
Submitted:
12 January 2026
Posted:
13 January 2026
You are already at the latest version
Abstract
Background/Objectives: Refractory macular holes (MH) that persist after conventional internal limiting membrane (ILM) peeling pose a significant surgical challenge. This study analyzed the anatomical and functional outcomes of epiretinal human amniotic membrane (hAM) transplantation in these patients. Methods: This retrospective study included 10 eyes of 10 patients with refractory MH. All patients underwent 25-gauge pars plana vitrectomy, epiretinal cryopreserved hAM transplantation, and C3F8 gas tamponade. The large hAM graft was placed over the macula with the chorion side facing the retina. Preoperative and postoperative best-corrected visual acuity (BCVA), optical coherence tomography (OCT) findings, and MH dimensions were recorded. Results: The mean follow-up period was 7 months (range 3–14 months). The mean preoperative minimum linear diameter and base diameter of the MHs were 715 ± 212 μm and 1114 ± 258 μm, respectively. Anatomical closure was achieved in all patients (100%). Postoperative OCT revealed rearrangement of the inner and other retinal layers in 7 out of 10 patients (70%), with partial restoration of the outer retinal layers. The mean logMAR BCVA improved significantly from 1.60 ± 0.37 preoperatively to 1.00 ± 0.45 postoperatively (p < .001). No graft dislocation, rejection, or other significant complications were observed. Conclusions: Epiretinal human amniotic membrane transplantation is an effective and safe surgical technique for achieving anatomical closure and functional improvement in refractory macular holes where conventional ILM peeling has failed.
Keywords:
epiretinal transplantation
; human amniotic membrane
; pars plana vitrectomy
; refractory macular hole
1. Introduction
Idiopathic full-thickness macular holes (MH) are significant vitreoretinal pathologies affecting all layers of the neurosensory retina in the foveal region, leading to severe reduction in central visual acuity, metamorphopsia, and central scotoma [1]. Until recent years, the combination of pars plana vitrectomy (PPV), internal limiting membrane (ILM) peeling, and gas tamponade is considered the “gold standard” for the surgical management of these cases [2]. Although this approach provides anatomical closure rates of 90% to 95%, particularly in holes smaller than 400 μm and stage 2–3 holes, success rates may decrease in cases with large diameters (>400 µm), chronic duration, or traumatic etiology [3,4]. More importantly, “refractory” macular holes that fail to close or recur despite primary surgery and ILM peeling remain one of the most complex challenges in vitreoretinal surgery [5,6].
In the management of refractory cases, the absence of residual ILM tissue around the hole (the “No-ILM” situation) limits surgical options [7]. Various reconstructive techniques, such as autologous neurosensory retinal transplantation (ART), lens capsule flaps, extended ILM peeling, or relaxing retinotomy, have been proposed to achieve anatomical closure in cases where standard techniques are insufficient [8,9,10]. However, some of these methods may entail disadvantages such as surgical difficulty, potential risk of retinal damage, visual field loss, or limited functional gain [3]. Furthermore, aggressive ILM peeling itself can disrupt retinal morphology by causing iatrogenic trauma, such as the appearance of a “dissociated optic nerve fiber layer” (DONFL) on the inner retinal surface [2,11]. Therefore, particularly in persistent cases, there is a need for “scaffold” materials that not only provide mechanical closure but also biologically support tissue regeneration [12].
Human amniotic membrane (hAM) stands out as a potent biomaterial in regenerative medicine due to its thick basal membrane, avascular stroma, and richness in growth factors (TGF-β, bFGF, EGF, NGF) [13,14]. Long used in ophthalmology for ocular surface reconstruction due to its low immunogenicity, anti-inflammatory properties, and fibrosis-suppressing structure, hAM has recently become a promising “salvage” treatment option in vitreoretinal surgery [15,16]. It has been reported that hAM provides excellent growth support for RPE cells, facilitates glial cell migration, and promotes the restoration of outer retinal layers by secreting neurotrophic factors [17,18].
In the literature, hAM is applied either as a plug (inlay) placed inside the hole or as a patch (overlay) placed over the retina [5]. Although the plug technique has been found successful in some studies, the difficulty of fitting the graft size exactly to the hole and the potential risk of RPE damage are debated [19]. In contrast, the epiretinal patch (overlay) technique is emphasized for interfering less with the natural anatomical structure of the retina, preserving RPE integrity, and providing biological support over a larger surface area during the healing process [20,21]. Recent studies demonstrate that hAM transplantation yields high anatomical closure rates (93–100%) not only in idiopathic refractory holes but also in much more challenging scenarios such as high myopia-associated macular holes, cases complicated by retinal detachment, and traumatic holes [22,23,24]. Additionally, systematic reviews have reported that hAM use presents low complication rates and offers statistically significant results in visual function improvement compared to other techniques [25,26].
The aim of this study is to evaluate the anatomical closure success, the healing process of outer retinal layers (ellipsoid zone and external limitan membrane), and the functional outcomes of epiretinal human amniotic membrane transplantation in refractory macular holes that failed to close despite conventional ILM peeling. Our study specifically aims to document the regenerative effects and surgical safety of hAM in an environment devoid of ILM.
2. Methods
2.1. Study Design and Ethics
This retrospective study was conducted at the Department of Ophthalmology, Ulucanlar Eye Training and Research Hospital. The study protocol adhered to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Numune Eye Training and Research Hospital (No. E-37-1685). Written informed consent was obtained from all participants prior to the surgery, following a detailed explanation of the procedure and potential risks.
