
Submitted:
05 January 2026
Posted:
06 January 2026
You are already at the latest version
Abstract
Background/Objectives: Angiosarcoma of the thorax is a very rare and malignant disease. We studied the incidence and survival of thoracic angiosarcomas with special focus on primary and secondary angiosarcoma. Methods: We analyzed data from the population-based cancer registry North Rhine-Westphalia (NRW), Germany, of the years 2008–2023. We included primary and secondary angiosarcoma of the thorax (ICD-O-3: morphology 9120/3, topography C34, C38, C44.51, C49.3, C50) and report age-standardized (Old European Standard population) incidence rates and survival (Kaplan-Meier Curves). Results: We analyzed 421 cases of thoracic angiosarcoma. 90.0% were female (n = 379). The age-standardized incidence rates of angiosarcoma of the thorax were 0.25 per million and year for male patients (SE 0.0) and 1.5 per million and year for female patients (SE 0.1). All male patients had primary angiosarcoma (n = 42). The majority of thoracic angiosarcoma among females were second primary tumors (n=262, 69.1%). The 5-year overall survival (OS) was 38.5% (SE 2.6). OS for women was 41.4% (SE 2.8) and for men was 12.0% (SE 5.4). OS for female patients was 40.9% (SE 4.1) and 41.8% (SE 3.8) for primary and second primary angiosarcoma respectively. The worst OS had patients with angiosarcoma of the lung (men 20.0% (SE 12.7) and mediastinum, heart and pleura (men 4.7% (SE 4.5). The OS for women was 0%, all females died within 2.2 years after diagnosis of angiosarcoma with these topographies. Conclusions: Angiosarcoma of the thorax is a rare condition with poor prognosis. Irrespective of the classification into primary and second primary, women with angiosarcoma have a better prognosis than men. Topography seems to be the most determining prognostic factor in this disease.
Keywords:
rare malignancy
; angiosarcoma
; thorax
; incidence
; survival
1. Introduction
Angiosarcoma is a rare disease that accounts for 1-2% of soft tissue sarcomas. It arises from the endothelial cells of small blood and lymphatic vessels and can occur in any part of the body [1,2]. Cutaneous angiosarcomas are the most common, affecting the skin, breast and soft tissues of the head and neck, particularly the scalp [2]. Angiosarcomas often occur as so-called second primary cancers after radiotherapy for breast cancer or skin cancer [3]. There is also an association with chronic lymphedema following lymph node dissection for treatment of breast cancer or malignant melanoma, known as Stewart-Treves syndrome [4]. It is therefore important to distinguish between spontaneous primary angiosarcomas and second primary angiosarcomas. The most studied and common causes of second primary angiosarcoma are previous cancer with subsequent radiation and/or chronic lymphedema. UV radiation, immunocompromised states, arteriovenous fistulas, xeroderma pigmentosum, trauma, foreign bodies, thorium dioxide and viral infections have also been discussed [5,6]. According to clinical experience and studies, the latency period between primary cancer and angiosarcoma is approximately 5-10 years [7]. It seems that causal factors are unknown or very difficult to assess. For example, in 1999 Maziak et al. reported a case of angiosarcoma in a thoracotomy incision 17 years after surgery for UICC stage I lung cancer [8].
In general, thoracic angiosarcomas often present with benign symptoms despite the presence of advanced disease with infiltrative growth and metastatic spread [6]. For example, in patients with pleural origin, the most common symptoms are dyspnoea, chest tightness, pain, pleural thickening, pleural effusion and recurrent haemothorax. However, symptoms depend on the location of the tumor. Diagnosis can be difficult, even with a valid biopsy, and misdiagnosis is possible [9]. Mimicry of other rare angiogenic malignancies (such as hemangioendothelioma or intimasarcoma) and even benign tumors is possible. Surgery is appropriate for localized tumors, but the prognosis is poor. Although most patients die shortly after diagnosis, some authors argue that a multidisciplinary approach consisting of surgery, radiotherapy and chemotherapy may result in prolonged survival [6].
Thoracic angiosarcoma is an extremely rare malignancy. Breast and chest wall are the most frequent locations. Banks et al. published a results of a cohort of 183 patients with 34 primary and 149 second primary angiosarcomas of the breast and chest wall [10]. Other sites are even rarer. For example, according to Wang et al. about 43 cases of pleural origin have been reported up to 2022 on PubMed [11].
The most recent comprehensive data and epidemiological evidence was published by Wagner et al. 2024 [3]. Their study included 19,289 patients in the USA with a new diagnosis of angiosarcoma between 2001 and 2020 recorded in the US Cancer Statistics database. However, angiosarcomas of the chest wall/thorax were included in the cutaneous, subcutaneous and breast angiosarcoma subgroup, whereas angiosarcomas of the heart, trachea, lung, pleura and mediastinum were included in the visceral angiosarcoma subgroup [3]. According to Sturm et al. 5-year overall survival (OS) ranges from 30% to 56% [6].
Although these publications provide relevant epidemiological findings on angiosarcoma, we can only apply their results to angiosarcoma of the thorax with limitations. To date, no differentiation has been made in the literature between primary and second primary angiosarcomas or according to their respective topography. Furthermore, specific survival analyses are missing. Thus, epidemiological evidence on angiosarcoma of the thorax and its associated parts is still lacking. The aim of this study was to provide population-based age-standardized incidence rates and 5-year OS thoracic angiosarcomas in North Rhine-Westphalia, Germany, between 2008 and 2023.
2. Material and Methods
The Cancer Registry of the Federal State of North Rhine-Westphalia (LKR NRW) covers a population of 18 million people. Cancer reporting is mandatory and since 2008 data with sufficient quality is available. For this study, we identified newly diagnosed thoracic angiosarcoma on the basis of the International Classification of Diseases for Oncology (ICD-O-3) morphology (9120/3 hemangiosarcoma) and topography (C34 bronchus and lung, C38 heart, mediastinum and pleura, C44.51 skin of thorax, C49.3 soft tissues of thorax, C50 breast). Patients diagnosed with thoracic angiosarcoma during the calendar years 2008 – 2023 were included. Mortality follow-up for cancer patients was routinely assessed by the LKR NRW through a passive mortality-follow-up with electronic reports on all deceased individuals in NRW obtained from population registration offices.
