
Submitted:
17 January 2026
Posted:
20 January 2026
You are already at the latest version
Abstract
Background/Objectives: Achieving a balanced wholefood diet while stabilising glycae-mic management is challenging for many people with type 2 diabetes (T2D) due to barri-ers such as food preparation skills, time, and medication effects. Diabetes-specific nutri-tional formulas (DSNF) are nutritionally complete products designed to support glycae-mic management and overall nutritional adequacy and may complement wholefood die-tary approaches when these are not feasible or are insufficient. Despite growing clinical evidence of efficacy, practical guidance for routine use is limited. Methods: A multidisci-plinary expert working group developed a Clinical Practice Guide (CPG) for integrating DSNF into diabetes care. Development was informed by a literature review and iterative consensus among experts, including representatives of the Australian Diabetes Society, Australian Diabetes Educators Association, and the Royal Australian College of General Practitioners. Results: The CPG outlines a three-step pathway: (1) Assess suitability (clinical indications, contraindications, preferences, cultural context); (2) Tailor the approach (indi-vidual goals, dose/timing relative to weight and body composition goals and observed glycaemic patterns, integration with lifestyle care); and (3) Monitor progress (baseline, 2–4 weeks to assess initial response, then 3, 6, and 12 months for glycaemic indices, weight/body composition where available, and medication review). Conclusions: This CPG provides practical, multidisciplinary guidance for the person-centred use of DSNF as an adjunct to standard care, supporting translation of current evidence into clinical prac-tice and promoting consistent, multidisciplinary implementation.
Keywords:
clinical guidance
; diabetes specific nutritional formula
; DSNF
; nutrition
; nutritional status
; type 2 diabetes
1. Introduction
Type 2 diabetes (T2D) is a growing global health concern, and effective nutrition management plays a critical role in improving glycaemic outcomes and reducing the risk of diabetes-related complications. Lifestyle interventions, including diet, exercise and associated reduction in adipose tissue, are recommended as first-line therapy for glycaemic management of T2D [1,2]. However, only approximately half of all people with T2D are able to follow the standard dietary and lifestyle advice due to various barriers, including access to affordable nutritious food, knowledge and skills for food preparation, time pressures, cultural and religious preferences, frailty, energy and appetite levels [3,4,5,6]. These challenges may contribute to the mean HbA1c in Australians with T2D remaining over 8% (higher than the target of 7% or below) over the last decade, despite significant advances in management and medications [7]. Australian Institute of Health and Welfare 2019-2020 data revealed 52% of adults with T2D had HbA1c results above the recommended targets [8].
Approximately 45% of people with T2D have multiple micronutrient deficiencies [9]. Multiple factors contribute to nutritional deficiencies in people with diabetes, including altered protein metabolism, increased fluid losses, impaired nutrient absorption, and inadequate or imbalanced dietary intake. Restrictive eating patterns further exacerbate these risks. In addition, diabetes treatments such as metformin, incretin-based therapies, including glucagon-like peptide-1 receptor agonists [GLP-1 RAs] and dual glucose-dependent insulinotropic polypeptide/GLP-1 receptor agonists [GIP/GLP-1 RAs]; and bariatric surgery can also precipitate or worsen micronutrient deficiencies [10]. The consequences of these nutritional deficiencies include destabilised glucose management [11], fatigue, lethargy, weakness and diabetes-related sarcopenia due to inadequate protein and micronutrient intakes [8]. These consequences can further exacerbate barriers to utilising the wholefoods dietary approach [12], emphasising the importance of tailored nutrition strategies to support the complex dietary needs of people with diabetes. The clinical relevance of sarcopenic obesity and sarcopenic diabetes is increasingly recognised as an unmet priority in diabetes care [13].
A recent expert consensus statement, with representatives from key diabetes stakeholders including the Australian Diabetes Society (ADS) and the Australian Diabetes Educators Association (ADEA), suggested Diabetes Specific Nutritional Formula (DSNF) as a simple and practical way to support people with T2D in optimising their nutritional intake, improving glycaemic management and overall health outcomes when wholefood options are not feasible or not achieving desired outcomes [3]. DSNF are a specialised oral nutritional supplement, formulated to support blood glucose management and nutritional needs for people with diabetes and/or impaired glucose tolerance (pre-diabetes). They have been shown to improve glycaemic management [6,14,15,16,17,18,19], nutritional status, weight management, body composition, and cardiometabolic health [14,18,19]. A meta-analysis (18 studies; n=845) found that compared to standard oral nutrition formulas, DSNF treatment in people with diabetes led to improvements in postprandial glucose, incremental glucose response, plasma insulin, mean blood glucose level, glycosylated haemoglobin (HbA1c), glucose variability, and mean administered insulin dose [18]. In a 90-day intervention study, those using DSNF had a twofold greater weight loss ( −1.74 kg vs. –0.76 kg, p < 0.001) compared to usual care. Importantly, the DSNF group also had a significantly greater loss of visceral adipose tissue (−6.52% vs. –0.95%) compared to usual care, while gaining twice as much fat-free mass (1.44% vs. 0.79%) [19]. The magnitude of these effects suggests meaningful benefits for glycaemic regulation, metabolic health, and body composition, supporting the use of DSNF as an evidence-based adjunct to conventional dietary approaches. However, limited health professional awareness and understanding of the benefits and practicalities of when and how to use DSNF remain barriers to their use [3,20,21]. This paper aims to present the rationale, development process, and core components of a national CPG that provides evidence-based direction for health professionals on incorporating DSNF into diabetes care. The primary focus of this CPG is type 2 diabetes, where the majority of evidence supporting the use of DSNF exists. While DSNF use has also been studied in other populations, including type 1 diabetes, gestational diabetes, and prediabetes, the evidence base in these groups is emerging [22,23,24,25,26]. Accordingly, recommendations for these populations should be applied with appropriate clinical judgment and consideration of individual clinical context.
