
Submitted:
15 January 2026
Posted:
16 January 2026
You are already at the latest version
Abstract
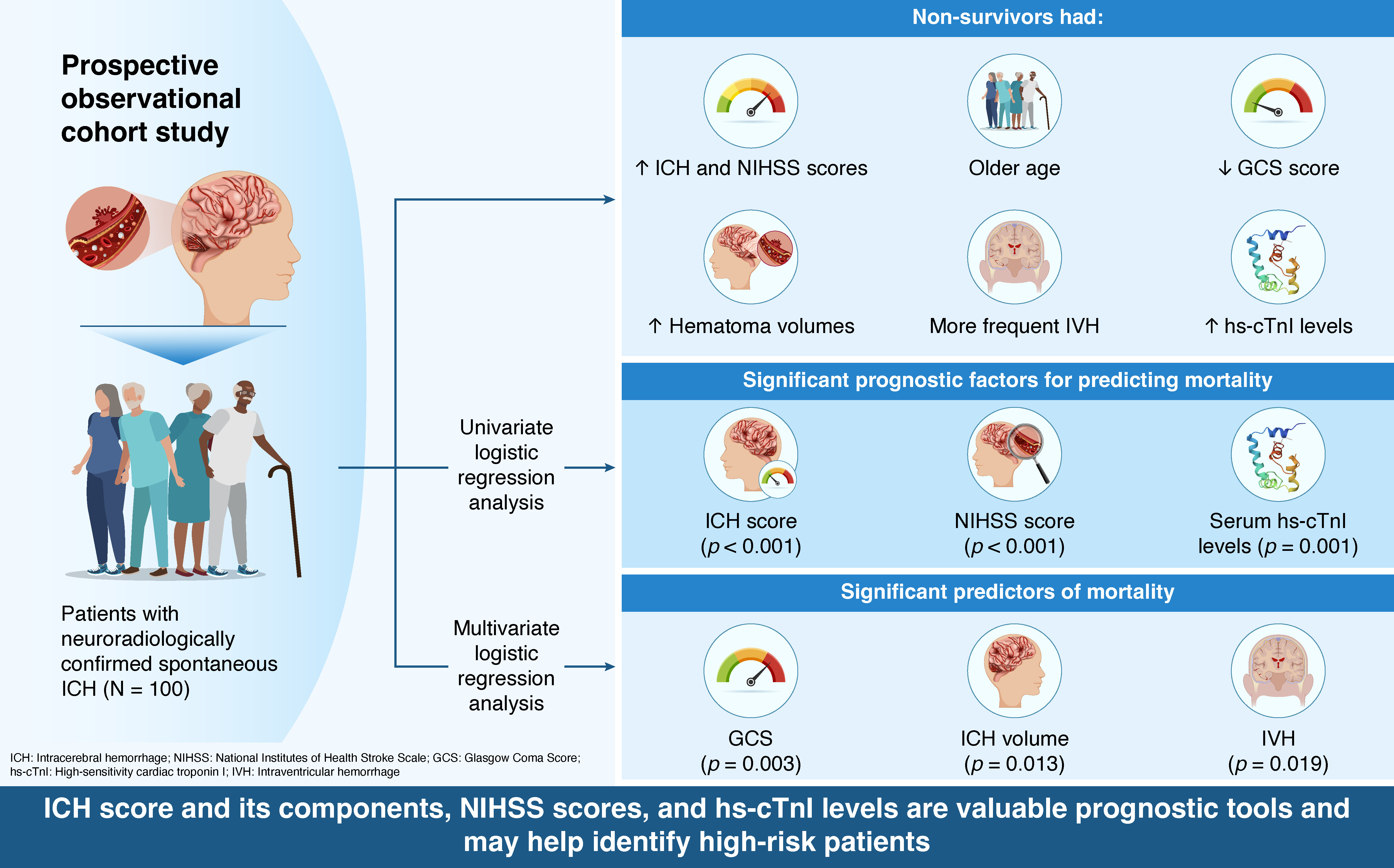
Background/Objectives: Spontaneous intracerebral hemorrhage (sICH) is a severe form of stroke associated with high mortality and disability rates, and reliable prognostic markers remain limited. This study aimed to evaluate the prognostic value of ICH score components, the National Institutes of Health Stroke Scale (NIHSS), and high-sensitivity cardiac troponin I (hs-cTnI) for predicting 30-day mortality in patients with sICH. Methods: In this prospective observational cohort study, 100 consecutive patients with neuroradiologically confirmed sICH were enrolled. Demographic data, clinical parameters, neuroimaging findings, and serum hs-cTnI levels were collected on admission. Subsequently, the ICH score, its individual components, and the NIHSS score were assessed. Results: Patients who died had significantly higher ICH and NIHSS scores, were older, had lower Glasgow Coma Scale (GCS) scores, larger hema-toma volumes, more frequent intraventricular hemorrhage (IVH), and elevated hs-cTnI levels compared with survivors. Serum hs-cTnI concentrations significantly correlated with ICH and NIHSS scores, lower GCS scores, larger hematoma volumes, and the presence of IVH. On univariate logistic regression, ICH score, NIHSS, and hs-cTnI were independent predictors of mortality, whereas multivariate analysis identified GCS score, hematoma volume, and IVH as significant determinants of fatal outcome. Conclusions: ICH score and its components, NIHSS, and serum hs-cTnI levels are valuable prognostic tools in patients with sICH. These markers may help clinicians identify high-risk pa-tients, optimize monitoring, and guide therapeutic decisions. Nevertheless, larger multicenter studies are warranted to further clarify their clinical implications in sICH management.
Keywords:
spontaneous intracerebral hemorrhage
; ICH score
; high-sensitivity cardiac troponin I
; age
; Glasgow Coma Scale
; hematoma volume
; intraventricular hemorrhage
; prognostic factors
; mortality
1. Introduction
Hemorrhagic stroke, defined as bleeding into the brain parenchyma with or without ventricular involvement, accounts for approximately 11% of all strokes in high-income countries and 22% in low- and middle-income countries [1,2,3]. It is associated with significantly higher morbidity and mortality than ischemic stroke, with a case fatality rate of 40% at one month and 54% at one year, whereas only 12% to 39% of survivors achieve long-term functional independence [4]. The most common form of hemorrhagic stroke is the spontaneous, non-traumatic rupture of cerebral blood vessels, known as spontaneous intracerebral hemorrhage (sICH), which carries a poor prognosis: approximately half of all patients die within the first month, and 80% of survivors require assistance with daily activities [1,3].
