Submitted:
21 January 2026
Posted:
22 January 2026
You are already at the latest version
Abstract
Introduction: Acute kidney injury (AKI) is defined as an increase in creatinine level with a possible decrease in urine output. Oxalate nephropathy (ON) is an uncommon cause of AKI in children. We report a case of oliguric AKI secondary to ON following exposure to an organic hair treatment product. To our knowledge, no similar pediatric cases have been reported in Saudi Arabia. This case aims to raise awareness of the potential adverse renal effects of cosmetic products among consumers and pediatricians. Case Presentation: An 8-year-old girl presented with a two-day history of facial swelling, abdominal distension, vomiting, decreased urine output, and hypertension after using an organic hair treatment product. She had a recent upper respiratory tract infection. Examination revealed mild ascites, and laboratory tests showed markedly elevated serum creatinine. She was admitted to the Pediatric Intensive Care Unit with an impression of severe oliguric AKI for further evaluation and management. Treatment included fluids, electrolyte correction, diuretics, and antihypertensive therapy, resulting in clinical stabilization. Renal biopsy showed acute tubular necrosis with calcium oxalate crystal deposition, confirming ON. Conclusion: Hair-straightening products may be associated with oxalate nephropathy. Further studies are warranted to identify nephrotoxic chemicals in hair products and reduce potential health risks.
Keywords:
acute kidney injury
; oxalate nephropathy
; hair-straightening products
; kidney biopsy
; case report
Introduction
Acute kidney injury (AKI) is a growing issue in the pediatric population [1]. A multinational study on pediatric AKI, involving 4,683 children, has reported that the incidence rate is 26.9% [1]. AKI is a pathological condition in which the kidneys fail to function properly, leading to a decrease in estimated glomerular filtration rate (eGFR), accumulation of waste products such as blood urea nitrogen (BUN), and imbalances in extracellular fluid and electrolytes [1]. It is also defined as an increase in serum creatinine level with a possible decrease in urine output according to the Kidney Disease Improving Global Outcomes (KDIGO) Guideline, as shown in Table 1 [2]. The etiology of AKI is classified into three groups based on the anatomical location of the original injury: prerenal, renal, and postrenal [3]. Most patients exhibit symptoms related to the cause of AKI rather than the clinical signs of renal damage; however, those with severe kidney function impairment might present with edema, hypertension, and decreased urine production, and some children present with signs of shock [3]. The KDIGO system is considered a diagnostic criteria for AKI; however, the baseline serum creatinine level of patients is frequently unknown [1]. Therefore, an alternative diagnostic tool is the patient history, physical examination, laboratory tests, imaging of the urinary tract, and renal biopsy in rare cases [4]. Generally, AKI is managed with intravenous (IV) fluid, diuretic medications, and electrolyte correction depending on the patient’s volume status, whether the patient is hypovolemic, euvolemic, or hypervolemic [4]. Approximately 19% of AKI patients required renal replacement therapy, with peritoneal dialysis being the most frequently used modality [3]. Additionally, certain patients require antihypertensive medications for persistent hypertension or inotropic support if they develop hypovolemic shock [4]. In this report, we describe the case of a young girl who presented to our emergency department with a two-day history of facial swelling and abdominal distension following the use of an unidentified organic hair treatment product. Renal biopsy findings revealed acute calcium oxalate crystal nephropathy, which was attributed to exposure to the hair treatment product. To our knowledge, Oxalate nephropathy (ON) secondary to exposure to hair-straightening products is a well-recognized cause of AKI in adults; however, this is the first published case related to a pediatric patient in Saudi Arabia. Our aim is to raise awareness among consumers and pediatricians about the potential adverse effects of cosmetic products.