2. Materials and Methods
To inform the development of this CPG, an expert working group was formed in April 2025 to build on the previously published consensus statement and develop this CPG using a structured, evidence-informed and consensus-based methodology, consistent with established approaches to guideline development in these areas. Development of the CPG followed structured consensus methods consistent with internationally recognised guidance frameworks, including the World Health Organisation Handbook for Guideline Development and National Institute for Health and Care Excellence guideline development principles [27,28].
2.1. Literature Review
A scoping literature review was undertaken by the working group to summarise the current evidence on DSNF and to inform the structure and content of the initial draft guidance. The review aimed to map the breadth of available evidence rather than to conduct a formal systematic review.
Searches were conducted for studies published between January 2010 and June 2024 using PubMed, Embase, and Google Scholar. Search strategies combined terms related to DSNF with terms relating to diabetes type and relevant clinical outcomes. Key search terms included, but were not limited to: “diabetes-specific nutritional formula”, “diabetes-specific formula”, “glycaemia-targeted specialised nutrition”, “specialised nutrition formula”, AND “type 2 diabetes”, “type 1 diabetes”, “gestational diabetes”, “prediabetes”, AND “glycaemic control”, “HbA1c”, “weight management”, “body composition”, “nutritional status”, “cardiometabolic risk”.
An example PubMed search strategy was:
("diabetes-specific nutritional formula"[tiab] OR "diabetes-specific formula"[tiab] OR "glycaemia-targeted specialised nutrition"[tiab] OR "glycemia-targeted specialized nutrition"[tiab] OR "specialised nutrition formula"[tiab] OR "specialized nutrition formula"[tiab] OR "diabetes formula"[tiab] OR "diabetes-specific oral nutrition supplement"[tiab] OR "oral nutrition supplement"[tiab] OR "medical nutrition therapy formula"[tiab] OR "enteral nutrition"[MeSH] OR "food, formulated"[MeSH])
AND
("type 2 diabetes"[tiab] OR "type 1 diabetes"[tiab] OR "gestational diabetes"[tiab] OR "prediabetes"[tiab] OR "Diabetes Mellitus, Type 2"[MeSH] OR "Diabetes Mellitus, Type 1"[MeSH] OR "Diabetes, Gestational"[MeSH] OR "Prediabetic State"[MeSH])
AND
( "glycaemic control"[tiab] OR "glycemic control"[tiab] OR "HbA1c"[tiab] OR "weight management"[tiab] OR "body composition"[tiab] OR "nutritional status"[tiab] OR "cardiometabolic risk"[tiab] OR "Hemoglobin A, Glycosylated"[MeSH] OR "Body Composition"[MeSH] OR "Nutritional Status"[MeSH] OR "Blood Glucose"[MeSH])
Equivalent terms and controlled vocabulary (e.g., MeSH and Emtree terms) were used where applicable in PubMed and Embase. Google Scholar searches were used to identify additional relevant studies and recent publications not yet indexed in bibliographic databases. Searches were limited to human studies published in English. Evidence types included randomised controlled trials, observational studies, secondary analyses, and relevant systematic reviews.
Studies were included if they involved adults with diabetes or prediabetes and evaluated the effects of DSNFs on relevant clinical or nutritional outcomes. This included studies involving adults with type 2 diabetes, type 1 diabetes, gestational diabetes, or prediabetes. Exclusion criteria included animal studies, non-English publications, paediatric populations, and interventions not related to DSNF use. Evidence from included studies was synthesised narratively, with emphasis on study design, sample size, and clinical relevance. No formal evidence-grading framework was applied in this version of the guide.
2.2. Consensus Development
Following the literature review, a structured Consensus Development Workshop was conducted using established approaches such as the RAND/UCLA Appropriateness Method and formal consensus techniques [29,30]. Experts representing key disciplines contributed to small-group discussions, voting rounds, and thematic review of recommendations. Consensus on each recommendation required a minimum agreement threshold of ≥80%. Areas of agreement and divergence were documented, refined through written feedback, and finalised across multiple review cycles to ensure methodological rigour and alignment with best-practice consensus frameworks.
The expert working group included representatives from the ADS, ADEA, and Royal Australian College of General Practitioners (RACGP) as well as independent experts in their fields. This diverse, multidisciplinary team included experts across primary care, nutrition and dietetics, diabetes education, pharmacy, nursing, endocrinology, and research, ensuring the CPG is informed by published literature, expert consensus, and clinical experience, and is practical and applicable to real-world clinical practice.
The overall aim of this CPG is to inform health professionals with evidence-based guidance, supporting them to confidently integrate DSNF into the management of diabetes, with a focus on T2D or those at risk, in clinical practice. The target audience for this CPG is any health professional involved in the diabetes care pathway, including but not limited to General Practitioners, Dietitians, Diabetes Educators, Pharmacists, Nurse Practitioners, Endocrinologists, Exercise Physiologists, Geriatricians, and Practice Nurses. Engaging a multi-disciplinary audience is important to ensure that people with diabetes receive consistent guidance from all members of their healthcare team, enhancing the patient experience and increasing the likelihood of beneficial outcomes [31,32,33,34]. This DSNF CPG is intended to be used in conjunction with existing guidelines, including the ADS T2D Glycaemic Management Algorithm [1], ADS Obesity Treatment Algorithm [35], and the RACGP Management of Type 2 Diabetes: A handbook for General Practice Guidelines [36]. Please note, the sponsor had no role in evidence appraisal, consensus development, or manuscript preparation.
3. Results
3.1. What are DSNF?
DSNF feature slow-release, low glycaemic index (GI) carbohydrates, high-biological value protein, healthy monounsaturated (MUFAs) and/or polyunsaturated fatty acids (PUFAs), added dietary fibre, vitamins and minerals, delivered in kilojoule-controlled portions.
DSNF can be used irrespective of body weight and tailored according to an individual’s needs. They can be used as partial replacements for selected eating occasions in those with healthy weight and body composition, low-kilojoule replacements for two eating occasions for those who carry excess adipose tissue, or nutritional supplements as determined by appropriate health professionals [3]. Their specific formulation and versatility across multiple clinical scenarios, regardless of body weight, distinguish DSNF from very low energy diets (VLED) and standard oral nutrition supplements (ONS) (Table 1) [3,37,38].