Systemic arterial hypertension and cerebral amyloid angiopathy are the two most important and well-established risk factors for sICH [5,6]. Additional factors associated with sICH include advanced age, men, Asian ethnicity, excessive alcohol consumption, current smoking, low plasma low-density lipoprotein cholesterol and triglyceride levels, cerebral microbleeds, chronic kidney disease, and the use of medications such as anticoagulants, antiplatelets, and sympathomimetics. Clinical manifestations of ICH vary according to the size and location of the hemorrhage and may include headache, nausea and vomiting, decreased level of consciousness, stupor or coma, seizures, higher cortical dysfunction, cranial nerve abnormalities, motor deficits, and cognitive impairment [4].
In recent years, substantial progress has been made in understanding the pathophysiology, identifying causative mechanisms, and improving the acute management of sICH [7]. Despite several therapeutic approaches, including hemostatic agents, acute blood pressure reduction, intraventricular alteplase administration, and surgical intervention, none have been conclusively shown to improve functional outcomes in patients with sICH [8]. This highlights the ongoing clinical challenges and the critical need for reliable prognostic biomarkers [7].
Prognostic factors consistently associated with poor outcomes include increased ICH and National Institutes of Health Stroke Scale (NIHSS) scores, age over 80 years, low Glasgow Coma Scale (GCS) score at admission, hematoma volume greater than 30 mL, delayed perihematomal edema, intraventricular hemorrhage (IVH), and infratentorial location of bleeding [4,9,10]. Comorbidities such as diabetes and renal dysfunction further worsen the prognosis in patients with sICH [11]. A post hoc analysis of a large randomized multicenter trial in China (CRRICH) identified right hemispheric involvement, IVH, advanced age, and higher NIHSS scores as predictors of poor outcomes in conservatively treated patients [12,13]. Furthermore, unfavorable outcomes following hematoma surgery have been associated with age over 58 years, elevated plasma glucose levels, GCS ≤8, larger hematoma volume, IVH, infratentorial hematoma location, and midline shift [14]. In this context, prognostic scoring systems such as the ICH score and NIHSS have been developed to assist physicians in assessing prognosis [15,16].
The cardiac troponin (cTn) complex, comprising three regulatory proteins (cTnI, cTnT, and cTnC), plays a crucial role in regulating cardiac contractility [17]. Among them, cTnI and cTnT are cardiac-specific isoforms and are clinically recognized as highly sensitive and specific “gold-standard” biomarkers for acute myocardial infarction [18,19,20]. Beyond myocardial ischemia, elevated cTn levels are frequently observed in various acute conditions, including tachyarrhythmias, heart failure, pulmonary embolism, shock, sepsis, and non-cardiac surgical procedures [21]. In patients with sICH, elevated cTnI levels are commonly observed, suggesting potential prognostic significance [22,23,24]. It has been suggested that this increase in cTnI reflects acute myocardial injury mediated by the brain–heart axis rather than primary myocardial ischemia [25]. Several studies have demonstrated associations between elevated serum cTn levels and poor functional outcomes as well as increased mortality [26,27], although others have failed to confirm such relationships [22,28]. Thus, the prognostic relevance of elevated cTn in the context of sICH remains uncertain [25].
Although several studies have investigated the prognostic value of the ICH score and its components, NIHSS, and serum cTnI levels in patients with sICH, findings remain inconsistent and insufficiently comprehensive. Accordingly, this study aimed to investigate the relationship between ICH characteristics and serum cTnI levels, as well as their potential to predict mortality in patients with sICH.
2. Materials and Methods
2.1. Study Design and Participants
A total of 100 hospitalized patients, including 46 men and 54 women, with neuroradiologically confirmed sICH were enrolled in this prospective observational cohort study conducted between April 2024 and April 2025 at the Department of Neurology, University Hospital Center (UHC) Mostar, Bosnia and Herzegovina. Exclusion criteria were incomplete medical documentation, traumatic ICH, and secondary ICH attributable to ruptured aneurysm, vascular malformation, or hemorrhagic transformation of ischemic stroke. The mean age of participants was 73.59 ± 12.57 years (range, 38–93 years). The follow-up period lasted 30 days from hospital admission. Vital status at 30 days was ascertained for all patients through hospital medical records and telephone contact with patients or their families after discharge, when applicable. In-hospital deaths were recorded directly from institutional databases, while post-discharge outcomes were verified using electronic health records and follow-up calls. No patient was lost to follow-up during the 30-day observation period.
The exclusive aim of the study was to collect data for scientific research purposes. Prior to participation, all patients provided written informed consent confirming their understanding of the study procedures, potential risks and benefits, and overall purpose. For patients unable to provide consent owing to their medical condition, consent was obtained from their closest relatives or legal guardians. Consent forms were written in Croatian to ensure comprehensibility. Participants were informed of their right to withdraw at any time without providing a reason and were assured of full anonymity and protection of personal information. Access to medical documentation was restricted to authorized research personnel and members of the Ethics Committee.
Ethical approval was granted by the Ethics Committee of the UHC Mostar (Approval No. 02-I-1479/23). The study was conducted in accordance with the principles of the Declaration of Helsinki and the Law on the Rights, Obligations, and Responsibilities of Patients in Bosnia and Herzegovina.
2.2. Data Collection
All patients underwent neurological examination, standard laboratory testing, and neuroradiological brain imaging with multislice computed tomography using a 256-slice GE Revolution CT scanner (GE Medical Systems, Waukesha, WI, USA). The ICH score is a widely used prognostic tool for estimating 30-day mortality in patients with sICH [29]. It is calculated by summing points across five clinical and radiological variables: GCS score, ICH volume, presence of IVH, infratentorial hematoma location, and age (Table 1). A higher score corresponds to an increased risk of short-term mortality [15].
The GCS score, used to assess the level of consciousness, comprises three components: eye response (1–4 points), verbal response (1–5 points), and motor response (1–6 points), with total scores ranging from 3 (deep coma) to 15 (fully alert). In general, a score ≤8 indicates a comatose state. The volume of intracerebral hematoma was estimated using the simplified ABC/2 method, a validated and widely applied approach in clinical practice. In this method, A represents the greatest diameter of the hematoma on the axial CT slice (cm), B is the diameter perpendicular to A on the same slice (cm), and C is calculated by multiplying the number of axial slices showing hemorrhage by the slice thickness (cm). The hematoma volume was calculated using the formula: Volume = (A × B × C)/2 and expressed in cubic centimeters (cm3), equivalent to milliliters (1 cm3 = 1 mL). A volume ≥30 mL was considered a significant risk factor and was scored accordingly on the ICH scale.
The NIHSS is a standardized clinical tool used to assess the severity of neurological deficits in patients with acute stroke. It consists of 11 items evaluating consciousness, vision, motor and sensory function, coordination, speech, and language. Higher scores indicate more severe neurological impairment. In addition to its role in clinical monitoring, the NIHSS is widely recognized as a prognostic tool [16].