We calculated age-standardized incidence rates for the study period by sex using the old European standard population [12]. Furthermore, we estimated annual percentage changes (EAPC) of the age-standardized incidence rates by using the Joinpoint regression program [13].
The Kaplan-Meier method was applied to estimate 5-year overall survival [14]. Censoring occurred at the last date of mortality follow-up which was 31 December 2023. Survival analysis was stratified according to primary thoracic angiosarcoma and second primary thoracic angiosarcoma (i.e., an angiosarcoma occurring after a previous diagnosis of breast or skin cancer) and according to topography.
Since we know that most angiosarcomas are associated with malignant melanoma and/or breast cancer and therefore represent second primary angiosarcomas, we formed a subgroup with (called second primary angiosarcoma) and another subgroup without evidence of breast cancer and/or malignant melanoma located in the thoracic region in the past (called primary angiosarcoma). According to clinical evidence and the literature [7,8], we used a differentiated approach to latency of tumor genesis - between previous cancer diagnosis and angiosarcoma – with two groups 0-5 years and >5 years. Further subgroup analysis showed that the majority of cutaneous malignancies were basal cell carcinomas (n = 32). This type of cancer was excluded due to lack of association with angiosarcoma.
3. Results
The cancer registry recorded a total of 421 cases of hemangiosarcoma (hereinafter called angiosarcoma) during 2008 – 2023. 10% were male (n = 42) and 90% female (n = 379). The most frequent anatomical origins were the breast (n = 250) and the soft tissue of the thorax (n = 86). However, 20.2% of all angiosarcomas were located elsewhere than in the breast or soft tissue of the thorax (Table 1).
The median age at diagnosis of all patients was 69.1 years (standard error, SE 14.3). While median age at diagnosis for women was 70.8 years (SE 12.5), men were diagnosed at an earlier median age of 54.4 years (SE 19.8) (Table 1).
Between 2008 and 2023, the age-standardized incidence of angiosarcoma of the thorax ranged from 0.00 to 0.70 per million and year for male patients and ranged from 1.0 to 2.3 per million and year for female patients (Figure 1).
67.7% of patients (n = 285) experienced at least one other thoracic cancer diagnosis before thoracic angiosarcoma. Breast cancer (n = 262) and skin cancers (n = 38) were the most common entities. 51.1% of all patients with a thoracic angiosarcoma experienced breast cancer or malignant melanoma >5 years before angiosarcoma. Considering these conditions (breast and/or skin cancer and >5 years latency), all 42 male patients had primary angiosarcoma. 56.7% of female patients experienced previous malignant melanoma and/or breast cancer >5 years before angiosarcoma (n = 215), 12.4% within the last 5 years before angiosarcoma (n=47) and 30.9% had primary angiosarcoma of the thorax (n = 117) (Figure 2).
The 5-years OS for patients diagnosed with angiosarcoma was 38.5% (SE 2.6). OS for woman was 41.4% (SE 2.79) and for men was 12.0% (SE 5.4). OS for female patients with primary angiosarcoma and second primary angiosarcoma was 40.9% (SE 4.1) and 41.8% (SE 3.8) respectively (Table 2, Figure 3).

Table 2.
1, 2 and 5-year-survival of patients with thorax angiosarcoma stratified by status in North Rhine-Westphalia, 2008-2023.
Table 2.
1, 2 and 5-year-survival of patients with thorax angiosarcoma stratified by status in North Rhine-Westphalia, 2008-2023.
| sex | Status concerning previous diagnosis of skin/breast cancer | n | Overall Survival (SE) | ||
|---|---|---|---|---|---|
| 1 year | 2 years | 5 years | |||
| Overall | Overall | 421 | 76.6 (2.1) | 62.2 (2.5) | 38.5 (2.6) |
| M | Overall | 42 | 41.2 (7.8) | 25.7 (7.0) | 12.0 (5.4) |
| W | Overall | 379 | 80.1 (2.1) | 66.3 (2.5) | 41.4 (2.8) |
| M | Primary | 42 | 41.2 (7.8) | 25.7 (7.0) | 12.0 (5.4) |
| W | Primary | 116 | 79.2 (3.2) | 63.3 (3.9) | 40.9 (4.1) |
| W | Secondary (0-5 years before) | 47 | 80.0 (6.0) | 68.4 (7.0) | 44.7 (7.6) |
| W | Secondary (> 5 years before) | 216 | 80.8 (2.7) | 68.7 (3.3) | 41.8 (3.8) |
Table 3.
1, 2 and 5-year-survival of patients with thorax angiosarcoma stratified by status in North Rhine-Westphalia, 2008-2023.
Table 3.
1, 2 and 5-year-survival of patients with thorax angiosarcoma stratified by status in North Rhine-Westphalia, 2008-2023.
