
Submitted:
18 January 2026
Posted:
20 January 2026
You are already at the latest version
Abstract
National Institute for Health and Care Excellence (NICE) and National Clinical Guideline for Stroke 2023 (NCGFS23) guidelines recommend specialist TIA clinic assessment within 24 hours of symptom onset of suspected TIA. There is limited evaluation of TIA clinic services in the United Kingdom (UK) and Republic of Ireland (ROI). This study aims to assess attendee characteristics, NICE/NCGFS23 adherence, and clinical outcomes across the UK and ROI.DelAys in TIA Evaluation and Service (DATES) is a prospective national audit and service evaluation delivered through an established collaborative (The Neurology and Neurosurgery Interest Group (NANSIG)). All UK and ROI outpatient rapid-access TIA clinics are eligible. All index suspected TIA presentations will be included, irrespective of final diagnosis. Centres will register as an audit/service evaluation without altering routine practice. Data will be collected electronically, with blinded independent validation. The primary outcome is adherence to the NICE/NCGFS23 recommended 24-hour target. Secondary outcomes include presenting symptoms, diagnosis, investigations, treatment, and onward referral.DATES is anticipated to be the largest prospective study presenting in-depth evaluation of UK/ROI TIA clinic attendances. Our results will provide real-world data on TIA pathways and potentially improve existing services.
Keywords:
transient ischaemic attack
; service evaluation
; diagnosis
; investigation
; TIA
; stroke
1. Introduction
1.1. Background and Rationale
Transient ischaemic attacks (TIA) occur due to transient interruption in blood flow to the brain and are an important risk factor for future stroke. Stroke represents a leading cause of mortality and morbidity globally, exerting a significant burden on healthcare systems worldwide, and its incidence continues to rise [1]. Delays in assessment and intervention for TIAs influence subsequent stroke risk [2,3].
Current NICE guidelines [4] and National Clinical Guideline for Stroke 2023 (NCGFS23) [5] outline recommendations regarding the initial management of suspected TIA namely 1) offer 300mg aspirin (unless contraindicated) to start immediately; and 2) immediate referral for specialist assessment and investigation, to be seen within 24 hours of symptom onset. A caveat from NCGFS23 lists if the TIA occurred more than a week previously, then individuals should be seen as soon as possible within 7 days.
NICE and NCGFS23 outline recommendations at/after attendance at TIA clinic, namely: 1) consider MRI brain 2) everyone with a TIA who is a candidate for carotid endarterectomy should have urgent carotid imaging and 3) offer secondary prevention (in addition to antiplatelet therapy where appropriate) as soon as possible after the diagnosis of TIA is confirmed. NICE guidelines add that if an MRI is done, it should be performed on the same day as the assessment.
To date, TIA clinic attendances have not been subject to in-depth evaluation at the national level. The Sentinel Stroke National Audit Programme [6] is a longitudinal population study across 182 acute centres in the UK focusing on the quality of stroke care and related outcomes; however, it has limited coverage of TIA clinic services.
DelAys in TIA Evaluation and Service (DATES) proposes a prospective audit and service evaluation study with in-depth review of TIA clinic attendances in the UK and ROI, capturing all attendees regardless of a definitive TIA diagnosis. This study would provide evidence for local and national adherence to existing guidelines, and improve our understanding of attendee characteristics, including TIA prevalence. We aim to evaluate the utilisation of TIA clinics, characteristics of attendees and adherence to NICE and NCGFS23 guidelines, clinic outcomes, nationally.
1.2. Objectives
1.2.1. Primary objectives
To assess adherence to the NICE guideline NG128 recommendations in the UK, relating to the
1) Initial management of suspected and confirmed TIA (1.1.4 - 1.1.7) and
2) Imaging for people who have had a suspected TIA (1.2)
To assess adherence to the National Clinical Guideline for Stroke 2023 (NCGFS23) recommendations in the UK and Ireland, relating to the
1) Initial management of suspected and confirmed TIA (NCGFS 3.2 A-G) and
2) Management of TIA and minor stroke - treatment and vascular prevention (NCGFS 3.3 A-K)

Table 1.
NICE guideline NG128 (accessed August 2023) [4].
Table 1.
NICE guideline NG128 (accessed August 2023) [4].
| Stroke and transient ischaemic attack in over 16s: diagnosis and initial management |
|
1.1.4 Offer aspirin (300 mg daily), unless contraindicated, to people who have had a suspected TIA, to be started immediately. 1.1.5 Refer immediately people who have had a suspected TIA for specialist assessment and investigation, to be seen within 24 hours of onset of symptoms. [2019] 1.1.6 Do not use scoring systems, such as ABCD2, to assess risk of subsequent stroke or to inform urgency of referral for people who have had a suspected or confirmed TIA. [2019] 1.1.7 Offer secondary prevention, in addition to aspirin, as soon as possible after the diagnosis of TIA is confirmed. [2008, amended 2019] 1.2.1 Do not offer CT brain scanning to people with a suspected TIA unless there is clinical suspicion of an alternative diagnosis that CT could detect. [2019] 1.2.2 After specialist assessment in the TIA clinic, consider MRI (including diffusion-weighted and blood-sensitive sequences) to determine the territory of ischaemia, or to detect haemorrhage or alternative pathologies. If MRI is done, perform it on the same day as the assessment. [2019] 1.2.3 Everyone with TIA who after specialist assessment is considered as a candidate for carotid endarterectomy should have urgent carotid imaging. [2008, amended 2019] 1.2.4 Ensure that people with stable neurological symptoms from acute non-disabling stroke or TIA who have symptomatic carotid stenosis of 50% to 99% according to the NASCET (North American Symptomatic Carotid Endarterectomy Trial) criteria, or 70% to 99% according to the ECST (European Carotid Surgery Trial) criteria:
|
Table 2.
National Clinical Guideline for Stroke 2023.
| 3.2 Management of TIA and minor stroke - assessment and diagnosis (accessed December 2023) [5] |
|
1.2.2. Secondary Objectives
Symptoms: To characterise the presenting symptoms of the index episode leading to referral to TIA clinic.
Referral: To describe the pathway to attendance at TIA clinic. This includes the care setting and date of the index presentation [such as GP, pharmacy or emergency department], initial investigations, changes to medication, health care provider referring to TIA clinic, details of local referral criteria/ templates/pathway, as well as date and time of TIA clinic.
Baseline characteristics: To characterise attendee demographics and cerebrovascular risk factors (as informed by past medical history, physiological risk factors for clotting or bleeding for clotting or bleeding, and medications).
Investigations performed: To characterise additional investigations such as:
- Blood pressure in clinic
- Blood tests [including full blood count, urea and electrolytes, liver function tests, clotting screen, lipids, HbA1c, C-reactive protein, erythrocyte sedimentation rate, thyroid screen,]
- Electrocardiography [12 lead or continuous ambulatory ECG]
- Echocardiography
TIA clinic assessment: To describe the care and management initiated at the TIA clinic. This encompasses proposed diagnosis (neurovascular vs non-neurovascular), and subsequent secondary prevention including antiplatelet use/anticoagulation, lifestyle advice and driving advice.
Post-TIA clinic care: To describe care and management arranged following TIA clinic attendance, including further referrals for risk factor optimisation or investigation/management of non-TIA diagnosis.
Antiplatelet prescribing: To categorise different antiplatelet prescribing regimes, noting variation within or across trusts and deviations from the proposed regime outlined by the NGFS23 (see Table 2).
TIA clinic follow up: To describe existing follow up after diagnosis of TIA and associated variation.
Associations:
- To explore association of individual and centre-level variables with delays in care (including adherence to guideline target of clinic review within 24 hours).
