
Submitted:
20 January 2026
Posted:
20 January 2026
You are already at the latest version
Abstract
Psychological factors such as depression, anxiety, and loneliness significantly affect sleep quality, particularly among elderly individuals living in nursing homes. This study aimed to examine the relationship between sleep quality and depression, anxiety, and loneliness among elderly residents of nursing homes in Indonesia, as well as to explore the underlying pathway mechanisms. A quantitative cross-sectional design was used to assess correlational relationships among elderly individuals residing in nursing homes in Jakarta and Tangerang. Data were analyzed using JASP statistical software through descriptive, bivariate, and path analyses. The results demonstrated significant associations between poorer sleep quality and higher levels of loneliness, anxiety, and depression. Path analysis revealed a significant chain mediation effect, in which loneliness was associated with increased anxiety, subsequently leading to exacerbated depressive symptoms and ultimately reduced sleep quality (β = −0.040, p = 0.045). These findings indicate that sleep disturbances in the elderly arise from a sequential interaction among loneliness, anxiety, and depression, highlighting the importance of comprehensive psychosocial interventions to improve sleep quality in this population.
Keywords:
sleep quality
; loneliness
; depression
; anxiety
; elderly
; nursing homes
1. Introduction
The global number of elderly adults has been steadily increasing. According to the United Nations Department of Economic and Social Affairs (UNDESA) World Population Ageing report, the number of people aged 65 years and older reached 703 million in 2019 and is expected to reach 1.5 billion by 2050 [1]. Asia is the region with the fastest-growing elderly population, particularly in countries such as Japan, South Korea, and China. In Indonesia, data from the 2020 Population Census indicate that adults aged 60 years and above accounted for 10.8% of the total population, or approximately 29 million individuals. This proportion is expected to continue rising in line with increasing life expectancy [2].
The growing elderly population highlights the importance in healthcare and public welfare, including challenges in maintaining adequate sleep quality. Age-related physiological changes in sleep patterns, such as reduced sleep efficiency, increased nighttime awakenings, and alterations in circadian rhythms, predispose the elderly individuals to sleep disturbances [3,4] Poor sleep quality in the elderly not only impairs function but also correlates to cognitive impairment, low immunity, mood disorders, and rising morbidity and mortality factors [5].
Some psychological factors play important roles in sleep quality, mainly depression, anxiety, and loneliness. A bidirectional relationship between depression and sleep disorders has been well established in epidemiological and longitudinal studies, demonstrating that depressive symptoms can worsen sleep quality, while chronic insomnia increases the risk of developing depression [6]. Anxiety contributes to sleep difficulties through mechanisms such as hyperarousal, rumination, and increased autonomic nervous system activity, which interfere with the initiation and maintenance of sleep [7]. Furthermore, loneliness also has a substantial impact on sleep quality in the elderly. Hawkley and Cacioppo (2010) reported that loneliness increases biological and emotional vigilance, disrupts stress regulation, and reduces feelings of safety, all of which may contribute to sleep disturbances [8]. These findings are supported by meta-analytic evidence demonstrating a strong association between loneliness and poor sleep quality across all age groups, including older adults [9,10].
In addition to psychological factors, demographic characteristics such as gender, education level, marital status, and social support influence sleep quality. Sleep problems are more prevalent among elderly women than men [11]. Furthermore, strong social relationships and support from family or community networks have been shown to improve sleep quality, particularly among elderly individuals who are emotionally vulnerable [12].
In Indonesia, research on the relationship between psychological states and sleep quality in the elderly, particularly those in nursing homes, is very sparse. Elderly adults in care institutions frequently experience environmental changes, restricted social connections, and perhaps diminished emotional support from family members, all of which might raise the risk of developing depression, anxiety, and loneliness. As a result, more study is needed to offer an empirical summary of the parameters related with sleep quality in elderly in this setting.
The aim of this study is to investigate the association between sleep quality and depression, anxiety, loneliness, and demographic features among elderly nursing home patients in Indonesia. The findings are expected to provide a scientific foundation for the development of intervention programs or community-based services to promote sleep quality and overall well-being among elderly individuals living in nursing homes.
