Submitted:
15 January 2026
Posted:
16 January 2026
You are already at the latest version
Abstract
Objective: The development of ABCB1-mediated resistance limits the clinical efficacy of paclitaxel. Lapatinib is a small-molecule reversible tyrosine kinase and ABCB1 inhibitor that could prevent resistance. Our objective was to de-termine a recommended phase 2 dose (RP2D) of the combination of paclitax-el and lapatinib. Methods: A phase 1 dose-escalation study utilizing a Bayesian optimal interval (BOIN) design in recurrent ovarian cancer patients. Patients were pretreated with pulsed lapatinib in the 48 hours preceding weekly paclitaxel (80 mg/m2) in 28-day cycles for up to 3 cycles. We evaluated three lapatinib doses, escalating from 750 to 2,000 mg orally twice daily. Results: Sixteen patients were eligible and evaluable for efficacy and toxicity. Patients received a median of three prior therapies. Three patients were treated at dose level 1, six at dose level 2, and seven at dose level 3. There was one dose-limiting toxicity (DLT) in dose level 2 (diarrhea) and another in dose level 3 (neutropenia), with a posterior DLT estimate of 0.17, 95% credible in-terval of (0.01, 0.53) for dose level 3 based on isotonic regression. The most common grade 1-2 adverse effects were diarrhea (87.5%), leukopenia (56.3%), and anemia (50%). One (6.25%) patient had a complete response, and 7 (43.75%) patients had partial responses for an overall response rate (ORR) of 50%. The clinical responses are supported by a significant decreasing trend in CA 125 over six cycles (p=0.0001). Among the seven patients treated at the RP2D, the ORR was 71.4%. Conclusions: The combination of paclitaxel and lapatinib is safe and with an efficacy signal. The RP2D is weekly paclitaxel 80 mg/m2 combined with lapatinib 2,000 mg twice daily two days before the paclitaxel dose. This trial was registered at ClinicalTrials.gov ID: NCT04608409.
Keywords:
lapatinib
; paclitaxel
; recurrent ovarian cancer
1. Introduction
In 2025, 20,890 new cases of ovarian cancer and 12,730 deaths are estimated. Ovarian cancer encompasses histologically similar tumors that arise from the epithelial tissue of the ovary, fallopian tube, or peritoneum and is the sixth leading cause of cancer-related deaths in females [1]. Most women are diagnosed with advanced-stage disease with a 5-year survival rate of approximately 50% with minimal improvement in survival outcomes in the past decade [2].
Initial therapy for ovarian cancer includes cytoreductive surgery and platinum-based chemotherapy. However, the majority of patients will recur and become platinum-resistant. The treatment for platinum-resistant ovarian cancer often consists of a nonplatinum agent (e.g., weekly paclitaxel, pegylated liposomal doxorubicin, gemcitabine, or topotecan) administered either as a single agent or in combination with bevacizumab [3]. In recent phase 3 trials, objective response rates to single-agent nonplatinum chemotherapy in patients with platinum-resistant ovarian cancer ranged from 4 to 13% [4,5,6]. The addition of bevacizumab, as compared with chemotherapy alone, significantly improved the response rate (27.3% vs 11.8%) but without benefit in overall survival [7]. Chemotherapy-associated adverse effects, including gastrointestinal toxicity, hematological toxicity, and cumulative neuropathy, limit continued administration and contribute to the observed poor survival. Therefore, new treatment strategies are needed for recurrent ovarian cancer.
Lapatinib is a small-molecule reversible tyrosine kinase inhibitor that targets epidermal growth factor receptor (EGFR) and human epidermal growth factor receptor-2 (HER2). Lapatinib is approved for continuous oral dosing at 1,000-1,250 mg daily in combination with either an aromatase inhibitor, trastuzumab, or capecitabine in HER2-positive recurrent unresectable breast cancer [8,9,10,11]. Given that many tumors express EGFR and/or HER2, high-dose pulsed lapatinib has been evaluated in advanced solid tumors in a phase I dose escalation study of lapatinib administered as a two-day pulse prior to weekly nab-paclitaxel, demonstrating a maximum tolerated dose of 5,250 mg/day and a recommended phase 2 dose (RP2D) of 3,750 mg/day in divided doses. Dose-limiting toxicities (DLTs) included grade 3 vomiting and grade 4 neutropenia. Among 23 evaluable patients, 5 had a partial response, and another 10 experienced stable disease, suggesting the regimen was tolerable with a preliminary efficacy signal [12].
ABCB1, an ATP-binding cassette subfamily B, member 1, also known as P-glycoprotein (P-gp) or multidrug resistance protein 1 (MDR1), protects normal cells from xenobiotics and other toxic substances [13]. However, in cancer cells, overexpression of ABCB1 can result in drug resistance, especially to taxanes. Paclitaxel administration results in ABCB1 upregulation, inducing its own resistance. ABCB1 overexpression is associated with poor response to taxanes and unfavorable clinical outcomes for patients with ovarian cancer [14].
In addition to inhibiting EGFR and HER2, ABCB1 inhibition is an off-target activity of lapatinib [15,16]. Adding lapatinib to paclitaxel in paclitaxel-resistant ovarian cancer cell lines overcame taxane resistance via inhibition of ABCB1 [16]. We hypothesized the combination of weekly paclitaxel and lapatinib could prevent ABCB1 overexpression and the development of taxane resistance; therefore, we performed a phase I dose escalation study of the combination of intermittent lapatinib and weekly paclitaxel in recurrent ovarian cancer patients.
2. Patients and Methods
2.1. Study Design
This study was an open-label, single-center, single-arm, investigator-initiated phase 1 dose escalation study of the safety of lapatinib with weekly paclitaxel in patients with recurrent ovarian cancer. This trial was registered at ClinicalTrials.gov ID: NCT04608409. The study was conducted using a Bayesian optimal interval (BOIN) design. Patients were enrolled in cohorts of three with brief suspension in enrollment on the trial for evaluation of DLTs. Once DLT evaluation is complete for a cohort of patients, the next dose level is determined by available DLT information from all evaluable patients at that dose level based on the BOIN dose escalation/de-escalation rule. The study protocol and modifications were approved by the University of Kentucky Institutional Review Board MCC-20-GYN-06-PMC 8/12/2020 and were conducted in accordance with the Declaration of Helsinki, Good Clinical Practice, and all local and federal regulatory guidelines.
The primary objective of this study was to determine the RP2D of the combination of lapatinib with weekly paclitaxel. Secondary objectives include determining adverse events of the combination of lapatinib and paclitaxel, assessing the plasma concentration of lapatinib, and assessing the proportion of patients with clinical benefit defined as clinical progression-free survival (PFS) at one year from the start of study therapy. Exploratory objectives include the evaluation of ABCB1 expression in cell-free RNA blood samples.
