
Submitted:
14 January 2026
Posted:
15 January 2026
You are already at the latest version
Abstract
Background/Objectives: Obesity and type 2 diabetes are increasingly common among patients undergoing hip and knee arthroplasty and are associated with higher risks of prosthetic joint infection, impaired wound healing, and prolonged hospitalization. Dietary carbohydrate restriction has demonstrated benefits in glycemic control and weight reduction, but its feasibility and safety in the perioperative arthroplasty population remain underexplored. This pilot study evaluated the safety, feasibility, and short-term metabolic effects of a low-carbohydrate diet supported by WhatsApp-based meal photo-logging in patients undergoing total hip or knee arthroplasty. Methods: A retrospective cohort analysis was performed on 43 patients enrolled in a carbohydrate-restricted dietary programme between 2021 and 2024. Patients submitted photographs of all meals via WhatsApp with a minimum contact frequency of four times daily, enabling real-time feedback and medication adjustment. Anthropometric and metabolic parameters, including weight, BMI, HbA1c, renal function, and lipid profile, were assessed before and after the intervention. Results: Participants (mean age 69.12 ± 7.51 years) demonstrated significant improvement across several metabolic markers. Mean weight decreased by 5.74 kg (p < 0.001), BMI by 2.26 kg/m² (p < 0.001), and HbA1c by 0.72% (p < 0.001). No episodes of severe hypoglycemia or perioperative discharge delays related to glycemic instability were observed. Renal function remained stable, with no significant change in eGFR (p = 0.442). Among patients with available lipid data, LDL-cholesterol and total cholesterol increased, while triglycerides showed a non-significant downward trend. Conclusions: A low-carbohydrate diet combined with high-frequency digital monitoring appears feasible and safe in an elderly arthroplasty population, achieving meaningful short-term improvements in weight and glycemic control without adverse renal or hypoglycemic events. The lipid changes observed warrant cautious interpretation. Larger prospective studies are needed to confirm the clinical impact of this approach and its relevance to perioperative optimization.
Keywords:
diabetes
; digital health
; low-carbohydrate diet
; perioperative optimization
; total joint arthroplasty
; weight loss
1. Introduction
Diabetes represents a major global health challenge, with the IDF Diabetes Atlas (2024) reporting that approximately 1 in 9 adults aged 20–79 years currently lives with diabetes worldwide and projecting a substantial further increase by 2050, with four in five affected individuals residing in low- and middle-income countries [1]. In Malaysia, this burden is particularly pronounced: national data indicate an age-standardised adult diabetes prevalence of about 21%, alongside a high and rising prevalence of obesity documented in The Malaysian Cohort and reflected in the Ministry of Health’s Clinical Practice Guidelines on obesity management [1,2].
These metabolic comorbidities are highly relevant to hip and knee arthroplasty, as obesity and suboptimal glycaemic control have been associated with increased risks of prosthetic joint infection, impaired wound healing, cardiovascular events, and prolonged length of stay, and several large arthroplasty studies have demonstrated that elevated preoperative HbA1c and perioperative hyperglycaemia correlate with higher rates of postoperative infection and early complications [3,4,5,6,7,8,9].
In response, orthopaedic and endocrine guidelines—such as the AAOS Clinical Practice Guideline on the management of knee osteoarthritis and recommendations on perioperative diabetes care—now emphasise optimisation of weight and glycaemic control before elective arthroplasty, often advocating weight loss and postponement of surgery when HbA1c exceeds defined thresholds [2,3,4,6,7,8,9].
However, achieving stable glucose levels in the perioperative period remains challenging because of stress-induced insulin resistance, variability in perioperative carbohydrate intake, and the limitations of traditional sliding-scale insulin protocols [8,10,11]. These challenges have prompted growing interest in low-carbohydrate and ketogenic dietary strategies, which have demonstrated improvements in weight and HbA1c in patients with type 2 diabetes, and in digital health tools such as smartphone-based coaching, mobile social networking applications, and continuous glucose monitoring as potential adjuncts for safer and more effective perioperative metabolic optimisation in total joint arthroplasty candidates [5,12,13,14,15,16,17,18,19,20,21].