3.2. Steps to Implementing DSNF in Practice.
The steps of the CPG are shown in Figure 1. The companion to the guide, which includes additional details, is included in the Supplementary Material (S1).
3.2.1. Step 1: Assess Suitability
DSNF are a valuable tool primarily indicated for people with T2D, but they may also be suitable for those with type 1 and gestational diabetes, or impaired glucose tolerance (pre-diabetes), noting that the evidence base in these populations is emerging and application should be guided by clinical judgment [22,23,24,25,26]. They are particularly useful when a wholefood dietary approach is not achieving glycaemic targets (e.g., HbA1c) or is not always feasible. DSNF can assist in overcoming common barriers to healthful nutrition, including supporting people who are time-poor, travelling, overwhelmed or anxious about managing their condition, low in health literacy, limited in cooking skills, low appetite, post-surgery, or are dealing with another acute or chronic illness.
Additionally, they can support individuals whose current dietary intake does not meet recommended nutritional requirements. This may include people with low appetite, those recovering from surgery, older adults with frailty, individuals after acute illnesses or with chronic illnesses, or those using diabetes medications, such as Sodium-Glucose Transport 2 (SGLT2) inhibitors and incretin-mimetic medications (e.g. GLP-1 RAs and GIP/GLP-1 RAs), which are associated with loss of lean mass including skeletal muscle [14,39]. Importantly, DSNF can be used in people with a range of body weights and compositions, including those with excess adiposity, those of ‘healthy’ weight and those who are underweight [21].
DSNF are generally not recommended for people who have allergies or intolerances to any of the product’s ingredients, follow cultural dietary practices that may not align with the formula’s composition, or have other specific medical needs that may preclude use. They may not be necessary if a wholefoods diet is followed consistently.
3.2.2. Step 2: Tailor the Approach
To ensure effective and person-centred use of DSNF, it is necessary to discuss and prioritise the individual's goals. These may include improving glycaemic management, supporting nutritional intake, reducing body fat, achieving a healthy body weight, improving muscle mass, increasing energy levels and reducing cardiovascular risk [3,27,40].
Once goals are identified, a personalised DSNF plan should be developed based on weight- and body-composition related goals. For fat mass reduction, a common approach is to use two servings per day to replace main meals (for example, breakfast and lunch). Or, if the individual currently includes snacks in their meal plan, a snack may be replaced (for example, breakfast and afternoon tea). For weight maintenance, one serving per day may be sufficient, replacing all or part of a main meal or another, smaller eating portion such as a snack. For those aiming to gain weight, two servings per day may be added between main meals, for example, morning and afternoon tea, as a nutritional supplement to boost energy and nutrient consumption [32]. DSNF should always be used as part of a broader diabetes management plan.
DSNF reduce glucose variability [41]. For maximum impact, it is recommended that meal timing should be individualised. For example, if blood glucose excursions consistently occur after specific eating occasions, consider using a DSNF to replace the food/snack that leads to the highest excursions. If hypoglycaemia is more of a concern, DSNF may potentially be used as a snack prior to the expected low blood glucose to help stabilise blood glucose levels [42]. For example, where a person is at risk of nocturnal hypoglycaemia while sleeping, a DSNF may be added as an ‘evening supplement’ to help reduce the risk. If blood glucose patterns are unknown, breakfast is often a good starting point for replacement, followed by additional eating occasions like morning or afternoon tea, as these are the most studied timings in existing research [6,16,17,25,40,43,44,45]. Other eating occasions may also be appropriate, depending on social, cultural, and lifestyle factors. Ultimately, the choice of when and how to incorporate DSNF should be tailored to individual preferences and guided by health professional advice.
Although DSNF formulations vary in macronutrient composition, fat sources, and fibre type, they share core formulation principles relevant to clinical practice, including low-GI carbohydrate blends, predominantly unsaturated fat sources, and micronutrient profiles designed to support glycaemic management and nutritional adequacy in people with diabetes. Accordingly, this CPG adopts a category-based, product-neutral approach, with selection tailored to individual clinical goals (e.g., glycaemic patterns, weight management, or nutritional support) rather than specific brands or formulations.
3.2.3. Step 3: Monitor Progress
Monitoring of patients using DSNF should tie in with standard best practice guidelines. Baseline attributes should be noted at commencement, and progress should be regularly monitored to allow adaptation of the implementation plan as needed. Monitoring of targets, such as glucose profile including HbA1c, lipid profile including triglycerides and HDL-C, liver function tests, body composition, weight, waist circumference or other targets, should continue as per standard care, with additional early review at 2-4 weeks to assess whether the individual is successfully incorporating the DSNF into their routine.
Evidence from randomised and observational studies suggests that DSNF are generally acceptable to patients and associated with high short- to medium-term adherence. Studies have reported sustained hedonic ratings and compliance exceeding 88–98% across intake levels ranging from one to four servings per day over periods of three to six months [14,19,46]. Several studies have also reported improvements in quality of life following DSNF use over three to six months [23,47,48]. These findings support routine clinical monitoring of acceptability, tolerance, taste fatigue, and patient-reported outcomes when DSNFs are prescribed.
At 3, 6, and 12 months, a broader assessment should be conducted, including (but not limited to) ongoing DSNF use, evaluating glycaemic measures, including markers such as fasting blood glucose and HbA1c, tracking changes in weight and/or waist circumference, assessing body composition where possible, and conducting a medication review. It is important to note that improvements in glycaemic management or weight loss may increase the risk of hypoglycaemia, requiring adjustment of glucose-lowering medication. Achieving clinically significant fat mass loss may necessitate adjustment of their antihypertension medication.