2.2. Patient Population
Patients with histologically or cytologically confirmed ovarian cancer who recurred within 12 months after platinum-based chemotherapy, age ≥ 18 years, ECOG performance status ≤ 2, and with adequate organ and marrow function at baseline were eligible for enrollment. Patients with prior or concurrent malignancy whose natural history does not have the potential to interfere with the safety or efficacy of the investigational regimen were also eligible. Patients with a history of hypersensitivity to lapatinib or paclitaxel or uncontrolled intercurrent illness were ineligible for enrollment. Additionally, patients with a malabsorption syndrome, left ventricular ejection fraction < 50%, active HIV, hepatitis B, and hepatitis C with detectable viral load, and patients with baseline > grade 1 neuropathy were not eligible. Patients on medications that are strong inhibitors or inducers of CYP 450 3A4 were ineligible unless transitioned off prior to study initiation.
2.3. Treatment Plan
The cycle length was 28 days. On days 1, 8, and 15, patients received a fixed dose of paclitaxel 80 mg/m2 intravenously. On days 6-7 and 13-14, oral lapatinib was self-administered twice a day. In dose level one, lapatinib 750 mg was administered twice daily and was escalated with three patients per cohort to dose level two, lapatinib 1,500 mg twice daily, and dose level three, lapatinib 2,000 mg twice daily. After cycle one, patients were continued on the combination of lapatinib and paclitaxel for an additional two cycles. Patients could then continue on weekly paclitaxel as a single agent.
2.4. Assessments
All patients who received at least one dose of study treatment were evaluated for toxicity. Toxicity was graded by the Common Terminology Criteria for Adverse Events version 5. DLT was assessed after the first cycle of treatment. Patients who completed 75% of doses were evaluable for DLTs. DLT was defined by grade 3 febrile neutropenia, grade 4 neutropenia, grade 4 thrombocytopenia, grade 4 anemia not explained by underlying disease, ≥ grade 3 nausea, vomiting, or diarrhea that persisted > 72 hours despite optimal supportive management, or any ≥ grade 3 adverse event or any ≥ grade 2 adverse event not improved after stopping the drug combination. The response was assessed by their treating physician in patients who received at least one cycle of treatment by standard-of-care clinical assessments, which were performed after three cycles of a combination of lapatinib and paclitaxel. Blood samples were collected on days 1, 8, and 15 of each cycle for analysis of lapatinib concentrations and ABCB1 expression using cell-free RNA.
2.5. Statistical Methods
DLT rate is calculated as the total number of patients experiencing DLTs at the current dose level divided by the total number of patients treated at the current dose level. A target DLT toxicity rate was set to be 30% for the study. Dose escalation and de-escalation decisions were determined by all evaluable patients at the current dose level using BOIN dose escalation/de-escalation rule. The study was planned to enroll a maximum of 15 patients. The RP2D was determined by isotonic regression to pool information across all dose levels.
Patient characteristics, antitumor activity of the drug combination, and safety and tolerability of lapatinib were summarized using descriptive statistics. Clinical benefit rate was defined as the proportion of patients with clinical progression-free survival (PFS) at one year defined as the time from start of protocol to time of progression of disease or death, whichever occurred first.
Changes in lapatinib levels from baseline throughout the treatment period were represented by longitudinal profiles and analyzed by a mixed effects model. Changes in ABCB1 RNA expression were compared pre- and post-paclitaxel administration.
2.6. Plasma Drug Concentrations
Plasma lapatinib concentrations were analyzed among samples from patients who completed dosing for the assigned treatment arm and had blood drawn within 24 hours of the last lapatinib dose. The concentration of lapatinib was measured in plasma samples using a 1260 Infinity II LC system interfaced with an Ultivo triple quadrupole mass spectrometer (LC/MSMS) (Agilent Technologies). Stock solutions of lapatinib (1 mg/mL) and lapatinib-d7 (1 mg/mL) were prepared in methanol. Assay calibration was performed for lapatinib using solutions prepared in blank human peripheral blood plasma (StemCell Technologies) at concentrations ranging from 25–10000 ng/mL, and calibration curves were linear (R2 > 0.999). The lower limit of quantitation was 100 ng/mL, and the upper limit of quantitation was 10000 ng/mL. Quality controls of 200 and 5000 ng/mL were included with each run.
Each patient specimen, standard, and quality control sample was combined with three parts acetonitrile containing lapatinib-d7 (50 ng/mL). The tubes were vortexed for 0.5 minutes and then centrifuged for 10 minutes at 15,000xg. Supernatants were transferred to multi-well plates and dried under a stream of nitrogen gas at 40oC. The dried sample was resuspended in a 1:1 mixture of 10mM ammonium acetate (pH 4.5) + 0.1% formic acid and acetonitrile + 0.1% formic acid, placed on an orbital shaker for 10 minutes at 750 rpm and loaded into the autosampler.
Liquid chromatography was performed using an Agilent InfinityLab Poroshell 120 PFP column (50 mm × 2.1 mm, 2.7 μm) equipped with a guard column. The mobile phase consisted of (A) 10mM ammonium acetate (pH 4.5) + 0.1% formic acid and (B) acetonitrile + 0.1% formic acid delivered at 0.3 mL/minute as a linear gradient as follows: 0-2.5 minutes, 30% to 95% B; 2.5-3.5 minutes, 95% to 100% B; 3.5-4.0 minutes, 100% B; 4.0-4.5 minutes, 100% to 30% B. A 5-minute re-equilibration occurred before the injection of the next sample. Electrospray ionization was operated in positive mode (ESI+) with nitrogen as both curtain and collision gas. The Ultivo instrument parameters were drying gas temperature 250oC, drying gas flow 11 L/minute, sheath gas temperature 400oC, sheath gas flow 11.0 L/minute, and nebulizer 50 psi. MRM detected the transitions of lapatinib at m/z 581.1 → 365.1 (fragmentor voltage 190 V; collision energy 41 V). Data was analyzed using MassHunter Workstation (Agilent Technologies) software.
2.7. Plasma CA125 Concentrations
Patients blood was draw and processed at the University of Kentucky HealthCare Laboratory to determine serum CA125 concentrations.
3. Results
3.1. Patient Characteristics
Between March 2021 and May 2023, 19 women with ovarian cancer were enrolled on the study. Two patients were subsequently determined to be ineligible; the first patient had leukocytosis and anemia, and the second patient developed uncontrolled intercurrent infection and leukocytosis prior to starting study therapy. A third patient withdrew consent from the study (Figure 1). Sixteen patients were evaluable for efficacy, toxicity, and response. The median age was 66; fifteen subjects had high-grade serous histology, and one had endometrioid histology. The median number of prior lines of systemic therapy was 3 (range 1-7). The median platinum-free interval for this cohort was 4 months (range 1-9 months). All sixteen patients received paclitaxel in the primary setting, and seven received prior bevacizumab (Supplementary Table S1).
