
Submitted:
08 January 2026
Posted:
09 January 2026
You are already at the latest version
Abstract
Background: Accurate and consistent measurement of physical activity (PA) is essential for evaluating interventions, informing clinical and public health decision-making, and enabling comparisons across populations. Wearable device–based measures are increasingly used to quantify PA, but the extent to which populations at risk of health inequity, as defined by established equity frameworks, are represented in wearable-based PA studies, and whether measurement protocols are appropriate and comparable across these groups, remains insufficiently characterised. Aim: To synthesise evidence on the use of wearable devices for measuring PA in populations at risk of health inequity, as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks, and to identify methodological features relevant to equity in PA measurement. Methods: A scoping review was conducted in accordance with PRISMA-ScR guidelines. PubMed, Scopus, Web of Science, and grey literature were searched for peer-reviewed randomised controlled trials published between January 2020 and October 2025. Eligible studies quantitatively measured PA using pedometers, accelerometers, or smartwatches in populations at risk of health inequity. Data were extracted on study design, population characteristics, device type and placement, monitoring protocols, and equity-related considerations. Results: Of 1,027 records screened, 13 studies met inclusion criteria. Wrist-worn pedometers and hip-worn accelerometers were most common. Adaptations were minimal and largely limited to language translation. Several high-risk equity groups according to the frameworks used including LGBTQ+, people experiencing homelessness, those with learning difficulties, substance misuse, and justice system involvement were absent. Conclusions: This review demonstrates that wearable-based PA measurement has been applied to only a narrow subset of populations at risk of health inequity, with notable gaps across several key PROGRESS-Plus and CORE20PLUS5 groups. Methodological adaptations to support equitable measurement were uncommon and largely superficial, raising concerns about the appropriateness, acceptability, and comparability of PA data generated in these contexts. Addressing these methodological and reporting deficiencies is essential to strengthen the evidence base and prevent the widening of inequities in PA surveillance and intervention evaluation.
Keywords:
underserved populations
; accelerometery
; self-reported
; MVPA
; sedentary behaviour
; measurement validity
; health equity
Background
Physical activity (PA), defined as ‘any bodily movement from skeletal muscles that uses energy’ (WHO 2024) [1], reduces the risk of premature mortality and contributes to the prevention and management of conditions including cardiovascular disease, Type 2 diabetes, and several cancers, while supporting mental health and overall well-being [1,2,3,4]. Given its central role in health, accurate and consistent measurement of PA is essential for evaluating interventions, understanding exposure–response relationships, and informing clinical and public health decision-making [5,6]. The most commonly used wearable devices - accelerometers, pedometers, and smart watches [7] enable quantification of PA intensity, duration, and frequency while reducing recall bias relative to self-report [8].
However, the validity and feasibility of these methods are influenced by device characteristics, wear-time adherence, and data-processing decisions [9,10], and these factors may vary across social groups where socioeconomic disadvantage, digital exclusion, language or literacy barriers, multimorbidity, or differing occupational and cultural activity patterns shape PA behaviour [11,12,13,14,15]. Differences in measurement performance may therefore limit comparability of PA estimates across populations and contribute to uncertainty in surveillance and intervention evaluation [16].
These methodological concerns sit alongside persistent inequities in PA participation. Substantial proportions of adults and adolescents worldwide do not achieve recommended PA levels [1,17], and participation remains socially patterned by age, sex, socioeconomic status, disability, ethnicity, and geography [18]. Frameworks such as PROGRESS-Plus and CORE20PLUS5 were developed to support systematic identification of populations at risk of health inequity [19,20] - outlined in Figure 1 and Figure 2 - yet previous reviews indicate that such groups remain under-represented in PA intervention research, with limited inclusion of co-production approaches [21]. Individuals experiencing socioeconomic disadvantage, multimorbidity, or constrained living conditions may also face barriers to PA participation, including limited facilities, transport and environmental challenges, competing priorities, and restricted access to resources and social support [22,23]. Where equity considerations are not explicitly incorporated into PA research design and measurement protocols, differential uptake, adherence, or data quality may contribute to “intervention-generated inequality” [24].
Although previous reviews have examined the validity and application of the most commonly used wearable PA measures in general populations [8], the extent to which wearable devices are used appropriately and consistently to measure PA in populations at risk of health inequity remains insufficiently characterised. Evidence is limited on whether device selection, wear protocols, data-processing approaches, and reporting practices adequately account for equity considerations, or how these factors influence the robustness and comparability of PA estimates across social groups. This scoping review therefore, aims to examine evidence on the use of wearable devices specifically accelerometers, pedometers and smart watches - to measure physical activity in populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks, and to identify methodological challenges relevant to equity in PA measurement.
Methods
Study Design
This scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-Sc) [25], as outlined in Supplementary Table 1. Standard systematic review methods were adapted to facilitate timely evidence synthesis while maintaining methodological transparency and reproducibility.
Inclusion Criteria
- Peer-reviewed studies published in English between January 2020 and October 2025. The search was restricted to studies published within the last five years (January 2020–October 2025) to ensure relevance to contemporary practice and technology. Wearable devices and associated data-processing algorithms have evolved rapidly, and this timeframe also captures the post-COVID acceleration in digital health adoption, during which wearable-assisted interventions became more widely implemented and equity frameworks such as PROGRESS-Plus and CORE20PLUS5 gained prominence in research design.
- Studies that quantitatively measured PA using wearable devices, including pedometers, accelerometers, and smart watches.
- Studies reporting at least one PA metric (e.g. minutes of moderate-to-vigorous physical activity [MVPA], step count, energy expenditure, light intensity exercise), or sedentary time captured by a wearable device.
- Randomised controlled trials were the only study design included ensure a higher and more consistent level of methodological rigour in study design and reporting. This facilitated comparison of wearable device–based physical activity measurement approaches used in intervention evaluation contexts
Exclusion Criteria
- Non-original research, including reviews, editorials, commentaries, or conference abstracts, observations, protocols, pilot studies, quasi-experiments
- English language restriction was applied to facilitate accurate interpretation and synthesis, as translation of technical content can introduce bias and errors.
Information Sources and Search Strategy
Three databases were searched: PubMed, Scopus, and Web of Science. Search strategies combined controlled vocabulary (MeSH and Emtree) and free-text terms relating to three main concepts: (1) PA and exercise, (2) measurement and monitoring methods, and (3) populations at risk of health inequity. Search terms for physical activity included “physical activity,” “exercise,” “fitness,” “sedentary behaviour,” “sitting time”, “MVPA,” and “step count.” Measurement terms included “accelerometer,” “pedometer,” “wearable device,” “questionnaire,” and “self-report.” Population terms included “underserved,” “low-income,” “minority,” “marginalised,” “health disparities,” and “low-resource.” This was later refined to wearable devices only. The search strategy was developed with input from a clinical and physical activity specialists and piloted in PubMed before being adapted for other databases. Hand searches of grey literature were also conducted.