| sex | Topography | n | Overall Survival (SE) | ||
|---|---|---|---|---|---|
| 1 year | 2 years | 5 years | |||
| overall | C34 | 15 | 51.3 (13.3) | 22.0 (11.2) | 14.7 (9.6) |
| C38 | 37 | 35.1 (8.1) | 14.6 (6.0) | 2.9 (2.9) | |
| C44.51 | 33 | 81.8 (6.7) | 69.4 (8.1) | 34.7 (8.4) | |
| C49.3 | 86 | 78.2 (4.6) | 62.9 (5.4) | 38.2 (5.9) | |
| C50 | 250 | 82.3 (2.5) | 70.5 (3.0) | 46.1 (3.5) | |
| M | C34 | 10 | 40.0 (15.5) | 30.0 (14.5) | 20.0 (12.7) |
| C38 | 23 | 37.3 (10.3) | 18.6 (8.4) | 4.7 (4.5) | |
| C44.51 | 0 | - | - | - | |
| C49.3 | 8 | 46.9 (18.7) | 31.3 (17.8) | 15.6 (14.2) | |
| C50 | 1 | - | - | - | |
| W | C34 | 5 | 80.0 (17.9) | - | - |
| C38 | 14 | 31.4 (12.9) | 7.9 (7.5) | - | |
| C4451 | 33 | 81.8 (6.7) | 69.4 (8.1) | 34.7 (8.4) | |
| C493 | 78 | 81.3 (4.5) | 66.0 (5.5) | 40.4 (6.3) | |
| C50 | 249 | 82.2 (2.5) | 70.3 (3.0) | 45.9 (3.5) | |
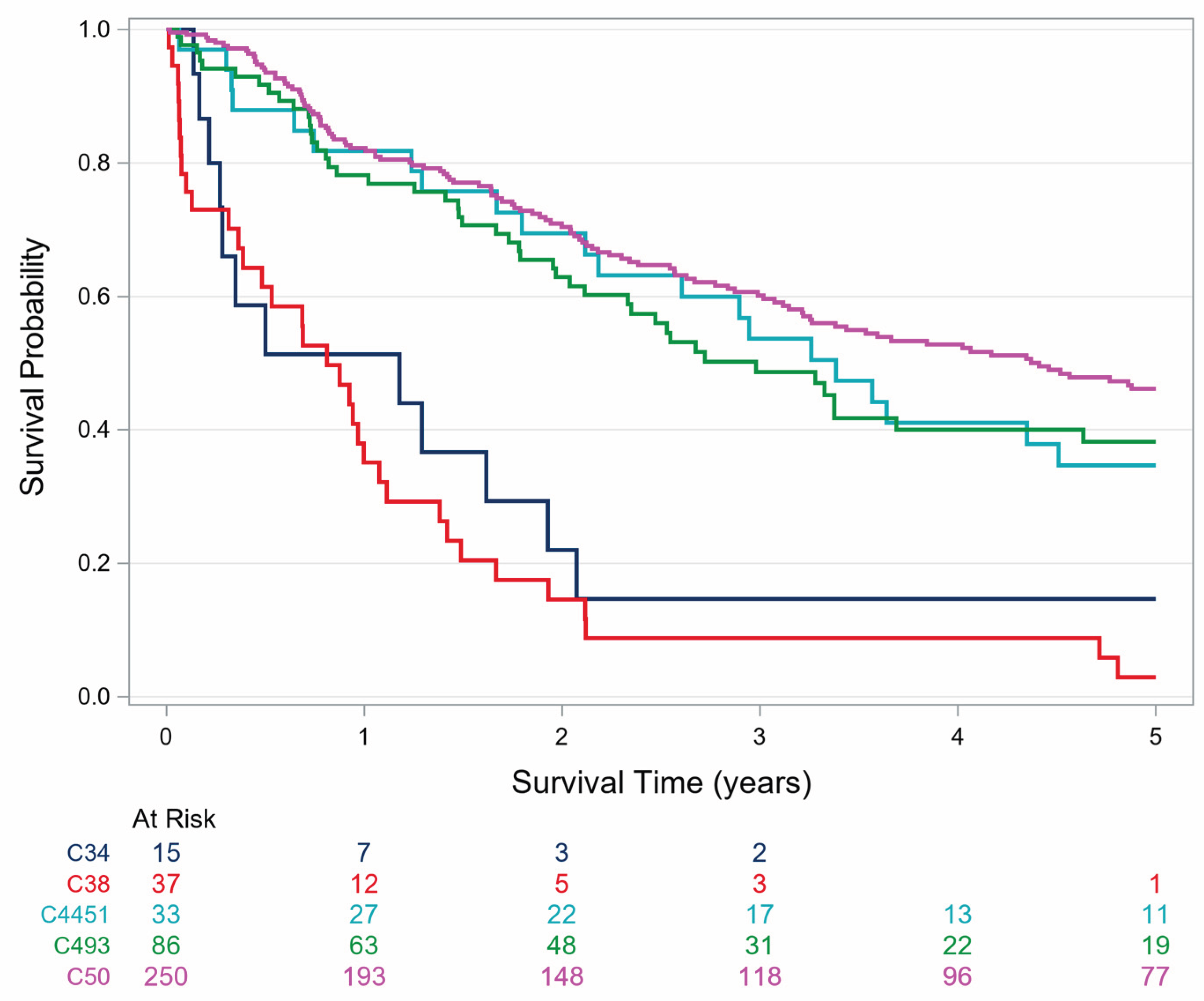
For women and men together, it appears that angiosarcomas of the lung (C34) and angiosarcomas of the pleura, heart and mediastinum (C38) have a markedly poorer OS than all other topographies (Figure 6). Female patients with angiosarcoma of these topographies have a poor prognosis. 5 years OS was 0%. All females died within 2.2 years after diagnosis of angiosarcoma (C34 and C38) which is even worse than OS of their male counterparts (Figure 4 and Figure 5).
Figure 4.
Survival of male patients with thorax angiosarcoma stratified by topography in North Rhine-Westphalia, 2008-2023.
Figure 4.
Survival of male patients with thorax angiosarcoma stratified by topography in North Rhine-Westphalia, 2008-2023.
