Submitted:
14 January 2026
Posted:
14 January 2026
You are already at the latest version
Abstract
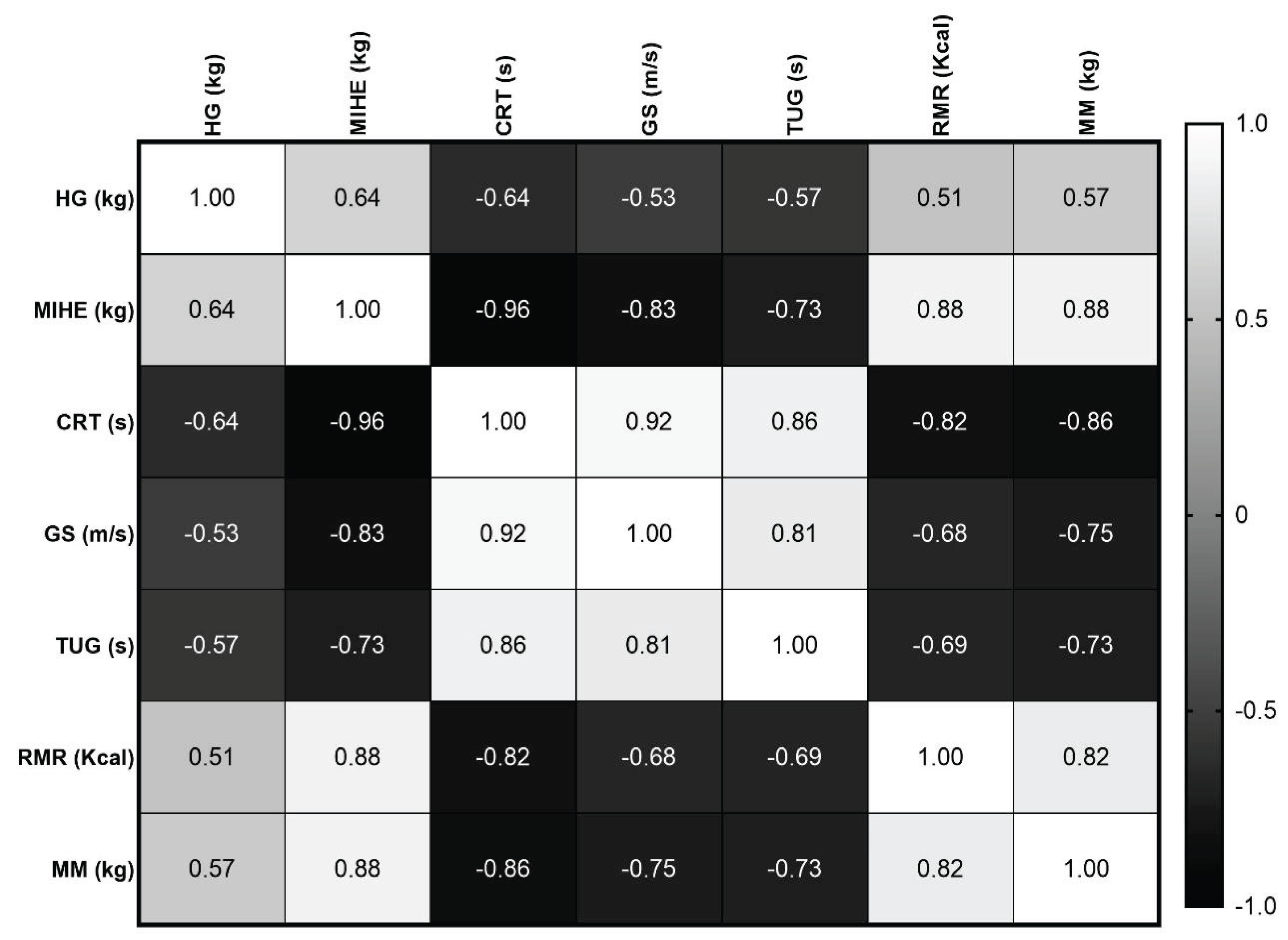
Sarcopenia is a complex condition marked by reductions in muscle strength, mass, and overall physical performance, which has significant consequences for functional autonomy and metabolic health in elderly women. This study sought to examine the correlations between lower limb strength, functional capabilities, and metabolic indicators in community-dwelling older women categorized according to the EWGSOP2 criteria. A total of thirty-eight women aged ≥ 60 years underwent assessments, including anthropometric, hemodynamic, and metabolic evaluations, along with functional tests such as handgrip strength, chair-rise test, gait speed, Timed Up-and-Go, and maximal isometric hip extension strength (MIHE). The criteria for probable sarcopenia were established using the handgrip thresholds set by the EWGSOP2. Women identified as having probable sarcopenia displayed markedly lower MIHE, diminished gait speed, inferior performance in chair-rise and Timed Up-and-Go tests, decreased muscle mass, and a lower resting metabolic rate than their non-sarcopenic counterparts. MIHE exhibited robust correlations with muscle mass, resting metabolic rate, and functional performance metrics. These results suggest that assessments of lower limb and trunk strength yield pertinent insights beyond handgrip strength alone. Function-oriented evaluations may improve sarcopenia screening and facilitate the identification of older women at risk of functional and metabolic deficiencies in community-based environments.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Sarcopenia Classification
2.4. Functional Tests
Handgrip Strength (HG)
Chair Rise Test (CRT)
Gait Speed (GS)
Maximal Isometric Hip Extension (MIHE)
Timed Up-and-Go Test (TUG)
2.5. Statistical Methods
3. Results
3.1. Anthropometric Characteristics of Participants
3.2. Hemodynamic Parameters, Disease History, and Lifestyle Habits
3.3. Physical Activity Modalities and Habits
3.4. Strength and Functional Performance
3.5. Muscle Strength, Functional Performance, and Metabolic Parameters in Sarcopenic and Non-Sarcopenic Groups
3.6. Correlation Analysis
4. Discussion
4.1. Anthropometric and Cardiometabolic Profile as a Substrate for Sarcopenia Risk
4.2. Physical Activity Patterns and Their Functional Implications
4.3. Functional Performance and EWGSOP2-Based Sarcopenia Screening
4.4. Maximal Isometric Hip Extension Strength as an Integrative Marker
4.5. Muscle Strength, Metabolic Rate, and Muscle Mass Interdependence
4.6. Functional Test Interrelationships and Sarcopenia Phenotyping