The duration of DSNF use should be guided by the individual’s progress toward their goals. If goals are met, the individual or caregiver and healthcare provider can collaboratively decide whether to continue (maintain, decrease or use intermittent) or pause DSNF use, keeping in mind that the benefits may diminish if use is discontinued, as research data only exists for the duration of use. If goals have not been achieved, it is important to revisit and refine the goals or the way DSNF are being used. If the individual is not already seeing an Accredited Practising Dietitian, referral can be helpful at this point for more tailored support.
Available evidence is largely derived from short-term studies (≤12 months), which have not identified any major safety concerns. DSNF are specifically formulated to meet the nutritional needs of people with diabetes, with nutrient levels within established safety limits. However, data on long-term safety, durability, and maintenance of benefits are limited, highlighting the need for ongoing monitoring, clinical discretion and further long-term research. Importantly, DSNF should always be integrated into a comprehensive diabetes care plan that includes support for adopting a nutritious wholefoods eating pattern, regular physical activity, quality sleep, effective blood glucose and medication management, and regular input from the diabetes care team.
4. Discussion
4.1. Clinical and Practical Implications
This CPG provides a structured, evidence-based framework to support health professionals in integrating DSNF into routine diabetes care. DSNF can be effectively incorporated alongside pharmacotherapy, lifestyle modification, and diabetes education, offering a flexible nutritional option for individuals who are unable to meet dietary goals through wholefoods alone. When used in combination with contemporary agents such as incretin-mimetic therapies and SGLT2 inhibitors, DSNF may enhance glycaemic stability, support weight management, and help preserve lean mass, particularly in older adults or those with frailty. Integration within multidisciplinary care models ensures safe and person-centred implementation. From a system-level perspective, adoption of DSNF is influenced by cost, product access, and cultural relevance. Addressing these factors through clinician education, patient engagement, and potential reimbursement mechanisms will be essential to achieving equitable uptake and sustainable outcomes. While this CPG was developed within the Australian healthcare context, its principles may be relevant to other settings. However, implementation outside Australia may require adaptation to local healthcare systems, resource availability, workforce structures, and cultural practices.
Equity considerations are central to the implementation of this CPG. Access to DSNF and appropriately trained healthcare professionals may be constrained in low-socioeconomic, rural, and remote settings, where availability, cost, and workforce capacity vary substantially [49,50,51]. While DSNFs are generally low-cost nutritional interventions, affordability alone does not ensure equitable access, particularly in settings where supply chains, prescribing pathways, and workforce support are limited. Local adaptation of recommendations for DSNF use will therefore be required to support equitable uptake within existing service structures and resource limitations [50,52]. Future research and implementation efforts should prioritise evaluation of strategies that address these geographic, socioeconomic, and workforce-related barriers, to ensure that the potential benefits of DSNF use are realised across diverse populations [49,51].
4.2. Strengths and Limitations
This CPG is the first of its kind to provide practical, multidisciplinary recommendations for integrating DSNF into routine diabetes care. Developed by a diverse expert working group, including representatives from the ADEA, ADS, and RACGP, the guide is grounded in current evidence, consensus, and real-world clinical experience. The three-step pathway offers clear, actionable guidance for health professionals, supporting person-centred care and consistent implementation across disciplines. The CPG addresses a significant gap in diabetes management by offering solutions for individuals who face barriers to wholefood dietary approaches, and it is designed to be adaptable to a wide range of clinical scenarios and patient needs.
Recommendations in this CPG are product-neutral and based on a category-wide evidence base rather than on specific commercial brands. Evidence supporting DSNF use was drawn from multiple manufacturers and independent studies, including systematic reviews and meta-analyses, to ensure recommendations reflect the category as a whole. Some of the evidence cited originates from meta-analyses commissioned by the Diabetes Nutrition Study Group (DNSG) of the European Association for the Study of Diabetes (EASD) [37], and from recommendations developed by the European Society for Clinical Nutrition and Metabolism (ESPEN) and the DNSG [13]. Importantly, these works were conducted without industry involvement or funding support. In areas where independent comparative data or long-term validation remain limited, recommendations are based on expert consensus and should be applied with clinical judgment. Further independent research will help strengthen future iterations of this guide.
However, a limitation of this CPG is that recommendations are not linked to a formal evidence-grading framework such as GRADE. While the guide draws on the best available evidence and structured expert consensus, the strength and certainty of evidence underpinning individual recommendations are not formally graded. Future updates of this guide will incorporate a formal evidence-grading framework to enhance evidence-based recommendations for clinicians. Also, the majority of studies informing this CPG evaluate short-term outcomes (typically ≤12 months). Evidence on long-term effectiveness, maintenance, and safety beyond one year is limited. While evidence supports the good acceptability, adherence, and short-term quality-of-life improvements associated with DSNF use, most studies are limited to follow-up periods of three to six months and vary in outcome measures and populations. Long-term acceptability, sustainability, and patient-reported outcomes beyond six months remain less well characterised, highlighting an important area for future research. Heterogeneity in DSNF formulations and varying comparators complicate pooled inference and generalisation. Cost-effectiveness, adherence over time, patient-reported outcomes, and equity considerations are under-reported. Although evidence supporting DSNF use is strongest in T2D, data in other diabetes populations are less extensive, representing an important limitation and an area for future research. A further limitation is that this guide was developed within the Australian healthcare system, where funding models, service delivery structures, and workforce roles may differ from those in other countries. As such, recommendations should be interpreted and adapted within local policy and practice contexts when applied internationally.
4.3. Future Research
Pragmatic, longer-term randomised controlled trials and real-world implementation studies evaluating DSNF-augmented care in individuals facing barriers to wholefood nutrition, compared to standard lifestyle care alone, with ≥12–24 month follow-ups are required. Future research should investigate areas including (1) health economic evaluations and equity analyses across diverse populations and settings, building on existing evidence such as the Transcultural Diabetes Nutrition Algorithm; (2) studies with further clinical outcomes (cardiovascular events, microvascular endpoints), body composition (sarcopenia risk, lean mass preservation with incretin-mimetic medications), and durability of outcomes with long-term use; (3) trials examining personalisation parameters (timing relative to glucose excursions, medication class interaction, protein intake targets in older adults/frailty, cultural dietary patterns); and (4) person-centred endpoints including satisfaction, acceptability, dietary quality, food literacy, and transition strategies to sustainable wholefood patterns. Following the dissemination of this CPG, an evaluation will be undertaken alongside a quality improvement program to assess its effectiveness and usefulness in real-world clinical settings and inform future updates.