2.2. Patient Selection
We reviewed records of patients who underwent surgery for refractory MH (March 2023–April 2025). Inclusion criteria were the presence of a persistent full-thickness MH despite previous PPV with ILM peeling and intraocular gas tamponade. Exclusion criteria included a history of retinal vascular occlusion, diabetic retinopathy, retinal neovascularization, or severe ocular trauma. A total of 10 eyes of 10 patients met the inclusion criteria.
2.3. Preoperative Assessment
All patients underwent a comprehensive ophthalmic examination, including measurement of best-corrected visual acuity (BCVA), slit-lamp biomicroscopy, and spectral-domain optical coherence tomography (SD-OCT) (Spectralis, Heidelberg Engineering GmbH, Germany). BCVA was measured using a Snellen chart and converted to the logarithm of the minimum angle of resolution (logMAR) for statistical analysis. MH dimensions, including the minimum linear diameter and base diameter, were measured using the caliper function of the OCT software. Axial length was measured for all patients.
2.4. Surgical Technique
All surgeries were performed by the same experienced surgeon using a standard 25-gauge 4-port transconjunctival micro-incision vitrectomy system (Constellation Vision System, Alcon Surgical, Fort Worth, TX, USA). After core vitrectomy, Brilliant Blue G dye was used to stain the retinal surface to confirm the absence of any residual ILM or epiretinal membranes.
A 4 to 8 mm diameter graft of cryopreserved hAM was prepared. The graft was inserted into the vitreous cavity through a 25-gauge trocar. Using end-gripping forceps, the hAM was positioned over the macular hole. Crucially, the graft was oriented with the sticky stromal (chorion) side facing the retina and the epithelial side facing the vitreous. The orientation was verified intraoperatively by identifying the sticky surface with forceps. Perfluorocarbon liquid (PFCL) was injected over the posterior pole to flatten the graft and ensure stable positioning over the macula. Following a fluid-air exchange, the PFCL was carefully removed, ensuring the graft remained in place. Finally, a non-expansile concentration of 14% perfluoropropane (C3F8) gas was exchanged for air. Patients were instructed to maintain a face-down position for 3 days postoperatively.
2.5. Outcome Measures and Statistical Analysis
The primary outcome was anatomical closure of the MH confirmed by OCT. Secondary outcomes included improvement in BCVA and restoration of retinal layers. Statistical analysis was performed using SPSS (IBM Corp., Armonk, NY, USA) software. The normality of data distribution was assessed using the Shapiro–Wilk test. Continuous variables were expressed as mean ± standard deviation (SD). Preoperative and postoperative values were compared using the paired Student’s t-test. A p-value of less than .05 was considered statistically significant.
3. Results
3.1. Demographics and Baseline Characteristics
The study included 10 patients (7 females, 3 males) with a mean age of 56.7 ± 6.1 years (range: 50–68 years). Nine patients presented with idiopathic refractory MH, while one patient had a persistent MH following surgery for retinal detachment (RD) with macular hole. The mean axial length was 23.24 ± 0.71 mm. The baseline characteristics of the study population are summarized in Table 1.
3.2. Anatomical Outcomes
The mean preoperative minimum linear diameter of the MHs was 715 ± 162 μm, and the mean base diameter was 1114 ± 258 μm. Anatomical closure was achieved in all 10 eyes (100%) after a single surgery with hAM transplantation. No cases of graft dislocation, contracture, or immunologic rejection were observed during the follow-up period.
Postoperative OCT analysis demonstrated the integration of the hAM graft into the retinal defect. Rearrangement of the inner retinal layers and partial restoration of the outer retinal layers, including the ellipsoid zone, were observed in 7 out of 10 patients (70%). Representative cases demonstrating preoperative and postoperative OCT findings are shown in Figure 1, Figure 2 and Figure 3.
3.3. Functional Outcomes
The mean follow-up time was 7 months (range: 3–14 months). Visual acuity improved in all patients. The mean preoperative BCVA was 1.60 ± 0.37 logMAR, which significantly improved to 1.00 ± 0.45 logMAR at the final follow-up visit (p < .001). Patients with better baseline visual acuity tended to achieve better final visual outcomes (p = .012).
4. Discussion
Refractory macular holes that fail to close despite standard pars plana vitrectomy and ILM peeling constitute one of the most complex scenarios in vitreoretinal surgery. In these cases, the absence of residual ILM tissue around the hole (the “No-ILM” situation) restricts surgical options. In our study, the 100% anatomical closure rate and statistically significant increase in visual acuity achieved with epiretinal cryopreserved hAM transplantation in this challenging patient group indicate that hAM acts not merely as a mechanical plug, but as a regenerative scaffold for retinal tissue, contributing to the restoration of foveal architecture. This high anatomical success strongly parallels similar challenging case series in the literature. For instance, Khaqan et al. reported 100% closure using hAM in giant and persistent macular holes [4]; similarly, Calis Karanfil et al. and Ferreira et al. reported full success with a single surgery in refractory cases [13,27]. The multicenter ReMaHo study conducted by Lorenzi et al. also supports our findings, confirming that hAM use provides statistically superior closure rates compared to autologous ILM flap techniques, particularly in holes larger than 680 μm [7].
