
Submitted:
05 January 2026
Posted:
07 January 2026
You are already at the latest version
Abstract
Melanoma, a highly aggressive and metastatic cancer, poses significant challenges due to its propensity to spread to distant organs, with brain metastasis representing a particularly devastating complication. This review synthesizes recent advances in understanding the molecular, cellular, and microenvironmental mechanisms driving melanoma metastasis, with a specific emphasis on brain metastasis. We explore the unique challenges of brain metastasis, including blood-brain barrier penetration, brain-specific microenvironment interactions, and genomic distinctions. Advances in diagnostic tools, such as imaging and liquid biopsies, are discussed alongside current and emerging therapeutic strategies, including novel small molecules, immunotherapies, and combination approaches tailored for brain metastases. The review also highlights the immunological landscape of the brain, translational models, and multidisciplinary clinical management strategies. Finally, we identify critical research gaps, including the need for brain metastasis-specific clinical trials, AI-driven predictive models, and preventive strategies, to guide future efforts in improving outcomes for patients with melanoma brain metastasis.
Keywords:
melanoma
; brain metastases
; NRAS
; BRAF
; PI3K/AKT
; immune checkpoint inhibitors
; brain microenvironment
; preclinical models
; therapeutic resistance
1. Introduction
Melanoma is an aggressive form of skin cancer and the 5th leading cause of cancer-related deaths worldwide [1]. While frontline treatment strategies have greatly improved patient outcomes over the last decade, melanoma remains a deadly disease. Importantly, the majority of melanoma-related deaths result from distant metastases [1,2]. In the United States, an estimated 8,430 melanoma-related deaths occurred in 2025 [3]. Although melanoma incidence continues to increase, mortality rates began decreasing in 2013, largely due to the development of both targeted therapies and immunotherapies [4]. However, while the 5-year survival rate for patients with localized melanoma approaches 100%, survival still drops below 35% for patients with distant metastatic disease despite current treatments.
Melanoma arises from melanocytes, pigment-producing cells that synthesize melanin, which serves as a protective barrier against ultraviolet (UV) radiation. Melanocytes are derived from neural crest cells during embryonic development and reside in the basal layer of the epidermis [5]. Historically, melanoma progression has been described as a linear, stepwise process in which metastatic dissemination does not occur until late-stage disease progression, as outlined by the Clark model staging system [6]. This model outlines critical steps in melanoma progression, beginning with the formation of benign melanocytic and dysplastic nevi, followed by primary tumor growth, and ultimately culminating in metastasis, driven by the accumulation of genetic alterations [7]. In this framework, metastasis is restricted to advanced stages of disease and is attributed to a limited subset of tumor clones with metastatic potential. However, accumulating evidence indicates that melanoma progression is frequently non-linear and biologically more complex than this traditional model suggests.
Melanoma is characterized by a pronounced capacity for metastatic dissemination, driven by biological features that facilitate vascular invasion, immune evasion, and colonization of distant organs. Metastasis is initiated when malignant cells from superficial primary lesions invade the deeper dermal layers, enabling entry into the vascular and lymphatic compartments. Following intravasation, melanoma cells disseminate to regional and distant sites via lymphatic and hematogenous circulation [8]. Melanoma cells also acquire endothelial-like properties that enhance survival within the circulation and facilitate adhesion and extravasation at secondary sites (Figure 1). In parallel, the expression of pro-inflammatory and pro-angiogenic mediators supports tumor vascularization and metastatic outgrowth [9,10,11].
Metastatic progression is the primary determinant of melanoma prognosis. Notably, metastatic dissemination frequently precedes clinical detection of the primary lesion, limiting the effectiveness of surgical resection alone and necessitating aggressive multimodal treatment strategies, as removal of the primary lesion does not reliably prevent further spread [1]. Among metastatic sites, melanoma exhibits a particularly high propensity for brain colonization, which represents a major source of morbidity and mortality. An estimated 40–75% of patients with stage IV disease develop intracranial metastases, which is associated with a median survival of ~9 months from the time of brain metastasis diagnosis in the modern treatment era [12].
Although metastatic melanoma has historically been associated with poor outcomes, recent advances in immune checkpoint inhibition and targeted therapies have begun to improve survival, including in patients with brain involvement [13,14,15,16,17,18,19]. This review summarizes current insights into the mechanisms underlying melanoma metastasis, with a particular emphasis on brain colonization, and highlights emerging therapeutic strategies and future research directions.
2. Mechanisms of Melanoma Metastasis
Cutaneous melanoma is distinguished by an exceptionally high mutational burden and intratumoral heterogeneity, reflecting the involvement of numerous genetic drivers in disease initiation and progression. This extensive genetic complexity poses substantial challenges for therapeutic targeting and contributes to the rapid emergence of treatment resistance [20,21,22,23]. Notably, melanoma recurrence rarely occurs at the primary tumor site and instead frequently presents as metastatic lesions at distant sites [24], suggesting that dissemination likely occurs prior to surgical removal of the primary lesion.
The likelihood of melanoma metastasis is influenced by multiple factors, ranging from tumor microenvironment cues to intrinsic changes in cell state and differentiation [25]. Activation of diverse oncogenic cell signaling pathways is a hallmark of melanoma development, progression, and metastasis. Among these, aberrant activation of the mitogen-activated protein kinase (MAPK) pathway occurs in the majority of melanoma cases, most commonly through oncogenic mutations in BRAF, which are present in over 50% of all cutaneous melanoma cases and represent the most frequently altered oncogene in this malignancy (Figure 2). The most common oncogenic alteration, BRAFT1799A, encodes the BRAFV600E oncoprotein kinase which induces a strong gain-of-function phenotype and leads to constitutive BRAF signaling with sustained ERK activation.
Clinically, BRAF-mutant melanomas exhibit an increased propensity for brain metastasis [26,27], with specific mutational subtypes (e.g., V600K) associated with distinct survival outcomes [28]. Beyond proliferative signaling, BRAF mutations have been implicated in melanogenesis, phenotypic plasticity, and immune modulation within the tumor microenvironment, collectively facilitating metastatic spread [26]. Consequently, selective mutant BRAF inhibitors, in combination with MEK inhibitors, have become a cornerstone of targeted therapy for patients with BRAF-mutant melanoma [29].
NRAS, which encodes a membrane-associated GTPase in the RAS family upstream of the RAF family kinases, is mutated in approximately 20% of cutaneous melanomas and was among the earliest oncogenic drivers identified in this disease [30]. NRAS transduces receptor-mediated signals through the Ras-regulated>RAF>MEK>ERK MAPK cascade, leading to ERK-mediated phosphorylation of numerous cytoplasmic and nuclear targets, including the lineage-defining transcription factor MITF [23,31,32] (Figure 2). Although targeting RAS has historically proven challenging in numerous solid tumor types, earning its reputation as “undruggable”, recent advancements in targeted therapies have begun to show promise. This is further discussed in Section 5.
Activation of RAS isoforms (H-, N-, or K-) also triggers downstream activation of the phosphatidylinositol 3-kinase (PI3K) pathway, another critical driver of melanoma progression. PI3K activation leads to downstream phosphorylation of the serine/threonine kinase, AKT, which promotes cell survival through inhibition of pro-apoptotic mediators such as Bad. In melanoma, PI3K pathway activation is associated with enhanced tumor growth, angiogenesis, metastatic dissemination, and therapeutic resistance [33] (Figure 2).
Importantly, silencing of PTEN or activation of PI3K (H1047R) has minimal effects on normal melanocytes, indicating that these alterations likely do not drive melanoma initiation but promote its disease progression [34]. While it is well-established that melanomagenesis requires numerous cooperating events beyond activation of common drivers such as BRAF or NRAS, melanoma metastasis likewise depends on additional genetic events, the majority of which converge on activation of PI3K lipid signaling [35,36]. Specifically, loss of PTEN has been shown to cooperate with the BRAFV600E mutation to drive metastatic melanoma [37]. In parallel, activation of AKT can independently promote melanoma metastasis to the lung and brain, even in the absence of PTEN inactivation [38,39,40,41,42]. Notably, melanomas with brain metastases frequently exhibit upregulated PI3K signaling (Figure 2), and although pharmacologic inhibition of this pathway can suppress tumor growth in preclinical and early clinical settings, therapeutic efficacy has been limited by dose-limiting toxicities and the requirement for simultaneous inhibition of multiple paralogs in the pathway [43,44,45,46].
2.1. Epithelial-to-Mesenchymal Transition [EMT] and Plasticity in Melanoma
Epithelial-to-mesenchymal transition (EMT) is a key driver of metastasis in many solid tumors. Although not epithelial in origin, melanoma cells can exhibit an EMT-like transition that shares molecular parallels with classical EMT in epithelial cancers, involving transcription factors such as ZEB1, TWIST1, and TCF4 that repress differentiation markers and facilitate metastatic propensity. This EMT-like transition is particularly relevant to central nervous system (CNS) dissemination in melanoma, where brain-metastatic variants exhibit upregulated EMT-associated genes, enabling enhanced aggressiveness and adaptation to the cerebral microenvironment during invasion and colonization. Through this EMT-like process, melanoma cells acquire mesenchymal traits that enhance motility, invasiveness, and resistance to therapy, as well as evasion of immune surveillance, thereby facilitating vascular transit and traversal of the blood-brain barrier (BBB) (21). This phenotypic plasticity is orchestrated by autocrine and paracrine signaling networks that induce extensive transcriptional reprogramming [47].
A central regulator of melanocyte biology and melanoma behavior is microphthalmia-associated transcription factor (MITF), a lineage-specific transcription factor essential for melanocyte survival [48,49,50,51]. MITF controls a broad transcriptional program encompassing melanogenesis, cell-cycle regulation, mitochondrial biogenesis, tricarboxylic acid cycle metabolism, and lipid utilization [52]. In melanoma, dysregulated MITF activity promotes multiple oncogenic phenotypes, including enhanced proliferation, invasion, immune evasion, and resistance to therapy. Importantly, MITF functions according to a “rheostat” model, in which low intracellular levels are associated with cell-cycle arrest and increased invasive capacity, whereas moderate to high expression promotes proliferation and cellular de-differentiation [53,54,55].
Upstream signaling pathways, including the MAPK pathway described above, frequently converge on MITF regulation, while additional pathways further modulate MITF regulation to drive melanoma progression and immune escape. The Wnt signaling pathway, a highly conserved regulator of development and tissue homeostasis, signals through both canonical β-catenin-dependent and noncanonical β-catenin-independent mechanisms. Specifically, MITF expression is directly regulated by β-catenin as part of the canonical Wnt signaling pathway, where it acts as a co-activator in complex with TCF/LEF family transcription factors that bind to the MITF promoter [56,57]. The MITF promoter is also activated by the lineage-specific transcription factor SOX10 [58,59,60,61], a marker strongly associated with metastatic melanoma in patient samples [62].
Although the role of β-catenin in melanoma metastasis has been debated, owing in part to reports that it can suppress migration, critical studies have demonstrated that expression of mutant β-catenin significantly increased metastasis in BRAF- or NRAS-driven melanoma mouse models [63,64]. A defining feature of EMT is the loss of epithelial adhesion mediated by E-cadherin coupled with a gain of mesenchymal markers such as N-cadherin, a switch that promotes cellular motility and survival during immune-mediated stress [65,66]. In melanoma, oncogenic NRAS and BRAF signaling drives EMT-like transcriptional programs, including a shift from ZEB2/SNAIL2 to ZEB1/TWIST1 expression, which has been linked to enhanced invasiveness and metastatic competence [10,67,68].
Additional regulators, such as autocrine secreted protein acidic and rich in cysteine (SPARC) signaling and upregulation of the homeobox transcription factor PRRX1, further reinforce EMT through repression of E-cadherin and activation of β-catenin and TGF-β pathways, respectively [22,55,69,70,71]. Collectively, these EMT-like programs promote the phenotypic flexibility required for melanoma cells to extravasate, adapt, and proliferate within the brain microenvironment.
2.2. Tumor Microenvironment Contributions to Metastasis
The tumor microenvironment (TME) surrounding melanoma brain metastasis plays a central role in immune evasion, therapeutic resistance, as well as metastatic outgrowth, and has therefore emerged as a critical focus of clinical and translational research. The melanoma brain metastatic TME is highly heterogenous, comprising immune and stromal cell populations, extracellular matrix (ECM) components, and a wide array of soluble factors including cytokines, chemokines, and growth factors. A major focus of TME investigation has centered on the immune landscape within this niche and the mechanisms of melanoma cell immune evasion.
A principal mechanism of immune escape involves activation of inhibitory immune checkpoints that suppress cytotoxic T lymphocyte (CTL) function. Melanoma cells induce upregulation of CTLA-4 and PD-1 on CTLs, leading to impaired T-cell activation and exhaustion in the context of chronic antigen exposure [72]. These pathways are therapeutically targeted by immune checkpoint inhibitors (ICIs), including monoclonal antibodies against CTLA-4 and PD-1, which aim to restore antitumor immunity [73,74,75,76,77]. Despite these advances, resistance to immune checkpoint blockade remains a major therapeutic obstacle in this disease [73,75,78,79].
Beyond T cells, innate and adaptive immune populations also contribute to immune evasion in melanoma brain metastasis. Neutrophils have emerged as key mediators of therapeutic resistance, with non-responding intracranial tumors exhibiting neutrophil-rich microenvironments despite comparable levels of T-cell infiltration [80]. In particular, IL-8–expressing neutrophil subpopulations, along with those producing interferons and calprotectin, promote angiogenesis, aggressive tumor growth, and EMT, suggesting that neutrophil-driven inflammation contributes to immune escape and metastatic persistence within the central nervous system [81].
B-cells also represent a prominent immunomodulatory population in melanoma brain metastases, occurring at higher frequencies than in brain metastases derived from breast or lung cancers [82]. Regulatory B-cells secrete anti-inflammatory cytokines such as IL-10, which suppress CTL activity and impair antigen presentation, thereby attenuating antitumor immune responses [83].
Stromal cells further shape the immunosuppressive and pro-metastatic niche of melanoma brain metastases. Although normally essential for maintaining BBB integrity and immune homeostasis, stromal cells can undergo tumor-induced reprogramming that supports metastatic growth, inflammation, and immune evasion [84]. Activated stromal signaling pathways, including YAP1 downstream of β-catenin, promote EMT-like transition through induction of a ZEB2-to-ZEB1 transcriptional switch in adjacent melanoma cells and may also drive tumor vasculogenesis [85,86,87]. Age-associated fibroblast changes further exacerbate metastatic progression, including secretion of the Wnt antagonist sFRP2, which suppresses β-catenin, MITF, and APE1, thereby promoting angiogenesis, metastasis, and resistance to BRAF-targeted therapies [19].
Remodeling of the ECM is another defining feature of melanoma brain metastasis. Loss of basement membrane integrity, particularly through collagen IV degradation, facilitates tumor invasion, while increased matrix stiffness promotes hypoxia, focal adhesion signaling, drug resistance, and metastatic fitness [88,89]. Aged fibroblasts contribute to ECM remodeling by increasing endothelial permeability, impairing lymphatic function, and promoting visceral metastasis. These fibroblasts also secrete ceramide lipids that are taken up by melanoma cells via fatty acid transport protein 2 (FATP2), encoded by the SLC27A2 gene, supporting resistance to oxidative stress and targeted therapies such as BRAF/MEK inhibitors [90,91].
Finally, melanoma cells actively remodel their metastatic niche through intercellular communication. The secretion of nerve growth factor receptor (NGFR)-containing extracellular vesicles enhances lymphangiogenesis and tumor-endothelial adhesion, thereby facilitating metastatic dissemination and colonization of the brain [92].
3. Melanoma Brain Metastasis: Unique Challenges and Mechanisms
Brain metastases occur far more frequently than primary brain tumors, and melanoma represents the third most common primary malignancy to metastasize to the brain, following lung and breast cancers [11,93,94,95]. Although lung cancer accounts for the greatest absolute number of brain metastases due to its higher overall incidence, melanoma exhibits the highest relative propensity for CNS dissemination among all solid tumors [11]. Epidemiological analyses have also identified sex-based disparities in melanoma brain metastasis. Recent healthcare database studies demonstrate that male patients have a 22% higher risk of developing brain metastases, and among affected individuals, experience poorer clinical outcomes compared with women [96].
The BBB serves as a formidable obstacle to metastatic dissemination, requiring tumor cells to actively traverse endothelial interfaces to colonize the CNS [97,98]. Although the precise mechanisms remain incompletely defined, emerging evidence suggests that direct interactions between melanoma cells and cerebral endothelial cells facilitate extravasation into the brain parenchyma [99,100]. Advances in in vivo modeling and live-cell imaging have substantially improved our understanding of the melanoma brain tropism, highlighting critical points in the metastatic cascade.
Dissemination of melanoma cells to the brain is a complex, multistep process that begins with intravasation into lymphatic or blood vessels. Circulating tumor cells must survive the hostile conditions of the circulation, express adhesion molecules that mediate interactions with vascular endothelium, and ultimately extravasate across the BBB [101,102,103]. This process is particularly challenging due to the presence of tight-junction adhesions and low permeability within the brain endothelium [104].
Within the CNS microenvironment, astrocytes and microglia represent key stromal populations that critically influence metastatic progression. Astrocytes contribute to BBB integrity through their perivascular end-feet, whereas microglia function as the resident immune cells of the CNS [105,106]. Although these cells were historically viewed as protective against metastatic invasion, accumulating evidence indicates that melanoma cells can co-opt astrocytes and microglia, inducing aberrant activation states that promote tumor survival, invasion, and therapeutic resistance [107,108]. Activated microglia, in particular, have been shown to suppress apoptosis in metastatic melanoma cells, further facilitating intracranial tumor expansion [109]. Collectively, these findings suggest that CNS stromal cells, while initially tumor-suppressive, can be rapidly subverted to support metastatic progression.
In addition to microenvironmental influences, melanoma brain metastases exhibit distinct genomic and transcriptomic profiles compared with primary tumors or extracranial metastases. Specifically, next-generation sequencing has identified increased frequencies of mutations in BRAF, SETD2, PBRM1, and DICER1, along with increased PD-L1 expression, underscoring distinct genetic and epigenetic features that may contribute to CNS tropism and therapeutic resistance [110]. Supporting this, Biermann et al. performed multi-modal single-cell and spatial genomics of treatment-naive melanoma brain metastases compared with extracranial metastases and discovered that cancer cells from melanoma brain metastases adopt a ‘neural-like’ cell state, expressing genes with essential roles in synapse formation and interactions among brain niche-cells [111]. This phenotype, beyond baseline neural crest lineage, may enhance brain-metastatic organotropism, invasiveness, and drug resistance, warranting further mechanistic and therapeutic exploration.
4. Diagnostic Advances in Melanoma Metastasis
Contrast-enhanced magnetic resonance imaging (MRI) with gadolinium is widely regarded as the most sensitive imaging modality for the detection of brain metastases [112]. T1-weighted sequences acquired after contrast administration are particularly sensitive, as metastatic lesions typically appear hyperintense relative to surrounding brain tissue. T2-weighted sequences, while less specific, provide complementary information and are useful for evaluating associated hemorrhage, edema, and mass effect [113]. Accordingly, MRI plays a central role across all stages of melanoma brain metastasis management, including initial detection, lesion characterization, precise anatomic localization, and longitudinal assessment of therapeutic response [112,114,115].
Despite its status as the imaging gold standard, MRI has important limitations. Gadolinium-based contrast agents are contraindicated in patients with impaired renal function, and MRI is not feasible for individuals with incompatible implanted devices such as pacemakers or metallic hardware. In such cases, alternative imaging modalities, including positron emission tomography (PET), are employed [112]. PET imaging most commonly utilizes the glucose analogue 18F-fluorodeoxyglucose (18F-FDG), which is preferentially taken up by metabolically active tumor cells [116]. FDG-PET is therefore useful for systemic staging and early detection of metastatic disease. However, its application in the brain is limited by high baseline glucose uptake in normal neural tissue, which reduces lesion contrast and spatial resolution. PET also provides limited anatomic detail than MRI, complicating accurate delineation of tumor margins, and is susceptible to false-positive findings in regions of inflammation, infection, or other metabolically active non-neoplastic processes. Nevertheless, FDG-PET remains a valuable tool for diagnosis, staging, treatment planning, and disease monitoring, particularly when MRI is contraindicated [112,116].