5. Conclusions
DSNF are scientifically formulated for the nutritional management of people with or at risk of diabetes. DSNF are an evidence-based nutritional supplement that can be a valuable adjunct to standard dietary and lifestyle interventions, particularly when healthy, wholefood-based approaches are not feasible, or not achieving desired health outcomes. With only one in two people with T2D able to follow dietary recommendations, DSNF may provide an additional option when wholefood approaches are not feasible to improve both nutrition and glycaemic outcomes. This approach helps people with or at risk of diabetes meet their nutritional needs, reduce risk of micronutrient deficiencies, improve glycaemia, weight management and body composition, and reduce the risk of long-term complications, including cardiovascular disease. With the aid of this CPG, health professionals will be equipped to better understand the evidence base supporting the use of DSNF and adopt a tailored evidence-based approach to their use in clinical practice.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Document S1: Use of Diabetes Specific Nutritional Formulas: Clinical Practice Guide - Companion.
Author Contributions
Conceptualisation, Lin, S. and Andrikopoulos, S.; methodology, Lin, S. and Andrikopoulos, S.; writing-original draft preparation, Lin, S. and Andrikopoulos, S.; writing-review and editing, Deed, G., Khoo, C., Murfet, G., Barclay, A., Maberly, G., Blackie, A., and Peng, W.; All authors have read and agreed to the published version of the manuscript.
Funding
The content and recommendations in this guide were developed independently by the expert panel. Abbott Australasia Pty Ltd had no role in the interpretation of evidence or final recommendations. The expert meeting and writing support for the preparation of this manuscript were funded by Abbott Australasia Pty Ltd. The authors did not receive any honorarium from Abbott Australasia Pty Ltd for the development of this manuscript.
Institutional Review Board Statement
Not applicable. This study did not involve human participants, patient data, or identifiable information.
Informed Consent Statement
Not applicable.
Acknowledgments
Facilitation and writing support were provided by FOODiQ Global. Content accuracy and interpretation remain the sole responsibility of the authors. The Clinical Practice Guide was developed by an expert working group comprising representatives from the Australian Diabetes Society (ADS), Australian Diabetes Educators Association (ADEA) and Royal Australian College of General Practitioners (RACGP) and other experts in diabetes care. It builds on the previously published consensus statement1 and aims to equip health professionals with evidence-based guidance to confidently integrate Diabetes Specific Nutrition Formulas (DSNF) into the management of diabetes in clinical practice.This Clinical Practice Guide was written for health professionals who manage people with diabetes or those at risk, including general practitioners, diabetes educators, dietitians, pharmacists, endocrinologists and other primary healthcare team members.
Conflicts of Interest
The authors declare the following interests: SL, SA and GD have received honoraria from Abbott Australasia Pty Ltd for educational presentations unrelated to this Clinical Practice Guide. The remaining authors declare no conflicts of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ADS | Australian Diabetes Society |
| ADEA | Australian Diabetes Educators Association |
| CPG | Clinical Practice Guide |
| DSNF | Diabetes Specific Nutritional Formula |
| GI | Glycaemic index |
| GIP | Glucose-dependent insulinotropic polypeptide |
| GLP-1 RA | Glucagon-like peptide-1 receptor agonist |
| HbA1c | Glycosylated haemoglobin |
| RACGP | Royal Australian College of General Practitioners |
| T2D | Type 2 diabetes |
| MUFAs | Mono-unsaturated fatty acids |
| ONS | Oral Nutrition Supplements |
| PUFAs | Polyunsaturated fatty acids |
| SGLT2 | Sodium-Glucose Transport 2 |
| VLED | Very Low Energy Diets |
References
- Australian Diabetes Society. Australian type 2 diabetes glycaemic management algorithm. Available online: https://www.diabetessociety.com.au/guideline/australian-t2d-glycaemic-management-algorithm-june-2024/ (accessed on 6 January 2025).
- Katsaridis, S.; Grammatikopoulou, M.G.; Gkiouras, K.; et al. Low reported adherence to the 2019 American Diabetes Association Nutrition recommendations among patients with type 2 diabetes mellitus, indicating the need for improved nutrition education and diet care. Nutrients 2020, 12, 3516. [Google Scholar] [CrossRef]
- Lin, S.; Stuk, S.; Jackson, H.; Deed, G.; Ross, G.P.; Andrikopoulos, S. Consensus statement: The use of diabetes specific nutritional formulas in type 2 diabetes. Available online: https://www.diabetessociety.com.au/guideline/consensus-statement-diabetes-specific-nutritional-formulas-in-t2d/ (accessed on 16 January 2024).
- Paudel, G.; Vandelanotte, C.; Dahal, P.K.; et al. Self-care behaviours among people with type 2 diabetes mellitus in South Asia: A systematic review and meta-analysis. J Glob Health 2022, 12, 04056. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Yang, D. Overcoming dietary complexity in type 2 diabetes: influencing factors and coping strategies. Eur J Med Res 2025, 30, 82. [Google Scholar] [CrossRef]
- Mustad, V.A.; Hegazi, R.A.; Hustead, D.S.; et al. Use of a diabetes-specific nutritional shake to replace a daily breakfast and afternoon snack improves glycemic responses assessed by continuous glucose monitoring in people with type 2 diabetes: a randomized clinical pilot study. BMJ Open Diabetes Res Care 2020, 8, e001258. [Google Scholar] [CrossRef] [PubMed]
- Australian Diabetes Clinical Quality Registry, ADCQR 2024 annual report. 2024. Available online: https://www.monash.edu/medicine/sphpm/adcqr/publications (accessed on 6 March 2024).