2. Materials and Methods
2.1. Study Design & Population
A retrospective cohort analysis was performed on 43 patients treated at a single centre between 2021 and 2024. This study was conducted in accordance with current legislation and ethical standards for clinical research and was approved by the Medical Research Ethics Committee of University of Malaya Medical Centre on 22 June 2025 (MREC ID NO.: 2025320-14882). Patients included were informed about the rationale of the treatment and provided informed consent. They were then recruited into the low carbohydrate diet program in Arthro Associates Clinic and underwent elective primary TJA (Hip or Knee) in Quill Orthopedic Specialist Centre (Figure 1).
Inclusion criteria were those age ≥ 18 years; type II diabetes or overweight patients; patients who underwent total joint arthroplasty (hip or knee) and those who were willing and able to provide informed consent. The exclusion criteria were those age < 18 years; type I diabetes; history of bariatric surgery for weight loss; factors that may affect HbA1c: haemoglobin < 11 mg/dl (cut point for moderate-to-severe anaemia, which could lead to falsely elevated or lowered HbA1c), recent blood donation or blood transfusion (self-reported, past 4 months), human immunodeficiency virus (self-report); self-reported history of intensive care unit stays due to COVID-19 3 months prior to initiation of dietary plan, as severe COVID-19 may affect blood glucose levels; and for women - pregnancy, breastfeeding [6].
2.2. Intervention Protocol
- Dietary Substrate: One portion of carbohydrate, one portion of protein ~ 40g (fish or chicken), one portion of simple protein (egg or tofu) and vegetables, with a calorie between 300-400 kcal. Rice was replaced with cauliflower rice.
- Digital Liaison: Patients were required to send photos of every meal and glucose readings to a dedicated team via WhatsApp when they are in the program, lasting between 2-4 months.
- Frequency: A minimum contact frequency of 4x daily was enforced. This allowed for immediate correction of dietary errors and safe titration of diabetic medication.
- Monitoring: Transition from finger-prick to Continuous Glucose Monitoring (CGM) pre-operatively.
2.3. Primary & Secondary Outcomes
- Primary: (a) occurrence of severe hypoglycaemia; (b) discharge delay due to glycaemic instability.
- Secondary: changes in weight, BMI, HbA1c, FBS, lipid and renal parameters, perioperative RBS range.
2.4. Statistical Analysis
Data was collected and managed using Microsoft Excel and analyzed using IBM SPSS Statistics (version 31) software. Descriptive statistics were utilized to summarize the data. Continuous variables were expressed as mean ± standard deviation or median with interquartile range (IQR). Categorical variables were presented as frequencies and percentages. Differences in baseline characteristics were analysed using independent and paired sample T-tests, while categorical data were compared using Fisher exact test. A P-value of < 0.05 was taken as statistically significant.
3. Results
3.1. Patient Demographic
The mean age of our study population is 69.12 ± 7.5 years; with 69.8% of them female. 23 patients underwent bilateral TKR, 14 underwent unilateral TKR and 6 underwent unilateral THR. 27 patients were diabetic, in which 23 of them were on oral agents and 4 were on insulin. The rest were under the non-diabetic/overweight category (Table 1).
Many patients were able to reduce or stop diabetic medications after the low-carbohydrate intervention. Among the 26 patients on OHA, 11 patients (42.3%) reduced the number of OHA used and 7 patients (26.9%) were able to completely stop all OHA. This indicates that about 69% either reduced or discontinued their oral diabetic medications, consistent with improved glycaemic control.
Among 4 patients on insulin, 1 patient reduced insulin dose and 3 patients were able to stop insulin completely and switch to OHA (Table 2). This suggests that, in this small insulin-treated subgroup, most patients improved enough to de-escalate from insulin to oral therapy, which supports the metabolic effectiveness of the intervention while maintaining safety.
