
Submitted:
05 January 2026
Posted:
05 January 2026
You are already at the latest version
Abstract
Background. Conservative management of port-related bacteremia often includes locally administered antimicrobials, known as antimicrobial lock therapy (ALT). Current guidelines recommend daily replacement of antimicrobial lock solutions (ALS). We aimed to evaluate whether ALS could remain effective with extended dwell times of up to 10 days. Methods. In this randomized clinical trial, patients with noninfected, recently implanted ports were assigned to one of five ALS dwell-time groups, ranging from 1 to 10 days. Each ALS contained heparin plus an antimicrobial at standard intraluminal concentrations: vancomycin 2 mg/mL, teicoplanin 10 mg/mL, linezolid 1.8 mg/mL, daptomycin 5 mg/mL, or tigecycline 4.5 mg/mL. The primary endpoint was the time at which intraluminal drug concentrations decreased below 1 mg/mL (ClinicalTrials.gov NCT01592032). Results. Vancomycin and linezolid concentrations fell significantly below 1 mg/mL after 3 days of dwell time. Daptomycin and tigecycline concentrations decreased significantly after 7 days but remained above 1 mg/mL. Teicoplanin concentrations did not decline significantly after 7 days. Conclusions. Optimal ALS dwell time depends on the antimicrobial agent. Vancomycin and linezolid locks require daily replacement, whereas daptomycin, tigecycline, and teicoplanin locks maintain therapeutic concentrations for up to 7 days. These findings support individualized ALS replacement strategies, potentially reducing the need for daily interventions.
Keywords:
catheters
; ports
; implantable
; bacteremia
; indwelling
; anti-infective agents
; vancomycin
; tigecycline
; linezolid
; daptomycin
1. Background
Totally implantable venous access ports are widely used in cancer patients, but their use is frequently complicated by thrombosis and infection [1]. The risk of catheter-related bloodstream infection (BSI) is estimated at 0.1 per 1,000 port-days [2], and repeated device manipulation further increases this risk [3]. Overall, up to 10% of port carriers will experience device-related infectious complications [4], and more than half of these cases ultimately require port removal [5]. Staphylococci account for nearly 70% of all port-related BSIs [6].
Management of uncomplicated catheter-related bacteremia (CRB) typically combines systemic therapy with local antimicrobial administration through antimicrobial lock therapy (ALT). Current recommendations suggest 10–14 days of treatment [7]. ALT involves instilling a highly concentrated antimicrobial solution into the catheter lumen and maintaining it for a defined dwell time to eradicate intraluminal microorganisms [8]. According to the Infectious Diseases Society of America (IDSA), antimicrobial lock solutions (ALS) should generally be replaced every 24 hours, except in the case of hemodialysis catheters [7]. However, evidence is lacking to determine the optimal replacement interval for ALS.
Extending ALS dwell time could reduce port manipulation to only once or twice during the course of therapy, thereby lowering costs and minimizing procedure-related morbidity without compromising efficacy. Encouraged by previous reports and by our own clinical experience [9,10,11], we designed a randomized clinical trial to evaluate the optimal replacement intervals for five commonly used ALS—vancomycin, teicoplanin, linezolid, daptomycin, and tigecycline—instilled into noninfected ports and maintained in situ for variable dwell times.
2. Patients and Methods
Setting and study population. This clinical trial was conducted at the University Hospital, Clínica Universidad de Navarra (Pamplona, Spain) between May 2012 and January 2015. All patientteicoplanins with recently implanted venous access ports were eligible. Exclusion criteria were: clinical or microbiological evidence of infection (with or without systemic antimicrobial therapy); known allergy to heparin or any of the study antimicrobials; concomitant systemic anticoagulation; pregnancy; and inability to provide written informed consent. The study was approved by the local Institutional Review Board (79/2010) and the Spanish Agency of Medicines and Medical Devices (EudraCT 2010-023814-29). All participants gave written informed consent. The trial was registered at ClinicalTrials.gov (NCT01592032).
Trial design. Patients were randomly assigned, in a single-blind design, to receive one of five antimicrobial lock solutions (ALS). Each ALS contained 100 IU/mL of 1% sodium heparin plus one antimicrobial: vancomycin 2 mg/mL, teicoplanin 10 mg/mL, linezolid 1.8 mg/mL, daptomycin 5 mg/mL, or tigecycline 4.5 mg/mL, for a final volume of 10 mL. Antimicrobial concentrations were chosen based on the highest levels reported in the literature [12,13,14] and our clinical experience [9,10,15]. All antimicrobials were reconstituted in normal saline, except linezolid (ready-to-use) and daptomycin (lactated Ringer’s solution). Randomization was computer-generated, and the research team was blinded to antimicrobial assignment. Each patient could participate only once.