3.2. Safety and Tolerability
The majority of adverse events in all the patients receiving lapatinib and paclitaxel were mild to moderate in severity (Table 1 and Supplementary Table S2.). Diarrhea (n=14, 87.5%) was the most common adverse event. Other non-hematological toxicities included hypokalemia (n=9, 56.3%), hypocalcemia (n=8, 50%), and hyponatremia (n=8, 50%). The grade 3/4 non-hematological toxicities included diarrhea (n=3, 18.8%), hypokalemia (n=2, 12.5%), acute kidney injury (n=2, 12.5%), and hyponatremia (n=1, 6.3%). The most common hematological toxicities were leukopenia (n=9; 56.3%) and anemia (n=8; 50%). One patient with a history of prior PARP inhibitor use went off the study after developing a secondary malignancy, which was attributed to prior PARP therapy and determined to be unrelated to the study treatment.
There were two DLTs observed, one for diarrhea and one for neutropenia. One DLT was observed in a subject on dose level 2, and one DLT occurred in a subject treated on dose level 3, with a posterior DLT estimate of 0.17, 95% credible interval of (0.01, 0.53) for dose level 3. Therefore, the RP2D is 80 mg/m2 of weekly paclitaxel combined with 2,000 mg bid of lapatinib administered two days before the paclitaxel dose. The estimated posterior DLT rate yielded a credible interval of (0.01, 0.53) for both dose level 2 and dose level 3. Following isotonic regression analysis of pooled data from 15 patients across all dose levels, dose level 3 was identified as the recommended maximum tolerated dose (MTD).
3.3. Efficacy
The median number of cycles of paclitaxel and lapatinib was three (range 1-3), and the median total cycles given, including weeklypaclitaxel alone was 5.5 (range 1-8). At the time of data cut-off, all sixteen patients were off treatment. One (6.25%) patient had a complete response (CR), and seven (43.75%) had partial responses (PR) for an overall response rate (ORR) of 50%. Two (12.5%) had stable disease (SD) (Figure 2). At dose level 1, only one patient had SD, while three patients achieved a PR at dose level 2. Among the seven patients treated at dose level 3, one patient had a CR, four experienced a PR, and one had a SD for an ORR of 71.4%. Of 16 patients, one patient had endometrioid histology and 15 patients with high-grade serous histology; however, all responses (n=10) were reported among patients with high-grade serous histology (Supplementary Figure S1). These responses are supported by a significant decreasing trend in CA 125 values over six cycles (p=0.0001) (Figure 3). Fifteen progression events occurred at the time of data cut-off, and the median PFS was 5.0 months (95% CI: 3.13-6.07) (Figure 4). Six patient deaths were recorded, and the median OS was 7.7 months (95% CI: 5.9-NE) (Figure 5).
3.4. Plasma Lapatinib Concentrations
Twice daily lapatinib dosing on days 6, 7, 13, and 14 aimed to achieve a therapeutic concentration of 2,000 ng/mL at the time of paclitaxel dosing. Plasma lapatinib concentrations were evaluated in patients on days 8 (192 hours) and 15 (360 hours) of each treatment cycle, prior to paclitaxel administration, using a validated LC/MS assay (Figure 5; Supplementary Table S3). The plasma concentrations were highly variable, ranging from 1439–2579 ng/mL for dose level 1, 1031–3393 ng/mL for dose level 2, and 1824–2951 ng/mL for dose level 3. No statistically significant intercycle or intracycle differences were observed.
Plasma lapatinib concentrations reached 2,000 ng/mL in at least one cycle for 67% of patients in dose level 1, 60% in dose level 2, and 50% in dose level 3. The target threshold was achieved in all three cycles for 33% of patients in dose level 1, 20% in dose level 2, and 50% in dose level 3. Patients were categorized as achieving lapatinib plasma concentrations greater or less than 2,000 ng/mL. Among six patients with lapatinib concentrations less than 2,000 ng/mL the ORR was 67% (1 CR, 3 PR) and all reported best responses (1 CR, 2 SD, and 3 PR). Among 10 patients who had lapatinib plasma concentration greater than 2,000 ng/mL, four patients achieved a PR for an ORR of 40% (Supplementary Figure S2).
4. Discussion
This is the first study to report the combination of weekly paclitaxel with pulsed lapatinib in ovarian cancer. The RP2D is 80 mg/m2 of weekly paclitaxel combined with 2,000 mg twice daily of lapatinib given as a pulsed pretreatment two days before the paclitaxel dose. This was the maximum dose planned for this study due to pill burden and anticipated toxicity. This dose is lower than a prior phase I clinical study conducted in patients with advanced solid tumors which defined the MTD of lapatinib as 2,625 mg twice daily dosing as a two-day pulse prior to weekly infusion of nab-paclitaxel, which demonstrated a grade 3-4 rate of febrile neutropenia of 32%. This prior phase I study included up to six dose levels with the highest lapatinib dose 7,500 mg daily. The majority of the patients included had lung (9/25), esophageal (3/25), and prostate cancers (3/25); one ovarian cancer patient was included. The grading of diarrhea was in the setting of maximal supportive antidiarrheal medication [12].
We observed two DLTs, one for diarrhea and one for neutropenia, which is similar to the prior study where dose limiting toxicities were vomiting and neutropenia. The prior study also reported a higher incidence of grade 1-2 diarrhea than continuous dosing schedules of lapatinib that was manageable with anti-diarrheal medication [12]. In our study, any grade diarrhea was the most common AE at 87.5%, which was manageable with antidiarrheals. Other studies have reported diarrhea rates as high as 83-100% [17,18]. The incidence of rash with lapatinib ranges from 25-64% and is typically grade 1 or grade 2 and either resolves without treatment or improves with topical steroid use [12,18,19]. In our study three (18.8%) patients reported maculopapular rash. Neuropathy is common and grade 2-3 neutropenia occurs in 4-23% of patients receiving weeklypaclitaxel [20,21]. Our study findings of leukopenia are consistent with expected effects of weekly paclitaxel.
Though prior phase II study showed minimal activity of single-agent lapatinib in recurrent ovarian cancer, [22] there was encouraging anticancer activity of the combination. Among the seven patients treated at the RP2D, one patient had a CR, four experienced a PR, and one had SD for an ORR of 71.4%. Despite patients receiving only three cycles of lapatinib in combination with paclitaxel, these results are an improvement from the expected ORR of 20.9% with single agent weekly paclitaxel in platinum-resistant ovarian cancer patients [20]. In addition, the study population was heavily pre-treated, receiving a median of three prior lines of systemic therapy. A prior phase II study published in 2012 failed to demonstrate a clinical benefit of lapatinib 1250 mg daily orally in combination with topotecan 3.2 mg/m IV on days 1, 8, and 15 after first recurrence; [23] this study evaluated daily dosing of lapatinib, which is different than the pulsed dosage used in this study. Recently the development of antibody-drug conjugate mirvetuximab soravantansine has altered the treatment paradigms in platinum-resistant ovarian cancer for those with tumors who are folate receptor α positive. The MIRAOL study demonstrated improved overall survival with mirvetuximab than chemotherapy (median 16.46 months vs. 12.75 months; HR for death 0.67; 95% CI (0.50-0.89) in patients who are folate receptor α positive [24]. In the earlier SORAYA trial, over half of the patients screened were found to be folate receptor α negative and ineligible for treatment, demonstrating the ongoing need for treatments in ovarian cancer patients without targetable mutations [25].
