Submitted:
19 January 2026
Posted:
21 January 2026
You are already at the latest version
Abstract
Delays in diagnosis are unfortunately quite common in most health systems. It is apparent that timely diagnosis is more likely to have a favourable outcome. However, there may be many reasons why timely diagnosis is not always achieved. The poor outcomes due to delayed diagnosis go beyond the obvious perception. There have been multiple studies looking into this aspect, and most have focused on the median delays as per disease types and their outcomes. Our focus in this study was to understand if there is a time scale beyond which the delay becomes detrimental. This topic is particularly important and pertinent now given the significant burdens many health systems are facing during the post-pandemic recovery period. It is important to understand the factors leading to a delay to rectify and offer solutions.
Keywords:
IBD
; delayed diagnosis of IBD
; sustained chronic inflammation
; complications of delayed diagnosis
; challenges in endoscopy services
1. Background
Inflammatory bowel diseases (IBD) can cause significant physical and psychological distress, leading to a diminished quality of life for those affected. Unfortunately, delayed diagnosis of IBD is not uncommon, and it can have profound consequences on patients' well-being and long-term prognosis. [1]
These delays could be multifactorial. Firstly, the diagnostic journey for patients with IBD often begins with a wide range of nonspecific symptoms, such as abdominal pain, diarrhoea, rectal bleeding, vomiting, weight loss, and fatigue. [2] During the initial stages, these symptoms are often erroneously attributed to other more common gastrointestinal (GI) conditions (such as irritable bowel syndrome or GI infections). [2] In some cases, they could even be dismissed as a result of stress or dietary factors, until the time they present repeatedly with persistent or worsening symptoms. Secondly, healthcare professionals, particularly in the community, face challenges in recognizing and distinguishing IBD from other gastrointestinal conditions. The location and type of disease could also have an impact on delayed diagnosis. [3] The lack of specific and easily accessible diagnostic tests such as endoscopic procedures and imaging studies also result in a delay. Thirdly, in addition to clinical hurdles, delays in diagnosis can also result from patient-related factors. Some patients may delay seeking medical attention due to fear, embarrassment, or a belief that their symptoms are transient and will resolve on their own. Others may face genuine barriers in accessing healthcare services, such as long wait times for appointments or limited access to gastroenterologists. The conventional patient journey within the community and primary care and the process within a hospital setting after referral by GP are illustrated in Figure 1A and 1B.
The consequences of delayed diagnosis of IBD can be far-reaching. Chronic untreated inflammation can lead to complications like intestinal strictures, abscesses, and fistulae. [4], necessitating more aggressive treatment approaches. Patients are more likely to require biological therapies and intestinal surgery due to delays.[5,6] Delays may also result in later initiation of appropriate therapeutic interventions, which could further worsen disease progression and risk of long-term complications.
Aside of the physical complications that patients endure, the psychological impact of delayed diagnosis cannot be overlooked. The uncertainty and anxiety experienced by patients during the prolonged diagnostic journey can significantly impact their mental well-being, leading to increased stress, depression, and reduced overall quality of life. [7]
With growing evidence that delayed diagnosis has a detrimental effect in both UC and CD, [8] it is crucial that the issue is addressed effectively, which begins with an understanding of factors causing delays. These may vary from one hospital/health-system to another. Once these have been identified, including bottlenecks of delay, appropriate measures can be taken to address them. In general, they require addressing both health-system related and patient-related factors.
2. Aims of the Study
The time leading up from onset of symptoms to formal diagnosis of IBD is considered a delay if the duration is beyond accepted timelines. Unfortunately, delays are common in the health system due to various factors and inevitably the patients are left untreated.
The aims of this study were to understand the impact of delays in diagnosis of IBD and report on IBD-related adverse outcomes (AOs). In this retrospective study, we aimed to study the following-
- To record any delays faced by newly diagnosed IBD patients at our centre
- If so, to understand the various points at which there are delays and identify bottlenecks
- To understand the factors leading to delays i.e., patient-related factors, community-related factors, or hospital-related factors
- To understand if the clinical outcomes were worse in patients who faced a delay compared to those who did not.
3. Patients and Methods
All new patients referred by the General Practitioner (GP) in Primary Care (community health care) over a 5-year period (January 2013 to December 2017), to the Gastroenterology services at our tertiary care centre, for a suspected diagnosis of IBD, were identified using Electronic Medical Records (EMR). All relevant demographic and clinical information were collected using hospital EMR.
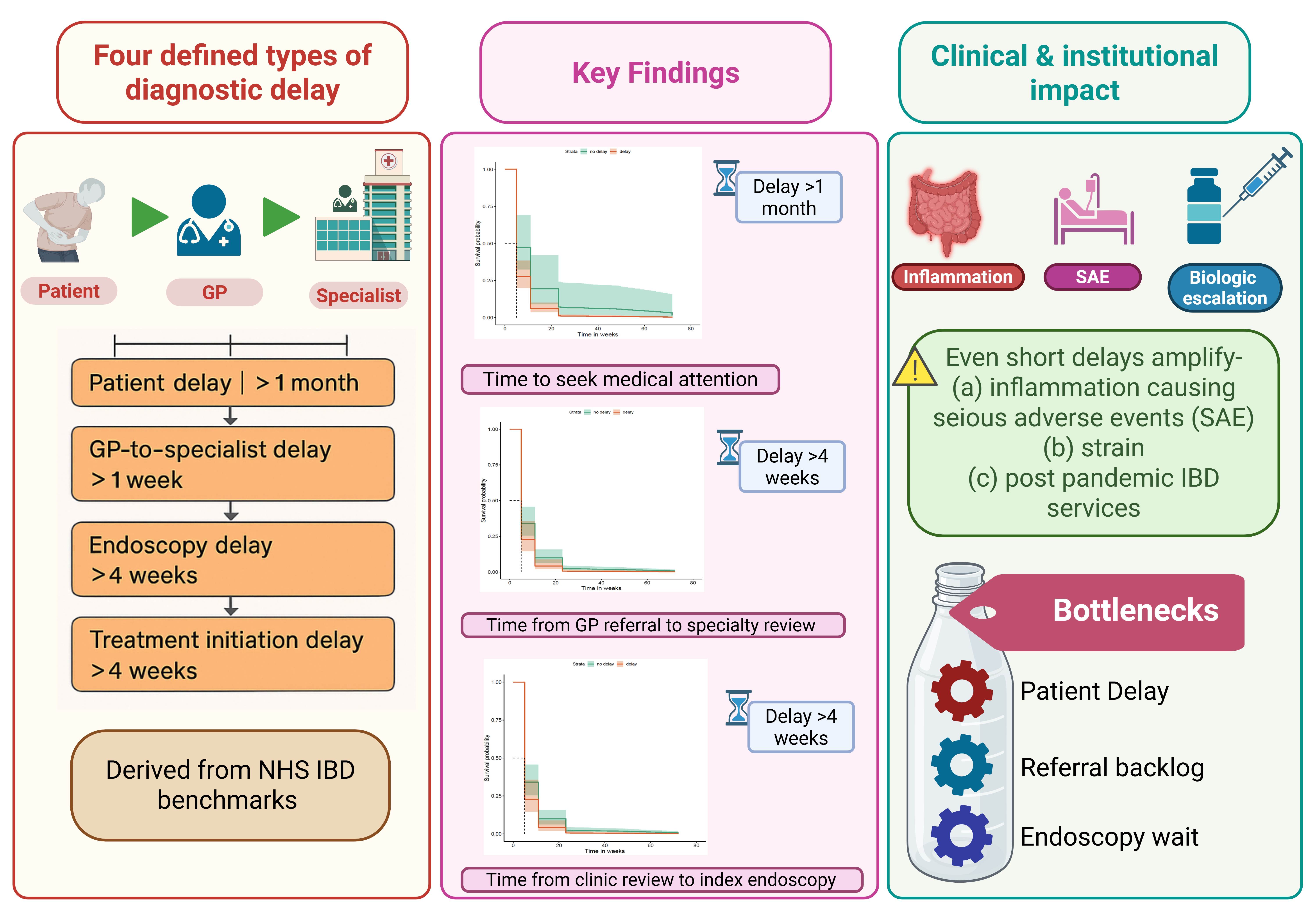
For purposes of the study, different delay-types were defined, and respective cut-off times were assigned by investigators for each delay-type. The cut-off times were assigned based on best average hospital waiting times for IBD benchmarking in the National Health Services, UK (NHS).[9] We considered reasonably stringent cut-offs given that our centre is a tertiary care centre with a large, dedicated service for IBD patients. The definitions of delay-type and the details of cut-off times are in Table 1, Figure 2. All primary care referral letters and clinic letters in the hospital were scrutinised for each episode for all included patients. The reasons for delays in patient journey until start of treatment, and data on pre-defined AOs (steroid & other rescue therapies, hospitalisation, surgery, including perianal, and death) were recorded for each patient until the end of June 2021.