3.2. Anthropometric & Metabolic Efficacy (Table 3)
The intervention delivered rapid, statistically significant optimization:
- Weight: Mean loss of 5.74 ± 4.10 kg (p < 0.001), ranging from 0.7 - 22.0 kg
- BMI: Reduction of 2.26 ± 1.47 kg/m2 (p < 0.001), ranging from 0.27 – 7.18 kg/m2
- HbA1c: Improved by 0.72 ± 0.49% (p < 0.001), ranging from -0.2 – 1.9%, with the highest HbA1c post intervention recorded at 7.2%

Table 3.
Parameters measured pre- and post-intervention.
| Parameters | Before | After | Difference | p-value | Total (n) |
| Height (m) | 1.58 ± 0.08 | - | 43 | ||
| Weight (kg) | 75.13 ± 17.18 | 69.38 ± 15.21 | 5.74 ± 4.10 | <0.001 | 43 |
| BMI (kg/m2) | 29.86 ± 5.66 | 27.60 ± 5.16 | 2.26 ± 1.47 | <0.001 | 43 |
| Waist circumference | 39.76 ± 5.32 | 35.47 ± 4.82 | 3.83 ± 2.14 | <0.001 | 18 |
| HbA1c | 6.36 ± 0.81 | 5.82 ± 0.49 | 0.72 ± 0.49 | <0.001 | 24 |
| FBS | 7.23 ± 2.49 | 5.91 ± 0.84 | 1.30 ± 2.12 | 0.002 | 27 |
| Total cholesterol | 4.79 ± 0.97 | 5.35 ± 1.45 | 0.71 ± 1.24 | 0.26 | 14 |
| Triglyceride | 1.88 ± 1.01 | 1.50 ± 0.65 | 0.38 ± 0.89 | 0.065 | 14 |
| HDL | 1.49 ± 0.45 | 1.37 ± 0.33 | 0.12 ± 0.22 | 0.032 | 14 |
| LDL | 2.77 ± 0.83 | 3.60 ± 1.37 | 0.81 ± 1.20 | 0.012 | 14 |
| Urea | 6.38 ± 3.08 | 9.01 ± 4.51 | 1.59 ± 3.36 | 0.030 | 18 |
| Creatinine | 85.70 ± 33.35 | 92.65 ± 26.26 | 8.44 ± 25.76 | 0.080 | 20 |
| eGFR | 75.49 ± 23.19 | 62.94 ± 20.40 | 0.63 ± 16.91 | 0.442 | 16 |
*Baseline anthropometric and metabolic parameters were taken and recorded during enrolment. During follow-up after surgery, ranging from 1-3 months, these parameters were repeated.
3.3. The Safety Profile
Safety was the primary endpoint of this pilot study.
- Hypoglycaemia: Despite 27 patients being on diabetic medication, none experienced dangerous hypoglycaemia (< 4.0 mmol/L) requiring rescue intervention.
- Discharge Delays: none of the patients had their discharge delayed due to glycaemic instability.
- Renal Stability: While Urea increased significantly (p=0.030), likely due to protein turnover, Creatinine (p=0.080) and eGFR (p=0.442) showed no significant change. This confirms that renal filtration function was preserved.
3.4. The Lipid Profile
The data revealed a distinct divergence in lipid markers:
- LDL-C: Increased significantly by 0.81 mmol/L (p=0.012).
- Total Cholesterol: Increased significantly (p=0.026).
- Triglycerides: Remained low (1.50 ± 0.65 mmol/L) with a trend toward reduction (p=0.065).
- HDL: decreased modestly but remained within generally favorable ranges (1.37 mmol/L).
The most critical finding for the orthopaedic community is the absence of life-threatening hypoglycaemia. In standard care, the combination of carbohydrate intake (raising sugar) and insulin (lowering sugar) creates glycaemic volatility. This approach may have contributed to a more stable perioperative glycaemia, preventing perioperative discharge delays and rendering it cost-effective.
The elevation in LDL-cholesterol (p=0.012) observed in this cohort warrants careful interpretation. Lipid elevations during active weight loss have been described in other low-carbohydrate or ketogenic diet studies, and several mechanistic models, including the Lipid Energy Model [22], propose physiologic explanations for this pattern. However, these hypotheses remain under active investigation, and the long-term cardiovascular implications of LDL changes in this specific population cannot be determined from this short-term study. Importantly, lipid measurements were available for only a subset of participants, underscoring the need for more complete data collection in future work.
