
Submitted:
08 January 2026
Posted:
09 January 2026
You are already at the latest version
Abstract
Study design: A series of 26 patients, submitted to decompressive craniectomy for su-pratentorial cerebral ischemia was retrospectively analyzed. Objectives: The aim of this study is to highlight the experience with this surgical tech-nique in our Institution and to analyze comparatively the preoperative and postoperative clinical and radiological data, as well as the prognostic factors verifying the agreement between our findings and the relevant literature data. Methods: From January 2018 to January 2023, we recruited 26 patients that underwent decompressive craniectomy for supratentorial cerebral ischemia. Demographic, medical history, clinical, laboratory, radiological and surgical data were collected. Statistical analysis was also performed to determine if any variable had a significant impact pre-viously and post-operatively or if they were predictive of favorable outcome. Results: The average age of the patients was 56.55 y, range between 26-80 y. Patients under 60 y were 51.8% and 59,25% of the whole sample were male. The outcome score calculated with the Modified Ranking Scale after about 1 year was < =4 in 11 patient; it distributed as follows: 2 pts with MRS 2, 5 pts with MRS 3 and 4 pts with MRS 4. The remaining were dead or in a vegetative state. Univariate statistical analysis was focused on neuroradiological parameters, studied both in pre- and post-operative CT scans. The variables that proved to be statistically significant were the presence or absence of visible cortical sulci, basal cisterns compression (cisterna ambiens in particular), quadrigeminal and sylvian cisterns. Of these parameters, the only one that maintained statistical sig-nificance even in the multivariate analysis was the presence of visible cisterna ambiens in post-operative radiological studies proving to be associated with a favorable outcome. Conclusions: Our study confirmed that decompressive craniectomy in cerebral ischemic stroke is an effective life-saving treatment in a subgroup of patients with intracranial hypertension. Standardization of the surgical indication remains a challenge and our analysis could suggest potentially useful work patterns in daily clinical practice, eventough our expe-rience had the important limitation of measuring only physical disability; further studies considering psychosocial, financial and caregiving aspects are needed. Moreover, sur-gical management remains in our opinion a tailored choice based on the experience of the surgeon and on the expectations of the patient and family.
Keywords:
decompressive craniectomy
; ischemic stroke
; supratentorial
; cerebral cisterns
; neuroradiological
; prognostic factors
1. Introduction
Malignant cerebral supratentorial stroke is a life-threatening condition, due to the development of cerebral edema with consequent increase in intracranial pressure, and the most affected are relates to the middle cerebral artery vascular territory. It is associated with a mortality rate up to 80%, and survival is affected by a serious degree of disability [1]. Limited effectiveness of medical therapies has resulted in decompressive craniectomy being increasingly considered as a treatment option, although evidence of its efficacy is still inconclusive. Decompressive surgery can be a life-saving procedure after malignant cerebral stroke, but severe residual disability can happen in a significant number of surviving patients, and there is no consensus on which clinical features should be used in patients’ selection and on the best timing of the procedure. In all these cases, the ultimate goal is to try to reduce the intracranial pressure (life-saving goal) and avoid further extension of the suffering brain parenchyma (damage control). Despite in an ever-increasing number of studies the role of decompressive craniectomy in acute supratentorial cerebral strokes has been reported to be lifesaving and improve in some cases functional outcome [2,3], in daily clinical practice the treatment decisions still remain individualized on a patient-specific basis, on the surgeon’s experience and on the expectations of the patient or mostly of the family (Figure 1). The goal of this study is to understand the agreement between our findings and the relevant literature data trying to identify the patients who could benefit from this surgical procedure; in addition, we aimed to evaluate the effectiveness of decompressive craniectomy, in terms of mortality reduction and postoperative disability. In particular our manuscript focuses on what’s “before” and “after” the neurosurgical procedure of decompressive craniectomy following a supratentorial ischemic stroke. The aim is to try to clarify the impact of pre-operative parameters (clinical, laboratory or radiological findings) on the decision of the neurosurgeon to select a patient for this particularly invasive surgical procedure. Furthermore, the evaluation also includes clinical and radiological parameters that improve following surgical decompression, the anamnestic or clinical risk factors that improve the global outcome and understanding the most appropriate surgical timing. The identification of specific pre and postoperative parameters that could provide indications on the prognosis of patients is of particular importance from a therapeutic point of view, as they guide the choice for the best treatment.