1. Delay in patients seeking medical attention in the community (cut-off: 1 month) — reflects late presentation of symptoms to general practitioners (GPs). 2. Delay in GP referral to the point of review in the gastroenterology clinic (cut-off: 1 week) — reflects outpatient waiting times. 3. Delay between first speciality review and index endoscopy (cut-off: 4 weeks) reflects waiting list for endoscopy units. 4. Delay between first formal diagnosis and initiation of treatment for IBD (cut-off: 4 weeks) — reflects local hospital practices and treatment pathways. Together, these categories highlight patient-, system-, and hospital-level factors influencing the timeliness of IBD diagnosis and management. Image created with BioRender.com.

Table 1.
Definition of delay-type and cut-off times for each type.
| Type of delay | Cut-off time |
|---|---|
|
Delay in patients seeking medical attention in community (Reflects late self-presentation to GP) |
1 month |
|
Delay in GP referral to the point of review in Gastroenterology clinic (Reflects waiting list for outpatient appointments in hospital) |
1 week |
|
Delay between first specialty review and index endoscopy (Reflects waiting list for endoscopy) |
4 weeks |
|
Delay between first formal diagnosis to start of treatment for IBD (Reflects local guidelines and practices in hospital) |
4 weeks |
3.1. Statistical Analysis
The data were analysed using multiple Pearson correlations and Cox proportional Hazard model to determine whether there was a difference in survival without AOs between patients with and without a delay. We tested the significance of each delay and performed Kaplan-Meier [10] and Cox proportional hazards [11] survival analysis to compare patient outcomes when there was a delay versus no delay (as per pre-defined cut-off values).
3.2. Ethical Considerations
This study was registered with hospital research governance & ethics committee and was given approval to proceed in July 2019. (Reference number CARMS-15813)
4. Results
Among a large number of referrals from the GP to the specialty, patients who underwent investigations in our centre and reached a final definitive diagnosis of IBD were first screened. Stringent criteria were applied for patient selection (for e.g.,- pre-existing diagnosis or new to area IBD patients were excluded) and only newly diagnosed IBD patients were included.
A total of 105 patients were identified (M=58; median age=32y), with a long median follow-up of 55 months (range 5-72m). The demographics of patients are in Table 2. The most frequent presenting complaints were abdominal pain (44, 41,9%), loose stools (40, 38,1%), bloody diarrhoea (37, 35,2%) and bleeding per-rectum (33, 31,4%) and only 16% declared a family history. 65, 27 and 13 patients had final diagnosis of Ulcerative colitis, Crohn’s disease and IBD-unclassified respectively, and analysed collectively. The breakdown of clinical details re in Table 3. The number of patients with durations of follow-up is illustrated in a plot graph. (Figure 3-3)
In our total cohort, we identified that there were delays at almost every step. The longest delay-types in order were -
- -
- Delay in patients seeking medical attention (median= 4 months; range 1 to 84 months)
- -
- Delay between GP referral to Gastroenterology clinic appointment (median=5 weeks; range 1 to 30 weeks)
- -
- Delay between first specialty review and index endoscopy (median=3 weeks; 1 to 36 weeks)
- -
- Delay between first formal diagnosis to start of treatment for IBD (median=2 weeks; range 0 to 12 weeks)
After patient stratification based on these delay-types and applying the specific cut-off times for each, we noted a statistically significant difference in survival without AOs for all, when comparing delay versus no delay.
When patients delayed seeking medical attention beyond 1 month of onset of symptoms, they were more likely to suffer AOs up to at least 60 months, compared to those who did not delay. This was statistically significant and is illustrated in Figure 4.
When patients faced a delay of more than 1 week between referral from primary care to their first specialty review in the Gastroenterology clinic, they were more likely to suffer AOs. This is illustrated in Figure 5.
When patients faced a delay of more than 4 weeks within the health system, between their first specialty review and index endoscopy, they were more likely to suffer AOs during the follow-up period for up to 60 months. (p=0.01) This is illustrated in Figure 6.
When patients faced a delay of more than 4 weeks between their first formal diagnosis and start of treatment for IBD, they were more likely to suffer AOs during the follow-up period for up to 60 months. (p=0.03). This is illustrated in Figure 7.
Delays and Biologic Use During Disease Course
We also examined if delay in diagnosis had an influence on the use of biologics during the follow-up period in our cohort. Using ‘biologic-use’ at any time during follow-up as an outcome variable, different delay types were compared keeping the cut-off times the same as before. It was noted that any delay increased the risk of biologic use during the follow-up period. The details of delay-type and odds-ratio of biologic use is given in Table 4.
We then combined more than one type of delay to examine if a cumulative effect was able to predict use of biologics. In our cohort, a model that combined delay in seeking medical attention, and delay between specialty review to index endoscopy exhibited the best predictive power with average AUROC of 0.67.
On further analysis of patient-related delay and health-system related delays, there was a statistically significant increase noted in the risk of requiring biologics at any time during the follow-up period. A patient-related delay of more than 2 weeks showed a statistically significant increased risk of requiring biologics compared to less than 2 weeks. Figure 8 illustrates this risk, and it is noted that this remains higher for more than 4 consecutive years.
Once patients were within the health system, a cumulative delay of more than 6 weeks increased the risk of biologic therapy over the next 4 years. This is illustrated in Figure 9.
5. Discussion
Delays in diagnosis are unfortunately quite common in most health systems. It is apparent that timely diagnosis is more likely to have a favourable outcome. However, there may be many reasons why timely diagnosis is not always achieved. The poor outcomes due to delayed diagnosis go beyond the obvious perception. There have been multiple studies looking into this aspect, and most have focused on the median delays as per disease types and their outcomes. Our focus in this study was to understand if there is a time scale beyond which the delay becomes detrimental. This topic is particularly important and pertinent now given the significant burdens many health systems are facing during the post-pandemic recovery period. It is important to understand the factors leading to a delay to rectify and offer solutions.
In one study, Vavricka et al. reported on risk factors that led to delays in diagnosis of IBD. The authors used data from a comprehensive Swiss national IBD database during a three-year period. They found median delay in CD patients from first onset of IBD-related symptoms to IBD diagnosis was 9 months, significantly longer than UC patients which was 4 months. We found no significant differences between UC and CD. They also reported that younger CD patients with ileal disease were most at risk of long diagnostic delay, probably due to an overlap of IBS-type symptoms. [3] In another study, the authors reported similar risk for CD patients. In addition, active smoking status and symptom onset during summer were found to be independent risk factors. A long diagnostic delay was noted to increase the risk of stricturing disease (OR, 3.38; p < 0.01), fistulae (OR, 2.64; p = 0.08), and IBD-related surgery. [12]
In our cohort, for each of the delay-types defined, there were generally more patients who faced a delay compared to those who did not. We were able to compare these within each delay-type.
5.1. Delay in Patients Seeking Medical Attention
This delay-type which was patient-related was the longest one with a median of 4 months. This is consistent with findings from other studies. [8] Although there are prospective studies that have reported a significantly longer median time to diagnosis for CD [13], this was not noted in our cohort. For this delay-type, when patients waited beyond a month to seek medical attention, they were more likely to have AOs, and they are more likely to need biologics to manage their condition. In a real-world setting, patients do not always consult the GP immediately for various reasons. Moreover, it remains unclear if a particular timescale (to wait) is acceptable. Based on our findings, it would be reasonable to educate patients not to wait beyond 2-3 weeks to seek medical attention.
5.2. Delay Between GP Referral to Gastroenterology Clinic Appointment
This delay-type is health-system related, with a median time of 5 weeks in our cohort. In our cohort, a delay of more than 1 week resulted in worse outcomes. This is perhaps the most likely bottleneck that affect hospitals, particularly worse after the COVID-19 pandemic. There is no reliable data on breakdown of delay-types comparing clinical outcomes. Most studies report on a cumulative delay only. This particular delay reflects the waiting lists in hospitals before a patient is offered an appointment in the specialty clinic. The waiting time for this critical stage in the patient journey has very likely expanded in almost all healthcare settings due to increasing demand, clearance of backlog of appointments, lack of workforce and shortage of experts. As IBD is a complex disease it is unlikely that treatment is started empirically in primary care before a formal diagnosis can be established. Also, GPs are understandably more comfortable maintaining treatment as advised by experts, than initiating treatment. [14,15] This inevitable delay in starting treatment leaves patients in a state of sustained chronic inflammation, thereby worsening outcomes.