2. Materials and Methods
This study used a quantitative approach with cross-sectional design, to analyze correlational relationship and path mechanism between variables of loneliness, anxiety, and depression on sleep quality in the elderly patient at a single measurement point. The study population consisted of elderly residents living in nursing homes in the Jakarta and Tangerang areas. Sampling was conducted using a purposive sampling technique, selecting elderly individuals who were functionally independent and had adequate communication skills. A total of 123 elderly participants from 15 nursing homes were included in the study.
The inclusion criteria were individuals aged ≥60 years who were willing to participate and provided informed consent. The exclusion criteria were participants who did not complete the questionnaire in full and those with cognitive impairments that could interfere with comprehension of the research instructions.
Data were collected using four standardized instruments translated into Indonesian, as follows:
- Generalized Anxiety Disorder-7 (GAD-7)
The GAD-7 is used to measure anxiety levels, with a score of 0-4 indicating no anxiety, a score of 5-9 indicating mild anxiety, a score of 10-14 indicating moderate anxiety, and a score of 15-21 indicating severe anxiety. This can be categorized into two groups: a score <5 indicating no anxiety, and a score ≥5 indicating anxiety.
- Patient Health Questionnaire-9 (PHQ-9)
The PHQ-9 is used to assess depression, with a score of 0-4 indicating no depression, a score of 5-9 indicating mild depression, a score of 10-14 indicating moderate depression, a score of 15-19 indicating moderate-severe depression, and a score of 20-27 indicating severe depression. These scores are categorized into two groups: a score <5 indicating no depression, and a score ≥5 indicating depression.
- University of California, Los Angeles (UCLA) Loneliness Scale Version 3
Loneliness levels are measured using the UCLA Loneliness Scale Version 3. Scores of 20-34 indicate no loneliness, 35-49 indicating low loneliness, 50-64 indicating moderate loneliness, and 65-80 indicating severe loneliness. These scores are further categorized into two groups: a score of 20-34 indicating no loneliness and a score >34 indicating loneliness.
- Pittsburgh Sleep Quality Index (PSQI)
The PSQI questionnaire was used to assess sleep quality, with a score of 5 or less indicating good sleep quality and 5 or more indicating poor sleep quality.
Data Collection Procedure
The research instruments, originally developed in English, were translated into Indonesian and pre-tested to assess their reliability and validity. The finalized questionnaires were then administered in the form of a Google Form. Data collection was conducted by trained enumerators. The procedure began with an explanation of the study to potential participants, followed by the provision of written informed consent. Participants completed the questionnaires independently; however, enumerators provided assistance with reading or explaining instructions when necessary, without influencing participants’ responses.
Data Analysis
Data were analyzed using JASP statistical software through four stages: descriptive analysis, bivariate analysis, correlation matrix and path analysis. The analysis began with univariate analysis to provide a comprehensive overview of the participants’ demographic characteristics and the frequency distribution of each psychological variable studied. Bivariate analysis using Pearson’s correlation test examined pairwise associations among loneliness, anxiety, depression, and sleep quality. A correlation matrix was subsequently generated to present the overall interrelationships among the study variables and to assess their suitability for further modeling. As the core step, this study applied path analysis with a Structural Equation Modeling (SEM) approach to test the proposed theoretical model. This analysis aimed to prove the hypothesis regarding the direct effect of loneliness on sleep quality, while simultaneously testing the indirect effect through anxiety and depression as mediator variables. This test allowed researchers to observe the chain mediation mechanism to understand how psychological burdens in elderly residents in nursing homes simultaneously contribute to their decreased sleep quality.