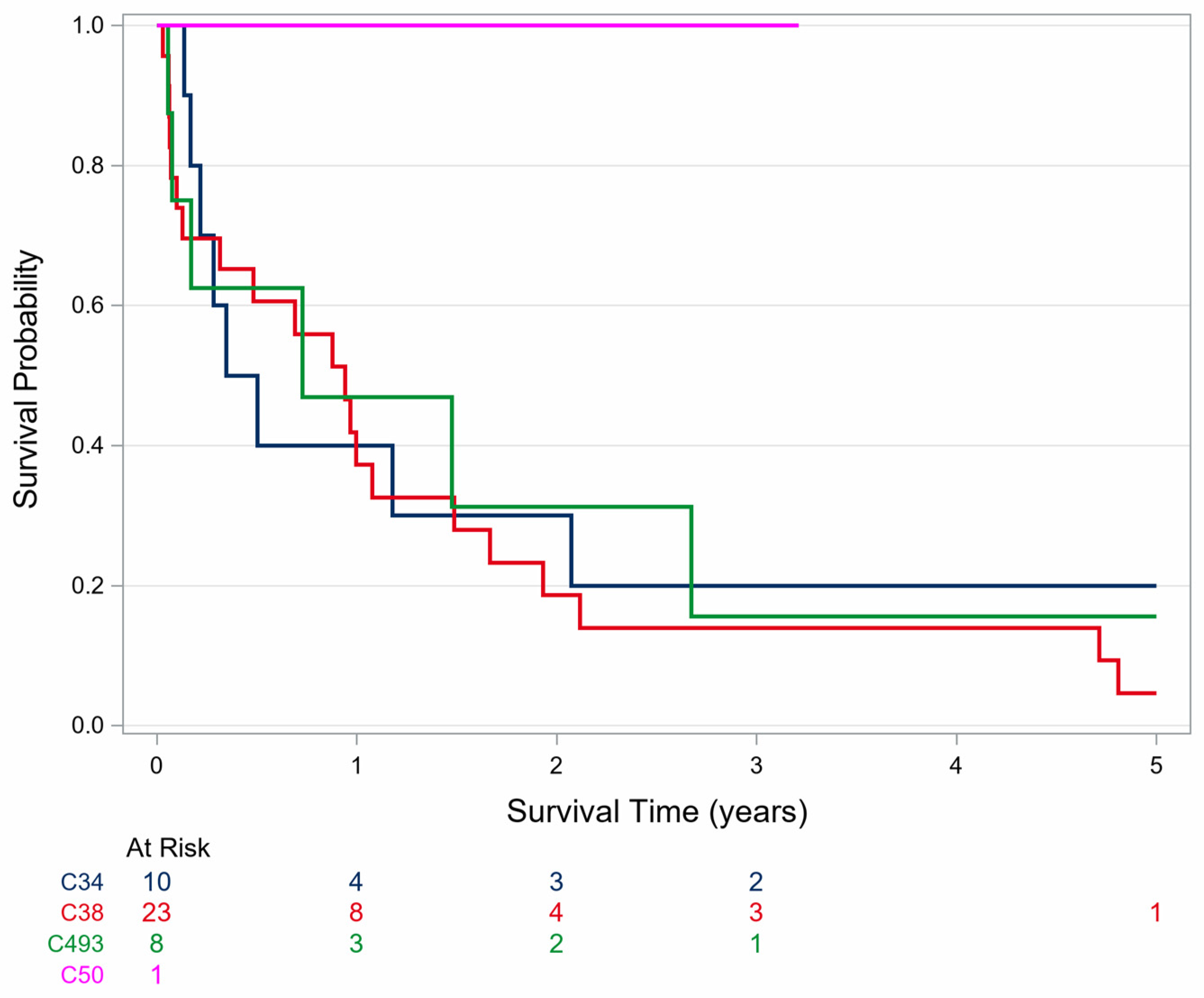
Figure 5.
Survival of female patients with thorax angiosarcoma stratified by topography in North Rhine-Westphalia, 2008-2023.
Figure 5.
Survival of female patients with thorax angiosarcoma stratified by topography in North Rhine-Westphalia, 2008-2023.
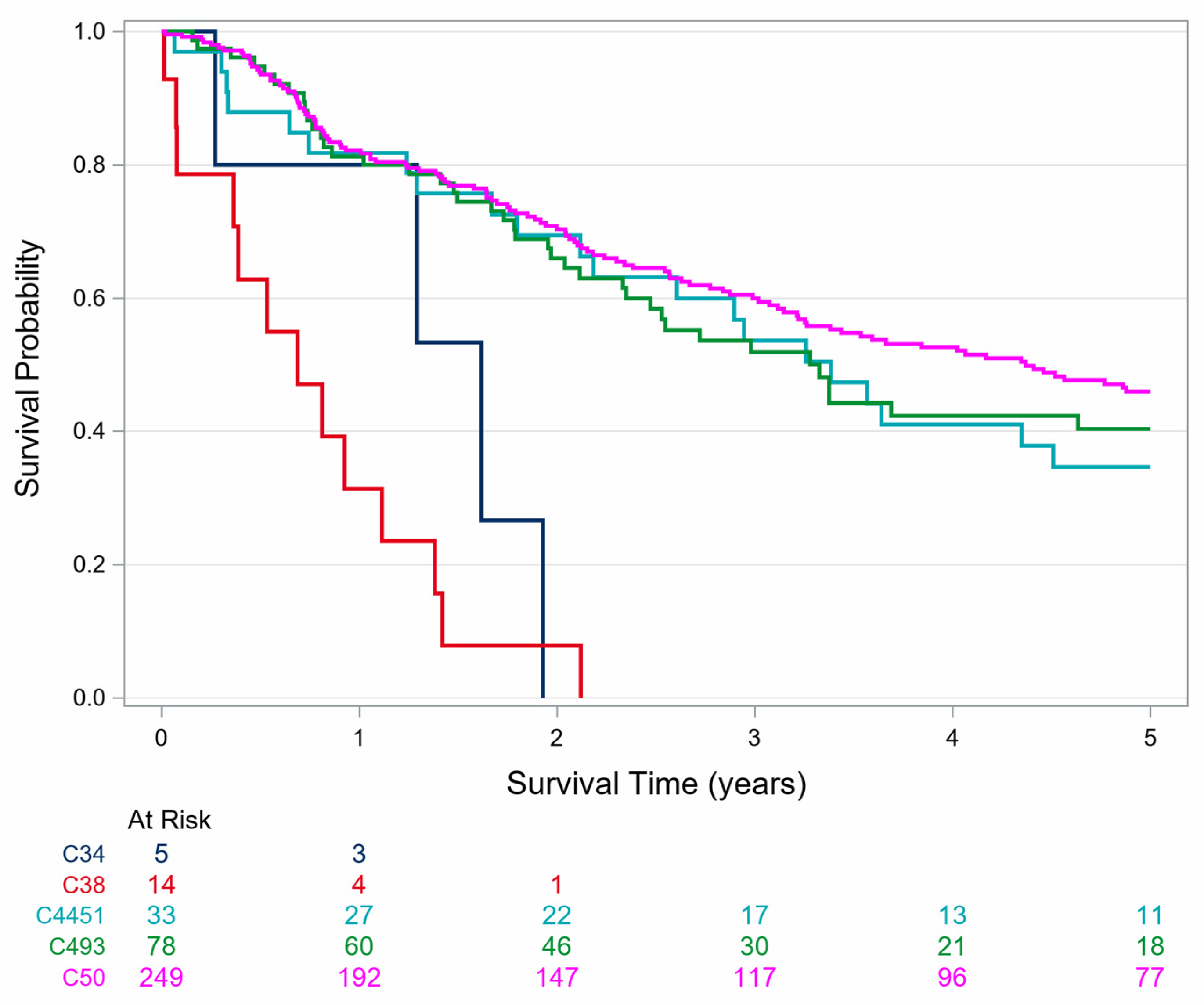
Figure 6.