Peripheral venous blood samples were obtained from each participant via cubital venipuncture and analyzed at the Laboratory for Molecular Diagnostics, UHC Mostar. Quality control was maintained using internal laboratory procedures compliant with ISO 15189 accreditation standards. All analyses were performed in a sex-partitioned manner based on the established upper reference limits. In addition to routine laboratory tests (complete blood count, metabolic panel, lipid profile, etc.), serum high-sensitivity cTnI (hs-cTnI) was measured using a chemiluminescent microparticle immunoassay (catalog no. 11291347, version 22.0) on the ADVIA Centaur XPT analyzer (Siemens Healthineers, Erlangen, Germany). The assay has a limit of detection of 1.6 pg/mL and a limit of quantitation of 2.5 pg/mL. The upper reference limits were 34.2 pg/mL for men and 15.6 pg/mL for women, according to manufacturer’s specifications and validated laboratory reference standards. Analytical imprecision (coefficient of variation) was <10% at both decision limits.
2.3. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics, version 25.0 (IBM Corp., Chicago, IL, USA) and JASP 0.95.4 (2025, University of Amsterdam, Netherlands). The Shapiro–Wilk test was used to assess the normality of variables. Results are presented as mean ± standard deviation or as frequencies and percentages. Group comparisons were conducted using the independent-samples t test for normally distributed variables and the Mann–Whitney U test for non-normally distributed variables. The independent-samples t test, Chi-square test, and Fisher’s exact test were used to assess differences between groups. Associations between variables were evaluated using Pearson’s correlation coefficient. Univariate and multivariate logistic regression analyses were performed to identify independent predictors of mortality. A p-value <0.05 was considered statistically significant. p-values not reportable to three decimal places are shown as <0.001.
3. Results
3.1. Outcome-Based Comparison of Clinical and Radiological Parameters
Table 2 compares clinical and radiological features between patients who survived and those who died following sICH. The groups differed significantly in age, GCS scores, ICH volume, IVH, and ICH and NIHSS scores. Patients who died had lower GCS scores (p < 0.001), larger hematoma volumes (p < 0.001), a higher incidence of IVH (p < 0.001), higher ICH and NIHSS scores (both p < 0.001), and were older (p = 0.015). In contrast, the infratentorial origin of hemorrhage did not differ significantly between the two groups (p = 0.304).
3.2. Serum Concentrations of High-Sensitivity Cardiac Troponin I
Figure 1 shows the serum concentrations of hs-cTnI in patients with sICH, comparing survivors and non-survivors. Serum hs-cTnI levels were significantly higher in patients who died (p < 0.001).
3.3. Correlation Values
Table 3 presents the correlation between serum hs-cTnI levels and various clinical and radiological characteristics of sICH. A moderate positive correlation was observed between serum hs-cTnI levels and total ICH score (r = 0.311, p = 0.002), as well as with individual parameters including lower GCS (r = -0.262, p = 0.009), larger ICH volume (r = 0.347, p < 0.001), and the presence of IVH (r = 0.342, p = 0.001). Positive correlations were also noted with infratentorial origin (r = 0.119, p = 0.240) and age (r = 0.031, p = 0.762), although these did not reach statistical significance. Furthermore, serum hs-cTnI concentrations showed a significant positive correlation with NIHSS (r = 0.381, p < 0.001).
3.4. Predictors of Mortality
Table 4 summarizes the results of univariate logistic regression analysis evaluating the predictive value of the ICH score, NIHSS, and serum hs-cTnI levels for patient mortality. All three parameters were significant predictors: higher ICH scores (p < 0.001), higher NIHSS scores (p < 0.001), and elevated serum hs-cTnI concentrations (p = 0.001) were associated with increased mortality in patients with sICH.
Table 5 presents the results of multivariate logistic regression analysis, in which the individual components of the ICH score were evaluated as predictors of mortality. GCS score, ICH volume, and IVH emerged as significant predictors, indicating that patients with lower GCS scores (p = 0.003), larger ICH volumes (p = 0.013), and the presence of IVH (p = 0.019) had a higher risk of death. Although infratentorial hematoma location and age showed a trend toward significance, they did not meet the conventional threshold to be considered predictors of mortality.
4. Discussion
ICH, the second most common subtype of stroke, is associated with considerably higher morbidity and mortality compared to ischemic stroke, representing a major social and healthcare burden [4]. Despite diagnostic advances over the past few decades, no highly effective biomarker for predicting outcomes has yet been identified [30]. Numerous factors have been reported in the literature as potential predictors of poor outcomes and mortality in patients with sICH; however, the results often show inconsistency and lack comprehensive coverage [4,9,10,25,31]. Therefore, we aimed to systematically assess the prognostic value of the ICH score and its components, NIHSS, and serum hs-cTnI levels in patients with sICH.
In this study, we found that overall ICH and NIHSS scores were significantly higher in patients who did not survive sICH. Notably, both parameters were also identified as significant independent predictors of mortality. These findings are consistent with that of a study conducted in Bangladesh by Ray SK et al., which reported that higher ICH scores were independent predictors of 30-day mortality and were significantly associated with poor functional outcomes [32]. Similarly, other studies have also shown that higher NIHSS scores are linked to a greater risk of death and worse functional recovery [12,31].
The results of our study indicated that patients who died from sICH were significantly older than those who survived. Although age showed a trend toward significance, it did not meet the conventional threshold to be considered an independent predictor of mortality. An international randomized controlled trial conducted among 2,839 patients with sICH (INTERACT2) revealed that subjects older than 75 years were four times more likely to die or be disabled compared with those younger than 52 years [33]. A study conducted by Bahrami M et al. found that age over 65 years was significantly associated with increased risks of IVH and subarachnoid hemorrhage [34]. An aging population, coupled with the growing indications for the use of oral anticoagulant and antithrombotic agents, suggests that the number of anticoagulated patients will continue to increase, which might negatively impact the epidemiology of sICH [31,35]. Moreover, the incidence of hypertension, diabetes, and coronary heart disease, recognized as significant risk factors for worsening prognosis in patients with sICH, is higher in older individuals [34].
Patients who died in our study exhibited significantly lower GCS scores and greater hematoma volumes compared with those who survived. Furthermore, multiple logistic regression analysis identified GCS score and ICH volume as independent predictors of mortality. In Asian populations, low initial GCS scores and larger hematoma volumes have consistently been reported as independent predictors of poor outcomes [4,9]. A large multicenter case-control study in South Korea involving 1,321 patients with sICH found that extensive white matter lesions were associated with lower GCS scores and higher mortality [36]. Ulger H et al. reported that patients with GCS values ≤9 had an increased risk of mortality and that hematoma volumes exceeding 44.16 mL were significant predictors of poor outcomes [30]. Initial ICH volumes greater than 30 mL have also been identified as significant predictors of mortality [9]. Conversely, some studies suggest that initial hematoma volume may serve as a better predictor of hematoma expansion rather than mortality [37].