Case Presentation
An 8-year-old Saudi girl, previously healthy and up to date on vaccinations, who was brought to our pediatrics emergency room (ER) with a two-day history of facial swelling and abdominal distention following the use of an unknown organic hair treatment product. The facial edema was accompanied by a burning sensation in the scalp and behind the ears, while the abdominal distention was generalized and not associated with pain. Additional symptoms included nausea, vomiting, decreased urine output, and a 3-kg weight gain. The patient also had a recent history of pharyngitis over the past two weeks. There was no history of exposure to nephrotoxic medications, such as nonsteroidal anti-inflammatory drugs (NSAIDs), or food allergies, including fish and shrimp. She denied any dizziness, headache, or blurred vision. The patient did not notice any changes in the color or odor of her urine, nor did she report any history of joint or muscle pain or skin rashes. Before visiting our ER, the patient’s family sought medical care at another hospital, where she was treated with an epinephrine injection for a suspected allergic reaction; however, no improvement was observed. She then visited a second hospital, where her blood pressure was recorded as elevated (141/84 mmHg) along with an abnormal renal profile. At that point, she was referred to our ER for further investigation and management. The remainder of her medical history was unremarkable. Upon general examination, the patient’s face was edematous with erythema in the scalp and behind the ears. Her weight was 33.5 kg, placing her at the 95th percentile, while her height was appropriate for her age and gender based on the World Health Organization (WHO) chart. The blood pressure was elevated (136/85 mmHg), above the 95th percentile, while the other vital signs were within normal limits. On systemic physical examination, the patient had mild abdominal ascites; however, the abdomen was soft and lax with no organomegaly. The skin appeared healthy, with no evidence of rashes, lesions, or discoloration. There were no signs of trauma, infection, or allergic reaction. A nephrology consultation was performed in our ER, and several laboratory tests were recommended, including a complete blood count (CBC), peripheral blood smear, renal function tests (RFT), urine protein-to-creatinine ratio, anti-streptolysin O (ASO) titer, bone profile, antinuclear antibody (ANA), anti-double-stranded DNA (anti-dsDNA), complement proteins C3 and C4, lactate dehydrogenase (LDH), and liver function test. The renal profile revealed a significant increase in creatinine (574.85 µmol/L) and blood urea nitrogen (BUN) (30.6 mmol/L), along with elevated phosphorus levels. At that time, the patient was receiving IV fluids cautiously and diuretic medication. She was then admitted to the Pediatric Intensive Care Unit (PICU) with the impression of severe oliguric AKI secondary to post-streptococcal glomerulonephritis, which might have been triggered by upper respiratory tract infection (URTI) or toxic nephropathy secondary to hair product application. During her PICU stay, we closely monitored the AKI and electrolyte disturbances through frequent renal profile and electrolyte tests. The second RFT showed worsening kidney function, with creatinine rising to 590 µmol/L and BUN to 32.7 mmol/L. Repeated electrolyte tests revealed hyperkalemia, hyperphosphatemia, hyponatremia, hypochloremia, and hypocalcemia. To manage the oliguria, we initially restricted her fluid intake and then gradually increased it to maintain adequate renal perfusion. She was also given oral kayexalate, sevelamer, sodium chloride, and calcium carbonate. As her blood pressure remained above the 95th percentile, the nephrology team added amlodipine with IV labetalol. Based on the laboratory test results, we ruled out post-infectious glomerulonephritis, as the patient had a negative ASO titer, normal C3 level, and a negative urinalysis. Lupus nephritis was also excluded due to negative ANA and anti-dsDNA tests. Furthermore, the patient did not meet the full diagnostic criteria for hemolytic uremic syndrome (HUS), which includes thrombocytopenia, microangiopathic hemolytic anemia, and AKI. The urine protein-to-creatinine ratio showed no evidence of proteinuria, and the urine culture was negative. On the third day of admission, after stabilization with improved kidney function, corrected electrolytes, controlled blood pressure, and symptom relief, the patient was transferred from the PICU to the pediatric ward to prepare for a renal biopsy, as the cause of AKI remained unknown. Serum creatinine and BUN levels began to decrease on day four and improved significantly by day seven, as shown in Chart 1. An imaging-guided percutaneous kidney biopsy was performed on day ten, the earliest available appointment. Based on the histopathology result, we concluded that the patient had acute tubular necrosis (ATN) due to ON after using the organic hair treatment, as shown in Figure 1. The patient was discharged on oral amlodipine and scheduled for nephrology follow-up to monitor kidney function and blood pressure. During follow-up, her kidney function gradually improved and returned to normal within one month of admission. Her antihypertensive medication was discontinued after her blood pressure normalized.
Discussion
Oxalate nephropathy (ON) is a pathological syndrome in which calcium oxalate (CaOx) crystals are formed in kidney tubules, leading to renal function impairment [5]. The main cause of ON is hyperoxaluria, which can be classified as either primary or secondary [6]. Primary hyperoxaluria (PH) is a group of autosomal recessive genetic disorders characterized by the overproduction of endogenous hepatic oxalate due to accumulation of the oxalate glyoxylate precursor [6].
