antiviral Treatment of Cytomegalovirus Infection.” Pediatr Clin North Al 60(2):1–17. [CrossRef]
- Fernandez, Catarina, Maria Jesus Chasqueira, Augusta Marques, Lúcia Rodrigues, Mónica Marçal, Madalena Tuna, Mónica Cró Braz, Ana Serrão Neto, Cândida Mendes, David Lito, Paula Rocha, Gabriela Vasconcellos, Maria Favila Menezes, Maria José Sousa, Carla Nunes, and Paulo Paixão. Lower Prevalence of Congenital Cytomegalovirus Infection in Portugal: Possible Impact of COVID-19 Lockdown? European Journal of Pediatrics 2022, 181(3), 1259–1262. [CrossRef]
- Korver, A. M. H., J. J. C. de Vries, J. W. de Jong, F. W. Dekker, A. C. T. M. Vossen, and A. M. Oudesluys-Murphy. Awareness of Congenital Cytomegalovirus among Doctors in the Netherlands. Journal of Clinical Virology 2009, 46 (SUPPL. 4). [CrossRef]
- Lanzieri, Tatiana M., Sheila C. Dollard, Stephanie R. Bialek, and Scott D. Grosse. Systematic Review of the Birth Prevalence of Congenital Cytomegalovirus Infection in Developing Countries. International Journal of Infectious Diseases 2014, 22, 44–48. [CrossRef]
- Lawrence, Shelley M., Tyler Goshia, Mridu Sinha, Stephanie I. Fraley, and Marvin Williams. Decoding Human Cytomegalovirus for the Development of Innovative Diagnostics to Detect Congenital Infection. Pediatric Research 2024, 95(2), 532–542. [CrossRef]
- Manicklal, Sheetal, Vincent C. Emery, Tiziana Lazzarotto, Suresh B. Boppana, and Ravindra K. Gupta. The ‘Silent’ Global Burden of Congenital Cytomegalovirus. Clinical Microbiology Reviews 2013, 26(1), 86–102. [CrossRef]
- Marsico, Concetta, Concetta Kimberlin, David W, and David W. Kimberlin. Congenital Cytomegalovirus Infection: Advances and Challenges in Diagnosis, Prevention AnCongenital Cytomegalovirus Infection: Advances and Challenges in Diagnosis, Prevention and Treatmentd Treatment. Italian Journal of Pediatrics 2017, 43(1), 1–8.
- Moglad, Ehssan H., Ahmed O. Hassan, Mawada S. Atta Elmanan, Samar M. Saeed, Mohammed Siddig, A. B. D. Elaziz, and Hind Haidar Ahmed. 2023. “Seroepidemiological Survey of Cytomegalovirus Infection among Pregnant Women in Sudan.” 72(3):269–75.
- Noyola, Daniel E., Gail J. Demmler, Christopher T. Nelson, Carol Griesser, W. Daniel Williamson, Jane T. Atkins, Judith Rozelle, Marie Turcich, Antolin M. Llorente, Sherry Sellers-Vinson, Ann Reynolds, James F. Bale, Paul Gerson, and Martha D. Yow. Early Predictors of Neurodevelopmental Outcome in Symptomatic Congenital Cytomegalovirus Infection. Journal of Pediatrics 2001, 138(3), 325–331. [CrossRef]
- Olusanya, Bolajoko O., Tina M. Slusher, and Suresh B. Boppana. Prevalence of Congenital Cytomegalovirus Infection in Nigeria: A Pilot Study. Pediatric Infectious Disease Journal 2015, 34(3), 322–324. [CrossRef]
- Payne, Helen, and Shaun Barnabas. “Congenital Cytomegalovirus in Sub-Saharan Africa — a Narrative Review with Practice Recommendations.” (May). 2024. [CrossRef]
- Ramchandar, Nanda, Yan Ding, Lauge Farnaes, David Dimmock, Charlotte Hobbs, Stephen F. Kingsmore, and Matthew Bainbridge. Diagnosis of Cytomegalovirus Infection from Clinical Whole Genome Sequencing. Scientific Reports 2020, 10(1), 1–6. [CrossRef]
- Roilides, Editors Emmanuel, Shamez Ladhani, and George Syrogiannopoulos. 2023. “Congenital Infections: Priorities and Possibilities for Resource-Limited Settings.” 42(2):2022–24. [CrossRef]