3. Results
3.1. Demographic Characteristics of Participants
This study involved 123 elderly residents across 15 nursing homes in the Jakarta and Tangerang areas. Based on the univariate analysis, the majority of participants were women (98 individuals) (79.7%), and men (25 individuals) (20.3%). In terms of age, the largest proportion was in the 66-70 age group (52%), followed by the 71-90 age group (44.7%). Regarding length of stay in the institution, most elderly residents had resided in the nursing home for 1 to 4 years (52.8%). (Table 1)
3.2. Psychological Conditions and Sleep Quality
The distribution data shows that the majority of elderly people in nursing homes experience poor sleep quality, amounting to 88 people (71.5%). Regarding psychological conditions, the majority of participants are in the mild loneliness category (85.4%). As for anxiety, 62.6% of participants showed no symptoms of anxiety, but 37.4% of elderly people experienced mild to moderate anxiety. Meanwhile, regarding depression, 43.9% of participants were identified as having depressive symptoms with levels of severity varying from mild to moderate-severe. (Table 2)
3.3. Bivariate Relationship Analysis (Categorical and Correlation)
Bivariate analysis using the Chi-Square test showed that demographic variables such as age (p = 0.647), gender (p = 0.660), and duration of residency (p = 0.845) did not have a statistically significant relationship with sleep quality. A similar finding was found in the binary analysis of psychological variables, where depression (p = 0.668), anxiety (p = 0.388), and loneliness (p = 0.786) did not show a significant relationship with sleep quality when tested categorically.
However, a Pearson correlation test for numerical data revealed a more detailed picture. Depression (r = 0.351, p < 0.001) and anxiety (r = 0.310, p < 0.001) were shown to have a significant positive relationship with PSQI scores, indicating that increasing symptoms were associated with worsening sleep quality. In contrast, loneliness had a very low and non-significant correlation with sleep quality directly (r = -0.043). The strongest correlation was found between anxiety and depression (r = 0.637, p < 0.001), indicating that these two conditions often co-occur in the elderly. (Table 3 and Table 4)
3.4. Correlation Analysis Between Research Variables
Based on the Pearson correlation test to determine the initial linear relationship between latent variables (Table 5), the following relationship pattern was found:
3.4.1. Relationship Between Research Variables and Sleep Quality
The depression variable showed a significant positive correlation with sleep quality (r = 0.351, p < 0.001), indicating that higher levels of depression increase the PSQI score (indicating poorer sleep quality). A similar finding was found for the anxiety variable, which had a significant positive correlation with sleep quality (r = 0.310, p < 0.001). Conversely, loneliness showed a very low and insignificant correlation with sleep quality directly (r = -0.043, p > 0.05). (Table 5)
3.4.2. Relationship Between Psychological Conditions
There was a very strong and significant positive correlation between anxiety and depression (r = 0.637, p < 0.001). These findings indicate that elderly people in nursing homes who experience anxiety tend to have a higher risk of also experiencing depressive symptoms (comorbidity). (Table 5)
3.4.3. Relationship Between Loneliness and Other Research Variables
Loneliness was found to have a significant negative correlation with depression (r = -0.430, p < 0.001) and anxiety (r = -0.332, p < 0.001). This suggests that the dimension of loneliness is closely related to fluctuations in the elderly’s emotional state. (Table 5)
3.5. Path Analysis and Mediation Mechanism
The data were analyzed with path analysis and confirmed that loneliness did not have a significant direct effect on sleep quality (p = 0.566). The effect of loneliness on sleep quality occurred entirely through an indirect pathway, or a full mediation. The mediation pathway through anxiety was found to be significant (β = 0.085, p = 0.004), as was the mediation pathway through depression (β = -0.053, p = 0.048). (Table 6) The most crucial finding was the existence of a chain mediation mechanism where loneliness triggers anxiety, which then triggers depression, and ultimately results in a significant decline in sleep quality in the elderly (β = -0.040, p = 0.045). (Figure 1)
4. Discussion
The results of this study indicate that 71.5% of elderly individuals residing in nursing homes experience poor sleep quality, a finding consistent with previous research. A meta-analysis by Vaquero-Álvarez et al. (2021) reported a prevalence of sleep disorders ranging from 55% to 80% among elderly populations, particularly among those with psychological comorbidities [13]. Studies focusing on elderly individuals living in institutional settings have consistently shown a higher prevalence of poor sleep quality compared to those living in the community, likely due to reduced autonomy, rigid daily routines, and limited control over the sleep environment [3,4]. These findings support the view that institutionalization constitutes a contextual risk factor that amplifies the impact of psychological stress on sleep quality. In contrast, demographic variables such as age, gender, and duration of residence did not demonstrate statistically significant associations with sleep quality in this study.