Survival of patients with thorax angiosarcoma stratified by topography in North Rhine-Westphalia, 2008-2023.
Figure 6.
Survival of patients with thorax angiosarcoma stratified by topography in North Rhine-Westphalia, 2008-2023.
4. Discussion
In our analysis we included 421 patients with angiosarcoma from the largest German population-based registry. Women are affected at least 4 times more often and have a median age at diagnosis about 15 years higher than men. In the US 54.5% of all angiosarcomas affect women and for the thoracic subgroup angiosarcoma is more frequent in elder women [3]. However, angiosarcoma in young men is reported [15].
In our study 80% of all angiosarcomas were located in the breast or soft tissue of the thorax. However, 20% occur elsewhere in the thorax. Thus, angiosarcoma of the pleura or lung is an extremely rare condition. Slightly more than half of female patients have second primary angiosarcoma, which is related to the history of previous cancers. In our study we did not observe any male patient with second primary angiosarcoma. Thus, we emphasize this is an absolute rarity in men with thoracic angiosarcoma.
We assumed that all patients with angiosarcomas for whom no other cancers had been reported to the cancer registry prior to the diagnosis of angiosarcoma had primary angiosarcomas. Since we were only able to trace the history of cancer cases back to 2008, it is likely that the proportion of second tumors has been underestimated as other primary cancers may also have occurred before 2008. Furthermore, the differentiation between primary and second primary angiosarcoma is vague due to the sometimes very difficult to determine relationship.
We observed a 5-year OS of 38.5%. Interestingly, the prognosis of women with angiosarcoma was markedly better than that of men. Even women with primary angiosarcoma had a better prognosis than men. Only 12.0% of men were still alive 5 years after the diagnosis of thoracic angiosarcoma, while about 41.4% of all women were still alive after 5 years.
Our results show no decisive differences with regard to primary and second angiosarcoma. 2023 Chau et al. identified a trend of increasing incidence of second primary breast angiosarcoma while the incidence of primary breast angiosarcoma remained stable [16]. Our findings do not support this conclusion.
Other scientists merely investigated whether other cancers besides angiosarcomas were present, without taking into account the temporal relationship to the time of diagnosis of the angiosarcomas [3].
Our analyses show a much better prognosis for women compared to men with angiosarcomas of the thorax. We were able to clearly show that the advantage in terms of survival cannot be explained by the distinction between second primary and primary angiosarcoma, but rather by the different topographies. Almost 80% of angiosarcoma in men were diagnosed in the lung, heart, pleura and mediastinum, whereas these topographies account for only about 5% in women. Patients who develop angiosarcoma of the lung, heart, mediastinum, or pleura have a considerably worse prognosis than patients with angiosarcoma of the breast or thoracic skin. It appears plausible that this is due to earlier diagnosis during breast cancer follow-up and to the greater accessibility and feasibility of R0 resections of breast and thoracic skin tumours. This contrasts with the supposedly late detection and high-risk surgical treatment of, for example, angiosarcomas of the mediastinum.
There are some other factors that limit our results. First, as already emphasized in the introduction, angiosarcoma is associated with prior malignancies but also with prior trauma, foreign bodies, thorium dioxide, and viral infections [5]. Since cancer registry data do not provide information on these risk factors only prior malignancies were evaluated. Second, misclassification of primary and second angiosarcoma is possible due to incomplete in cancer registration before 2008. However, the survival estimates do not differ markedly between primary and second primary angiosarcoma and therefore this is not a major limitation.
Third, angiosarcoma is an extremely rare diagnosis with poor prognosis. It must be assumed that angiosarcoma of the heart, mediastinum, pleura, or lung are diagnoses that even experienced pathologists rarely have to evaluate. Thus, confusion with other angiogenic malignancies, and misdiagnosis with even benign diagnosis are possible [9].
Fourth, we did not include prognostically relevant information on treatment (for example radiation) to estimate more detailed OS because this information was too frequently missing and was available only from 2016 onwards. Future studies should explore these associations.
5. Conclusion
In conclusion, male patients suffering from angiosarcoma of the thorax have a markedly worse prognosis than women. According to 5-year OS, even women with a primary angiosarcoma had a better prognosis than men with a primary angiosarcoma. Contrary to our assumption, the distinction between primary and second primary angiosarcomas played no or only a subordinate role with regard to survival. The topography of the angiosarcoma had the greatest impact on the prognosis with the worst OS for angiosarcoma of the lung, heart, pleura und mediastinum. Finally, these topographies are the most frequent in men with thoracic angiosarcoma while they are very rare in women.
Author Contributions
Niels Michael Dörr-Jerat: Conceptualization, Writing – original draft. Ina Wellmann: Data curation, Methodology, Validation, Writing – review & editing. Franziska Rees: Methodology, Validation, Writing – review & editing. Andreas Stang: Writing – review & editing. Marcus Krüger: Writing – review & editing. Hiltraud Kajüter: Conceptualization, Methodology, Writing – review & editing.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability Statement
Data is available on request.
Conflicts of Interest
The authors declare no conflict of interest.
Conference submission
We presented our results at the annual meeting of the German Society for Hematology and Oncology 2025 in Cologne (Germany) and the fall meeting of the Central German Society for Pneumology and Thoracic Surgery 2025 in Magdeburg (Germany).