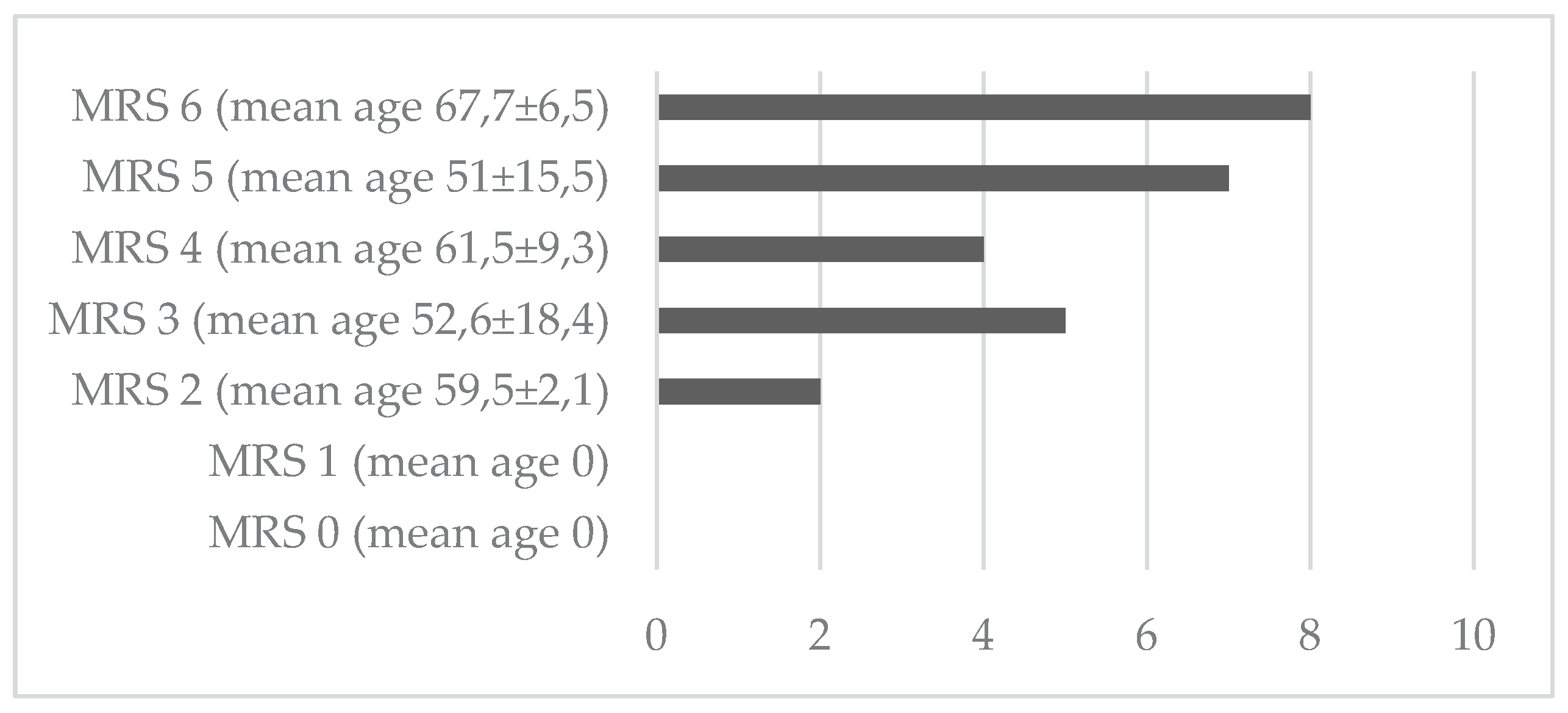
Graph 1.
Overall outcome.
2. Materials and Methods
This single-center retrospective study included a series of 26 patients who underwent decompressive craniectomy for supratentorial cerebral ischemic stroke between January 2018 and January 2023 at our Institution. Patients’ data, clinical, laboratory, radiological and surgical findings were collected from digital medical records along with radiological and laboratory data. In addition, missing postoperative details were obtained through interviews or outpatient clinical evaluations at 3-, 6- and 12-months follow-up. This research was performed with the full respect of privacy, professional secrecy and medical deontology. Preoperative evaluation prevented surgical indication ot the basis of the following exclusion criteria: GCS less than 6/15, serious and massive bihemispheric ischemic damage and/or extension to the brainstem and/or ICA strokes, severe dementia or chronic bedridden patients, bilateral mydriasis, age over 80 years and terminal illness.
3. Clinical Records
The following data were obtained: personal and clinical information, medical history (including cardiovascular risk factors), comorbidities such as diabetes, hypertension, dyslipidemia, tumor history, hereditary coagulation disorders (hyperhomocysteinemia, autoimmune diseases) overweight or obesity and admission GCS value. Regarding the postoperative neurological assessment, the MRS (Modified Rankin Scale) was applied, evaluated at 3, 6 months and 1 year after surgery. Although an MRS of 4 is usually identified as an unfavourable outcome, it is argued that considering the severity of a condition such as supratentorial cerebral ischemic stroke, recovery back to an MRS score of 1 or 2 is highly unlikely. Thus, we included an MRS of 4 in the overall good or socially acceptable outcome category. We chose not to use other reference scales such as the GOS (Glasgow outcome scale), because among the exclusion criteria we decided not to include previous head trauma history.
3.1. Blood Chemistry Values
These parameters were recorded before and after the neurosurgical procedure, up to 1 month postoperatively: numeric value and percentage of neutrophils and lymphocytes, NLR (neutrophil-lymphocyte ratio), PLR (platelet-lymphocyte ratio), haemoglobin, hematocrit, platelet count, PTT, INR, renal function, serum fibrinogen, and glucose blood level.
3.2. Surgical Details
The surgical information analyzed were the intervention timing and the occurence of postoperative complications (syndrome of trephined, localized or systemic infection, haemorrhage). Any preliminary therapy that the patients received before surgery, such as I.V. fibrinolysis or mechanical thrombectomy, were also considered. Technically the surgical procedure is quite standardized worldwide according to the relevant literature and consists of a large bone flap removal with the opening of the dura mater and subsequent duroplasty. In our department we performed a large hemicraniectomy that removed, ipsilateral to the stroke territory, a bone flap as large as possible, however related to the size of the ischemic area, including temporal, frontal, parietal, and sometimes occipital areas. The dura was always opened, and watertight duraplasty was performed in at least half of the patients based on the intraoperative findings and on the neurosurgeons’ discretion. In our series, no patient underwent partial or total resection of the necrotic cerebral tissue. Some Authors described the decompressive technique associated with stokectomy, which however include small retrospective series [4,5]. We normally do not perform strokectomy as we believe that “ischemic penumbra” includes temporarily non-functioning neurons with a potential for functional recovery without a structural damage, provided that local blood flow can be re-established within a certain time window that is dependent on the residual flow [6].
3.3. Neuroradiological Imaging
All patients underwent preoperative brain CT scan and we retrospectively reviewed images from the institutional diagnostic imaging recording software. Therefore, the side of the ischemic stroke, the artery involved and the diameter and volume of the ischemic area including the related perilesional edema (calculated by the neuroradiologist through Centricity Pacs System – General Electrics Healthcare) were analysed. Furthermore, in the pre- and postoperative period, the midline shift, the presence of compression of the lateral and the third ventricle ipsilateral to the lesion, basal cisterns, the presence of cerebral herniation and hemorrhagic reperfusion were evaluated. The development of hydrocephalus as well as the evidence of interhemispheric subdural collections were analyzed.