ALS dwell times were escalated sequentially (1, 3, 5, 7, and 10 days). Each dwell-time period required inclusion of five patients per antimicrobial group. Prior to ALS instillation, a 10 mL blood sample was drawn to confirm port sterility. After flushing with 10 mL of 0.9% sodium chloride, 5 mL of ALS was instilled into each port, which then remained untouched until the end of the dwell time. After completion, the first 2 mL withdrawn from the port was analyzed for antimicrobial concentration using high-performance liquid chromatography (HPLC; Agilent Technologies, Santa Clara, CA, USA). Urea concentrations were determined (Synchron® Clinical Systems, Beckman Coulter, Brea, CA, USA), and the systemic-to-sample urea ratio was used to correct antimicrobial concentrations for individual blood dilution [16].
If the median antimicrobial concentration remained above 1 mg/mL for a given ALS group, a new set of five patients was randomized to the next dwell-time interval. A median concentration <1 mg/mL terminated randomization for that ALS group. The primary endpoint was the time until intraluminal antimicrobial concentration fell below 1 mg/mL.
Statistical analysis. Antimicrobial concentrations were compared between groups using the Kruskal–Wallis test, and paired comparisons of concentrations at baseline versus end of dwell time were analyzed with the Wilcoxon test. Statistical significance was set at an alpha level of 0.05 (two-tailed). Analyses were performed using SPSS software, version 15.0.1 (SPSS Inc., Chicago, IL, USA).
3. Results
Over the 32-month study period, 484 consecutive patients were screened for eligibility (Figure 1). A total of 93 patients were randomized into the five ALS groups: 11 to vancomycin, 24 to teicoplanin, 10 to linezolid, 26 to daptomycin, and 22 to tigecycline. Baseline characteristics, including sex, age, underlying malignancy, and mean time from catheter placement to study entry, were comparable across groups (Table 1). No port-related infections occurred in any of the patients during the study, and no serious drug-related adverse events were observed.
After 1 day of dwell time, all five ALS maintained antimicrobial concentrations above 1 mg/mL. At 3 days, the median concentrations of vancomycin and linezolid had fallen below 1 mg/mL, leading to termination of further randomization in these groups. The decrease in concentrations of both drugs compared with baseline was statistically significant (P = .043).
Patients continued to be enrolled in the teicoplanin, daptomycin, and tigecycline groups for dwell times of 5 and 7 days. Teicoplanin median concentrations remained above 1 mg/mL at both time points, with no significant difference compared with the instilled concentration (P = .893). In contrast, daptomycin and tigecycline concentrations decreased significantly after 7 days (P = .043), but still remained above 1 mg/mL (Table 2).
Due to limited enrollment, the 10-day dwell time group could not be completed, and the study concluded without data for this interval.
4. Discussion
Antimicrobial lock replacement should be tailored to the agent: vancomycin and linezolid require daily changes, while teicoplanin, daptomycin, and tigecycline remain effective for up to 7 days, reducing interventions without compromising efficacy.
The Infectious Diseases Society of America (IDSA) guidelines recommend that the dwell time of an antimicrobial lock solution (ALS) should not exceed 24 hours, except for hemodialysis catheters [7]. Nevertheless, the optimal replacement interval remains undefined, with reported recommendations ranging between 8 and 24 hours per day [17]. Our trial demonstrates that the decline in antimicrobial concentration within ALS instilled into ports is critical for determining replacement time. Consequently, the general recommendation to replace ALS every 24 hours should be tailored according to the antimicrobial agent employed. Specifically, ALS containing teicoplanin (10 mg/mL), daptomycin (5 mg/mL), or tigecycline (4.5 mg/mL) could be safely replaced every 7 days, whereas ALS with vancomycin or linezolid should be replaced daily.
The duration of ALS exposure to the catheter lumen is pivotal for biofilm eradication. Our study was designed to establish the longest effective dwell time without compromising intraluminal concentrations. Extrapolating findings from hemodialysis catheter–related bacteremia (CRB) to port-related infections is problematic, as hemodialysis catheters are accessed every 48–72 hours, whereas ports are generally used daily or intermittently for chemotherapy administration.
Several factors influence antimicrobial concentrations and activity [14], including catheter design [18], intrinsic drug properties [19], protein-binding capacity [20], free drug fraction [21], and degradation rate [22]. Fluid dynamics also contribute: the Hagen–Poiseuille velocity distribution for flow [23], passive diffusion into the bloodstream [24], density differences between the lock solution and blood [25], and exchange driven by postural changes [26].
Soriano et al. described a gradient of vancomycin concentrations along hemodialysis catheters [27], inferred from sequential aspiration of three blood samples. However, this indirect approach is limited by assumptions regarding catheter segment representation. By contrast, our study analyzed a single 2 mL aspirate from five independent patients per ALS and dwell time, thereby reducing reliance on sequential sampling. Still, we recognize that recommendations based on the median of only five samples per group are limited.