In addition to anatomical success, the biological form and preparation method of the amniotic membrane play a decisive role in surgical outcomes. The efficacy of lyophilized (dried) versus cryopreserved (frozen) grafts is frequently compared in the literature. While Garcin et al. reported an 80% closure rate in their series using lyophilized amniotic membrane [20], a 100% success rate was achieved in our study with cryopreserved membrane. This aligns perfectly with the results of a comprehensive meta-analysis by Zhang et al.; the authors emphasized that cryopreserved grafts provide a distinct advantage with a 99% closure rate compared to lyophilized grafts (73%) and have a much lower risk of dislocation (3% vs. 26%) [15]. Sharma et al. and Carlà also state that the cryopreservation process better preserves the membrane’s growth factors, anti-inflammatory cytokines, and structural integrity compared to the lyophilized form, thereby strengthening the graft-host tissue interaction [16,28]. Although Huang et al. noted that both graft types could be effective [29], our experience and current literature data suggest that the thicker stromal structure of cryopreserved grafts facilitates surgical manipulation and shortens the learning curve when applied with the “Triple S” (Staining, Sizing, Sliding) technique [30].
Regarding surgical technique, the “epiretinal overlay” (patch) technique preferred in our study is based on the principle of laying the graft over the retina rather than stuffing it into the hole, and this approach has been a critical factor in our anatomical and functional outcomes. Teoh and Garcin et al. state that this “overlay” position respects the natural organization of retinal layers more and carries a lower risk of triggering foveal gliosis compared to subretinal plugging [5,20]. Ventre et al. reported that in the plug technique, if the graft is cut larger than the hole diameter, the resulting “centrifugal thrust” can create a mechanical barrier and delay closure [19]. The rapid healing process and orderly organization of retinal layers under the graft in our series confirm the mechanical advantages of epiretinal placement. Furthermore, as suggested by Iannetta et al., placing the graft with the chorion (sticky) side facing the retina increased adhesion [21], preventing graft dislocation and contributing to the absence of graft displacement in any patient in our study. This technique maximizes surgical safety when combined with adjunctive methods such as viscoelastic, PFCL or intraoperative OCT use, as proposed by Qian and Saab [31].
Although anatomical closure in refractory cases does not always translate to full functional recovery, a statistically significant improvement in visual acuity (from logMAR 1.60 to 1.00) was recorded in our study. This finding is consistent with results reported by Proença et al. and Caporossi et al., showing that visual gain is maintained in long-term follow-ups [17,18]. The basis of visual improvement lies in hAM’s neurotrophic factors (NGF, bFGF, EGF) supporting photoreceptor viability and promoting the restoration of outer retinal layers (ellipsoid zone and external limiting membrane) [14]. The outer retinal restoration observed in 70% of cases in our study suggests that hAM is not just a barrier but a biological healer. A systematic review by Frisina et al., concluding that hAM transplantation is the method providing the highest visual acuity increase (mean 0.99 logMAR gain) compared to free ILM flaps or other techniques [25], strongly supports our findings. Although Özdemir Zeydanlı et al. reported limited regeneration despite anatomical success in very complex and high myopic cases [23], it appears that functional potential is preserved in isolated refractory holes like those in our series, and hAM unlocks this potential.
Alternative surgical techniques exist for the management of refractory holes; however, hAM transplantation stands out with its safety profile and ease of application. For example, although autologous neurosensory retinal transplantation (ART) offers high anatomical success (94%) as reported by Hanai et al. and Grewal et al. [3,9], it harbors disadvantages such as its invasive nature, potential risk of retinal detachment, peripheral visual field loss, and failure of the graft to fully integrate with surrounding tissue [6,8]. Similarly, Descemet membrane transplantation described by Gürelik et al. yields successful results but graft procurement may involve logistical challenges [32]. Additionally, it is known that extended ILM peeling maneuvers in refractory cases lead to iatrogenic trauma such as the “dissociated optic nerve fiber layer” (DONFL) appearance on the retinal surface and can leave permanent damage in the inner retinal layers [2,11]. In this context, hAM transplantation is an advantageous “salvage” treatment option as it is less traumatic compared to ART, does not require autologous tissue harvesting, and initiates biological repair without causing additional damage to the retina. Szurman et al. also emphasized that hAM use in revision surgeries is one of the most reliable adjuvant techniques with 100% success [12].
Regarding the safety profile, the absence of complications such as graft rejection, endophthalmitis, chronic hypotony, or severe inflammation in our study can be explained by hAM’s low immunogenicity and potent anti-inflammatory properties [26]. Although Trivedi et al. suggested using the graft temporarily and removing it later [33], our long-term follow-ups and large-series data in the literature show that permanent integration of the graft is safe, it organizes under retinal layers over time, and there is no need for additional surgical trauma [17,18]. Furthermore, the fact that researchers like Caporossi et al. and Yamamoto et al. achieved successful results with hAM even in much more severe presentations complicated by trauma or retinal detachment proves the reliability and versatility of the material [22,24]. Bokor and Fodor also stated in their review that biological scaffolds like hAM are among the most important instruments compensating for the insufficiency of standard techniques, especially in large holes over 600 µm [1].
The retrospective design of our study, the relatively small number of patients, and the absence of a control group are its main limitations. Additionally, the lack of advanced functional tests such as microperimetry or multifocal ERG limited our quantitative assessment of changes in retinal sensitivity. Despite all these limitations, considering that refractory macular holes are a rare and difficult-to-treat condition, this 100% success rate obtained in a homogeneous patient group sheds light on clinical practice.