5.3. Delay Between First Specialty Review and Index Endoscopy
This delay-type is the next step in establishing the diagnosis, with a median of 3 weeks in our cohort. It reflects the waiting list in endoscopy departments. Endoscopy is an essential tool not only for diagnosis but also for ongoing assessment of disease activity and monitoring of patients on advanced therapies. Although the median time was less than the assigned cut-off in our cohort, patients who faced delays beyond 4 weeks had a statistically higher risk of having AOs during follow-up. This was made worse by the backlogs during the pandemic and post-pandemic recovery. As predicted by experts during the pandemic, patients are waiting longer to undergo procedures. [16] The ever increasing waiting lists will leave a larger number of patients at risk of having untreated CI and more AOs.
5.4. Delay Between First Formal Diagnosis to Start of Treatment for IBD
This delay-type generally varies from one hospital to another, based on local policies and guidelines. In our cohort, the median time to start of treatment was 2 weeks which was better than our cut-off of 4 weeks. Among patients who faced a delay beyond 4 weeks, there was a statistically significant risk of AOs. This delay should ideally be minimal as treatment can be started immediately at the time of contact with patients during their index endoscopy. One study reported more than 75% patients to have started treatment within 2 weeks of diagnosis. [9] It is possible this proportion may have reduced owing to pressures on the outpatient departments during the post-pandemic era. There have been reports of a drop in prescription rates during the immediate post-pandemic phase. One study reported a sharp fall in prescriptions for thiopurines (-81%), with lesser reductions for biologics (-38%) and oral prednisolone (-20%). [17] It is likely to have improved to some extent but not to baseline.
This is important to consider as a cumulative delay within the health-system of more than 6 weeks significantly increases the risk of patients requiring biologics over the next 4 years.
It is clear from our data that any delay in diagnosis, whether patient-related or health-system related, results in worse outcomes. Our study is one of the few that has analysed and reported the details of the break-up of delay-types and relevant timelines for each. By doing so, it is possible to work on those areas identified as causing the longest delays. Such bottlenecks once identified, frequently can be managed with minor changes in patient flow, referral systems, vetting process and so on. For example, one of the simplest to implement that could reduce delays in starting treatment would be to hand out a prescription in endoscopy for patients newly diagnosed with IBD. Individual centres will need to work on respective bottlenecks using these timelines as a target to be achieved. Timely diagnosis will very likely result in better outcomes and fewer AOs, ultimately reducing the burden on the health-system. Overall, achieving adequate control of chronic inflammation would improve short and long term outcomes for IBD patients.
5.5. Strengths and Limitations of the Study
Out study has several strengths. We applied very stringent criteria for inclusion to ensure only inception patients are part of the study cohort. This was done to ensure we are able to study the outcomes of sustained chronic inflammation at the start of the disease process. We have analysed delay-types in great detail and shown that specific timelines are definitely relevant to clinical outcomes. We assigned stringent but fair cut-off times to measure performance of the service, making it quite robust.
Our study has several limitations. As this was a retrospective study, there was some data missing, particularly data such as smoking status and up to date biomarkers, and it is possible that AOs may be under-reported. This data was from one tertiary care centre and the number of patients included in the study were relatively low. As our centre is a tertiary care with dedicated IBD service, we assume our timelines may be better than other centres. Despite this advantage, even short delays appear to have an impact on clinical outcomes. Due to smaller number of patients, we were unable to perform statistically meaningful univariate or multivariate regression analysis to identify risk factors that could predict delays.
6. Conclusions
To conclude, we have shown from our data that delays, and subsequent untreated chronic inflammation leads to poor outcomes in newly diagnosed IBD patients.
Our study has shown that delays in diagnosis could be potentially detrimental. Whether it is patient-related, or health-system related, they lead to poorer outcomes. There are often several bottlenecks in a service that contribute to delays, increasing AOs in IBD over the follow-up period.
In our cohort, a delay as short as a week, between GP referral and specialty review, is statistically significant in determining AOs, hence their negative impact should not be underestimated.
Each delay-type is unique in some ways and highlights a different area for improvement. Any delays by patients in seeking medical attention from the GP identifies that patients may not be aware of the potential seriousness of their GI symptoms. This could perhaps be addressed by undertaking patient education and awareness programmes locally, regionally, and also nationally. Delays in clinical appointments and endoscopy appointments can be variable based on the centres. This particular problem is pertinent during the post-pandemic recovery period as almost every hospital in the UK is struggling to clear backlogs, while simultaneously grappling with unprecedented demands placed on an already stretched workforce. This is also applicable to specialist IBD centres where our data is likely to have implications on service delivery and planning. The data on high proportion of AOs may prove supportive in planning business cases to redesign services, add workforce and prioritise IBD patients, to minimise the damage done by excessive delays. Our data also suggests that cumulative delays in the hospital increase the use of biologics for consecutive years. This will undoubtedly add to pressures of IBD teams and infusion suites at hospitals. Specialist services will need to allocated resources appropriately to meet this demand in the long term. Both hospitals and policy makers will need to consider this and allocate necessary resources to minimise delays and keep the standards of best practice.
Author Contributions
Shivaji, UN - literature search, data collection, data analysis, writing & editing manuscript, revision and final approval Majumder, S - data collection, data analysis, writing & editing manuscript, revision and approval Abhishek Rao - data collection, data analysis, writing & editing manuscript, revision and approval Alina Bazarova - data analysis, statistical analysis, writing & editing sections of manuscript, revision and approval Tommaso Parigi - writing & editing sections of manuscript, revision and final approval Subrata Ghosh – conceptualisation, critical revision of manuscript and final approval Marietta Iacucci – conceptualisation, critical revision of manuscript and final approval.
Funding
statement- This paper presents independent research funded and supported by the NIHR Birmingham Biomedical Research Centre at the University Hospitals Birmingham NHS Foundation Trust and the University of Birmingham. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Institutional Review Board Statement
This study was registered with hospital research governance & ethics committee and was given approval to proceed in July 2019. (Reference number CARMS-15813).
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
None to declare.