- Australian Institute of Health and Welfare. Diabetes: Australian facts. Available online: https://www.aihw.gov.au/reports/diabetes/diabetes/contents/treatment-and-management/pathology (accessed on 3 February 2025).
- Mangal, D.K.; Shaikh, N.; Tolani, H.; et al. Burden of micronutrient deficiency among patients with type 2 diabetes: systematic review and meta-analysis. BMJ Nutr Prev Health 2025, 8, e000950. [Google Scholar] [CrossRef] [PubMed]
- Butsch, W.S.; Sulo, S.; Chang, A.T.; et al. Nutritional deficiencies and muscle loss in adults with type 2 diabetes using GLP-1 receptor agonists: A retrospective observational study. Obes Pillars 2025, 15, 100186. [Google Scholar] [CrossRef]
- Kheriji, N.; Boukhalfa, W.; Mahjoub, F.; et al. The role of dietary intake in type 2 diabetes mellitus: importance of macro and micronutrients in glucose homeostasis. Nutrients 2022, 14, 2132. [Google Scholar] [CrossRef]
- Basiri, R.; Seidu, B.; Cheskin, L.J. Key nutrients for optimal blood glucose control and mental health in individuals with diabetes: a review of the evidence. Nutrients 2023, 15, 3929. [Google Scholar] [CrossRef]
- Barazzoni, R.; Sievenpiper, J.L.; Genton, L.; et al. Sarcopenic diabetes is an under-recognized and unmet clinical priority: a call for action from the European Society for Clinical Nutrition and Metabolism and the Diabetes Nutrition Study Group. Clin Nutr 2025, 55, 208–218. [Google Scholar] [CrossRef]
- Chee, W.S.S.; Gilcharan Singh, H.K.; Hamdy, O.; et al. Structured lifestyle intervention based on a trans-cultural diabetes-specific nutrition algorithm (tDNA) in individuals with type 2 diabetes: a randomized controlled trial. BMJ Open Diabetes Res Care 2017, 5, e000384. [Google Scholar] [CrossRef]
- Gulati, S.; Misra, A.; Nanda, K.; et al. Efficacy and tolerance of a diabetes specific formula in patients with type 2 diabetes mellitus: An open label, randomized, crossover study. Diabetes Metab Syndr 2015, 9, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Mottalib, A.; Mohd-Yusof, B.N.; Shehabeldin, M.; Pober, D.M.; Mitri, J.; Hamdy, O. Impact of diabetes-specific nutritional formulas versus oatmeal on postprandial glucose, insulin, GLP-1 and postprandial lipidemia. Nutrients 2016, 8, 443. [Google Scholar] [CrossRef]
- Peng, J.; Lu, J.; Ma, X.; et al. Breakfast replacement with a liquid formula improves glycaemic variability in patients with type 2 diabetes: a randomised clinical trial. Br J Nutr 2019, 121, 560–566. [Google Scholar] [CrossRef]
- Sanz-París, A.; Matía-Martín, P.; Martín-Palmero, Á.; Gómez-Candela, C.; Camprubi Robles, M. Diabetes-specific formulas high in monounsaturated fatty acids and metabolic outcomes in patients with diabetes or hyperglycaemia. A systematic review and meta-analysis. Clin Nutr 2020, 39, 3273–3282. [Google Scholar] [CrossRef]
- Tey, S.L.; Chee, W.S.S.; Deerochanawong, C.; et al. Diabetes-specific formula with standard of care improves glycemic control, body composition, and cardiometabolic risk factors in overweight and obese adults with type 2 diabetes: results from a randomized controlled trial. Front Nutr 2024, 11, 1400580. [Google Scholar] [CrossRef]
- Eyemienbai, E.J.; Logue, D.; McMonagle, G.; Doherty, R.; Ryan, L.; Keaver, L. Enhancing nutrition care in primary healthcare: exploring practices, barriers, and multidisciplinary solutions in Ireland. Int J Environ Res Public Health 2025, 22, 771. [Google Scholar] [CrossRef]
- Noronha, J.C.; Mechanick, J.I. Is there a role for diabetes-specific nutrition formulas as meal replacements in type 2 diabetes? Frontiers in Endocrinology 2022, 13, 874968. [Google Scholar] [CrossRef]
- Tatti, P.; Masselli, L.; di Mauro, P.; Pipicelli, G.; Strollo, F. The use of a nutritional formula with slow release carbohydrates can reduce the frequency and the depth of the hypoglycemic events in subjects with type 1 diabetes mellitus. Med J Nutrition Metab 2011, 4, 141–145. [Google Scholar]
- de Luis Román, D.; Rodas, L.V.; Reyes, L.M.; et al. A prospective, observational study of the use of a high-calorie, high-protein tube feeding formula with slow-release carbohydrates and monounsaturated fatty acids in a malnourished population with diabetes. Clin Nutr Open Sci 2022, 44, 107–117. [Google Scholar] [CrossRef]
- Yu, X.Y.; Zhang, H. Effects of a nutritional liquid supplement designed for diabetes mellitus on postprandial glucose and pregnancy outcomes in patients with gestational diabetes mellitus. Zhonghua Yi Xue Za Zhi 2013, 93, 3450–3453. [Google Scholar]
- Yang, R.; Han, W.; Zheng, W.; et al. Administration of a diabetes-specific formula can improve postprandial glycemic control and delay insulin use in gestational diabetes mellitus: A randomized controlled trial from two centers. Clin Nutr 2024, 43, 265–274. [Google Scholar] [CrossRef]
- Quimby, K.R.; Sobers, N.; George, C.; Greaves, N.; Browman-Jones, F.; Samuels, T.A. Implementation of a community-based low-calorie dietary intervention for the induction of type-2 diabetes and pre-diabetes remission: a feasibility study utilising a type 2 hybrid design. Implement Sci Commun 2021, 2, 95. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO handbook for guideline development, 2nd ed; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- National Institute for Health and Care Excellence. Developing NICE guidelines: The manual. 2025. Available online: https://www.nice.org.uk/process/pmg20 (accessed on 1 June 2024).