Deposits accumulating in the port reservoir may contribute to the gradual decline of intraluminal concentrations. To date, no in vivo studies have characterized antimicrobial loss in port-locked solutions. This knowledge gap has reinforced the practice of daily ALS replacement, rather than exploring the benefits of instilling maximal concentrations and allowing prolonged dwell times, provided safety and efficacy are maintained. Key unanswered questions remain: would increasing antimicrobial concentrations be safer than extending dwell time, or could higher concentrations enable longer dwell intervals?
Previous studies have reported success with dwell times beyond 24 hours. Sánchez-Muñoz et al. described an 85.7% clinical success rate in 14 patients treated with a 3-day lock combining heparin and vancomycin or amikacin [28], though without measuring residual concentrations. Conversely, Haimi-Cohen et al. found a residual vancomycin concentration of 0.13 mg/mL even 28 days after instillation [12]. While maintaining residual drug levels is relevant, avoiding prolonged exposure to subtherapeutic concentrations is paramount, given the risk of resistance development [29]. Indeed, low vancomycin concentrations can enhance staphylococcal biofilm density [30]. In our trial, we established a conservative threshold of 1 mg/mL, representing at least 1000-fold the MIC for planktonic staphylococci [31] and safely above the mutant prevention concentration [19].
Our findings confirmed a progressive decline in ALS concentrations over time. After 3 days, vancomycin concentrations decreased by 77%, falling below bactericidal thresholds [31]. Adequate antimicrobial levels are essential for targeting persister cells, which tolerate high concentrations despite intrinsic susceptibility, thereby contributing to therapeutic failure and biofilm persistence [32]. Similarly, linezolid concentrations decreased by 60% after 3 days. Clinical data on linezolid as lock therapy remain scarce [10,27], though Sofroniadou et al. reported that linezolid locks prevented CRB in hemodialysis patients [35]. While linezolid may be valuable in specific scenarios—such as prosthetic infections [36] or endocarditis [34,35]—evidence for its use in lock solutions remains limited.
Teicoplanin emerged as the most stable ALS in our study. Median concentrations remained unchanged after 7 days (P = 0.89), possibly due to its affinity for catheter materials [39]. Clinical success rates with daily teicoplanin locks for CRB range from 88% to 100% [11,37]. Our data suggest that this efficacy may derive from the remarkable stability of the 10 mg/mL solution over extended dwell times.
There is increasing evidence for daptomycin in CRB treatment, both in vivo [12,30] and in vitro [31,32]. Experimental catheter infection models with daptomycin 2–5 mg/mL have shown significant eradication of staphylococci [33,34]. Raad et al. and Meije et al. demonstrated superior outcomes with daptomycin locks compared to glycopeptides [45]. In our trial, daptomycin maintained concentrations >2000 times the staphylococcal MIC for up to 7 days, supporting extension of replacement intervals to once or twice during the 10–14 days recommended by IDSA [7].
Tigecycline has been rarely used in ALT. Aslam et al. reported an 83% success rate with a lock containing N-acetylcysteine, heparin, and tigecycline 1 mg/mL in hemodialysis CRB [11]. However, tigecycline monotherapy for BSI remains controversial [46]. Minocycline–EDTA locks have demonstrated efficacy in hemodialysis [47] and pediatric oncology patients [48], with dwell times up to 7 days. Our findings suggest that tigecycline may be considered in select scenarios when alternatives are lacking.
Overall, we observed that teicoplanin (10 mg/mL), tigecycline (4.5 mg/mL), and daptomycin (5 mg/mL) maintained intraluminal concentrations above 1 mg/mL for 7 days, whereas vancomycin and linezolid did not. We acknowledge the limitations of our study, including small sample sizes and heterogeneity in antimicrobial concentrations. Furthermore, maintaining high intraluminal concentrations for 7 days does not guarantee therapeutic success, given the variability in antimicrobial biofilm penetration [49].
In conclusion, our findings suggest that replacement intervals for ALS in ports could be extended from daily to once every 7 days when using teicoplanin, daptomycin, or tigecycline against coagulase-negative staphylococci (CoNS). By contrast, vancomycin and linezolid locks should continue to be replaced every 24 hours.
5. Strengths and Limitations
Strengths
- This is the first randomized clinical trial specifically designed to evaluate the optimal dwell time of antimicrobial lock solutions (ALS) in totally implantable venous access ports.
- The study directly quantified intraluminal antimicrobial concentrations in vivo, using standardized high-performance liquid chromatography with urea correction, thereby providing robust pharmacokinetic data under clinical conditions.
- Multiple antimicrobials commonly used in lock therapy (vancomycin, teicoplanin, linezolid, daptomycin, tigecycline) were compared simultaneously, allowing drug-specific recommendations for replacement intervals.