It is also considered an inborn metabolic error caused by a deficiency in specific enzymes, which can be divided into three types: PH1, 2, and 3 [7]. Secondary hyperoxaluria is more common than PH, and its causes include a high intake of oxalate or oxalate precursor foods, fat malabsorption, and decreased oxalate breakdown in the intestine due to flora alterations ( Table 2) [8]. Oxalate metabolism remains unclear, but studies indicate that 60–80% of oxalate originates from the glyoxylate pathway in the liver and food consumption [8]. In the gut, oxalate binds to calcium for excretion in stool and decomposes via intestinal bacteria [8]. Approximately 5–15% of oxalate is absorbed into the plasma, and the kidneys rapidly eliminate it because it has no clear function in the human body [7]. Literature reviews have reported that acute oxalate nephropathy causes renal failure following the excessive consumption of starfruit [7]. Moreover, several cases of ON linked to vitamin C ingestion have been published [7]. In this case, we identified the use of hair treatment in children as an additional cause of secondary hyperoxaluria. Although our patient’s organic hair product was vague, we thought it contained the same toxic compounds of hair-straightening treatment that have been linked in the literature reviews to crystal-induced nephropathy. Studies have found that glycolic acid is used in keratin treatment instead of formaldehyde, and both substances can be harmful to the kidneys [9]. After systemic absorption of a hair straightening treatment, glycolic acid is oxidized to glyoxylic acid by the glycolate oxidase enzyme in hepatocytes [8]. Glyoxylic acid can be further metabolized to oxalic acid by lactate dehydrogenase. Oxalic acid then dissociates to form oxalate ions that can precipitate as calcium oxalate crystals within the renal parenchyma and tubules [9]. Children with ON may develop AKI, chronic kidney disease (CKD), or end-stage renal disease (ESRD) [8]. Our patient presented with AKI stage 3 according to the KDIGO guidelines. In 2023, a retrospective case series of AKI and hair-straightening products was conducted in 14 Israeli medical centers, and it was found that 26 patients experienced severe AKI following a hair-straightening procedure [10]. The patients also complained of nausea, vomiting, and abdominal pain, and 10 of them had a scalp rash [10]. Following kidney biopsy, the results showed that 6 patients had calcium oxalate deposits in the renal tubes and 1 patient in the kidney tubules [9]. ON is a histopathological diagnosis [5]. Management includes fluid intake, a diet with low oxalate and fat, and supplements such as calcium and sodium bicarbonate to lower the plasma and urine oxalate concentrations [10]. Furthermore, we consider treating kidney injury and its underlying causes [10]. We treated our patient with a low-oxalate and low-fat diet, addressing AKI with limited fluid intake, lasix, and electrolyte correction. Our patient did not require dialysis because her renal profile showed improvement from day three.
Conclusions
Hair-straightening products containing glycolic acid and formaldehyde are associated with ON. A limitation of our case is that we did not perform toxicological screening. Therefore, further studies on the toxic chemicals in hair are required to prevent their use. Furthermore, campaigns can play a role in educating the pediatric population about the risks of using these products and encouraging safer alternatives.
Funding Sources
There was no financial support available for this case report.
Conflicts of Interest Statement
The authors have no conflicts of interest to declare.
Author Contributions
Conceptualization and case design, A.J. and A.A.; clinical data collection and patient management, A.J., A.A., F.A., Y.A., A.Q., L.A. and S.A.; data interpretation, A.J. and A.A.; writing—original draft preparation, A.J.; writing—review and editing, A.J., A.A., F.A., A.Q., L.A., J.A. and S.A.; supervision, A.A. All authors have read and approved the final manuscript.
Institutional Review Board Statement
This case report was reviewed and approved by the Research Committee of Maternity and Children Hospital in Al-Ahsa (approval number [0604-EP-2025]. Written informed consent was obtained from participants’ parents.
Data Availability Statement
The data supporting the findings of this case report are available from the corresponding author upon reasonable request, with appropriate consideration of patient privacy.
Acknowledgments
We thank the medical team involved in the patient’s care and the pathology department for their diagnostic support. We also appreciate the patient and her family for their cooperation and consent to share this case.