- To identify variables associated with TIA versus non-TIA diagnosis at TIA clinic.
- To explore the association of socioeconomic deprivation with aspects of care.
Table 3.
National Clinical Guideline for Stroke for the United Kingdom and Ireland:.
| Management of TIA and minor stroke – treatment and vascular prevention [5] |
|
1.3. Standard Diagnostic Service and Relevant Audit Standards
In preparation of this protocol, we reviewed the following guidelines / documents:
- Clinical Knowledge Summary: Stroke and TIA (Last revised in April 2023) [7].
- National Clinical Guideline for Stroke for the United Kingdom and Ireland (Accessed August 2023) [5].
- NICE guideline NG128 (accessed August 2023) Stroke and transient ischaemic attack in over 16s: diagnosis and initial management [4].
- NICE scenario: Secondary prevention following stroke and TIA[8].
- The American Heart Association (AHA)/American Stroke Association (ASA) guidelines: Adult stroke rehabilitation and recovery [9].
- Guideline for the prevention of stroke in patients with stroke and transient ischemic attack [10].
- Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke [11].
- the BMJ Best Practice guidelines Transient ischaemic attack [14].
- NICE guideline NG196 Atrial fibrillation: diagnosis and management [15].
2. Methods
2.1. Study Design
DATES is a prospective, observational, multicentre audit and service evaluation study of TIA clinic attendances in the UK and Republic of Ireland. This study reviews the presentation and management of attendees, regardless of their diagnosis (TIA versus other diagnosis) and assesses adherence to national stroke guidelines (NCGFS23 [5] and NICE [4]). Included individuals will be identified prospectively, with collection of data from preexisting clinical records by trained Collaborators. The study is led by NANSIG [16], a medical student and junior doctor-led collaborative, and supported by their existing university and hospital-affiliated collaborator networks. This network builds on NANSIG’s previous work in neurology, including in areas of epilepsy (NAPIER [17], BECTs [18]) and multiple sclerosis (DIMES [19]).
2.2. Centre Eligibility Criteria
All centres/hospital trusts in the UK or ROI that provide a rapid-access TIA clinic service are eligible. For the purposes of this study, we define a TIA clinic as an outpatient, rapid-access service dedicated to referrals for suspected TIA. In the absence of a listed definition in national guidelines we suggest a TIA clinic is an outpatient clinic with the purpose of assessing individuals with suspected TIA, usually (though not always) run by stroke or other specialist clinicians. Rapid-access meaning an urgent first-contact assessment, known in some countries as “hot” clinics.
Based on the existing NANSIG regional lead network of university students we expect that DATES will enrol many teaching hospitals. In order to achieve more comprehensive coverage, we will contact NHS hospital trusts that currently or have previously worked with the SSNAP audit to make them aware of the study and potential for participation.
2.3. Patient Eligibility Criteria & Inclusion + Exclusion Criteria
2.3.1. Inclusion Criteria
Centres will identify eligible individuals using TIA clinic appointment lists during a prospectively declared 4-week, Monday to Sunday, period that they can self-select after securing the necessary local approvals and registrations.
All attendees will be included, regardless of whether TIA or other conditions were diagnosed. We will include individuals irrespective of investigations or treatments received; the completeness/accessibility of their clinical information; whether or not they have been seen by the emergency department or stroke team previously, or whether they attended the clinic appointment. A limited subset of data will be collected for individuals who did not attend their TIA clinic appointment.
2.3.2. Exclusion Criteria
Individuals listed in the National Data Opt Out in NHS England will be excluded.
Individuals with an initial TIA clinic appointment prior to the patient eligibility period would be excluded (even if they have (follow up) appointments during the eligibility period).
Individuals who were seen as part of an emergency department or inpatient admission without review in TIA clinic will be excluded.
2.4. Patient Identification
Local teams will work with a Supervising Consultant at participating centres to identify all individuals meeting inclusion criteria. This will most likely involve searching TIA clinic appointment lists and identifying individuals with first appointments within the period specified.
2.5. Recorded Variables
2.5.1. Centre-Level Variables
This will characterise each centre’s local practice regarding TIA clinics. We anticipate there to be variation between centres in terms of clinic frequency, investigations and follow up with potential implications for waiting times and patient outcomes.
Centre-focused variables include: local referral and triage criteria sent to Steering Committee; use of ABCD2 criteria to triage patients; referral to TIA clinic method; most common professional grade of clinicians delivering TIA clinic; number of consultants forming the TIA clinic team; frequency of TIA clinic; investigation timing; occupation of individual performing carotid ultrasound; ultrasound training among consultants; time and mode for follow up of confirmed TIA; mode of follow up regarding results for individuals with likely non-neurovascular aetiology of symptoms.
2.5.2. Demographic Variables
In order to ascertain the impact of socioeconomic deprivation on TIA clinic attendances, we will calculate the index of multiple deprivation decile and ranks for UK residents and the Pobal deprivation index decile and ranks for ROI residents. We will collect the distance from the individual’s postcode to the clinic in miles, without storing postcode information at any stage.
Demographic variables include: age; sex; ethnicity; index of multiple deprivation decile and rank (UK); Pobal deprivation index decile and rank (ROI); distance to clinic (postcode of residence to clinic distance, miles); distance to the sea (miles); employment status; driving status
2.5.3. Variables Selected from Risk Scores
We intend to calculate the following risk scores. Below are each of the variables to calculate each respective score, and these have been incorporated into our data dictionary.
- ABCD2: Age >60; BP >140/90; unilateral weakness; speech disturbance without weakness; duration of symptoms; history of diabetes
- ATRIA bleeding score: Anaemia; severe renal disease (dialysis dependency/ eGFR <30); age >75; prior haemorrhage diagnosis; previous stroke history
- ATRIA stroke score: Age; sex; history of diabetes mellitus; CHF history; hypertension history; proteinuria; end stage renal disease/ eGFR<45
- CHADS2: CHF history; hypertension history; age >75; diabetes mellitus history; previous stroke/TIA history;
- CHA2DS2 VASC: Age (65-74/>75); sex; CHF history; hypertension history; previous stroke/TIA/ thromboembolism history; history of vascular disease (MI, PAD, aortic plaque); diabetes history
- DOAC score: Age; BMI <18.5; creatinine clearance/ eGFR; stroke/TIA/systemic embolism history; diabetes; antiplatelet use (aspirin/ dual antiplatelet); nonsteroidal anti-inflammatory use; bleeding history; liver disease; hypertension
- HAS-BLED: Hypertension; renal disease (dialysis/ kidney transplant / Cr >2.26 mg/dL or >200 µmol/L); liver disease (known liver cirrhosis/ bilirubin >2x above normal and AST/ALT/AP >3x above normal); previous stroke history; prior major bleeding or predisposition to bleeding; labile INR; age >65; medication predisposing to bleeding; alcohol history (>8 drinks/week)
- HEMORR2HAGES: Hepatic or renal disease; ethanol abuse; age (>75); aspirin use or reduced platelet count/ function; past bleeding/ rebleeding risk; anaemia; genetic factors (CYP 2C9 single nucleotide polymorphisms); excessive falls risk (by chart review for “high risk of falling, dementia, Parkinson’s disease, or psychiatric disease”); previous stroke history
- ORBIT: Sex; age >74; bleeding history (GI/ intracranial/ haemorrhagic stroke); eGFR <60; antiplatelet use
- QRisk3: Age; sex; ethnicity; height; weight; BMI; smoking status; hypertension; diabetic status; lupus/rheumatoid arthritis; migraine including cluster headache; AF history; history of heart failure; severe mental illness; family history of angina/myocardial infarction in first degree relative; atypical antipsychotic use; corticosteroid use; creatinine; cholesterol/HDL ratio; systolic BP
- QStroke: Age; sex; ethnicity; height; weight; BMI; smoking status; hypertension; diabetic status; lupus/rheumatoid arthritis; AF history; previous angina/ myocardial infarction; history of heart failure; history of valvular heart disease, severe mental illness; family history of angina/myocardial infarction in first degree relative; creatinine; cholesterol/HDL ratio; systolic BP
- ROSIER: Loss of consciousness/syncope; seizure activity; asymmetric facial weakness; unilateral arm/leg weakness; speech disturbance; visual field defect
2.5.4. Variables Extracted from NICE and National Stroke Guidelines
As an audit and service evaluation study, we aim to assess adherence to NICE guidelines in the UK, and NCGFS23 in the UK and ROI. Listed here are all the points which we measure adherence to, within our collected variables.