The target therapeutic concentration of lapatinib of 2,000 ng/mL at time of paclitaxel dosing was achieved in all three cycles for 33% of patients in dose level 1, 20% in dose level 2 and 50% in dose level 3, suggesting a lack of a linear dose response with pulsed dosing. Interestingly, plasma concentration did not predict response. The ORR was 67% among subjects with lapatinib concentrations less than 2,000 ng/mL compared to 40% for those with plasma concentrations greater than 2000 ng/mL. The lack of prognostic power is likely influenced by the high degree of variability observed in plasma lapatinib concentrations. A number of factors may have contributed to this variability, including small sample size, variable plasma sampling times and dose reductions.
Strengths of the study include BOIN design, enrollment of patients with predominantly high grade serous ovarian cancer histology, long-term follow up data, and pharmacokinetic analysis to assess whether therapeutic concentrations of lapatinib were achieved. Limitations of this study include small cohort size without backfilled cohorts, a single institution and limited patient diversity that may limit generalizability of the findings. A limitation of this study is the treating physician assessed efficacy, although this is common in phase 1 trials where efficacy is not the primary endpoint. This study did not evaluate for HER2 markers and this is an area of future investigation. In addition, patients only received three cycles of lapatinib in combination with weekly paclitaxel, limiting assessment of outcomes if lapatinib were continued.
5. Conclusions
In conclusion, combination of weekly paclitaxel with high-dose pulsed lapatinib demonstrated encouraging clinical anticancer activity in heavily pre-treated, recurrent ovarian cancer patients. This combination warrants further exploration in ovarian cancer.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
JMK and FRU were involved in conceptualization. CDC and JRM prepared the original draft. DY and RJ performed the formal statistical analysis. JRM and HSE were involved in data curation and tested patient plasma for lapatinib concentration. All authors reviewed, edited, and approved final manuscript. Correspondence should be addressed to JMK.
Funding
This research was supported by Markey Cancer Center Cancer Center Support Grant, supplemental funding from Markey IIT Executive Steering Committee, and NCI T32 CA160003. This research was also supported by the Biospecimen procurement and Translational Pathology, and Biostatistics and Bioinformatics Shared Resources of the University of Kentucky Markey Cancer Center (P30CA177558).
Institutional Review Board Statement
The study protocol and modifications were approved by the University of Kentucky Institutional Review Board MCC-20-GYN-06-PMC 8/12/2020 and were conducted in accordance with the Declaration of Helsinki, Good Clinical Practice, and all local and federal regulatory guidelines.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to informed consent restrictions.
Conflicts of Interest
Jill Kolesar is a founder and owner of VesiCure Technologies. Jill Kolesar is the founder and owner of Helix Diagnostics. Jill Kolesar received grant support to the institution from ArtemiLife and LOXO@Lilly. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. All other authors declare no conflicts of interest.
References
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA: A Cancer J. Clin. 2025, 75, 10–45. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA: a cancer journal for clinicians 2024, 74, 12–49. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guideline in Oncology, Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer. Version 1.2020—March 11, 2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf (accessed on).
- Gaillard, S.; Oaknin, A.; Ray-Coquard, I.; Vergote, I.; Scambia, G.; Colombo, N.; Fernandez, C.; Alfaro, V.; Kahatt, C.; Nieto, A.; et al. Lurbinectedin versus pegylated liposomal doxorubicin or topotecan in patients with platinum-resistant ovarian cancer: A multicenter, randomized, controlled, open-label phase 3 study (CORAIL). Gynecol. Oncol. 2021, 163, 237–245. [Google Scholar] [CrossRef]
- Hamanishi, J.; Takeshima, N.; Katsumata, N.; Ushijima, K.; Kimura, T.; Takeuchi, S.; Matsumoto, K.; Ito, K.; Mandai, M.; Nakai, H.; et al. Nivolumab Versus Gemcitabine or Pegylated Liposomal Doxorubicin for Patients With Platinum-Resistant Ovarian Cancer: Open-Label, Randomized Trial in Japan (NINJA). J. Clin. Oncol. 2021, 39, 3671–3681. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Fujiwara, K.; A Ledermann, J.; Oza, A.M.; Kristeleit, R.; Ray-Coquard, I.-L.; E Richardson, G.; Sessa, C.; Yonemori, K.; Banerjee, S.; et al. Avelumab alone or in combination with chemotherapy versus chemotherapy alone in platinum-resistant or platinum-refractory ovarian cancer (JAVELIN Ovarian 200): an open-label, three-arm, randomised, phase 3 study. Lancet Oncol. 2021, 22, 1034–1046. [Google Scholar] [CrossRef] [PubMed]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab Combined With Chemotherapy for Platinum-Resistant Recurrent Ovarian Cancer: The AURELIA Open-Label Randomized Phase III Trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Geyer, C.E.; Forster, J.; Lindquist, D.; Chan, S.; Romieu, C.G.; Pienkowski, T.; Jagiello-Gruszfeld, A.; Crown, J.; Chan, A.; Kaufman, B.; et al. Lapatinib plus Capecitabine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2006, 355, 2733–2743. [Google Scholar] [CrossRef]