5. Conclusions
In conclusion, epiretinal cryopreserved human amniotic membrane transplantation is a reliable surgical method that guarantees anatomical closure, allows for functional improvement, and carries a low risk of complications in refractory macular holes where conventional surgery has failed.
Author Contributions
All authors contributed equally to the conception, design, execution, analysis, and writing of this study. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Numune Training and Research Hospital Clinical Research Ethics Committee (Approval No: E-37-1685).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ART | Autologous (neurosensory) Retinal Transplantation |
| BCVA | Best-Corrected Visual Acuity |
| bFGF | Basic Fibroblast Growth Factor |
| DONFL | Dissociated Optic Nerve Fiber Layer |
| EGF | Epidermal Growth Factor |
| hAM | Human Amniotic Membrane |
| ILM | Internal Limiting Membrane |
| logMAR | Logarithm of the Minimum Angle of Resolution |
| MH | Macular Hole |
| NGF | Nerve Growth Factor |
| OCT | Optical Coherence Tomography |
| PFCL | Perfluorocarbon Liquid |
| PPV | Pars Plana Vitrectomy |
| RD | Retinal Detachment |
| RPE | Retinal Pigment Epithelium |
| SD-OCT | Spectral-Domain Optical Coherence Tomography |
| SO | Silicone Oil |
| TGF-β | Transforming Growth Factor-beta |
References
- Bokor, Á.; Fodor, M. Surgical management of refractory full-thickness macular holes with emphasis on autologous retinal transplantation: A narrative review. Regen. Med. Rep. 2025, 3, 1–5. [Google Scholar] [CrossRef]
- Steel, D.H.W.; Dinah, C.; Habib, M.; White, K. ILM peeling technique influences the degree of a dissociated optic nerve fibre layer appearance after macular hole surgery. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 691–698. [Google Scholar] [CrossRef]
- Hanai, M.; Amaral, D.C.; Jacometti, R.; et al. Large macular hole and autologous retinal transplantation: A systematic review and meta-analysis. Int. J. Retina Vitreous 2024, 10, 56. [Google Scholar] [CrossRef]
- Khaqan, H.A.; Sahyoun, J.Y.; Haider, M.A.; Buksh, H.M. Amniotic membrane graft for the treatment of large refractory macular hole. Retina 2022, 42, 1479–1483. [Google Scholar] [CrossRef]
- Teoh, C.S. An insight into current and novel treatment practices for refractory full-thickness macular hole. J. Clin. Transl. Ophthalmol. 2025, 3, 15. [Google Scholar] [CrossRef]
- Carlà, M.M.; Mateo, C. Autologous retina transplantation for refractory highly myopic macular holes: A long-term follow-up. Jpn. J. Ophthalmol. 2025, 69, 259–267. [Google Scholar] [CrossRef]
- Lorenzi, U.; Mehech, J.; Caporossi, T.; Romano, M.R.; De Fazio, R.; Parrat, E.; Matonti, F.; Mora, P. A retrospective, multicenter study on the management of macular holes without residual internal limiting membrane: The refractory macular hole (ReMaHo) study. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 3837–3845. [Google Scholar] [CrossRef]
- Rojas-Juárez, S.; Cisneros-Cortés, J.; Ramirez-Estudillo, A.; Velez-Montoya, R. Autologous full-thickness retinal transplant for refractory large macular holes. Int. J. Retina Vitreous 2020, 6, 60. [Google Scholar] [CrossRef] [PubMed]
- Grewal, D.S.; Charles, S.; Parolini, B.; Kadonosono, K.; Mahmoud, T.H. Autologous retinal transplant for refractory macular holes: Multicenter international collaborative study group. Ophthalmology 2019, 126, 1399–1408. [Google Scholar] [CrossRef]
- Lumi, X.; Petrovic Pajic, S.; Sustar, M.; Fakin, A.; Hawlina, M. Autologous neurosensory free-flap retinal transplantation for refractory chronic macular hole - outcomes evaluated by OCT, microperimetry, and multifocal electroretinography. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 1443–1453. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Xu, J.; He, S.; et al. Quantitative evaluation of dissociated optic nerve fibre layer (DONFL) following idiopathic macular hole surgery. Eye 2022, 37, 1451–1457. [Google Scholar] [CrossRef] [PubMed]
- Szurman, P.; Wakili, P.; Stanzel, B.V.; Siegel, R.; Boden, K.T.; Rickmann, A. Persistent macular holes - what is the best strategy for revision? Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 1781–1790. [Google Scholar] [CrossRef] [PubMed]
- Calis Karanfil, F.; Toklu, Y.; Arikan Yorgun, M. Amniotic membrane transplantation for macular hole closure. Beyoğlu Eye J. 2023, 8, 55–59. [Google Scholar] [CrossRef]
- Tartaro, R.; Caporossi, T.; Virgili, G.; Barca, F.; Giansanti, F.; Rizzo, S. Insights on the human amniotic membrane in clinical practice with a focus on the new applications in retinal surgery. Regen. Eng. Transl. Med. 2022, 8, 22–31. [Google Scholar] [CrossRef]
- Zhang, H.; Li, Y.; Chen, G.; Han, F.; Jiang, W. Human amniotic membrane graft for refractory macular hole: A single-arm meta-analysis and systematic review. J. Fr. Ophtalmol. 2023, 46, 276–286. [Google Scholar] [CrossRef]