Variables extracted from NICE NG128 include: Aspirin 300mg upon initial presentation; A&E presentation warrants use of validated screening tool; seen in TIA clinic within 24 hours; not using scoring systems (ABCD2) to aid triage; MRI if conducted being conducted same day; only offering CT if alternate pathology suspected; anyone considered a candidate for carotid endarterectomy should have urgent carotid imaging; secondary prevention (in addition to aspirin) as soon as diagnosis is confirmed; carotid endarterectomy performed if NASCET 50-99% or ESCT 70-99%; best medical care for carotid endarterectomy candidates and non-candidates
Variables extracted from the NCGFS23 add: If TIA occurs >7 days prior patients should be seen by a stroke specialist clinician within 7 days; proton pump inhibitor co-prescription with dual antiplatelet therapy; high intensity statin therapy; antiplatelet therapy provided no contraindication; blood pressure lowering therapy; carotid imaging within 24 hours for all patients considered candidates
2.5.5. All Variables
Medical history risk factors prior to attendance variables: Height; weight; BMI; smoking status; e-cigarette use; cocaine or illicit opioid or cannabis use; hypertension; diabetic status; diabetic status; pre-clinic HBA1c reading; history of liver disease; history of renal disease; history of lupus/rheumatoid arthritis; migraine history including cluster headaches; history of malignancy; previous stroke history; previous TIA history; AF history; previous venous thromboembolism; bleeding history; history of genetic factors related to clotting or bleeding; history of angina/ myocardial infarction; history of peripheral vascular disease or aortic plaque; history of congestive heart failure; history of valvular heart disease; alcohol excess; previous severe mental illness; falls risk status; family history of stroke/TIA; family history of angina or heart attack in first degree relative
Medication use prior to clinic variables: Antiplatelet use; anticoagulant use; NSAID use; atypical antipsychotic use; corticosteroid tablet use; combined oral contraceptive pill use; hormonal replacement therapy use; regular opioid prescription
Physiological risk factors at time of clinic variables: Haemoglobin; platelets; creatinine; 12 month lowest creatinine; unstable/high INR; hypercholesterolaemia/ hyperlipidaemia; LDL level; cholesterol/HDL ratio.
TIA symptom and features variables: Onset time/date; sudden onset; maximum neurological deficit at onset; duration of symptoms; vascular territory; monocular/binocular visual defect; diplopia; positive visual phenomenon; visual hallucination; other visual disturbance; dysarthria; dysphasia/aphasia; vertigo; coordination; loss of consciousness; dysphagia; unilateral/bilateral motor deficit; facial motor deficit; face pattern of motor deficit; upper limb motor deficit; lower limb motor deficit; distal/proximal motor deficit pattern; unilateral/bilateral sensory symptoms ; facial sensory symptoms ; upper limb sensory symptoms ; lower limb sensory symptoms ; headache; aura; seizure; post-ictal phase; incontinence; confusion; amnesia; co-occurring with intoxication; co-presenting with fall or collapse; recurrence of symptoms with/without complete resolution before TIA clinic presentation
Initial presentation of TIA variables: Location of initial presentation; time and date of initial presentation; ABCD2 score; ROSIER score; aspirin prescription; referral to service other than TIA clinic; service referring to TIA clinic; date and time of referral to TIA clinic; purpose of referral; referral method to TIA clinic
TIA clinic contents variables: TIA clinic location; clinician grade; clinician speciality; clinic time and date; attendance; reason for non-attendance; non-attendance due to hospital admission; previous non-attendance; clinic TIA diagnosis; non-TIA diagnosis; other diagnosis; diagnostic uncertainty remaining at data entry date; blood pressure measurement; systolic blood pressure; lifestyle advice given; smoking cessation advice given; driving advice given; informed of yearly influenza vaccination
Prescribing variables: Anticoagulation prescription; PPI prescription; statin prescription; antihypertensive prescription before/after clinic
Investigation variables: HBA1c; FBC; renal function; LFTs; coagulation; lipid screen; CRP; ESR; TSH or T3/4; young stroke screen; sleep apnea screening; EEG; other investigations;
Imaging variables: Carotid imaging requested; US doppler request and date performed; CT angiogram request and date performed; MR angiogram request and date performed; degree of stenosis on carotid imaging; carotid ECST/NASCET value; MRI head request date, date performed, date of report; MRI head sequences; MRI findings (bleed, cerebral small vessel disease, infarction/ischaemia, free text); CT scan performed, date performed and indication
AF investigations: Irregular pulse; ECG [12 lead, ambulatory, 24 hour] request date/ date performed; echocardiogram (request date/ date performed); AF diagnosis; clotting risk calculated; bleeding risk calculated.
Further referral variables: Further referral after TIA clinic; clinic outcome
2.6. Outcomes
The primary outcomes relate to adherence to the NG128 and NCGFS23 recommendations and include: 1) the initial antiplatelet prescription after suspected TIA; 2) the time from symptom onset and referral to TIA clinic to attendance, and proportion of referrals seen within 24 hours; and 3) the proportion of suspected TIA patients who have CT , MR, or US Doppler imaging of the brain and/or carotid arteries.
Secondary outcomes relating to the diagnostic journey include: 1) presenting symptoms leading to index event; care setting of the index presentation; 2) baseline characteristics; 3) healthcare provider referring to TIA clinic; 4) initial investigations prior to clinic attendance.
Secondary outcomes relating to TIA clinic assessment include: 1) proportion with consensus/probable TIA diagnosis after specialist review (PPV of referral); 2) non-attendance rate; 3) arranged investigations; and 4) onward referrals from TIA clinic. TIA clinic diagnosis will list proportions in each of the following categories: a) Consensus/confirmed/definite/unspecified TIA; b) Likely/probable TIA; c) Unlikely/Possible TIA; d) Non-TIA diagnosis or Not TIA; e) Stroke (not TIA); and f) Not documented.
3. Study Data and Analysis
The 3.1 Team Structure, 3.2 Data Collection and 3.3 Data Validation and Quality Assurance sections of this protocol follow a similar structure to NANSIGs previous neurology study, DIMES - DelAys In MultiplE Sclerosis management in the UK and ROI [19].
3.1. Team Structure
Each centre will have a base team structure of a Supervising Consultant, a Centre Lead, and a suggested maximum of 10 Collaborators. One of the Collaborators, or the Centre Lead, is expected to abstain from data collection in order to act as a Data Validator as per 3.3 Data Validation and Quality Assurance. For in-depth descriptions of each role, and authorship requirements, please see 5.2 Authorship Eligibility.