Radiomics has emerged as a promising computational imaging approach that converts conventional radiographic and histopathologic data into high-dimensional, quantitative features using advanced computational algorithms [117]. By extracting subtle patterns related to tumor shape, texture, and signal intensity that are not readily discernible by visual inspection alone, radiomics has the potential to improve tumor characterization and prognostication [117,118]. This approach may be particularly valuable in melanoma, which demonstrates marked heterogeneity in lesion size, morphology, and growth behavior, and where early detection could limit metastatic progression [21]. Despite its promise, clinical implementation of radiomics is currently limited by challenges related to reproducibility, lack of standardization across imaging platforms, and variability in analytic pipelines, underscoring the need for further validation before widespread clinical implementation [117,118].
Liquid biopsy represents a minimally invasive alternative to conventional tissue biopsy and has gained increasing attention in the evaluation of metastatic melanoma. This approach involves the analysis of bodily fluids, such as blood, cerebrospinal fluid, or saliva, for tumor-derived biomarkers such as circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), and extracellular vesicles. Liquid biopsies enable real-time monitoring of disease burden, capture temporal genomic evolution, and facilitate assessment of therapeutic response in real time [119]. However, limitations include incomplete detection of tumor heterogeneity and the potential for false-positive or false-negative results [120].
CTCs, also known as circulating melanoma cells (CMCs), are shed from primary or metastatic lesions into the circulation and are of particular interest given melanoma’s high metastatic potential. Elevated CTC levels correlate with poorer prognosis and reduced overall survival. To persist in circulation, these cells undergo phenotypic changes, including epithelial-mesenchymal transition [120,121]. Similarly, ctDNA released through tumor cell apoptosis or active secretion provides molecular insight into actionable mutations, such as BRAF alterations, enabling treatment selection and response monitoring [122].
Exosome-based analyses represent an additional and promising diagnostic modality. Exosomes are small, stable extracellular vesicles released by both normal and malignant cells and are readily detectable in bodily fluids including blood and urine. They contain tumor-specific cargo, such as proteins, lipids, DNA, and RNA, that reflects the molecular characteristics of the originating tumor [120,123,124,125]. Selective packaging of exosomal contents, together with surface markers indicative of tissue origin, enables enrichment and characterization of tumor-derived vesicles. Increasing evidence suggests that combining multiple liquid biopsy approaches, such as ctDNA and exosome analysis, enhances sensitivity, reduces false-negative rates, and provides complementary molecular information [120]. Importantly, exosomes have been implicated in therapeutic resistance mechanisms in melanoma [126,127]. Specifically, exosome-mediated transfer of platelet-derived growth factor (PDGFR) to melanoma cells can activate the PI3K signaling pathway allowing bypass of BRAF and MAPK pathway inhibition [128].
Recent advances in liquid biopsy research have also focused on extracellular RNA, driven in part by large-scale initiatives such as the NIH-funded Extracellular RNA Communication Consortium [129]. Extracellular RNA molecules are protected from degradation through association with ribonucleoprotein complexes (e.g., Argonaute-2), binding to high- or low-density lipoproteins, or encapsulation within extracellular vesicles [130,131]. Integrating multiple extracellular RNA detection strategies has been shown to further enhance the sensitivity and clinical utility of liquid biopsy approaches [120].
Micrometastases represent an early and clinically occult stage of brain dissemination in which tumor cells colonize the CNS without forming detectable macroscopic lesions or producing neurological symptoms. Early identification of micrometastatic disease could enable timely therapeutic intervention and improve patient outcomes; however, detection remains challenging due to minimal tumor burden and weak biological signal [132]. Critically, reports of melanoma transmission from organ donors to recipients years after apparent disease resolution provide compelling evidence for long-term micrometastatic persistence [133].
Conventional imaging modalities often lack the resolution and specificity to distinguish micrometastases from treatment-related changes such as pseudoprogression or radiation necrosis, as well as from primary brain tumors or metastases of other origins [134,135]. Similarly, existing metabolic assays are insufficiently sensitive or specific to reliably detect micrometastatic disease. Ongoing research is therefore focused on identifying molecular and imaging biomarkers specific to melanoma brain metastases, including cerebrospinal fluid markers of tumor presence and neural tissue injury [136]. Advanced imaging techniques, such as amino acid–based PET tracers, are also under investigation. Notably, O-(2-18F-Fluoroethyl)-l-tyrosine (FET) PET has demonstrated a sensitivity of approximately 90%, highlighting its potential utility in detecting early intracranial melanoma involvement [137,138].
5. Therapeutic Strategies for Melanoma Brain Metastasis
The current standard of care for melanoma brain metastases encompasses three principal therapeutic modalities: systemic therapy, neurosurgical resection, and radiation therapy, delivered either as stereotactic radiosurgery (SRS) or whole-brain radiotherapy (WBRT) [139]. Treatment selection is guided by multiple factors, including symptom burden, number and size of lesions, molecular tumor profile, and patient performance status [16,140]. Historically, melanoma brain metastases were associated with a dismal prognosis, with median survival estimates of approximately 4–6 months. However, the advent of immunotherapies and advances in radiation delivery have led to meaningful survival improvements in survival for patients [12,141].
Neurosurgical resection is recommended for selected patients with large (e.g., >2.5 cm), symptomatic brain metastases, particularly those associated with hemorrhage or significant mass effect. Surgical intervention provides rapid decompression, symptomatic relief, and durable local control, and may improve overall survival in appropriately selected cases. However, surgery may be contraindicated for lesions located within critical brain regions or in patients with elevated perioperative complication risks [142,143].
Radiation therapy remains a cornerstone of intracranial disease management. SRS delivers high-dose radiation with submillimeter precision to discrete lesions while minimizing exposure to surrounding brain tissue. In contrast, WBRT exposes the entire brain to radiation and is generally reserved for patients with extensive intracranial disease or those who are not candidates for surgery or SRS. Although WBRT may provide symptomatic benefit and modest survival benefit, its use is limited by cumulative neurotoxicity and the risk of long-term cognitive decline [144,145]. Comparative studies have demonstrated no significant difference in recurrence rates between SRS and WBRT, with a trend toward improved survival in patients treated with SRS [146]. Consequently, current treatment paradigms favor systemic immunotherapy for patients with asymptomatic or small-volume brain metastases [147]. For patients with asymptomatic disease who progress on immunotherapy and harbor one to three lesions, SRS is preferred over WBRT [15,147]. The most favorable outcomes are observed in patients undergoing surgical resection followed by adjuvant SRS [15].
Systemic therapy for melanoma brain metastases consists primarily of immunotherapy and molecularly targeted agents. Systemic therapy alone has historically demonstrated limited efficacy, likely due to restricted drug penetration across the BBB, while radiotherapy alone offers only marginal benefit over supportive care and is frequently associated with neurotoxicity and subsequent cognitive decline [148,149]. Conventional chemotherapeutic agents, including dacarbazine and temozolomide, which can cross the BBB, have shown limited clinical benefit in this setting [150,151]. More favorable outcomes have been observed in patients undergoing surgical resection followed by adjuvant immunotherapy, although immune-related adverse events (IRAEs) frequently limit treatment durability[152].
Recent trials have highlighted the potential benefits of neoadjuvant immunotherapy. Studies comparing neoadjuvant vs. adjuvant pembrolizumab in resectable late-stage cutaneous melanoma demonstrated improved outcomes with neoadjuvant treatment; however, these trials excluded patients with brain metastases, underscoring the continued therapeutic gap for unresectable intracranial disease [153]. In 2022, joint American Society of Clinical Oncology (ASCO), Society for Neuro-Oncology (SNO), and American Society for Radiation Oncology (ASTRO) guidelines recommended combination immunotherapy with ipilimumab plus nivolumab for patients with asymptomatic melanoma brain metastases, irrespective of BRAF mutation status. For patients with BRAFV600E/K-mutant disease, combined dabrafenib and trametinib therapy was also recommended as an alternative first-line option [154].
Multiple studies have evaluated mutation-specific targeted therapies in melanoma brain metastases. In the Phase II BREAK-MB trial, treatment with dabrafenib achieved an overall intracranial response rate of 35% in patients with BRAFV600E- or BRAFV600K alterations [155]. New evidence also supports the efficacy of newer BRAF and MEK inhibitors, including recently approved encorafenib and binimetinib for patients with brain metastatic melanoma [156,157]. Other targeted approaches have yielded mixed results. For example, the PI3K inhibitor buparlisib was well tolerated but produced no intracranial responses [14], while a Phase II study of the CDK4/6 inhibitor abemaciclib failed to meet its primary endpoint despite evidence of strong BBB penetration and intracranial clinical benefit in a subset of patients [158].
Despite these advances, effective pharmacologic treatment of melanoma brain metastases remains limited by the BBB, which is composed of tightly connected endothelial cells, pericytes, and astrocytic end-feet that collectively restrict CNS drug delivery [159]. While radiation and surgery may effectively control macroscopic disease, micrometastatic lesions often remain undetected and untreated [132]. Moreover, although immunotherapies demonstrate robust extracranial activity, their efficacy within the CNS remains variable, and even newer agents with partial BBB penetration have not consistently translated into improved overall survival [160,161].
Therapeutic resistance remains a major clinical challenge in advanced metastastic melanoma. A key mechanism of therapeutic resistance arises from tumor–stromal interactions, particularly with astrocytes [13]. Melanoma cells form gap junctions with astrocytes via connexin-43, which facilitates the settlement of metastatic melanoma cells in the brain [162].
Emerging therapeutic strategies aim to overcome resistance and exploit CNS-specific vulnerabilities. Chimeric antigen receptor (CAR) T cells have demonstrated efficacy in numerous hematologic malignancies and show promise in melanoma [163,164,165,166,167]. Oncolytic viruses represent another promising approach, leveraging tumor-selective viral replication to induce direct oncolysis and stimulate antitumor immunity [168]. A Phase III clinical trial led to FDA-approval of Talimogene Laherparepvec (TVEC), a modified herpes simplex virus type 1 (HSV-1) encoding granulocyte-macrophage colony-stimulating factor (GM-CSF) for advanced melanoma [169]. However, BBB penetration remains an obstacle to oncolytic virus efficacy, and further studies are needed to assess CNS delivery of candidate viruses such as parvovirus H-1PV [170].
Additional innovative approaches include repurposing BBB-penetrant antipsychotic agents such as trifluoperazine, fluphenazine, and clozapine, which disrupt lysosomal function, induce cell-cycle arrest, and modulate the immune microenvironment in melanoma brain metastases [171,172]. While targeting RAS was long considered unfeasible, the advent of novel RAS inhibitors has recently revolutionized the treatment landscape for cancers driven by oncogenic RAS signaling and is now being clinically explored in NRAS-mutant melanoma [173,174].
Finally, recent studies have identified focal adhesion kinase (FAK) as a critical mediator of melanoma brain metastasis downstream of PI3K signaling [42,175]. In a seminal study, Almazan and colleagues demonstrated that combined inhibition of FAK and RAF/MEK signaling suppressed melanoma tumor growth, reduced brain metastasis formation, and prolonged survival, including in mice with established intracranial disease. FAK inhibition alone significantly reduced the development of brain metastases, while the combined inhibition of FAK and RAF/MEK induced robust apoptosis and tumor regression leading to prolonged survival in preclinical models [175]. Notably, this study employed the novel RAF/MEK inhibitor, avutometinib, which functions as a molecular clamp to inhibit MAPK signaling. Promising preclinical studies such as these have catalyzed ongoing clinical trials for solid tumors using these combination therapies and offer renewed hope for patients with melanoma brain metastases [176,177] (Table 1).
6. Immunological Perspectives in Melanoma Brain Metastasis
The brain microenvironment is composed of a unique cellular framework, characterized by a distinct immune landscape that differs markedly from other common sites of melanoma metastasis. While the immune landscape of the brain has been historically considered immunologically isolated due to the BBB, recent studies have challenged this paradigm, particularly in the context of brain metastases where the BBB is frequently compromised, permitting infiltration of peripheral immune cells [178]. Thus, in addition to resident microglia, macrophages, and dendritic cells, peripheral immune cells such as neutrophils and lymphocytes are also commonly present within the metastatic brain microenvironment [178].
Tumor-associated macrophages (TAMs) are highly expressed in the brain microenvironment and play a critical role in the pathogenesis of brain metastasis. Two principal TAM subpopulations reside in the CNS: microglia and border-associated macrophages (BAMs). Microglia are phenotypically plastic cells and represent the predominant immune cell population in the healthy brain [179]. Notably, the composition of TAMs is distinctly dynamic and evolves over the course of metastatic progression. In early-stage disease, characterized by smaller metastatic brain lesions, microglia comprise the majority of TAMs. However, as disease progresses and peripheral monocytes infiltrate the brain, the TAM population shifts toward monocyte-derived macrophage cells [180,181,182]. Microglia, in particular, directly interact with melanoma cells and facilitate their establishment and survival in the brain microenvironment [183,184].
The lymphocytic compartment of the brain microenvironment is primarily composed of T-cells, including both CD4+ and CD8+ populations, which represent the most phenotypically diverse immune cells in this niche [82,185,186]. Interactions between microglia cells and T-cells have been shown to exert context-dependent effects, contributing to both immunosuppression and immune activation. Several reports demonstrate that microglia-T cell interactions suppress T cell activity and promote metastatic growth [187]. Conversely, brain resident T-cells have also been shown to exhibit antigen-presentation capacity, enhancing anti-tumor immune response within the brain metastatic compartment [188,189].
Despite the challenges targeting brain metastases, growing insight into the immune microenvironment in the brain, along with recent advances in immunotherapeutic strategies capable of crossing the BBB, offers renewed promise [190]. One such strategy involves targeting TAMs, given their central role in promoting brain metastatic outgrowth. Approaches to modulate TAMs include macrophage depletion through inhibition of the colony-stimulating factor 1 receptor (CSF1R), which regulates macrophage survival and differentiation. However, while depletion strategies may counteract the pro-tumorigenic role of TAMs, they could be limited by compensatory recruitment of other myeloid cells, such as myeloid-derived suppressor cells. Another approach is reprogramming macrophages toward anti-tumor phenotypes. Tumoral interferon beta (IFNβ), often induced by radiotherapy, has been shown to repolarize TAMs in murine melanoma brain metastasis models [191]. This re-education shifts TAMs toward an immune-stimulatory state, and has the potential to improve clinical outcomes in patients, including better responses to combined radioimmunotherapy. IFNβ could act as a predictive biomarker in this context, providing mechanistic insights into synergistic therapies with immunotherapies. While preclinical studies have shown promising effects in vivo, further investigation is needed before these modalities can be translated into the clinic [184,192,193,194].
Immunotherapy has revolutionized the treatment landscape for patients with melanoma. However, baseline immune status plays a critical role in determining therapeutic response. Tumors are often described along an immunologic spectrum ranging from “hot” to “cold” [195]. While primary brain tumors are typically immunologically “cold,” brain metastases, especially originating from melanoma primary tumors, can exhibit “hot” immune profiles due to infiltrating lymphocytes and antitumor immune cells [178]. Because melanoma cells, including metastatic melanoma cells, frequently express high levels of PD-1 and PD-L1, clinical trials have focused on assessing the efficacy of immune checkpoint inhibitors in melanoma brain metastases [82].
A recent Phase II clinical trial evaluating the PD-1 antibody pembrolizumab in patients (both treatment naive and pretreated) from multiple primary tumor types, including melanoma, demonstrated an intracranial response of ~40%. However, more than half of patients experienced treatment-related adverse events, highlighting a major therapeutic obstacle. Similarly, trials evaluating the combination therapy with the CTLA-4 inhibitor ipilimumab and the PD-1 inhibitor nivolumab in melanoma brain metastases reported intracranial responses of 46-57%, yet again with adverse events in over half of all treated patients [17,19].
Recent efforts have focused on enhancing immune activation within the brain microenvironment while overcoming immunosuppressive barriers [196,197]. Encouragingly, studies in other metastatic tumor types, as well as novel immunotherapeutic combination strategies, have demonstrated substantial improvements in intracranial progression-free survival and prolonged time to brain metastasis [81,198,199]. Nonetheless, significant work is needed to improve immunotherapeutic efficacy and tolerability for patients with melanoma brain metastases who have exhausted currently available treatment options.
7. Translational and Preclinical Models for Studying Brain Metastasis
The development and application of diverse experimental models has been essential for advancing our understanding of melanoma biology, including tumor behavior, metastatic progression, therapeutic resistance, immune interactions, and early oncogenic events [200]. Current approaches encompass a broad spectrum of in vivo and in vitro systems including zebrafish models, genetically-engineered mouse models (GEMMs), tumor-derived cell lines, patient-derived xenografts (PDX), and a growing array of three-dimensional (3D) culture platforms, such as organoid models [200].
Mouse models have long formed the foundation of preclinical melanoma research and have played a central role in the development of effective therapeutic strategies. However, interspecies genetic and physiological differences can limit translational relevance, particularly in PDX models [200,201]. Notably, only ~30% of findings from animal studies advance to human clinical trials, and fewer than 8% ultimately progress beyond Phase I testing, underscoring the need for more predictive experimental systems [202,203].
Tumor-derived melanoma cell lines remain widely used due to their reproducibility, suitability for high-throughput experimentation, and ease of genetic manipulation. While these systems enable mechanistic interrogation and drug discovery efforts, they are inherently limited by selection bias toward culture-adapted clones, absence of a physiologically relevant microenvironment, and lack of critical stromal, vascular, and immune components that influence tumor behavior in vivo [204,205].
PDX models partially address these shortcomings by engrafting human tumor tissue into immunocompromised mice, thereby preserving intratumoral heterogeneity and enabling assessment of therapeutic responses across architectural, histological, phenotypic, and mutational dimensions. However, dependence on murine host stroma and lack of a fully functioning immune system limits the capability of PDX models to faithfully recapitulate human tumor-microenvironment interactions [200,206].
Advances in 3D melanoma modeling have yielded platforms that more closely mimic native tissue architecture and tumor microenvironments. Spheroid cultures, composed of aggregated melanoma cells grown in suspension, develop oxygen and nutrient gradients that generate intratumoral heterogeneity and enhance physiological relevance relative to two-dimensional cultures [207,208]. When co-cultured with additional cell types, spheroids can provide insight into early steps of the metastatic cascade; nevertheless, their capacity to model complex host–tumor interactions remain limited [209,210].
Organoid models represent a further evolution of 3D systems, incorporating layered skin cell populations within supportive scaffolds. Recent bioengineering innovations have enabled the inclusion of appendages such as hair follicles, sebaceous and sweat glands, and vascular-like structures, reducing necrosis and enhancing tissue fidelity [211]. Importantly, patient-derived melanoma organoids generated from metastatic lesions have recently been shown to be feasible, enabling personalized modeling of disease progression and therapeutic response [212,213,214].
Skin reconstruct models employ primary human keratinocytes, melanocytes, and fibroblasts embedded within extracellular matrix components to generate stratified epidermal structures that closely resemble native human skin. These platforms enable detailed investigation of cell–cell interactions, stromal influences, and melanoma initiation and progression within a customizable microenvironment [215,216].
Finally, integration of multi-omics approaches, spanning genomics, transcriptomics, proteomics, metabolomics, and epigenomics, has substantially advanced understanding of the molecular determinants that enable melanoma cells to thrive and spread in the brain. Recent studies reveal that melanoma brain metastases harbor distinct molecular programs that drive CNS tropism, immune escape, metabolic reprogramming, and therapeutic resistance [217]. Single-cell multi-omic analyses have identified a pre-metastatic melanoma subpopulation with upregulated neural adhesion genes (e.g. NRG3, NCAM1) that predisposes tumors to brain colonization [111,217,218]. Complementary genomic and transcriptomic profiling reveals that melanoma brain metastases frequently harbor mutations such as loss of function PTEN and display brain-like gene expression signatures not observed in extracranial lesions, underscoring the importance of context-specific modeling platforms [111,217,218].
8. Clinical Management and Multidisciplinary Approaches
Management of melanoma brain metastases requires a comprehensive, multidisciplinary approach involving neuro-oncologists, medical oncologists, radiation oncologists, neurosurgeons, rehabilitation specialists, and palliative care teams, each of whom plays a critical role in optimizing patient outcomes. Given the complexity and heterogeneity of intracranial disease, coordinated care across specialties is essential for effective symptom control, therapeutic decision-making, and longitudinal management.
Neuro-oncologists are central to the care of patients with melanoma brain metastases, as these individuals frequently experience a broad spectrum of neurological complications arising from both tumor burden and treatment-related toxicities [112,219]. Clinical manifestations vary according to lesion location and extent and may include seizures, neurocognitive decline, focal neurological deficits, and altered mental status. Accordingly, neuro-oncologic management emphasizes precise pharmacologic and supportive interventions tailored to individual neurological symptoms, with the overarching goal of preserving function and quality of life [112,219].