4. Discussion
To our knowledge, this retrospective pilot study is among the first to examine the use of a carbohydrate-restricted dietary intervention supported by high frequency WhatsApp monitoring for patients with type 2 diabetes or obesity undergoing hip and knee arthroplasty. The findings suggest that this combined approach is feasible in an elderly surgical cohort and may contribute to improvements in weight, glycaemic control and several perioperative metabolic parameters.
Metabolic comorbidities such as obesity and diabetes are well-established risk factors for perioperative complications, notably prosthetic joint infection (PJI), the most devastating complication in arthroplasty . Furthermore, glycemic variability — the rapid fluctuation between high and low blood sugar — has been identified as a potent pro-inflammatory stressor that impairs wound healing , increasing length of hospital stay.
Traditional perioperative glycaemic management relied on reactive insulin titration. Patients are often admitted with suboptimal metabolic parameters, and hyperglycaemia is managed perioperatively using sliding-scale insulin. This approach presents a dual risk:
- Inefficacy: It treats the symptom (high sugar) without addressing the root cause (insulin resistance/dietary input).
- Safety: Aggressive insulin therapy increases the risk of iatrogenic hypoglycaemia, which is associated with arrhythmias, falls, and increased mortality in the elderly.
In contrast, dietary carbohydrate restriction targets the primary driver of hyperglycaemia and may offer a more physiologic method to mitigate perioperative glycaemic volatility. In this study, patients achieved significant reductions in body weight and HbA1c over a short preoperative window without observed episodes of severe hypoglycaemia, supporting the potential safety of this approach.
A notable component of this intervention was the use of a WhatsApp-based “tight feedback loop,” requiring patients to submit meal photographs and glucose readings several times daily. This strategy appeared to enhance engagement and adherence, demonstrating that elderly patients can successfully utilise simple digital tools when appropriately guided [15,16,17,18,19]. Digital health applications have been increasingly recognised as valuable adjuncts in chronic disease management, and the present study extends this concept into the preoperative optimisation phase for major orthopaedic surgery.
This pilot study aimed to:
- Establish Safety: Verify that strict carbohydrate restriction does not cause hypoglycaemia or renal impairment in a surgical cohort.
- Evaluate Feasibility: Assess the efficacy of WhatsApp-based photo-logging for elderly patients.
- Analyse Lipid Physiology: Interpret the “Lipid Paradox” (rising LDL with weight loss) through the lens of the Lipid Energy Model [22].
Major orthopaedic surgery induces a hypermetabolic stress response characterized by the release of cortisol, catecholamines, and glucagon . This state induces transient insulin resistance, often termed “stress hyperglycaemia.” In patients with poor baseline metabolic health, this response is exaggerated, significantly increasing the risk of deep infection . Despite this, this intervention gives value in reducing the fluctuations of peri-operative blood sugar.
The Ketogenic Diet shifts the body’s primary fuel source from glucose to ketones and fatty acids . While effective for weight loss and diabetes reversal, it is often criticized for raising Low-Density Lipoprotein Cholesterol (LDL-C). In a carbohydrate-restricted state, the liver packages triglycerides into Very Low-Density Lipoproteins (VLDL) to fuel peripheral tissues. As lean tissue (muscle) rapidly hydrolyses these triglycerides for energy, the VLDL particle shrinks and becomes an LDL particle.
In this context, elevated LDL is a “remnant” of high energy trafficking (fat burning), not a marker of broken cholesterol metabolism. The profile of High LDL + Low Triglycerides + High HDL is characteristic of the Lean Mass Hyper-Responder phenotype , which differs fundamentally from the atherogenic triad (High TG, Low HDL, Small LDL) associated with cardiovascular disease.
The success of this intervention relied on “Digital Dosage.” The requirement to photograph every meal created a Hawthorne Effect (behaviour change due to observation). This transformed the diet from a static prescription into a dynamic, managed process, suggesting that elderly patients can successfully engage with digital health tools [15,16,17,18,19].