Study Selection
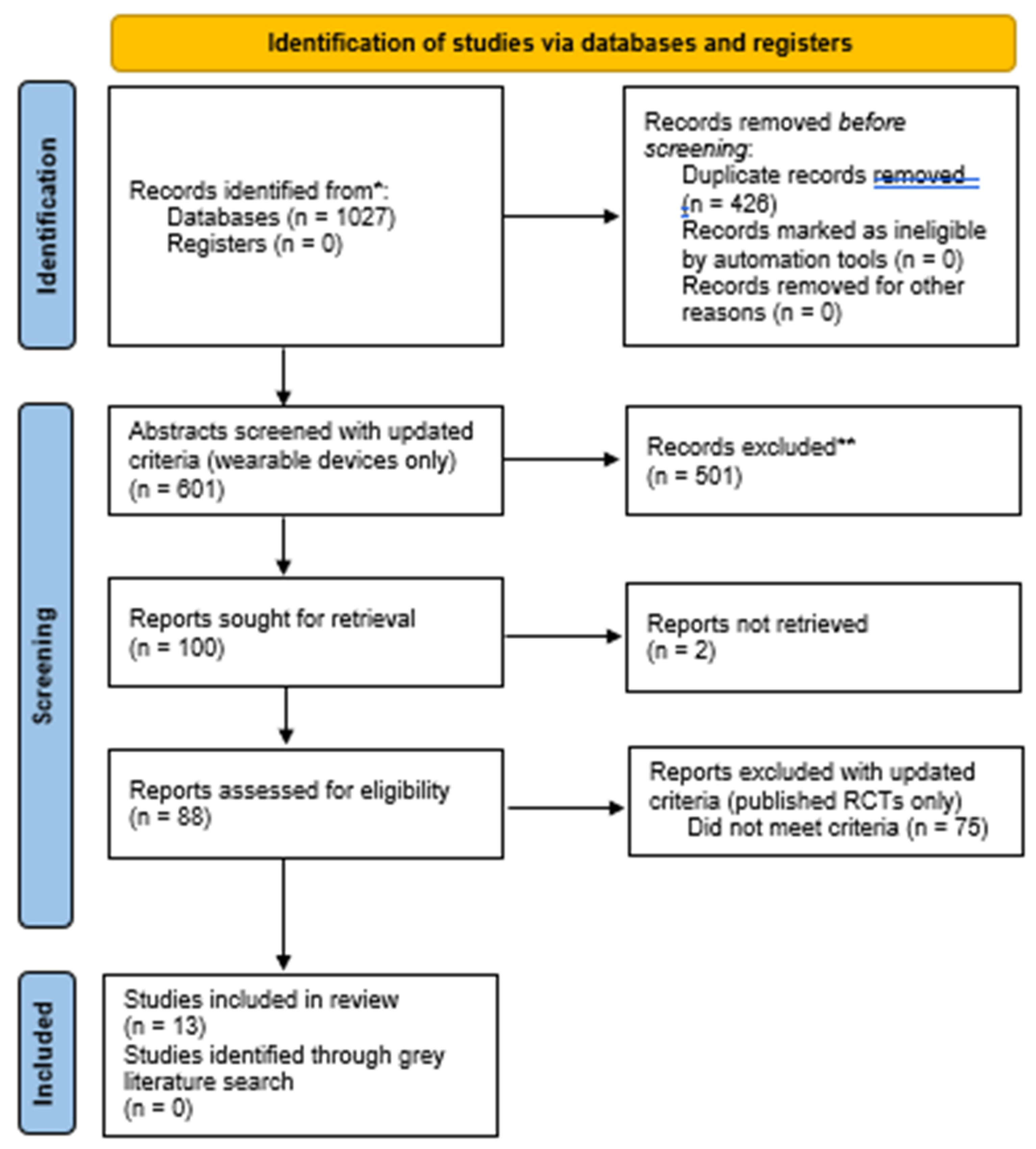
Search results were exported to Rayyan QCRI for deduplication and screening. Two reviewers (LS and LM) independently screened titles and abstracts, followed by full-text assessment against the inclusion criteria. Discrepancies were resolved through discussion with AJ The study selection process is presented in the Figure 1 PRISMA flow diagram.
Data Extraction
Equity-relevant variables were mapped against the PROGRESS-Plus and CORE20PLUS5 frameworks to provide a structured assessment of whether, and to what extent, populations at heightened risk of health inequity were represented in wearable-based PA research. These frameworks were used to allow comparability with existing equity analyses and to ensure systematic, rather than ad-hoc, consideration of social stratifiers. In addition, we documented contextual and implementation factors with potential implications for equitable PA measurement ; such as literacy level, digital access, device affordability and accessibility, cultural or language adaptation, and burden of participation ; to identify barriers that may influence the feasibility, acceptability, and validity of wearable device use in underserved groups. Finally, we extracted information on whether and how study design or implementation incorporated co-production or participatory approaches with underserved communities, recognising that partnership-based research may enhance relevance, inclusion, and methodological appropriateness in equity-focused PA measurement.
Data Synthesis
Given the heterogeneity of study designs, populations, and outcome measures, meta-analysis was not possible. Instead, data were synthesised narratively. Studies were grouped according to measurement approach and population type. Key findings were summarised to identify methodological trends, feasibility considerations, and evidence gaps relevant to PA measurement in populations at risk of health inequity. Formal quality appraisal was not conducted, consistent with accepted scoping review methodology [25].
Results
Our search identified 601 papers, of which 13 were eligible and included in this review, with no additional articles identified through grey literature (Figure 3).
Study Characteristics
The studies mostly spanned high-income countries: the United States (n = 6) and Australia (n = 3). Middle-income countries included China (n = 2), India (n = 1), and South Africa (n = 1). Sample sizes ranged from 64 to over 1,300 individuals, and study duration ranged from 1 week to 2 years. A range of populations at risk of health inequity were assessed, with two involving multiple (ID6,7). At-risk populations included mostly rural communities (n = 5), low-income individuals (n = 3), ethnic minorities (n = 2), and those with cardiovascular disease (n = 2). Migrants (ID7), individuals aged 65+ (ID13), and people with mental illness (ID6) were assessed in one study each. In addition, children and adolescents were the focus in four studies, while three studies specifically assessed women (ID4,7,9).
Findings on Effects of Physical Activity Interventions
Across the 13 included studies, effects on physical activity were mixed. Three studies reported sustained positive outcomes, with long-term improvements in MVPA or adherence among adults with heart failure (ID1), cancer survivors in remote Australia (ID5), and Hispanic adults participating in a culturally tailored dance programme (ID9). One study demonstrated short-term gains that were not maintained, with initial improvements in MVPA among marginalised school-aged children declining by two-year follow-up (ID2). Two studies reported no significant improvement in MVPA, including interventions involving rural older adults in China (although daily steps and grip strength increased) (ID3) and low-income adolescents in Australia, where MVPA was lower in the intervention group than in controls (ID11). The remaining seven studies generally reported short-term positive effects without long-term follow-up, including increased step counts among rural women in India (ID4), adults with heart failure and depression (ID6), rural children in the United States (ID7), rural women in the United States (ID8), low-income children in Australia (ID10), adults aged ≥70 years (ID12), and migrant workers in China (ID13). Effects among children and adolescents from low-income settings (ID10, ID11) were minimal or negative, potentially reflecting limited home engagement and low programme fidelity.
Methodological Features Relevant to Equity in PA Measurement
The included studies used wearable devices to assess a range of physical activity behaviours across diverse equity-relevant populations. Hip-worn accelerometers were most commonly used, particularly in studies involving children, adolescents, and older adults (ID2,3,7,8,10,11,12). Wrist-worn or armband devices were applied in culturally tailored or clinical populations (ID1,5,6,9,13), and thigh-worn devices were used in one rural, low-income setting to better capture posture and ambulatory activity (ID4). In several studies, wearable measurements were supplemented with self-report (ID1,5,7,9), although reporting of data-processing protocols was variable. Equity-relevant subgroup analyses were limited. Only four studies reported stratified analyses, most commonly by sex (ID2,9,11,12), with few assessing other PROGRESS-Plus or CORE20PLUS5 dimensions. Age and sex were routinely described, but socioeconomic indicators such as income, education, or employment were inconsistently reported across studies (e.g. ID1–4,7,9–13), restricting interpretation of differential effects across equity groups. Cultural or contextual adaptation of device use and measurement protocols was inconsistently reported. Adaptations typically involved language translation or rural contextual tailoring (ID3–5,7), addressing literacy or financial barriers (ID1,4), or aligning activity types with cultural preferences such as Latin dance (ID9). Device placement or monitoring parameters were occasionally adapted to participant characteristics or activity type (ID1,4,9). No studies reported consideration of potential bias related to skin tone or body composition. Co-production or participatory involvement of underserved communities was uncommon. Two studies explicitly incorporated co-production into intervention design (ID4,9), and one reported limited formative engagement with participants (ID12). Overall, participatory approaches to support equitable and appropriate wearable-based PA measurement were rarely adopted.