- Ross, Shannon A., Zdenek Novak, Sunil Pati, Raj Kumar Patro, Jennifer Blumenthal, Vishwanath R. Danthuluri, Amina Ahmed, Marian G. Michaels, Pablo J. Sánchez, David I. Bernstein, Robert W. Tolan, April L. Palmer, William J. Britt, Karen B. Fowler, and Suresh B. Boppana. Mixed Infection and Strain Diversity in Congenital Cytomegalovirus Infection. Journal of Infectious Diseases 2011, 204(7), 1003–1007. [CrossRef]
- Ross, Shannon A., Pravasini Pati, Travis L. Jensen, Johannes B. Goll, Casey E. Gelber, Amy Singh, Monica McNeal, Suresh B. Boppana, and David I. Bernstein. Cytomegalovirus Genetic Diversity Following Primary Infection. Journal of Infectious Diseases 2020, 221(5), 715–720. [CrossRef]
- van der Sande, Marianne A. B., Steve Kaye, David J. C. Miles, Pauline Waight, David J. Jeffries, Olubukola O. Ojuola, Melba Palmero, Margaret Pinder, Jamila Ismaili, Katie L. Flanagan, Akum A. Aveika, Akram Zaman, Sarah Rowland-Jones, Samuel J. McConkey, Hilton C. Whittle, and Arnaud Marchant. Risk Factors for and Clinical Outcome of Congenital Cytomegalovirus Infection in a Peri-Urban West-African Birth Cohort. PLoS ONE 2007, 2(6). [CrossRef]
- Scarborough, Jessica A., Jessica Scarborough, and James Sikes. 2016. “Phylogenetic Analysis of Human Cytomegalovirus PUS27 and PUS28: Ascertaining an Independent or Linked Evolutionary History Ascertaining an Independent or Linked Evolutionary History”.
- Variation, Strain. 2016. “HHS Public Access.” 29(3):401–14. [CrossRef]
- Zenebe, Mengistu Hailemariam, Zeleke Mekonnen, Eskindir Loha, and Elizaveta Padalko. Congenital Cytomegalovirus Infections Mother-Newborn Pair Study in Southern Ethiopia. Canadian Journal of Infectious Diseases and Medical Microbiology 2021. [CrossRef]

Table 1.
Primers used for nested PCR amplification of the HCMV gB gene.
| Name | Sequence (5′→3′) | Type | Strand | Amplicon Size |
|---|---|---|---|---|
| gB 1138 | CAAGARGTGAACATGTCCGA | Outer primer | Sense | 661 bp |
| gB 1638 | GTCACGCAGCTGGCCAG | Outer primer | Antisense | |
| gB 1276 | GGTTTGGTGGTGTTCTGGCA | Inner primer | Sense | 249 bp |
| gB 1524 | CACACACCAGGCTTCTGCGA | Inner primer | Antisense |
Primers were adopted from previously published studies. (Choudhary et al. 2015).
Table 2.
Age and Sex Distribution of Neonates in Jos Metropolis.
| Age | Sex | Total | Percent | |
|---|---|---|---|---|
| Male | Female | |||
| 1-5 | 85(58.6) | 60(41.4) | 145 | 80.6 |
| 6-10 | 6( 28.6) | 15(71.4) | 21 | 11.7 |
| >10 | 11(78.6) | 3(21.4) | 14 | 7.8 |
| Total | 102(56.7) | 78(43.3) | 180 | 100.0 |
Table 3.
Distribution of Maternal Demographic Characteristics According to Neonatal CMV PCR Status.
| Maternal Characteristic | CMV PCR Positive (n=1) | CMV PCR Negative (n=179) | Total |
|---|---|---|---|
| Age group (years) | |||
| ≤25 | 1 | 30 | 31 |
| 26–30 | 0 | 65 | 65 |
| 31–35 | 0 | 68 | 68 |
| ≥35 | 0 | 16 | 16 |
| Marital status | |||
| Monogamous | 1 | 151 | 152 |
| Polygamous | 0 | 28 | 28 |
| Parity | |||
| 1–2 | 1 | 99 | 100 |
| 3–4 | 0 | 60 | 60 |
| ≥5 | 0 | 20 | 20 |
| Occupation | |||
| Housewife | 1 | 80 | 81 |
| Business | 0 | 42 | 42 |
| Civil servant | 0 | 33 | 33 |
| Tailor | 0 | 6 | 6 |
| Student | 0 | 8 | 8 |
| Others | 0 | 10 | 10 |
| Education level | |||
| Primary | 0 | 20 | 20 |
| Secondary | 1 | 75 | 76 |
| Tertiary | 0 | 84 | 84 |
| Ward of recruitment | |||
| SCBU | 1 | 140 | 141 |
| Immunization | 0 | 28 | 28 |
| Postnatal | 0 | 10 | 10 |
| Delivery | 0 | 1 | 1 |
Note: Statistical association testing was not performed due to the presence of only one PCR-positive case.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