- Sharma, R.; Nappi, V.; Empeslidis, T. The developments in amniotic membrane transplantation in glaucoma and vitreoretinal procedures. Int. Ophthalmol. 2023, 43, 1771–1783. [Google Scholar] [CrossRef]
- Proença, H.; Antunes, M.; Ferreira, J.T.; Magro, P.; Faria, M.; Marques-Neves, C. Outcomes of amniotic membrane transplant for refractory macular hole - an optical coherence tomography and autofluorescence long term study. Graefes Arch. Clin. Exp. Ophthalmol. 2025, 263, 315–326. [Google Scholar] [CrossRef]
- Caporossi, T.; Scampoli, A.; Baldascino, A.; et al. Subretinal transplant of human amniotic membrane in advanced age-related macular degeneration. Life 2022, 12. [Google Scholar] [CrossRef]
- Ventre, L.; Marolo, P.; Reibaldi, M. A human amniotic membrane plug to treat persistent macular hole. Case Rep. Ophthalmol. 2020, 11, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Garcin, T.; Gain, P.; Thuret, G. Epiretinal large disc of blue-stained lyophilized amniotic membrane to treat complex macular holes: A 1-year follow-up. Acta Ophthalmol. 2022, 100, e598–e608. [Google Scholar] [CrossRef]
- Iannetta, D.; Chhablani, J.; Valsecchi, N.; Mesiani, M.; de Smet, M.D.; Fontana, L. Epiretinal implant of human amniotic membrane to treat highly myopic macular hole retinal detachments: A novel surgical technique. Eur. J. Ophthalmol. 2024, 34, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Caporossi, T.; Governatori, L.; Gambini, G.; et al. Treatment of recurrent high myopic macular hole associated with retinal detachment using a human amniotic membrane. Jpn. J. Ophthalmol. 2022, 66, 518–526. [Google Scholar] [CrossRef]
- Özdemir Zeydanlı, E.; Özdek, Ş.; Yalçın, E.; Özdemir, H.B. Human amniotic membrane: A seal for complex retinal detachments. Turk. J. Ophthalmol. 2024, 54, 268–274. [Google Scholar] [CrossRef]
- Yamamoto, M.H.; Marin, A.I.; Tsui, I. Management of traumatic macular hole and retinal detachment using amniotic membrane transplantation: A case report. Am. J. Ophthalmol. Case Rep. 2025, 37, 102267. [Google Scholar] [CrossRef] [PubMed]
- Frisina, R.; Gius, I.; Tozzi, L.; Midena, E. Refractory full thickness macular hole: Current surgical management. Eye 2022, 36, 1344–1354. [Google Scholar] [CrossRef]
- Quiroz-Reyes, M.A.; Quiroz-Gonzalez, E.A.; Quiroz-Gonzalez, M.A.; Lima-Gomez, V. Safety and efficacy of human amniotic membrane plug transplantation in cases of macular hole. A scoping review. Int. J. Retina Vitreous 2024, 10, 82. [Google Scholar] [CrossRef]
- Ferreira, M.A.; Maia, A.; Machado, A.J.; Ferreira, R.E.A.; Hagemann, L.F.; Ribeiro Júnior, P.H.E.; Rezende, F.A. Human amniotic membrane for the treatment of large and refractory macular holes: a retrospective, multicentric, interventional study. Int. J. Retina Vitreous 2021, 7, 38. [Google Scholar] [CrossRef]
- Carlà, M.M.; Giannuzzi, F.; Hu, L.; Rizzo, C.; Crincoli, E.; Catania, F.; Gambini, G.; Caporossi, T.; Mateo, C.; Rizzo, S. The human amniotic membrane in vitreoretinal surgery: Applications, outcomes and limitations. Surv. Ophthalmol. 2025, 71, 14–24. [Google Scholar] [CrossRef]
- Huang, Y.H.; Tsai, D.C.; Wang, L.C.; Chen, S.J. Comparison between cryopreserved and dehydrated human amniotic membrane graft in treating challenging cases with macular hole and macular hole retinal detachment. J. Ophthalmol. 2020, 2020, 9157518. [Google Scholar] [CrossRef]
- Shroff, D.; Bhatia, G.; Kumar, S.; Grewal, D.S. Staining and sizing technique for human amniotic membrane graft in refractory macular holes. J. VitreoRetin. Dis. 2025, 9, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Qian, S.Y.; Saab, M. Human amniotic membrane graft with viscodissection and intraoperative OCT for macular hole repair. Am. J. Ophthalmol. Case Rep. 2025, 38, 102302. [Google Scholar] [CrossRef] [PubMed]
- Gürelik, İ.G.; Özdemir, H.B.; Acar, A.B.; Aydın, B. Descemet’s membrane transplantation for the treatment of recurrent high myopic macular hole associated with retinal detachment. Graefes Arch. Clin. Exp. Ophthalmol. 2025, 263, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, V.; You, Q.; Me, R.; Lee, P.S.Y.; Le, K.; Tran, D.; Lin, X. Temporary amniotic membrane graft placement for treatment of refractory macular holes. Retin. Cases Brief Rep. 2026, 20, 39–42. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Preoperative and postoperative spectral-domain optical coherence tomography (SD-OCT) images of a patient with refractory macular hole. (A) Preoperative OCT scan showing a full-thickness macular hole with atrophic edges. (B) Postoperative OCT scan at 2 months showing complete anatomical closure of the hole following human amniotic membrane transplantation. The graft is well-integrated, and there is visible restoration of the foveal contour (arrow).