4. Statistical Analysis
The aim of the statistical analysis was to determine if some the variables considered had a significant difference between the pre- and post-operative period and if some of these were predictive of a better outcome. The statistical study was carried out using the STATA software applying the McNemar Test. Univariate and multivariate analysis were performed, considering a p-value lower than 0.05 as the significant cut-off.
5. Results
Our study included 26 patients undergoing decompressive craniotomy for supratentorial cerebral ischemia. Sixteen were males (59.25%) and 10 were females (40.74%). At clinical onset of the ischemic event, 1 patient was less than 30 years old, 5 were between 31 and 50 y (18,5%), 16 between 51 and 70 y (62,9%) and 4 patients were older than 70 y (14,8%). The age distribution was between 26 to 80 y, with a mean age of 58.7. The medical records showed that 50% of the patients had already presented a cardiovascular event in the previous years (myocardial stroke, previous stroke, etc), while the remaining had no history of these conditions (50%). The preoperative comorbidities that the patients presented were also analyzed and in detail they were distributed as follows: diabetes mellitus in 46.1% of cases, arterial hypertension in 69.2%, dyslipidemia in 57.7%, neoplasms in 19.2%, hereditary coagulation disorders (such as hyperhomocysteinemia) in 26.9% where patients had at least one mutation, autoimmune disorders in 15.4% and overweight/obesity in more than half of the patients (57.7%). The preoperative GCS was < 8 in the majority of cases (88.5%), while in the remaining it was of moderate severity (between 8 and 12) (Table 1). In the post-operative period, the syndrome of the trephined occurred in 3.8% of cases and a systemic infection in 57.7%. No patient experienced hemorrhage requiring redo surgery and we did not have any surgical site infection. (Table 1).
Concerning the post-operative outcome, the evaluation with the MRS (Modified Rankin Scale) was performed at 3, 6 months and at one year after decompressive surgery, when all the patients who had survived had repositioned the bony flap. Assuming a value of MRS equal to or less than 4 as a cut-off for good / acceptable post-operative outcome, the patients who belonged to this category were 11, distributed as follows; 2 patients in MRS 2 (61 and 58 years), 5 in MRS 3 (31, 58, 42, 52, 80 years) and 4 patients in MRS 4 (70, 58, 50, 68 years). The mean age of these eleven patients was 57.1 years (range 31-80 y.o.). (Graphic 1).
Six patients were female and 5 were male. Six of these 11 patients underwent preoperative revascularization treatments (pharmacological thrombolysis / endovascular therapy). Regarding the ischemic territory and the affected side, seven patients had an stroke of the MCA in the right side, 3 of the left MCA and only one involving both the left MCA and ACA territories. In the group of patients with MRS equal to or less than 4, the mean volume of ischemic alteration was 412.22 mL and timing of surgery was > 48 hours from admission in six cases and in the remaining was < 48 hours. (Table 2).
The univariate statistical analysis focused on the neuroradiological parameters, studied in both pre- and post-operative CT scans. The variables that have proven to be statistically significant are the presence or absence of visible cortical sulci, the possible compression of the basal cisterns in general and in particular of cisterna ambiens, quadrigeminal and sylvian cisterns. Of all these parameters, the only one that maintained statistical significance even in the multivariate analysis was the better visualization of the cisterna ambiens in the post-operative CT scan, which proved to be correlated with the favorable outcome assessed with the MRS scale. This, in our opininion and from our surgical experience, resulted as the main predictive factor for an overall better clinical outcome after decompressive craniectomy surgery (Table 3 and Table 4).
6. Discussion
Malignant middle cerebral artery (MCA) stroke may occur in patients who suffer from acute ischemic stroke up to 10% of cases, and it is associated with high mortality if untreated. Since medical therapies present several limits, decompressive hemicraniectomy has been proposed for patients with space-occupying hemispheric stroke. The rationale lies in allowing the brain parenchyma to herniate outside the craniectomy, reducing intracranial pressure and avoiding internal cerebral herniation, which seriously threatens patient’s life. However, given the lack of reliable data, neurosurgeons could be reluctant to perform this procedure [7]. Performing decompressive craniectomy for malignant middle cerebral artery stroke (mMCAI) is controversial in literature, because it is an emergency neurosurgical procedure for a life-threatening condition whose success is not simply measurable considering only the survival rate. Post-operative quality of life is an important factor in complex elective neurosurgical decision making, but it is not always possible to make an adequate decision-making process in the case of patients in a rapidly deteriorating situation. Based on current evidence, in some cases, decompressive surgery is not only a life-saving therapy but also reduces the incidence of mortality without increasing risk of severe disability [3,8,9]. Optimal timing of DC for malignant cerebral stroke is a main concern. Many studies failed to show a benefit of early DC (within 48 hours of stroke onset) compared with late DC (after 48 hours) [7,10,11,12,13], even if we believe in the concept of “time is brain” which can be applied, in our opinion, in this particular subgroup of neurosurgical emergency cases too. Decompression after the onset of herniation symptoms is less effective or may even be ineffective in reducing mortality and improving neurologic outcome, hence in certain cases with high risk for herniation, early decompressive craniectomy within 24 hours should be considered, rather than waiting for 48 hours or longer. [14,15,16,17,18]. Furthermore, literature has shown that decompressive craniectomy, performed before the occurence of massive edema and brain herniations, not only allows for better preservation of collateral vessels, but also provides a better chance for recanalization in those that have a good collateral supply [19]. In our sample (n=26) ICP was invasively monitored in 15 patients (57%); in 10 cases the value was found to be <= 20 mmHg, , in line with the international literature [42,43]. Alongside severe radiological progression, 5 had ICP > 20 mmHg: surgical treatment was indicated in relation to radiological parameters (ischemic volume, midline shift). The remaining 11 patients did not undergo invasive ICP monitoring: clinical deterioration showing the main signs of malignant endocranial hypertension (intense and worsening headache, nausea and vomiting along with altered state of consciousness; bradycardia, arterial hypertension, and respiratory irregularity and focal neurological deficits) was therefore the indication to perform DC. Although elevated ICP was correlated with higher mortality [20]. ICP monitoring should not be the only parameter in the determination of surgical timing as clinical or radiological signs of deterioration or herniation can precede the increase in ICP [21]. In our experience, in fact, we have performed decompressive craniectomy in patients with cerebral ischemia when the volume of the ischemic territory was significant in terms of parenchymal compression and signs of initial intracranial hypertension occured, in association with a progressive neurological decline of the patient. Moreover, it is unclear which age groups of patients benefit most from the procedure. Vahedi et al. [3] demonstrated that surgery was beneficial independently of age and time to randomization (above and below 24 h) when compared to conservative treatment. Kuroki et al. [22] describe that decompressive surgery outcome is better than the conservative treatment cohort even in patients with more than 70 years old. We agree with the above-mentioned Authors and believe that age should not be considered itself, but comorbidities should be