References
- Ghosh, S; Mitchell, R. Impact of inflammatory bowel disease on quality of life: Results of the European Federation of Crohn's and Ulcerative Colitis Associations (EFCCA) patient survey. J Crohns Colitis 2007, 1(1), 10–20. [Google Scholar] [CrossRef] [PubMed]
- Burgmann, T; Clara, I; Graff, L; Walker, J; Lix, L; Rawsthorne, P; et al. The Manitoba Inflammatory Bowel Disease Cohort Study: prolonged symptoms before diagnosis--how much is irritable bowel syndrome? Clin Gastroenterol Hepatol. 2006, 4(5), 614–20. [Google Scholar] [CrossRef] [PubMed]
- Vavricka, SR; Spigaglia, SM; Rogler, G; Pittet, V; Michetti, P; Felley, C; et al. Systematic evaluation of risk factors for diagnostic delay in inflammatory bowel disease. Inflamm Bowel Dis. 2012, 18(3), 496–505. [Google Scholar] [CrossRef] [PubMed]
- Moon, CM; Jung, SA; Kim, SE; Song, HJ; Jung, Y; Ye, BD; et al. Clinical Factors and Disease Course Related to Diagnostic Delay in Korean Crohn's Disease Patients: Results from the CONNECT Study. PLoS One 2015, 10(12), e0144390. [Google Scholar] [CrossRef] [PubMed]
- Lee, DW; Koo, JS; Choe, JW; Suh, SJ; Kim, SY; Hyun, JJ; et al. Diagnostic delay in inflammatory bowel disease increases the risk of intestinal surgery. World J Gastroenterol. 2017, 23(35), 6474–81. [Google Scholar] [CrossRef] [PubMed]
- Kang, HS; Koo, JS; Lee, KM; Kim, DB; Lee, JM; Kim, YJ; et al. Two-year delay in ulcerative colitis diagnosis is associated with anti-tumor necrosis factor alpha use. World J Gastroenterol. 2019, 25(8), 989–1001. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, A; Heatley, RV. Review article: psychosocial factors in the quality of life of patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2005, 21(5), 499–508. [Google Scholar] [CrossRef] [PubMed]
- Jayasooriya, N; Baillie, S; Blackwell, J; Bottle, A; Petersen, I; Creese, H; et al. Systematic review with meta-analysis: Time to diagnosis and the impact of delayed diagnosis on clinical outcomes in inflammatory bowel disease. Aliment Pharmacol Ther. 2023, 57(6), 635–52. [Google Scholar] [CrossRef] [PubMed]
- Hawthorne, AB; Glatter, J; Blackwell, J; Ainley, R; Arnott, I; Barrett, KJ; et al. Inflammatory bowel disease patient-reported quality assessment should drive service improvement: a national survey of UK IBD units and patients. Aliment Pharmacol Ther. 2022, 56(4), 625–45. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E; Meier, P. Nonparametric Estimation from Incomplete Observations. Journal of the American Statistical Association 1958, 53(282), 457–81. [Google Scholar] [CrossRef]
- Cox, DR. Regression Models and Life-Tables. Journal of the Royal Statistical Society Series B (Methodological 1972, 34(2), 187–220. [Google Scholar] [CrossRef]
- Zaharie, R; Tantau, A; Zaharie, F; Tantau, M; Gheorghe, L; Gheorghe, C; et al. Diagnostic Delay in Romanian Patients with Inflammatory Bowel Disease: Risk Factors and Impact on the Disease Course and Need for Surgery. J Crohns Colitis 2016, 10(3), 306–14. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, M; Chang, M; Chow, EJ; Tabibzadeh, S; Kirit-Kiriak, V; Targan, SR; et al. Identification of a prodromal period in Crohn's disease but not ulcerative colitis. Am J Gastroenterol. 2000, 95(12), 3458–62. [Google Scholar] [CrossRef] [PubMed]
- Tan, M; Holloway, RH; Lange, K; Andrews, JM. General practitioners' knowledge of and attitudes to inflammatory bowel disease. Intern Med J. 2012, 42(7), 801–7. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, R; Almahmudi, F; Makhdoom, Y; Mosli, M. Knowledge and attitudes of primary healthcare physicians toward the diagnosis and management of inflammatory bowel disease following an educational intervention: A comparative analysis. Saudi J Gastroenterol. 2019, 25(5), 277–85. [Google Scholar] [PubMed]
- Iacucci, M; Cannatelli, R; Labarile, N; Mao, R; Panaccione, R; Danese, S; et al. Endoscopy in inflammatory bowel diseases during the COVID-19 pandemic and post-pandemic period. Lancet Gastroenterol Hepatol. 2020, 5(6), 598–606. [Google Scholar] [CrossRef] [PubMed]
- Bodger, K; Bloom, S; Dobson, L; Cummings, F; Grainger, S; Kennedy, N; et al. PMO-37 COVID-19 impact on care and prescribing for inflammatory bowel disease: Data from the IBD Registry. Gut 2021, 70 (Suppl 4), A95–A6. [Google Scholar] [CrossRef]
Figure 1.
The conventional patient journey from symptom onset to follow-up in gastrointestinal disease. (A) Community and primary care pathway: The patient develops symptoms (1), consults a general practitioner (GP) (2), and is referred to secondary care (3). (B) Hospital pathway: The patient is reviewed in the gastroenterology outpatient clinic (1), referred for endoscopy and imaging (2), and undergoes endoscopy-guided biopsies for histological confirmation of diagnosis (3). Treatment is initiated based on findings (4), followed by regular follow-up (5).Image created with BioRender.com.
Figure 1.
The conventional patient journey from symptom onset to follow-up in gastrointestinal disease. (A) Community and primary care pathway: The patient develops symptoms (1), consults a general practitioner (GP) (2), and is referred to secondary care (3). (B) Hospital pathway: The patient is reviewed in the gastroenterology outpatient clinic (1), referred for endoscopy and imaging (2), and undergoes endoscopy-guided biopsies for histological confirmation of diagnosis (3). Treatment is initiated based on findings (4), followed by regular follow-up (5).Image created with BioRender.com.
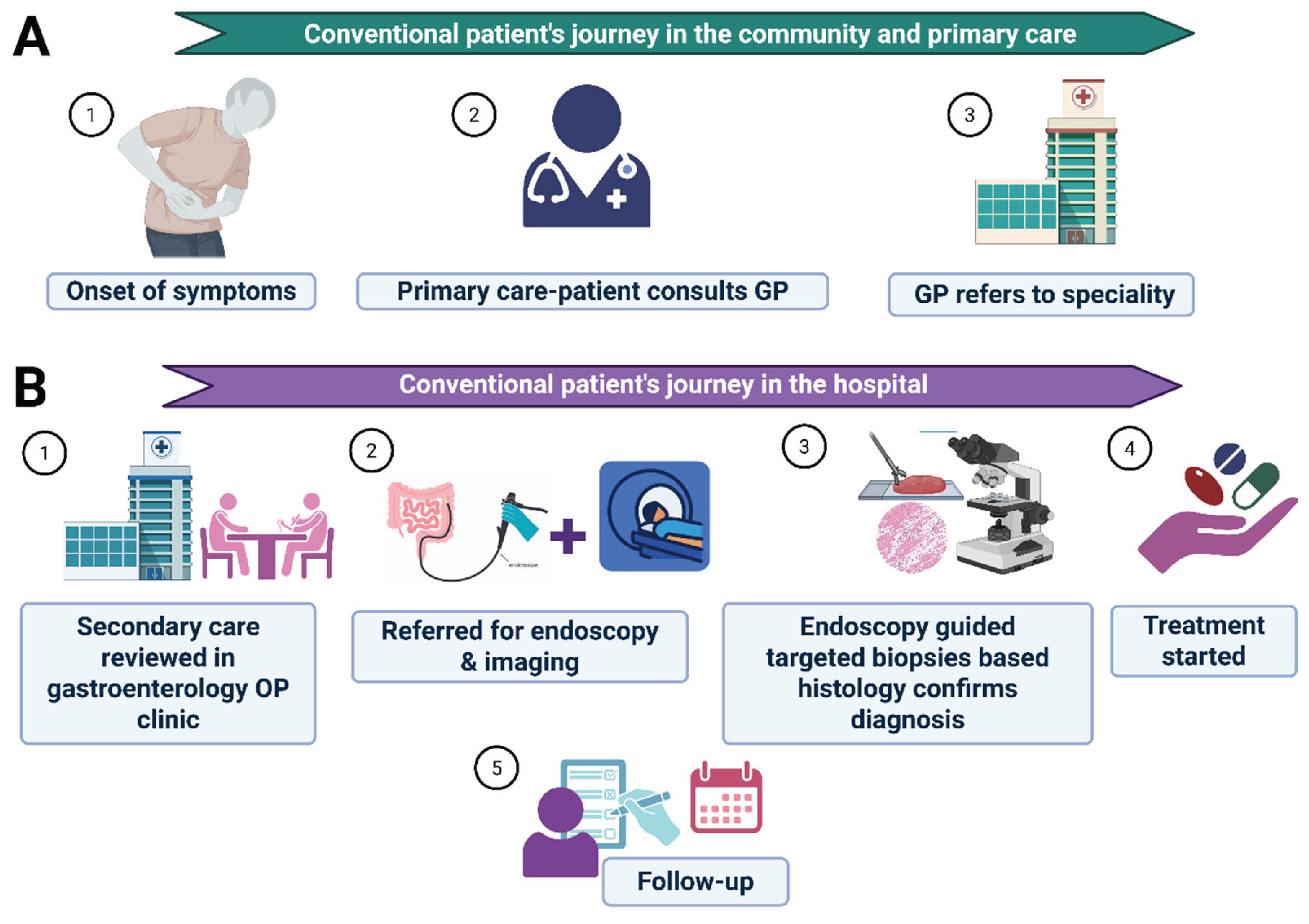
Figure 2.
Types of delays contributing to Inflammatory Bowel Disease (IBD) diagnosis. Schematic representation of four key types of diagnostic delays in IBD.
Figure 2.
Types of delays contributing to Inflammatory Bowel Disease (IBD) diagnosis. Schematic representation of four key types of diagnostic delays in IBD.