This study also has several limitations inherent to its retrospective design. Selection bias is possible, as individuals who agreed to intensive dietary monitoring may differ from typical arthroplasty patients in motivation or digital literacy. Missing data, particularly for lipid and renal parameters, reduce the robustness of some conclusions. The dietary intervention was not strictly standardised, and meal assessments relied on photographs rather than objective nutritional analysis. Finally, the study did not include a control group, preventing causal inference regarding the superiority of this approach relative to standard care.
Despite these limitations, the results support the feasibility of implementing a digitally supported low-carbohydrate diet in the perioperative setting and suggest potential metabolic benefits that may justify further study. Prospective, controlled trials with larger sample sizes, complete biochemical data, and longer postoperative follow-up will be necessary to determine the true clinical impact of this protocol on surgical outcomes, complication rates, and healthcare utilisation.
5. Conclusions
A low-carbohydrate diet combined with high-frequency digital monitoring appears feasible and safe in an elderly arthroplasty population, achieving meaningful short-term improvements in weight and glycemic control without adverse renal or hypoglycemic events. The lipid changes observed warrant cautious interpretation. Larger prospective studies are needed to confirm the clinical impact of this approach and its relevance to perioperative optimization.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Each author has made substantial contributions to the work. More specifically, each author has developed the following roles: Conceptualization, S.K.C.; methodology, V.H.; validation, S.K.C.; formal analysis, H.W.O.; investigation, V.H.; resources, S.K.C.; data curation, H.W.O.; writing—original draft preparation, H.W.O.; writing—review and editing, H.W.O.; visualization, H.W.O.; supervision, S.K.C. and K.A.A.; project administration, S.K.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with current legislation and ethical standards for clinical research and was approved by the Medical Research Ethics Committee of University of Malaya Medical Centre on 22 June 2025 (MREC ID NO.: 2025320-14882).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The authors wish to acknowledge National Orthopedic Centre of Excellence for Research and Learning (NOCERAL) for the support and guidance for the preparation of this study, and Arthro Associates Sdn Bhd and Quill Orthopedic Specialist Centre for providing the groundwork of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AAOS | American Academy of Orthopaedic Surgeons |
| BMI | Body mass index |
| CGM | Continuous Glucose Monitoring |
| CPG | Clinical Practice Guidelines |
| eGFR | Renal filtration |
| FBS | Fasting blood sugar |
| HbA1c | Glycated hemoglobin |
| HDL | High-density lipoprotein |
| IDF | International Diabetes Federation |
| IQR | Interquartile range |
| LDL | Low-density lipoprotein |
| LEM | Lipid Energy Model |
| OHA | Oral hypoglycaemic agents |
| RBS | Random blood sugar |
| TG | Triglyceride |
| THR | Total hip replacement |
| TJA | Total joint arthroplasty |
| TKR | Total knee replacement |
| TMC | The Malaysian Cohort |
| PJI | Prosthetic joint infection |
| RCT | Randomized Controlled Trial |
| VLDL | Very low-density lipoprotein |
References
- Diabetes Atlas. “Diabetes Fact Sheets & Key Data | IDF Atlas Resources,” August 18, 2025. https://diabetesatlas.org/resources/factsheets/.
- Ministry of Health Malaysia et al., eds., CLINICAL PRACTICE GUIDELINES MANAGEMENT OF OBESITY 2ND EDITION (2023), PDF, 2nd ed. (Ministry of Health Malaysia, 2023), https://moh.gov.my/moh/resources/Penerbitan/CPG/Endocrine/CPG_Management_of_Obesity_(Second_Edition)_2023.pdf.
- American Academy of Orthopaedic Surgeons Management of Osteoarthritis of the Knee (Non Arthroplasty) Evidence-Based Clinical Practice Guideline. https://www.aaos.org/oak3cpg Published 08/31/2021.