Figure 1.
Preoperative and postoperative spectral-domain optical coherence tomography (SD-OCT) images of a patient with refractory macular hole. (A) Preoperative OCT scan showing a full-thickness macular hole with atrophic edges. (B) Postoperative OCT scan at 2 months showing complete anatomical closure of the hole following human amniotic membrane transplantation. The graft is well-integrated, and there is visible restoration of the foveal contour (arrow).
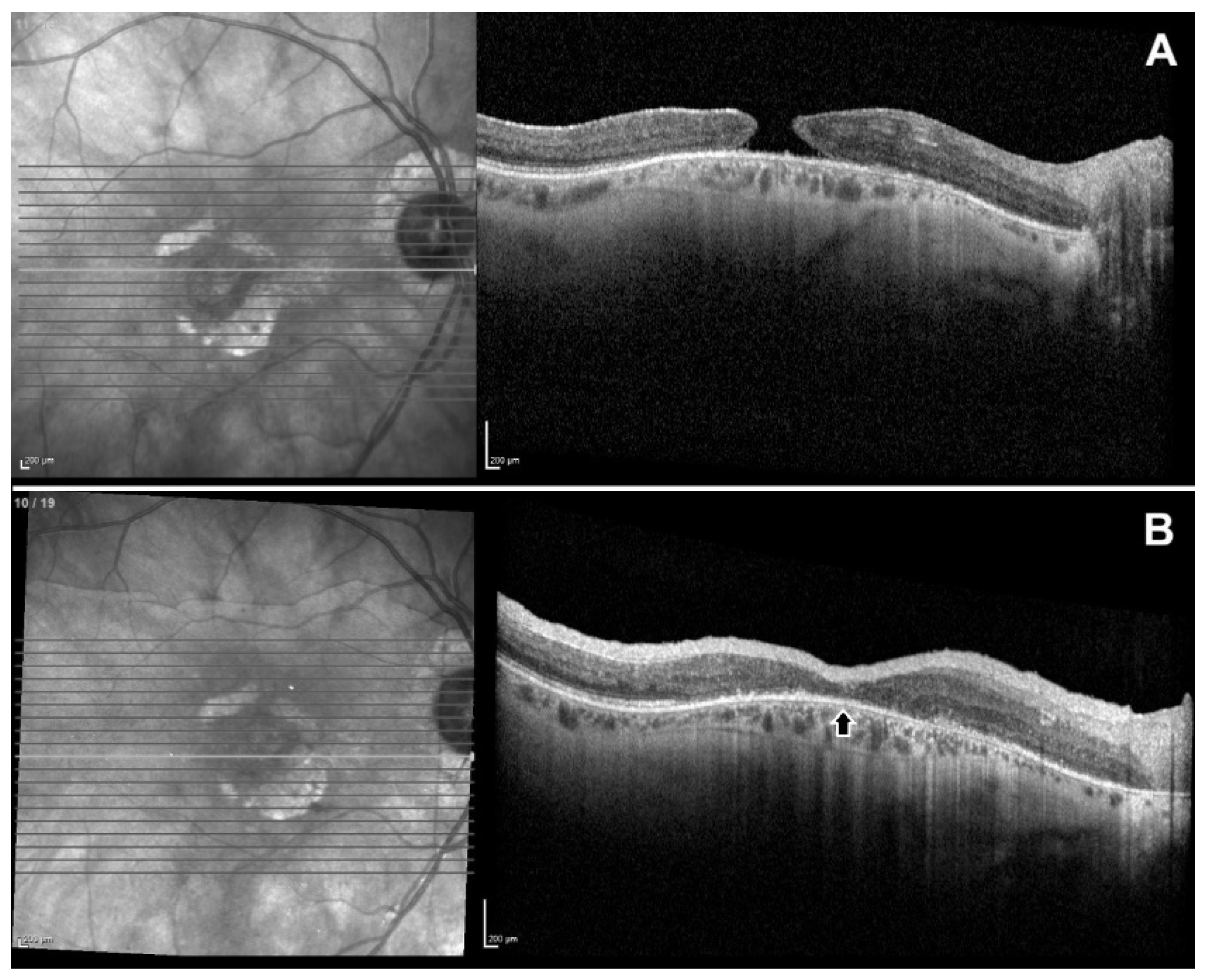
Figure 2.
Preoperative and postoperative fundus photographs and spectral-domain optical coherence tomography (SD-OCT) images of a patient with refractory macular hole (after retinal detachment and macular hole surgery with silicon oil). (A) Preoperative color fundus photography of the patient; retina attached with intravitreal silicon oil but there is refractory macular hole (B) Postoperative fundus photography; large human amniotic patch is over the macula. (C) Preoperative OCT scan showing a large full-thickness macular hole with atrophic edges (D) Postoperative OCT scan at 2 months showing complete anatomical closure of the hole following epiretinal human amniotic membrane transplantation. The amniotic graft is well-integrated, inner and outer retinal layers are rearranged.
Figure 2.
Preoperative and postoperative fundus photographs and spectral-domain optical coherence tomography (SD-OCT) images of a patient with refractory macular hole (after retinal detachment and macular hole surgery with silicon oil). (A) Preoperative color fundus photography of the patient; retina attached with intravitreal silicon oil but there is refractory macular hole (B) Postoperative fundus photography; large human amniotic patch is over the macula. (C) Preoperative OCT scan showing a large full-thickness macular hole with atrophic edges (D) Postoperative OCT scan at 2 months showing complete anatomical closure of the hole following epiretinal human amniotic membrane transplantation. The amniotic graft is well-integrated, inner and outer retinal layers are rearranged.