evaluatec: a healthy seventy-year-old patient could be a surgical candidate rather than a 50-year-old patient with several risk factors for example. However, we believe that offering surgery over 80 years, with particular exceptions, is perhaps not worthy for patients in most cases as the risks of post-operative complications are very high and the chances of good recovery are very low [23,24]. In this respect, a review of the literature, taking into account data from both retrospective and prospective analyses, as well as the most recent multicenter randomized trials, indicates unequivocally that age is the strongest predictor of disability and long-term dependence after decompressive hemicraniectomy for hemispheric stroke. Most of the studies report an age cut-off for functional benefit (i.e., survival with independency or acceptable degree of dependency) between 50 and 60 years [25,26,27,28,29,30,31]. Age is an issue, but also the side of ischemia could sometimes lead the surgeon in the position of not offering surgery to the patient. Instead, we believe that stroke side should not be always an exclusion criterion for surgery. We agree with some authors that language deficits may be of small consequence in patients who are severely disabled by hemiplegia; also, non-dominant hemisphere strokes can lead to severe depressive, abulic, or neglect states that may interfere with rehabilitation efforts and are as disabling as aphasia [32,33,34]. On the other side, global disability scales such as the mRS may emphasize mobidity as opposed to language dysfunction. However, although the side is not a discriminating factor, in our series the patients with stroke in the right hemisphere had an overall better outcome. Our manuscript reports the results of a small population of patients who received the diagnosis of ischemic stroke and were subsequently treated with decompressive craniectomy. Results obtained from clinical, blood chemistry, surgical and neuroradiological data were analyzed in order to describe the population and identify which, among all the parameters, could be significant for the purpose of the study. The clinical parameters made it possible to describe the population most affected by ischemic issues. In fact, we found that the risk factors most correlated with ischemic stroke were also present among our patient sample, including hypertension, dyslipidemia and overweight/obesity, as well as a positive history of previous cardiovascular events. The cerebral ischemic event unfortunately represents a serious condition which has consequences on the overall outcome. Haematochemical records were collected, analyzed and studied in detail but no variations were found that could be significant for the purposes of the study or that could appropriately describe the population, also due to a patient selection bias: there was no correlation between the moment in which the event occurred (at night, after a meal, on an empty stomach, in the morning...). Considering the preliminary treatments for DC, certainly, as reported by some studies, they have led to a reduction of the cases that were taken to the operating room for DC, but it has also been highlighted that there are no significant differences between the outcome of patients who underwent mechanical thrombectomy or fibrinolysis before craniectomy [35,36]. The neuroradiological findings were particularly interesting and also significant in statistical terms. The artery most involved in the obstruction is the middle cerebral artery, as also shown in related studies [36,37,38,39,40,41]. Decompressive craniectomy results in an improvement of various radiological parameters studied both pre- and post-operatively, which statistically analyzed. The presence or absence of the cortical sulci (p value 0.045), ambiens (p value 0.019), quadrigeminal (p value 0.002) and sylvian cisterns (p value 0.020) were statistically significant outcome predictors in our series. All these radiological parameters were introduced into the multivariate analysis to understand which most correlated with a favorable outcome. These results certainly add greater definition and validity in the analysis of the outcome of post-decompressive craniectomy, as previous studies had not focused on neuroradiological parameters which were linked to a favorable prognosis. The development of hydrocephalus as evidenced in literature in ischemic stroke treated with DC, in about 38% of patients, with shunt required in ~10%. Due to the small number of patients considered, this occurrence never showed up at the postoperative follow-up, as well as evidence of interhemispheric subdural collections (IHH), which from the literature appears in 23-56% of cases after DC [47]. Only one study by Fatima et al. [40] had considered the radiological factors that improved with the DC and that could be traced back to a more favorable prognosis. In particular, the Authors correlated a GOS-E between 5 and 8 in the long term with the absence in the post-operative CT scans of compression of the cortical sulci, lateral ventricle and absence of hemorrhagic transformation. Our study, in addition to the above-mentioned aspects, aimed to highlight how another parameter such as the better visualization of the ambiens cistern in the post-operative CT scan can help in predicting a favorable functional outcome. Standing to the overall outcome of the procedure, there are various multicenter studies that outline the superiority of the surgical treatment compared to medical treatment alone, like the DECIMAL, DESTINY and HAMLET [18,26,27,41]. As already underlined, it is well demonstrated in the literature that decompressive craniectomy following a severe ischemic stroke, such as the one provoked by middle cerebral artery occlusion, can significantly reduce mortality of patients but at the same time increase long-term disability. Randomized controlled trials (RCTs), including the abovementioned cited DECIMAL, DESTINY and HAMLET have evaluated the efficacy of decompressive craniectomy in patients with malignant ACM stroke. The main evidence included a reduced mortality compared to patients not treated with DC (mortality reduced up to 20-30%) associated to moderate or severe long-term disability. This concept was confirmed by our study, and we highlighted that the caregivers have a central role in the decision-making when surgery is proposed, considering the degree of disability that they can manage and primarily the wishes of the involved patient in terms of acceptable quality of life [36,37,38,40]. Standardization of the surgical indication remains a challenge and our analysis could suggest potentially useful work patterns in daily clinical practice; further studies considering psychosocial, financial and caregiving aspects are needed overcoming the limits of our study where the use of GOSE scale was excluded. Despite the critical issues, decompressive craniectomy remains a viable therapeutic possibility in cases of malignant ACM stroke offering possibilities for partial recovery in selected patients
7. Conclusions
Decompressive craniectomy is a life-saving procedure after malignant brain stroke, but patient selection remains controversial. Age may be a key factor guiding surgical decisions because elderly patients have a significantly higher post-operative mortality rate and worse overall outcome. However, factors other than age should be considered, and the treatment decision should be tailored on every single case. There are several limitations to this study: its retrospective nature and single center experience. In addition, the sample may not have been well represented due to the relatively small cohort of patients and the selection bias may have been introduced because of family-member involvement in the surgical decision making. Moreover, in our opinion, there may be some pitfalls in the evaluation of the postoperative outcome, because the outcome evaluation scores measured only the physical disability, while other factors must also be considered (psychosocial, financial, caregiving context). Surgical management remains in our opinion a tailored choice based on the experience of the surgeon and on the expectations of the patient and family.