Our results showed that patients who died had significantly higher rates of IVH compared with those who survived. Moreover, the presence of IVH appeared to be a significant factor in predicting mortality. The occurrence of IVH in patients with sICH has been established as a poor prognostic factor for hematoma expansion and fatal outcomes [9,31,37]. Neuroimaging features linked to increase in-hospital mortality include the presence of IVH, brainstem hemorrhage, and signs of recurrent bleeding [38]. Recent studies have also demonstrated that perihematomal edema, a radiological marker of secondary brain injury, is also associated with worsened outcomes in patients with ICH, particularly those with basal ganglia hemorrhage [10,39]. Baseline factors associated with larger perihematomal edema include higher NIHSS scores, older age, lower GCS scores, larger ICH volume, irregularly shaped hematomas, and higher glucose levels [40,41].
In our study, no significant differences were observed between groups with respect to hemorrhage location. Infratentorial hemorrhage did not appear to be a significant prognostic factor for fatal outcomes in patients with sICH, which contrasts with the findings of most other studies [15,29,42]. This discrepancy may be at least partially explained by the relatively small sample size of our study.
Over the years, the uncertain and often poor prognosis of patients with sICH has prompted researchers to investigate the pathophysiological role of peripheral blood biomarkers in brain injury and their prognostic potential. In this context, serum concentrations of numerous biomarkers, including angiogenic and growth factors, inflammatory markers, coagulation parameters, and blood counts, have been evaluated in several studies [43,44]. Among these, cTnI is one of the most frequently measured biomarkers, as randomized controlled trials and observational studies have reported severe adverse cardiac events in patients with stroke, including acute myocardial injury, acute coronary syndromes, systolic and diastolic left ventricular dysfunction, and arrhythmias [45,46].
Our study demonstrated that serum concentrations of hs-cTnI were significantly higher in patients who died compared with those who survived. Furthermore, univariate logistic regression analysis indicated that hs-cTnI is an independent predictor of mortality in patients with sICH. Analysis of data from a large, multicenter, prospective randomized trial (FAST) suggested that patients with sICH and elevated serum hs-cTnI levels face increased risks of poor outcomes and higher mortality at 15 and 90 days compared with those without acute myocardial injury [26]. In addition, several other studies have reported associations between elevated cTnI or cTnT levels and adverse functional outcomes as well as increased mortality [27,45,47]. The American Heart Association and the American Stroke Association recommend that patients with sICH be evaluated for acute coronary ischemia and coexisting myocardial injury using electrocardiography and cTn measurements [48]. Evidence from clinical studies and animal research indicates that the release of cTn is primarily driven by neurocardiogenic injury resulting from autonomic dysfunction. Excessive activation of the central autonomic network can lead to increased catecholamine release, which in turn may cause heightened adrenergic stimulation of the heart, resulting in coronary vasoconstriction, myocardial ischemia and necrosis, and arrhythmias. These cardiac changes associated with stroke have been collectively termed “stroke-heart syndrome” [22,46,49].
Results of our study showed a moderate positive correlation between serum hs-cTnI levels and NIHSS, total ICH score, and its individual components, including lower GCS score, larger hematoma volume, and the presence of IVH. These findings are consistent with those reported by Qin G et al., who identified insular involvement, hematoma volume greater than 30 mL, and the presence of IVH as among the strongest predictors of elevated myocardial enzyme levels following the onset of sICH [50]. Elevated serum cTn levels were also significantly correlated with lower GCS and higher NIHSS scores [51]. Such associations may be explained by the crucial role of the insular cortical and subcortical regions in maintaining cardiac sympathetic output [52]. Furthermore, IVH expansion may trigger acute activation of the sympathetic nervous system, leading to myocardial injury and cardiac arrhythmia [51,53].
At the same time, some studies have not confirmed a clear link between elevated serum cTn levels and worse outcomes in patients with stroke [22,28,54]. Gulia A et al. suggested that elevated cTn levels may predict mortality in patients with acute ischemic stroke and subarachnoid hemorrhage, although this association was not observed in patients with sICH, highlighting the complexity of using cTn as a prognostic marker [23]. Overall, the literature presents conflicting evidence regarding the prognostic significance of cTn in acute stroke, which may be partly explained by the influence of factors unrelated to sICH on myocardial enzyme levels [50,55].
This study has some limitations that should be acknowledged. First, it was a prospective observational cohort study conducted at a single center, which may limit the generalizability of the findings to other populations or healthcare settings. Second, the relatively small number of participants may have contributed to the lack of statistically significant associations between hs-cTnI levels and certain ICH characteristics, as well as to why some individual components of the ICH score did not emerge as significant predictors of mortality. Third, serum hs-cTnI was measured only once at admission, preventing assessment of dynamic changes over time and whether elevated levels were transient or persistent. Additionally, data on long-term functional outcomes, such as scores from the Modified Rankin Scale or mortality beyond 30 days, were not collected, limiting the ability to fully evaluate the prognostic relevance of hs-cTnI. Finally, although we adjusted for major clinical and radiological variables, the potential influence of unmeasured confounders, such as underlying coronary artery disease or variations in prehospital care, cannot be excluded. Despite these limitations, our findings provide valuable insights into the potential role of clinical scores and hs-cTnI as prognostic markers in patients with sICH and offer a foundation for future, larger prospective studies.
5. Conclusions
Results of our study indicate that ICH score and its components, NIHSS, and serum hs-cTnI levels provide valuable prognostic information in patients with sICH. These markers can help clinicians identify patients at higher risk of mortality and guide optimized monitoring and care. Combining hs-cTnI assessment with the ICH scores and NIHSS may enhance early risk stratification and support more informed therapeutic decisions. Nevertheless, future multicenter studies with larger cohorts and serial hs-cTnI measurements are warranted to confirm these findings and further clarify their role in patient management.
Author Contributions
Conceptualization, N.M., I.Ć., K.V., M.B., and A.K.; methodology, N.M., I.Ć., M.B., S.L. and A.K.; formal analysis, N.M., I.Ć., J.S., and M.B.; investigation, N.M. and J.S.; validation, N.M., I.Ć., J.S., K.V., M.B., S.L. and A.K.; writing—original draft preparation, N.M., I.Ć., K.V. and S.L.; writing—review and editing, N.M., I.Ć., J.S., K.V., S.L. and A.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Our study is not a newly initiated prospective experiment by the authors. Instead, it is a secondary analysis of de-identified data from the English Longitudinal Study of Ageing (ELSA).
Informed Consent Statement
Informed consent is waived due to secondary analysis.