- Blackwell, K.L.; Burstein, H.J.; Storniolo, A.M.; Rugo, H.; Sledge, G.; Koehler, M.; Ellis, C.; Casey, M.; Vukelja, S.; Bischoff, J.; et al. Randomized Study of Lapatinib Alone or in Combination With Trastuzumab in Women With ErbB2-Positive, Trastuzumab-Refractory Metastatic Breast Cancer. J. Clin. Oncol. 2010, 28, 1124–1130. [Google Scholar] [CrossRef]
- Guan, Z.; Xu, B.; DeSilvio, M.L.; Shen, Z.; Arpornwirat, W.; Tong, Z.; Lorvidhaya, V.; Jiang, Z.; Yang, J.; Makhson, A.; et al. Randomized Trial of Lapatinib Versus Placebo Added to Paclitaxel in the Treatment of Human Epidermal Growth Factor Receptor 2–Overexpressing Metastatic Breast Cancer. J. Clin. Oncol. 2013, 31, 1947–1953. [Google Scholar] [CrossRef]
- Di Leo, A.; Gomez, H.L.; Aziz, Z.; Zvirbule, Z.; Bines, J.; Arbushites, M.C.; Guerrera, S.F.; Koehler, M.; Oliva, C.; Stein, S.H.; et al. Phase III, Double-Blind, Randomized Study Comparing Lapatinib Plus Paclitaxel With Placebo Plus Paclitaxel As First-Line Treatment for Metastatic Breast Cancer. J. Clin. Oncol. 2008, 26, 5544–5552. [Google Scholar] [CrossRef]
- Chien, A.J.; Illi, J.A.; Ko, A.H.; Korn, W.M.; Fong, L.; Chen, L.-M.; Kashani-Sabet, M.; Ryan, C.J.; Rosenberg, J.E.; Dubey, S.; et al. A Phase I Study of a 2-Day Lapatinib Chemosensitization Pulse Preceding Nanoparticle Albumin-Bound Paclitaxel for Advanced Solid Malignancies. Clin. Cancer Res. 2009, 15, 5569–5575. [Google Scholar] [CrossRef] [PubMed]
- Nanayakkara, A.K.; Follit, C.A.; Chen, G.; Williams, N.S.; Vogel, P.D.; Wise, J.G. Targeted inhibitors of P-glycoprotein increase chemotherapeutic-induced mortality of multidrug resistant tumor cells. Sci. Rep. 2018, 8, 1–18. [Google Scholar] [CrossRef]
- Penson, R.T.; Oliva, E.; Skates, S.J.; Glyptis, T.; Fuller, A.F.; Goodman, A.; Seiden, M.V. Expression of multidrug resistance-1 protein inversely correlates with paclitaxel response and survival in ovarian cancer patients: a study in serial samples. Gynecol. Oncol. 2004, 93, 98–106. [Google Scholar] [CrossRef]
- Moasser, M.M.; Wilmes, L.J.; Wong, C.H.; Aliu, S.; Li, K.-L.; Wang, D.; Hom, Y.K.; Hann, B.; Hylton, N.M. Improved tumor vascular function following high-dose epidermal growth factor receptor tyrosine kinase inhibitor therapy. J. Magn. Reson. Imaging 2007, 26, 1618–1625. [Google Scholar] [CrossRef]
- McCorkle, J.R.; Gorski, J.W.; Liu, J.; Riggs, M.B.; McDowell, A.B.; Lin, N.; Wang, C.; Ueland, F.R.; Kolesar, J.M. Lapatinib and poziotinib overcome ABCB1-mediated paclitaxel resistance in ovarian cancer. PLOS ONE 2021, 16, e0254205. [Google Scholar] [CrossRef]
- Morikawa, A.; de Stanchina, E.; Pentsova, E.; Kemeny, M.M.; Li, B.T.; Tang, K.; Patil, S.; Fleisher, M.; Van Poznak, C.; Norton, L.; et al. Phase I Study of Intermittent High-Dose Lapatinib Alternating with Capecitabine for HER2-Positive Breast Cancer Patients with Central Nervous System Metastases. Clin. Cancer Res. 2019, 25, 3784–3792. [Google Scholar] [CrossRef]
- Yu, A.; Faiq, N.; Green, S.; Lai, A.; Green, R.; Hu, J.; Cloughesy, T.F.; Mellinghoff, I.; Nghiemphu, P.L. Report of safety of pulse dosing of lapatinib with temozolomide and radiation therapy for newly-diagnosed glioblastoma in a pilot phase II study. J. Neuro-Oncology 2017, 134, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Burris, H.A.; Hurwitz, H.I.; Dees, E.C.; Dowlati, A.; Blackwell, K.L.; O’NEil, B.; Marcom, P.K.; Ellis, M.J.; Overmoyer, B.; Jones, S.F.; et al. Phase I Safety, Pharmacokinetics, and Clinical Activity Study of Lapatinib (GW572016), a Reversible Dual Inhibitor of Epidermal Growth Factor Receptor Tyrosine Kinases, in Heavily Pretreated Patients With Metastatic Carcinomas. J. Clin. Oncol. 2005, 23, 5305–5313. [Google Scholar] [CrossRef]
- Markman, M.; Blessing, J.; Rubin, S.C.; Connor, J.; Hanjani, P.; Waggoner, S. Phase II trial of weekly paclitaxel (80 mg/m2) in platinum and paclitaxel-resistant ovarian and primary peritoneal cancers: A Gynecologic Oncology Group study. Gynecol. Oncol. 2006, 101, 436–440. [Google Scholar] [CrossRef]
- Markman, M.; Hall, J.; Spitz, D.; Weiner, S.; Carson, L.; Van Le, L.; Baker, M. Phase II Trial of Weekly Single-Agent Paclitaxel in Platinum/Paclitaxel-Refractory Ovarian Cancer. J. Clin. Oncol. 2002, 20, 2365–2369. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.A.; Sill, M.W.; Lankes, H.A.; Godwin, A.K.; Mannel, R.S.; Armstrong, D.K.; Carolla, R.L.; Liepman, M.K.; Spirtos, N.M.; Fischer, E.G.; et al. A phase II evaluation of lapatinib in the treatment of persistent or recurrent epithelial ovarian or primary peritoneal carcinoma: A gynecologic oncology group study. Gynecol. Oncol. 2012, 124, 569–574. [Google Scholar] [CrossRef]
- Lheureux, S.; Krieger, S.; Weber, B.; Pautier, P.; Fabbro, M.; Selle, F.; Bourgeois, H.; Petit, T.; Lortholary, A.; Plantade, A.; et al. Expected Benefits of Topotecan Combined With Lapatinib in Recurrent Ovarian Cancer According to Biological Profile. Int. J. Gynecol. Cancer 2012, 22, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.N.; Angelergues, A.; Konecny, G.E.; García, Y.; Banerjee, S.; Lorusso, D.; Lee, J.-Y.; Moroney, J.W.; Colombo, N.; Roszak, A.; et al. Mirvetuximab Soravtansine in FRα-Positive, Platinum-Resistant Ovarian Cancer. New Engl. J. Med. 2023, 389, 2162–2174. [Google Scholar] [CrossRef] [PubMed]
- Matulonis, U.A.; Lorusso, D.; Oaknin, A.; Pignata, S.; Dean, A.; Denys, H.; Colombo, N.; Van Gorp, T.; Konner, J.A.; Marin, M.R.; et al. Efficacy and Safety of Mirvetuximab Soravtansine in Patients With Platinum-Resistant Ovarian Cancer With High Folate Receptor Alpha Expression: Results From the SORAYA Study. J. Clin. Oncol. 2023, 41, 2436–2445. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Trial diagram.