4.7. Integrative Interpretation
4.8. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BIA | Bioelectrical Impedance Analysis |
| BMI | Body Mass Index |
| CRT | Chair Rise Test |
| DBP | Diastolic Blood Pressure |
| EWGSOP2 | European Working Group on Sarcopenia in Older People 2 |
| GS | Gait Speed |
| HG | Handgrip Strength |
| HR | Heart Rate |
| MAP | Mean Arterial Pressure |
| MIHE | Maximal Isometric Hip Extension |
| MM | Muscle Mass |
| RMR | RMR: Resting Metabolic Rate |
| RPE | Rate of Perceived Exertion |
| SARC-F | Sarcopenia Risk Questionnaire |
| SBP | Systolic Blood Pressure |
| TUG | Timed Up-and-Go |
| WHO | World Health Organization |
| WHR | Waist-to-Hip Ratio |
References
- Buch, A.; Eldor, R.; Kis, O.; Ben-Yehuda, A.; Green, G.; Greenman, Y.; Barak, S. Metabolic and functional factors associated with a change in resting metabolic rate among older adults with type 2 diabetes: Results from the CEV-65 randomized trial. Heliyon 2025, 11, e41593. [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [CrossRef]
- Fragala, M.S.; Alley, D.E.; Shardell, M.D.; Harris, T.B.; McLean, R.R.; Kiel, D.P.; et al. Comparison of handgrip and leg extension strength in predicting slow gait speed in older adults. J. Am. Geriatr. Soc. 2016, 64, 144–150. [CrossRef]
- Granacher, U.; Gollhofer, A.; Hortobágyi, T.; Kressig, R.W.; Muehlbauer, T. The importance of trunk muscle strength for balance, functional performance, and fall prevention in seniors: A systematic review. Sports Med. 2013, 43, 627–641. [CrossRef]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking speed: The functional vital sign. J. Aging Phys. Act. 2015, 23, 314–322.
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [CrossRef]
- Bohannon, R.W. Reference values for the Timed Up and Go Test: A descriptive meta-analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68.
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [CrossRef]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go test a useful predictor of risk of falls in community-dwelling older adults? A systematic review and meta-analysis. BMC Geriatr. 2014, 14, 14. [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [CrossRef]
- Pua, Y.H.; Wrigley, T.V.; Cowan, S.M.; Bennell, K.L. Intrarater test–retest reliability of hip range of motion and hip muscle strength measurements in persons with hip osteoarthritis. Arch. Phys. Med. Rehabil. 2008, 89, 1146–1154. [CrossRef]
- Anand, A.; Mohta, S.; Agarwal, S.; et al. EWGSOP2 criteria with population-based skeletal muscle index best predicts mortality in Asians with cirrhosis. J. Clin. Exp. Hepatol. 2022, 12, 52–60.