Data Availability Statement
Data will be provided upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| cTn | Cardiac troponin |
| GCS | Glasgow Coma Scale |
| hs-cTnI | High-sensitivity cardiac troponin I |
| ICH | Intracerebral hemorrhage |
| IVH | Intraventricular hemorrhage |
| NIHSS | National Institutes of Health Stroke Scale |
| sICH | Spontaneous intracerebral hemorrhage |
| UHC | University Hospital Center |
References
- Al-Shahi Salman, R.; Frantzias, J.; Lee, R.J.; Lyden, P.D.; Battey, T.W.K.; Ayres, A.M.; Goldstein, J.N.; Mayer, S.A.; Steiner, T.; Wang, X.; et al. Absolute risk and predictors of the growth of acute spontaneous intracerebral haemorrhage: a systematic review and meta-analysis of individual patient dana. Lancet Neurol 2018, 17, 885–894. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Lawes, C.M.M.; Bennett, D.A.; Barker-Collo, S.L.; Parag, V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol 2009, 8, 355–369. [Google Scholar] [CrossRef]
- van Asch, C.J.; Luitse, M.J.; Rinkel, G.J.; van der Tweel, I.; Algra, A.; Klijn, C.J. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol 2010, 9, 167–176. [Google Scholar] [CrossRef]
- An, S.J.; Kim, T.J.; Yoon, B.W. Epidemiology, Risk Factors, and Clinical Features of Intracerebral Hemorrhage: An Update. J Stroke 2017, 19, 3–10. [Google Scholar] [CrossRef]
- Ariesen, M.J.; Claus, S.P.; Rinkel, G.J.; Algra, A. Risk factors for intracerebral hemorrhage in the general population: a systematic review. Stroke 2003, 34, 2060–2065. [Google Scholar] [CrossRef]
- Yamada, M. Cerebral amyloid angiopathy: emerging concepts. J Stroke 2015, 17, 17–30. [Google Scholar] [CrossRef]
- Hostettler, I.C.; Seiffge, D.J.; Werring, D.J. Intracerebral hemorrhage: an update on diagnosis and treatment. Expert Rev Neurother 2019, 19, 679–694. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.; Biller, J. Recent advances in spontaneous intracerebral hemorrhage. F1000Res 2019, 8, F1000 Faculty Rev–302. [Google Scholar] [CrossRef]
- Chen, H.S.; Hsieh, C.F.; Chau, T.T.; Yang, C.D.; Chen, Y.W. Risk factors of in-hospital mortality of intracerebral hemorrhage and comparison of ICH scores in a Taiwanese population. Eur Neurol 2011, 66, 59–63. [Google Scholar] [CrossRef]
- Huang, Q.; Wu, L.; Song, Z.; Zhang, Z.; Kuang, H.; Zhu, Y.; Zeng, C.; Zhang, L.; Zhang, H.; Xu, Z.; et al. Hematoma, Perihematomal Edema, and Total Lesion Predict Outcome in Patients With Intracerebral Hemorrhage. Brain Behav 2025, 15, e70340. [Google Scholar] [CrossRef] [PubMed]
- Miyagi, T.; Koga, M.; Yamagami, H.; Okuda, S.; Okada, Y.; Kimura, K.; Shiokawa, Y.; Nakagawara, J.; Furui, E.; Hasegawa, Y.; et al. Reduced estimated glomerular filtration rate affects outcomes 3 months after intracerebral hemorrhage: the stroke acute management with urgent risk-factor assessment and improvement-intracerebral hemorrhage study. J Stroke Cerebrovasc Dis 2015, 24, 176–182. [Google Scholar] [CrossRef]
- Zeng, L.; Zhang, Q.; Xia, Z.; Cui, W.; Guo, J. Predictors of poor outcomes in patients with intracerebral hemorrhage. Front Neurol 2025, 16, 1517760. [Google Scholar] [CrossRef] [PubMed]
- Diringer, M.N.; Skolnick, B.E.; Mayer, S.A.; Steiner, T.; Davis, S.M.; Brun, N.C.; Broderick, J.P. Thromboembolic events with recombinant activated factor VII in spontaneous intracerebral hemorrhage: results from the Factor Seven for Acute Hemorrhagic Stroke (FAST) trial. Stroke 2010, 41, 48–53. [Google Scholar] [CrossRef]
- Zhang, K.; Wei, L.; Zhou, X.; Yang, B.; Meng, J.; Wang, P. Risk factors for poor outcomes of spontaneous supratentorial cerebral hemorrhage after surgery. J Neurol 2022, 269, 3015–3025. [Google Scholar] [CrossRef] [PubMed]
- Hemphill, J.C.; Bonovich, D.C.; Besmertis, L.; Manley, G.T.; Johnston, S.C. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke 2001, 32, 891–897. [Google Scholar] [CrossRef]
- Lyden, P.; Brott, T.; Tilley, B.; Welch, K.M.; Mascha, E.J.; Levine, S.; Haley, E.C.; Grotta, J.; Marler, J. Improved reliability of the NIH Stroke Scale using video training. NINDS TPA Stroke Study Group. Stroke 1994, 25, 2220–2226. [Google Scholar] [CrossRef] [PubMed]
- Tiambeng, T.N.; Tucholski, T.; Wu, Z.; Zhu, Y.; Mitchell, S.D.; Roberts, D.S.; Jin, Y.; Ge, Y. Analysis of cardiac troponin proteoforms by top-down mass spectrometry. Methods Enzymol 2019, 626, 347–374. [Google Scholar] [CrossRef]
- Apple, F.S.; Sandoval, Y.; Jaffe, A.S.; Ordonez-Llanos, J. IFCC Task Force on Clinical Applications of Cardiac Bio-markers. Cardiac Troponin Assays: Guide to Understanding Analytical Characteristics and Their Impact on Clinical Care. Clin Chem 2017, 63, 73–81. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). J Am Coll Cardiol 2018, 72, 2231–2264. [Google Scholar] [CrossRef]