Abbreviations
The following abbreviations are used in this manuscript:
AKI Acute kidney injury
ON Oxalate nephropathy
eGFR estimated glomerular filtration rate
BUN Blood urea nitrogen
KDIGO Kidney Disease Improving Global Outcomes
IV Intravenous
ER Emergency room
NSAIDs Nonsteroidal anti-inflammatory drugs
WHO World Health Organization
CBC Complete blood count
RFT Renal function tests
ASO Anti-streptolysin O
ANA. Antinuclear antibody
Anti-dsDNA Anti-double-stranded DNA
LDH lactate dehydrogenase
PICU Pediatric Intensive Care Unit
URTI Upper respiratory tract infection
HUS Hemolytic uremic syndrome
ATN Acute tubular necrosis
CaOx Calcium oxalate
PH Primary hyperoxaluria
CKD Chronic kidney disease
ESRD end-stage renal disease
References
- Kopac, M. Acute Kidney Injury in Children: Classification, Recognition and Treatment Principles. Children 2024, 11(11), 1308. [Google Scholar] [CrossRef] [PubMed]
- Alayed, T; Alansary, A; Al-Nahdi, M; Alotaibi, A; Alhuthil, R; Al Abdulsalam, M; et al. Incidence, outcomes, and mortality risk factors of acute kidney injury in critically ill children: a tertiary care center study in Saudi Arabia. Annals of Saudi Medicine 2025, 45(1), 62–68. [Google Scholar] [CrossRef] [PubMed]
- Bai, S; Moorani, K; Naeem, B; Ashfaq, M; Rajesh, R; Rehman, E. Etiology, clinical profile, and short-term outcome of children with acute kidney injury. Cureus 2022, 14(2), e22563. [Google Scholar] [CrossRef] [PubMed]
- Rivetti, G; Gizzone, P; Petrone, D; Sessa, A; Giudice, E; Guarino, S. Acute Kidney Injury in Children: A Focus for the General Pediatrician. Children 2024, 11(8), 1004. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, J; Joab, T; DeVita, M; Yang, Y; Sharma, P; Bijol, V. Oxalate nephropathy: a review. Clinical Kidney Journal 2022, 15(2), 194–204. [Google Scholar] [CrossRef] [PubMed]
- Bao, D; Wang, Y; Zhao, M. Oxalate Nephropathy and the Mechanism of Oxalate-Induced Kidney Injury. Kidney Diseases 2023, 9(6), 459–468. [Google Scholar] [CrossRef] [PubMed]
- Shee, K; Stoller, M. Perspectives in primary hyperoxaluria: Historical, current, and future clinical interventions. Nature Reviews Urology 2021, 19(3), 137–146. [Google Scholar] [CrossRef] [PubMed]
- Demoulin, N; Aydin, S; Gillion, V; Morelle, K; Jadoul, M. Pathophysiology and Management of Hyperoxaluria and Oxalate Nephropathy: A Review. American Journal of Kidney Diseases 2021, 79(5), 717–727. [Google Scholar] [CrossRef] [PubMed]
- Huber, A; Deffert, C; Moll, S; Seigneux, S; Berchtold, L. Acute Kidney Injury and Hair-Straightening Products. Kidney International Reports 2024, 9(8), 2571–2573. [Google Scholar] [CrossRef] [PubMed]
- Bnaya, A; Abu-Amer, N; Beckerman, P; Volkov, A; Cohen-Hagai, K; Greenberg, M; et al. Acute kidney injury and hair straightening products: A case series. American Journal of Kidney Diseases 2023, 82(1), 43–52. [Google Scholar] [CrossRef] [PubMed]
Chart 1.
The trend of serum creatinine and BUN levels during hospitalization.