Narrative Synthesis of Recommendations for PA Trials Using Wearables Targeting Health Inequity
The narrative synthesis identified six key recommendations. First, equity considerations should be explicitly integrated into the design and evaluation of wearable-assisted PA interventions, including systematic use of co-production with underserved communities to ensure cultural and contextual relevance (ID1,2,4,6,9). This includes adapting device protocols to local contexts — such as language, attire, and culturally meaningful activity formats, to enhance feasibility and acceptability. Second, trials should prespecify equity-relevant endpoints and conduct stratified analyses to detect differential effects across social groups, as illustrated in adolescent (ID11) and older-adult (ID12) populations. Third, longer monitoring periods or continuous wear protocols are recommended to better capture habitual activity patterns and reduce bias associated with short-term sampling (ID1,9). Fourth, implementation should be supported by structural enablers; for example, adequate training and resources in school settings (ID2), facilitated access to exercise spaces in clinical populations (ID1), and sustained community engagement; to improve participation and data completeness in equity groups. Finally, scalability and reach may be strengthened through policy-level strategies that subsidise wearable technologies and integrate digital coaching within community and public health programmes (ID5,7).
Figure 4.
A visual summary of six key implications for tailoring wearable devices for studies assessing populations at risk of health inequity.
Figure 4.
A visual summary of six key implications for tailoring wearable devices for studies assessing populations at risk of health inequity.


Table 1.
Study characteristics for articles with evidence on use of wearable devices to measure physical activity in populations at risk of health inequity.
Table 1.
Study characteristics for articles with evidence on use of wearable devices to measure physical activity in populations at risk of health inequity.
| Author, year [ID] | Population | Co-production with participants? | Physical activity type | Wearable device type | Study duration | Key findings |
| Alonso et al., 2022 [1] | Adults with heart failure in the US (n = 204) | No | Moderate-intensity continuous aerobic training (40–80% HRR) plus resistance training (10–15 reps to volitional fatigue) taught prerandomization; ongoing independent facility access for 18 months. | Polar heart rate monitor | 18 months | In HFpEF, HEART Camp improved adherence, 6min walk distance, and KCCQ overall/clinical/total symptom scores vs enhanced usual care. |
| Arnaiz et al., 2023 [2] | Low-income children (grades in South Africa (n = 1181) | No | School-based P.E. lessons (once weekly), moving-to-music (once weekly), plus health/nutrition/hygiene education classes | ActiGraph wGT3X-BT | 2 years | Significant intervention effect on MVPA during school hours for physically inactive children, and among active as well as inactive girls. In contrast, the intervention lowered HbA1c and TC to HDL ratio only in children with glucose or lipid values within the norm, respectively. At follow-up, the intervention effects were not maintained in at-risk children, who showed a decline in MVPA, and an increase in BMI-for-age, MAP, HbA1c and TC to HDL ratio. |
| Cai et al., 2022 [3] | Rural adults aged ≥ 60 in China (n = 64) | No | Community walking led by peers + in-person group sessions based on behaviour-change theory | PD03 3D Step Counter | 3 months | (1) Peer support and mobile application-based walking programme increased physical activity and grip strength but not gait speed, chair-rising time, or body composition in rural older Chinese adults. (2) Increases in daily steps were associated with gains in gait speed and decreases in chair-rising time. |
| DiPietro et al., 2024 [4] | Women in rural India (n = 292) | Participatory approach | Habitual movement | ActivPal accelerometer | 6 months | No significant change in overall physical activity (MET-hours/day) or VO₂max. Significant increase in steps/day in the intervention group: about 1,354 more steps/day compared to control. This increase was independent of hemoglobin changes, BMI, or VO₂max. |
| Hardcastle et al., 2024 [5] | Cancer survivors in regional/remote Australia (n = 87) | No | Distance-based intervention combining wearable-guided self-monitoring and telephone health coaching | Fitbit Charge 2, ActiGraph GT9X | 24 weeks | 12 weeks (end-intervention), and 24 weeks (follow-up) [bmjopen.bmj.com], [europepmc.org]Intervention group increased MVPA (~49.8 min/week net; p = 0.007) and MVPA bouts (+39.5 min/week, p = 0.005); both groups improved light PA and sedentary 8behaviour, but no between-group differences there |
| Holber et al., 2022 [6] | Adults with heart failure and depression in the US (n = 222) | No | Free-living daily ambulatory activity post discharge (step counts). | SenseWear® Pro | 1 week | Higher median daily step counts were associated with lower New York Heart Association class and better physical- and HF-specific HRQoL, but not mood symptoms, mental HRQoL, or LVEF. |
| Kim et al., 2022 [7] | Female Korean-Chinese migrant workers in China (n = 120) | No | Walking program with step goals and social support via mobile app | Fitbit Zip or similar clip-on tracker | 24 weeks | There were significant between-group differences regarding the number of steps (B = 1.295, P < .001) and moderate physical activity time (OR = 6.396, P = .030) at week 12. ET group had significant changes in high-density lipoprotein cholesterol (B = 10.522, P = .007), low-density lipoprotein cholesterol (B = -16.178, P = .024), total cholesterol (B = -20.325, P = .039), fasting blood sugar (B = − 8.138, P = -.046). In addition, there was a significant reduction of 10-year CVD risk for the ET group over 12 weeks compared to the ST group (B = -0.521, P<. 001). |
| Kramer-Kostecka et al., 2024 [8] | Rural children in the US (n = 97) | No | Any self-chosen activity (no intervention) | ActiGraph wGT3x-BT, GT3XP-BTLE on right hip (complemented by self reports) | 1 week | On weekdays, the most commonly reported activities were free play (75.3%), biking (37.1%), and walking (37.1%); mean METy-minutes=480±693, 92±210, and 72±233, respectively. On weekends, the most commonly reported activities were free play (61.9%), walking (50.5%), and swimming (29.9%); mean METy-minutes=714±1009, 151±280, and 520±1030, respectively. Farm chores were prevalent and were reported on weekdays (9.2%) and weekends (17.5%). |
| Maddock et al., 2022 [9] | Rural women in the US (n = 182) | SHHC-1.0 created based on focus groups, surveys, and community audits | Twice-weekly experiential 60-minute classes focused on exercise, nutrition, and civic engagement involving progressive strength training and aerobic exercise |
ActiGraph GT3XE on hip (complemented by self reports) | 24 weeks | SHHC-2.0 intervention increased physical activity level and related outcome measures compared to controls and SHHC-1.0 |
| Márquez et al., 2022 [10] | Hispanic adults in the US (n = 333) | Proficient participants became volunteer dance instructors during maintenance period | Hour long sessions of Merengue, Cha Cha Cha, Bachata, and Salsa twice a week | ActiGraph GT3X-Plus on nondominant wrist (complemented by self reports) | 8 months | Dance group to significantly increased their MVPA, dance PA, leisure PA, and total PA at months 4 and 8. Household PA and activity counts from accelerometery data did not demonstrate significant interaction effects. |
| Okely et al., 2020 [11] | Low-income children in Australia (n = 508) | Some activities are child-led | Structured gross motor lessons, music-based activities, activities designed to connect learning and movement | Actigraph GT1M, GT3X+, GT3X | 18 months | There were no significant intervention effects on mins/hr. spent in physical activity (adjusted difference = − 0.17 mins/hr., 95% CI (− 1.30 to 0.97), p = 0.78). A priori sub-group analyses showed a greater effect among overweight/obese children in the control group compared with the intervention group for mins/hr. of physical activity (2.35mins/hr., [0.28 to 4.43], p = 0.036). |
| Ridgers et al., 2021 [12] | Low-income adolescents in Australia (n = 275) | Students provided thoughts on how to integrate wearable activity trackers into a physical activity intervention | Not specified | Fitbit Flex, hip-mounted ActiGraph GT3X+ (complemented by self reports) |
12 weeks | At 6-months post-intervention, adolescents in the intervention group engaged in 5 min (95% CI: − 9.1 to − 1.0) less MVPA per day than those in the wait-list control group. Males in the intervention group engaged in 11 min (95% CI: − 17.6 to − 4.5) less MVPA than males in the wait-list control group at 6-months post-intervention. No significant differences were observed for females at either time point. |
| Sheshadri et al., 2023 [13] | Adults aged 70+ in the US (n = 1381) | No | Moderate intensity structured exercise (walking + strength, flexibility, balance) vs health education | ActiGraph GT3X on hip | 2 years | Randomization to exercise did not change kidney health biomarkers at group level; higher achieved steps were observationally associated with favourable biomarker changes (e.g., ↓urine IL18, NGAL; ↑EGF, uromodulin) |
Table 2.