3.2. Data Collection
The Centre Lead will first identify all eligible individuals under the guidance of the Supervising Consultant, noting each individual’s hospital number and allocating them a centre number (e.g. patient 1, patient 2, etc.). This will later be used for traceability and avoiding duplication, data quality assurance, compliance with NHS England’s Check for National Data Opt-Out, and the opportunity for a follow up substudy. This should be stored on the hospital/trusts password-protected server.
At the end of the 4-week patient eligibility period, Centre Leads will provide their audit or information governance department with a list of individuals for checking against the NHS England’s Check for National Data Opt-Out Service. Those who have opted-out will be listed under this exclusion reason.
The Centre Lead +/- any additional Collaborators will extract information from available records, as described in 3.4 Information Sources. This will be anonymised and each individual will only be referred to by their centre number. All collected, non-identifiable data will be entered into a standardised Microsoft Excel spreadsheet stored on password-protected NHS computers.
Upon data collection and post-quality assurance completion, the Centre Lead will send the anonymised Excel sheet to our secure study-specific NHS email address at Barts Health NHS Trust. To ensure encryption and confidentiality, it must be sent from an @nhs (or local equivalent) email.
3.3. Data Validation & Quality Assurance
3.3.1. Design
This protocol was developed with input from a diverse multi-speciality expert advisory group and informed by approaches from NANSIG’s most recent neurology project [19].
3.3.2. Training
Prior to beginning any data collection, all Centre Leads and Collaborators will attend a centralised induction session delivered by the DATES Steering Committee. It aims to give Collaborators a broad understanding of TIA, the purposes of TIA clinics and risk of stroke after TIA. It will also explain the data collection process, ensure a clear understanding of the principles of data governance, and allow for any questions. We encourage Centre Leads to host regular meetings with Collaborators, providing ample opportunity for Collaborators to raise issues and ensure smooth data collection.
3.3.3. Data Completeness
Post data collection only datasets >95% completeness will be considered for inclusion in central analysis. In this study, data completeness is defined as the proportion of Excel spreadsheet cells containing appropriate entries, including “not reported/not documented.” To emphasise the significance of data completeness to Collaborators, centres with >5% missing data points (excluding “not reported/not documented”) will not be included in the study. Collaborators whose centres do not contribute any individuals to the study would be withdrawn from the published list of citable Collaborators. The term ‘missing data’ specifically indicates either incomplete data field entries or a lack of explanation for not completing the data field. After Excel spreadsheet submission, the Steering Committee will review the submitted spreadsheet for any omissions or potential issues. These concerns will be highlighted, and the spreadsheets will be sent back to centre teams for resolution by the local participating team.
3.3.4. Data Accuracy
Each centre will conduct additional data validation, using inter-Collaborator agreement as a marker for data accuracy. This will be conducted by an independent Data Validator who was not involved in previous data collection, who can be a previously agreed Centre Lead or Collaborator. Not every data variable will undergo this validation assessment. Prior to review of submitted data, approximately 50 variables will be selected based on the Steering Committee’s opinion on their salience to our study objectives.
The Steering Committee will randomly select 10% of the centre’s cases for validation using Microsoft Excel random number generator. The Data Validator will perform data extraction for these cases blinded to existing data entries. After return by the Centre Lead to the Steering Committee, initial and Data Validator entries will be compared to assess inter-Collaborator agreement with a target of ≥90%. If inter-Collaborator agreement is below, a further 10% of the centre’s cases will be randomly selected and assigned to the Data Validator for repetition of the above process. If inter-Collaborator agreement remains below 90% the Centre Lead will review all data extraction for all cases and their data may be analysed and/or presented separately.
We do not intend to reconcile conflicts between the initial and Data Validator entries as the primary purpose of this assessment data accuracy is to determine an estimate of variable-level accuracy for the dataset.
3.4. Data Dictionary
See appendix for data dictionary.
3.5. Information Sources
Collaborators will be expected to identify and review all of the listed information sources, where available, to enable standardised and appropriately comprehensive data extraction.
TIA clinic appointment list -
Definition: Comprehensive list of all scheduled appointments at TIA clinic with associated dates, appointment times and patient details.
TIA referral -
Definition: This is a document relating to the request or referral for the individual to be seen in a TIA clinic. Depending on local practices this may be a standard template, unstandardised email/letter correspondence or electronic request.
TIA episode reviews -
Definition: All available correspondence relating to the index suspected TIA episode which may be listed in related documentation of clinical review of the referrer. Examples include documentation from the emergency department documentation, ambulance services, hospital speciality, general practice or other teams.
TIA clinic letter-
Definition: This is any appointment documentation relating to this index referral. This letter would be expected to relate to a clinic within the study dates; however, based on local practice, it may not be available on systems until some time after.
Reviews after TIA clinic -
Definition: This includes any reviews by clinical teams that are visible to the hospital electronic system such as further reviews in TIA/stroke team clinics, presentation to the emergency department, or hospital admissions.
Hospital EPR record - (electronic patient record)
Definition: This refers to the digital system that contains up-to-date health information regarding individuals such as demographics, relevant clinic notes, clerkings, and diagnostics tests, along with current management record and discharge summaries.
Prescription record -
Definition: A locally used, reliable source for a patient’s current and historical prescription record.
Radiology record -
Definition: The locally used system(s) listing requests, request dates, imaging and reports of radiological investigations of interest (CT head / MRI brain / Ultrasound Carotids).
Cardiac investigations record -
Definition: The locally used system(s) listing requests and results of cardiac investigations which may include: 12-lead ECGs, ambulatory ECGs, loop records, echocardiograms.
Blood result record -
Definition: The locally used system(s) to access results for investigations including blood tests.
We do not expect Data Collectors to review/access General Practice records for further information if this is not accessible via local hospital electronic systems.
3.6. Centre Practice
See Centre Survey section of the Data Dictionary (appendix 1.)
3.7. Sample Size
Enrolled centres are expected to include all eligible individuals. While the aim is to enrol all eligible centres, this is not likely to be comprehensive (i.e. 100% of all eligible centres) and is not random, and as such the population represents a convenience sample. We have not performed a formal sample size calculation as our primary objectives do not have minimum effect sizes of interest.
To inform the feasibility and appropriateness of suggested analyses we have instead estimated a potential target sample size for the study, informed by 1) national estimates of TIA incidence and 2) SSNAP audit data on clinic attendances.
3.7.1. National Estimates of TIA Incidence
-
The annual incidence of first-ever TIA is estimated to be:
- Suggests a monthly estimate of 3833 / month as per the most recent data for the UK.
- There are approximately 205 centres delivering acute stroke care in the United Kingdom [22].
From our existing regional lead network across 39 UK/ROI medical schools we expect to enrol a minimum of 39 centres. In addition, through the engagement of our regional representatives (working as doctors), and UK/ROI stroke services we anticipate enrolling a further 10 centres (Target number of centres = 49 centres).
If 49 centres are included, this represents 24% (49/205) of UK centres delivering acute stroke care.
Assuming equal caseloads across centres, approximately 920 individuals would have a TIA (24% of 3833 patients). Assuming 62% managed as outpatient [23], 570 individuals with TIA (62% of 920) would be seen in TIA clinic. Assuming an equivalent number of individuals with a non-TIA diagnosis attend clinic, 570 individuals with non-TIA diagnosis would be seen in TIA clinic.
During the 4-week patient eligibility period, this yields a sample of 1140 individuals (mean = 23 individuals per centre).
3.7.2. SSNAP Audit Data on Clinic Attendances
In the 2021 SSNAP audit [6], involving 183 hospitals and 157 NHS trusts, 151 NHS trusts had a rapid-access TIA clinic (also known as a neurovascular clinic). During their four week period, 10656 patients were seen in clinic, of which 4609 patients had a “final diagnosis of TIA.”