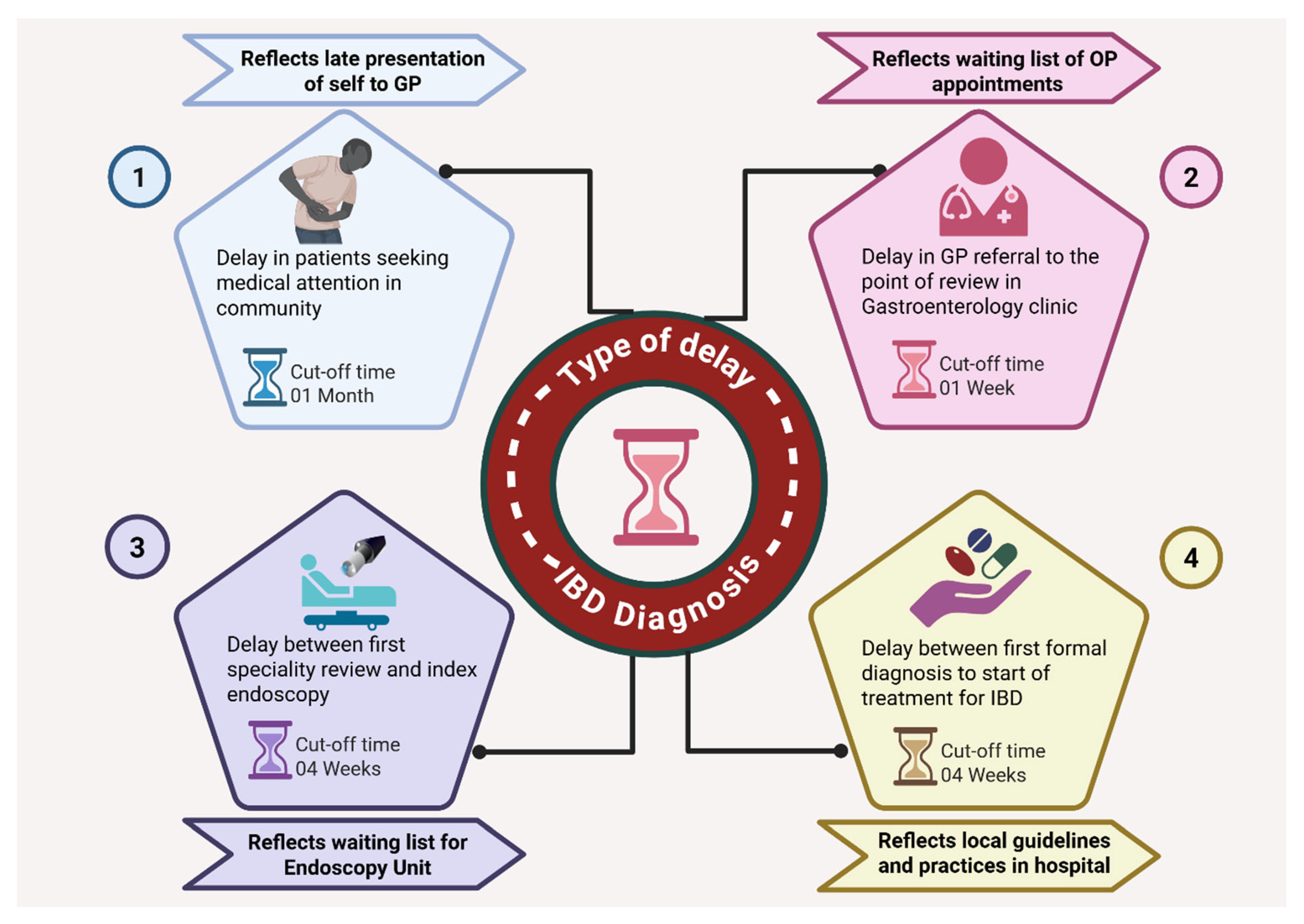
Figure 3.
Follow up data for all patients (in months). In this plot, X-axis indicates time in months. The blue dots indicate patient’s maximum follow-up at specific time periods. The red dot indicates the median follow-up for the cohort.
Figure 3.
Follow up data for all patients (in months). In this plot, X-axis indicates time in months. The blue dots indicate patient’s maximum follow-up at specific time periods. The red dot indicates the median follow-up for the cohort.
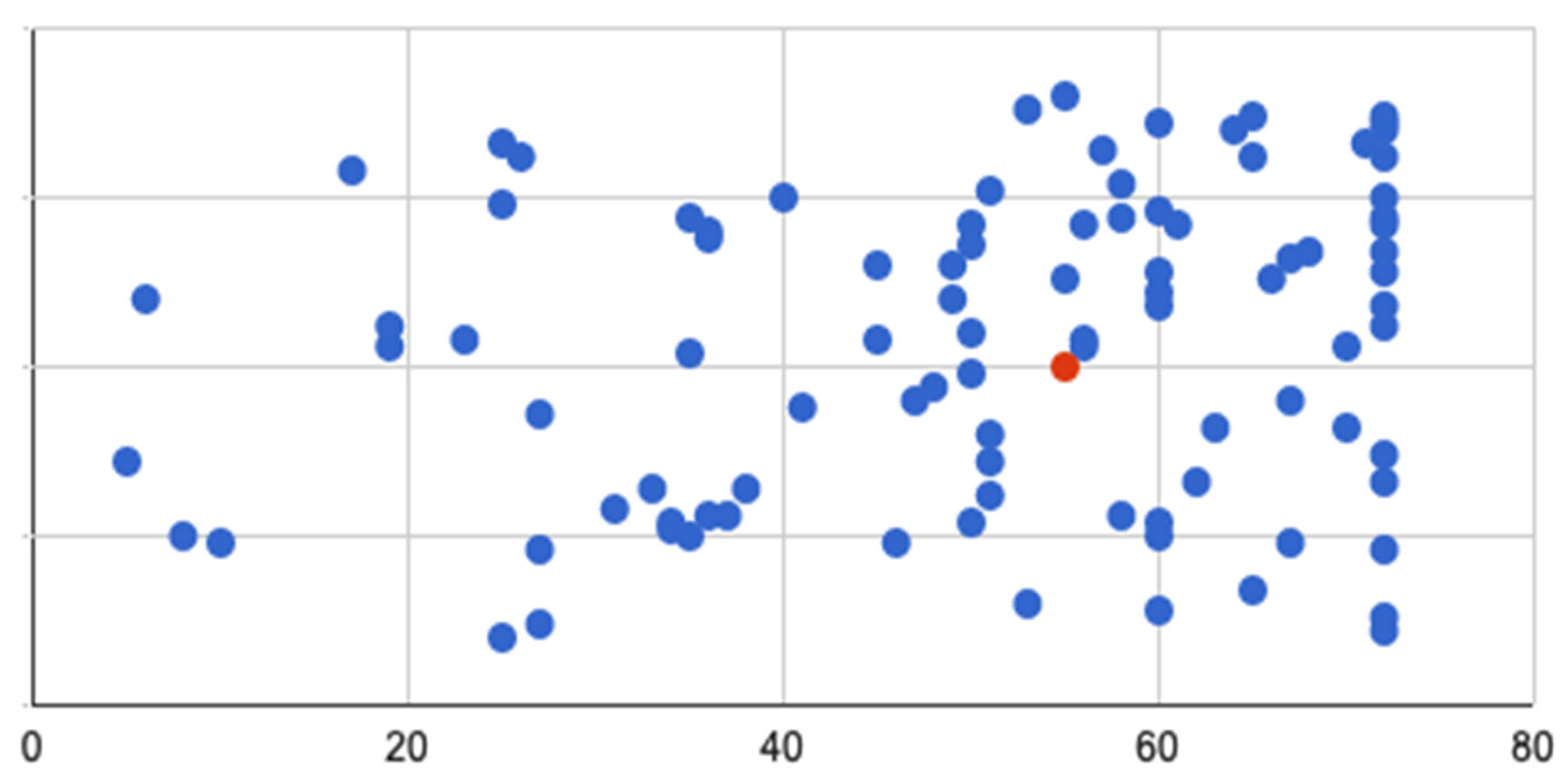
Figure 4.
Time to seek medical attention of >1month (survival without AOs; p=0.004). The curve illustrates the higher probability of AO due to delay, and the curves remains separated up to follow up period.
Figure 4.
Time to seek medical attention of >1month (survival without AOs; p=0.004). The curve illustrates the higher probability of AO due to delay, and the curves remains separated up to follow up period.