- Murphy, M.K.; Black, N.A.; Lamping, D.L.; et al. Consensus development methods, and their use in clinical guideline development. Health Technol Assess 1998, 2, 1–88. [Google Scholar] [CrossRef]
- Fitch, K.; Bernstein, S.J.; Aguilar, M.D.; Burnand, B.; LaCalle, J.R. The RAND/UCLA appropriateness method user's manual; RAND Corporation: Santa Monica, Canada, 2001. [Google Scholar]
- Ojo, O.; Weldon, S.M.; Thompson, T.; Crockett, R.; Wang, X.H. The effect of diabetes-specific enteral nutrition formula on cardiometabolic parameters in patients with type 2 diabetes: A systematic review and meta–analysis of randomised controlled trials. Nutrients 2019, 11, 1905. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Marchetti, A.E.; Apovian, C.; et al. Diabetes-specific nutrition algorithm: a transcultural program to optimize diabetes and prediabetes care. Curr Diab Rep 2012, 12, 180–194. [Google Scholar] [CrossRef] [PubMed]
- Mongkolsucharitkul, P.; Pinsawas, B.; Surawit, A.; et al. Diabetes-specific complete smoothie formulas improve postprandial glycemic response in obese type 2 diabetic individuals: a randomized crossover trial. Nutrients 2024, 16, 395. [Google Scholar] [CrossRef]
- Wang, C.K.; Li, K.X.; Sun, S.Q.; Liu, T.C. The impact of a complete nutrition diabetic formula on glycemic control and nutritional status in hospitalized patients with diabetes mellitus. Front Endocrinol 2025, 16, 1629741. [Google Scholar] [CrossRef] [PubMed]
- Australian Diabetes Society. Australian Obesity Management Algorithm: A simple tool to guide the management of obesity in primary care. 2025. Available online: https://www.diabetessociety.com.au/guideline/obesity (accessed on 30 November 2025).
- Royal Australian College of General Practitioners. Management of type 2 diabetes: A handbook for general practice. Available online: https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/management-of-type-2-diabetes/introduction (accessed on 6 January 2025).
- Steur, M. Very low-energy diets-opportunity for greater weight loss, but risk of bone loss. JAMA Netw Open 2019, 2, e1913752. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin Nutr 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Agarwal, M.; Aggarwal, M.; et al. Nutritional priorities to support GLP-1 therapy for obesity: a joint Advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and The Obesity Society. Am J Clin Nutr 2025, 122, 344–367. [Google Scholar] [CrossRef]
- Noronha, J.C.; Nishi, S.K.; Braunstein, C.R.; et al. The effect of liquid meal replacements on cardiometabolic risk factors in overweight/obese individuals with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabetes Care 2019, 42, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Alish, C.J.; Garvey, W.T.; Maki, K.C.; et al. A diabetes-specific enteral formula improves glycemic variability in patients with type 2 diabetes. Diabetes Technol Ther 2010, 12, 419–425. [Google Scholar] [CrossRef]
- Eckert, I.; Kumbier, M.C.C.; Silva, F.M.; Franzosi, O.S.; de Almeida, J.C. Association of specialized enteral nutrition with glycemic control and clinical outcomes in critically ill patients: A meta-analysis of randomized controlled trials. Clin Nutr 2021, 40, 3940–3949. [Google Scholar] [CrossRef] [PubMed]
- Stenvers, D.J.; Schouten, L.J.; Jurgens, J.; et al. Breakfast replacement with a low-glycaemic response liquid formula in patients with type 2 diabetes: a randomised clinical trial. Br J Nutr 2014, 112, 504–512. [Google Scholar] [CrossRef]
- Thomas, S.; Besecker, B.; Choe, Y.; Christofides, E. Postprandial glycemic response to a high-protein diabetes-specific nutritional shake compared to isocaloric instant oatmeal in people with type 2 diabetes: a randomized, controlled, crossover trial. Front Clin Diabetes Healthc 2024, 5, 1399410. [Google Scholar] [CrossRef] [PubMed]
- Zagury, R.L.; P. Lacativa, P.; de Gregório, L.H.; et al. Randomised clinical trial to evaluate the effect on postprandial glycemia of Nutren Control®, a glycemia-targeted specialized supplement, compared to standardized breakfast in patients with type-2 diabetes: the CONTROL DIABETES study. Nutr Hosp 2023, 40, 41–48. [Google Scholar]
- Trenell, M.; Camprubi Robles, M.; Taylor, L.; et al. A pathway to type 2 diabetes remission: weight reduction and A1C improvements are facilitated by a low-calorie diet including diabetes-specific nutritional formula and the use of digitally enabled reinforcement. Clin Diabetes 2025, 43, 772–780. [Google Scholar] [CrossRef]
- Martin, P.M.; Agudo, F.R.; Medina, J.A.L.; et al. Effectiveness of an oral diabetes-specific supplement on nutritional status, metabolic control, quality or life, and functional status in elderly patients. A multicentre study. Clin Nutr 2019, 38, 1253–1261. [Google Scholar] [CrossRef]
- Sun, J.; Wang, Y.; Chen, X.; et al. An integrated intervention program to control diabetes in overweight Chinese women and men with type 2 diabetes. Asia Pac J Clin Nutr 2008, 17, 514–524. [Google Scholar]
- World Health Organization. Global report on diabetes. Available online: https://www.who.int/publications/i/item/9789241565257 (accessed on 6 January 2025).
- Australian Institute of Health and Welfare. Rural and remote health. Available online: https://www.aihw.gov.au/reports/rural-remote-australians/rural-and-remote-health (accessed on 6 January 2025).
- Australian Institute of Health and Welfare. Diabetes. Available online: https://www.aihw.gov.au/reports/diabetes/diabetes (accessed on 6 January 2025).
- Royal Australian College of General Practitioners. General practice: Health of the nation. Available online: https://www.racgp.org.au/advocacy/health-of-the-nation (accessed on 6 January 2025).