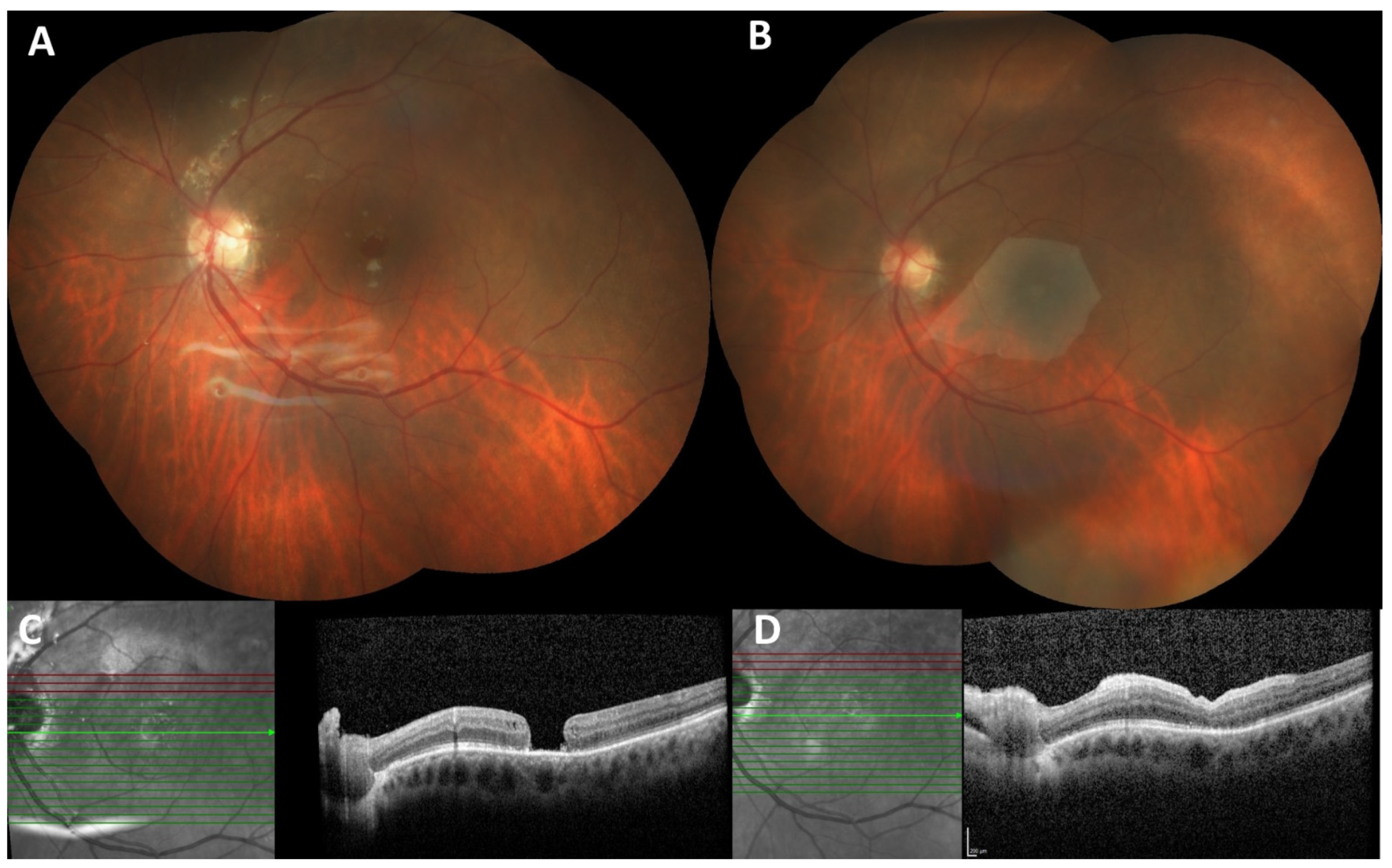
Figure 3.
Preoperative and postoperative spectral-domain optical coherence tomography (SD-OCT) images of a patient with refractory macular hole. (A) Preoperative OCT scan showing a full-thickness large macular hole with cystoid changes. (B) Postoperative OCT scan at 3 months showing complete anatomical closure of the hole, there is visible restoration of the foveal contour and retinal layers.
Figure 3.
Preoperative and postoperative spectral-domain optical coherence tomography (SD-OCT) images of a patient with refractory macular hole. (A) Preoperative OCT scan showing a full-thickness large macular hole with cystoid changes. (B) Postoperative OCT scan at 3 months showing complete anatomical closure of the hole, there is visible restoration of the foveal contour and retinal layers.