4.1. Depression and Anxiety as Predictors of Sleep Quality
This study found that depression (r = 0.351) and anxiety (r = 0.310) were significantly associated with poorer sleep quality among elderly individuals living in nursing homes. These findings are consistent with existing literature describing a strong bidirectional relationship between sleep disturbances and mood disorders [13]. A meta-analysis by Baglioni et al. (2011) demonstrated that insomnia doubles the risk of subsequent depression, while depressive symptoms exacerbate sleep fragmentation and prolong sleep latency [6]. From a neurobiological perspective, both depression and anxiety contribute to sleep disturbances through activation of the hypothalamic–pituitary–adrenal (HPA) axis and elevated nocturnal cortisol secretion, which interferes with slow-wave sleep [14]. This mechanism is particularly relevant in elderly individuals, for whom homeostatic sleep regulation is already compromised due to aging.
4.2. Perfect Mediation Mechanism: Why Loneliness Does Not Directly Affect Sleep Quality
One of the key findings of this study is the absence of a significant direct effect of loneliness on sleep quality, as demonstrated by both correlation analysis and direct path analysis within the SEM model (p = 0.566). This finding supports the Social Hypervigilance Theory proposed by Hawkley and Cacioppo (2010), which posits that loneliness does not directly impair physiological functioning but instead operates through heightened emotional and cognitive vigilance [8]. In the context of elderly individuals living in nursing homes, loneliness appears to increase vulnerability to anxiety and depression, which in turn become the primary determinants of sleep disturbance.
4.3. Chain Mediation: Loneliness → Anxiety → Depression → Sleep Quality
The most important finding of this study is the significant chain mediation pathway in which loneliness increases anxiety, anxiety heightens the risk of depression, and depression ultimately leads to poorer sleep quality (β = −0.040, p = 0.045). This result aligns with findings by Steptoe et al. (2015), which emphasize that emotional well-being in elderly individuals is strongly influenced by long-term affective stability rather than objective social conditions alone. Lonely elderly individuals in nursing homes may experience persistent rumination and excessive worry related to health, dependency, or uncertainty about the future, manifesting as anxiety. When sustained, this anxiety can evolve into depressive symptoms characterized by helplessness and hopelessness, which are strongly associated with sleep disruption [15,16]. Heightened sympathetic nervous system activity associated with these emotional states maintains physiological arousal, thereby impairing sleep initiation and maintenance.
The strong correlation between anxiety and depression observed in this study (r = 0.637) is consistent with the tripartite model of anxiety and depression proposed by Clark and Watson (1991), which describes shared negative affect as a common underlying component of both conditions. In elderly individuals, this comorbidity is often chronic and contributes to persistent sleep disturbances [17].
4.4. Clinical and Policy Implications for Elderly Individuals in Nursing Homes
The finding that loneliness affects sleep quality entirely through psychological mediators has important clinical and policy implications. Interventions that focus exclusively on improving the physical sleep environment or prescribing pharmacological treatments for insomnia may be insufficient if anxiety and depression are not concurrently addressed. Evidence from intervention studies suggests that social support–based programs, group activities, and structured psychosocial interventions are more effective in improving sleep quality among elderly individuals than symptom-focused approaches alone [18].
Furthermore, the correlation matrix results indicate that depression has the strongest association with poor sleep quality compared to anxiety, underscoring the need to prioritize mental health interventions in nursing homes. Psychoeducational programs, routine screening for anxiety and depression, and the provision of meaningful social activities may help mitigate loneliness and disrupt the psychological cascade leading to sleep disturbances. Overall, these findings highlight that improving sleep quality among elderly individuals living in nursing homes requires a holistic approach that integrates psychosocial care alongside environmental and medical interventions.