This would be consistent with:
- A mean of 71 (10656/151) individuals attending clinic per NHS trust per month [58 (44-89.5), Median (IQR)].
- A mean of 31(4609/151) individuals attending clinic with “final diagnosis of TIA” per NHS trust per month.
If 49 centres are included this represents 27% (49/183) of UK centres delivering acute stroke care.
Assuming equal caseloads across centres, approximately 2877 individuals would attend TIA clinic (27% of 10656 patients), of which 1244 (27% of 4609) have a TIA. During the 4-week patient eligibility period, this yields a sample of 2877 individuals (mean = 58 individuals per centre).
3.8. Statistical Analysis
3.8.1. Descriptive Statistics
Continuous data will be summarised as mean (with standard deviation) or median (with interquartile ranges) based on visual and statistical evaluation for normality, with testing using appropriate parametric or non-parametric tests. Categorical data will be cross-tabulated, and differences in proportions will be tested using χ2 and Fisher’s exact tests, as required. Missing data will be included in flowcharts and descriptive analyses, allowing denominators to remain consistent in calculations.
Tables will present demographic and clinical characteristics, alongside adherence to audit/quality standards expressed as percentages. Notable proportions will be reported:
-
Proportions with each of the diagnostic categories:
- (1)
- Consensus/confirmed/definite/unspecified TIA;
- (2)
- Likely/probable TIA;
- (3)
- Unlikely/Possible TIA;
- (4)
- Non-TIA diagnosis or Not TIA;
- (5)
- Stroke (not TIA); and
- (6)
- Not documented.
-
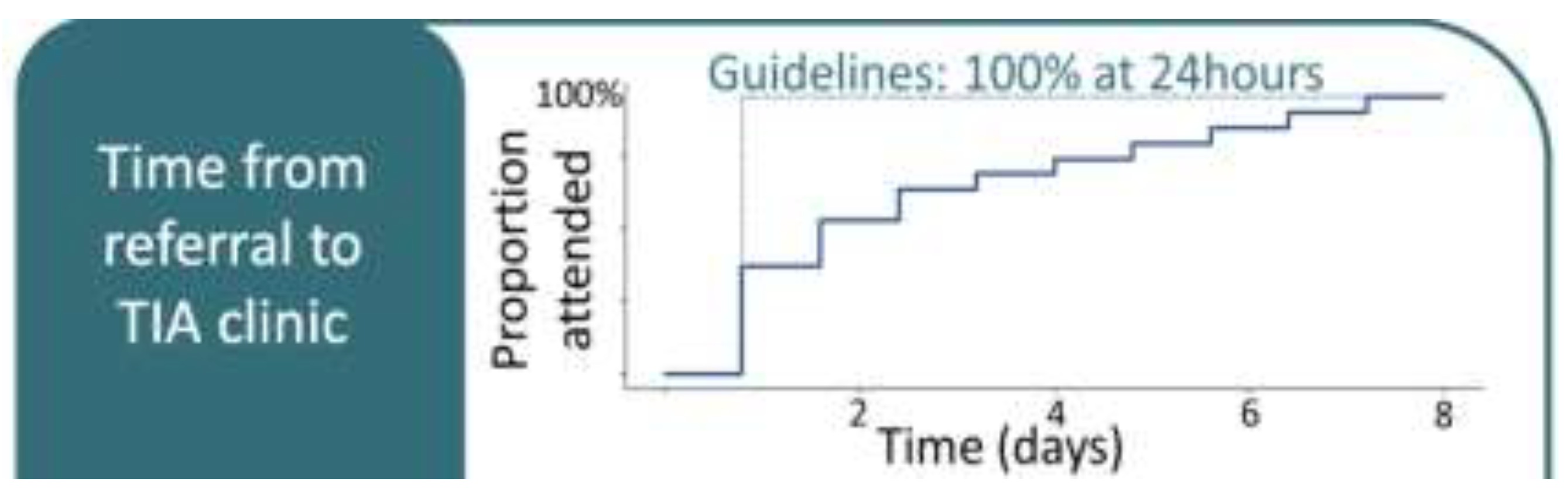
Proportions with each non-TIA diagnosisData visualisation, including survival plots, will illustrate:
- Proportion of individuals seen within 24 hours of symptom onset to TIA clinic, as per both NICE clinical guideline NG128 and NCGFS23, demonstrated in survival plots.
Figure 1.
Example graph depicting one of our predicted outcomes.
3.8.2. Primary Analysis
We intend to explore variables associated with the primary outcome, adherence to clinic review within 24 hours, using multivariable regression models selecting from variables from centre-level and individual-level data.
For certain analyses we will stratify clinic diagnosis into two groups: TIA versus non-TIA. TIA diagnosis will only include those with diagnostic group 1) Consensus/confirmed/definite/unspecified TIA; or 2) Likely/probable TIA.
Using multivariable logistic regression, we intend to explore the association of variables with a diagnosis of TIA (versus non-TIA). Suggested variables include patient demographics (age, sex, ethnicity, deprivation), symptoms, comorbidities, diagnosing clinician group (stroke / neurology / other) and grade, and ROSIER score. ROSIER score will be calculated from individual data points included in the data dictionary in relation to the index episode.
3.8.3. Sensitivity Analysis
For above analyses where individuals are stratified into TIA versus non-TIA groups we will perform sensitivity analyses with reclassification with a more stringent TIA definition using diagnostic category 1) only (Consensus/confirmed/definite/unspecified TIA), and less stringent, with inclusion of category 3) (Unlikely/Possible TIA). Differences between the sensitivity analysis groups and primary analysis will be examined to understand the classification’s effect.
3.8.4. Secondary Analyses
We will assess for association of socioeconomic deprivation and ethnicity with outcomes and measures of quality of care. We will use indices of deprivation (Index of multiple deprivation, UK or Pobal deprivation index, ROI) as regional measures of deprivation. Measures of the quality of care relate to: time from referral to TIA clinic to attendance, proportions with CT head, MRI brain, or US Carotid Doppler imaging, and proportions with cardiac investigation.
3.8.5. Statistical Software and Significance
Analyses will be conducted using R (R Foundation for Statistical Computing, Vienna, Austria). Results will be presented with 95% confidence intervals to estimate the precision of the observed effects.
4. Ethics
4.1. Study Approval and Registration
The local lead at each centre is responsible for registering the study with the necessary approvals required within their country/area.
4.1.1. United Kingdom
In the United Kingdom, DATES should be registered as an audit and/or service evaluation study, as per the Health Research Authority (HRA) Decision Tool (Figure 2) [24]. Where necessary, Caldicott Guardian approvals should be sought for the collection of, and transfers of data out of the hospital/trust. A named Supervising Consultant is required at each centre, for supervision and help with local registration. All necessary approvals should be in place prior to data collection and/or data transfer. The DATES Steering Committee have provided dedicated templates for local registration as an audit/service evaluation and application for Caldicott Guardian approvals. All centres in NHS England must be compliant with National Data Opt-Out.