References
- Lammy, S; Al-Romhain, B; Osborne, L; St George, EJ. 10-Year Institutional Retrospective Case Series of Decompressive Craniectomy for Malignant Middle Cerebral Artery Stroke (mMCAI). World Neurosurg;Epub 2016, 96, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J; Su, YY; Zhang, Y; Zhang, YZ; Zhao, R; Wang, L; Gao, R; Chen, W; Gao, D. Decompressive hemicraniectomy in malignant middle cerebral artery infarct: a randomized controlled trial enrolling patients up to 80 years old. Neurocrit Care 2012, 17(2), 161–71. [Google Scholar] [CrossRef] [PubMed]
- Vahedi, K; Hofmeijer, J; Juettler, E; Vicaut, E; George, B; Algra, A; Amelink, GJ; Schmiedeck, P; Schwab, S; Rothwell, PM; Bousser, MG; van der Worp, HB; Hacke, W. DECIMAL, DESTINY, and HAMLET investigators. Early decompressive surgery in malignant stroke of the middle cerebral artery: a pooled analysis of three randomised controlled trials. Lancet Neurol 2007, 6(3), 215–22. [Google Scholar] [CrossRef] [PubMed]
- Moughal, S; Trippier, S; Al-Mousa, A; Hainsworth, AH; Pereira, AC; Minhas, PS; Shtaya, A. Strokectomy for malignant middle cerebral artery stroke: experience and meta-analysis of current evidence. J Neurol 2022, 269(1), 149–158. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tartara, F; Colombo, EV; Bongetta, D; Pilloni, G; Bortolotti, C; Boeris, D; Zenga, F; Giossi, A; Ciccone, A; Sessa, M; Cenzato, M. Strokectomy and Extensive Cisternal CSF Drain for Acute Management of Malignant Middle Cerebral Artery Stroke: Technical Note and Case Series. Front Neurol 2019, 10, 1017. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Heiss, WD; Rosner, G. Functional recovery of cortical neurons as related to degree and duration of ischemia. Ann Neurol 1983, 14(3), 294–301. [Google Scholar] [CrossRef] [PubMed]
- Hao, Z; Chang, X; Zhou, H; Lin, S; Liu, M. A Cohort Study of Decompressive Craniectomy for Malignant Middle Cerebral Artery Stroke: A Real-World Experience in Clinical Practice. Medicine (Baltimore) 2015, 94(25), e1039. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wu, J; Wei, W; Gao, YH; Liang, FT; Gao, YL; Yu, HG; Huang, QL; Long, XQ; Zhou, YF. Surgical Decompression versus Conservative Treatment in Patients with Malignant Stroke of the Middle Cerebral Artery: Direct Comparison of Death-Related Complications. World Neurosurg 2020, 135, e366–e374. [Google Scholar] [CrossRef] [PubMed]
- Lin, TK; Chen, SM; Huang, YC; Chen, PY; Chen, MC; Tsai, HC; Lee, TH; Chen, KT; Lee, MH; Yang, JT; Huang, KL. The Outcome Predictors of Malignant Large Stroke and the Functional Outcome of Survivors Following Decompressive Craniectomy. World Neurosurg;Epub 2016, 93, 133–8. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y; Liu, W; Yang, X; Hu, W; Li, G. Is decompressive craniectomy for malignant middle cerebral artery territory stroke of any benefit for elderly patients? Surg Neurol 2005, 64(2), 165–9; discussion 169. [Google Scholar] [CrossRef] [PubMed]
- Harscher, S; Reichart, R; Terborg, C; Hagemann, G; Kalff, R; Witte, OW. Outcome after decompressive craniectomy in patients with severe ischemic stroke. Acta Neurochir (Wien) 2006, 148(1), 31–7; discussion 37. [Google Scholar] [CrossRef] [PubMed]
- Rai, VK; Bhatia, R; Prasad, K; Padma Srivastava, MV; Singh, S; Rai, N; Suri, A. Long-term outcome of decompressive hemicraniectomy in patients with malignant middle cerebral artery stroke: a prospective observational study. Neurol India 2014, 62(1), 26–31. [Google Scholar] [CrossRef] [PubMed]
- Dasenbrock, HH; Robertson, FC; Vaitkevicius, H; Aziz-Sultan, MA; Guttieres, D; Dunn, IF; Du, R; Gormley, WB. Timing of Decompressive Hemicraniectomy for Stroke: A Nationwide Inpatient Sample Analysis. Stroke;Epub 2017, 48(3), 704–711. [Google Scholar] [CrossRef] [PubMed]
- Elsawaf, A; Galhom, A. Decompressive Craniotomy for Malignant Middle Cerebral Artery Stroke: Optimal Timing and Literature Review. World Neurosurg 2018, 116, e71–e78. [Google Scholar] [CrossRef] [PubMed]
- Mori, K; Nakao, Y; Yamamoto, T; Maeda, M. Early external decompressive craniectomy with duroplasty improves functional recovery in patients with massive hemispheric embolic stroke: timing and indication of decompressive surgery for malignant cerebral stroke. Surg Neurol 2004, 62(5), 420-9; discussion 429-30. [Google Scholar] [CrossRef] [PubMed]