Abbreviations
The following abbreviations are used in this manuscript:
| AS | angiosarcoma |
| OS | overall survival |
| NRW | North Rhine-Westphalia |
| EAPC | estimated annual percentage changes |
References
- Alexiou, C.; Clelland, C.A.; Robinson, D.; Morgan, W.E. Primary angiosarcomas of the chest wall and pleura. Eur J Cardiothorac Surg. 1998, 14, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Young, R.J.; Brown, N.J.; Reed, M.W.; Hughes, D.; Woll, P.J. Angiosarcoma. Lancet Oncol. 2010, 11, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.J.; Ravi, V.; Schaub, S.K.; Kim, E.Y.; Sharib, J.; Mogal, H.; et al. Incidence and Presenting Characteristics of Angiosarcoma in the US, 2001-2020. JAMA Netw Open. 2024, 7, e246235. [Google Scholar] [CrossRef] [PubMed]
- Vojtíšek, R.; Sukovská, E.; Kylarová, M.; Kacerovská, D.; Baxa, V.; Divišová, B.; et al. Stewart-Treves syndrome: Case report and literature review. Rep Pract Oncol Radiother. 2020, 25, 934–938. [Google Scholar] [CrossRef] [PubMed]
- Maziak, D.E.; Shamji, F.M.; Peterson, R.; Perkins, D.G. Angiosarcoma of the chest wall. Ann Thorac Surg. 1999, 67, 839–841. [Google Scholar] [CrossRef] [PubMed]
- Sturm, E.C.; Marasco, I.S.; Katz, S.C. Multidisciplinary Management of Angiosarcoma - A Review. J. Surg Res. 2021, 257, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Verdin, V.; Mattart, L.; Cusumano, P.G.; De Hertogh, O.; De Meester, C.; Francart, D.; et al. Angiosarcoma associated with radiation therapy after treatment of breast cancer. Retrospective study on ten years. Cancer Radiother. 2021, 25, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Del Mastro, L.; Garrone, O.; Guenzi, M.; Cafiero, F.; Nicolò, G.; Rosso, R.; et al. Angiosarcoma of the residual breast after conservative surgery and radiotherapy for primary carcinoma. Ann Oncol. 1994, 5, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Dörr-Jerat, N.M.; May, C.J.; Knolle, J.; Schmidt, S.; Krüger, M. Case Report: Epithelioid angiosarcoma of the pleura. Front Surg. 2024, 27, 1393159. [Google Scholar] [CrossRef] [PubMed]
- Banks, J.; George, J.; Potter, S.; Gardiner, M.D.; Ives, C.; Shaaban, A.M. Breast Angiosarcoma Surveillance Study: UK national audit of management and outcomes of angiosarcoma of the breast and chest wall. Br J Surg. 2021, 108, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lu, Z.; Luo, Y.; Cai, J.; Wei, J.; Liu, A.; et al. Characteristics and outcomes of primary pleural angiosarcoma: a retrospective study of 43 published cases. Medicine (Baltimore) 2022, 101, e28785. [Google Scholar] [CrossRef] [PubMed]
- Doll, R.; Cook, P. Summarizing indices for comparison of cancer incidence data. Int. J. Cancer 1967, 2, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Individual Nonparametric Estimation from Incomplete Observations. Journal of the American Statistical Association 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Gonçalves, I.; Nunes, C.; Vieira, C.; Freitas, D.; Pinto, L. Primary Cardiac Angiosarcoma: A Rare and Fatal Diagnosi. Cureus 2021, 13, e20816. [Google Scholar] [CrossRef] [PubMed]
- Chau, B.; Loggers, E.T.; Cranmer, L.D.; Mogal, H.; Sharib, J.M.; Kim, E.Y.; et al. Secondary Breast Angiosarcoma After a Primary Diagnosis of Breast Cancer: A Retrospective Analysis of the Surveillance, Epidemiology, and End Results (SEER) Database. Am J Clin Oncol. 2023, 46, 567–571. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Age distribution of newly diagnosed male and female primary and second primary angiosarcoma in North Rhine-Westphalia, 2008-2023.
Figure 1.
Age distribution of newly diagnosed male and female primary and second primary angiosarcoma in North Rhine-Westphalia, 2008-2023.
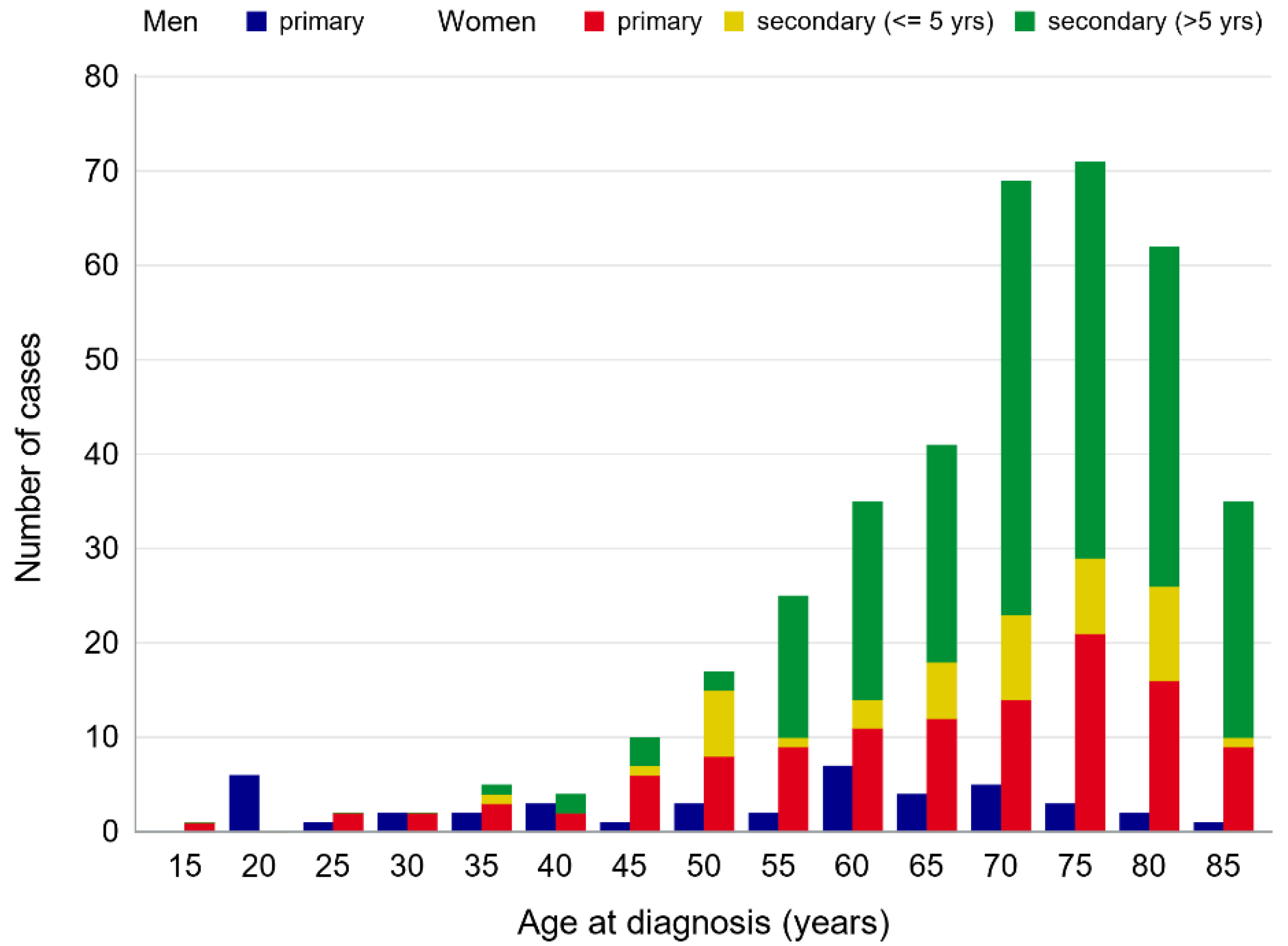
Figure 2.