- Gadelha, A.B.; Dutra, M.T.; Oliveira, R.J.; Safons, M.P.; Lima, R.M. Associação entre força, sarcopenia e obesidade sarcopênica com o desempenho funcional de idosas. Motricidade 2014, 10, 31–39.
- Vilaça, K.H.C.; Alves, N.M.C.; Carneiro, J.A.O.; Ferriolli, E.; Lima, N.K.C.; Moriguti, J.C. Body composition, muscle strength and quality of active elderly women according to the distance covered in the 6-minute walk test. Rev. Bras. Fisioter. 2013, 17, 289–296. [CrossRef]
- Ohara, D.G.; Pegorari, M.S.; Santos, N.L.O.; Silva, C.F.R.; Monteiro, R.L.; Matos, A.P.; Jamami, M. Respiratory muscle strength as a discriminator of sarcopenia in community-dwelling elderly. J. Nutr. Health Aging 2018, 22, 952–958. [CrossRef]
- Soares, L.A.; Lima, L.P.; Prates, A.C.N.; et al. Accuracy of handgrip and respiratory muscle strength in identifying sarcopenia in older Brazilian women. Sci. Rep. 2023, 13, 28549. [CrossRef]
- Domiciano, D.S.; Figueiredo, C.P.; Lopes, J.B.; et al. Discriminating sarcopenia in community-dwelling older women with high frequency of overweight/obesity. Osteoporos. Int. 2013, 24, 595–603. [CrossRef]
- Frisoli, A.; Duque, G.; Paes, A.T.; et al. Sarcopenic obesity definitions and their associations with physical frailty in older Brazilian adults. Arch. Endocrinol. Metab. 2023, 67, 361–371. [CrossRef]
- Kemp, V.L.; Piber, L.D.S.; Ribeiro, A.P.C. Physical activity, energy expenditure and clinical aspects of sarcopenia in elderly women. Sao Paulo Med. J. 2021, 139, 285–292.
- Genaro, P.S.; Pinheiro, M.M.; Szejnfeld, V.L.; Martini, L.A. Dietary protein intake in elderly women: Association with muscle and bone mass. Nutr. Clin. Pract. 2015, 30, 283–289.
- Magalhães, N.V.; Waitzberg, D.L.; Lopes, N.C.; et al. High prevalence of energy and nutrient inadequacy among Brazilian older adults. Nutrients 2023, 15, 3246. [CrossRef]
- Pereira, C.C.; Pagotto, V.; Oliveira, C.D.; Silveira, E.A. Sarcopenia and mortality risk in community-dwelling Brazilian older adults. Sci. Rep. 2022, 12, 22153. [CrossRef]
- Paludo, C.S.; Gonzalez, T.N.; Soares, P.S.M.; Meucci, R.D. Prevalence and factors associated with probable sarcopenia in southern Brazil. Rural Remote Health 2024, 24, 8711. [CrossRef]
- Sutil, D.V.; Parentoni, A.N.; Teixeira, L.A.C.; et al. Prevalence of sarcopenia and agreement between EWGSOP2 instruments in older women. BMC Musculoskelet. Disord. 2023, 24, 287.
- Zanotti, J.; Wender, M.C.O. Sarcopenia: Prevalence and associated factors among older women in southern Brazil. Rev. Bras. Geriatr. Gerontol. 2021.
- Mattos, K.M.D.; Costodio, A.R.; Leme, D.E.C.; et al. Prevalence of sarcopenia in socially active older adults: Bayesian network analysis. Rev. Bras. Geriatr. Gerontol. 2024, 28.
- Campos, G.C.; Lourenço, R.A.; Molina, M.C.B. Mortality, sarcopenic obesity and frailty in Brazilian older adults (FIBRA-RJ). Rev. Saude Publica 2021, 55.
- Casagrande, M.L.; Dell’Osbel, R.S.; Zanotti, J.; Wender, M.C.O. Sarcopenia, obesity and sarcopenic obesity in older women. ABCS Health Sci. 2022, 47, e022215.
- Nascimento, R.A.; Vieira, M.C.A.; Fernandes, J.; et al. Anthropometric adiposity indices and physical performance in Brazilian women. Epidemiol. Health 2022, 44, e2022074.