5. Conclusions
Based on the findings from 123 elderly individuals residing in nursing homes, the majority of participants experienced poor sleep quality. Loneliness did not have a direct effect on sleep quality but exerted its influence entirely through anxiety and depression. These results confirm the presence of a significant chain mediation mechanism, whereby loneliness increases anxiety, which subsequently exacerbates depressive symptoms and ultimately reduces sleep quality among elderly individuals. Accordingly, interventions aimed at improving sleep quality in nursing homes should prioritize strengthening social support to reduce loneliness, alongside comprehensive mental health strategies to disrupt the interconnected cycle of anxiety and depression in this population.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Path analysis illustrating the effect of loneliness on sleep quality through anxiety and depression in elderly; Table S1: Distribution of demographic characteristics of the participants; Table S2: Descriptive statistics of research variables; Table S3: Bivariate analysis (multilevel); Table S4: Bivariate analysis (binary); Table S5: Correlation matrix of loneliness, depression, anxiety, and sleep quality in elderly; Table S6: Pathway coefficients of direct, indirect, and total effects among loneliness, anxiety, depression, and sleep quality in elderly.
Author Contributions
Conceptualization, S.H. and C.R.P.A.; methodology, S.H., C.R.P.A., H.C., I.L.G., L.A.K.; software, H.C., I.L.G., L.A.K.; validation, S.H., C.R.P.A., and J.R.W.; formal analysis, I.L.G. and H.C.; investigation, S.H., I.L.G., L.A.K., J.B.; resources, S.H., H.C., I.L.G.; data curation, I.L.G., L.A.K., J.B.; writing—original draft preparation I.L.G., L.A.K, J.B.; writing—review and editing, H.C., I.L.G, J.B.; visualization, S.H., C.R.P.A., H.C.; supervision, S.H. and C.R.P.A.; project administration, S.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Acknowledgments
The authors would like to thank the nursing home management and staff for their cooperation during this study. The authors also acknowledge Atma Jaya Catholic University of Indonesia and Atma Jaya Teaching & Research Hospital, particularly the Department of Psychiatry and Behavioral Sciences, School of Medicine and Health Sciences; Department of Psychology and the Centre of Societal and Development Studies; and the Department of Neurology for their valuable collaboration, academic support, and institutional assistance in conducting this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| GAD-7 | Generalized Anxiety Disorder-7 |
| HPA | Hypothalamic–Pituitary–Adrenal |
| PHQ-9 | Patient Health Questionnaire-9 |