Key populations, technological challenges, and limitations of articles with evidence on use of wearable devices to measure physical activity in populations at risk of health inequity.
Table 2.
Key populations, technological challenges, and limitations of articles with evidence on use of wearable devices to measure physical activity in populations at risk of health inequity.
| Author, year [ID] | PROGRESS-Plus/CORE20PLUS5 characteristics | Equity-relevant subgroup analysis? | Outcome measurements of wearable device | Duration of wearable device use | Tailoring of device or PA to at risk population? | Reported study limitations | Conclusions/recommendations |
| Alonso et al., 2022 [1] | Cardiovascular disease | No | Average heart rate, minutes within individualised target heart rate zone, minutes below 40% heart rate reserve, weekly minutes of moderate-intensity exercise | During exercise sessions | Personalized heart rate zone, paid access to a hospital-based facility | The article is a secondary analysis of the parent RCT focusing on HFpEF vs HFrEF; conducted at two US urban centers; adherence minutes used selfreport diaries validated by HR monitor; authors note results provide rationale for a larger HFpEF trial (i.e., not powered for clinical events). (Limitations not listed in a dedicated section) | A multicomponent behavioural intervention improved long-term exercise adherence, physical function, and PROs in HFpEF and supports conducting a large HFpEF clinical trial to confirm findings and refine delivery mechanisms. |
| Arnaiz et al., 2023 [2] | Low-income | Yes, by sex | Daily and school-time MVPA (minutes/day), device wear-time minutes | 7 consecutive days at baseline, post-intervention, follow-up | Culturally adapted toolkit | Limited long-term sustainability; follow-up only for at-risk sub-cohort; potential wear-time compliance issues; non-randomized follow-up; pandemic effects unclear. | Schools are key settings in which to promote PA and improve health; however, structural changes are necessary to ensure that effective interventions reach marginalized school populations and achieve sustainable impact. |
| Cai et al., 2022 [3] | Rural, predominantly 65+ | No | Daily walking steps | 3 consecutive days at baseline and post-intervention | App adapted to rural context | Small sample; short duration; pedometer worn only 3 days; no SES subgrouping; limited generalizability beyond rural China | Peer support and mobile application-based walking programme improved physical activity and physical function in rural older adults. |
| DiPietro et al., 2024 [4] | Rural | No | Daily step count, sitting, standing, reclining time, MET-hours/day | 3 consecutive days | Delivered in local language (Odiya), addressed barriers like low literacy and gender norms through group sessions and social norms messaging, lowered height step due to small stature and sari attire of participants | Short duration of accelerometer wear (3 days) may not reflect habitual activity. QCST provides indirect VO₂max estimates, less accurate than lab tests. No significant change in overall physical activity or haemoglobin. Limited generalizability beyond rural Odisha. | The potential to modify walking and other health-seeking behaviours using a social norms approach is worthy of further investigation among women living in rural India. |
| Hardcastle et al., 2024 [5] | Rural | No | MVPA (minutes/week), MVPA-bouts | 7 consecutive days of accelerometry | Distance-based intervention tailored to regional/remote context | Small sample; high female proportion; no patient co-design; Fitbit not used for primary outcome; MVPA self-reported improvements; mixed improvements on light PA/sedentary; HRQoL improvements limited by high baseline | Distance-based wearable-guided coaching led to clinically meaningful MVPA increases in remote cancer survivors, supporting scalable remote interventions; improvements maintained at 24 weeks. |
| Holber et al., 2022 [6] | Cardiovascular disease, mental illness, predominantly 65+ | No | Median daily steps | 7 days post discharge | No | Cross sectional baseline only; low usable return rate (~42% of those mailed; 35% of all enrolled) with potential selection bias; no MVPA recorded; reliance on mailed devices. | Patients with HF and comorbid depression are generally sedentary after hospital discharge. Although mood symptoms and LVEF were unrelated to objective PA, patients with higher step counts self-reported better HRQoL. |
| Kim et al., 2022 [7] | Migrants, ethnic minority | No | Daily step count, adherence | 24 weeks | App culturally adapted (Korean-Chinese language | Small sample; single region; self-reported diet; device wear compliance not objectively verified | Long-term studies are needed to reduce the risk of cardiovascular disease in large-scale migrant workers and to confirm the direct and indirect effects of social-cognitive determinants on health outcomes. |
| Kramer-Kostecka et al., 2024 [8] | Rural | No | Youth metabolic equivalent of task (METy, (activity-specific energy costs), METy-minute values (activity-specific energy costs over a given duration), MVPA | 7 consecutive days except when sleeping or during water-based activities | No | Not generalisable, self-report bias, no consideration of seasonal changes | Compendia expansion work is needed to include activities commonly reported by rural youth |
| Maddock et al., 2022 [9] | Rural | Yes, subsample of 60+ | MVPA | 7 consecutive days (except when sleeping or during water-based activities) | No | Limited ethnic diversity, short study duration, poor adherence, attrition | Future research should focus on testing this intervention in more diverse populations across the United States. The feasibility of dissemination of this intervention throughout state Extension networks should be explored. |
| Márquez et al., 2022 [10] | Ethnic minority, predominantly 65+ | No | Total PA counts | 7 days at baseline and intervention | On wrist instead of waist, Latin dance | Single area, control group received health education, possible contamination, unsure of effects different device location, under-dosage | Efforts are needed to make dancing programs available and accessible, and to find ways for older Latinos to add more PA to their daily lives. |
| Okely et al., 2020 [11] | Low income | Yes, by sex, age | Mins/hours spent in PA | 7 consecutive days (except during sleep and water-based activities) | No | Measures only during childcare hours, low implementation home components | Increasing fidelity may result in higher levels of physical activity when outcomes are assessed at 18-months. |
| Ridgers et al., 2021 [12] | Low income (area lowest 50%, income not reported) | Yes, by sex | MVPA | 8 consecutive days | No | Limited self-monitoring, low compliance with accelerometer, limited generalisability | Future research is needed to better understand whether wearable activity trackers combined with appropriately engaging digital resources can effectively promote physical activity for adolescents, particularly for males |
| Sheshadri et al., 2023 [13] | 65+ years | No | Daily step count, minutes of moderate-intensity PA | 7 days at baseline, 6, 12, 24 months | Exercise designed for older adults | Original LIFE not designed for kidney outcomes; non-White and advanced CKD under-represented in biomarker analysis | Exercise assignment didn’t change kidney biomarkers overall, but more daily steps were associated with favorable biomarker shifts—supporting increasing PA volume in older adults; future trials should pre-specify kidney endpoints |
Discussion
This review synthesised evidence on wearable device–based measurement of PA in populations at risk of health inequity, mapped to the PROGRESS-Plus and CORE20PLUS5 frameworks, and examined methodological features relevant to equitable measurement. Thirteen studies were identified, predominantly involving rural communities, with additional focus on low socioeconomic status, ethnic minority groups, cardiovascular disease, severe mental illness, migrant status, and older age. Representation was uneven, with no studies including people with long-term conditions outside cardiovascular disease, LGBTQ+ populations, people experiencing homelessness, individuals with learning disabilities, or those with justice system involvement or substance use. Co-production and equity-relevant subgroup analyses were rare. Device type, placement, and activity protocols varied across populations, emphasising the need for context-sensitive measurement approaches. Although some cultural adaptations were reported, none addressed potential bias related to skin tone or body composition. Overall, wearable devices are increasingly used in equity-relevant populations, but methodological inconsistency and limited equity-focused adaptation constrain accuracy and comparability, highlighting the need for more systematic integration of equity considerations in study design and reporting.