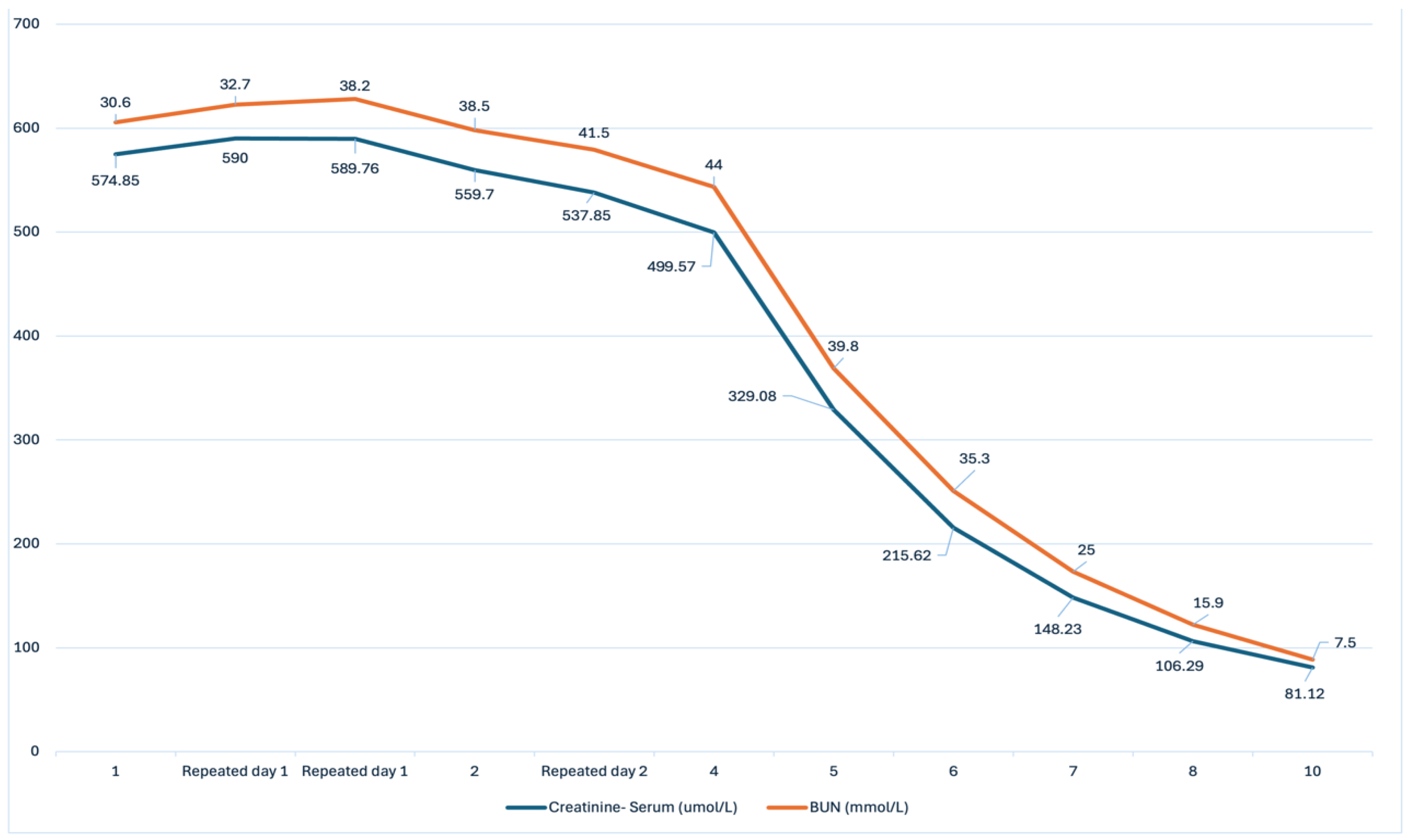
Figure 1.
Kidney biopsy samples of oxalate nephropathy. a: Oxalate nephropathy under a light microscope (hematoxylin and eosin stain x 100). b: Under a light microscope (hematoxylin and eosin stain x 200), we observed the deposition of gray crystal substances in the kidney tubules, identified as calcium oxalate (white arrows), and the flattening of epithelial cells with the loss of their brush borders (black arrow). c: Oxalate nephropathy under the polarized light microscopy (hematoxylin and eosin stain x 100). d: On the polarized light microscopy (hematoxylin and eosin stain, x 200), calcium oxalate crystals appear as birefringent (white arrow).
Figure 1.
Kidney biopsy samples of oxalate nephropathy. a: Oxalate nephropathy under a light microscope (hematoxylin and eosin stain x 100). b: Under a light microscope (hematoxylin and eosin stain x 200), we observed the deposition of gray crystal substances in the kidney tubules, identified as calcium oxalate (white arrows), and the flattening of epithelial cells with the loss of their brush borders (black arrow). c: Oxalate nephropathy under the polarized light microscopy (hematoxylin and eosin stain x 100). d: On the polarized light microscopy (hematoxylin and eosin stain, x 200), calcium oxalate crystals appear as birefringent (white arrow).