Medical oncologists oversee systemic disease management, including tissue biopsy, molecular and genomic profiling, and administration of systemic therapies such as immune checkpoint inhibitors and targeted agents. Although they do not directly perform surgical or radiation-based interventions, medical oncologists play a key role in therapeutic strategy selection, coordination of multidisciplinary care, management of treatment-related adverse effects, and provision of patient education and longitudinal support [220].
Diagnostic radiologists contribute to accurate detection and characterization of brain metastases through advanced imaging techniques, while radiation oncologists determine the appropriateness, modality, and dosing of radiotherapy and manage treatment-related toxicities in close collaboration with the broader care team [221,222].
Despite the substantial symptom burden associated with intracranial disease, palliative care and quality-of-life considerations remain underemphasized in patients with melanoma brain metastases. Patients commonly experience debilitating symptoms, including headaches, seizures, fatigue, and progressive neurological impairment, which significantly disrupt daily functioning. Early integration of palliative care has been shown to improve quality of life and reduce symptom severity, particularly when sustained for longer than three months [223,224]. In addition to addressing physical and psychological distress, palliative care facilitates informed decision-making and aligns treatment strategies with patient goals. Given the rapid and often unpredictable progression of brain metastases, early multidisciplinary involvement, including neurology, psychiatry, oncology, and supportive care services, is essential for optimizing patient-centered outcomes [220,224].
As therapeutic options continue to evolve, there is a growing need for expanded research and education focused on the genetic, molecular, and biological drivers of melanoma metastasis to enable more personalized treatment strategies. Advances in genomic profiling, including liquid biopsy approaches such as CTC analysis and ctDNA detection, now permit minimally invasive acquisition of molecular data that can inform therapeutic selection, monitor disease progression, and detect emerging resistance mechanisms [112].
In parallel, predictive modeling approaches that integrate clinical variables, imaging data, germline genetic markers, and computational analyses are increasingly being used to assess metastatic risk and guide individualized management [21,119,120,135]. These models have demonstrated improved accuracy in early detection and prognostication, supporting more tailored treatment paradigms. Although limitations remain, particularly in model generalizability and data standardization, emerging tools such as liquid biopsy platforms and artificial intelligence-driven radiomics hold significant promise for enhancing metastatic risk prediction and further refining precision care in melanoma [112,225,226].
9. Future Directions and Research Gaps
Future research on melanoma brain metastases converges on a few major challenges, including, overcoming therapeutic barriers to drug delivery across the BBB, advancing biomarker identification to detect early metastatic spread, and further elucidating mechanisms of how melanoma spreads to the brain. A major priority of metastatic melanoma research is to identify therapeutics that can reach the brain microenvironment, as the BBB prevents adequate drug penetration and can lead to uneven drug distribution [97]. This, along with unique immune profiles and an immunosuppressive microenvironment in the brain, makes current systemic treatments for melanoma brain metastases less effective [227]. Concurrent efforts in biomarker discovery aim to identify molecular signatures to help predict patients with a higher risk of brain metastasis in order to guide therapeutic options. Multi-omics platforms (such as genomic, transcriptomic, proteomic, and spatial profiling approaches) and liquid biopsies are leveraged to uncover new predictive biomarkers and therapeutic targets [228].
Equally important is expanding our mechanistic understanding of how melanoma cells invade and adapt in the brain microenvironment. From reaching the BBB to co-opting astrocytes and microglia to evade the immune system and ultimately propagate in the brain. Emerging approaches such as multi-omic profiling and AI-driven modeling are promising to accelerate progress. For example, a recent multi-omic analysis revealed distinct immunosuppressive and metabolic tumor microenvironments in melanoma brain metastases [218]. Moreover, machine learning models can integrate radiomic, genomic, and clinical data in order to improve prognostic predictions and aid in personalizing treatment [229]. By addressing these gaps to improve drug delivery across the BBB, establish robust biomarkers for early metastatic spread, and further identifying brain colonization, the field will continue to make strides to deliver more effective and personalized interventions for patients with melanoma brain metastases.
10. Conclusions
Melanoma brain metastasis is unique in its aggressive tumor-intrinsic programs and targeting the CNS-microenvironment is uniquely challenging, thus, exemplifying one of the most clinically challenging manifestations in cancer [1,11]. Advances in molecular biology, multi-omic profiling, and preclinical modeling have clarified mechanisms of CNS tropism, including lineage-specific transcriptional programs, metabolic rewiring, and stromal co-option by astrocytes and microglia [35,69,107,183,193,230]. However, these insights are only the beginning in translating effective intracranial therapies. Clinically, progress in immune checkpoint blockade and targeted MAPK pathway inhibitors have improved outcomes for some patients [17,43,75,76,152,153,157,175,231,232,233], but the BBB, intratumoral heterogeneity, and adaptive resistance pathways continue to limit durable therapeutic benefit for these patients [218]. Moving forward, it will be critical to further investigate and develop therapeutic strategies to deliver effective and safe CNS penetrating treatments, develop liquid biopsy approaches to detect micrometastases to guide treatment strategies, and further drive integrated multi-omics and AI analytics to deconvolute brain-specific metastatic biology and resistance mechanisms. With translational pipelines and clinical trials designed specifically for intracranial disease, there is potential to translate mechanistic discoveries into therapies to extend survival and preserve neurological function for patients with this devastating disease.
Author Contributions
Kayla T. O’Toole, Brandon M. Roan, Timothy M. Hardman, Peyton P. Phillips, Evan M. VanBrocklin, Gennie L. Parkman, and Sheri L. Holmen jointly wrote the paper.
Funding
This research received no external funding
Acknowledgments
We thank the members of the VanBrocklin and Holmen labs for critical review of the manuscript. This work was supported by R01 CA121118 from the National Cancer Institute (to Sheri L. Holmen).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| 18F-FDG | 18F-fluorodeoxyglucose |
| AE | Adverse events |
| ARE | Adverse Radiation Effect |
| AKT | Serine/threonine kinase |
| APE1 | Apurinic/apyrimidinic endodeoxyribonuclease 1 |
| ASCO | American Society of Clinical Oncology |
| ASTRO | American Society for Radiation Oncology |
| BAMs | Border-associated macrophages |
| BBB | Blood-brain barrier |
| BRAF | B-Raf proto-oncogene |
| CAR | Chimeric antigen receptor |
| CDK4/6 | Cyclin-dependent kinase 4/6 |
| CMCs | Circulating melanoma cells |
| CNS | Central nervous system |
| CSF1R | Colony-stimulating factor 1 receptor |
| CTCs | Circulating tumor cells |
| CTL | Cytotoxic T lymphocyte |
| CTLA-4 | Cytotoxic T-lymphocyte antigen 4 |
| ctDNA | Circulating tumor DNA |
| DICER1 | Dicer 1, ribonuclease III |
| DNA | Deoxyribonucleic acid |
| DLTs | Dose limiting toxicities |
| ECM | Extracellular matrix |
| EMT | Epithelial-to-mesenchymal transition |
| ERK | Extracellular signal-regulated kinase |
| FAK | Focal adhesion kinase |
| FATP2 | Fatty acid transport protein 2 |
| FDG-PET | Fluorodeoxyglucose positron emission tomography |
| FET | O-(2-18F-Fluoroethyl)-l-tyrosine |
| GEMM | Genetically-engineered mouse model |
| GM-CSF | Granulocyte-macrophage colony-stimulating factor |
| GTPase | Guanosine triphosphatase |
| HSV-1 | Herpes simplex virus type 1 |
| ICIs | Immune checkpoint inhibitors |
| icPFS | Intracranial progression-free survival |
| IFNβ | Interferon beta |
| IL-8 | Interleukin 8 |
| IL-10 | Interleukin 10 |
| iORR | Intracranial objective response rate |
| IRAEs | Immune-related adverse events |
| MAPK | Mitogen-activated protein kinase |
| MEK | Mitogen-activated protein kinase kinase |
| MITF | Microphthalmia-associated transcription factor |
| MRI | Magnetic resonance imaging |
| MSD | Most Successful Dose |
| NGFR | Nerve growth factor receptor |
| NIH | National Institutes of Health |
| NRAS | Neuroblastoma RAS viral oncogene |
| ORR | Objective response rate |
| OS | overall survival |
| PBRM1 | Polybromo 1 |
| PD-1 | Programmed cell death protein 1 |
| PD-L1 | Programmed death-ligand 1 |
| PDGFR | Platelet-derived growth factor receptor |
| PDX | Patient-derived xenograft |
| PET | Positron emission tomography |
| PFS | progression-free survival |
| PI3K | Phosphatidylinositol 3-kinase |
| PRRX1 | Paired related homeobox 1 |
| PTEN | Phosphatase and tensin homolog |
| RNA | Ribonucleic acid |
| SETD2 | SET domain containing 2 |
| sFRP2 | Secreted frizzled related protein 2 |
| SLC27A2 | Solute carrier family 27 member 2 |
| SNO | Society for Neuro-Oncology |
| SOX10 | SRY-box transcription factor 10 |
| SPARC | Secreted protein acidic and rich in cysteine |
| SRS | Stereotactic radiosurgery |
| S&T | Safety and tolerability |
| TAMs | Tumor-associated macrophages |
| TCF/LEF | Transcription factor / lymphoid enhancer-binding factor |
| TFs | Transcription factors |
| TGF-β | Transforming growth factor beta |
| TME | Tumor microenvironment |
| TVEC | Talimogene Laherparepvec |
| UV | Ultraviolet |
| WBRT | Whole-brain radiotherapy |
| YAP1 | Yes-associated protein 1 |
| ZEB1 | Zinc finger E-box binding homeobox 1 |
| ZEB2/SNAIL2 | Zinc finger E-box binding homeobox 2 / snail family transcriptional repressor 2 |
References
- Sundararajan, S.; Thida, A. M.; Yadlapati, S.; Mukkamalla, S. K. R.; Koya, S. Metastatic Melanoma. In StatPearls; StatPearls Publishing, Copyright © 2025, StatPearls Publishing LLC.: Treasure Island (FL), 2025. [Google Scholar]
- Lee, D.; Yang, A.; McNamara, M.; Kluger, H. M.; Tran, T.; Olino, K.; Clune, J.; Sznol, M.; Ishizuka, J. J. Causes of death and patterns of metastatic disease at the end of life for patients with advanced melanoma in the immunotherapy era. Journal of Clinical Oncology 2024, 42, e21522–e21522. [Google Scholar] [CrossRef]
- Siegel, R. L.; Kratzer, T. B.; Giaquinto, A. N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA Cancer J Clin 2025, 75((1)), 10–45. [Google Scholar] [CrossRef] [PubMed]
- Kahlon, N.; Doddi, S.; Yousif, R.; Najib, S.; Sheikh, T.; Abuhelwa, Z.; Burmeister, C.; Hamouda, D. M. Melanoma Treatments and Mortality Rate Trends in the US, 1975 to 2019. JAMA Netw Open 2022, 5((12)), e2245269. [Google Scholar] [CrossRef] [PubMed]
- Shain, A. H.; Bastian, B. C. From melanocytes to melanomas. Nature Reviews Cancer 2016, 16((6)), 345–358. [Google Scholar] [CrossRef]
- Clark, W. H., Jr.; Elder, D. E.; Guerry, D. t.; Epstein, M. N.; Greene, M. H.; Van Horn, M. A study of tumor progression: the precursor lesions of superficial spreading and nodular melanoma. Hum Pathol 1984, 15((12)), 1147–65. [Google Scholar] [CrossRef]
- Miller, A. J.; Mihm, M. C., Jr. Melanoma. N Engl J Med 2006, 355((1)), 51–65. [Google Scholar] [CrossRef]
- Kasumova, G. G.; Haynes, A. B.; Boland, G. M. Lymphatic versus Hematogenous Melanoma Metastases: Support for Biological Heterogeneity without Clear Clinical Application. J Invest Dermatol 2017, 137((12)), 2466–2468. [Google Scholar] [CrossRef]
- Serratì, S.; Raho, L.; De Giosa, G.; Porcelli, L.; Di Fonte, R.; Fasano, R.; Lacal, P. M.; Graziani, G.; Iacobazzi, R. M.; Azzariti, A. Unraveling vascular mechanisms in melanoma: roles of angiogenesis and vasculogenic mimicry in tumor progression and therapeutic resistance. Cancer Biol Med 2025, 22((11)), 1327–52. [Google Scholar]
- Caramel, J.; Papadogeorgakis, E.; Hill, L.; Browne, G. J.; Richard, G.; Wierinckx, A.; Saldanha, G.; Osborne, J.; Hutchinson, P.; Tse, G.; Lachuer, J.; Puisieux, A.; Pringle, J. H.; Ansieau, S.; Tulchinsky, E. A switch in the expression of embryonic EMT-inducers drives the development of malignant melanoma. Cancer Cell 2013, 24((4)), 466–80. [Google Scholar] [CrossRef]
- Cohen, J. V.; Tawbi, H.; Margolin, K. A.; Amravadi, R.; Bosenberg, M.; Brastianos, P. K.; Chiang, V. L.; de Groot, J.; Glitza, I. C.; Herlyn, M.; Holmen, S. L.; Jilaveanu, L. B.; Lassman, A.; Moschos, S.; Postow, M. A.; Thomas, R.; Tsiouris, J. A.; Wen, P.; White, R. M.; Turnham, T.; Davies, M. A.; Kluger, H. M. Melanoma central nervous system metastases: current approaches, challenges, and opportunities. Pigment Cell Melanoma Res 2016, 29((6)), 627–642. [Google Scholar] [CrossRef]
- Pedersen, S.; Johansen, E. L.; Hojholt, K. L.; Pedersen, M. W.; Mogensen, A. M.; Petersen, S. K.; Haslund, C. A.; Donia, M.; Schmidt, H.; Bastholt, L.; Friis, R.; Svane, I. M.; Ellebaek, E. Survival improvements in patients with melanoma brain metastases and leptomeningeal disease in the modern era: Insights from a nationwide study (2015-2022). Eur J Cancer 2025, 217, 115253. [Google Scholar] [CrossRef] [PubMed]
- Abate-Daga, D.; Ramello, M. C.; Smalley, I.; Forsyth, P. A.; Smalley, K. S. M. The biology and therapeutic management of melanoma brain metastases. Biochem Pharmacol 2018, 153, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Amaral, T.; Niessner, H.; Sinnberg, T.; Thomas, I.; Meiwes, A.; Garbe, C.; Garzarolli, M.; Rauschenberg, R.; Eigentler, T.; Meier, F. An open-label, single-arm, phase II trial of buparlisib in patients with melanoma brain metastases not eligible for surgery or radiosurgery-the BUMPER study. Neurooncol Adv 2020, 2((1)), vdaa140. [Google Scholar] [CrossRef] [PubMed]
- Bonzano, E.; Barruscotti, S.; Chiellino, S.; Montagna, B.; Bonzano, C.; Imarisio, I.; Colombo, S.; Guerrini, F.; Saddi, J.; La Mattina, S.; Tomasini, C. F.; Spena, G.; Pedrazzoli, P.; Lancia, A. Current Treatment Paradigms for Advanced Melanoma with Brain Metastases. Int J Mol Sci 2025, 26((8)). [Google Scholar] [CrossRef] [PubMed]
- Gutzmer, R.; Vordermark, D.; Hassel, J. C.; Krex, D.; Wendl, C.; Schadendorf, D.; Sickmann, T.; Rieken, S.; Pukrop, T.; Höller, C.; Eigentler, T. K.; Meier, F. Melanoma brain metastases - Interdisciplinary management recommendations 2020. Cancer Treat Rev 2020, 89, 102083. [Google Scholar] [CrossRef]
- Long, G. V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A. D.; Brown, M. P.; Wilmott, J. S.; Edwards, J.; Gonzalez, M.; Scolyer, R. A.; Menzies, A. M.; McArthur, G. A. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: a multicentre randomised phase 2 study. Lancet Oncol 2018, 19((5)), 672–681. [Google Scholar] [CrossRef]
- Nowacka, A.; Fajkiel-Madajczyk, A.; Ohla, J.; Woźniak-Dąbrowska, K.; Liss, S.; Gryczka, K.; Smuczyński, W.; Ziółkowska, E.; Bożiłow, D.; Śniegocki, M.; Wiciński, M. Current Treatment of Melanoma Brain Metastases. Cancers (Basel) 2023, 15, 16. [Google Scholar] [CrossRef]