Comparison to Existing Literature
Prior research has highlighted a systemic lack of consideration for low-income and ethnic minority populations in the design and development of wearable technologies [39]. For example, accuracy limitations in devices such as the Apple Watch and Fitbit have been reported for individuals with darker skin tones [40]. Our review indicates that these equity concerns remain insufficiently addressed in contemporary PA measurement studies using wearables. Similarly, most devices are validated in younger populations, and their accuracy in older adults—who may differ in body composition and mobility—remains uncertain [41], yet this issue was not considered in the included studies.
Barriers such as digital health literacy, device ownership, and internet access are well-established in PA interventions [42], and targeted approaches to strengthen digital engagement have been shown to improve outcomes [43]. However, none of the included studies incorporated these factors. Cultural tailoring was also limited. Meaningful adaptation requires consideration of cultural values, social context, and relational norms, beyond simple language translation [44,45]. Aside from one study that addressed cultural attire, tailoring rarely extended beyond translation, reflecting patterns previously noted in the literature [46].
Co-production with marginalised communities - widely recommended to enhance relevance and acceptability [47] - was infrequently applied, aligning with earlier findings that co-production remains uncommon in wearable-focused research involving low-income and ethnic minority populations [48]. Collectively, these gaps highlight the need for participatory and equity-informed approaches in the design and implementation of wearable-based PA studies [49].
Several equity groups were absent across the 13 studies, including LGBTQ+ populations, who are consistently found to engage less in PA [50]; individuals with learning disabilities, who experience very low activity levels [51]; and people with experience of the justice system, where limited PA research exists outside custodial rehabilitation settings [52]. People experiencing homelessness were also not represented, consistent with previous reviews [53]. Ongoing exclusion of these populations’ risks perpetuating inequities and limits opportunities to use PA interventions involving wearables to support psychological and social wellbeing among those who may benefit most [54].
Strengths and Limitations
To our knowledge, this is the first review to apply the PROGRESS-Plus and CORE20PLUS5 frameworks to systematically characterise representation of populations at risk of health inequity in studies using wearable devices to measure physical activity. By focusing specifically wearable-based PA measurement within an equity lens, this review provides contemporary evidence aligned with current policy priorities emphasising a shift toward digitally enabled, prevention-focused health systems [55]. It also moves beyond outcome reporting to identify methodological gaps and propose actionable recommendations to strengthen equity integration and reproducibility in future research.
This review has limitations. Selection and extraction bias are possible, and restriction to English-language, peer-reviewed publications may have limited global representation. We included only randomised controlled trials; while this ensured a high standard of evidence, it may have excluded quasi-experimental and observational studies that frequently involve at-risk populations, thereby narrowing the scope of synthesis.
Our focus on three wearable device categories - pedometers, accelerometers, and smartwatches - reflects their widespread use, validation, and accessibility in physical activity research and applied settings [7]. Other technologies (e.g., multisensor armbands, GPS watches, smart rings, textile-based sensors) were not included and some relevant studies may therefore have been omitted. Finally, use of a scoping review methodology without formal quality appraisal may limit interpretation of the evidence base [56].
Policy Implications and Conclusion
To reduce health inequities, wearable-assisted physical activity research and implementation must move beyond uniform approaches that assume devices perform similarly across populations. Policymakers and researchers should prioritise culturally and contextually tailored programmes, consider subsidising or providing wearable devices for low-income groups, and embed digitally enabled behaviour-change support within community and primary care services. Equity frameworks such as PROGRESS-Plus and CORE20PLUS5 should be applied prospectively to guide study design, recruitment, analysis, and reporting. Meaningful co-production with underserved communities, alongside structural supports that address barriers such as digital literacy and access, will be essential to ensure that wearable technologies are acceptable, scalable, and capable of delivering sustained public health benefit.
Author Contributions
Conceptualisation: LVM, LS, JF, JK, HDM; methodology: LVM, LS, HDM; data collection: LVM, LS; data extraction: LVM, AJ; data analysis: LVM, LS; writing and review: LS, LVM, AJ, JF, JK, HDM.
Funding
This report is independent research funded by the National Institute for Health Research (Artificial Intelligence for Multiple Long-Term Conditions (AIM), “The development and validation of population clusters for integrating health and social care: A mixed-methods study on Multiple Long-Term Conditions,” “NIHR202637”). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. HDM receives funding from the National Institute for Health and Care Research (NIHR) Multiple Long-Term Conditions (MLTC) Cross NIHR Collaboration (CNC) (NIHR207000).
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
All articles utilised are publicly available.
Disclaimer
The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care.
Acknowledgements
Not applicable.
Competing interests
No competing interests declared by all authors.