- Schwab, S; Steiner, T; Aschoff, A; Schwarz, S; Steiner, HH; Jansen, O; Hacke, W. Early hemicraniectomy in patients with complete middle cerebral artery stroke. Stroke 1998, 29(9), 1888–93. [Google Scholar] [CrossRef] [PubMed]
- Wang, KW; Chang, WN; Ho, JT; Chang, HW; Lui, CC; Cheng, MH; Hung, KS; Wang, HC; Tsai, NW; Sun, TK; Lu, CH. Factors predictive of fatality in massive middle cerebral artery territory stroke and clinical experience of decompressive hemicraniectomy. Eur J Neurol 2006, 13(7), 765–71. [Google Scholar] [CrossRef] [PubMed]
- Hofmeijer, J; Kappelle, LJ; Algra, A; Amelink, GJ; van Gijn, J; van der Worp, HB; HAMLET investigators. Surgical decompression for space-occupying cerebral stroke (the Hemicraniectomy After Middle Cerebral Artery stroke with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol 2009, 8(4), 326–33. [Google Scholar] [CrossRef] [PubMed]
- Yoo, BR; Yoo, CJ; Kim, MJ; Kim, WK; Choi, DH. Analysis of the Outcome and Prognostic Factors of Decompressive Craniectomy between Young and Elderly Patients for Acute Middle Cerebral Artery Stroke. J Cerebrovasc Endovasc Neurosurg;Epub 2016, 18(3), 175–184. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Frank, JI. Large hemispheric stroke, deterioration, and intracranial pressure. Neurology 1995, 45(7), 1286–90. [Google Scholar] [CrossRef] [PubMed]
- Schwab, S; Aschoff, A; Spranger, M; Albert, F; Hacke, W. The value of intracranial pressure monitoring in acute hemispheric stroke. Neurology 1996, 47(2), 393–8. [Google Scholar] [CrossRef] [PubMed]
- Kuroki, K; Taguchi, H; Sumida, M; Yukawa, O; Murakami, T; Onda, J; Eguchi, K. Decompressive craniectomy for massive stroke of middle cerebral artery territory; No Shinkei Geka: Japanese, Sep 2001; Volume 29, 9, pp. 831–5. [Google Scholar] [PubMed]
- Mattos, JP; Joaquim, AF; Almeida, JP; Albuquerque, LA; Silva, EG; Marenco, HA; Oliveira, Ed. Decompressive craniectomy in massive cerebral stroke. Arq Neuropsiquiatr 2010, 68(3), 339–45. [Google Scholar] [CrossRef] [PubMed]
- Li, YP; Hou, MZ; Lu, GY; Ciccone, N; Wang, XD; Dong, L; Cheng, C; Zhang, HZ. Neurologic Functional Outcomes of Decompressive Hemicraniectomy Versus Conventional Treatment for Malignant Middle Cerebral Artery Stroke: A Systematic Review and Meta-Analysis. World Neurosurg 2017, 99, 709–725.e3. [Google Scholar] [CrossRef] [PubMed]
- Uhl, E; Kreth, FW; Elias, B; Goldammer, A; Hempelmann, RG; Liefner, M; Nowak, G; Oertel, M; Schmieder, K; Schneider, GH. Outcome and prognostic factors of hemicraniectomy for space occupying cerebral stroke. J Neurol Neurosurg Psychiatry 2004, 75(2), 270–4. [Google Scholar] [PubMed] [PubMed Central]
- Vahedi, K; Vicaut, E; Mateo, J; Kurtz, A; Orabi, M; Guichard, JP; Boutron, C; Couvreur, G; Rouanet, F; Touzé, E; Guillon, B; Carpentier, A; Yelnik, A; George, B; Payen, D; Bousser, MG. DECIMAL Investigators. Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery stroke (DECIMAL Trial). Stroke 2007, 38(9), 2506–17. [Google Scholar] [CrossRef] [PubMed]
- Jüttler, E; Schwab, S; Schmiedek, P; Unterberg, A; Hennerici, M; Woitzik, J; Witte, S; Jenetzky, E; Hacke, W; DESTINY Study Group. Decompressive Surgery for the Treatment of Malignant Stroke of the Middle Cerebral Artery (DESTINY): a randomized, controlled trial. Stroke 2007, 38(9), 2518–25. [Google Scholar] [CrossRef] [PubMed]
- Rabinstein, AA; Mueller-Kronast, N; Maramattom, BV; Zazulia, AR; Bamlet, WR; Diringer, MN; Wijdicks, EF. Factors predicting prognosis after decompressive hemicraniectomy for hemispheric stroke. Neurology 2006, 67(5), 891–3. [Google Scholar] [CrossRef] [PubMed]
- Maramattom, BV; Bahn, MM; Wijdicks, EF. Which patient fares worse after early deterioration due to swelling from hemispheric stroke? Neurology 2004, 63(11), 2142–5. [Google Scholar] [CrossRef] [PubMed]
- Holtkamp, M; Buchheim, K; Unterberg, A; Hoffmann, O; Schielke, E; Weber, JR; Masuhr, F. Hemicraniectomy in elderly patients with space occupying media stroke: improved survival but poor functional outcome. J Neurol Neurosurg Psychiatry 2001, 70(2), 226–8. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Woertgen, C; Erban, P; Rothoerl, RD; Bein, T; Horn, M; Brawanski, A. Quality of life after decompressive craniectomy in patients suffering from supratentorial brain ischemia. Acta Neurochir (Wien) Epub. 2004, 146(7), 691–5. [Google Scholar] [CrossRef] [PubMed]