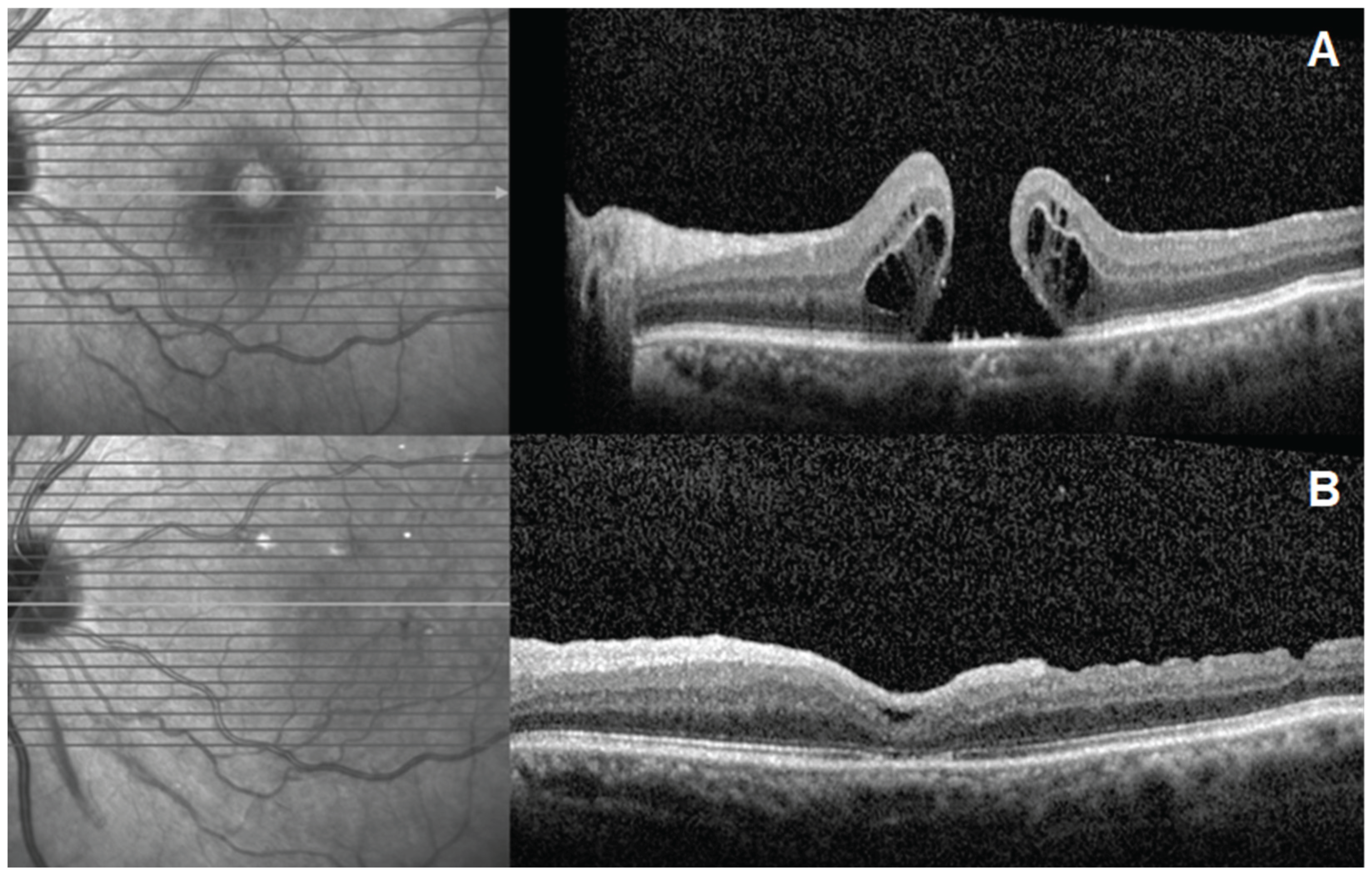

Table 1.
Demographics and baseline clinical characteristics of patients.
| ID | Age | Gender | Eye | Dx | Prior Surgery | AL (mm) | MH min (µm) | MH base (µm) | BCVA (logMAR) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 53 | F | R | RMH | PPV + ILMp + C3F8 | 22.6 | 715 | 1115 | 1.6 |
| 2 | 58 | M | L | RMH | PPV + ILMp + C3F8 | 23.7 | 760 | 1234 | 1.4 |
| 3 | 59 | F | R | RMH | PPV + ILMp + C3F8 | 24.2 | 682 | 1087 | 1.2 |
| 4 | 50 | F | L | RD + RMH | PPV + ILMp + SO | 24.1 | 502 | 1205 | 1.8 |
| 5 | 63 | M | R | RMH | PPV + ILMp + C3F8 | 23.2 | 730 | 945 | 1.8 |
| 6 | 61 | M | L | RMH | PPV + ILMp + C3F8 | 22.3 | 712 | 1118 | 1.7 |
| 7 | 50 | F | R | RMH | PPV + ILMp + C3F8 | 22.7 | 812 | 1302 | 1.6 |
| 8 | 68 | F | R | RMH | PPV + ILMp + C3F8 | 23.0 | 612 | 989 | 1.7 |
| 9 | 50 | F | L | RMH | PPV + ILMp + C3F8 | 24.0 | 724 | 1023 | 1.6 |
| 10 | 55 | F | R | RMH | PPV + ILMp + C3F8 | 22.6 | 714 | 1145 | 1.6 |
AL: axial length; BCVA: best-corrected visual acuity; C3F8: perfluoropropane gas; Dx: diagnosis; F: female; ILMp: internal limiting membrane peeling; L: left; M: male; MH: macular hole; MH base: macular hole base diameter; MH min: macular hole minimum diameter; PPV: pars plana vitrectomy; R: right; RD: retinal detachment; RMH: refractory macular hole; SO: silicone oil.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