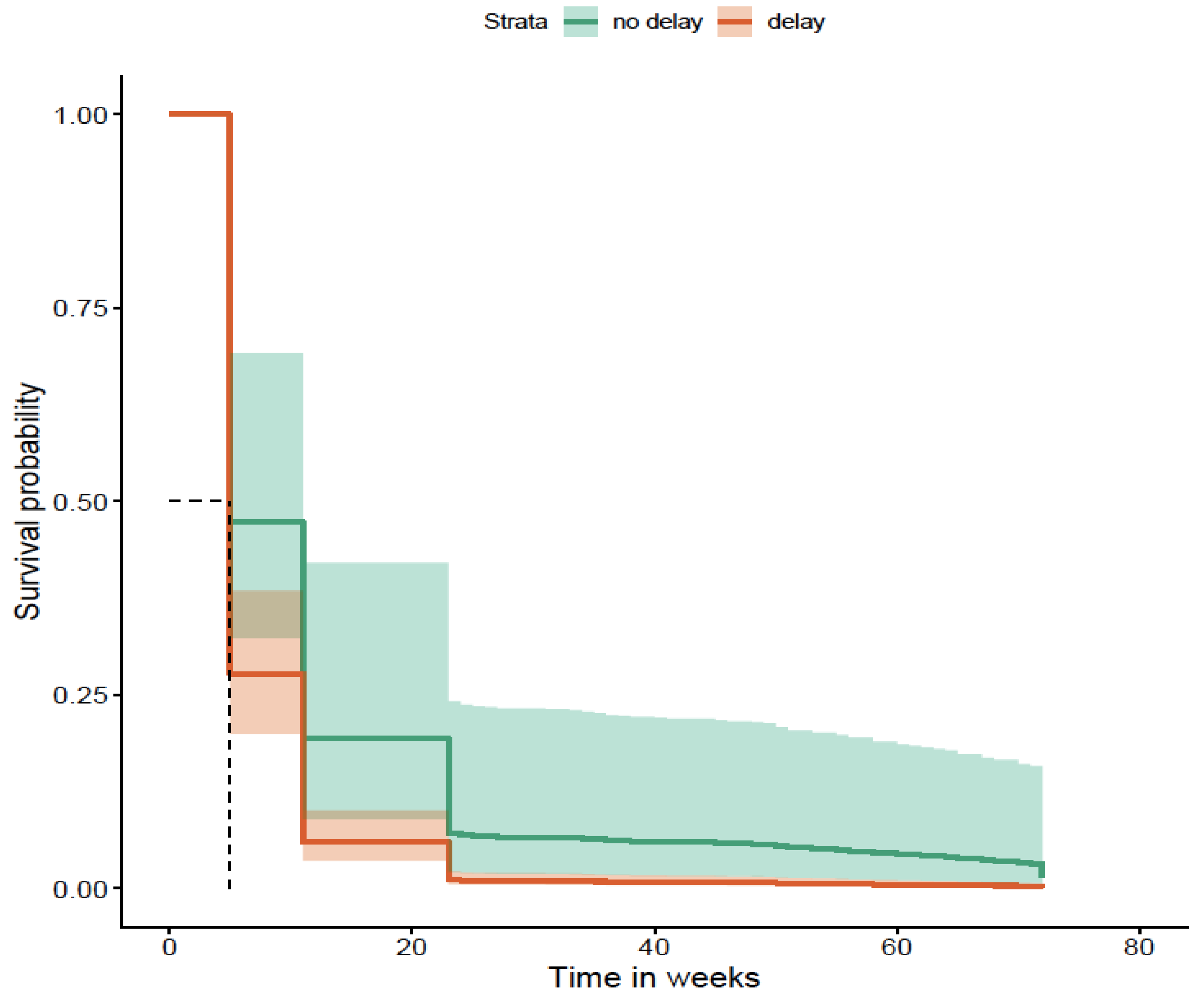
Figure 5.
Time from GP referral to specialty review of >1 week (survival without AO; p=0.048). The K-M curve illustrates higher probability of AO due to delay.
Figure 5.
Time from GP referral to specialty review of >1 week (survival without AO; p=0.048). The K-M curve illustrates higher probability of AO due to delay.
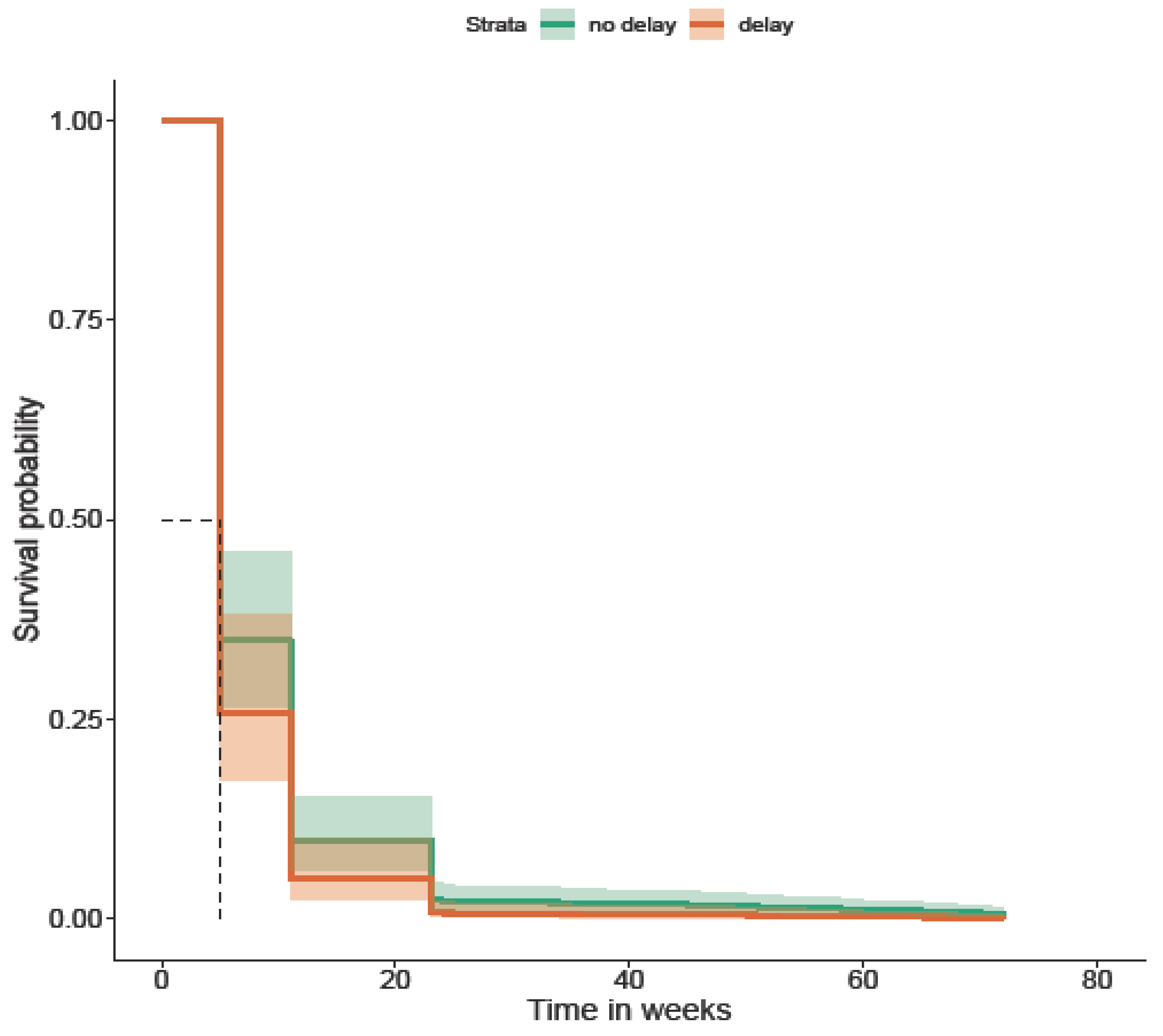
Figure 6.
Time from clinic review to index endoscopy of >4 weeks (survival without AOs; p=0.01). The K-M curve illustrates the higher probability of AO due to delay.
Figure 6.
Time from clinic review to index endoscopy of >4 weeks (survival without AOs; p=0.01). The K-M curve illustrates the higher probability of AO due to delay.