- Solomon, NA; Glick, HA; Russo, CJ; Lee, J; Schulman, KA. Patient preferences for stroke outcomes. Stroke 1994, 25(9), 1721–5. [Google Scholar] [CrossRef] [PubMed]
- Walz, B; Zimmermann, C; Böttger, S; Haberl, RL. Prognosis of patients after hemicraniectomy in malignant middle cerebral artery stroke. J Neurol 2002, 249(9), 1183–90. [Google Scholar] [CrossRef] [PubMed]
- Kerkhoff, G. Spatial hemineglect in humans. Prog Neurobiol 2001, 63(1), 1–27. [Google Scholar] [CrossRef] [PubMed]
- Göttsche, J; Flottmann, F; Jank, L; Thomalla, G; Rimmele, DL; Czorlich, P; Westphal, M; Regelsberger, J. Decompressive craniectomy in malignant MCA stroke in times of mechanical thrombectomy. Acta Neurochir (Wien) 2020, 162(12), 3147–3152. [Google Scholar] [CrossRef] [PubMed]
- Beez, T; Munoz-Bendix, C; Steiger, HJ; Beseoglu, K. Decompressive craniectomy for acute ischemic stroke. Crit Care 2019, 23(1), 209. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Das, S; Mitchell, P; Ross, N; Whitfield, PC. Decompressive Hemicraniectomy in the Treatment of Malignant Middle Cerebral Artery Stroke: A Meta-Analysis. World Neurosurg 2019, 123, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Mohan Rajwani, K; Crocker, M; Moynihan, B. Decompressive craniectomy for the treatment of malignant middle cerebral artery stroke. Br J Neurosurg 2017, 31(4), 401–409. [Google Scholar] [CrossRef] [PubMed]
- Daou, B; Kent, AP; Montano, M; Chalouhi, N; Starke, RM; Tjoumakaris, S; Rosenwasser, RH; Jabbour, P. Decompressive hemicraniectomy: predictors of functional outcome in patients with ischemic stroke. J Neurosurg 2016, 124(6), 1773–9. [Google Scholar] [CrossRef] [PubMed]
- Fatima, N; Razzaq, S; El Beltagi, A; Shuaib, A; Saqqur, M. Decompressive Craniectomy: A Preliminary Study of Comparative Radiographic Characteristics Predicting Outcome in Malignant Ischemic Stroke. World Neurosurg;Epub 2020, 133, e267–e274. [Google Scholar] [CrossRef] [PubMed]
- Pallesen, LP; Barlinn, K; Puetz, V. Role of Decompressive Craniectomy in Ischemic Stroke. Front Neurol 2019, 9, 1119. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schwab, S; Aschoff, A; Spranger, M; Albert, F; Hacke, W. The value of intracranial pressure monitoring in acute hemispheric stroke. Neurology 1996, 47(2), 393–8. [Google Scholar] [CrossRef] [PubMed]
- Poca, MA; Benejam, B; Sahuquillo, J; Riveiro, M; Frascheri, L; Merino, MA; Delgado, P; Alvarez-Sabin, J. Monitoring intracranial pressure in patients with malignant middle cerebral artery infarction: is it useful? J Neurosurg 2010, 112(3), 648–57. [Google Scholar] [CrossRef] [PubMed]
- Vahedi, K; Vicaut, E; Mateo, J; Kurtz, A; Orabi, M; Guichard, JP; Boutron, C; Couvreur, G; Rouanet, F; Touzé, E; Guillon, B; Carpentier, A; Yelnik, A; George, B; Payen, D; Bousser, MG. DECIMAL Investigators. Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECIMAL Trial). Stroke 2007, 38(9), 2506–17. [Google Scholar] [CrossRef] [PubMed]
- Fotakopoulos, G; Gatos, C; Georgakopoulou, VE; Lempesis, IG; Spandidos, DA; Trakas, N; Sklapani, P; Fountas, KN. Role of decompressive craniectomy in the management of acute ischemic stroke (Review). Biomed Rep. 2024, 20(2), 33. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hofmeijer, J; Kappelle, LJ; Algra, A; Amelink, GJ; van Gijn, J; van der Worp, HB; HAMLET investigators. Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol 2009, 8(4), 326–33. [Google Scholar] [CrossRef] [PubMed]
- De Bonis, P; Sturiale, CL; Anile, C; Gaudino, S; Mangiola, A; Martucci, M; Colosimo, C; Rigante, L; Pompucci, A. Decompressive craniectomy, interhemispheric hygroma and hydrocephalus: a timeline of events? Clin Neurol Neurosurg 2013, 115(8), 1308–12. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Example of a supratentorial cerebral ischemic stroke (left image, white arrow) and typical intraoperative view during decompressive craniectomy (right image).
Figure 1.
Example of a supratentorial cerebral ischemic stroke (left image, white arrow) and typical intraoperative view during decompressive craniectomy (right image).