| PSQI | Pittsburgh Sleep Quality Index |
| r | Pearson correlation coefficient |
| β | Standardized regression coefficient |
| SEM | Structural Equation Modeling |
| UCLA | University of California, Los Angeles |
| UNDESA | United Nations Department of Economic and Social Affairs |
References
- United Nations Department of Economic and Social Affairs. World Population Ageing 2020 Highlights: Living Arrangements of Older Persons.; United Nations: New York, NY, USA, 2020. [Google Scholar]
- Badan Pusat Statistik. Statistics of the Elderly Population 2021.; BPS: Jakarta, Indonesia, 2021. [Google Scholar]
- Miner, B.; Kryger, M.H. Sleep in the aging population. Sleep Med. Clin. 2017, 12, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Crowley, K. Sleep and sleep disorders in older adults. Neuropsychol. Rev. 2011, 21, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; et al. Sleep disturbances and risk of cognitive decline in older adults: A meta-analysis. Sleep Med. Rev. 2018, 40, 1–11. [Google Scholar] [CrossRef]
- Baglioni, C.; Battagliese, G.; Feige, B.; et al. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef]
- Harvey, A.G. A cognitive model of insomnia. Behav. Res. Ther. 2002, 40, 869–893. [Google Scholar] [CrossRef] [PubMed]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Cacioppo, S. Social relationships and health: The toxic effects of perceived social isolation. Soc. Personal. Psychol. Compass 2014, 8, 58–72. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.C.; Williams, A.B.; Mladen, S.N.; Perrin, P.B.; Dzierzewski, J.M. Reciprocal effects between loneliness and sleep disturbance in older Americans. Health Psychol. Open 2020, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gulia, K.K.; Kumar, V.M. Sleep disorders in the elderly: A growing challenge. Psychogeriatrics 2018, 18, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef] [PubMed]
- Vaquero-Álvarez, M.; Mota-Romero, E.; Ríos-León, M.; et al. Anxiety, depression and sleep quality in the elderly: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 11842. [Google Scholar] [CrossRef]
- Meerlo, P.; Sgoifo, A.; Suchecki, D. Restricted and disrupted sleep: Effects on autonomic function, neuroendocrine stress systems and stress responsivity. Sleep Med. Rev. 2008, 12, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Shankar, A.; Demakakos, P.; Wardle, J. Social isolation, loneliness, and all-cause mortality in older men and women. Proc. Natl. Acad. Sci. U.S.A. 2013, 110, 5797–5801. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective wellbeing, health, and ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.A.; Watson, D. Tripartite model of anxiety and depression: Psychometric evidence and taxonomic implications. J. Abnorm. Psychol. 