Age standardized annual incidence rates (ASR, cases per million person-years) of angiosarcoma of the thorax in North Rhine-Westphalia, 2008-2023.
Figure 2.
Age standardized annual incidence rates (ASR, cases per million person-years) of angiosarcoma of the thorax in North Rhine-Westphalia, 2008-2023.
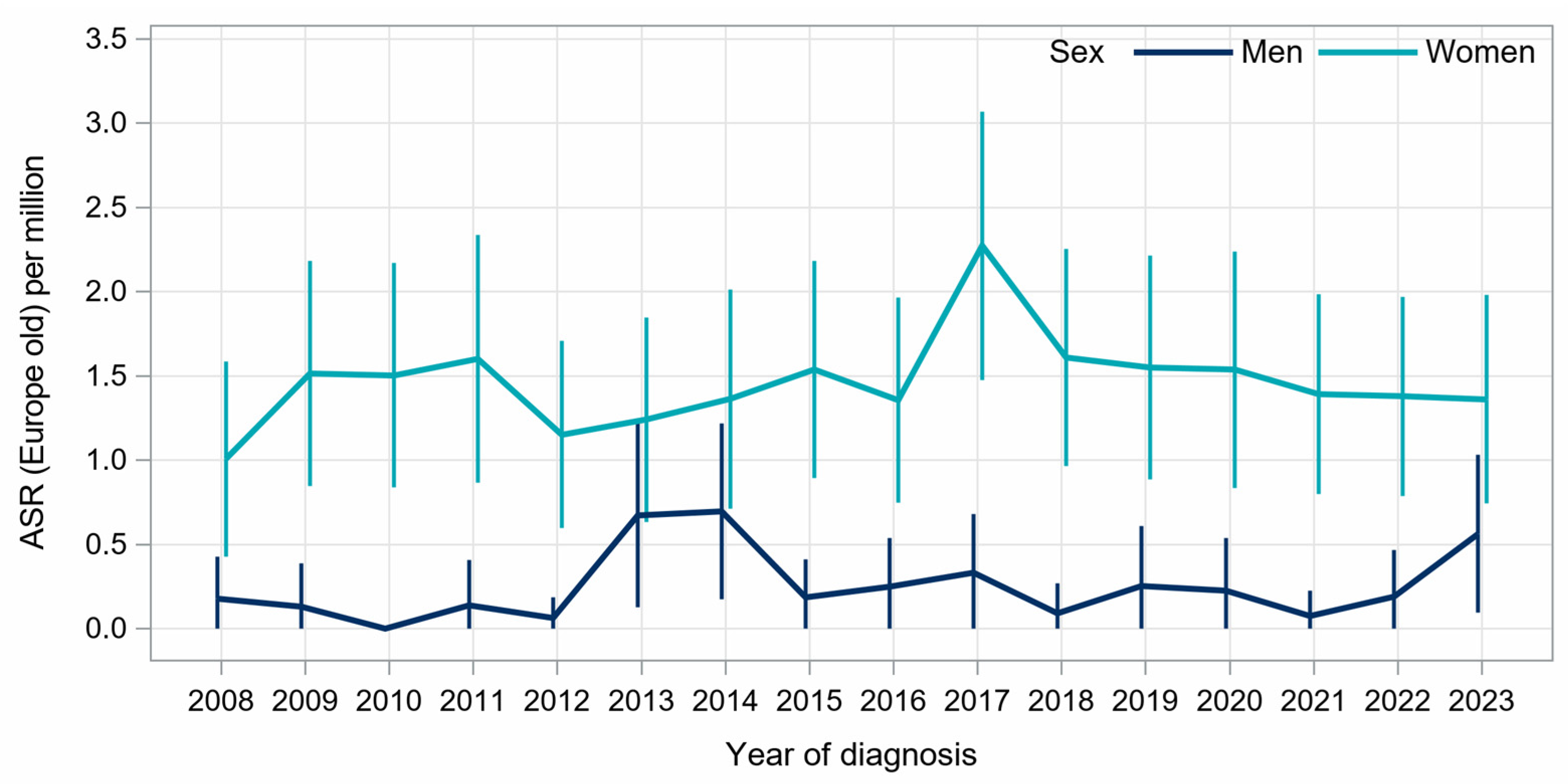
Figure 3.
Sex-specific survival of patients with thoracic angiosarcoma stratified by a previous skin and/or breast cancer history in North Rhine-Westphalia, 2008-2023.
Figure 3.