- Gerner, S.T.; Auerbeck, K.; Sprügel, M.I.; Sembill, J.A.; Madžar, D.; Gölitz, P.; Hoelter, P.; Kuramatsu, J.B.; Schwab, S.; Huttner, H.B. Peak Troponin I Levels Are Associated with Functional Outcome in Intraerebral Hemorrhage. Cerebrovasc Dis 2018, 46, 72–81. [Google Scholar] [CrossRef]
- Gualandro, D.M.; Puelacher, C.; Mueller, C. High-sensitivity cardiac troponin in acute conditions. Curr Opin Crit Care 2014, 20, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Lesch, H.; Haucke, L.; Kruska, M.; Ebert, A.; Becker, L.; Szabo, K.; Akin, I.; Alonso, A.; Fastner, C. Myocardial injury in spontaneous intracerebral hemorrhage is not predicted by prior cardiac disease or neurological status: results from the Mannheim Stroke database. Front Neurol 2025, 16, 1510361. [Google Scholar] [CrossRef]
- Gulia, A.; Srivastava, M.; Kumar, P. Elevated troponin levels as a predictor of mortality in patients with acute stroke: a systematic review and meta-analysis. Front Neurol 2024, 15, 1351925. [Google Scholar] [CrossRef] [PubMed]
- Wettersten, N.; Maisel, A. Role of cardiac troponin levels in acute heart failure. Card Fail Rev 2015, 1, 102–106. [Google Scholar] [CrossRef]
- Lesch, H.; Kruska, M.; Marx, A.; Haucke, L.; Ebert, A.; Becker, L.; Szabo, K.; Akin, I.; Alonso, A.; Fastner, C. The phenomenon of dynamic change of cardiac troponin levels in patients with spontaneous intracerebral hemorrhage increases in-hospital mortality independent of macrovascular coronary artery disease. J Neurol Sci 2025, 476, 123633. [Google Scholar] [CrossRef] [PubMed]
- Rosso, M.; Stengl, H.; Scheitz, J.F.; Lewey, J.; Mayer, S.A.; Yaghi, S.; Kasner, S.E.; Witsch, J. Acute myocardial injury in spontaneous intracerebral hemorrhage: a secondary observational analysis of the FAST trial. J Am Heart Assoc 2024, 13, e035053. [Google Scholar] [CrossRef]
- Hays, A.; Diringer, M.N. Elevated troponin levels are associated with higher mortality following intracerebral hemorrhage. Neurology 2006, 66, 1330–1334. [Google Scholar] [CrossRef]
- Maramattom, B.V.; Manno, E.M.; Fulgham, J.R.; Jaffe, A.S.; Wijdicks, E.F.M. Clinical importance of cardiac troponin release and cardiac abnormalities in patients with supratentorial cerebral hemorrhages. Mayo Clin Proc 2006, 81, 192–196. [Google Scholar] [CrossRef]
- Safatli, D.A.; Günther, A.; Schlattmann, P.; Schwarz, F.; Kalff, R.; Ewald, C. Predictors of 30-day mortality in patients with spontaneous primary intracerebral hemorrhage. Surg Neurol Int 2016, 7 Supplement 18, S510–S517. [Google Scholar] [CrossRef]
- Ulger, H.; Icme, F.; Parlatan, C.; Avci, B.S.; Aksay, E.; Avci, A. Prognostic relationship between high sensitivity troponin I level, hematoma volume and glasgow coma score in patients diagnosed with spontaneous intracerebral hemorrhage. Ir J Med Sci 2024, 193, 2559–2565. [Google Scholar] [CrossRef]
- De Rosa, L.; Manara, R.; Vodret, F.; Kulyk, C.; Montano, F.; Pieroni, A.; Viaro, F.; Zedde, M.L.; Napoletano, R.; Ermani, M.; et al. The “SALPARE study” of spontaneous intracerebral hemorrhage: part 1. Neurol Res Pract 2023, 5, 5. [Google Scholar] [CrossRef]
- Ray, S.K.; Sadekur Rahman Sarkar, M.; Ahmed, K.M.A.; Hasan, M.; Esteak, T.; Uddin, M.N.; Alam, J.A.J.; Hasan, F.M.M.; Chowdhury, M.T.I.; Mondal, M.B.A. Predicting 30-Day Outcomes in Primary Intracerebral Hemorrhage Using the Intracerebral Hemorrhage Score: A Study in Bangladesh. Cureus 2024, 16, e73227. [Google Scholar] [CrossRef] [PubMed]
- Rådholm, K.; Arima, H.; Lindley, R.I.; Wang, J.; Tzourio, C.; Robinson, T.; Heeley, E.; Anderson, C.S.; Chalmers, J.; INTERACT2 Investigators. Older age is a strong predictor for poor outcome in intracerebral haemorrhage: the INTERACT2 study. Age Ageing 2015, 44, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, M.; Keyhanifard, M.; Afzali, M. Spontaneous intracerebral hemorrhage, initial computed tomography (CT) scan findings, clinical manifestations and possible risk factors. Am J Nucl Med Mol Imaging 2022, 12, 106–112. [Google Scholar] [PubMed]
- Béjot, Y.; Cordonnier, C.; Durier, J.; Aboa-Eboulé, C.; Rouaud, O.; Giroud, M. Intracerebral haemorrhage profiles are changing: results from the Dijon population-based study. Brain 2013, 136, 658–664. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, B.J.; Ryu, W.S.; Kim, C.K.; Kim, N.; Park, B.J.; Yoon, B.W. White matter lesions and poor outcome after intracerebral hemorrhage: a nationwide cohort study. Neurology 2010, 74, 1502–1510. [Google Scholar] [CrossRef]
- Bakar, B.; Akkaya, S.; Say, B.; Yuksel, U.; Alhan, A.; Turğut, E.; Ogden, M.; Ergun, U. In spontaneous intracerebral hematoma patients, prediction of the hematoma expansion risk and mortality risk using radiological and clinical markers and a newly developed scale. Neurol Res 2021, 43, 482–495. [Google Scholar] [CrossRef]