- Tawbi, H. A.; Forsyth, P. A.; Algazi, A.; Hamid, O.; Hodi, F. S.; Moschos, S. J.; Khushalani, N. I.; Lewis, K.; Lao, C. D.; Postow, M. A.; Atkins, M. B.; Ernstoff, M. S.; Reardon, D. A.; Puzanov, I.; Kudchadkar, R. R.; Thomas, R. P.; Tarhini, A.; Pavlick, A. C.; Jiang, J.; Avila, A.; Demelo, S.; Margolin, K. Combined Nivolumab and Ipilimumab in Melanoma Metastatic to the Brain. N Engl J Med 2018, 379((8)), 722–730. [Google Scholar] [CrossRef]
- Ng, M. F.; Simmons, J. L.; Boyle, G. M. Heterogeneity in Melanoma. Cancers (Basel) 2022, 14, 12. [Google Scholar] [CrossRef]
- Beigi, Y. Z.; Lanjanian, H.; Fayazi, R.; Salimi, M.; Hoseyni, B. H. M.; Noroozizadeh, M. H.; Masoudi-Nejad, A. Heterogeneity and molecular landscape of melanoma: implications for targeted therapy. Mol Biomed 2024, 5((1)), 17. [Google Scholar] [CrossRef]
- Chapman, A.; Fernandez del Ama, L.; Ferguson, J.; Kamarashev, J.; Wellbrock, C.; Hurlstone, A. Heterogeneous tumor subpopulations cooperate to drive invasion. Cell Rep 2014, 8((3)), 688–95. [Google Scholar] [CrossRef]
- Shain, A. H.; Yeh, I.; Kovalyshyn, I.; Sriharan, A.; Talevich, E.; Gagnon, A.; Dummer, R.; North, J.; Pincus, L.; Ruben, B.; Rickaby, W.; D'Arrigo, C.; Robson, A.; Bastian, B. C. The Genetic Evolution of Melanoma from Precursor Lesions. N Engl J Med 2015, 373((20)), 1926–36. [Google Scholar] [CrossRef]
- Balch, C. M.; Urist, M. M.; Karakousis, C. P.; Smith, T. J.; Temple, W. J.; Drzewiecki, K.; Jewell, W. R.; Bartolucci, A. A.; Mihm, M. C., Jr.; Barnhill, R. Efficacy of 2-cm surgical margins for intermediate-thickness melanomas (1 to 4 mm). Results of a multi-institutional randomized surgical trial. Ann Surg 1993, 218((3)), 262-7; discussion 267-9. [Google Scholar] [CrossRef] [PubMed]
- Damsky, W. E.; Theodosakis, N.; Bosenberg, M. Melanoma metastasis: new concepts and evolving paradigms. Oncogene 2014, 33((19)), 2413–2422. [Google Scholar] [CrossRef] [PubMed]
- Castellani, G.; Buccarelli, M.; Arasi, M. B.; Rossi, S.; Pisanu, M. E.; Bellenghi, M.; Lintas, C.; Tabolacci, C. BRAF Mutations in Melanoma: Biological Aspects, Therapeutic Implications, and Circulating Biomarkers. Cancers (Basel) 2023, 15, 16. [Google Scholar] [CrossRef] [PubMed]
- Long, G. V.; Menzies, A. M.; Nagrial, A. M.; Haydu, L. E.; Hamilton, A. L.; Mann, G. J.; Hughes, T. M.; Thompson, J. F.; Scolyer, R. A.; Kefford, R. F. Prognostic and clinicopathologic associations of oncogenic BRAF in metastatic melanoma. J Clin Oncol 2011, 29((10)), 1239–46. [Google Scholar] [CrossRef]
- Zengarini, C.; Mussi, M.; Veronesi, G.; Alessandrini, A.; Lambertini, M.; Dika, E. BRAF V600K vs. BRAF V600E: a comparison of clinical and dermoscopic characteristics and response to immunotherapies and targeted therapies. Clin Exp Dermatol 2022, 47((6)), 1131–1136. [Google Scholar] [CrossRef]
- Holderfield, M.; Deuker, M. M.; McCormick, F.; McMahon, M. Targeting RAF kinases for cancer therapy: BRAF-mutated melanoma and beyond. Nat Rev Cancer 2014, 14((7)), 455–67. [Google Scholar] [CrossRef]
- Padua, R. A.; Barrass, N.; Currie, G. A. A novel transforming gene in a human malignant melanoma cell line. Nature 1984, 311((5987)), 671–3. [Google Scholar] [CrossRef]
- Colombino, M.; Capone, M.; Lissia, A.; Cossu, A.; Rubino, C.; De Giorgi, V.; Massi, D.; Fonsatti, E.; Staibano, S.; Nappi, O.; Pagani, E.; Casula, M.; Manca, A.; Sini, M.; Franco, R.; Botti, G.; Caracò, C.; Mozzillo, N.; Ascierto, P. A.; Palmieri, G. BRAF/NRAS mutation frequencies among primary tumors and metastases in patients with melanoma. J Clin Oncol 2012, 30((20)), 2522–9. [Google Scholar] [CrossRef]
- Jakob, J. A.; Bassett, R. L., Jr.; Ng, C. S.; Curry, J. L.; Joseph, R. W.; Alvarado, G. C.; Rohlfs, M. L.; Richard, J.; Gershenwald, J. E.; Kim, K. B.; Lazar, A. J.; Hwu, P.; Davies, M. A. NRAS mutation status is an independent prognostic factor in metastatic melanoma. Cancer 2012, 118((16)), 4014–23. [Google Scholar] [CrossRef] [PubMed]
- Parkman, G. L.; Foth, M.; Kircher, D. A.; Holmen, S. L.; McMahon, M. The role of PI3'-lipid signalling in melanoma initiation, progression and maintenance. Experimental Dermatology 2022, 31((1)), 43–56. [Google Scholar] [CrossRef] [PubMed]
- Marsh Durban, V.; Deuker, M. M.; Bosenberg, M. W.; Phillips, W.; McMahon, M. Differential AKT dependency displayed by mouse models of BRAFV600E-initiated melanoma. J Clin Invest 2013, 123((12)), 5104–18. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P. B.; Kuperwasser, C.; Brunet, J. P.; Ramaswamy, S.; Kuo, W. L.; Gray, J. W.; Naber, S. P.; Weinberg, R. A. The melanocyte differentiation program predisposes to metastasis after neoplastic transformation. Nat Genet 2005, 37((10)), 1047–54. [Google Scholar] [CrossRef]
- Hodis, E.; Watson, I. R.; Kryukov, G. V.; Arold, S. T.; Imielinski, M.; Theurillat, J. P.; Nickerson, E.; Auclair, D.; Li, L.; Place, C.; Dicara, D.; Ramos, A. H.; Lawrence, M. S.; Cibulskis, K.; Sivachenko, A.; Voet, D.; Saksena, G.; Stransky, N.; Onofrio, R. C.; Winckler, W.; Ardlie, K.; Wagle, N.; Wargo, J.; Chong, K.; Morton, D. L.; Stemke-Hale, K.; Chen, G.; Noble, M.; Meyerson, M.; Ladbury, J. E.; Davies, M. A.; Gershenwald, J. E.; Wagner, S. N.; Hoon, D. S.; Schadendorf, D.; Lander, E. S.; Gabriel, S. B.; Getz, G.; Garraway, L. A.; Chin, L. A landscape of driver mutations in melanoma. Cell 2012, 150((2)), 251–63. [Google Scholar] [CrossRef]
- Dankort, D.; Curley, D. P.; Cartlidge, R. A.; Nelson, B.; Karnezis, A. N.; Damsky, W. E., Jr.; You, M. J.; DePinho, R. A.; McMahon, M.; Bosenberg, M. Braf(V600E) cooperates with Pten loss to induce metastatic melanoma. Nat Genet 2009, 41((5)), 544–52. [Google Scholar] [CrossRef]
- Stahl, J. M.; Sharma, A.; Cheung, M.; Zimmerman, M.; Cheng, J. Q.; Bosenberg, M. W.; Kester, M.; Sandirasegarane, L.; Robertson, G. P. Deregulated Akt3 activity promotes development of malignant melanoma. Cancer Res 2004, 64((19)), 7002–10. [Google Scholar] [CrossRef]
- Dai, D. L.; Martinka, M.; Li, G. Prognostic significance of activated Akt expression in melanoma: a clinicopathologic study of 292 cases. J Clin Oncol 2005, 23((7)), 1473–82. [Google Scholar] [CrossRef]
- Davies, M. A.; Stemke-Hale, K.; Lin, E.; Tellez, C.; Deng, W.; Gopal, Y. N.; Woodman, S. E.; Calderone, T. C.; Ju, Z.; Lazar, A. J.; Prieto, V. G.; Aldape, K.; Mills, G. B.; Gershenwald, J. E. Integrated Molecular and Clinical Analysis of AKT Activation in Metastatic Melanoma. Clin Cancer Res 2009, 15((24)), 7538–7546. [Google Scholar]
- Cho, J. H.; Robinson, J. P.; Arave, R. A.; Burnett, W. J.; Kircher, D. A.; Chen, G.; Davies, M. A.; Grossmann, A. H.; VanBrocklin, M. W.; McMahon, M.; Holmen, S. L. AKT1 Activation Promotes Development of Melanoma Metastases. Cell Rep 2015, 13((5)), 898–905. [Google Scholar] [CrossRef]
- Kircher, D. A.; Trombetti, K. A.; Silvis, M. R.; Parkman, G. L.; Fischer, G. M.; Angel, S. N.; Stehn, C. M.; Strain, S. C.; Grossmann, A. H.; Duffy, K. L.; Boucher, K. M.; McMahon, M.; Davies, M. A.; Mendoza, M. C.; VanBrocklin, M. W.; Holmen, S. L. AKT1(E17K) Activates Focal Adhesion Kinase and Promotes Melanoma Brain Metastasis. Mol Cancer Res 2019, 17((9)), 1787–1800. [Google Scholar] [CrossRef] [PubMed]
- Tehranian, C.; Fankhauser, L.; Harter, P. N.; Ratcliffe, C. D. H.; Zeiner, P. S.; Messmer, J. M.; Hoffmann, D. C.; Frey, K.; Westphal, D.; Ronellenfitsch, M. W.; Sahai, E.; Wick, W.; Karreman, M. A.; Winkler, F. The PI3K/Akt/mTOR pathway as a preventive target in melanoma brain metastasis. Neuro Oncol 2022, 24((2)), 213–225. [Google Scholar] [CrossRef] [PubMed]
- Parkman, G. L.; Turapov, T.; Kircher, D. A.; Burnett, W. J.; Stehn, C. M.; O'Toole, K.; Culver, K. M.; Chadwick, A. T.; Elmer, R. C.; Flaherty, R.; Stanley, K. A.; Foth, M.; Lum, D. H.; Judson-Torres, R. L.; Friend, J. E.; VanBrocklin, M. W.; McMahon, M.; Holmen, S. L. Genetic Silencing of AKT Induces Melanoma Cell Death via mTOR Suppression. Molecular Cancer Therapeutics 2024, 23((3)), 301–315. [Google Scholar] [CrossRef] [PubMed]
- Yap, T. A.; Patnaik, A.; Fearen, I.; Olmos, D.; Papadopoulos, K.; Tunariu, N.; Sullivan, D.; Yan, L.; De Bono, J. S.; Tolcher, A. W. First-in-class phase I trial of a selective Akt inhibitor, MK2206 (MK), evaluating alternate day (QOD) and once weekly (QW) doses in advanced cancer patients (pts) with evidence of target modulation and antitumor activity. Journal of Clinical Oncology 28, 3009–3009. [CrossRef]
- Shimizu, T.; Tolcher, A. W.; Papadopoulos, K. P.; Beeram, M.; Rasco, D. W.; Smith, L. S.; Gunn, S.; Smetzer, L.; Mays, T. A.; Kaiser, B.; Wick, M. J.; Alvarez, C.; Cavazos, A.; Mangold, G. L.; Patnaik, A. The Clinical Effect of the Dual-Targeting Strategy Involving PI3K/AKT/mTOR and RAS/MEK/ERK Pathways in Patients with Advanced Cancer. Clinical Cancer Research 2012, 18((8)), 2316–2325. [Google Scholar] [CrossRef]
- Pedri, D.; Karras, P.; Landeloos, E.; Marine, J. C.; Rambow, F. Epithelial-to-mesenchymal-like transition events in melanoma. 2022, 289((5)), 1352–1368. [Google Scholar] [CrossRef]
- Tachibana, M.; Takeda, K.; Nobukuni, Y.; Urabe, K.; Long, J. E.; Meyers, K. A.; Aaronson, S. A.; Miki, T. Ectopic expression of MITF, a gene for Waardenburg syndrome type 2, converts fibroblasts to cells with melanocyte characteristics. Nature Genetics 1996, 14((1)), 50–54. [Google Scholar] [CrossRef]
- Bertolotto, C.; Abbe, P.; Hemesath, T. J.; Bille, K.; Fisher, D. E.; Ortonne, J. P.; Ballotti, R. Microphthalmia gene product as a signal transducer in cAMP-induced differentiation of melanocytes. J Cell Biol 1998, 142((3)), 827–35. [Google Scholar] [CrossRef]
- Buscà, R.; Ballotti, R. Cyclic AMP a key messenger in the regulation of skin pigmentation. Pigment Cell Res 2000, 13((2)), 60–9. [Google Scholar] [CrossRef]
- Price, E. R.; Horstmann, M. A.; Wells, A. G.; Weilbaecher, K. N.; Takemoto, C. M.; Landis, M. W.; Fisher, D. E. alpha-Melanocyte-stimulating hormone signaling regulates expression of microphthalmia, a gene deficient in Waardenburg syndrome. J Biol Chem 1998, 273((49)), 33042–7. [Google Scholar] [CrossRef]
- Chauhan, J. S.; Hölzel, M.; Lambert, J. P.; Buffa, F. M.; Goding, C. R. The MITF regulatory network in melanoma. Pigment Cell Melanoma Res 2022, 35((5)), 517–533. [Google Scholar] [CrossRef]
- Taylor, K. L.; Lister, J. A.; Zeng, Z.; Ishizaki, H.; Anderson, C.; Kelsh, R. N.; Jackson, I. J.; Patton, E. E. Differentiated melanocyte cell division occurs in vivo and is promoted by mutations in Mitf. Development 2011, 138((16)), 3579–89. [Google Scholar] [CrossRef] [PubMed]
- Hoek, K. S.; Schlegel, N. C.; Brafford, P.; Sucker, A.; Ugurel, S.; Kumar, R.; Weber, B. L.; Nathanson, K. L.; Phillips, D. J.; Herlyn, M.; Schadendorf, D.; Dummer, R. Metastatic potential of melanomas defined by specific gene expression profiles with no BRAF signature. Pigment Cell Res 2006, 19((4)), 290–302. [Google Scholar] [CrossRef] [PubMed]
- Carreira, S.; Goodall, J.; Denat, L.; Rodriguez, M.; Nuciforo, P.; Hoek, K. S.; Testori, A.; Larue, L.; Goding, C. R. Mitf regulation of Dia1 controls melanoma proliferation and invasiveness. Genes Dev 2006, 20((24)), 3426–39. [Google Scholar] [CrossRef] [PubMed]
- Takeda, K.; Yasumoto, K.; Takada, R.; Takada, S.; Watanabe, K.; Udono, T.; Saito, H.; Takahashi, K.; Shibahara, S. Induction of melanocyte-specific microphthalmia-associated transcription factor by Wnt-3a. J Biol Chem 2000, 275((19)), 14013–6. [Google Scholar] [CrossRef]
- Dorsky, R. I.; Raible, D. W.; Moon, R. T. Direct regulation of nacre, a zebrafish MITF homolog required for pigment cell formation, by the Wnt pathway. Genes Dev 2000, 14((2)), 158–62. [Google Scholar] [CrossRef]
- Lee, M.; Goodall, J.; Verastegui, C.; Ballotti, R.; Goding, C. R. Direct regulation of the Microphthalmia promoter by Sox10 links Waardenburg-Shah syndrome (WS4)-associated hypopigmentation and deafness to WS2. J Biol Chem 2000, 275((48)), 37978–83. [Google Scholar] [CrossRef]
- Verastegui, C.; Bille, K.; Ortonne, J. P.; Ballotti, R. Regulation of the microphthalmia-associated transcription factor gene by the Waardenburg syndrome type 4 gene, SOX10. J Biol Chem 2000, 275((40)), 30757–60. [Google Scholar] [CrossRef]
- Bondurand, N.; Pingault, V.; Goerich, D. E.; Lemort, N.; Sock, E.; Le Caignec, C.; Wegner, M.; Goossens, M. Interaction among SOX10, PAX3 and MITF, three genes altered in Waardenburg syndrome. Hum Mol Genet 2000, 9((13)), 1907–17. [Google Scholar] [CrossRef]
- Potterf, S. B.; Furumura, M.; Dunn, K. J.; Arnheiter, H.; Pavan, W. J. Transcription factor hierarchy in Waardenburg syndrome: regulation of MITF expression by SOX10 and PAX3. Hum Genet 2000, 107((1)), 1–6. [Google Scholar] [CrossRef]
- Willis, B. C.; Johnson, G.; Wang, J.; Cohen, C. SOX10: a useful marker for identifying metastatic melanoma in sentinel lymph nodes. Appl Immunohistochem Mol Morphol 2015, 23((2)), 109–12. [Google Scholar] [CrossRef] [PubMed]
- Damsky, William E.; Curley, David P.; Santhanakrishnan, M.; Rosenbaum, Lara E.; Platt, James T.; Gould Rothberg, Bonnie E.; Taketo, Makoto M.; Dankort, D.; Rimm, David L.; McMahon, M.; Bosenberg, M. β-Catenin Signaling Controls Metastasis in Braf-Activated Pten-Deficient Melanomas. Cancer Cell 2011, 20((6)), 741–754. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, S. J.; Rambow, F.; Kumasaka, M.; Champeval, D.; Bellacosa, A.; Delmas, V.; Larue, L. Beta-catenin inhibits melanocyte migration but induces melanoma metastasis. Oncogene 2013, 32((17)), 2230–8. [Google Scholar] [CrossRef] [PubMed]
- Alonso, S. R.; Tracey, L.; Ortiz, P.; Pérez-Gómez, B.; Palacios, J.; Pollán, M.; Linares, J.; Serrano, S.; Sáez-Castillo, A. I.; Sánchez, L.; Pajares, R.; Sánchez-Aguilera, A.; Artiga, M. J.; Piris, M. A.; Rodríguez-Peralto, J. L. A High-Throughput Study in Melanoma Identifies Epithelial-Mesenchymal Transition as a Major Determinant of Metastasis. Cancer Research 2007, 67((7)), 3450–3460. [Google Scholar] [CrossRef]
- Shields, B. D.; Koss, B.; Taylor, E. M.; Storey, A. J.; West, K. L.; Byrum, S. D.; Mackintosh, S. G.; Edmondson, R.; Mahmoud, F.; Shalin, S. C.; Tackett, A. J. Loss of E-Cadherin Inhibits CD103 Antitumor Activity and Reduces Checkpoint Blockade Responsiveness in Melanoma. Cancer Res 2019, 79((6)), 1113–1123. [Google Scholar] [CrossRef]
- Vandamme, N.; Denecker, G.; Bruneel, K.; Blancke, G.; Akay, Ö.; Taminau, J.; De Coninck, J.; De Smedt, E.; Skrypek, N.; Van Loocke, W.; Wouters, J.; Nittner, D.; Köhler, C.; Darling, D. S.; Cheng, P. F.; Raaijmakers, M. I. G.; Levesque, M. P.; Mallya, U. G.; Rafferty, M.; Balint, B.; Gallagher, W. M.; Brochez, L.; Huylebroeck, D.; Haigh, J. J.; Andries, V.; Rambow, F.; Van Vlierberghe, P.; Goossens, S.; van den Oord, J. J.; Marine, J. C.; Berx, G. The EMT Transcription Factor ZEB2 Promotes Proliferation of Primary and Metastatic Melanoma While Suppressing an Invasive, Mesenchymal-Like Phenotype. Cancer Res 2020, 80((14)), 2983–2995. [Google Scholar] [CrossRef]
- Casas, E.; Kim, J.; Bendesky, A.; Ohno-Machado, L.; Wolfe, C. J.; Yang, J. Snail2 is an essential mediator of Twist1-induced epithelial mesenchymal transition and metastasis. Cancer Res 2011, 71((1)), 245–54. [Google Scholar] [CrossRef]
- Fenouille, N.; Tichet, M.; Dufies, M.; Pottier, A.; Mogha, A.; Soo, J. K.; Rocchi, S.; Mallavialle, A.; Galibert, M. D.; Khammari, A.; Lacour, J. P.; Ballotti, R.; Deckert, M.; Tartare-Deckert, S. The epithelial-mesenchymal transition (EMT) regulatory factor SLUG (SNAI2) is a downstream target of SPARC and AKT in promoting melanoma cell invasion. PLoS One 2012, 7((7)), e40378. [Google Scholar] [CrossRef]