Appendices
Appendix 1. PRISMA Checklist for the Presented Review of Trials with Evidence on Use of Wearable Devices to Measure Physical Activity in Populations at Risk of Health Inequity as Defined by the PROGRESS-Plus and CORE20PLUS5 Frameworks
| SECTION | ITEM | PRISMA-ScR CHECKLIST ITEM | REPORTED ON PAGE # |
| TITLE | |||
| Title | 1 | Identify the report as a scoping review. | Front page of article |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | 1-2 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 3-4 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 3-4 |
| METHODS | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | No formal review protocol |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 5-6 |
| Information sources* | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 6 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | 6,33 |
| Selection of sources of evidence† | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | 6-7 |
| Data charting process‡ | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | 6 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 6,7,12-18 |
| Critical appraisal of individual sources of evidence§ | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | Not completed |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 7 |
| RESULTS | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | 7-8 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | 8-9 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | Not conducted as not part of scoping review methodology |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | 9-10 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | 10-11 |
| DISCUSSION | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | 19 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | 20 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 21 |
| FUNDING | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | 22 |
| JBI = Joanna Briggs Institute; PRISMA-ScR = Prefe rred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews. * Where sources of evidence (see second footnote) are compiled from, such as bibliographic databases, social media platforms, and Web sites. † A more inclusive/heterogeneous term used to account for the different types of evidence or data sources (e.g., quantitative and/or qualitative research, expert opinion, and policy documents) that may be eligible in a scoping review as opposed to only studies. This is not to be confused with information sources (see first footnote). ‡ The frameworks by Arksey and O’Malley [6] and Levac and colleagues [7] and the JBI guidance [4,5] refer to the process of data extraction in a scoping review as data charting. § The process of systematically examining research evidence to assess its validity, results, and relevance before using it to inform a decision. This term is used for items 12 and 19 instead of "risk of bias" (which is more applicable to systematic reviews of interventions) to include and acknowledge the various sources of evidence that may be used in a scoping review (e.g., quantitative and/or qualitative research, expert opinion, and policy document). From: Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann Intern Med. 2018;169:467–473. doi: 10.7326/M18-0850. | |||
Appendix 2. Search Terms to Systematically Identify Trials with Evidence on Use of Wearable Devices to Measure Physical Activity in Populations at Risk of Health Inequity as Defined by the PROGRESS-Plus and CORE20PLUS5 Frameworks Before Refinement
| MeSH and Free Text Search Terms | Filters/Refined by | Databases |
| (“physical activity” OR “physical activities” OR “exercise” OR “exercising” OR “workout” OR “working out” OR “fitness” OR “sport” OR “walking” OR “cycling” OR “movement” OR “active travel”) AND (“underserved” OR “under-served” OR “minoritised” OR “minoritized” OR “minority” OR “marginalised” OR “marginalized” OR “disadvantaged” OR “underprivileged” OR “under-privileged” OR “deprived” OR “underrepresented” OR “under-represented” OR “neglected” OR “poverty” OR “impoverished” OR “underresourced” OR “under-resourced” OR “low-income” OR “lower-income” OR “migrant” OR “immigrant” OR “migrants” OR “immigrants” OR “refugee” OR “refugees” OR “asylum seeking” OR “asylum seekers” OR “disabled” OR “queer” OR “LGBTQI+” OR “LGBT” OR “homeless” OR “homelessness” OR “non-White” OR “non-white” OR “rural”) AND (“randomised controlled trial” OR “randomized controlled trial” OR “clinical trial” OR “pragmatic trial” OR “adaptive trial” OR “cluster trial” OR “evaluation study” OR “quasi-experimental study” OR “experimental study” OR “empirical study” OR “observational study” OR “experimental study” OR “secondary study” OR “quantitative study”) AND (“sedentary” OR “sitting” OR “MVPA” OR “step” OR “steps” OR “accelerometer” OR “accelerometery” OR “accelerometry” OR “accelerometric” OR “accelerometers” OR “pedometer” OR “pedometric” OR “pedometers” OR “pedometry” OR “wearable device” OR “smart device” OR “smartwatch” OR “smart watch” OR “fitbit” OR “questionnaire” OR “self-report” OR “self report” OR “self reported” OR “survey”)) |
Restricted to the English language, RCTs using wearable device for PA measurement, populations at risk of health inequity only | PubMed (n = 335 before screening) Web of Science (n = 290 before screening) Scopus (n = 402 before screening) |
References
- WHO. Guidelines on physical activity and sedentary behaviour. Geneve: WHO; 2020. Available from: https://www.who.int/publications/i/item/9789240015128.
- Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 2012;380:219–29. [CrossRef]
- Wahid A, Manek N, Nichols M, Kelly P, Foster C, Webster P, et al. Quantifying the association between physical activity and cardiovascular disease and diabetes: a systematic review and meta-analysis. J Am Heart Assoc 2016;5:e002495. [CrossRef]
- Dibben, Grace O.Begum, Samina et al. Evidence for exercise-based interventions across 45 different long-term conditions: an overview of systematic reviews eClinicalMedicine, Volume 72, 102599.
- Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys. Lancet Glob Health 2018;6:e1077–86. [CrossRef]
- Celis-Morales CA, Perez-Bravo F, Ibanez L, Salas C, Bailey ME, Gill JM. Objective vs self-reported physical activity and sedentary time: effects of measurement method on relationships with health outcomes. Int J Epidemiol 2012;41:1328–39. [CrossRef]
- Ferguson, T., et al (2022) Effectiveness of wearable activity trackers to increase physical activity and improve health: a systematic review of systematic reviews and meta-analyses The Lancet Digital Health, Volume 4, Issue 8, e615 - e626=.
- Rowlands AV, Sherar LB, Fairclough SJ, Yates T, Edwardson CL, Harrington DM, et al. A data-driven, meaningful, and interpretable approach to accelerometer processing: the UK Biobank Physical Activity Study. Int J Behav Nutr Phys Act 2022;19:37. [CrossRef]
- Sylvia LG, Bernstein EE, Hubbard JL, Keating L, Anderson EJ. Practical guide to measuring physical activity. J Acad Nutr Diet 2014;114:199–208. [CrossRef]
- Craig CL, Marshall AL, Sjöström M, et al. International Physical Activity Questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 2003;35:1381–95. [CrossRef]
- Rowlands AV, Sherar LB, Fairclough SJ, Yates T, Edwardson CL, Harrington DM, et al. A data-driven, meaningful, and interpretable approach to accelerometer processing: the UK Biobank Physical Activity Study. Int J Behav Nutr Phys Act 2022;19:37. [CrossRef]
- Sylvia LG, Bernstein EE, Hubbard JL, Keating L, Anderson EJ. Practical guide to measuring physical activity. J Acad Nutr Diet 2014;114:199–208. [CrossRef]
- Craig CL, Marshall AL, Sjöström M, et al. International Physical Activity Questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 2003;35:1381–95. [CrossRef]
- Bull FC, Maslin TS, Armstrong T. Global Physical Activity Questionnaire (GPAQ): nine-country reliability and validity study. J Phys Act Health 2009;6:790–804. [CrossRef]
- Shaw PA, Deffner V, Keogh RH, Carroll RJ, Tooze JA, Prentice RL. Measurement error in dietary and physical activity research: past, present, and future opportunities. Stat Med 2022;41:1281–310. [CrossRef]
- Skender S, Ose J, Chang-Claude J, Paskow M, Brühmann B, Siegel EM, et al. Accelerometry and physical activity questionnaires—a systematic review. BMC Public Health 2016;16:515. [CrossRef]
- Kohl HW, Craig CL, Lambert EV, et al. The pandemic of physical inactivity: global action for public health. Lancet 2012;380:294–305. [CrossRef]
- Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys. Lancet Glob Health 2018;6:e1077–86. [CrossRef]
- Oliver S, Kavanagh J, Caird J, Lorenc T, Oliver K, Harden A. Health promotion, inequalities and young people’s health. A systematic review of research. 2008; Available from: http://eppi.ioe.ac.uk/cms/LinkClick.aspx?fileticket=lsYdLJP8gBI%3d&tabid=2412&mid=4471&language=en-US.
- NHS England and NHS Improvement. Core20PLUS5: an approach to reducing health inequalities. Supporting document. London: NHS England; 1 November 2021. Available from: https://www.england.nhs.uk/wp-content/uploads/2021/11/core20plus5-online-engage-survey-supporting-document-v1.pd.
- Veerle Michels L, Smith L, Keast J, Dambha-Miller H (2025) Equity in physical activity interventions to promote health: A scoping review of trials - in preparation.
- Accessed online 18th December 2025: Sport Works Summary Report: 10109795_SW_EXECUTIVE_SUMMARY_A.indd.