- Cull, Megan. “Weight Loss for Obese Patients as a Treatment of Hip and Knee Osteoarthritis: A Scoping Review.” Journal of Metabolic Health 7, no. 1 (2024). [CrossRef]
- Ahmed, S. R., S. Bellamkonda, M. Zilbermint, J. Wang, and R. R. Kalyani. “Effects of the Low Carbohydrate, High Fat Diet on Glycemic Control and Body Weight in Patients with Type 2 Diabetes: Experience from a Community-Based Cohort.” BMJ Open Diabetes Res Care 8, no. 1 (Mar 2020). https://www.ncbi.nlm.nih.gov/pubmed/32193200. [CrossRef]
- Premkumar, A., D. A. Kolin, K. X. Farley, J. M. Wilson, A. S. McLawhorn, M. B. Cross, and P. K. Sculco. “Projected Economic Burden of Periprosthetic Joint Infection of the Hip and Knee in the United States.” [In eng]. J Arthroplasty 36, no. 5 (May 2021): 1484-89.e3. [CrossRef]
- Holleyman, R. J., M. Clarkson, A. Shenfine, K. Martin, J. Prentis, M. Bowditch, G. Rayman, A. Judge, and M. R. Reed. “Association between Preoperative Glycaemic Control (Hba1c) and Early Outcomes Following Primary Hip and Knee Arthroplasty.” [In eng]. Bone Joint J 107-b, no. 6 (Jun 1 2025): 615-24. [CrossRef]
- Shohat, Noam, Camilo Restrepo, Arash Allierezaie, Majd Tarabichi, Rahul Goel, and Javad Parvizi. “Increased Postoperative Glucose Variability Is Associated with Adverse Outcomes Following Total Joint Arthroplasty.” JBJS 100, no. 13 (2018): 1110-17. https://journals.lww.com/jbjsjournal/fulltext/2018/07050/increased_postoperative_glucose_variability_is.5.aspx. [CrossRef]
- Cancienne, J. M., B. C. Werner, and J. A. Browne. “Is There a Threshold Value of Hemoglobin A1c That Predicts Risk of Infection Following Primary Total Hip Arthroplasty?” [In eng]. J Arthroplasty 32, no. 9s (Sep 2017): S236-s40. [CrossRef]
- Desborough, J. P. “The Stress Response to Trauma and Surgery.” [In eng]. Br J Anaesth 85, no. 1 (Jul 2000): 109-17. [CrossRef]
- Marik, P. E., and R. Bellomo. “Stress Hyperglycemia: An Essential Survival Response!” [In eng]. Crit Care 17, no. 2 (Mar 6 2013): 305. [CrossRef]