- Meng, Z.; Chen, Y.; Wu, W.; Yan, B.; Zhang, L.; Chen, H.; Meng, Y.; Liang, Y.; Yao, X.; Luo, J. PRRX1 Is a Novel Prognostic Biomarker and Facilitates Tumor Progression Through Epithelial-Mesenchymal Transition in Uveal Melanoma. Front Immunol 2022, 13, 754645. [Google Scholar] [CrossRef]
- Arozarena, I.; Bischof, H.; Gilby, D.; Belloni, B.; Dummer, R.; Wellbrock, C. In melanoma, beta-catenin is a suppressor of invasion. Oncogene 2011, 30((45)), 4531–43. [Google Scholar] [CrossRef]
- O'Day, S. J.; Hamid, O.; Urba, W. J. Targeting cytotoxic T-lymphocyte antigen-4 (CTLA-4): a novel strategy for the treatment of melanoma and other malignancies. Cancer 2007, 110((12)), 2614–27. [Google Scholar] [CrossRef]
- Hodi, F. S.; O'Day, S. J.; McDermott, D. F.; Weber, R. W.; Sosman, J. A.; Haanen, J. B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J. C.; Akerley, W.; van den Eertwegh, A. J.; Lutzky, J.; Lorigan, P.; Vaubel, J. M.; Linette, G. P.; Hogg, D.; Ottensmeier, C. H.; Lebbé, C.; Peschel, C.; Quirt, I.; Clark, J. I.; Wolchok, J. D.; Weber, J. S.; Tian, J.; Yellin, M. J.; Nichol, G. M.; Hoos, A.; Urba, W. J. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 2010, 363((8)), 711–23. [Google Scholar] [CrossRef]
- Tarhini, A. A.; Kirkwood, J. M. Tremelimumab, a fully human monoclonal IgG2 antibody against CTLA4 for the potential treatment of cancer. Curr Opin Mol Ther 2007, 9((5)), 505–14. [Google Scholar] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J. J.; Cowey, C. L.; Lao, C. D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; Ferrucci, P. F.; Hill, A.; Wagstaff, J.; Carlino, M. S.; Haanen, J. B.; Maio, M.; Marquez-Rodas, I.; McArthur, G. A.; Ascierto, P. A.; Long, G. V.; Callahan, M. K.; Postow, M. A.; Grossmann, K.; Sznol, M.; Dreno, B.; Bastholt, L.; Yang, A.; Rollin, L. M.; Horak, C.; Hodi, F. S.; Wolchok, J. D. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N Engl J Med 2015, 373((1)), 23–34. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Schachter, J.; Long, G. V.; Arance, A.; Grob, J. J.; Mortier, L.; Daud, A.; Carlino, M. S.; McNeil, C.; Lotem, M.; Larkin, J.; Lorigan, P.; Neyns, B.; Blank, C. U.; Hamid, O.; Mateus, C.; Shapira-Frommer, R.; Kosh, M.; Zhou, H.; Ibrahim, N.; Ebbinghaus, S.; Ribas, A. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N Engl J Med 2015, 372((26)), 2521–32. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Long, G. V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J. C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; Savage, K. J.; Hernberg, M. M.; Lebbé, C.; Charles, J.; Mihalcioiu, C.; Chiarion-Sileni, V.; Mauch, C.; Cognetti, F.; Arance, A.; Schmidt, H.; Schadendorf, D.; Gogas, H.; Lundgren-Eriksson, L.; Horak, C.; Sharkey, B.; Waxman, I. M.; Atkinson, V.; Ascierto, P. A. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med 2015, 372((4)), 320–30. [Google Scholar] [CrossRef]
- Valpione, S.; Galvani, E.; Tweedy, J.; Mundra, P. A.; Banyard, A.; Middlehurst, P.; Barry, J.; Mills, S.; Salih, Z.; Weightman, J.; Gupta, A.; Gremel, G.; Baenke, F.; Dhomen, N.; Lorigan, P. C.; Marais, R. Immune-awakening revealed by peripheral T cell dynamics after one cycle of immunotherapy. Nat Cancer 2020, 1((2)), 210–221. [Google Scholar] [CrossRef]
- Robert, C.; Thomas, L.; Bondarenko, I.; O'Day, S.; Weber, J.; Garbe, C.; Lebbe, C.; Baurain, J. F.; Testori, A.; Grob, J. J.; Davidson, N.; Richards, J.; Maio, M.; Hauschild, A.; Miller, W. H., Jr.; Gascon, P.; Lotem, M.; Harmankaya, K.; Ibrahim, R.; Francis, S.; Chen, T. T.; Humphrey, R.; Hoos, A.; Wolchok, J. D. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med 2011, 364((26)), 2517–26. [Google Scholar] [CrossRef]
- Maas, R. R.; Soukup, K.; Fournier, N.; Massara, M.; Galland, S.; Kornete, M.; Wischnewski, V.; Lourenco, J.; Croci, D.; Álvarez-Prado, Á. F.; Marie, D. N.; Lilja, J.; Marcone, R.; Calvo, G. F.; Santalla Mendez, R.; Aubel, P.; Bejarano, L.; Wirapati, P.; Ballesteros, I.; Hidalgo, A.; Hottinger, A. F.; Brouland, J.-P.; Daniel, R. T.; Hegi, M. E.; Joyce, J. A. The local microenvironment drives activation of neutrophils in human brain tumors. Cell 2023, 186((21)), 4546–4566.e27. [Google Scholar] [CrossRef]
- Alvarez-Breckenridge, C.; Markson, S. C.; Stocking, J. H.; Nayyar, N.; Lastrapes, M.; Strickland, M. R.; Kim, A. E.; de Sauvage, M.; Dahal, A.; Larson, J. M.; Mora, J. L.; Navia, A. W.; Klein, R. H.; Kuter, B. M.; Gill, C. M.; Bertalan, M.; Shaw, B.; Kaplan, A.; Subramanian, M.; Jain, A.; Kumar, S.; Danish, H.; White, M.; Shahid, O.; Pauken, K. E.; Miller, B. C.; Frederick, D. T.; Hebert, C.; Shaw, M.; Martinez-Lage, M.; Frosch, M.; Wang, N.; Gerstner, E.; Nahed, B. V.; Curry, W. T.; Carter, B.; Cahill, D. P.; Boland, G. M.; Izar, B.; Davies, M. A.; Sharpe, A. H.; Suvà, M. L.; Sullivan, R. J.; Brastianos, P. K.; Carter, S. L. Microenvironmental Landscape of Human Melanoma Brain Metastases in Response to Immune Checkpoint Inhibition. Cancer Immunol Res 2022, 10((8)), 996–1012. [Google Scholar] [CrossRef]
- Gonzalez, H.; Mei, W.; Robles, I.; Hagerling, C.; Allen, B. M.; Hauge Okholm, T. L.; Nanjaraj, A.; Verbeek, T.; Kalavacherla, S.; van Gogh, M.; Georgiou, S.; Daras, M.; Phillips, J. J.; Spitzer, M. H.; Roose, J. P.; Werb, Z. Cellular architecture of human brain metastases. Cell 2022, 185((4)), 729–745.e20. [Google Scholar] [CrossRef] [PubMed]
- Willsmore, Z. N.; Harris, R. J.; Crescioli, S.; Hussein, K.; Kakkassery, H.; Thapa, D.; Cheung, A.; Chauhan, J.; Bax, H. J.; Chenoweth, A.; Laddach, R.; Osborn, G.; McCraw, A.; Hoffmann, R. M.; Nakamura, M.; Geh, J. L.; MacKenzie-Ross, A.; Healy, C.; Tsoka, S.; Spicer, J. F.; Papa, S.; Barber, L.; Lacy, K. E.; Karagiannis, S. N. B Cells in Patients With Melanoma: Implications for Treatment With Checkpoint Inhibitor Antibodies. Front Immunol 2020, 11, 622442. [Google Scholar] [CrossRef] [PubMed]
- Mazurkiewicz, J.; Simiczyjew, A.; Dratkiewicz, E.; Ziętek, M.; Matkowski, R.; Nowak, D. Stromal Cells Present in the Melanoma Niche Affect Tumor Invasiveness and Its Resistance to Therapy. Int J Mol Sci 2021, 22((2)). [Google Scholar] [CrossRef] [PubMed]
- Ramaglia, V.; Florescu, A.; Zuo, M.; Sheikh-Mohamed, S.; Gommerman, J. L. Stromal Cell-Mediated Coordination of Immune Cell Recruitment, Retention, and Function in Brain-Adjacent Regions. J Immunol 2021, 206((2)), 282–291. [Google Scholar] [CrossRef]
- Zhao, Y.; Shen, M.; Wu, L.; Yang, H.; Yao, Y.; Yang, Q.; Du, J.; Liu, L.; Li, Y.; Bai, Y. Stromal cells in the tumor microenvironment: accomplices of tumor progression? Cell Death Dis 2023, 14((9)), 587. [Google Scholar] [CrossRef]
- Xiao, Y.; Zhou, L.; Andl, T.; Zhang, Y. YAP1 controls the N-cadherin-mediated tumor-stroma interaction in melanoma progression. Oncogene 2024, 43((12)), 884–898. [Google Scholar] [CrossRef]
- Purushothaman, A.; Uyama, T.; Kobayashi, F.; Yamada, S.; Sugahara, K.; Rapraeger, A. C.; Sanderson, R. D. Heparanase-enhanced shedding of syndecan-1 by myeloma cells promotes endothelial invasion and angiogenesis. Blood 2010, 115((12)), 2449–57. [Google Scholar] [CrossRef]
- Liu, Y.; Lv, J.; Liang, X.; Yin, X.; Zhang, L.; Chen, D.; Jin, X.; Fiskesund, R.; Tang, K.; Ma, J.; Zhang, H.; Dong, W.; Mo, S.; Zhang, T.; Cheng, F.; Zhou, Y.; Xie, J.; Wang, N.; Huang, B. Fibrin Stiffness Mediates Dormancy of Tumor-Repopulating Cells via a Cdc42-Driven Tet2 Epigenetic Program. Cancer Research 2018, 78((14)), 3926–3937. [Google Scholar] [CrossRef]
- Alicea, G. M.; Rebecca, V. W.; Goldman, A. R.; Fane, M. E.; Douglass, S. M.; Behera, R.; Webster, M. R.; Kugel, C. H., 3rd; Ecker, B. L.; Caino, M. C.; Kossenkov, A. V.; Tang, H. Y.; Frederick, D. T.; Flaherty, K. T.; Xu, X.; Liu, Q.; Gabrilovich, D. I.; Herlyn, M.; Blair, I. A.; Schug, Z. T.; Speicher, D. W.; Weeraratna, A. T. Changes in Aged Fibroblast Lipid Metabolism Induce Age-Dependent Melanoma Cell Resistance to Targeted Therapy via the Fatty Acid Transporter FATP2. Cancer Discov 2020, 10((9)), 1282–1295. [Google Scholar] [CrossRef]
- Alicea, G. M.; Patel, P.; Portuallo, M. E.; Fane, M. E.; Wei, M.; Chhabra, Y.; Dixit, A.; Carey, A. E.; Wang, V.; Rocha, M. R.; Behera, R.; Speicher, D. W.; Tang, H.-Y.; Kossenkov, A. V.; Rebecca, V. W.; Wirtz, D.; Weeraratna, A. T. Age-Related Increases in IGFBP2 Increase Melanoma Cell Invasion and Lipid Synthesis. Cancer Research Communications 2024, 4((8)), 1908–1918. [Google Scholar] [CrossRef]
- García-Silva, S.; Benito-Martín, A.; Nogués, L.; Hernández-Barranco, A.; Mazariegos, M. S.; Santos, V.; Hergueta-Redondo, M.; Ximénez-Embún, P.; Kataru, R. P.; Lopez, A. A.; Merino, C.; Sánchez-Redondo, S.; Graña-Castro, O.; Matei, I.; Nicolás-Avila, J.; Torres-Ruiz, R.; Rodríguez-Perales, S.; Martínez, L.; Pérez-Martínez, M.; Mata, G.; Szumera-Ciećkiewicz, A.; Kalinowska, I.; Saltari, A.; Martínez-Gómez, J. M.; Hogan, S. A.; Saragovi, H. U.; Ortega, S.; Garcia-Martin, C.; Boskovic, J.; Levesque, M. P.; Rutkowski, P.; Hidalgo, A.; Muñoz, J.; Megías, D.; Mehrara, B. J.; Lyden, D.; Peinado, H. Melanoma-derived small extracellular vesicles induce lymphangiogenesis and metastasis through an NGFR-dependent mechanism. Nat Cancer 2021, 2((12)), 1387–1405. [Google Scholar] [CrossRef] [PubMed]
- Gumusay, O.; Coskun, U.; Akman, T.; Ekinci, A. S.; Kocar, M.; Erceleb, O. B.; Yazıcı, O.; Kaplan, M. A.; Berk, V.; Cetin, B.; Taskoylu, B. Y.; Yildiz, A.; Goksel, G.; Alacacioglu, A.; Demirci, U.; Algin, E.; Uysal, M.; Oztop, I.; Oksuzoglu, B.; Dane, F.; Gumus, M.; Buyukberber, S. Predictive factors for the development of brain metastases in patients with malignant melanoma: a study by the Anatolian society of medical oncology. J Cancer Res Clin Oncol 2014, 140((1)), 151–7. [Google Scholar] [CrossRef] [PubMed]
- Taillibert, S.; Le Rhun, É. Epidemiology of brain metastases. Cancer Radiother 2015, 19((1)), 3–9. [Google Scholar] [CrossRef] [PubMed]
- Maher, E. A.; Mietz, J.; Arteaga, C. L.; DePinho, R. A.; Mohla, S. Brain metastasis: opportunities in basic and translational research. Cancer Res 2009, 69((15)), 6015–20. [Google Scholar] [CrossRef]
- Cioffi, G.; Ascha, M. S.; Waite, K. A.; Dmukauskas, M.; Wang, X.; Royce, T. J.; Calip, G. S.; Waxweiler, T.; Rusthoven, C. G.; Kavanagh, B. D.; Barnholtz-Sloan, J. S. Sex Differences in Odds of Brain Metastasis and Outcomes by Brain Metastasis Status after Advanced Melanoma Diagnosis. Cancers (Basel) 2024, 16((9)). [Google Scholar] [CrossRef]
- Wilhelm, I.; Molnár, J.; Fazakas, C.; Haskó, J.; Krizbai, I. A. Role of the blood-brain barrier in the formation of brain metastases. Int J Mol Sci 2013, 14((1)), 1383–411. [Google Scholar] [CrossRef]
- Kienast, Y.; von Baumgarten, L.; Fuhrmann, M.; Klinkert, W. E.; Goldbrunner, R.; Herms, J.; Winkler, F. Real-time imaging reveals the single steps of brain metastasis formation. Nat Med 2010, 16((1)), 116–22. [Google Scholar] [CrossRef]
- Anchan, A.; Kalogirou-Baldwin, P.; Johnson, R.; Kho, D. T.; Joseph, W.; Hucklesby, J.; Finlay, G. J.; O'Carroll, S. J.; Angel, C. E.; Graham, E. S. Real-Time Measurement of Melanoma Cell-Mediated Human Brain Endothelial Barrier Disruption Using Electric Cell-Substrate Impedance Sensing Technology. Biosensors (Basel) 2019, 9((2)). [Google Scholar] [CrossRef]
- Anchan, A.; Martin, O.; Hucklesby, J. J. W.; Finlay, G.; Johnson, R. H.; Robilliard, L. D.; O'Carroll, S. J.; Angel, C. E.; Graham, E. S. Analysis of Melanoma Secretome for Factors That Directly Disrupt the Barrier Integrity of Brain Endothelial Cells. Int J Mol Sci 2020, 21, 21. [Google Scholar] [CrossRef]
- Saxena, M.; Christofori, G. Rebuilding cancer metastasis in the mouse. Mol Oncol 2013, 7((2)), 283–96. [Google Scholar] [CrossRef]
- Obenauf, A. C.; Massagué, J. Surviving at a Distance: Organ-Specific Metastasis. Trends Cancer 2015, 1((1)), 76–91. [Google Scholar] [CrossRef]
- Soto, M. S.; Serres, S.; Anthony, D. C.; Sibson, N. R. Functional role of endothelial adhesion molecules in the early stages of brain metastasis. Neuro Oncol 2014, 16((4)), 540–51. [Google Scholar] [CrossRef]
- Scalise, A. A.; Kakogiannos, N.; Zanardi, F.; Iannelli, F.; Giannotta, M. The blood-brain and gut-vascular barriers: from the perspective of claudins. Tissue Barriers 2021, 9((3)), 1926190. [Google Scholar] [CrossRef]
- Fitzgerald, D. P.; Palmieri, D.; Hua, E.; Hargrave, E.; Herring, J. M.; Qian, Y.; Vega-Valle, E.; Weil, R. J.; Stark, A. M.; Vortmeyer, A. O.; Steeg, P. S. Reactive glia are recruited by highly proliferative brain metastases of breast cancer and promote tumor cell colonization. Clin Exp Metastasis 2008, 25((7)), 799–810. [Google Scholar] [CrossRef] [PubMed]
- Placone, A. L.; Quiñones-Hinojosa, A.; Searson, P. C. The role of astrocytes in the progression of brain cancer: complicating the picture of the tumor microenvironment. Tumour Biol 2016, 37((1)), 61–9. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, S.; Scomparin, A.; Ben-Shushan, D.; Yeini, E.; Ofek, P.; Nahmad, A. D.; Soffer, S.; Ionescu, A.; Ruggiero, A.; Barzel, A.; Brem, H.; Hyde, T. M.; Barshack, I.; Sinha, S.; Ruppin, E.; Weiss, T.; Madi, A.; Perlson, E.; Slutsky, I.; Florindo, H. F.; Satchi-Fainaro, R. MCP-1/CCR2 axis inhibition sensitizes the brain microenvironment against melanoma brain metastasis progression. JCI Insight 2022, 7, (17). [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhang, S.; Yao, J.; Lowery, F. J.; Zhang, Q.; Huang, W. C.; Li, P.; Li, M.; Wang, X.; Zhang, C.; Wang, H.; Ellis, K.; Cheerathodi, M.; McCarty, J. H.; Palmieri, D.; Saunus, J.; Lakhani, S.; Huang, S.; Sahin, A. A.; Aldape, K. D.; Steeg, P. S.; Yu, D. Microenvironment-induced PTEN loss by exosomal microRNA primes brain metastasis outgrowth. Nature 2015, 527((7576)), 100–104. [Google Scholar] [CrossRef]
- Rodriguez-Baena, F. J.; Marquez-Galera, A.; Ballesteros-Martinez, P.; Castillo, A.; Diaz, E.; Moreno-Bueno, G.; Lopez-Atalaya, J. P.; Sanchez-Laorden, B. Microglial reprogramming enhances antitumor immunity and immunotherapy response in melanoma brain metastases. Cancer Cell 2025, 43((3)), 413–427.e9. [Google Scholar] [CrossRef]
- In, G. K.; Poorman, K.; Saul, M.; O'Day, S.; Farma, J. M.; Olszanski, A. J.; Gordon, M. S.; Thomas, J. S.; Eisenberg, B.; Flaherty, L.; Weise, A.; Daveluy, S.; Gibney, G.; Atkins, M. B.; Vanderwalde, A. Molecular profiling of melanoma brain metastases compared to primary cutaneous melanoma and to extracranial metastases. Oncotarget 2020, 11((33)), 3118–3128. [Google Scholar] [CrossRef]
- Biermann, J.; Melms, J. C.; Amin, A. D.; Wang, Y.; Caprio, L. A.; Karz, A.; Tagore, S.; Barrera, I.; Ibarra-Arellano, M. A.; Andreatta, M.; Fullerton, B. T.; Gretarsson, K. H.; Sahu, V.; Mangipudy, V. S.; Nguyen, T. T. T.; Nair, A.; Rogava, M.; Ho, P.; Koch, P. D.; Banu, M.; Humala, N.; Mahajan, A.; Walsh, Z. H.; Shah, S. B.; Vaccaro, D. H.; Caldwell, B.; Mu, M.; Wunnemann, F.; Chazotte, M.; Berhe, S.; Luoma, A. M.; Driver, J.; Ingham, M.; Khan, S. A.; Rapisuwon, S.; Slingluff, C. L., Jr.; Eigentler, T.; Rocken, M.; Carvajal, R.; Atkins, M. B.; Davies, M. A.; Agustinus, A.; Bakhoum, S. F.; Azizi, E.; Siegelin, M.; Lu, C.; Carmona, S. J.; Hibshoosh, H.; Ribas, A.; Canoll, P.; Bruce, J. N.; Bi, W. L.; Agrawal, P.; Schapiro, D.; Hernando, E.; Macosko, E. Z.; Chen, F.; Schwartz, G. K.; Izar, B. Dissecting the treatment-naive ecosystem of human melanoma brain metastasis. Cell 2022, 185((14)), 2591–2608 e30. [Google Scholar] [CrossRef]
- (NCCN), N. C. C. N., NCCN clinical practice guidelines in oncology: melanoma. 2026, Version 1.2026.