- Ferrete-Araujo, A.M.; Egea-Guerrero, J.J.; Vilches-Arenas, Á.; Godoy, D.A.; Murillo-Cabezas, F. Predictors of mortality and poor functional outcome in severe spontaneous intracerebral hemorrhage: a prospective observational study. Med Intensiva 2015, 39, 422–432. [Google Scholar] [CrossRef]
- Murthy, S.B.; Moradiya, Y.; Dawson, J.; Lees, K.R.; Hanley, D.F.; Ziai, W.C.; VISTA-ICH Collaborators. Perihematomal Edema and Functional Outcomes in Intracerebral Hemorrhage: Influence of Hematoma Volume and Location. Stroke 2015, 46, 3088–3092. [Google Scholar] [CrossRef]
- Peng, W.J.; Li, Q.; Tang, J.H.; Reis, C.; Araujo, C.; Feng, R.; Yuan, M.H.; Jin, L.Y.; Cheng, Y.L.; Jia, Y.J.; et al. The risk factors and prognosis of delayed perihematomal edema in patients with spontaneous intracerebral hemorrhage. CNS Neurosci Ther 2019, 25, 1189–1194. [Google Scholar] [CrossRef]
- Wu, T.Y.; Sharma, G.; Strbian, D.; Putaala, J.; Desmond, P.M.; Tatlisumak, T.; Davis, S.M.; Meretoja, A. Natural History of Perihematomal Edema and Impact on Outcome After Intracerebral Hemorrhage. Stroke 2017, 48, 873–879. [Google Scholar] [CrossRef]
- Poon, M.T.C.; Fonville, A.F.; Al-Shahi Salman, R. Long-term prognosis after intracerebral haemorrhage: systematic review and meta-analysis. J Neurol Neurosurg Psychiatry 2014, 85, 660–667. [Google Scholar] [CrossRef]
- Sasongko, A.B.; Perdana Wahjoepramono, P.O.; Halim, D.; Aviani, J.K.; Adam, A.; Tsai, Y.T.; Wahjoepramono, E.J.; July, J.; Achmad, T.H. Potential blood biomarkers that can be used as prognosticators of spontaneous intracerebral hemorrhage: A systematic review and meta-analysis. PLOS One 2025, 20, e0315333. [Google Scholar] [CrossRef]
- Wu, X.; He, H.; Shen, D.; Ye, X.; Chen, Z.; Zou, S.; Zhou, K.; Ye, X.; Zhang, Z.; Li, H.; et al. Usefulness of Serum NOX4 as a Potential Biomarker to Predict Early Neurological Deterioration and Poor Outcome of Spontaneous Intracerebral Hemorrhage: A Prospective Observational Study. Neuropsychiatr Dis Treat 2025, 21, 295–307. [Google Scholar] [CrossRef]
- Garrett, M.C.; Komotar, R.J.; Starke, R.M.; Doshi, D.; Otten, M.L.; Connolly, E.S. Elevated troponin levels are predictive of mortality in surgical intracerebral hemorrhage patients. Neurocrit Care 2010, 12, 199–203. [Google Scholar] [CrossRef]
- Scheitz, J.F.; Sposato, L.A.; Schulz-Menger, J.; Nolte, C.H.; Backs, J.; Endres, M. Stroke-Heart Syndrome: Recent Advances and Challenges. J Am Heart Assoc 2022, 11, e026528. [Google Scholar] [CrossRef] [PubMed]
- Chung, P.W.; Won, Y.S.; Kwon, Y.J.; Choi, C.S.; Kim, B.M. Initial troponin level as a predictor of prognosis in patients with intracerebral hemorrhage. J Korean Neurosurg Soc 2009, 45, 355–359. [Google Scholar] [CrossRef]
- Hemphill, J.C.; Greenberg, S.M.; Anderson, C.S.; Becker, K.; Bendok, B.R.; Cushman, M.; Fung, G.L.; Goldstein, J.N.; Macdonald, R.L.; Mitchell, P.H.; et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2015, 46, 2032–2060. [Google Scholar] [CrossRef] [PubMed]
- Scheitz, J.F.; Nolte, C.H.; Doehner, W.; Hachinski, V.; Endres, M. Stroke-heart syndrome: clinical presentation and underlying mechanisms. Lancet Neurol 2018, 17, 1109–1120. [Google Scholar] [CrossRef]
- Qin, G.; Dai, C.; Feng, S.; Wu, G. Changes of Electrocardiogram and Myocardial Enzymes in Patients with Intracerebral Hemorrhage. Dis Markers 2022, 2022, 9309444. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Lin, J.; Wang, D.; Liu, M.; Hao, Z.; Lei, C. Cardiac troponin and cerebral herniation in acute intracerebral hemorrhage. Brain Behav 2017, 7, e00697. [Google Scholar] [CrossRef] [PubMed]
- Marins, F.R.; Limborço-Filho, M.; D’Abreu, B.F.; Machado de Almeida, P.W.; Gavioli, M.; Xavier, C.H.; Oppenheimer, S.M.; Guatimosim, S.; Fontes, M.A.P. Autonomic and cardiovascular consequences resulting from experimental hemorrhagic stroke in the left or right intermediate insular cortex in rats. Auton Neurosci 2020, 227, 102695. [Google Scholar] [CrossRef]
- Chen, C.H.; Tang, S.C.; Lee, D.Y.; Shieh, J.S.; Lai, D.M.; Wu, A.Y.; Jeng, J.S. Impact of Supratentorial Cerebral Hemorrhage on the Complexity of Heart Rate Variability in Acute Stroke. Sci Rep 2018, 8, 11473. [Google Scholar] [CrossRef]
- Etgen, T.; Baum, H.; Sander, K.; Sander, D. Cardiac troponins and N-terminal pro-brain natriuretic peptide in acute ischemic stroke do not relate to clinical prognosis. Stroke 2005, 36, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Abdi, S.; Oveis-Gharan, S.; Sinaei, F.; Ghorbani, A. Elevated troponin T after acute ischemic stroke: Association with severity and location of infarction. Iran J Neurol 2015, 14, 35–40. [Google Scholar] [PubMed]
Figure 1.
Serum levels of hs-cTnI in patients with sICH.
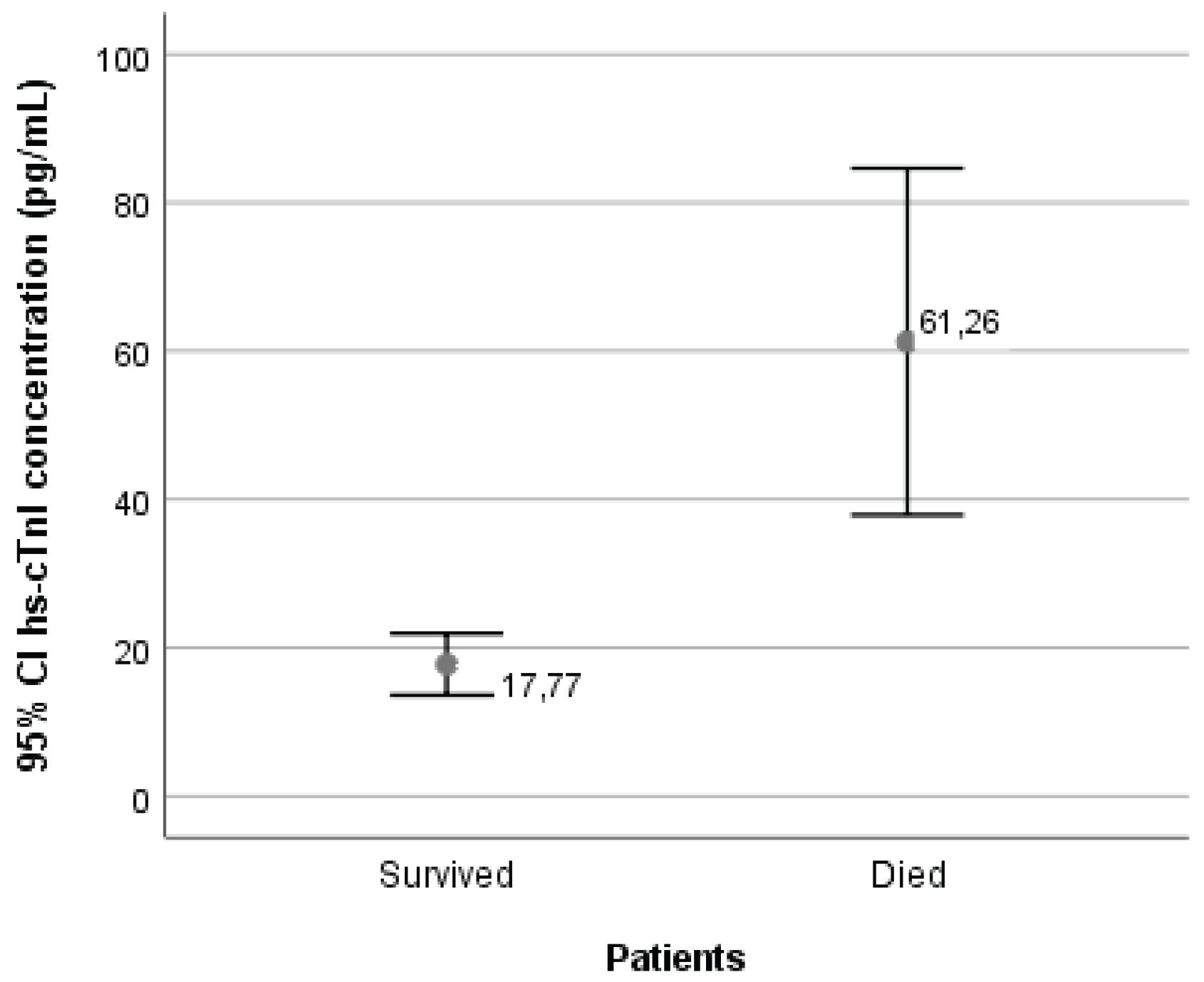

Table 1.