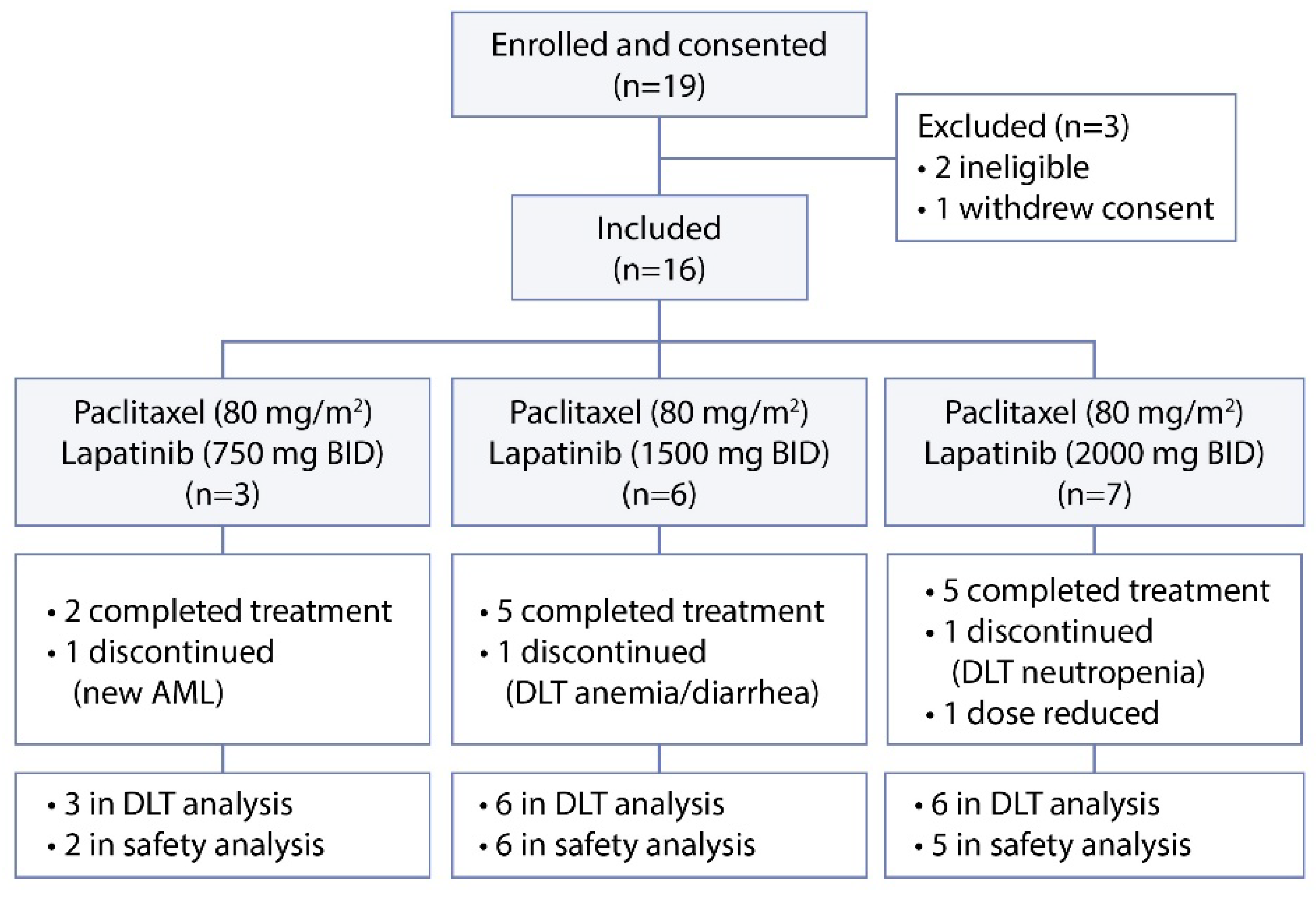
Figure 2.
Best responses by dose level.
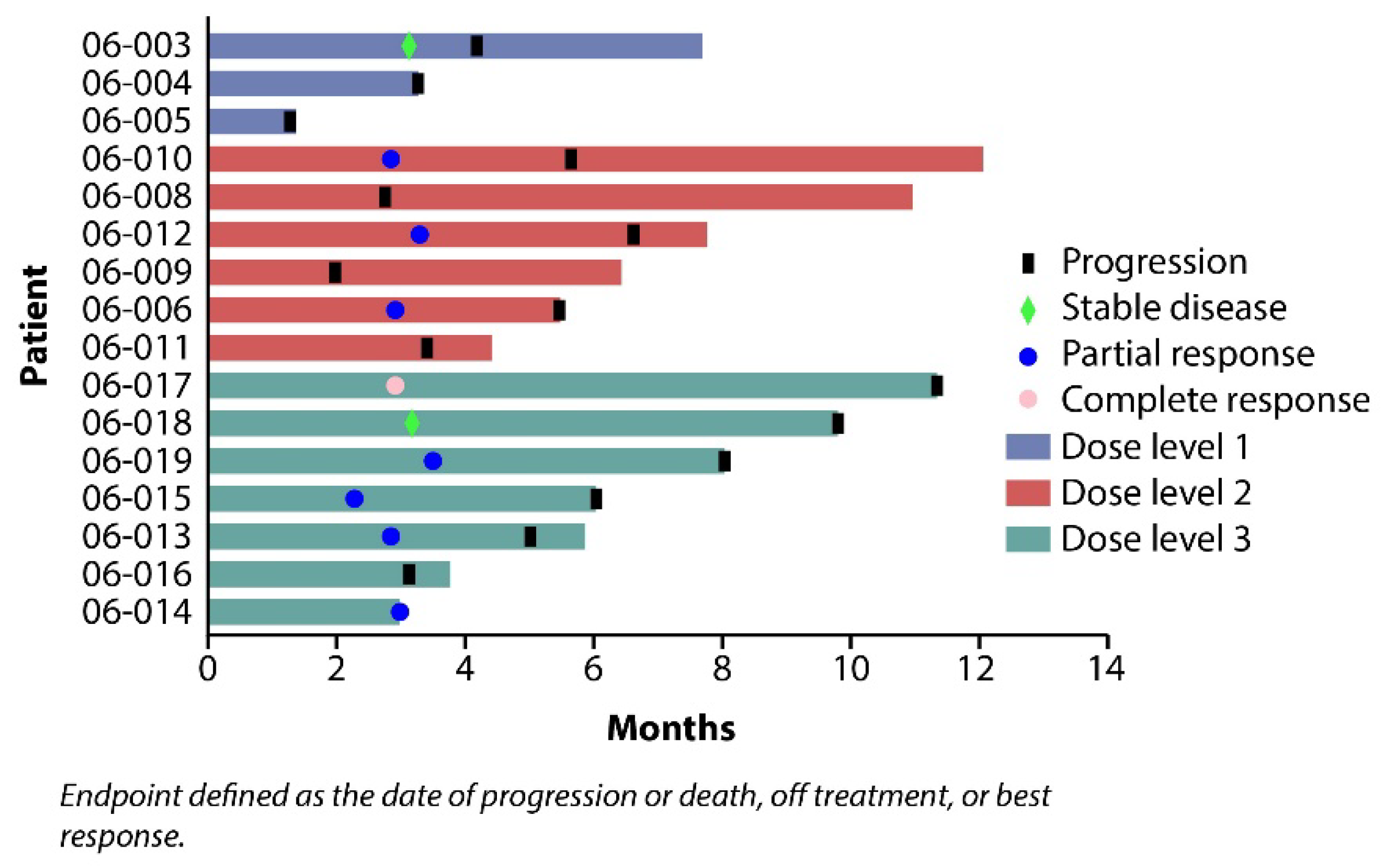
Figure 3.
CA125 trend with each treatment cycle separated by individual patients (numbers represent last two digits of patient number) (A). Cohort average (bars indicate standard error) (B.).
Figure 3.
CA125 trend with each treatment cycle separated by individual patients (numbers represent last two digits of patient number) (A). Cohort average (bars indicate standard error) (B.).