- Lorenc T, Petticrew M, Welch V, Tugwell P. What types of interventions generate inequalities? Evidence from systematic reviews. Journal of Epidemiology & Community Health. 2013;67(2):190–193. [CrossRef]
- Valerie J. Silfee, Christina F. Haughton, Danielle E. Jake-Schoffman, Andrea Lopez-Cepero, Christine N. May, Meera Sreedhara, Milagros C. Rosal, Stephenie C. Lemon, Objective measurement of physical activity outcomes in lifestyle interventions among adults: A systematic review, Preventive Medicine Reports, Volume 11, 2018, 74-80, ISSN 2211-3355. [CrossRef]
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018;169:467–73. [CrossRef]
- Alonso et al., 2022. The HEART Camp Exercise Intervention Improves Exercise Adherence, Physical Function, and Patient-Reported Outcomes in Adults With Preserved Ejection Fraction Heart Failure. J Card Fail 28(3):431-442. [CrossRef]
- Arnaiz et al., 2023. Intervention effects and long-term changes in physical activity and cardiometabolic outcomes among children at risk of noncommunicable diseases in South Africa: a cluster-randomized controlled trial and follow-up analysis. Front Public Health 11:1199381. eCollection 2023. [CrossRef]
- Cai et al., 2022. Effects of peer support and mobile application-based walking programme on physical activity and physical function in rural older adults: a cluster randomized controlled trial. European Geriatric Medicine (2022) 13:1187–1195. [CrossRef]
- DiPietro et al., 2024. The Effects of the RANI Project on 6-Month Physical Activity Among Women Living in Rural India: A Randomized-Controlled Trial. Women’s Health Rep 5(1):522-529. [CrossRef]
- Hardcastle et al., 2024. The promoting physical activity in regional and remote cancer survivors (PPARCS) trial: Physical activity maintenance. Scandinavian Journal of Medicine and Science in Sports 34(3). [CrossRef]
- Holber et al., 2024. The promoting physical activity in regional and remote cancer survivors (PPARCS) trial: Physical activity maintenance. Scandinavian Journal of Medicine and Science in Sports 34(3). [CrossRef]
- Kim et al., 2022. Living labs for a mobile app-based health program: effectiveness of a 24-week walking intervention for cardiovascular disease risk reduction among female Korean-Chinese migrant workers: a randomized controlled trial. Arch Public Health 80(1), 181.
- Kramer-Kostecka, et al., 2024. From Free Play to Farm Chores: Using the Youth Compendium to Characterize Physical Activity Behaviors Among Rural Children. Health Promotion Practice 26(6). [CrossRef]
- Maddock et al., 2022. Changes in physical activity outcomes in the Strong Hearts, Healthy Communities (SHHC-2.0) community-based randomized trial. Int J Behav Nutr Phys Act 19:159. [CrossRef]
- Marquez et al., 2022. BAILA: A Randomized Controlled Trial of Latin Dancing to Increase Physical Activity in Spanish-Speaking Older Latinos. Ann Behav Med 56(12):1231-1243. [CrossRef]
- Okely et al., 2020. 'Jump start' childcare-based intervention to promote physical activity in pre-schoolers: six-month findings from a cluster randomised trial. Int J Behav Nutr Phys Act 17(1):6. [CrossRef]
- Ridgers et al., 2021. Effect of commercial wearables and digital behaviour change resources on the physical activity of adolescents attending schools in socio-economically disadvantaged areas: the RAW-PA cluster-randomised controlled trial. . International Journal of Behavioral Nutrition and Physical Activity 18:52. [CrossRef]
- Sheshadri et al., 2023. Structured Moderate Exercise and Biomarkers of Kidney Health in Sedentary Older Adults: The Lifestyle Interventions and Independence for Elders Randomized Clinical Trial. Kidney Medicine 5. [CrossRef]
- 44Sheena Erete, Aarti Israni, and Tawanna Dillahunt. 2018. An intersectional approach to designing in the margins. Interactions 25, 3 (2018), 66–69.
- Peter J Colvonen, Pamela N DeYoung, Naa-Oye A Bosompra, and Robert L Owens. 2020. Limiting racial disparities and bias for wearable devices in health science research.
- J Schrack, R Cooper, A Koster, E Shiroma, JMurabito, W Rejeski, L Ferrucci, TB. Harris (2016) Assessing Daily Physical Activity in Older Adults: Unraveling the Complexity of Monitors, Measures, and Methods, The Journals of Gerontology: Series A, Volume 71, Issue 8, August 2016, Pages 1039–1048, . [CrossRef]
- Jaimon T. Kelly, Liam J. Caffery, Emma E. Thomas, Soraia de Camargo Catapan, Anthony C. Smith, Nicole Isbel, Hannah Mayr, Lindsey Webb, Katrina L. Campbell, Graeme A. Macdonald, Jeff S. Coombes, Shelley E. Keating, Ingrid J. Hickman, Determining the digital health literacy and potential solutions to support people with complex chronic conditions to engage with digital models of care, Patient Education and Counseling,Volume 140, 2025, 109278, ISSN 0738-3991. [CrossRef]
- T.S. Busse, J. Nitsche, S. Kernebeck, et al. Approaches to improvement of digital health literacy (eHL) in the context of Person-Centered care Int J Environ Res Public Health, 19 (14) (2022).
- Loya J, Garcia DO, Maldonado A, Villavicencio E. A Culturally Tailored Physical Activity Intervention for Hispanic Adults Living With Type 2 Diabetes: Pre-Post Pilot Feasibility Study. JMIR Diabetes. 2025 Jun 10;10:e62876. PMID: 40493665; PMCID: PMC12173091. [CrossRef]
- 11.Sanders Thompson VL, Ackermann N, Bauer KL, Bowen DJ, Goodman MS. Strategies of community engagement in research: definitions and classifications. Transl Behav Med. 2021 Mar 16;11(2):441–451. [CrossRef]
- .McCurley JL, Gutierrez AP, Gallo LC. Diabetes prevention in U.S. Hispanic adults: a systematic review of culturally tailored interventions. Am J Prev Med. 2017 Apr;52(4):519–529. [CrossRef]
- Nina B Wallerstein and Bonnie Duran. 2006. Using community-based participatory research to address health disparities. Health promotion practice 7, 3 (2006), 312–323.
- EquityWare: Co-Designing Wearables With And For Low Income Communities In The U.S.: Stefany Cruz, Alexander Redding, Connie W. Chau, Claire Lu, Julia Persche, Josiah Hester, Maia JacobsHYPERLINK "https://dl.acm.org/doi/10.1145/3544548.3580980#tab-contributors"Authors Info & Claims CHI '23: Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems Article No.: 277, Pages 1 – 18 . [CrossRef]
- Wearable devices—addressing bias and inequity Zinzuwadia, Aniket et al The Lancet Digital Health, Volume 4, Issue 12, e856 - e857.
- DeFoor, M. T., Stepleman, L. M., & Mann, P. C. (2018). Improving wellness for LGB collegiate student-athletes through sports medicine: A narrative review. Sports Medicine - Open, 4 (1),48. [CrossRef]
- Dairo, YM and others. Physical activity levels in adults with intellectual disabilities: A systematic review. Preventive Medicine Reports, 2016. 4: p. 209-219.
- Norman M, Sonoda J, Ricciardelli R. Sport, Physical Activity, and Young People Who Are Incarcerated: A Scoping Review. Youth Justice. 2024 Aug;24(2):313-336. Epub 2024 Jan 6. PMID: 39119285; PMCID: PMC11303121. [CrossRef]
- Silfee VJ, Haughton CF, Jake-Schoffman DE, Lopez-Cepero A, May CN, Sreedhara M, Rosal MC, Lemon SC. Objective measurement of physical activity outcomes in lifestyle interventions among adults: A systematic review. Preventive Medicine Reports. 2018;11:74–80. [CrossRef]
- Taylor P and others. (2015) A review of the Social Impacts of Culture and Sport.