1991, 100, 316–336. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Olmstead, R.; Carrillo, C.; et al. Cognitive behavioral therapy vs. tai chi for late life insomnia and inflammatory risk: A randomized controlled comparative efficacy trial. Sleep 2014, 37, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Path Analysis Illustrating the Effect of Loneliness on Sleep Quality through Anxiety and Depression in Elderly.
Figure 1.
Path Analysis Illustrating the Effect of Loneliness on Sleep Quality through Anxiety and Depression in Elderly.
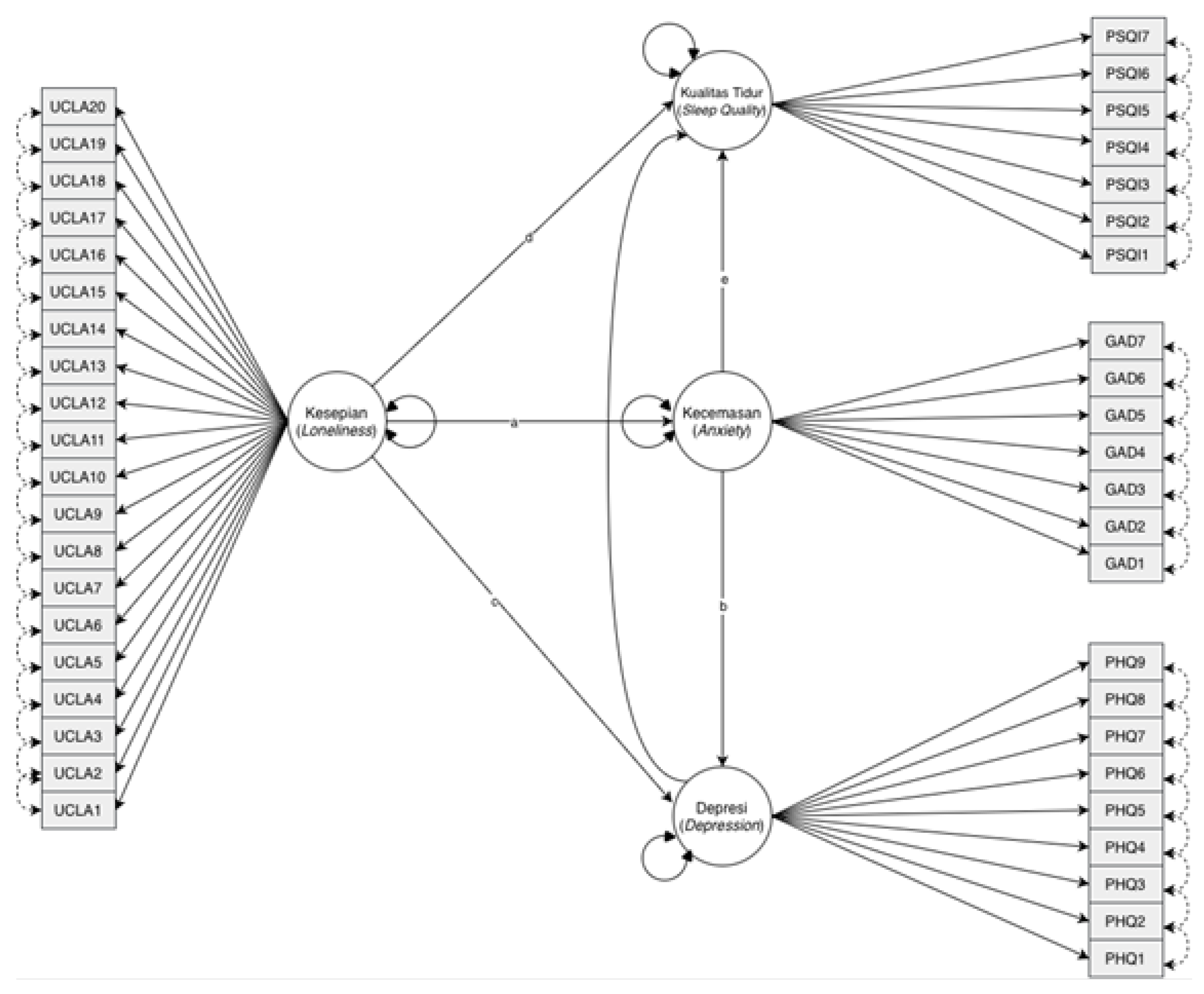

Table 1.
Distribution of Demographic Characteristics of the Participants.
| Category | N (%) |
|---|---|
|
Age Pre- elderly 66-70 years 71-90 years >90 years |
3 (2.4) 64 (52) 55 (44.7) 1 (8) |
|
Gender Women Men |
98(79.7) 25 (20.3) |
|
Duration of Residency <1 year 1-4 years 5–8 years >8 years |
11 (8.9) 65 (52.8) 23 (18.7) 21 (17.1) |
Table 2.
Descriptive Statistics of Research Variables.
| Variables | N% |
|---|---|
| Depression (PHQ) | |
| No depression | 69 (56.1) |
| Mild depression | 36 (29.3) |
| Moderate depression | 17 (13.8) |
| Moderate-severe depression | 1 (0.8) |
| Anxiety (GAD) | |
| No anxiety | 77 (62.6) |
| Mild anxiety | 34 (27.6) |
| Moderate anxiety | 12 (9.8) |
| Loneliness (UCLA) | |
| No loneliness | 6 (4.9) |
| Low loneliness | 105 (85.4) |
| Moderate loneliness | 11 (8.9) |
| Severe loneliness | 1 (0.8) |
| Sleep Quality (PSQI) | |
| Good | 35 (28.5) |
| Poor | 88 (71.5) |
Table 3.
Bivariate Analysis (Multilevel).
| Sleep Quality | p-value | ||
|---|---|---|---|
| Good (%) | Poor (%) | ||
| Age | 0.647 | ||
| Pre-elderly | 1 (33) | 2 (66.7) | |
| 66-70 years | 21 (32.8) | 43 (67.2) | |
| 71-90 years | 13 (23.6) | 42 (76.4) | |
| >90 years | - | 1 (100) | |
| Gender | 0.660 | ||
| Women | 27 (27.6) | 71 (72.4) | |
| Men | 8 (32) | 17 (68) | |
| Duration of Residency | 0.845 | ||
| <1 year | 4 (36.4) | 7 (63.6) | |
| 1-4 years | 17 (26.2) | 48 (73.8) | |
| 5-8 years | 6 (26.1) | 17 (73.9) | |
| >8 years | 7 (33.3) | 14 (66.7) | |
| Depression (PHQ) | 0.876 | ||
| No depression | 20 (29) | 49 (71) | |
| Mild depression | 11 (30.6) | 25 (69.4) | |
| Moderate depression | 4 (23.5) | 13 (76.5) | |
| Moderate-severe depression | - | 1 (100) | |
| Anxiety (GAD) | 0.559 | ||
| No anxiety | 24 (31.2) | 53 (68.8) | |
| Mild anxiety | 9 (26.5) | 25 (73.5) | |
| Moderate anxiety | 2 (16.7) | 10 (83.3) | |
| Loneliness (UCLA) | 0.439 | ||
| No loneliness | 2 (33.3) | 4 (66.7) | |
| Low loneliness | 32 (30.5) | 73 (69.5) | |
| Moderate loneliness | 1 (9.1) | 10 (90.9) | |
| Severe loneliness | - | 1(100) | |
Table 4.