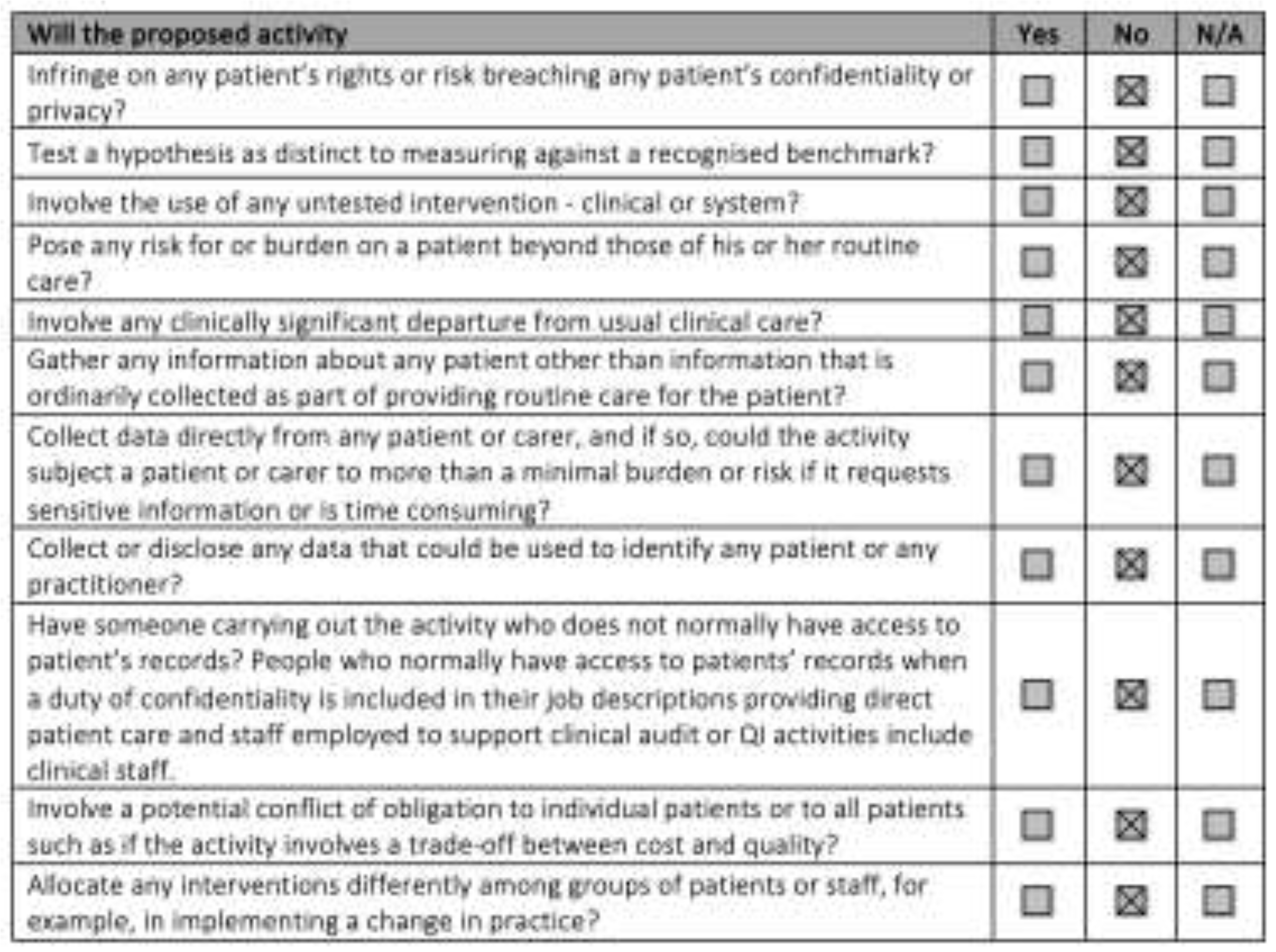
4.1.2. Republic of Ireland
DATES does not fall under the scope of the National Office for Research Ethics Committee (NREC), and as per the checklist provided by the Health Service Executive (HSE) below, does not require ethical oversight. This follows the below decision tool (Figure 3), found in Clinical Audit A Practical Guide 2023, HSE National Centre for Clinical Audit, National Quality and Patient Safety Directorate [25]. Local approvals may be necessary on a case-by-case basis.
4.2. Data Governance
DATES follows a similar approach to previous NANSIG studies such as DIMES [19].
Using a purpose-designed case report form, Collaborators will enter data onto a bespoke Microsoft Excel spreadsheet, stored on their hospital/trust’s password-protected server. DATES does not endorse use of data collection onto hard paper copies, but if used they should be destroyed as confidential waste at upload to local server. All data handling should be compliant with study-specific and local data governance policies.
DATES does not collate any patient identifiable information. Local teams may use identifier information for traceability and avoid duplication but should never be shared with DATES Steering Committee. Local teams in NHS England will need to use patient NHS numbers for purposes of compliance and checking against the NHS England’s Check for National Data Opt-Outs Service. Local teams are required to retain identifier information, until explicit advice from DATES Steering Committee for their destruction - this is to ensure 1) completion of Data Validation and Quality Assurance and 2) the opportunity for involvement in a subsequent follow up study.
Once data collection is complete, the Centre Lead is responsible for sending this de-identified data in original spreadsheet form to the DATES Steering Committee via a secure nhs.net encrypted email (or local equivalent). Prior to transfer, the Centre Lead must forward Caldicott Guardian approval/waiver to DATES Steering Committee.
All data cleaning and analysis will be performed by the DATES Steering Committee. Data may be stored for a period of no more than 10 years, and may used for future analyses at the Steering Committee’s discretion.
5. Dissemination and authorship
5.1. Dissemination of Results
Following study completion, the results will be written up for publication in a peer-reviewed medical journal, in accordance with STROBE guidelines [26]. This will be done primarily by a central Writing Group.
A teleconference will be held with all Collaborators to share study results alongside analysis methods. These results will be available to Collaborators to present at regional, national and international conferences by a standardised poster and PowerPoint presentation. These presentations will be coordinated by the DATES Steering Committee to fairly distribute presentation opportunities and avoid duplications.
Additionally, all Collaborators will be given a summary of results to share and present at their centres, with the aim to discuss results and possible improvements to local TIA care. Local teams can request summary reports of their own centre’s data from the Steering Committee following study completion. Individual centres will not be identified by their name in respect to their centre-level data (other than direct supply of a summary report above).
5.2. Authorship Eligibility
The DATES protocol will be published under a hybrid authorship model as per National Research Collaborative (NRC) authorship guidelines [27].
This protocol was finalised and circulated to collaborators on 01.06.24. Later version with minor edits was circulated on 16.12.24. Only minor edits relating to pre-print hosting platform specifications were made after this date.
All outputs following the protocol will be published under a full corporate model - i.e. Neurology and Neurosurgery Interest Group (NANSIG) collaborative (expandable). All Collaborators will be listed as PubMed-citable Collaborators per the roles defined below (so long as the minimum requirements for accreditation are met).
- Steering Committee: A central team comprising medical students and junior doctors who have the primary responsibility for designing protocols, coordinating projects, and managing data.
- Expert Advisory Group: Consists of experts in the field of stroke research or a relevant field to DATES study design. Individuals have been selected for their enthusiasm for supporting early researchers and for specific guidance to the Steering Committee. Responsibilities include:
- Critical review of study design, protocol, and study materials in order to improve their academic rigour.
- Critical review of drafted manuscripts for publication of study outputs.
- Writing and Data Analysis Group: consists of medical students, doctors, and Expert Advisory Group members responsible for overseeing the comprehensive scientific content, conducting data analysis, and preparing manuscripts.
- Centre Leads: Each centre’s primary liaison for data collection, overseeing local site setup, and managing governance. Centre Leads should be identified and recruited by NANSIG and are recommended to be a doctor or senior medical student within the local centre team. In the absence of extenuating circumstances, only one individual can fulfil the role of Centre Lead per local team. Requirements for accreditation on DATES outputs include:
- Overseeing site set-up, including recruitment of a Supervising Consultant and Collaborators.
- Attendance at a centralised induction session, conducted by the DATES Steering Committee.
- Primary individual responsible for securing local approvals for conduct of DATES (e.g. registration, seeking Caldicott Guardian permission and information governance approval – as required).