- Gaviani, P.; Mullins, M. E.; Braga, T. A.; Hedley-Whyte, E. T.; Halpern, E. F.; Schaefer, P. S.; Henson, J. W. Improved detection of metastatic melanoma by T2*-weighted imaging. AJNR Am J Neuroradiol 2006, 27((3)), 605–8. [Google Scholar] [PubMed]
- Escott, E. J. A variety of appearances of malignant melanoma in the head: a review. Radiographics 2001, 21((3)), 625–39. [Google Scholar] [CrossRef] [PubMed]
- Venur, V. A.; Funchain, P.; Kotecha, R.; Chao, S. T.; Ahluwalia, M. S. Changing Treatment Paradigms for Brain Metastases From Melanoma-Part 1: Diagnosis, Prognosis, Symptom Control, and Local Treatment. Oncology (Williston Park) 2017, 31((8)), 602–6. [Google Scholar] [PubMed]
- Schroeder, H. W.; Hall, L. T. Molecular Imaging of Brain Metastases with PET. In Metastasis; Sergi, C. M., Ed. Exon Publications Copyright: The Authors.: Brisbane (AU); The authors confirm that the materials included in this chapter do not violate copyright laws. Where relevant, appropriate permissions have been obtained from the original copyright holder(s), and all original sources have been appropriately acknowledged or referenced., 2022. [Google Scholar]
- Tabassum, M.; Suman, A. A.; Suero Molina, E.; Pan, E.; Di Ieva, A.; Liu, S. Radiomics and Machine Learning in Brain Tumors and Their Habitat: A Systematic Review. Cancers (Basel) 2023, 15, 15. [Google Scholar] [CrossRef]
- Parekh, V.; Jacobs, M. A. Radiomics: a new application from established techniques. Expert Rev Precis Med Drug Dev 2016, 1((2)), 207–226. [Google Scholar] [CrossRef]
- Ricciardi, E.; Giordani, E.; Ziccheddu, G.; Falcone, I.; Giacomini, P.; Fanciulli, M.; Russillo, M.; Cerro, M.; Ciliberto, G.; Morrone, A.; Guerrisi, A.; Valenti, F. Metastatic Melanoma: Liquid Biopsy as a New Precision Medicine Approach. Int J Mol Sci 2023, 24((4)). [Google Scholar] [CrossRef]
- Kamińska, P.; Buszka, K.; Zabel, M.; Nowicki, M.; Alix-Panabières, C.; Budna-Tukan, J. Liquid Biopsy in Melanoma: Significance in Diagnostics, Prediction and Treatment Monitoring. Int J Mol Sci 2021, 22((18)). [Google Scholar] [CrossRef]
- Alix-Panabières, C.; Mader, S.; Pantel, K. Epithelial-mesenchymal plasticity in circulating tumor cells. J Mol Med (Berl) 2017, 95((2)), 133–142. [Google Scholar] [CrossRef]
- Forschner, A.; Battke, F.; Hadaschik, D.; Schulze, M.; Weißgraeber, S.; Han, C. T.; Kopp, M.; Frick, M.; Klumpp, B.; Tietze, N.; Amaral, T.; Martus, P.; Sinnberg, T.; Eigentler, T.; Keim, U.; Garbe, C.; Döcker, D.; Biskup, S. Tumor mutation burden and circulating tumor DNA in combined CTLA-4 and PD-1 antibody therapy in metastatic melanoma - results of a prospective biomarker study. J Immunother Cancer 2019, 7((1)), 180. [Google Scholar] [CrossRef]
- Lin, J.; Li, J.; Huang, B.; Liu, J.; Chen, X.; Chen, X. M.; Xu, Y. M.; Huang, L. F.; Wang, X. Z. Exosomes: novel biomarkers for clinical diagnosis. ScientificWorldJournal 2015, 2015, 657086. [Google Scholar] [CrossRef]
- Nedaeinia, R.; Manian, M.; Jazayeri, M. H.; Ranjbar, M.; Salehi, R.; Sharifi, M.; Mohaghegh, F.; Goli, M.; Jahednia, S. H.; Avan, A.; Ghayour-Mobarhan, M. Circulating exosomes and exosomal microRNAs as biomarkers in gastrointestinal cancer. Cancer Gene Ther 2017, 24((2)), 48–56. [Google Scholar] [CrossRef] [PubMed]
- Kalluri, R. The biology and function of exosomes in cancer. J Clin Invest 2016, 126((4)), 1208–15. [Google Scholar] [CrossRef] [PubMed]
- Namee, N. M.; O'Driscoll, L. Extracellular vesicles and anti-cancer drug resistance. Biochim Biophys Acta Rev Cancer 2018, 1870((2)), 123–136. [Google Scholar] [CrossRef] [PubMed]
- Cesi, G.; Philippidou, D.; Kozar, I.; Kim, Y. J.; Bernardin, F.; Van Niel, G.; Wienecke-Baldacchino, A.; Felten, P.; Letellier, E.; Dengler, S.; Nashan, D.; Haan, C.; Kreis, S. A new ALK isoform transported by extracellular vesicles confers drug resistance to melanoma cells. Mol Cancer 2018, 17((1)), 145. [Google Scholar] [CrossRef]
- Vella, L. J.; Behren, A.; Coleman, B.; Greening, D. W.; Hill, A. F.; Cebon, J. Intercellular Resistance to BRAF Inhibition Can Be Mediated by Extracellular Vesicle-Associated PDGFRβ. Neoplasia 2017, 19((11)), 932–940. [Google Scholar] [CrossRef]
- Amolegbe, S. M.; Johnston, N. C.; Ambrosi, A.; Ganguly, A.; Howcroft, T. K.; Kuo, L. S.; Labosky, P. A.; Rudnicki, D. D.; Satterlee, J. S.; Tagle, D. A.; Happel, C. Extracellular RNA communication: A decade of NIH common fund support illuminates exRNA biology. J Extracell Vesicles 2025, 14((1)), e70016. [Google Scholar] [CrossRef]
- Carthew, R. W.; Sontheimer, E. J. Origins and Mechanisms of miRNAs and siRNAs. Cell 2009, 136((4)), 642–55. [Google Scholar] [CrossRef]
- Meister, G. Argonaute proteins: functional insights and emerging roles. Nat Rev Genet 2013, 14((7)), 447–59. [Google Scholar] [CrossRef]
- Moncrieff, M. D.; Lo, S. N.; Scolyer, R. A.; Heaton, M. J.; Nobes, J. P.; Snelling, A. P.; Carr, M. J.; Nessim, C.; Wade, R.; Peach, A. H.; Kisyova, R.; Mason, J.; Wilson, E. D.; Nolan, G.; Pritchard Jones, R.; Johansson, I.; Olofsson Bagge, R.; Wright, L. J.; Patel, N. G.; Sondak, V. K.; Thompson, J. F.; Zager, J. S. Clinical Outcomes and Risk Stratification of Early-Stage Melanoma Micrometastases From an International Multicenter Study: Implications for the Management of American Joint Committee on Cancer IIIA Disease. J Clin Oncol 2022, 40((34)), 3940–3951. [Google Scholar] [CrossRef]
- MacKie, R. M.; Reid, R.; Junor, B. Fatal melanoma transferred in a donated kidney 16 years after melanoma surgery. N Engl J Med 2003, 348((6)), 567–8. [Google Scholar] [CrossRef]
- Li, Y.; Ma, Y.; Wu, Z.; Xie, R.; Zeng, F.; Cai, H.; Lui, S.; Song, B.; Chen, L.; Wu, M. Advanced Imaging Techniques for Differentiating Pseudoprogression and Tumor Recurrence After Immunotherapy for Glioblastoma. Front Immunol 2021, 12, 790674. [Google Scholar] [CrossRef]
- Mao, X.; Mei, R.; Yu, S.; Shou, L.; Zhang, W.; Li, K.; Qiu, Z.; Xie, T.; Sui, X. Emerging Technologies for the Detection of Cancer Micrometastasis. Technol Cancer Res Treat 2022, 21, 15330338221100355. [Google Scholar] [CrossRef]
- Gaebe, K.; Li, A. Y.; Das, S. Clinical Biomarkers for Early Identification of Patients with Intracranial Metastatic Disease. Cancers (Basel) 2021, 13, 23. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.; Lee, D.; Shim, H. Metabolic positron emission tomography imaging in cancer detection and therapy response. Semin Oncol 2011, 38((1)), 55–69. [Google Scholar] [CrossRef] [PubMed]
- Galldiks, N.; Unterrainer, M.; Judov, N.; Stoffels, G.; Rapp, M.; Lohmann, P.; Vettermann, F.; Dunkl, V.; Suchorska, B.; Tonn, J. C.; Kreth, F. W.; Fink, G. R.; Bartenstein, P.; Langen, K. J.; Albert, N. L. Photopenic defects on O-(2-[18F]-fluoroethyl)-L-tyrosine PET: clinical relevance in glioma patients. Neuro Oncol 2019, 21((10)), 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J. F.; Williams, G. J.; Hong, A. M. Radiation therapy for melanoma brain metastases: a systematic review. Radiol Oncol 2022, 56((3)), 267–284. [Google Scholar] [CrossRef]
- Caruso, G.; Garcia Moreira, C. G.; Iaboni, E.; Tripodo, M.; Ferrarotto, R.; Abbritti, R. V.; Conte, L.; Caffo, M. Tumor Microenvironment in Melanoma Brain Metastasis: A New Potential Target? Int J Mol Sci 2025, 26((11)). [Google Scholar] [CrossRef]
- Sloot, S.; Chen, Y. A.; Zhao, X.; Weber, J. L.; Benedict, J. J.; Mulé, J. J.; Smalley, K. S.; Weber, J. S.; Zager, J. S.; Forsyth, P. A.; Sondak, V. K.; Gibney, G. T. Improved survival of patients with melanoma brain metastases in the era of targeted BRAF and immune checkpoint therapies. Cancer 2018, 124((2)), 297–305. [Google Scholar] [CrossRef]
- Ene, C. I.; Ferguson, S. D. Surgical Management of Brain Metastasis: Challenges and Nuances. Front Oncol 2022, 12, 847110. [Google Scholar] [CrossRef]
- Proescholdt, M. A.; Schödel, P.; Doenitz, C.; Pukrop, T.; Höhne, J.; Schmidt, N. O.; Schebesch, K.-M. The Management of Brain Metastases—Systematic Review of Neurosurgical Aspects. Cancers 2021, Vol. 13, 1616. [Google Scholar] [CrossRef]
- Hall, W. A.; Das, J. M. Stereotactic Radiosurgery (SRS) and Stereotactic Body Radiotherapy (SBRT). In StatPearls; StatPearls Publishing, Copyright © 2025, StatPearls Publishing LLC.: Treasure Island (FL), 2025. [Google Scholar]
- Manon, R.; O'Neill, A.; Knisely, J.; Werner-Wasik, M.; Lazarus, H. M.; Wagner, H.; Gilbert, M.; Mehta, M. Phase II trial of radiosurgery for one to three newly diagnosed brain metastases from renal cell carcinoma, melanoma, and sarcoma: an Eastern Cooperative Oncology Group study (E 6397). J Clin Oncol 2005, 23((34)), 8870–6. [Google Scholar] [CrossRef] [PubMed]
- Alrasheed, A. S.; Aleid, A. M.; Alharbi, R. A.; Alamer, M. A.; Alomran, K. A.; Bin Maan, S. A.; Almalki, S. F. Stereotactic radiosurgery versus whole-brain radiotherapy for intracranial metastases: A systematic review and meta-analysis. Surg Neurol Int 2025, 16, 18. [Google Scholar] [CrossRef] [PubMed]
- Amseian, G.; Aya, F.; Pineda, C.; González-Ortiz, S.; Mora, J. A.; Olondo, M. L.; Perissinotti, A.; Caballero, G. A.; Aldecoa, I.; Mezquita, L.; Puig, J.; Arance, A.; Bargalló, N.; Oleaga, L. Assessing brain metastasis response to immunotherapy: a pictorial review of atypical responses and intracranial adverse events. Insights Imaging 2025, 16((1)), 258. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Heisterkamp, C.; Huttenlocher, S.; Bohlen, G.; Dunst, J.; Haatanen, T.; Schild, S. E. Dose escalation of whole-brain radiotherapy for brain metastases from melanoma. Int J Radiat Oncol Biol Phys 2010, 77((2)), 537–41. [Google Scholar] [CrossRef]
- de la Fuente, M.; Beal, K.; Carvajal, R.; Kaley, T. J. Whole-brain radiotherapy in patients with brain metastases from melanoma. CNS Oncol 2014, 3((6)), 401–6. [Google Scholar] [CrossRef]
- Agarwala, S. S.; Kirkwood, J. M.; Gore, M.; Dreno, B.; Thatcher, N.; Czarnetski, B.; Atkins, M.; Buzaid, A.; Skarlos, D.; Rankin, E. M. Temozolomide for the treatment of brain metastases associated with metastatic melanoma: a phase II study. J Clin Oncol 2004, 22((11)), 2101–7. [Google Scholar] [CrossRef]
- Chang, J.; Atkinson, H.; A'Hern, R.; Lorentzos, A.; Gore, M. E. A phase II study of the sequential administration of dacarbazine and fotemustine in the treatment of cerebral metastases from malignant melanoma. Eur J Cancer 1994, 30a((14)), 2093–5. [Google Scholar] [CrossRef]
- Eggermont, A. M.; Chiarion-Sileni, V.; Grob, J. J.; Dummer, R.; Wolchok, J. D.; Schmidt, H.; Hamid, O.; Robert, C.; Ascierto, P. A.; Richards, J. M.; Lebbé, C.; Ferraresi, V.; Smylie, M.; Weber, J. S.; Maio, M.; Bastholt, L.; Mortier, L.; Thomas, L.; Tahir, S.; Hauschild, A.; Hassel, J. C.; Hodi, F. S.; Taitt, C.; de Pril, V.; de Schaetzen, G.; Suciu, S.; Testori, A. Prolonged Survival in Stage III Melanoma with Ipilimumab Adjuvant Therapy. N Engl J Med 2016, 375((19)), 1845–1855. [Google Scholar] [CrossRef]
- Patel, S. P.; Othus, M.; Chen, Y.; Wright, G. P.; Yost, K. J.; Hyngstrom, J. R.; Hu-Lieskovan, S.; Lao, C. D.; Fecher, L. A.; Truong, T.-G.; Eisenstein, J. L.; Chandra, S.; Sosman, J. A.; Kendra, K. L.; Wu, R. C.; Devoe, C. E.; Deutsch, G. B.; Hegde, A.; Khalil, M.; Mangla, A.; Reese, A. M.; Ross, M. I.; Poklepovic, A. S.; Phan, G. Q.; Onitilo, A. A.; Yasar, D. G.; Powers, B. C.; Doolittle, G. C.; In, G. K.; Kokot, N.; Gibney, G. T.; Atkins, M. B.; Shaheen, M.; Warneke, J. A.; Ikeguchi, A.; Najera, J. E.; Chmielowski, B.; Crompton, J. G.; Floyd, J. D.; Hsueh, E.; Margolin, K. A.; Chow, W. A.; Grossmann, K. F.; Dietrich, E.; Prieto, V. G.; Lowe, M. C.; Buchbinder, E. I.; Kirkwood, J. M.; Korde, L.; Moon, J.; Sharon, E.; Sondak, V. K.; Ribas, A. Neoadjuvant–Adjuvant or Adjuvant-Only Pembrolizumab in Advanced Melanoma. New England Journal of Medicine 2023, 388((9)), 813–823. [Google Scholar] [CrossRef]
- Vogelbaum, M. A.; Brown, P. D.; Messersmith, H.; Brastianos, P. K.; Burri, S.; Cahill, D.; Dunn, I. F.; Gaspar, L. E.; Gatson, N. T. N.; Gondi, V.; Jordan, J. T.; Lassman, A. B.; Maues, J.; Mohile, N.; Redjal, N.; Stevens, G.; Sulman, E.; van den Bent, M.; Wallace, H. J.; Weinberg, J. S.; Zadeh, G.; Schiff, D. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J Clin Oncol 2022, 40((5)), 492–516. [Google Scholar] [CrossRef]
- Long, G. V.; Trefzer, U.; Davies, M. A.; Kefford, R. F.; Ascierto, P. A.; Chapman, P. B.; Puzanov, I.; Hauschild, A.; Robert, C.; Algazi, A.; Mortier, L.; Tawbi, H.; Wilhelm, T.; Zimmer, L.; Switzky, J.; Swann, S.; Martin, A.-M.; Guckert, M.; Goodman, V.; Streit, M.; Kirkwood, J. M.; Schadendorf, D. Dabrafenib in patients with Val600Glu or Val600Lys BRAF-mutant melanoma metastatic to the brain (BREAK-MB): a multicentre, open-label, phase 2 trial. The Lancet Oncology 2012, 13((11)), 1087–1095. [Google Scholar] [CrossRef]
- Bloem, M.; Suijkerbuijk, K. P. M.; Aarts, M. J. B.; van den Berkmortel, F. W. P. J.; Blank, C. U.; Blokx, W. A. M.; Boers-Sonderen, M. J.; Boreel, C. D. M.; de Groot, J. W. B.; Haanen, J. B. A. G.; Hospers, G. A. P.; Kapiteijn, E.; van Not, O. J.; Piersma, D.; Rikhof, B.; Stevense-den Boer, A. M.; van der Veldt, A. A. M.; Vreugdenhil, G.; Wouters, M. W. J. M.; van den Eertwegh, A. J. M. Efficacy of encorafenib plus binimetinib in patients with BRAF-mutated melanoma brain metastases: Results from the Dutch Melanoma Treatment Registry. European Journal of Cancer 2025, 223, 115514. [Google Scholar] [CrossRef] [PubMed]
- Márquez-Rodas, I.; Álvarez, A.; Arance, A.; Valduvieco, I.; Berciano-Guerrero, M.; Delgado, R.; Soria, A.; Lopez Campos, F.; Sánchez, P.; Romero, J. L.; Martin-Liberal, J.; Lucas, A.; Díaz-Beveridge, R.; Conde-Moreno, A. J.; Álamo de la Gala, M. D. C.; García-Castaño, A.; Prada, P. J.; González Cao, M.; Puertas, E.; Vidal, J.; Foro, P.; Aguado de la Rosa, C.; Corona, J. A.; Cerezuela-Fuentes, P.; López, P.; Luna, P.; Aymar, N.; Puértolas, T.; Sanagustín, P.; Berrocal, A. Encorafenib and binimetinib followed by radiotherapy for patients with BRAFV600-mutant melanoma and brain metastases (E-BRAIN/GEM1802 phase II study). Neuro Oncol 2024, 26((11)), 2074–2083. [Google Scholar] [CrossRef] [PubMed]
- Tolaney, S. M.; Sahebjam, S.; Le Rhun, E.; Bachelot, T.; Kabos, P.; Awada, A.; Yardley, D.; Chan, A.; Conte, P.; Diéras, V.; Lin, N. U.; Bear, M.; Chapman, S. C.; Yang, Z.; Chen, Y.; Anders, C. K. A Phase II Study of Abemaciclib in Patients with Brain Metastases Secondary to Hormone Receptor-Positive Breast Cancer. Clin Cancer Res 2020, 26((20)), 5310–5319. [Google Scholar] [PubMed]
- Pardridge, W. M. The blood-brain barrier: bottleneck in brain drug development. NeuroRx 2005, 2((1)), 3–14. [Google Scholar]
- Gampa, G.; Vaidhyanathan, S.; Sarkaria, J. N.; Elmquist, W. F. Drug delivery to melanoma brain metastases: Can current challenges lead to new opportunities? Pharmacol Res 2017, 123, 10–25. [Google Scholar] [CrossRef]
- Zhou, D.; Gong, Z.; Wu, D.; Ma, C.; Hou, L.; Niu, X.; Xu, T. Harnessing immunotherapy for brain metastases: insights into tumor–brain microenvironment interactions and emerging treatment modalities. Journal of Hematology & Oncology 2023, 16((1)), 121. [Google Scholar] [CrossRef]
- Orellana, V. P.; Tittarelli, A.; Retamal, M. A. Connexins in melanoma: Potential role of Cx46 in its aggressiveness. Pigment Cell Melanoma Res 2021, 34((5)), 853–868. [Google Scholar] [CrossRef]
- Soltantoyeh, T.; Akbari, B.; Karimi, A.; Mahmoodi Chalbatani, G.; Ghahri-Saremi, N.; Hadjati, J.; Hamblin, M. R.; Mirzaei, H. R. Chimeric Antigen Receptor (CAR) T Cell Therapy for Metastatic Melanoma: Challenges and Road Ahead. Cells 2021, 10((6)). [Google Scholar] [CrossRef]
- Beard, R. E.; Zheng, Z.; Lagisetty, K. H.; Burns, W. R.; Tran, E.; Hewitt, S. M.; Abate-Daga, D.; Rosati, S. F.; Fine, H. A.; Ferrone, S.; Rosenberg, S. A.; Morgan, R. A. Multiple chimeric antigen receptors successfully target chondroitin sulfate proteoglycan 4 in several different cancer histologies and cancer stem cells. J Immunother Cancer 2014, 2, 25. [Google Scholar] [CrossRef]
- Simon, B.; Harrer, D. C.; Schuler-Thurner, B.; Schaft, N.; Schuler, G.; Dörrie, J.; Uslu, U. The siRNA-mediated downregulation of PD-1 alone or simultaneously with CTLA-4 shows enhanced in vitro CAR-T-cell functionality for further clinical development towards the potential use in immunotherapy of melanoma. Exp Dermatol 2018, 27((7)), 769–778. [Google Scholar] [CrossRef] [PubMed]
- Inoo, K.; Inagaki, R.; Fujiwara, K.; Sasawatari, S.; Kamigaki, T.; Nakagawa, S.; Okada, N. Immunological quality and performance of tumor vessel-targeting CAR-T cells prepared by mRNA-EP for clinical research. Mol Ther Oncolytics 2016, 3, 16024. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Tang, X.; Zhang, Z.; Gu, L.; Wei, H.; Zhao, S.; Zhong, K.; Mu, M.; Huang, C.; Jiang, C.; Xu, J.; Guo, G.; Zhou, L.; Tong, A. Tandem CAR-T cells targeting CD70 and B7-H3 exhibit potent preclinical activity against multiple solid tumors. Theranostics 2020, 10((17)), 7622–7634. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, H. L.; Kohlhapp, F. J.; Zloza, A. Oncolytic viruses: a new class of immunotherapy drugs. Nat Rev Drug Discov 2015, 14((9)), 642–62. [Google Scholar] [CrossRef]
- Andtbacka, R. H.; Kaufman, H. L.; Collichio, F.; Amatruda, T.; Senzer, N.; Chesney, J.; Delman, K. A.; Spitler, L. E.; Puzanov, I.; Agarwala, S. S.; Milhem, M.; Cranmer, L.; Curti, B.; Lewis, K.; Ross, M.; Guthrie, T.; Linette, G. P.; Daniels, G. A.; Harrington, K.; Middleton, M. R.; Miller, W. H., Jr.; Zager, J. S.; Ye, Y.; Yao, B.; Li, A.; Doleman, S.; VanderWalde, A.; Gansert, J.; Coffin, R. S. Talimogene Laherparepvec Improves Durable Response Rate in Patients With Advanced Melanoma. J Clin Oncol 2015, 33((25)), 2780–8. [Google Scholar] [CrossRef]
- Geletneky, K.; Huesing, J.; Rommelaere, J.; Schlehofer, J. R.; Leuchs, B.; Dahm, M.; Krebs, O.; von Knebel Doeberitz, M.; Huber, B.; Hajda, J. Phase I/IIa study of intratumoral/intracerebral or intravenous/intracerebral administration of Parvovirus H-1 (ParvOryx) in patients with progressive primary or recurrent glioblastoma multiforme: ParvOryx01 protocol. BMC Cancer 2012, 12, 99. [Google Scholar] [CrossRef]
- Xia, Y.; Xu, F.; Xiong, M.; Yang, H.; Lin, W.; Xie, Y.; Xi, H.; Xue, Q.; Ye, T.; Yu, L. Repurposing of antipsychotic trifluoperazine for treating brain metastasis, lung metastasis and bone metastasis of melanoma by disrupting autophagy flux. Pharmacol Res 2021, 163, 105295. [Google Scholar] [CrossRef]
- Xi, H.; Wu, M.; Ma, H.; Li, S.; Huang, Q.; Zhang, Y.; Xia, Y. Repurposing fluphenazine to suppress melanoma brain, lung and bone metastasis by inducing G0/G1 cell cycle arrest and apoptosis and disrupting autophagic flux. Clin Exp Metastasis 2023, 40((2)), 161–175. [Google Scholar] [CrossRef]
- Jiang, J.; Jiang, L.; Maldonato, B. J.; Wang, Y.; Holderfield, M.; Aronchik, I.; Winters, I. P.; Salman, Z.; Blaj, C.; Menard, M.; Brodbeck, J.; Chen, Z.; Wei, X.; Rosen, M. J.; Gindin, Y.; Lee, B. J.; Evans, J. W.; Chang, S.; Wang, Z.; Seamon, K. J.; Parsons, D.; Cregg, J.; Marquez, A.; Tomlinson, A. C. A.; Yano, J. K.; Knox, J. E.; Quintana, E.; Aguirre, A. J.; Arbour, K. C.; Reed, A.; Gustafson, W. C.; Gill, A. L.; Koltun, E. S.; Wildes, D.; Smith, J. A. M.; Wang, Z.; Singh, M. Translational and Therapeutic Evaluation of RAS-GTP Inhibition by RMC-6236 in RAS-Driven Cancers. Cancer Discov 2024, 14((6)), 994–1017. [Google Scholar] [CrossRef]
- Holderfield, M.; Lee, B. J.; Jiang, J.; Tomlinson, A.; Seamon, K. J.; Mira, A.; Patrucco, E.; Goodhart, G.; Dilly, J.; Gindin, Y.; Dinglasan, N.; Wang, Y.; Lai, L. P.; Cai, S.; Jiang, L.; Nasholm, N.; Shifrin, N.; Blaj, C.; Shah, H.; Evans, J. W.; Montazer, N.; Lai, O.; Shi, J.; Ahler, E.; Quintana, E.; Chang, S.; Salvador, A.; Marquez, A.; Cregg, J.; Liu, Y.; Milin, A.; Chen, A.; Ziv, T. B.; Parsons, D.; Knox, J. E.; Klomp, J. E.; Roth, J.; Rees, M.; Ronan, M.; Cuevas-Navarro, A.; Hu, F.; Lito, P.; Santamaria, D.; Aguirre, A. J.; Waters, A. M.; Der, C. J.; Ambrogio, C.; Wang, Z.; Gill, A. L.; Koltun, E. S.; Smith, J. A. M.; Wildes, D.; Singh, M. Concurrent inhibition of oncogenic and wild-type RAS-GTP for cancer therapy. Nature 2024, 629((8013)), 919–926. [Google Scholar] [CrossRef]
- Almazan, J.; Turapov, T.; Kircher, D. A.; Stanley, K. A.; Culver, K.; Medellin, A. P.; Field, M. N.; Parkman, G. L.; Colman, H.; Coma, S.; Pachter, J. A.; Holmen, S. L. Combined inhibition of focal adhesion kinase and RAF/MEK elicits synergistic inhibition of melanoma growth and reduces metastases. Cell Rep Med 2025, 6((2)), 101943. [Google Scholar] [CrossRef]
- Banerjee, S.; Krebs, M. G.; Greystoke, A.; Garces, A. I.; Perez, V. S.; Terbuch, A.; Shinde, R.; Caldwell, R.; Grochot, R.; Rouhifard, M.; Ruddle, R.; Gurel, B.; Swales, K.; Tunariu, N.; Prout, T.; Parmar, M.; Symeonides, S.; Rekowski, J.; Yap, C.; Sharp, A.; Paschalis, A.; Lopez, J.; Minchom, A.; de Bono, J. S.; Banerji, U. Defactinib with avutometinib in patients with solid tumors: the phase 1 FRAME trial. Nature Medicine 2025, 31((9)), 3074–3080. [Google Scholar] [CrossRef]
- Colman, H.; Holmen, S. L. Defactinib and Avutometinib, With or Without Encorafenib, for the Treatment of Patients With Brain Metastases From Cutaneous Melanoma (DETERMINE). https://clinicaltrials.gov/study/NCT06194929 (12/26/2025).