Sex-specific survival of patients with thoracic angiosarcoma stratified by a previous skin and/or breast cancer history in North Rhine-Westphalia, 2008-2023.
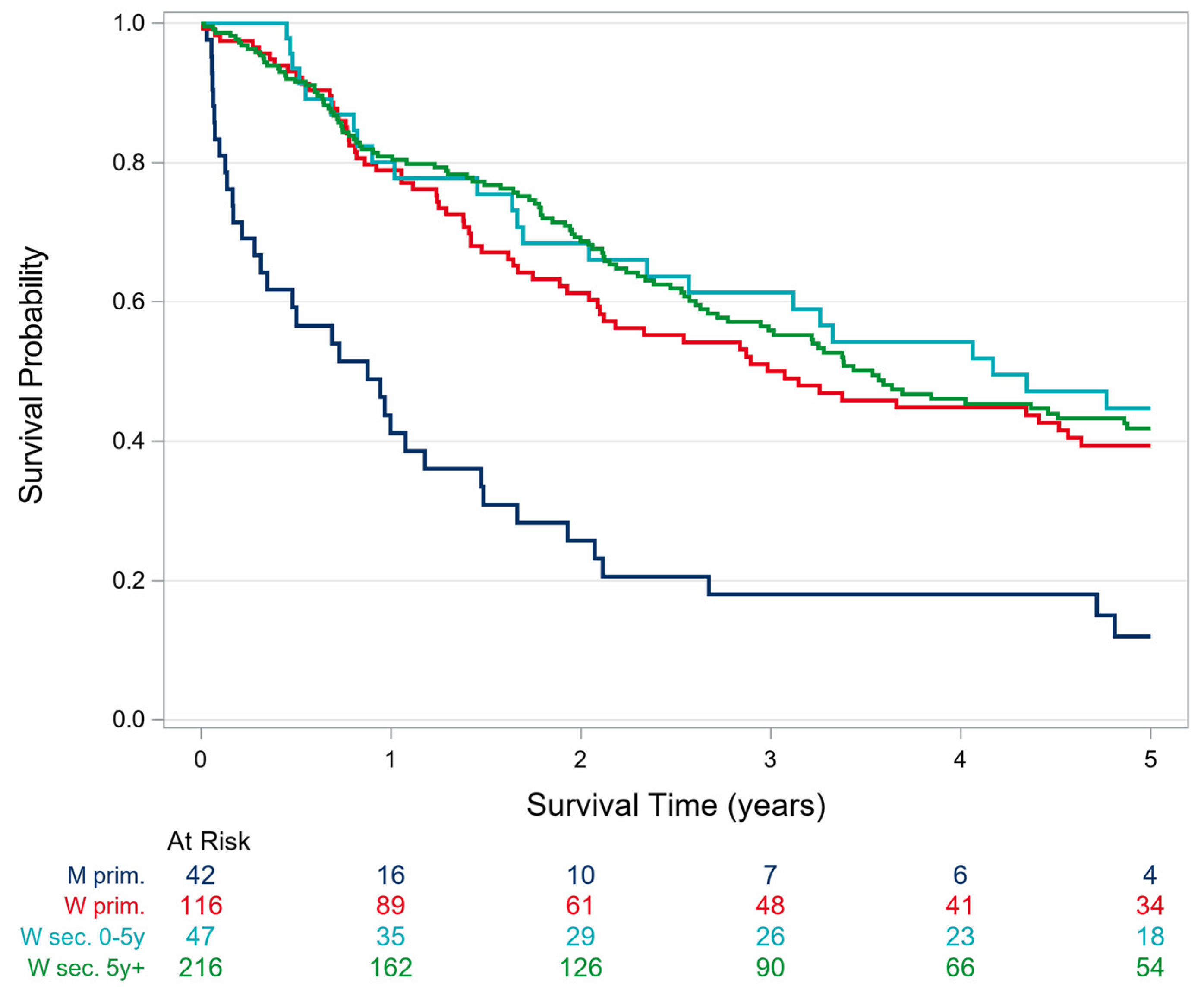
Table 1.
Baseline characteristics of newly diagnosed male and female patients with angiosarcoma of the thorax, North Rhine-Westphalia, 2008-2023.
Table 1.
Baseline characteristics of newly diagnosed male and female patients with angiosarcoma of the thorax, North Rhine-Westphalia, 2008-2023.
| Charakteristic | Men | Women | ||
|---|---|---|---|---|
| Angiosarcoma of thorax, morphology 9120/3 | 42 | 379 | ||
| Mean age of diagnosis (standard deviation) | 54.4 | (19.8) | 70.8 | (12.5) |
| Age at diagnosis (years), n (%) | ||||
| 0-19 | 0 | (0) | 1 | (0.3%) |
| 20-49 | 15 | (35.7%) | 23 | (6.1%) |
| 50-59 | 5 | (11.9%) | 41 | (10.8%) |
| 60-69 | 11 | (26.2%) | 76 | (20.1%) |
| 70-79 | 8 | (19%) | 140 | (36.9%) |
| 80+ | 3 | (7.1%) | 98 | (25.9%) |
| Topography, n (%) | ||||
| bronchus and lung (C34) | 10 | (23.8%) | 6 | (1.6%) |
| heart, mediastinum and pleura (C38) | 23 | (54.8%) | 14 | (3.7%) |
| skin of thorax (C44.51) | 0 | (0%) | 33 | (8.7%) |
| soft tissues of thorax (C49.3) | 8 | (19%) | 77 | (20.3%) |
| breast (C50) | 1 | (2.4%) | 249 | (65.7%) |
| Pre-existing diagnosis of skin or breast cancer | ||||
| Yes, more than 5 years before AT-diagnosis | 0 | (0%) | 215 | (56.7%) |
| Mean age of diagnosis (standard deviation) | 73.1 | (10.3) | ||
| Yes, up to 5 years before AT-diagnosis | 0 | (0%) | 47 | (12.4%) |
| Mean age of diagnosis (standard deviation) | 69.5 | (11.6) | ||
| No | 42 | (100%) | 117 | (30.9%) |
| Mean age of diagnosis (standard deviation) | 54.4 | (19.8) | 67.0 | (15.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