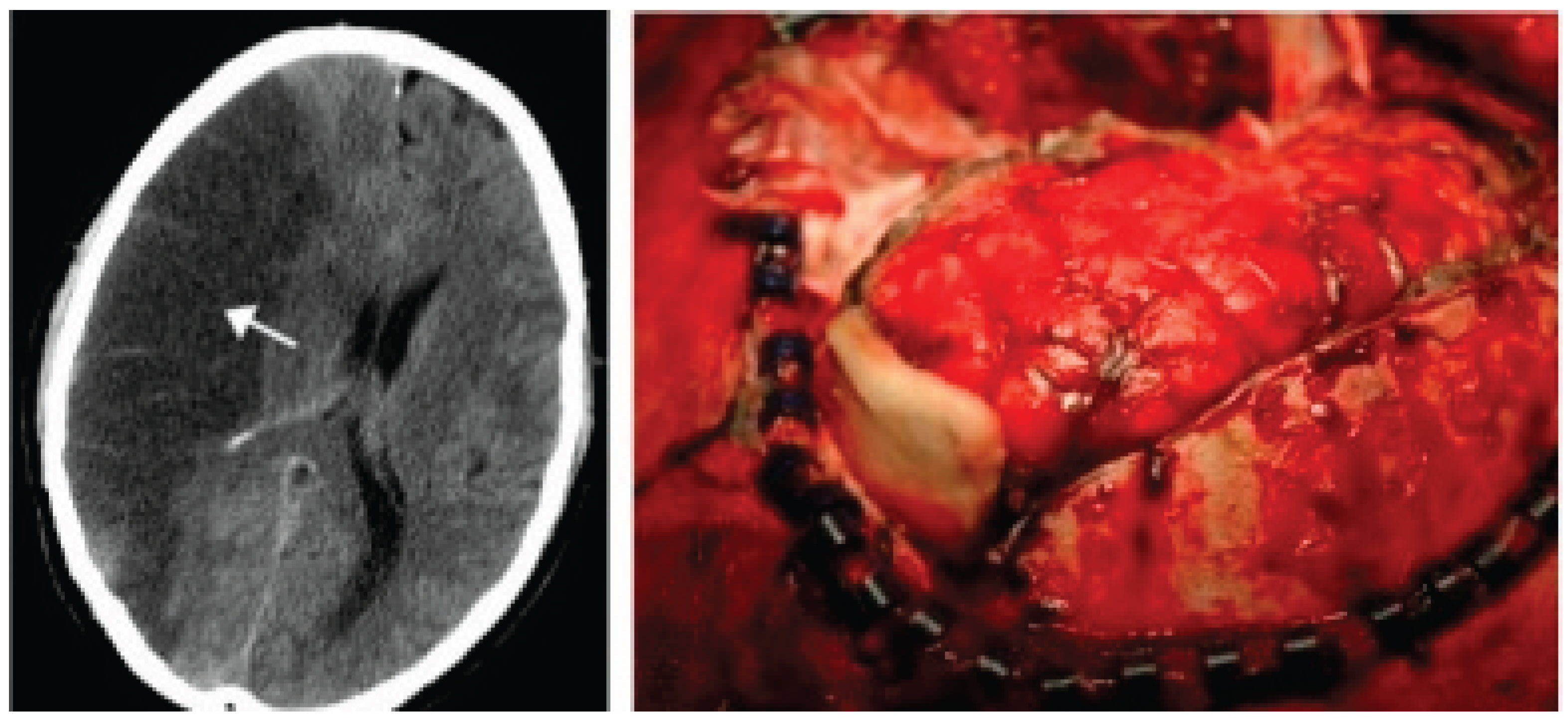

Table 1.
Patients overview. °DS: standard deviation, *GCS score: Glasgow Coma Scale, ∞GOS-E score: Glasgow Outcome Scale Extended.
Table 1.
Patients overview. °DS: standard deviation, *GCS score: Glasgow Coma Scale, ∞GOS-E score: Glasgow Outcome Scale Extended.
| Characteristics | Patients (n=26) |
|---|---|
| Sex male (n,%) female (n,%) |
16 (59.25) 10 (40.74) |
| Age (years, mean±DS°) | 58.7±13.6 |
| Anamnestic data Precedent cardiovascular event (n,%) Diabetes (n,%) Hypertension (n,%) Dyslipidemia (n,%) Neoplastic pathology (n,%) Hereditary coagulation pathology (n,%) Autoimmune disorders (n,%) Overweight/Obesity (n,%) |
13 (50) 12 (46.1) 18 (69.2) 15 (57.7) 5 (19.2) 7 (26.9) 4 (15.4) 15 (57.7) |
| Preoperative GCS score * < 8 (n,%) 8-12 (n,%) > 12 (n,%) Postoperative complication Syndrome of the trephined (n,%) Systemic infection (n,%) Redo surgery for hemorrhage (n,%) Surgical site infection (n,%) |
23 (88.5) 3 (11.5) 0 (0) 1 (3.8) 15 (57.7) 0 (0) 0 (0) |
Table 2.
Patients with MRS <4. °DS: standard deviation.
| Characteristics | Patients (n=11) |
|---|---|
| Sex Male (n,%) Female (n,%) Revascularization treatments (n,%) Territory of ischemia Right CMA (n,%) Left CMA (n,%) Left CMA and ACA (n,%) |
5 6 6 (23.1) 7 (63.6) 3 (27.3) 1 (9.0) |
| Volume of ischemic alteration (mm3, mean ±DS°) Timing of surgery from admission (n,%) < 48 hours > 48 hours |
412.2±194.6 5 (45.5) 6 (54.5) |
Table 3.
Pre and postoperative radiological data.
| Characteristics | Pre-operative | Post-operative | p-value (< 0.05) |
|---|---|---|---|
| Midline shift Compression of curtical sulci Obliteration of basal cystern of quadrigeminal cystern of ambiens cystern of Silvian cystern |
20 21 14 22 23 |
17 16 5 13 13 |
0.179 0.045 0.002 0.019 0.020 |
Table 4.
Multivariate analysis.
| Variables | Coef. | Std Error | t | P value | IC 95% |
|---|---|---|---|---|---|
| Presence of curtical sulci Obliteration of basal cystern of quadrigeminal cystern of ambiens cystern of Silvian cystern |
-0.282 0.560 -1.817 -0.202 |
0.615 0.739 0.786 0.788 |
-0.46 0.76 -2.31 -0.26 |
0.652 0.459 0.034 0.459 |
-1.587/1.021 -1.007/2.128 -3.485/-0.150 -1.007/2.128 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