- Teixeira, L.A.C.; Soares, L.A.; Fonseca, S.F.; et al. Body composition, functionality and muscle-specific strength in older women. Sci. Rep. 2024, 14, 76417.
- Lustosa, L.P.; Batista, P.P.; Ribeiro-Samora, G.A.; et al. Operational criteria related to muscle loss in elderly Brazilian women. Top. Geriatr. Rehabil. 2018, 34, 155–161. [CrossRef]
- Franco, M.F.; Leme, D.E.C.; Coimbra, I.B.; Coimbra, A.M.V. Prevalence and factors associated with sarcopenia in Brazilian older adults. Arch. Gerontol. Geriatr. 2024, 105438.

| Anthropometric parameters (N=38) | Mean ± SD |
|---|---|
| Age (y) | 69.9 ± 6.6 |
| Height (m) | 1.6 ± 0.1 |
| Body mass (kg) | 64.5 ± 12.9 |
| BMI (kg/m2) | 26.8 ± 5.0 |
| Waist circumference (cm) | 85.7 ± 10.3 |
| Abdominal circumference (cm) | 91.4 ± 11.2 |
| Hip circumference (cm) | 103.1 ± 10.2 |
| Waste and hip ratio | 0.8 ± 0.1 |
| Upper Arm Circumference (cm) | 28.2 ± 3.2 |
| Forearm Circumference (cm) | 24.5 ± 2.3 |
| Calf Circumference (cm) | 35.7 ± 3.8 |
| Blood parameters | Mean ± SD |
|---|---|
| Blood glucose (mg/dL) | 107.2 ± 46.4 |
| SBP (mmHg) | 143.4 ± 16.5 |
| DBP (mmHg) | 80.1 ± 11.5 |
| MAP (mmHg) | 101.2 ± 11.8 |
| HR rest (bpm) | 72.3 ± 11.7 |
| Daily habits | N (%) |
| Smoker | 4 (10.5%) |
| Alcohol consumption | 34 (89.5%) |
| History of illness | N (%) |
| Hypertension | 23 (60.53%) |
| Diabetes | 7 (18.42%) |
| Dyslipidemia | 3 (7.89%) |
| Hypothyroidism | 4 (10.53%) |
| Cancer | 1 (2.63%) |
| Exercise modalities | N (%) |
|---|---|
| Water Aerobics | 18 (47.4) |
| Gymnastics | 17 (44.7) |
| Yoga | 16 (42.1) |
| Physical Therapy and Acupuncture | 8 (21.1) |
| Memory Workshop | 8 (21.1) |
| Dance | 7 (18.4) |
| Tai Chi Chuan | 6 (15.8) |
| Beauty Salon | 5 (13.2 |
| Pilates | 5 (13.2) |
| Choir | 3 (7.9) |
| Crafts | 3 (7.9) |
| Global Postural Reeducation (GPR) | 2 (5.3) |
| Physical activity habits | Mean ± SD |
| Frequency (days/week) | 3.3 ± 1.2 |
| Intensity (RPE) | 3.4 ± 1.4 |
| Duration (min) | 45 to 60 |
| Time (mouths) | N (%) |
| 0 to 3 | 11 (28.9) |
| 3 to 6 | 3 (7.9) |
| 6 to 9 | 5 (13.2) |
| 9 to 12 | 7 (18.4) |
| > 12 | 12 (31.6) |
| Strength and physical ability tests | Mean ± SD |
|---|---|
| HG (kg) | 17.2 ± 5.5 |
| Chair rise test (s for 5 rises) | 12.0 ± 3.1 |
| Timed Up and Go (TUG, s) | 8.8 ± 1.6 |
| Gait Speed (m/s) | 1.2 ± 0.4 |
| MIHE (kg) | 52.3 ± 15.3 |
| Strength and physical ability tests | Mean ± SD | p-value | |
|---|---|---|---|
| < 16 kg | > 16 kg | ||
| MIHE (kg) | 43.7 ± 15.7 | 59.1 ± 11.1 | 0.001 |
| GS (m/s) | 1.0 ± 0.3 | 1.5 ± 0.5 | 0.002 |
| TUG (s) | 9.8 ± 1.9 | 7.9 ± 0.7 | 0.0002 |
| CRT (s for 5 rises) | 13.8 ± 3.5 | 10.5 ± 1.6 | 0.0004 |
| RMR (kcal/day) | 1008 ± 174 | 1149 ± 110 | 0.004 |
| MM (kg) | 37.6 ± 4.2 | 41.5 ± 3.9 | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.