Bivariate Analysis (Binary).
| Sleep Quality | p-value | ||
|---|---|---|---|
| Good (%) | Poor (%) | ||
| Age | 0.647 | ||
| Pre-elderly | 1 (33) | 2 (66.7) | |
| 66-70 years | 21 (32.8) | 43 (67.2) | |
| 71-90 years | 13 (23.6) | 42 (76.4) | |
| >90 years | - | 1 (100) | |
| Gender | 0.660 | ||
| Women | 27 (27.6) | 71 (72.4) | |
| Men | 8 (32) | 17 (68) | |
| Duration of Residency | 0.845 | ||
| <1 year | 4 (36.4) | 7 (63.6) | |
| 1-4 years | 17 (26.2) | 48 (73.8) | |
| 5-8 years | 6 (26.1) | 17 (73.9) | |
| >8 years | 7 (33.3) | 14 (66.7) | |
| Depression (PHQ) | 0.668 | ||
| No depression | 16 (26.7) | 44 (73.3) | |
| Depression | 19 (30.2) | 44 (69.8) | |
| Anxiety (GAD) | 0.388 | ||
| No anxiety | 24 (31.2) | 53 (68.8) | |
| Anxiety | 11 (23.9) | 35 (76.1) | |
| Loneliness (UCLA) | 0.786 | ||
| No loneliness | 2 (33.3) | 4 (66.7) | |
| Loneliness | 33 (28.2) | 84 (71.8) | |
Table 5.
Correlation Matrix of Loneliness, Depression, Anxiety and Sleep Quality in Elderly.
| Loneliness | Depression | Anxiety | Sleep Quality | |
|---|---|---|---|---|
| Loneliness | - | -.430** | -.332** | -.043 |
| Depression | -.430** | - | .637** | .351** |
| Anxiety | -.332** | .637** | - | .310** |
| Sleep Quality | -.043 | .351** | .310** | - |
** p-value < .001.
Table 6.
Coefficient pathway of direct effect, indirect effect, and total effect among loneliness, depression, anxiety, and sleep quality in elderly.
Table 6.
Coefficient pathway of direct effect, indirect effect, and total effect among loneliness, depression, anxiety, and sleep quality in elderly.
| Relationship between variables | Estimation | Std. Error | z-value | p-value |
|---|---|---|---|---|
|
Direct Effect Loneliness → Depression |
.666 |
.039 |
17.266 |
<.001 |
| Loneliness → Anxiety | .501 | .029 | 17.112 | <.001 |
| Anxiety→ Depression | .569 | .037 | 15.476 | <.001 |
| Anxiety → Sleep Quality | .091 | .025 | 3.597 | <.001 |
| Depression → Sleep Quality | -.139 | .071 | -1.971 | .049 |
| Indirect Effect | ||||
| Loneliness → Anxiety → Depression | .285 | .021 | 13.437 | <.001 |
| Loneliness → Anxiety → Sleep Quality | .085 | .030 | 2.888 | .004 |
| Loneliness → Depression → Sleep Quality | -.053 | .027 | -1.974 | .048 |
| Loneliness → Anxiety → Depression → Sleep Quality | -.040 | .021 | -1.925 | .045 |
| Total effect | ||||
| Loneliness → Sleep Quality | -.006 | .010 | -.574 | .566 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