- NHS England » Fit for the Future: 10 Year Health Plan for England accessed online 6th January 2025.
- Cherie Lucas, Shane P. Desselle (2024) Considerations for conducting a scoping review in pharmacy education, Exploratory Research in Clinical and Social Pharmacy, Volume 14, 100448, ISSN 2667-2766. [CrossRef]
Figure 1.
The CORE20PLUS5 NHS England 2021 Framework[19].
Figure 1.
The CORE20PLUS5 NHS England 2021 Framework[19].
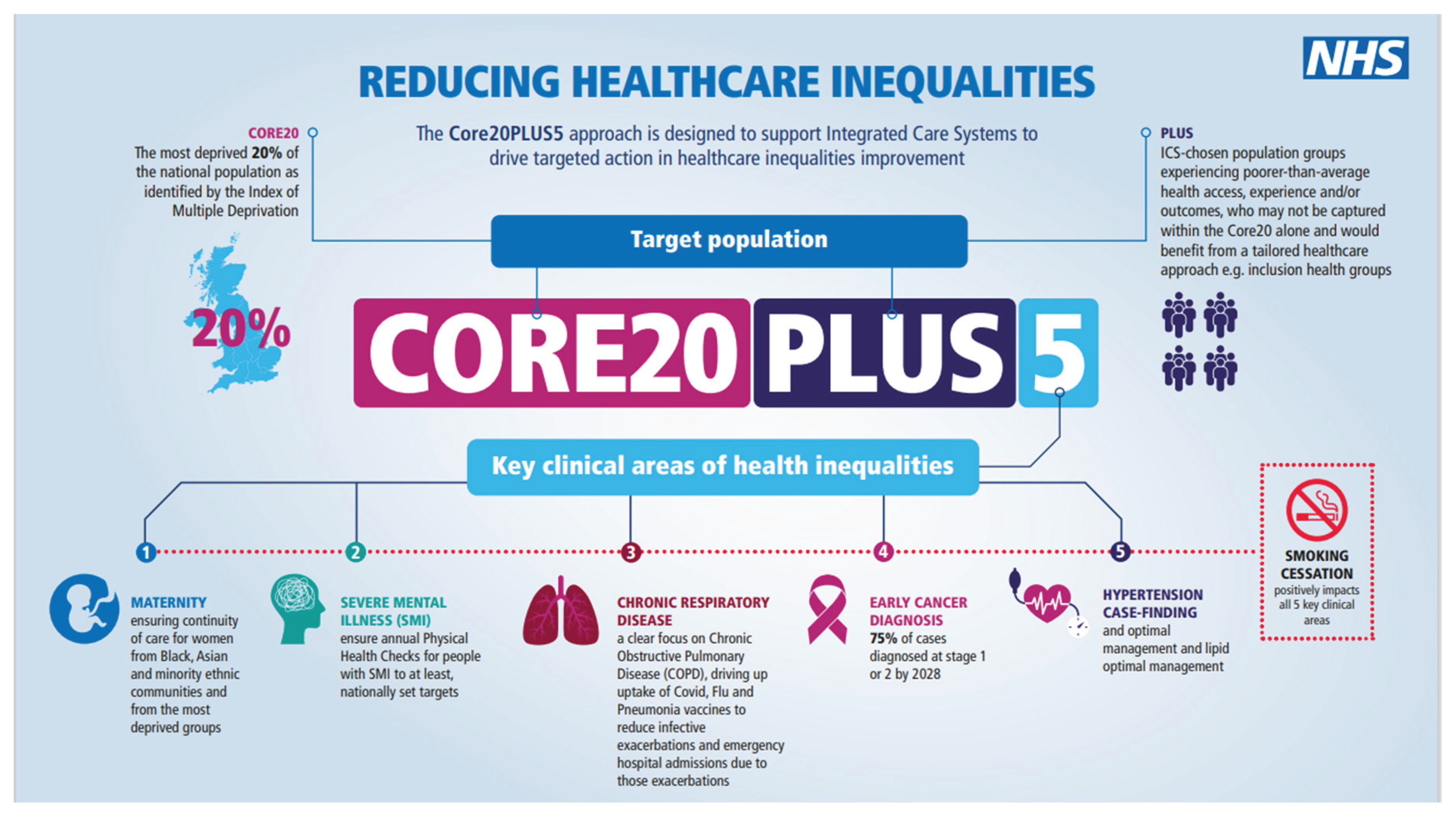
Figure 2.
The Progress Plus Framework [20].
Figure 2.
The Progress Plus Framework [20].
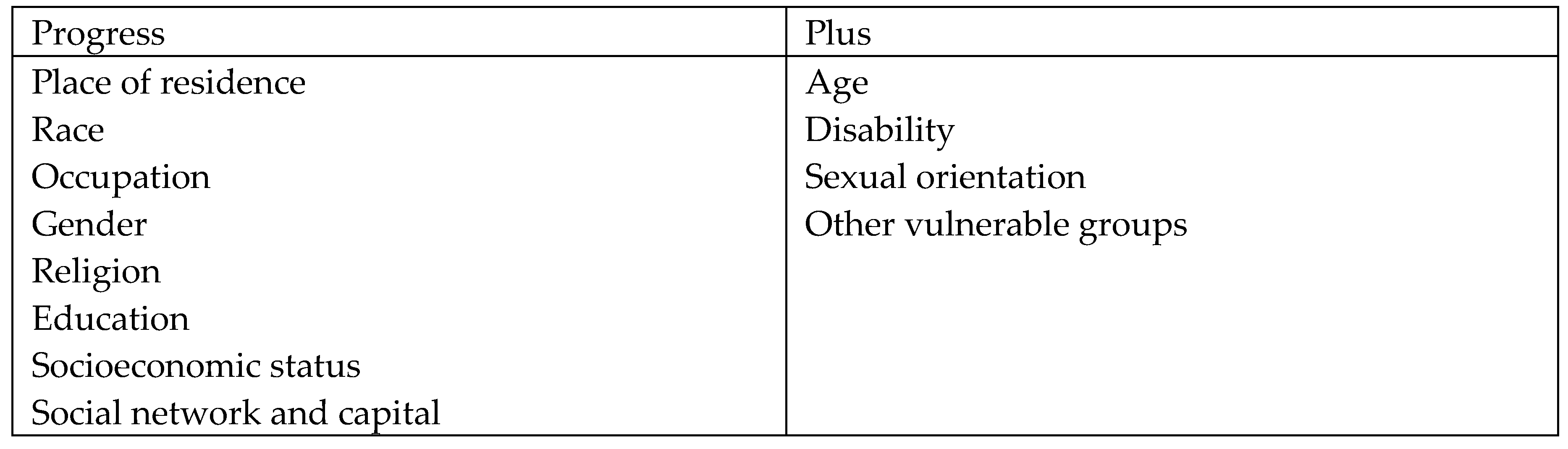
Figure 3.
PRISMA flow diagram with numbers of records identified, screened, excluded, and included for trials with evidence on use of wearable devices to measure physical activity in populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
Figure 3.
PRISMA flow diagram with numbers of records identified, screened, excluded, and included for trials with evidence on use of wearable devices to measure physical activity in populations at risk of health inequity as defined by the PROGRESS-Plus and CORE20PLUS5 frameworks.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