- Schreurs, L. D.; Vom Stein, A. F.; Jünger, S. T.; Timmer, M.; Noh, K. W.; Buettner, R.; Kashkar, H.; Neuschmelting, V.; Goldbrunner, R.; Nguyen, P. H. The immune landscape in brain metastasis. Neuro Oncol 2025, 27((1)), 50–62. [Google Scholar] [CrossRef] [PubMed]
- Sankowski, R.; Böttcher, C.; Masuda, T.; Geirsdottir, L.; Sagar; Sindram, E.; Seredenina, T.; Muhs, A.; Scheiwe, C.; Shah, M. J.; Heiland, D. H.; Schnell, O.; Grün, D.; Priller, J.; Prinz, M. Mapping microglia states in the human brain through the integration of high-dimensional techniques. Nat Neurosci 2019, 22((12)), 2098–2110. [Google Scholar] [CrossRef] [PubMed]
- Bowman, R. L.; Klemm, F.; Akkari, L.; Pyonteck, S. M.; Sevenich, L.; Quail, D. F.; Dhara, S.; Simpson, K.; Gardner, E. E.; Iacobuzio-Donahue, C. A.; Brennan, C. W.; Tabar, V.; Gutin, P. H.; Joyce, J. A. Macrophage Ontogeny Underlies Differences in Tumor-Specific Education in Brain Malignancies. Cell Rep 2016, 17((9)), 2445–2459. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.; Michels, B.; Niesel, K.; Stein, S.; Farin, H.; Rödel, F.; Sevenich, L. Cellular and Molecular Changes of Brain Metastases-Associated Myeloid Cells during Disease Progression and Therapeutic Response. iScience 2020, 23((6)), 101178. [Google Scholar] [CrossRef]
- Zhang, W.; Karschnia, P.; von Mücke-Heim, I. A.; Mulazzani, M.; Zhou, X.; Blobner, J.; Mueller, N.; Teske, N.; Dede, S.; Xu, T.; Thon, N.; Ishikawa-Ankerhold, H.; Straube, A.; Tonn, J. C.; von Baumgarten, L. In vivo two-photon characterization of tumor-associated macrophages and microglia (TAM/M) and CX3CR1 during different steps of brain metastasis formation from lung cancer. Neoplasia 2021, 23((11)), 1089–1100. [Google Scholar] [CrossRef]
- Lorger, M.; Felding-Habermann, B. Capturing changes in the brain microenvironment during initial steps of breast cancer brain metastasis. Am J Pathol 2010, 176((6)), 2958–71. [Google Scholar] [CrossRef]
- Klemm, F.; Möckl, A.; Salamero-Boix, A.; Alekseeva, T.; Schäffer, A.; Schulz, M.; Niesel, K.; Maas, R. R.; Groth, M.; Elie, B. T.; Bowman, R. L.; Hegi, M. E.; Daniel, R. T.; Zeiner, P. S.; Zinke, J.; Harter, P. N.; Plate, K. H.; Joyce, J. A.; Sevenich, L. Compensatory CSF2-driven macrophage activation promotes adaptive resistance to CSF1R inhibition in breast-to-brain metastasis. Nat Cancer 2021, 2((10)), 1086–1101. [Google Scholar] [CrossRef]
- Friebel, E.; Kapolou, K.; Unger, S.; Núñez, N. G.; Utz, S.; Rushing, E. J.; Regli, L.; Weller, M.; Greter, M.; Tugues, S.; Neidert, M. C.; Becher, B. Single-Cell Mapping of Human Brain Cancer Reveals Tumor-Specific Instruction of Tissue-Invading Leukocytes. Cell 2020, 181((7)), 1626–1642.e20. [Google Scholar] [CrossRef]
- Klemm, F.; Maas, R. R.; Bowman, R. L.; Kornete, M.; Soukup, K.; Nassiri, S.; Brouland, J. P.; Iacobuzio-Donahue, C. A.; Brennan, C.; Tabar, V.; Gutin, P. H.; Daniel, R. T.; Hegi, M. E.; Joyce, J. A. Interrogation of the Microenvironmental Landscape in Brain Tumors Reveals Disease-Specific Alterations of Immune Cells. Cell 2020, 181((7)), 1643–1660.e17. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, R.; Yong, V. W. Microglia-T cell conversations in brain cancer progression. Trends Mol Med 2022, 28((11)), 951–963. [Google Scholar] [CrossRef] [PubMed]
- Evans, K. T.; Blake, K.; Longworth, A.; Coburn, M. A.; Insua-Rodríguez, J.; McMullen, T. P.; Nguyen, Q. H.; Ma, D.; Lev, T.; Hernandez, G. A.; Oganyan, A. K.; Orujyan, D.; Edwards, R. A.; Pridans, C.; Green, K. N.; Villalta, S. A.; Blurton-Jones, M.; Lawson, D. A. Microglia promote anti-tumour immunity and suppress breast cancer brain metastasis. Nat Cell Biol 2023, 25((12)), 1848–1859. [Google Scholar] [CrossRef] [PubMed]
- Wischnewski, V.; Maas, R. R.; Aruffo, P. G.; Soukup, K.; Galletti, G.; Kornete, M.; Galland, S.; Fournier, N.; Lilja, J.; Wirapati, P.; Lourenco, J.; Scarpa, A.; Daniel, R. T.; Hottinger, A. F.; Brouland, J. P.; Losurdo, A.; Voulaz, E.; Alloisio, M.; Hegi, M. E.; Lugli, E.; Joyce, J. A. Phenotypic diversity of T cells in human primary and metastatic brain tumors revealed by multiomic interrogation. Nat Cancer 2023, 4((6)), 908–924. [Google Scholar] [CrossRef]
- Li, T.; Sun, S.; Li, Y.; Zhang, Y.; Wei, L. Immunotherapy revolutionizing brain metastatic cancer treatment: personalized strategies for transformative outcomes. Front Immunol 2024, 15, 1418580. [Google Scholar] [CrossRef]
- Gellert, J.; Agardy, D. A.; Kumar, S.; Kourtesakis, A.; Boschert, T.; Jahne, K.; Breckwoldt, M. O.; Bunse, L.; Wick, W.; Davies, M. A.; Platten, M.; Bunse, T. Tumoral Interferon Beta Induces an Immune-Stimulatory Phenotype in Tumor-Associated Macrophages in Melanoma Brain Metastases. Cancer Res Commun 2024, 4((8)), 2189–2202. [Google Scholar] [CrossRef]
- Qiao, S.; Qian, Y.; Xu, G.; Luo, Q.; Zhang, Z. Long-term characterization of activated microglia/macrophages facilitating the development of experimental brain metastasis through intravital microscopic imaging. J Neuroinflammation 2019, 16((1)), 4. [Google Scholar] [CrossRef]
- Benbenishty, A.; Gadrich, M.; Cottarelli, A.; Lubart, A.; Kain, D.; Amer, M.; Shaashua, L.; Glasner, A.; Erez, N.; Agalliu, D.; Mayo, L.; Ben-Eliyahu, S.; Blinder, P. Prophylactic TLR9 stimulation reduces brain metastasis through microglia activation. PLoS Biol 2019, 17((3)), e2006859. [Google Scholar] [CrossRef]
- Economopoulos, V.; Pannell, M.; Johanssen, V. A.; Scott, H.; Andreou, K. E.; Larkin, J. R.; Sibson, N. R. Inhibition of Anti-Inflammatory Macrophage Phenotype Reduces Tumour Growth in Mouse Models of Brain Metastasis. Front Oncol 2022, 12, 850656. [Google Scholar] [CrossRef]
- Galon, J.; Bruni, D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat Rev Drug Discov 2019, 18((3)), 197–218. [Google Scholar] [CrossRef]
- Surendran, A.; Jenner, A. L.; Karimi, E.; Fiset, B.; Quail, D. F.; Walsh, L. A.; Craig, M. Agent-Based Modelling Reveals the Role of the Tumor Microenvironment on the Short-Term Success of Combination Temozolomide/Immune Checkpoint Blockade to Treat Glioblastoma. J Pharmacol Exp Ther 2023, 387((1)), 66–77. [Google Scholar] [CrossRef]
- Smalley, I.; Chen, Z.; Phadke, M.; Li, J.; Yu, X.; Wyatt, C.; Evernden, B.; Messina, J. L.; Sarnaik, A.; Sondak, V. K.; Zhang, C.; Law, V.; Tran, N.; Etame, A.; Macaulay, R. J. B.; Eroglu, Z.; Forsyth, P. A.; Rodriguez, P. C.; Chen, Y. A.; Smalley, K. S. M. Single-Cell Characterization of the Immune Microenvironment of Melanoma Brain and Leptomeningeal Metastases. Clin Cancer Res 2021, 27((14)), 4109–4125. [Google Scholar] [CrossRef] [PubMed]
- Tawbi, H. A.; Schadendorf, D.; Lipson, E. J.; Ascierto, P. A.; Matamala, L.; Castillo Gutiérrez, E.; Rutkowski, P.; Gogas, H. J.; Lao, C. D.; De Menezes, J. J.; Dalle, S.; Arance, A.; Grob, J. J.; Srivastava, S.; Abaskharoun, M.; Hamilton, M.; Keidel, S.; Simonsen, K. L.; Sobiesk, A. M.; Li, B.; Hodi, F. S.; Long, G. V. Relatlimab and Nivolumab versus Nivolumab in Untreated Advanced Melanoma. N Engl J Med 2022, 386((1)), 24–34. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Ciuleanu, T. E.; Lee, J. S.; Schenker, M.; Zurawski, B.; Kim, S. W.; Mahave, M.; Alexandru, A.; Peters, S.; Pluzanski, A.; Caro, R. B.; Linardou, H.; Burgers, J. A.; Nishio, M.; Martinez-Marti, A.; Azuma, K.; Axelrod, R.; Paz-Ares, L. G.; Ramalingam, S. S.; Borghaei, H.; O'Byrne, K. J.; Li, L.; Bushong, J.; Gupta, R. G.; Grootendorst, D. J.; Eccles, L. J.; Brahmer, J. R. Systemic and Intracranial Outcomes With First-Line Nivolumab Plus Ipilimumab in Patients With Metastatic NSCLC and Baseline Brain Metastases From CheckMate 227 Part 1. J Thorac Oncol 2023, 18((8)), 1055–1069. [Google Scholar] [CrossRef] [PubMed]
- Patton, E. E.; Mueller, K. L.; Adams, D. J.; Anandasabapathy, N.; Aplin, A. E.; Bertolotto, C.; Bosenberg, M.; Ceol, C. J.; Burd, C. E.; Chi, P.; Herlyn, M.; Holmen, S. L.; Karreth, F. A.; Kaufman, C. K.; Khan, S.; Kobold, S.; Leucci, E.; Levy, C.; Lombard, D. B.; Lund, A. W.; Marie, K. L.; Marine, J. C.; Marais, R.; McMahon, M.; Robles-Espinoza, C. D.; Ronai, Z. A.; Samuels, Y.; Soengas, M. S.; Villanueva, J.; Weeraratna, A. T.; White, R. M.; Yeh, I.; Zhu, J.; Zon, L. I.; Hurlbert, M. S.; Merlino, G. Melanoma models for the next generation of therapies. Cancer Cell 2021, 39((5)), 610–631. [Google Scholar] [CrossRef]
- Day, C. P.; Merlino, G.; Van Dyke, T. Preclinical mouse cancer models: a maze of opportunities and challenges. Cell 2015, 163((1)), 39–53. [Google Scholar] [CrossRef]
- Frühwein, H.; Paul, N. W. Lost in translation?" Animal research in the era of precision medicine. J Transl Med 2025, 23((1)), 152. [Google Scholar] [CrossRef]
- Martić-Kehl, M. I.; Schibli, R.; Schubiger, P. A. Can animal data predict human outcome? Problems and pitfalls of translational animal research. Eur J Nucl Med Mol Imaging 2012, 39((9)), 1492–6. [Google Scholar] [CrossRef]
- Goodspeed, A.; Heiser, L. M.; Gray, J. W.; Costello, J. C. Tumor-Derived Cell Lines as Molecular Models of Cancer Pharmacogenomics. Mol Cancer Res 2016, 14((1)), 3–13. [Google Scholar] [CrossRef]
- Mirabelli, P.; Coppola, L.; Salvatore, M. Cancer Cell Lines Are Useful Model Systems for Medical Research. Cancers (Basel) 2019, 11((8)). [Google Scholar] [CrossRef]
- Liu, Y.; Wu, W.; Cai, C.; Zhang, H.; Shen, H.; Han, Y. Patient-derived xenograft models in cancer therapy: technologies and applications. Signal Transduction and Targeted Therapy 2023, 8((1)), 160. [Google Scholar] [CrossRef]
- Müller, I.; Kulms, D. A 3D Organotypic Melanoma Spheroid Skin Model. J Vis Exp 2018, 135. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, D. B.; Reis, R. L.; Pirraco, R. P. Modelling the complex nature of the tumor microenvironment: 3D tumor spheroids as an evolving tool. J Biomed Sci 2024, 31((1)), 13. [Google Scholar] [CrossRef]
- Mangani, S.; Kremmydas, S.; Karamanos, N. K. Mimicking the Complexity of Solid Tumors: How Spheroids Could Advance Cancer Preclinical Transformative Approaches. Cancers (Basel) 2025, 17((7)). [Google Scholar] [CrossRef]
- Kyriakopoulou, K.; Koutsakis, C.; Piperigkou, Z.; Karamanos, N. K. Recreating the extracellular matrix: novel 3D cell culture platforms in cancer research. 2023, 290((22)), 5238–5247. [Google Scholar] [CrossRef] [PubMed]
- Zeng, D.; Li, S.; Du, F.; Xia, Y.; Zhang, J.; Yu, S.; Qin, J. Advances in engineered organoid models of skin for biomedical research. Burns Trauma 2025, 13, tkaf016. [Google Scholar] [CrossRef]
- Abedellatif, S. E.; Hosni, R.; Waha, A.; Gielen, G. H.; Banat, M.; Hamed, M.; Güresir, E.; Fröhlich, A.; Sirokay, J.; Wulf, A. L.; Kristiansen, G.; Pietsch, T.; Vatter, H.; Hölzel, M.; Schneider, M.; Toma, M. I. Melanoma Brain Metastases Patient-Derived Organoids: An In Vitro Platform for Drug Screening. Pharmaceutics 2024, 16((8)). [Google Scholar] [CrossRef] [PubMed]