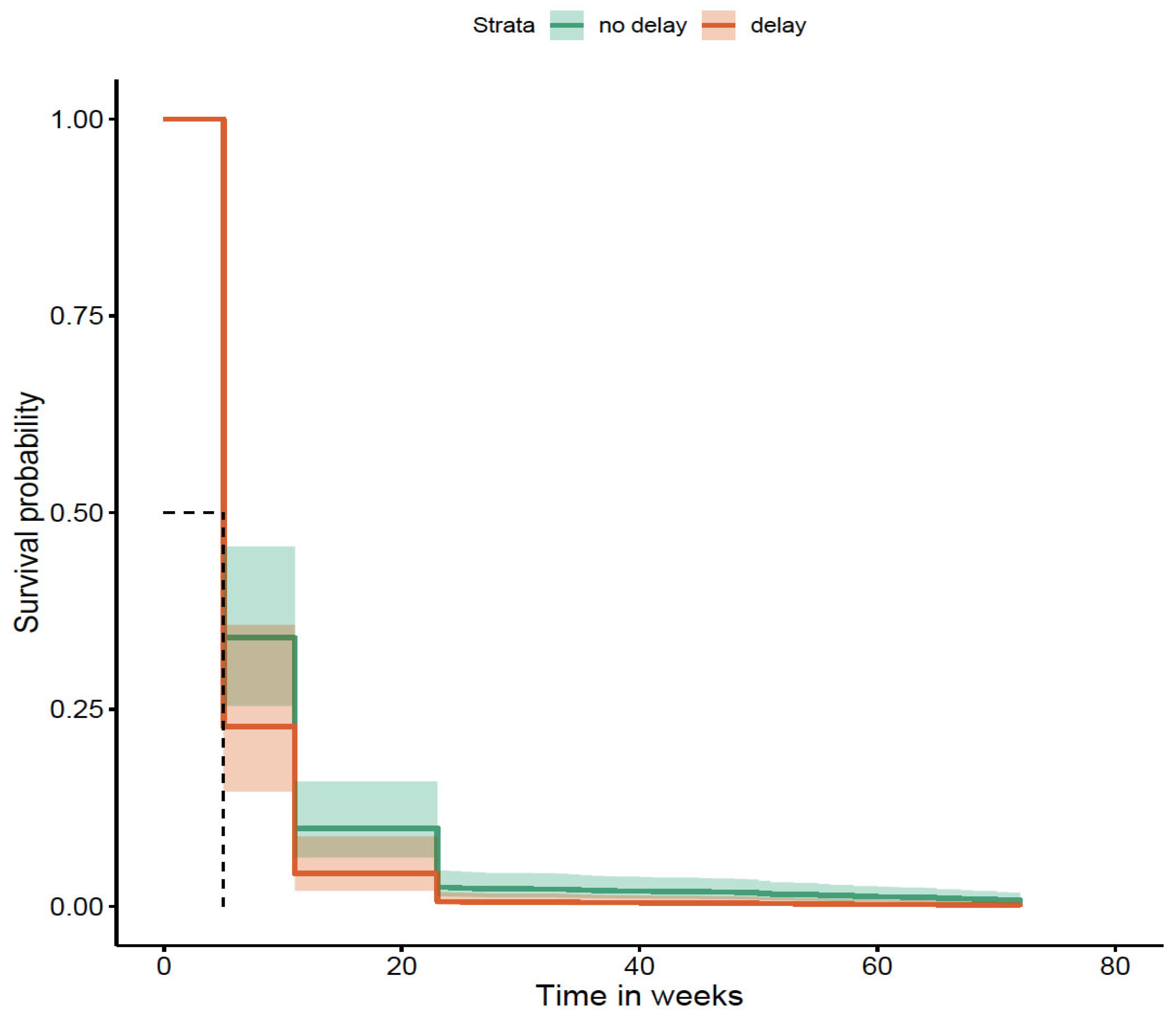
Figure 7.
Delay between formal diagnosis and start of treatment (p=0.03). The K-M curve illustrates the higher probability of AO due to delay.
Figure 7.
Delay between formal diagnosis and start of treatment (p=0.03). The K-M curve illustrates the higher probability of AO due to delay.
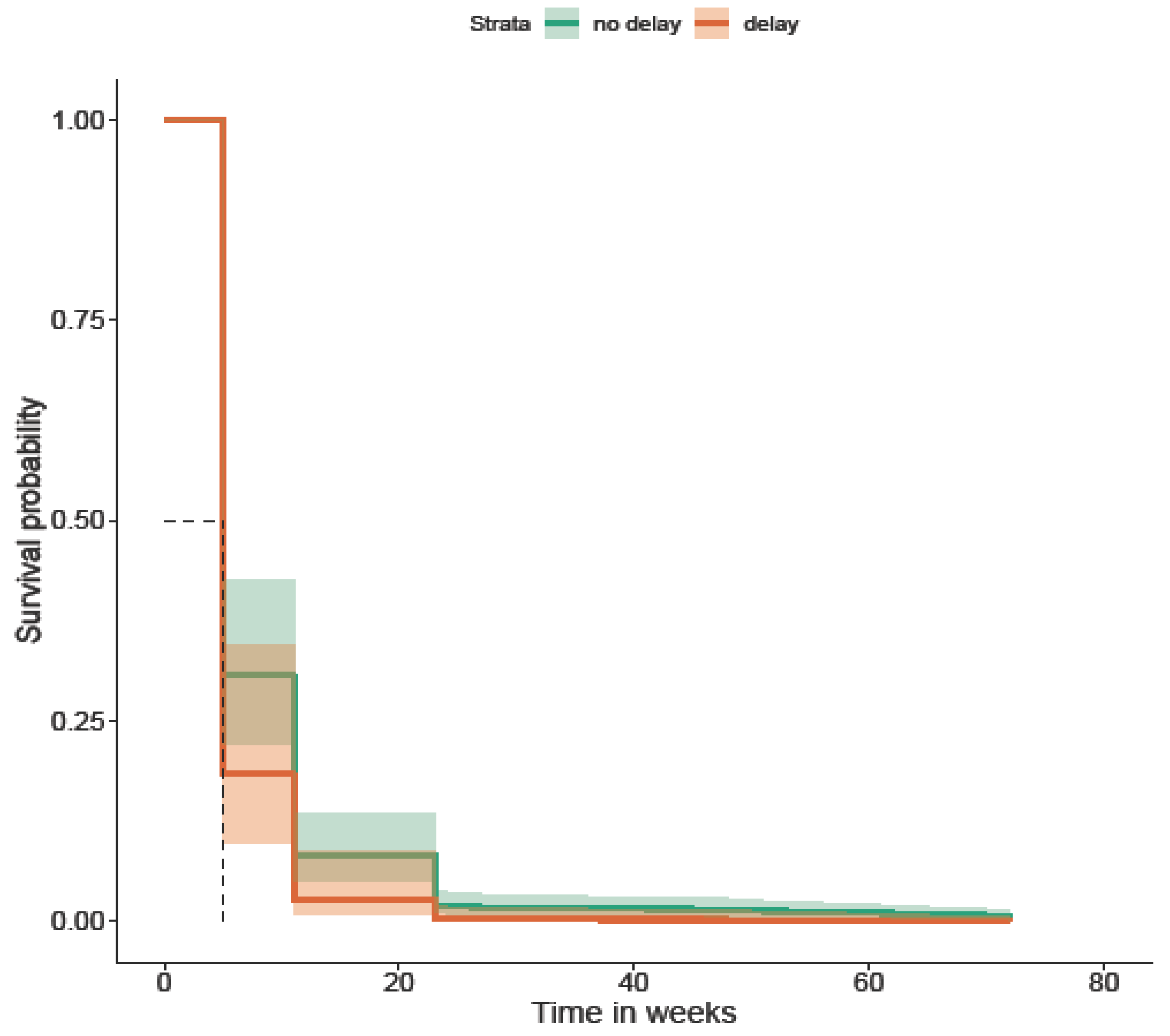
Figure 8.
Patient-related delay of >2weeks and risk of needing biologics (p=0.042).