- Selecting, or acting as, a Data Validator and performing subsequent quality assurance (as per 3.3 Data Validation and Quality Assurance).
- Direct engagement within a local team while collecting data at the centre that fulfils the criteria for inclusion in the DATES dataset.
- Presentation of local results at their centre from DATES (or otherwise arranges another Collaborator to present on their behalf).
- Local Collaborators (Data Collectors or Data Validators): In addition to the Centre Lead, a suggested maximum of 10 Collaborators are accountable for data collection at a specific centre, preferably comprising medical students. Minimum requirements for authorship on DATES outputs include:
- Attendance at a centralised induction session, ran by the DATES Steering Committee
- Compliance with local audit/ service evaluation approval processes and data governance policies
- Active involvement in data collection or data validation and quality assurance (as per 3.3 Data Validation and Quality Assurance).
- Collaboration with the Centre Lead to ensure that results are reported back to audit/ service evaluation and clinical teams.
- Many of these individuals will be medical students though some may be doctors or stroke nurses or stroke research nurses, who may take additional responsibility with local supervision and/or support to inform data collection and aid complete case ascertainment.
- Supervising Consultant: Data collection in each centre must be supervised by a consultant. Minimum requirements for authorship on DATES outputs include:
- Completion of the centre survey and supplying local TIA referral/triage criteria to the Steering Committee.
- Sponsoring local registration and ensuring Collaborators adhere to local governance guidelines.
- Assisting the presentation of local results.
- Completion of workplace-based assessments for students or trainees (ePortfolio), if requested.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Steering Group: Dr Dorota Duklas, Dr Ashvin Kuri, Mr Siddarth Kannan, Dr Daoud Chaudhry, Dr David E. Henshall Dr Dorota Duklas: Conceptualisation, methodology, writing - original draft, writing - review & editing, visualisation, project administration, resources. [Study Lead/First author]. Dr Ashvin Kuri: Conceptualisation, methodology, writing - original draft, writing - review & editing. Mr Siddarth Kannan: Conceptualisation, methodology, writing - original draft, writing - review & editing, project administration. Dr Daoud Chaudhry: Conceptualisation, methodology, writing - original draft, writing - review & editing, resources. Dr David E. Henshall: Conceptualisation, methodology, writing - original draft, writing - review & editing, visualisation, project administration, supervision. [Last author]. Expert Advisory Group: Professor Ruth Dobson, Professor Avril Drummond, Professor Christopher K Farmer, Professor Martin James, Professor Mary Joan Macleod, Dr Grant Mair, Dr Aaizza Naqvi, Ms Sarah Rickard, Professor Thompson G Robinson, Professor Christine Roffe, Dr Conn Sugihara, Professor David J Werring Professor Ruth Dobson: methodology, writing - review & editing, supervision, advice on regulatory approvals. Professor Avril Drummond: methodology, writing - review & editing, advice on regulatory approvals. Professor Christopher K Farmer: methodology Professor Martin James: advice on regulatory approvals. Professor Mary Joan Macleod: resources Dr Grant Mair: methodology, writing - review & editing. Dr Aaizza Naqvi: methodology Ms Sarah Rickard: resources Professor Thompson G Robinson: methodology, writing - review & editing Professor Christine Roffe: methodology Dr Conn Sugihara: methodology Professor David J Werring: methodology Pilot study: Maidstone Hospital, Maidstone and Tunbridge Wells NHS Trust Dr William Old: Centre Lead Dr Navraj Singh Chattha: Supervising Consultant.
Funding
This study received no external funding. DATES Steering Committee are in receipt of no specific funding for the development and undertaking of this multicentre audit and service evaluation study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The pilot for the protocol was registered by Maidstone and Tunbridge Wells NHS Trust clinical audit department, (ID: 2141, registration date: 01/11/2023, approval date: 01/03/2024).
Informed Consent Statement
In the United Kingdom, the DATES study should not be registered as research. The Health Research Authority (HRA) decision tools have been used to confirm that this study is not considered research by the NHS and does not require NHS research ethics committee (REC) approval. As this audit uses routinely collected, de-identified clinical data and does not involve direct participant contact, individual informed consent was not required.
Data Availability Statement
As this is a study protocol there is no data available for sharing.
Acknowledgments
The following individuals are not listed as authors on the byline, but are included as part of a corporate authorship under Neurology and Neurosurgery Interest Group (NANSIG) Martin James a https://orcid.org/0000-0001-6065-6018, Mary Joan Macleod b https://orcid.org/0000-0003-2115-8184, Sarah Rickard c, Christine Roffe d https://orcid.org/0000-0002-5259-6649, Conn Sugihara e, Navraj Singh Chattha f https://orcid.org/0000-0001-8076-4681, William Old g a University of Exeter Medical School b University of Aberdeen c Greater Manchester Neurorehabilitation & Integrated Stroke Delivery Network d Keele University e Maidstone and Tunbridge Wells NHS Trust f Maidstone Hyperacute Stroke Unit g Kent Surrey and Sussex Deanery.
Conflicts of interest
Protocol authors have declared no conflicts of interest with relation to this pre-print with the exception of the following Professor Avril Drummond - Trustee of the UK Stroke Association, Member of RCP Intercollegiate working party for stroke. Have received research grants over many years for stroke rehabilitation research. Dr Grant Mair - Consultancy fees from Canon Medical Research Europe, Ltd. Professor David J Werring - David Werring has received: grant funding from the Stroke Association, Rosetrees Trust and the British Heart Foundation; speaking honoraria from Bayer; speaking and chairing honoraria from Alexion and NovoNordisk; and consultancy fees from Alnylam, Bayer and NovoNordisk. He is Chief Investigator for the PROHIBIT-ICH and OPTIMAS trials. He has participated on data safety monitoring or advisory boards for OXHARP DSMB, and the LACI-2, TICH-2, TICH-3, RESTART, MACE-ICH and PLINTH Trial Steering Committees.
Glossary: / Standardised terms Of abbreviations, standardised words for consistency
| ABCD2 | Age, blood pressure, Clinical features of the TIA, Duration of symptoms |
| AHA | American Heart Association |
| ASA | American Stroke Association |
| ATRIA | Anticoagulation and Risk Factors in Atrial Fibrillation |
| CHA2DS2 VASC | Congestive heart failure, Hypertension, Age > 75, Diabetes, prior Stroke/transient ischemic attack, Vascular disease history, Sex |
| CHADS2 | Congestive heart failure, Hypertension, Age > 75, Diabetes, prior Stroke/transient ischemic attack |
| CRF | Case report form |
| CT | Computed Tomography |
| DIMES | Delays in Multiple Sclerosis diagnosis |
| EAG | Expert advisory group |
| ECG | electrocardiogram |
| ECST | European Carotid Surgery Trial |
| EPR | electronic patient record |
| HAS-BLED | Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile international normalized ratio, Elderly (> 65 years), Drugs/alcohol concomitantly. |
| HbA1c | Glycated hemoglobin |
| HSE | Health Service Executive |
| HEMORR2HAGES | Hepatic or renal disease, ethanol abuse, malignancy, older (age > 75 years), reduced platelet count or function, hypertension (uncontrolled), anemia, genetic factors, excessive fall risk, and stroke. |
| HRA | Health Research Authority |
| MACCE | Major adverse cardiovascular and cerebrovascular events |
| MRI | Magnetic resonance imaging |
| NANSIG | The Neurology and Neurosurgery Interest Group (NANSIG) |
| NAPIER | National Audit of Pathways in Epileptic Seizure Referrals |
| NASCET | North American Symptomatic Carotid Endarterectomy Trial |
| NCGFS23 | National Clinical Guideline for Stroke 2023 |
| ND | Not documented |
| NA | Not applicable |
| NG128 | NICE guideline 128 |
| NRC | National Research Collaborative |
| NREC | National Office for Research Ethics Committee |
| ORBIT | Outcomes Registry for Better Informed Treatment of Atrial Fibrillation |
| PPV | Positive Predictive Value |
| ROI | Republic of Ireland |
| ROSIER | Recognition of Stroke in the Emergency Room Scale |
| SSNAP | Sentinel Stroke National Audit Programme |
| STROBE | The Strengthening the Reporting of Observational Studies in Epidemiology |
| TIA | Transient ischaemic attack |
| TRIPOD | Transparent Reporting of a multivariable model for Individual Prognosis Or Diagnosis |
| uBECTS | Understanding Benign Epilepsy with Centro-Temporal Spikes |
| UK | United Kingdom |
Appendix A
Included are supplementary documents including the data dictionary, centre-survey containing centre level variables, and case-report form.