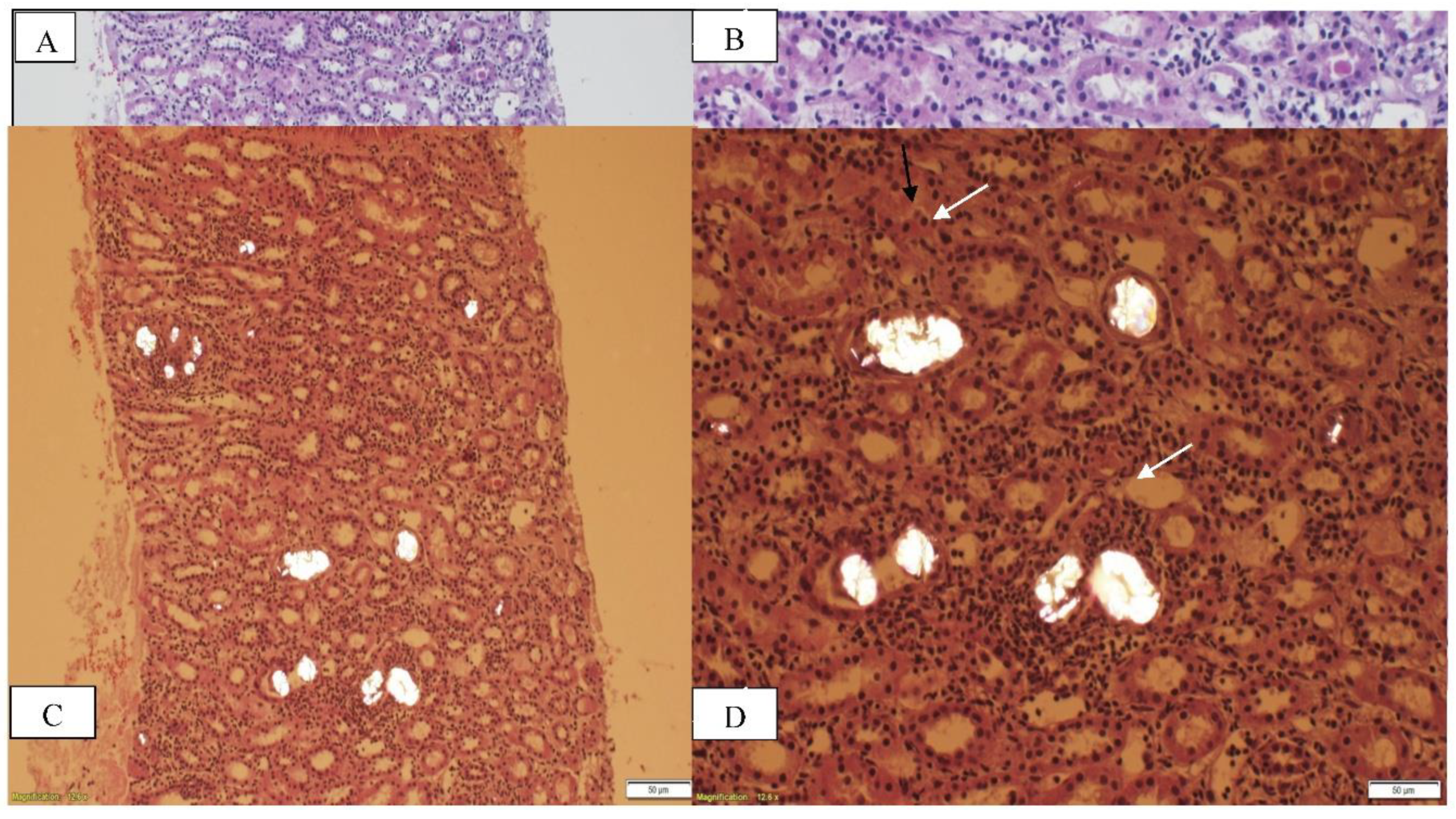

Table 1.
KDIGO Staging of AKI.
| AKI Stage | Serum Creatinine | Urine Output |
| 1 | The serum creatinine increases from the patient’s baseline 1.5-1.9 times or ≥ 0.3 mg/dL. | < 0.5 mL/kg/hr for 6-12 hr. |
| 2 | Increase 2–2.9 times baseline. | < 0.5 mL/kg/hr for ≥ 12 hr. |
|
3 |
Increase 3 times baseline or ≥ 4 mg/dL or initiation of renal replacement therapy or eGFR < 35 mL/min/1.73 m². |
< 0.3 mL/kg/hr ≥ 24 hr or anuria for ≥ 12 hr. |
Table 2.
Examples of secondary hyperoxaluria.
| Food contains oxalate and its precursor. Rhubarb, averrhoa carambola, averrhoa bilimbi, tea, nuts, fruits rich in vitamin C. |
| Increased intestinal oxalate absorption Chronic pancreatitis, small bowel resection, crohn’s disease, celiac disease, and cystic fibrosis |
| Decreased intestinal oxalate degradation Antibiotics use |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