Figure 1.
The 3-step DSNF Clinical Practice Guide. This figure was created by the authors for this study and is original to this publication.
Figure 1.
The 3-step DSNF Clinical Practice Guide. This figure was created by the authors for this study and is original to this publication.
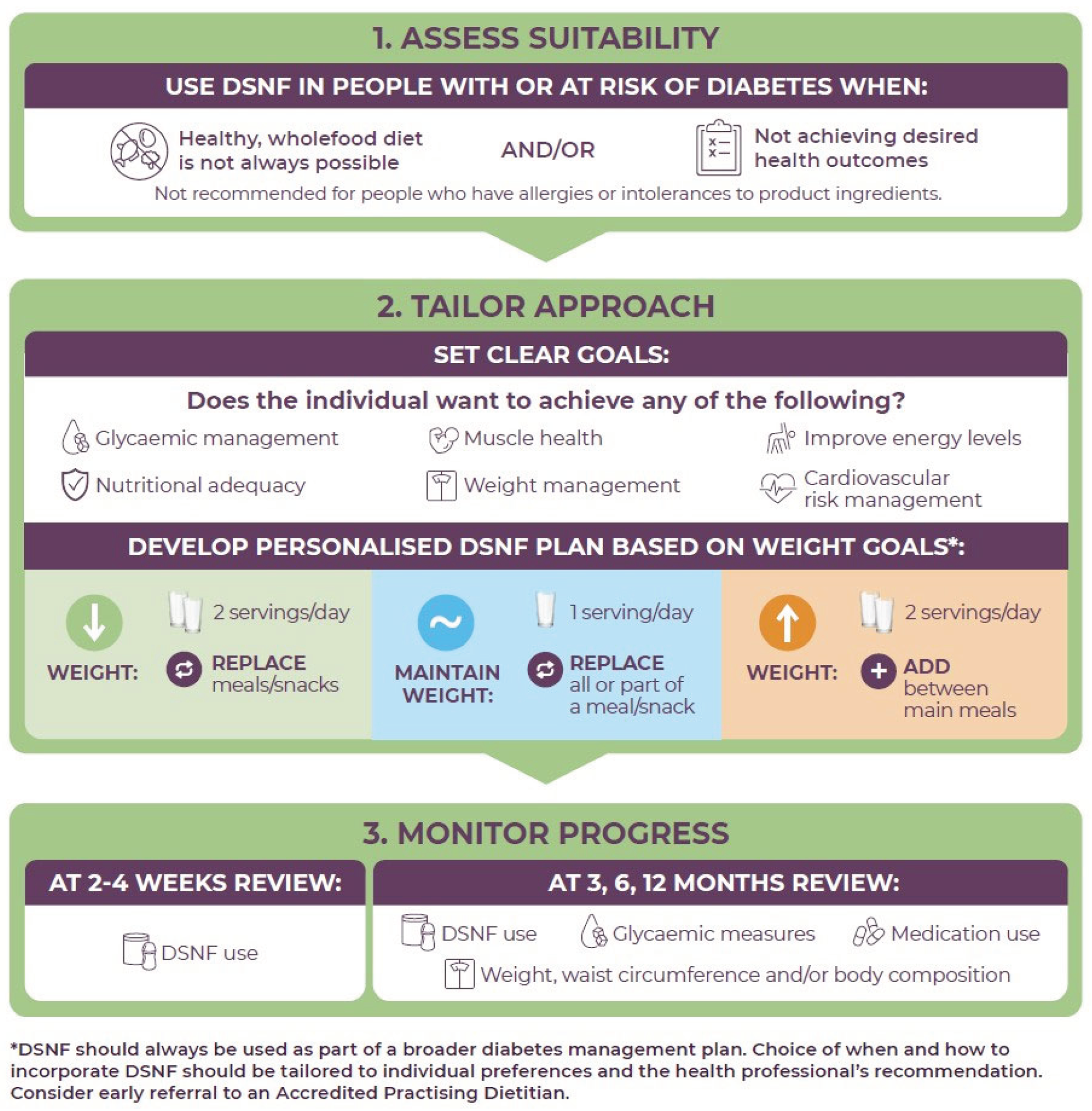

Table 1.
How Diabetes Specific Nutritional Formulas compare to other nutritional formulas available in Australia.
Table 1.
How Diabetes Specific Nutritional Formulas compare to other nutritional formulas available in Australia.
| Diabetes specific nutritional formula (DSNF) |
Very low energy diets (VLED) |
Oral nutrition supplements (ONS) |
Supermarket weight loss shakes | |
|---|---|---|---|---|
| Examplesa | Glucerna | Optifast | Ensure | The Man/Lady Shake Fat Blaster |
| Nutren Diabetes | Optislim | Sustagenb | ||
| Primary clinical goal | Glycaemic management | Rapid weight loss | Nutritional adequacy | Weight management |
| Nutritional adequacy | ||||
| Intended users | People with or at risk of diabetes, irrespective of body weight |
People with BMI ≥30 kg/m2 OR people with T2D BMI ≥27 kg/m2 | People with or at risk of under-nutrition | General population seeking weight loss |
| How to use | Replace a meal/snack or add between main meals as a nutritional supplement depending on needs | Meal replacement (total or partial diet replacement, depending on program) | Add as a nutritional supplement to oral intake |
Self-directed meal replacement |
| To be used under medical supervision | ✔ | ✔ | ✔ | x |
| Nutritionally complete | ✔ | ✔ | ✔ | x |
| Typically found only in pharmacies (or similar) | ✔ | ✔ | ✔ | x Available in supermarkets, with some also sold in pharmacies |
a examples are for illustrative purposes only and data collected in August 2025. b Sustagen is a brand with multiple formulations. Sustagen Optimum is classified as a Food for Special Medical Purposes and must be used under medical supervision. Other formulations, such as Sustagen Hospital Formula or supermarket versions, are considered supplementary foods and do not require medical supervision.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