- Thorel, L.; Perréard, M.; Florent, R.; Divoux, J.; Coffy, S.; Vincent, A.; Gaggioli, C.; Guasch, G.; Gidrol, X.; Weiswald, L.-B.; Poulain, L. Patient-derived tumor organoids: a new avenue for preclinical research and precision medicine in oncology. Experimental & Molecular Medicine 2024, 56((7)), 1531–1551. [Google Scholar] [CrossRef]
- Abedellatif, S.-E.; Hosni, R.; Waha, A.; Gielen, G. H.; Banat, M.; Hamed, M.; Güresir, E.; Fröhlich, A.; Sirokay, J.; Wulf, A.-L.; Kristiansen, G.; Pietsch, T.; Vatter, H.; Hölzel, M.; Schneider, M.; Toma, M. I. Melanoma Brain Metastases Patient-Derived Organoids: An In Vitro Platform for Drug Screening. Pharmaceutics 2024, 16((8)), 1042. [Google Scholar] [CrossRef]
- Meier, F.; Nesbit, M.; Hsu, M. Y.; Martin, B.; Van Belle, P.; Elder, D. E.; Schaumburg-Lever, G.; Garbe, C.; Walz, T. M.; Donatien, P.; Crombleholme, T. M.; Herlyn, M. Human melanoma progression in skin reconstructs: biological significance of bFGF. Am J Pathol 2000, 156((1)), 193–200. [Google Scholar] [CrossRef]
- Li, L.; Fukunaga-Kalabis, M.; Herlyn, M. The three-dimensional human skin reconstruct model: a tool to study normal skin and melanoma progression. J Vis Exp 2011, 54. [Google Scholar]
- Zeng, J.; Lin, L.; Ma, Y.; Huang, W.; Luo, Q.; Wen, J. Single-cell transcriptomics profiling reveals cellular origins and molecular drivers underlying melanoma brain metastasis. PLOS ONE 2025, 20((11)), e0336502. [Google Scholar] [CrossRef] [PubMed]
- In, G. K.; Ribeiro, J. R.; Yin, J.; Xiu, J.; Bustos, M. A.; Ito, F.; Chow, F.; Zada, G.; Hwang, L.; Salama, A. K. S.; Park, S. J.; Moser, J. C.; Darabi, S.; Domingo-Musibay, E.; Ascierto, M. L.; Margolin, K.; Lutzky, J.; Gibney, G. T.; Atkins, M. B.; Izar, B.; Hoon, D. S. B.; VanderWalde, A. M. Multi-omic profiling reveals discrepant immunogenic properties and a unique tumor microenvironment among melanoma brain metastases. npj Precision Oncology 2023, 7((1)), 120. [Google Scholar] [CrossRef] [PubMed]
- Davies, M. A.; Liu, P.; McIntyre, S.; Kim, K. B.; Papadopoulos, N.; Hwu, W. J.; Hwu, P.; Bedikian, A. Prognostic factors for survival in melanoma patients with brain metastases. Cancer 2011, 117((8)), 1687–96. [Google Scholar] [CrossRef]
- Lekkala, M. R.; Mullangi, S. Malignant Melanoma Metastatic to the Central Nervous System. In StatPearls; StatPearls Publishing, Copyright © 2025, StatPearls Publishing LLC.: Treasure Island (FL), 2025. [Google Scholar]
- Valentini, V.; Boldrini, L.; Mariani, S.; Massaccesi, M. Role of radiation oncology in modern multidisciplinary cancer treatment. Mol Oncol 2020, 14((7)), 1431–1441. [Google Scholar] [CrossRef]
- Palmer, J. D.; Perlow, H. K.; Lehrer, E. J.; Wardak, Z.; Soliman, H. Novel radiotherapeutic strategies in the management of brain metastases: Challenging the dogma. Neuro Oncol 2024, 26((12) Suppl 2, S46–s55. [Google Scholar] [CrossRef]
- Harrison, R. A.; Tang, M.; Shih, K. K.; Khan, M.; Pham, L.; De Moraes, A. R.; O'Brien, B. J.; Bassett, R.; Bruera, E. Characterization of patients with brain metastases referred to palliative care. BMC Palliat Care 2024, 23((1)), 13. [Google Scholar] [CrossRef]
- Wu, A.; Colón, G. R.; Lim, M. Quality of Life and Role of Palliative and Supportive Care for Patients With Brain Metastases and Caregivers: A Review. Front Neurol 2022, 13, 806344. [Google Scholar] [CrossRef]
- Cherukuri, S. P.; Kaur, A.; Goyal, B.; Kukunoor, H. R.; Sahito, A. F.; Sachdeva, P.; Yerrapragada, G.; Elangovan, P.; Shariff, M. N.; Natarajan, T.; Janarthanan, J.; Richard, S.; Pallikaranai Venkatesaprasath, S.; Karuppiah, S. S.; Iyer, V. N.; Helgeson, S. A.; Arunachalam, S. P. Artificial Intelligence-Enhanced Liquid Biopsy and Radiomics in Early-Stage Lung Cancer Detection: A Precision Oncology Paradigm. Cancers (Basel) 2025, 17, 19. [Google Scholar] [CrossRef]
- Rajendran, A.; Angelin Rajan, R.; Balasubramaniyam, S.; Elumalai, K. AI-Enhanced Predictive Imaging in Precision Medicine: Advancing Diagnostic Accuracy and Personalized Treatment. iRADIOLOGY 2025, 3((4)), 261–278. [Google Scholar] [CrossRef]
- Fischer, G. M.; Jalali, A.; Kircher, D. A.; Lee, W. C.; McQuade, J. L.; Haydu, L. E.; Joon, A. Y.; Reuben, A.; de Macedo, M. P.; Carapeto, F. C. L.; Yang, C.; Srivastava, A.; Ambati, C. R.; Sreekumar, A.; Hudgens, C. W.; Knighton, B.; Deng, W.; Ferguson, S. D.; Tawbi, H. A.; Glitza, I. C.; Gershenwald, J. E.; Vashisht Gopal, Y. N.; Hwu, P.; Huse, J. T.; Wargo, J. A.; Futreal, P. A.; Putluri, N.; Lazar, A. J.; DeBerardinis, R. J.; Marszalek, J. R.; Zhang, J.; Holmen, S. L.; Tetzlaff, M. T.; Davies, M. A. Molecular Profiling Reveals Unique Immune and Metabolic Features of Melanoma Brain Metastases. Cancer Discov 2019, 9((5)), 628–645. [Google Scholar] [CrossRef]
- Li, M.; Zhang, Y.; Yu, D.; Yu, Y.; Ma, W. Immunotherapy biomarkers in brain metastases: insights into tumor microenvironment dynamics. Front Immunol 2025, 16, 1600261. [Google Scholar] [CrossRef]
- Evangelou, K.; Zemperligkos, P.; Politis, A.; Lani, E.; Gutierrez-Valencia, E.; Kotsantis, I.; Velonakis, G.; Boviatsis, E.; Stavrinou, L. C.; Kalyvas, A. Diagnostic, Therapeutic, and Prognostic Applications of Artificial Intelligence (AI) in the Clinical Management of Brain Metastases (BMs). Brain Sci 2025, 15((7)). [Google Scholar] [CrossRef]
- Feng, Y.; Hu, X.; Zhang, Y.; Wang, Y. The Role of Microglia in Brain Metastases: Mechanisms and Strategies. Aging Dis 2024, 15((1)), 169–185. [Google Scholar] [CrossRef]
- Davies, M. A.; Saiag, P.; Robert, C.; Grob, J. J.; Flaherty, K. T.; Arance, A.; Chiarion-Sileni, V.; Thomas, L.; Lesimple, T.; Mortier, L.; Moschos, S. J.; Hogg, D.; Marquez-Rodas, I.; Del Vecchio, M.; Lebbe, C.; Meyer, N.; Zhang, Y.; Huang, Y.; Mookerjee, B.; Long, G. V. Dabrafenib plus trametinib in patients with BRAF(V600)-mutant melanoma brain metastases (COMBI-MB): a multicentre, multicohort, open-label, phase 2 trial. Lancet Oncol 2017, 18((7)), 863–873. [Google Scholar] [CrossRef]
- Long, G. V.; Margolin, K. A. Multidisciplinary approach to brain metastasis from melanoma: the emerging role of systemic therapies. Am Soc Clin Oncol Educ Book 2013, 393–8. [Google Scholar] [CrossRef]
- Subbiah, V.; Gutierrez, M.; Anders, C. K.; Ansstas, G.; Owonikoko, T. K.; Monga, V.; Forsyth, P. A. J.; Dagogo-Jack, I.; Chandra, S.; Tsai, K. K.; Diamond, E. L.; McKean, M.; Buchbinder, E. I.; Nepert, D.; Ingram, K.; Oliver, C.; Reddy, M.; Maharry, K.; Xing, Y. Trial in progress: Phase 1a/b study of PF-07284890 (brain-penetrant BRAF inhibitor) with/without binimetinib in patients with BRAF V600-mutant solid tumors. Journal of Clinical Oncology 2021, 39. [Google Scholar] [CrossRef]
Figure 1.
Steps involved in melanoma metastasis from the primary tumor to the brain. Figure created with BioRender.com.
Figure 1.
Steps involved in melanoma metastasis from the primary tumor to the brain. Figure created with BioRender.com.
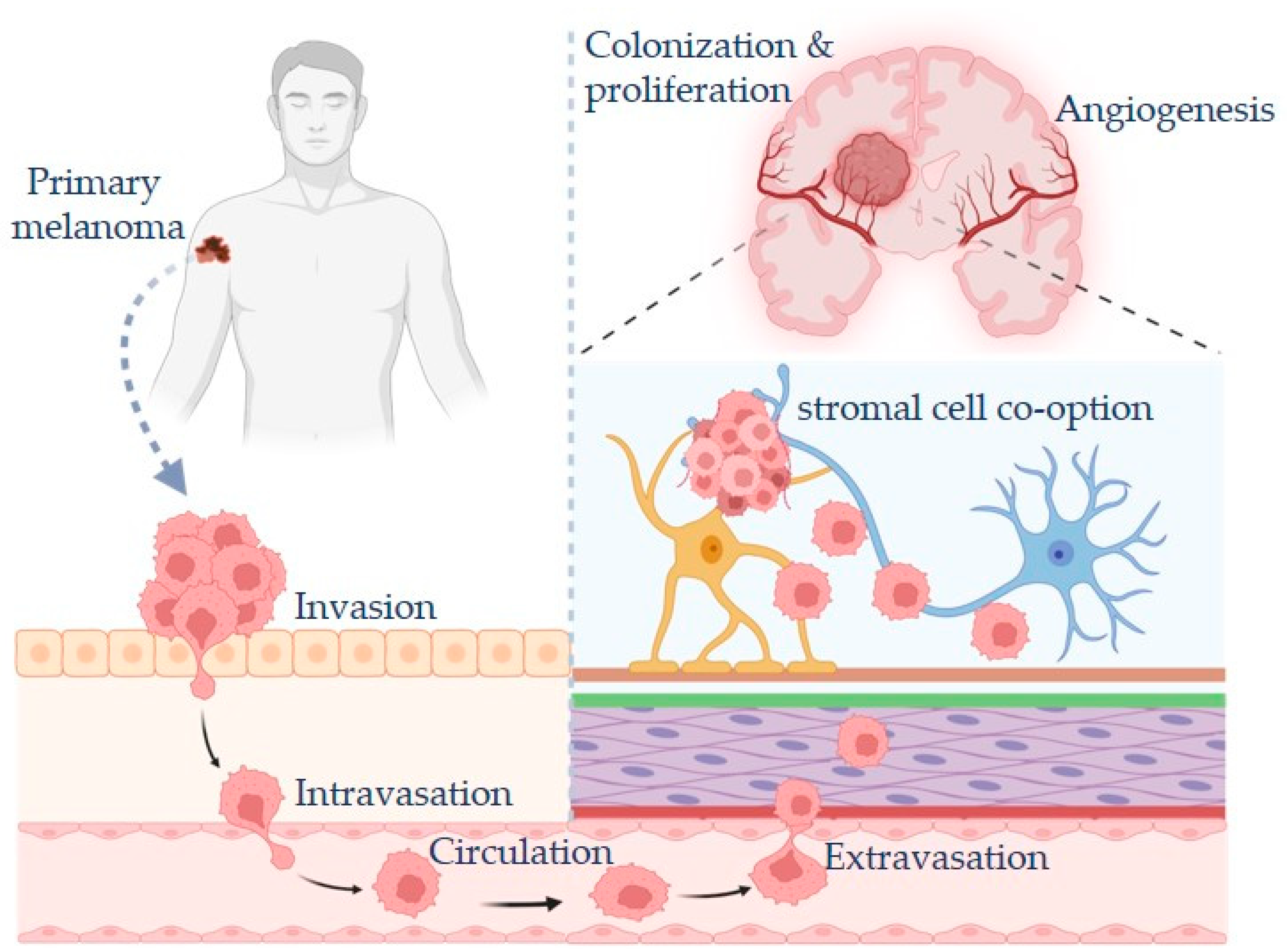
Figure 2.
Signaling pathways altered in melanoma with an emphasis on those that drive metastasis to the brain. TFs: transcription factors; ECM: extracellular matrix. Figure created with BioRender.com.
Figure 2.
Signaling pathways altered in melanoma with an emphasis on those that drive metastasis to the brain. TFs: transcription factors; ECM: extracellular matrix. Figure created with BioRender.com.
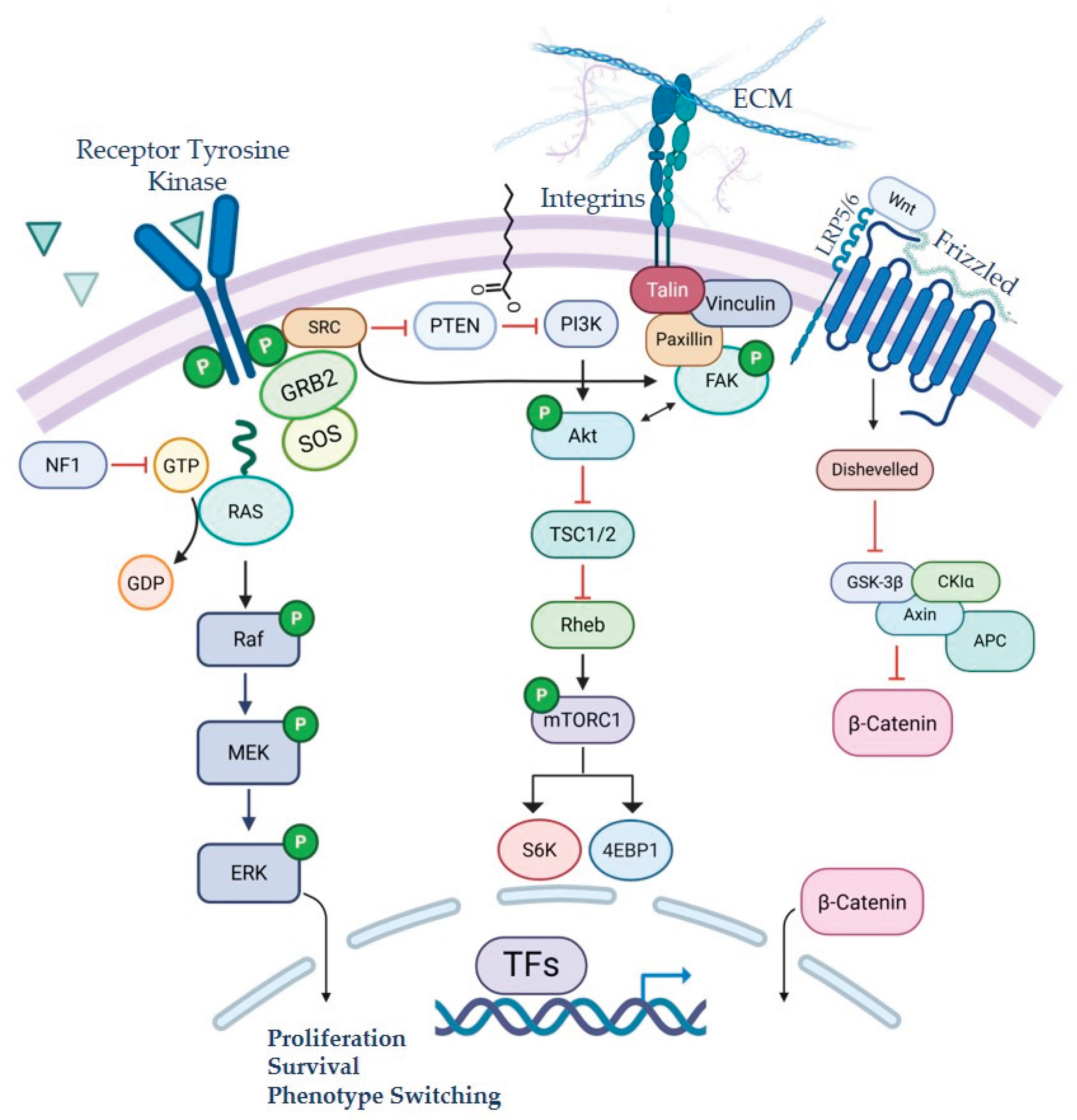

Table 1.
Summary of active clinical trials for patients with melanoma brain metastases1.
| NCT Number | Phase | Primary Outcome | Title |
| NCT06194929 | Phase I/II | ORR | Defactinib and Avutometinib, With or Without Encorafenib, for the Treatment of Patients With Brain Metastases From Cutaneous Melanoma (DETERMINE) |
| NCT03563729 | Phase II | 6 month PFS | Melanoma Metastasized to the Brain and Steroids (MEMBRAINS) |
| NCT06163820 | Phase I/II | S&T, iORR | Bevacizumab and ICIs + hSRT in Symptomatic Melanoma Brain Metastases (BETTER) |
| NCT06712927 | Phase II | iORR | Trial of Relatlimab, Nivolumab, and Ipilimumab in Patients With Asymptomatic and Symptomatic Melanoma Brain Metastases |
| NCT05704647 | Phase II | iORR, AEs | Phase II Study of Nivolumab in Combination With Relatlimab in Patients With Active Melanoma Brain Metastases |
| NCT06887088 | Phase II | icPFS | Encorafenib and biNimetinib Followed by CEmiplimab and FiAnLimab in Patients With BRAF Mutant melanOma and Symptomatic Brain Metastases (ENCEFALO) |
| NCT04511013 | Phase II | PFS | A Study to Compare the Administration of Encorafenib + Binimetinib + Nivolumab Versus Ipilimumab + Nivolumab in BRAF-V600 Mutant Melanoma With Brain Metastases |
| NCT03340129 | Phase II | Neurological death | Anti-PD 1 Brain Collaboration + Radiotherapy Extension (ABC-X Study) |
| NCT05026983 | Phase II | PFS, DLTs, and AEs | Binimetinib and Encorafenib for the Treatment of Metastatic Melanoma and Central Nervous System Metastases |
| NCT04899908 | Phase II | Local Recurrence | Stereotactic Brain-directed Radiation With or Without Aguix Gadolinium-Based Nanoparticles in Brain Metastases |
| NCT05703269 | Phase III | Occurrence of ARE | Comparing Single vs Multiple Dose Radiation for Cancer Patients With Brain Metastasis and Receiving Immunotherapy (HYPOGRYPHE) |
| NCT05909618 | Phase I/II | S&T, ORR | Crizanlizumab Alone or in Combination With Nivolumab for Glioblastoma and Melanoma With Brain Metastases |
| NCT05522660 | Phase III | CNS-specific PFS | Immunotherapy or Targeted Therapy With or Without Stereotactic Radiosurgery for Patients With Brain Metastases From Melanoma or Non-small Cell Lung Cancer (USZ-STRIKE) |
| NCT05588453 | Phase I/II | DLTs, iORR | Natural Killer Cell Therapy (UD TGFbetai NK Cells) and Temozolomide for the Treatment of Stage IV Melanoma Metastatic to the Brain |
| NCT06500455 | Phase III | Time to local failure | Testing Longer Duration Radiation Therapy Versus the Usual Radiation Therapy in Patients With Cancer That Has Spread to the Brain |
| NCT04021420 | Phase I/II | MSD | Safety and Efficacy of Sonocloud Device Combined With Nivolumab in Brain Metastases From Patients With Melanoma (SONIMEL01) |
| NCT06346067 | Phase III | PFS and OS | A Study to Assess Naporafenib (ERAS-254) Administered With Trametinib in Patients With NRAS-mutant Melanoma (SEACRAFT-2) |
| NCT01503827 | Phase III | Intracranial failure | Whole Brain Radiotherapy Following Local Treatment of Intracranial Metastases of Melanoma (WBRTMel) |
| NCT02460068 | Phase III | OS | A Study of Fotemustine (FTM) Vs FTM and Ipilimumab (IPI) or IPI and Nivolumab in Melanoma Brain Metastasis (NIBIT-M2) |
1Trials either focus on melanoma brain metastasis or do not exclude patients with melanoma brain metastasis. AE: adverse events; ARE: Adverse Radiation Effect; CNS: central nervous system; DLTs: dose limiting toxicities; icPFS: intracranial progression-free survival; iORR: intracranial objective response rate; MSD: Most Successful Dose; ORR: objective response rate; OS: overall survival; PFS: progression-free survival; S&T: Safety and tolerability. Data obtained from clinicaltrials.gov.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