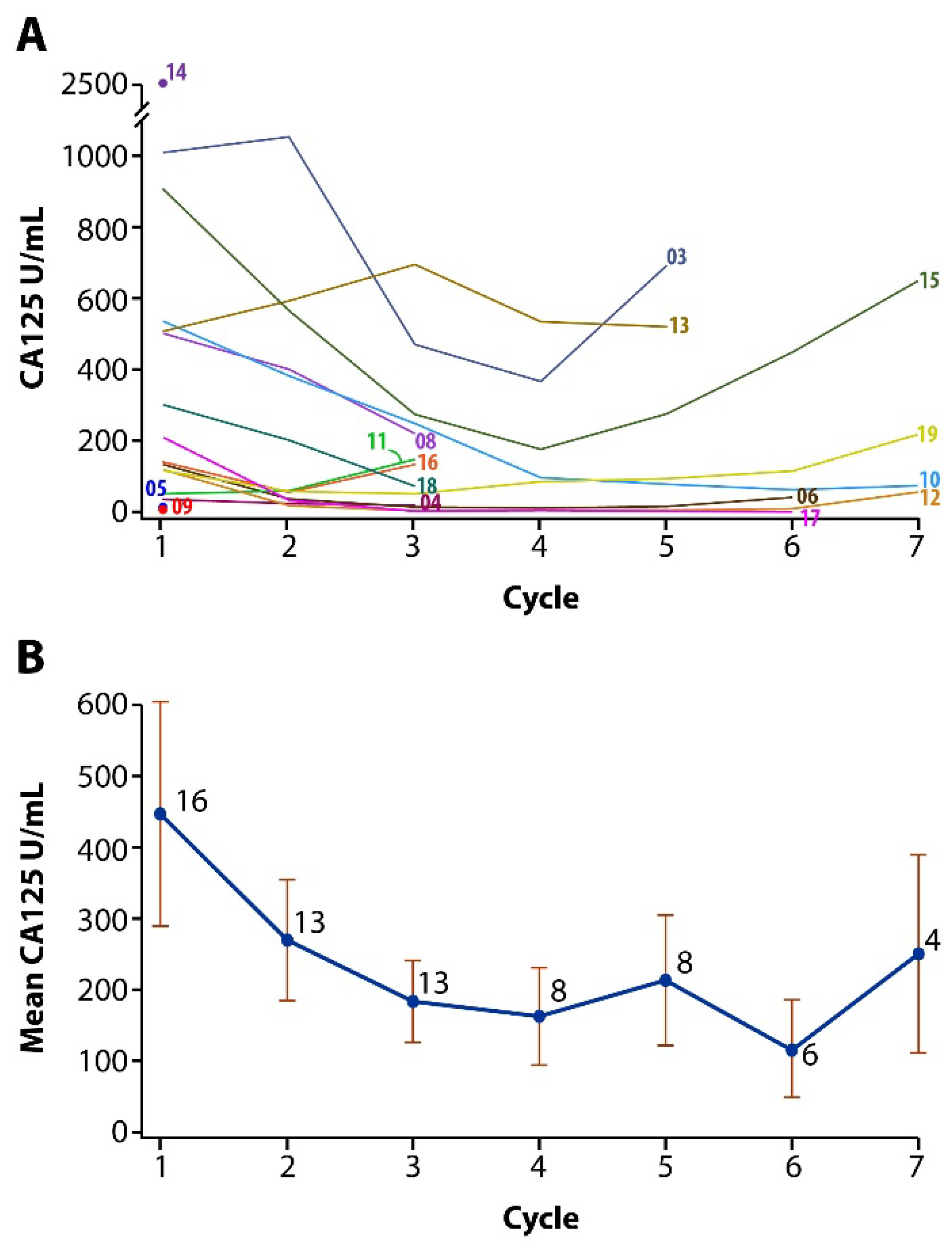
Figure 4.
Kaplan–Meier survival plots. (A) Progression-free survival. (B) Overall survival.
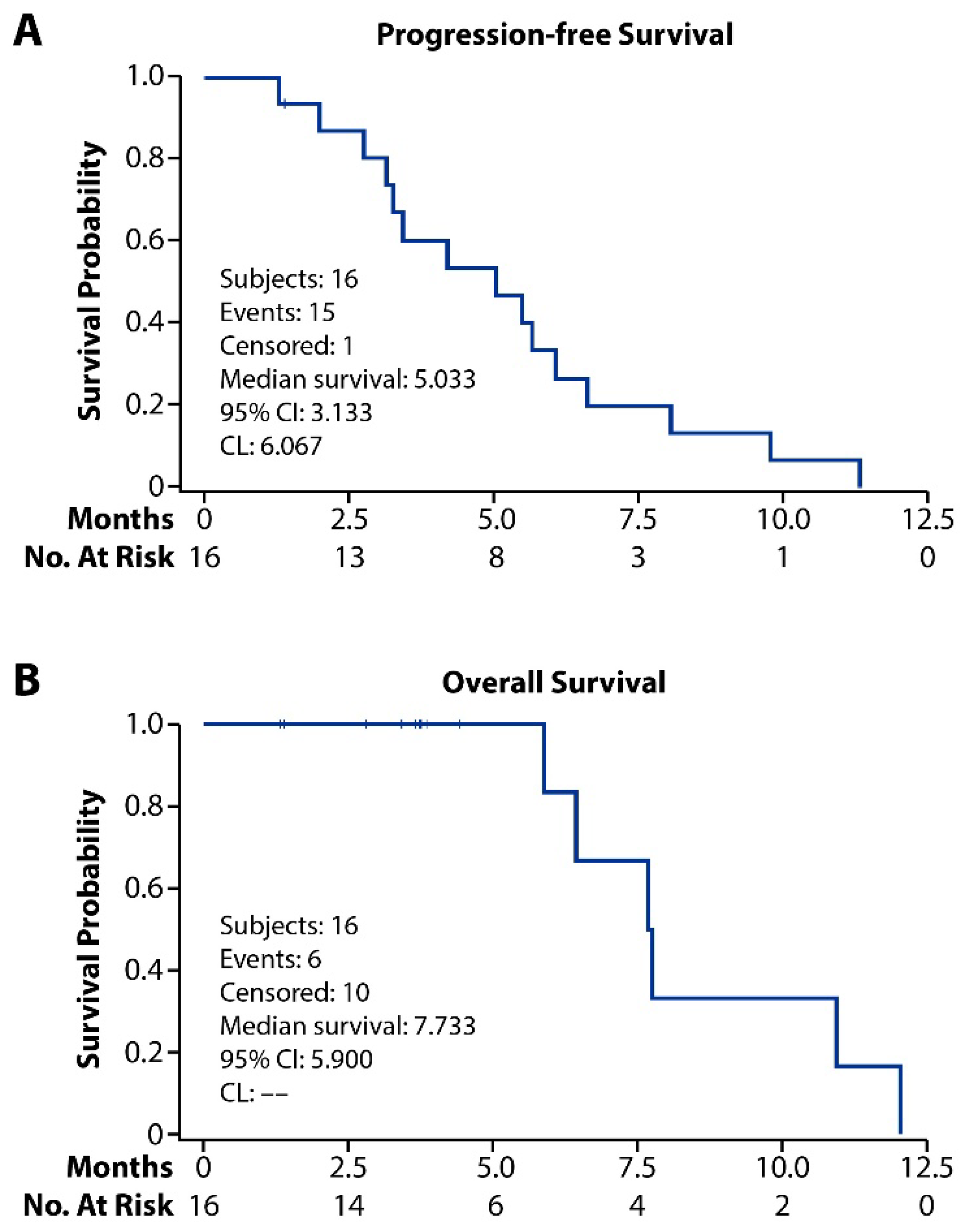
Figure 5.