Components of the ICH score.
| Component | Criteria | Points |
|---|---|---|
| GCS score | 3–4 | 2 |
| 5–12 | 1 | |
| 13–15 | 0 | |
| ICH volume | ≥30 mL | 1 |
| <30 mL | 0 | |
| IVH | Present | 1 |
| Absent | 0 | |
| Infratentorial origin | Yes | 1 |
| No | 0 | |
| Age | ≥80 years | 1 |
| <80 years | 0 | |
| Total Score Range | 0-6 | |
| Estimated 30-day mortality risk: 0 points: 0%, 1 point: 13%, 2 points: 26%, 3 points: 72%, 4 points: 97%, 5-6 points: 100% | ||
Abbreviations: GCS: Glasgow Coma Scale; ICH: Intracerebral Hemorrhage; IVH: Intraventricular Hemorrhage.
Table 2.
Comparison of ICH score and its components, and NIHSS between patient groups.
| Variable | Survived N=65 (%) |
Died N=35 (%) |
p |
| GCS score | <0.001A | ||
| 3-4 | 2 (3.1) | 11 (31.4) | |
| 5-12 | 9 (13.8) | 11 (31.4) | |
| 13-15 | 54 (83.1) | 13 (37.2) | |
| ICH volume (mL) | <0.001B | ||
| <30 | 47 (72.3) | 9 (25.7) | |
| ≥30 | 18 (27.7) | 26 (74.3) | |
| IVH | <0.001B | ||
| Yes | 15 (23.1) | 26 (74.3) | |
| No | 50 (76.9) | 9 (25.7) | |
| Infratentorial origin | 0.304B | ||
| Yes | 8 (12.3) | 7 (20.0) | |
| No | 57 (87.7) | 28 (80.0) | |
| Age (years) | 71.35±13.16 | 77.74±10.34 | 0.015C |
| ICH score | <0.001A | ||
| 0 | 17 (26.2) | 2 (5.7) | |
| 1 | 26 (40.0) | 2 (5.7) | |
| 2 | 11 (16.9) | 5 (14.3) | |
| 3 | 7 (10.8) | 13 (37.1) | |
| 4 | 4 (6.1) | 6 (17.2) | |
| 5 | 0 (0.0) | 3 (8.6) | |
| 6 | 0 (0.0) | 4 (11.4) | |
| NIHSS | 7.06±5.06 | 23.11±8.60 | <0.001C |
Abbreviations: N (%): number (percentage) of patients; GCS: Glasgow Coma Scale; ICH: intracerebral hemorrhage; IVH: intraventricular hemorrhage; NIHSS: National Institutes of Health Stroke Scale. Age is presented as mean ± standard deviation. AFisher’s exact test; BChi-square test; Ct test for independent samples.
Table 3.
Correlation of serum hs-cTnI levels with ICH score, its components, and NIHSS.
| Variable | Serum levels of hs-cTnI | |
| r | p | |
| ICH score | 0.311 | 0.002 |
| GCS score | -0.262 | 0.009 |
| ICH volume | 0.347 | <0.001 |
| IVH | 0.342 | 0.001 |
| Infratentorial origin | 0.119 | 0.240 |
| Age | 0.031 | 0.762 |
| NIHSS | 0.381 | <0.001 |
Abbreviations: hs-cTnI: high-sensitivity cardiac troponin I; GCS: Glasgow Coma Score; ICH: intracerebral hemorrhage; IVH: intraventricular hemorrhage; NIHSS: National Institutes of Health Stroke Scale.
Table 4.
Predictive value of ICH score, NIHSS, and hs-cTnI for patient mortality.
| Model | Variable | B | Exp (B) | 95% CI | p |
| 1 | ICH score | 1.017 | 2.764 | 1.829-4.178 | <0.001 |
| 2 | NIHSS | 0.367 | 1.443 | 1.241-1.679 | <0.001 |
| 3 | Serum hs-cTnI levels | 0.027 | 1.028 | 1.012-1.044 | 0.001 |
Abbreviations: ICH: intracerebral hemorrhage; NIHSS: National Institutes of Health Stroke. Scale; hs-cTnI: high-sensitivity cardiac troponin I.
Table 5.
Predictive value of ICH score components for patient mortality.
| Variable | B | Exp (B) | 95% CI | p |
| GCS score | -0.227 | 0.797 | 0.686-0.925 | 0.003 |
| ICH volume | 0.017 | 1.017 | 1.004-1.031 | 0.013 |
| IVH | 1.507 | 4.514 | 1.277-15.958 | 0.019 |
| Infratentorial origin | -0.183 | 0.833 | 0.139-4.996 | 0.841 |
| Age | 0.044 | 1.045 | 0.989-1.104 | 0.116 |
Abbreviations: GCS: Glasgow Coma Score; ICH: intracerebral hemorrhage; IVH: intraventricular hemorrhage.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