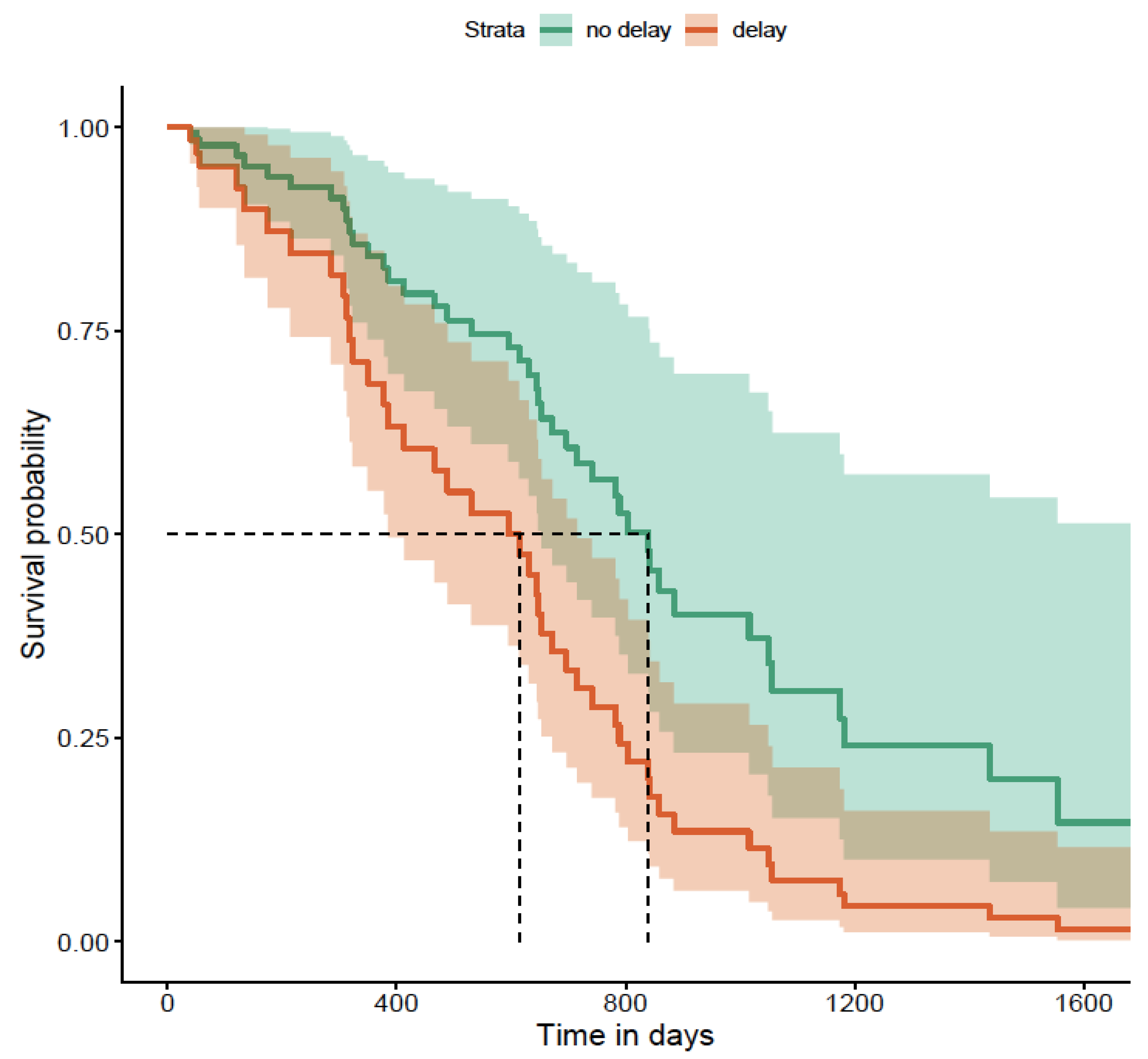
Figure 9.
Health-system related delay of >6weeks and risk of needing biologics (p=0.021).
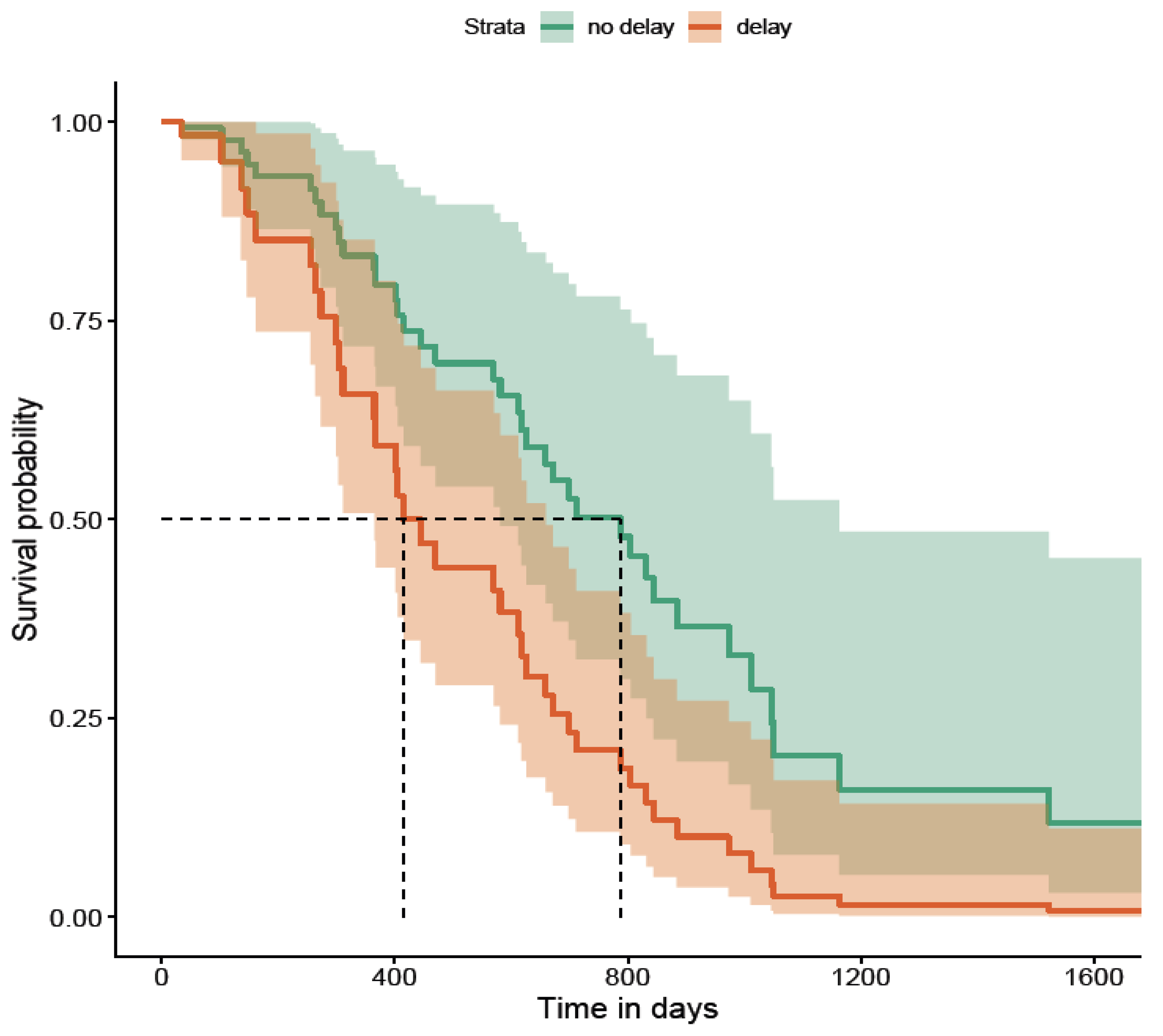
Table 2.
Demographics and classification.
| Age & gender | N=105 |
|---|---|
| Median age | 32 years (range 21-82 years) |
| Gender | Male=58; Female=47 |
| Race | |
| Caucasian | 65 (62%) |
| Asian | 28 (27%) |
| Afro-Caribbean | 1 (1%) |
| Unknown/Unreported | 11 (10%) |
| Disease type at first diagnosis | |
| Ulcerative colitis | 65 (62%) |
| Crohn’s disease | 27 (26%) |
| IBD-unclassified | 13 (12%) |
| Montreal classification for CD | |
| Age A1 A2 A3 |
2 22 3 |
| Location L1 L2 L3 L4 L3+L4 |
7 6 13 0 1 |
| Behaviour B1 B2 B3 B1+ perianal |
21 3 0 3 |
| Ulcerative colitis extent | |
| E1 E2 E3 |
12 36 17 |
Table 3.
Clinical data - symptoms, medications at start, and follow-up period.
| Symptoms at presentation | Number of patients |
|---|---|
| Abdominal pain | 44 |
| Loose stools | 40 |
| Loose stools with blood in stools | 37 |
| Bleeding per rectum | 33 |
| Weight loss | 16 |
| Vomiting | 5 |
| Medications started at first diagnosis | |
| Oral 5-ASA | 48 |
| Oral Steroids | 33 |
| Rectal 5-ASA | 32 |
| Rectal steroids | 8 |
| 5-ASA and steroids | 6 |
| Thiopurines | 5 |
| Biologics | 5 |
| Details of follow-up | |
| Median follow-up period of cohort | 55 months (range 5-72 months) |
| Patients with first follow-up <6 months | 101 |
| Patients with first follow-up 6-12 months | 2 |
| Patients with first follow-up 12-24 months | 2 |
| Patients with first follow-up >24 months | 0 |
Table 4.
Risk of biologic use due to delays in diagnosis.
| Type of delay | Risk of biologic use during follow up (OR with CI) |
|---|---|
| Delay in patients seeking medical attention in community | 1.08 (1.03, 1.17) |
|
Delay between GP referral to the point of review in Gastroenterology clinic |
1.10 (1.0, 1.23) |
|
Delay between first specialty review and index endoscopy |
1.09 (1.01, 1.21) |
| Delay between first formal diagnosis to start of treatment for IBD | 1.08 (1.0, 1.21) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