Plasma lapatinib concentrations among enrolled subjects. Concentrations were measured prior to paclitaxel administration following 2 days of BID dosing during Cycles 1–3. The target lapatinib plasma concentration at the time of paclitaxel administration (day 8 and day 15) was 2000 ng/mL (dashed line). Mean values (diamonds) ± standard deviation for each dose level are shown. Timing of lapatinib (brown arrows) and paclitaxel (blue arrows) doses are depicted along the x-axis. Numbers of patients reaching target plasma concentration in at least 1, 2, or all 3 cycles are summarized in the adjoining table.
Figure 5.
Plasma lapatinib concentrations among enrolled subjects. Concentrations were measured prior to paclitaxel administration following 2 days of BID dosing during Cycles 1–3. The target lapatinib plasma concentration at the time of paclitaxel administration (day 8 and day 15) was 2000 ng/mL (dashed line). Mean values (diamonds) ± standard deviation for each dose level are shown. Timing of lapatinib (brown arrows) and paclitaxel (blue arrows) doses are depicted along the x-axis. Numbers of patients reaching target plasma concentration in at least 1, 2, or all 3 cycles are summarized in the adjoining table.
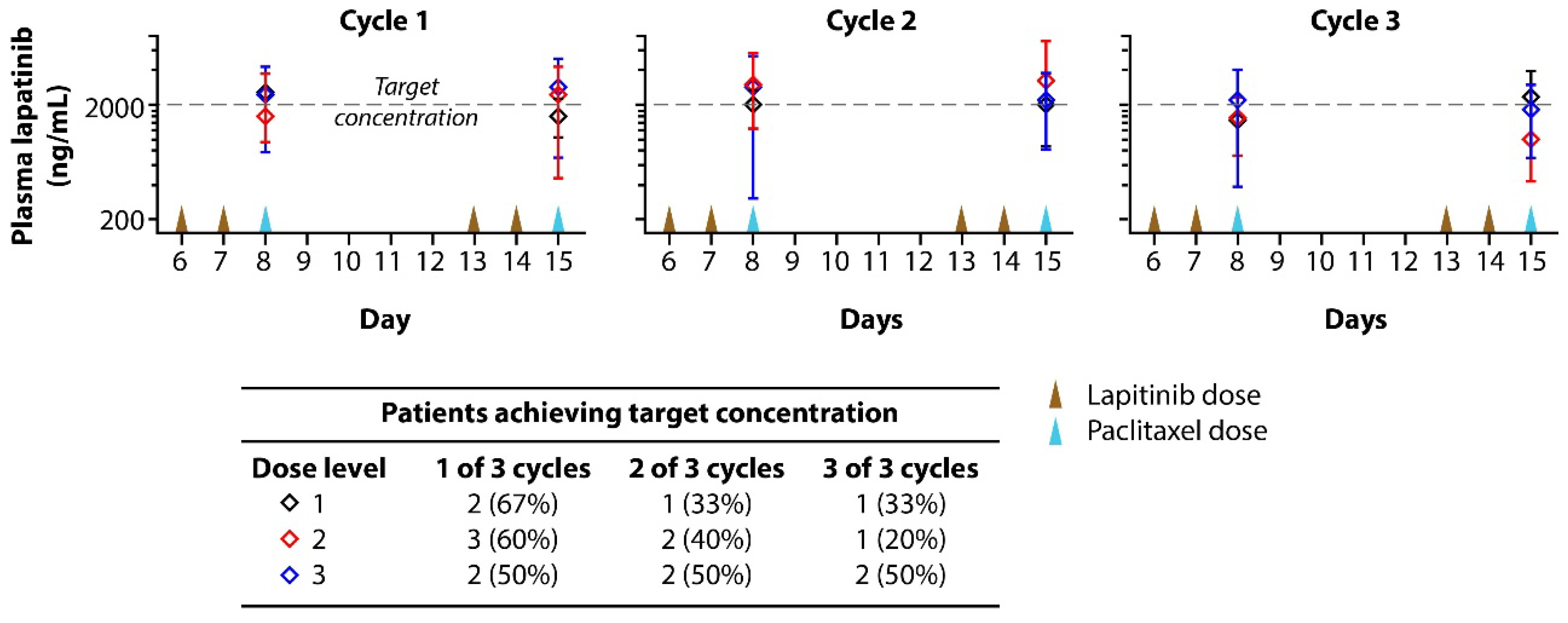

Table 1.
Adverse Events Grade 3/4 versus Any Grade.
| TOTAL N = 16 |
||
|---|---|---|
| Toxicity N (%) | GRADE 3 / 4 | ANY GRADE |
| Hematological toxicity | ||
| Anemia | 1 (6.3) | 8 (50.0) |
| Thrombocytopenia | 1 (6.3) | 3 (18.8) |
| Leukopenia | 1 (6.3) | 9 (56.3) |
| Non-hematological toxicity | ||
| Alanine aminotransferase increased | 0 (0) | 3 (18.8) |
| Aspartate aminotransferase increased | 0 (0) | 4 (25.0) |
| Creatinine increased | 2 (12.5) | 6 (37.5) |
| Abdominal pain | 0 (0) | 2 (12.5) |
| Constipation | 0 (0) | 2 (12.5) |
| Diarrhea | 3 (18.8) | 14 (87.5) |
| Nausea | 0 (0) | 4 (25.0) |
| Fatigue | 0 (0) | 3 (18.8) |
| Hyperkalemia | 0 (0) | 4 (25.0) |
| Hyperphosphatemia | 0 (0) | 2 (12.5) |
| Hypercalcemia | 0 (0) | 4 (25.0) |
| Hyponatremia | 1 (6.3) | 8 (50.0) |
| Hypokalemia | 2 (12.5) | 9 (56.3) |
| Hypophosphatemia | 0 (0.0) | 3 (18.8) |
| Hypocalcemia | 0 (0) | 8 (50.0) |
| Hypomagnesemia | 0 (0) | 7 (43.8) |
| Hypoalbuminemia | 0 (0) | 4 (25.0) |
| Back pain | 0 (0) | 3 (18.8) |
| Muscle cramp | 0 (0) | 2 (12.5) |
| Peripheral sensory neuropathy | 0 (0) | 2 (12.5) |
| Dyspnea | 0 (0) | 4 (25.0) |
| Alopecia | 0 (0) | 2 (12.5) |
| Rash maculo-papular | 0 (0) | 3 (18.8) |
Note: A subject is counted only once within a toxicity or a toxicity category. The toxicity with the highest grade is chosen when there are multiple toxicities with different grades for one subject. All percentages are based on the number of subjects in the safety population.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