References
- GBD Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet Neurology 2021;20(10):795. [CrossRef]
- Kennedy J, Hill MD, Ryckborst KJ, et al. Fast assessment of stroke and transient ischaemic attack to prevent early recurrence (FASTER): a randomised controlled pilot trial. The Lancet Neurology 2007;6(11):961-69. [CrossRef]
- Johnston SC, Easton JD, Farrant M, et al. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA. New England Journal of Medicine 2018;379(3):215-25. [CrossRef]
- National Institute for Health and Care Excellence. Stroke and transient ischaemic attack in over 16s: diagnosis and initial management [NG128]. 2019.
- Intercollegiate Stroke Working Party. National Clinical Guideline for Stroke for the UK and Ireland. London, 2023.
- Sentinel Stroke National Audit Programme. About SSNAP. London, 2024.
- NICE Clinical Knowledge Summaries. Stroke and TIA, 2023.
- NICE Clinical Knowledge Summaries. Stroke and TIA: Scenario: Secondary prevention following stroke and TIA, 2023.
- Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016;47(6):e98-e169.
- Kleindorfer DO, Towfighi A, Chaturvedi S, et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke 2021. [CrossRef]
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019;50(12):e344-e418. [CrossRef]
- Boulanger J, Lindsay M, Gubitz G, et al. Canadian stroke best practice recommendations for acute stroke management: prehospital, emergency department, and acute inpatient stroke care, update 2018. Int J Stroke 2018;13(9):949-84. [CrossRef]
- Gladstone DJ, Lindsay MP, Douketis J, et al. Canadian stroke best practice recommendations: secondary prevention of stroke update 2020. Can J Neurol Sci 2022;49(3):315-37. [CrossRef]
- BMJ Best Practice. Transient ischaemic attack. 2020.
- National Institute for Health and Care Excellence. Atrial fibrillation: diagnosis and management [NG196]. 2021.
- Park JJ, Ooi SZY, Gillespie CS, et al. The Neurology and Neurosurgery Interest Group (NANSIG)—ten years of cultivating interest in clinical neurosciences. Acta Neurochir (Wien) 2022;164(4):937-46. [CrossRef]
- Lee SH, Gillespie C, Bandyopadhyay S, et al. National audit of pathways in epileptic seizure referrals (NAPIER): A national, multicentre audit of first seizure clinics throughout the UK and Ireland. Seizure: European Journal of Epilepsy 2023;111:165-71. [CrossRef]
- Steinruecke M, Gillespie C, Ahmed N, et al. Care and three-year outcomes of children with benign epilepsy with centro-temporal spikes in England. Epilepsy Behav 2023;148:109465. [CrossRef]
- Kuri A, Henshall DE, Chaudhry D, et al. Delays in Multiple Sclerosis diagnosis (DIMES): protocol for a multicentre, observational study of multiple sclerosis diagnostic pathways in the United Kingdom and Republic of Ireland. BMC Neurol 2024;24(1):105. [CrossRef]
- National Institute for Health and Care Excellence. Stroke and TIA: What is the prevalence of stroke and TIA in the UK? 2023.
- Stroke Association. Not just a funny turn The real impact of TIA, 2014.
- Aguiar de Sousa D, Wilkie A, Norrving B, et al. Delivery of acute ischaemic stroke treatments in the European region in 2019 and 2020. Eur Stroke J 2023;8(3):618-28. [CrossRef]
- Giles MF, Rothwell PM. Substantial underestimation of the need for outpatient services for TIA and minor stroke. Age Ageing 2007;36(6):676-80. [CrossRef]
- Health Research Authority. Is my study research? 2023 [Available from: https://www.hra-decisiontools.org.uk/research/redirect.html2023.
- Health Service Executive National Centre for Clinical Audit. Clinical Audit A Practical Guide 2023. 2023.
- Von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. The lancet 2007;370(9596):1453-57. [CrossRef]
- Blencowe N, Glasbey J, Heywood N, et al. Recognising contributions to work in research collaboratives: guidelines for standardising reporting of authorship in collaborative research. Int J Surg 2018;52:355-60. [CrossRef]
Figure 2.
HRA decision tool outcomes, as applied to DATES.
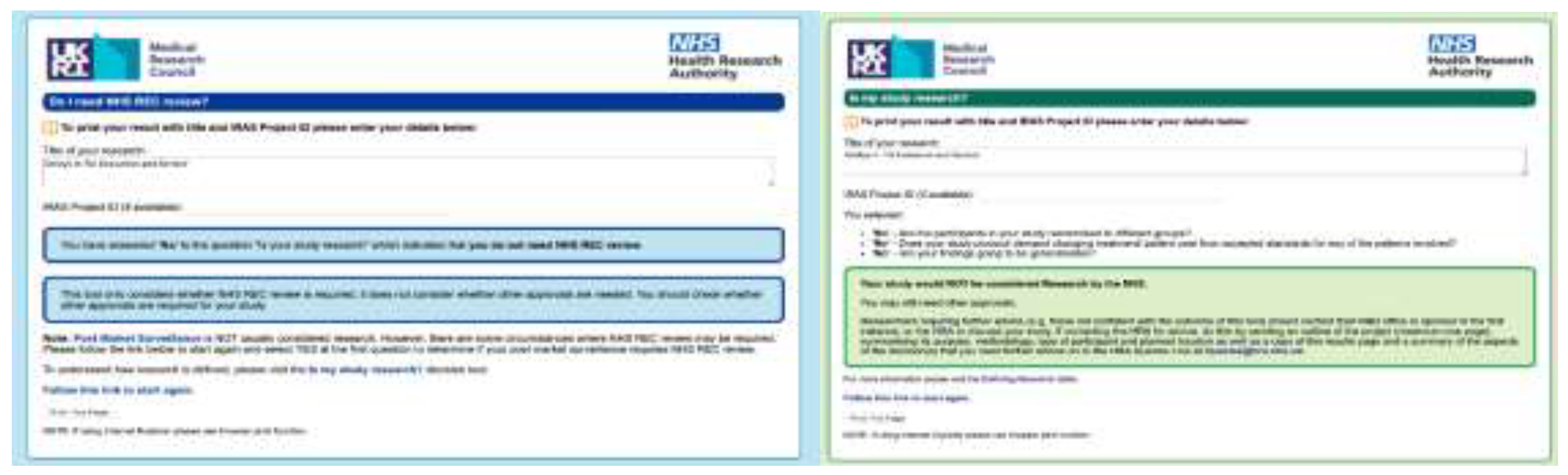
Figure 3.
The HSE National Centre for Clinical Audit example screening tool, as applied to DATES.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