- Dorans, K. S., L. A. Bazzano, L. Qi, H. He, L. J. Appel, J. M. Samet, J. Chen, et al. “Low-Carbohydrate Dietary Pattern on Glycemic Outcomes Trial (Adept) among Individuals with Elevated Hemoglobin A1c: Study Protocol for a Randomized Controlled Trial.” Trials 22, no. 1 (Feb 1 2021): 108. https://www.ncbi.nlm.nih.gov/pubmed/33522954. [CrossRef]
- Dorans, K. S., L. A. Bazzano, L. Qi, H. He, J. Chen, L. J. Appel, C. S. Chen, et al. “Effects of a Low-Carbohydrate Dietary Intervention on Hemoglobin A1c: A Randomized Clinical Trial.” JAMA Netw Open 5, no. 10 (Oct 3 2022): e2238645. https://www.ncbi.nlm.nih.gov/pubmed/36287562. [CrossRef]
- Son, H., S. H. Sohn, H. A. Kim, H. J. Choe, H. Lee, H. S. Jung, Y. M. Cho, et al. “Real-Time Continuous Glucose Monitoring Improves Postoperative Glucose Control in People with Type 2 Diabetes Mellitus Undergoing Coronary Artery Bypass Grafting: A Randomized Clinical Trial.” [In eng]. Diabetes Obes Metab 27, no. 4 (Apr 2025): 1836-44. [CrossRef]
- Alanzi, T., S. Bah, S. Alzahrani, S. Alshammari, and F. Almunsef. “Evaluation of a Mobile Social Networking Application for Improving Diabetes Type 2 Knowledge: An Intervention Study Using Whatsapp.” [In eng]. J Comp Eff Res 7, no. 9 (Sep 2018): 891-99. [CrossRef]
- Sun, S., O. Simonsson, S. McGarvey, J. Torous, and S. B. Goldberg. “Mobile Phone Interventions to Improve Health Outcomes among Patients with Chronic Diseases: An Umbrella Review and Evidence Synthesis from 34 Meta-Analyses.” [In eng]. Lancet Digit Health 6, no. 11 (Nov 2024): e857-e70. [CrossRef]
- Hallberg, S. J., A. L. McKenzie, P. T. Williams, N. H. Bhanpuri, A. L. Peters, W. W. Campbell, T. L. Hazbun, et al. “Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 year: An Open-Label, Non-Randomized, Controlled Study.” [In eng]. Diabetes Ther 9, no. 2 (Apr 2018): 583-612. [CrossRef]
- Bhanpuri, N. H., S. J. Hallberg, P. T. Williams, A. L. McKenzie, K. D. Ballard, W. W. Campbell, J. P. McCarter, S. D. Phinney, and J. S. Volek. “Cardiovascular Disease Risk Factor Responses to a Type 2 Diabetes Care Model Including Nutritional Ketosis Induced by Sustained Carbohydrate Restriction at 1 year: An Open Label, Non-Randomized, Controlled Study.” [In eng]. Cardiovasc Diabetol 17, no. 1 (May 1 2018): 56. [CrossRef]
- Lin, C. Q., H. R. Chmait, J. P. Conroy, N. J. Nelms, and M. Blankstein. “Can We Empower Patients for Joint Surgery? Assessing the Impact of a Telemedicine Coaching Intervention.” [In eng]. Arthroplast Today 33 (Jun 2025): 101701. [CrossRef]
- Paoli, A., A. Rubini, J. S. Volek, and K. A. Grimaldi. “Beyond Weight Loss: A Review of the Therapeutic Uses of Very-Low-Carbohydrate (Ketogenic) Diets.” [In eng]. Eur J Clin Nutr 67, no. 8 (Aug 2013): 789-96. [CrossRef]
- Norwitz, N. G., D. Feldman, A. Soto-Mota, T. Kalayjian, and D. S. Ludwig. “Elevated Ldl Cholesterol with a Carbohydrate-Restricted Diet: Evidence for a “Lean Mass Hyper-Responder” Phenotype.” [In eng]. Curr Dev Nutr 6, no. 1 (Jan 2022): nzab144. [CrossRef]
- Norwitz, N. G., A. Soto-Mota, B. Kaplan, D. S. Ludwig, M. Budoff, A. Kontush, and D. Feldman. “The Lipid Energy Model: Reimagining Lipoprotein Function in the Context of Carbohydrate-Restricted Diets.” [In eng]. Metabolites 12, no. 5 (May 20 2022). [CrossRef]
Figure 1.
Flow diagram.
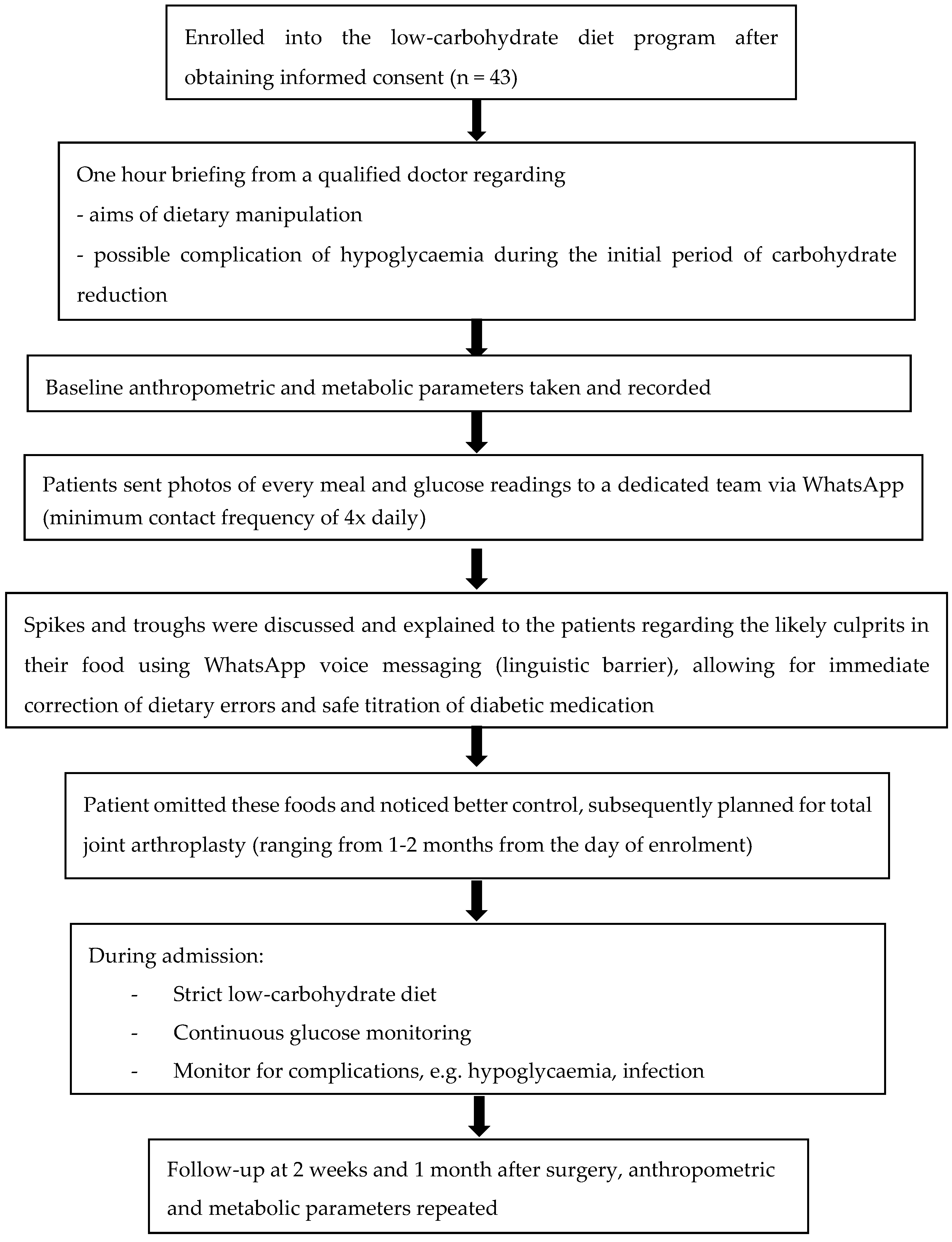
Table 1.
Patient demographic.
| Demographics | Total (n=43) | ||
| Age | 69.12 ± 7.51 | 43 | |
| Gender | Male | 13 (30.2%) | 43 |
| Female | 30 (69.8%) | ||
| Category | Non-diabetic | 12 (27.9%) | 43 |
| Diabetic (not on insulin) | 23 (53.5%) | ||
| Diabetic (on insulin) | 4 (9.3%) | ||
| Parkinson’s | 2 (4.7%) | ||
| Defaulter | 2 (4.7%) | ||
| Surgery | Unilateral TKR | 14 (32.6%) | 43 |
| Bilateral TKR | 23 (53.5%) | ||
| Unilateral THR | 6 (14.0%) | ||
| Medication | Not on diabetic medication | 13 (30.2%) | 43 |
| OHA | 26 (60.5%) | ||
| Insulin | 4 (9.3%) |
Table 2.
Changes in oral hypoglycaemic agents and insulin requirements following the low-carbohydrate intervention.
Table 2.
Changes in oral hypoglycaemic agents and insulin requirements following the low-carbohydrate intervention.
| Medication | Total (n) | ||
| OHA | No change in the number of OHA | 8 (30.8%) | 26 |
| Reduction in the number of OHA | 11 (42.3%) | ||
| Complete stop of all OHA | 7 (26.9%) | ||
| Insulin | Reduction in insulin units | 1 (25%) | 4 |
| Complete stop of insulin, change to OHA | 3 (75%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