- The trial design with stepwise dwell-time escalation enabled the identification of thresholds for loss of efficacy without exposing patients to unnecessary risk.
Limitations
- The sample size within each antimicrobial–dwell time subgroup was limited (n=5 per time point), reducing statistical power and generalizability.
- Port use in the study was restricted to noninfected, newly implanted devices, which may not fully reflect clinical practice in infected or long-term ports.
- Concentration thresholds were based on pharmacokinetic/pharmacodynamic principles (≥1 mg/mL) rather than direct clinical outcomes, so translation to real-world effectiveness requires caution.
- The 10-day dwell time arm could not be completed due to recruitment constraints, leaving the upper limit of safe dwell times undetermined.
- Findings apply to the antimicrobial concentrations tested, which may not account for alternative formulations, catheter materials, or patient populations.
Clinical Implications
- Replacement intervals for antimicrobial lock solutions (ALS) should be individualized according to the specific agent used.
- Vancomycin and linezolid locks require daily replacement, while teicoplanin, daptomycin, and tigecycline maintain effective concentrations for up to 7 days.
- Extending ALS dwell times could reduce port manipulations, lower healthcare costs, and minimize patient discomfort without compromising efficacy.
Funding
This study was supported by the Instituto de Salud Carlos III (ISCIII), Ministry of Health, Social Services and Equality, Madrid, Spain [Grant EC10-329], and by the School of Medicine, University of Navarra, Pamplona, Spain.
Acknowledgments
We are deeply grateful to D. Martínez-Urbistondo for statistical support, and to M. A. Casares and M. Fernández-Rivero for their expert assistance with laboratory analyses. We also extend our sincere thanks to the nursing staff of the Oncology Day Hospital for their commitment, collaboration, and invaluable contribution to the study. ChatGPT (OpenAI) was used to assist in the development of the graphical abstract, following a preliminary concept and step-by-step guidance from the authors. The AI tool did not generate independent scientific content. The authors critically reviewed, modified, and validated the final graphical abstract.
References
- Lee GJ, Hong SH, Roh SY, et al. A case-control study to identify risk factors for totally implantable central venous port-related bloodstream infection. Cancer Res Treat. 2014; 46(3):250–260. [CrossRef]
- Maki, D G; Kluger, D M; Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clin Proc. 2006; 81(9):1159–1171. [CrossRef]
- Adler A, Yaniv I, Solter E, et al. Catheter-associated bloodstream infections in pediatric hematology-oncology patients: factors associated with catheter removal and recurrence. J Pediatr Hematol Oncol. 2006; 28(1):23–28.
- Barbetakis N, Asteriou C, Kleontas A, Tsilikas C. Totally implantable central venous access ports. Analysis of 700 cases. J Surg Oncol. 2011; 104(6):654–656. [CrossRef]
- Chang L, Tsai JS, Huang SJ, Shih CC. Evaluation of infectious complications of the implantable venous access system in a general oncologic population. Am J Infect Control. 2003; 31(1):34–39. [CrossRef]
- Raad I, Hachem R, Hanna H, et al. Sources and outcome of bloodstream infections in cancer patients: the role of central venous catheters. Eur J Clin Microbiol Infect Dis. 2007; 26(8):549–556. [CrossRef]
- Mermel, Leonard A.; Allon, Michael; Bouza, Emilio; Craven, Donald E.; Flynn, Patricia; O’Grady, Naomi P.; Raad, Issam I.; Rijnders, Bart J. A.; Sherertz, Robert J.; Warren DK. Clinical Practice Guidelines for the Diagnosis and Management of Intravascular Catheter-Related Infection: 2009 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2009; 49:1–45. [CrossRef]
- Messing, Bernard; Peitra-Cohen, Sophie; Debure, Alain; Beliah, Martine; Bernier J-J. Antibiotic-lock technique: a new approach to optimal therapy for catheter-related sepsis in home-parenteral nutrition patients. J Parenter Enter Nutr. 1988; 12(2):185–189. [CrossRef]
- Pozo JL Del, Garcia Cenoz M, Hernaez S, et al. Effectiveness of teicoplanin versus vancomycin lock therapy in the treatment of port-related coagulase-negative staphylococci bacteraemia: a prospective case-series analysis. Int J Antimicrob Agents. 2009; 34(5):482–485. [CrossRef]
- Pozo JL Del, Rodil R, Aguinaga A, et al. Daptomycin lock therapy for grampositive long-term catheter-related bloodstream infections. Int J Clin Pract. 2012; 66(3):305–308. [CrossRef]
- Aslam, Saima; Trautner, Barbara W; Ramanathan, Venkat; Darouiche RO. Pilot Trial of N -acetylcysteine and Tigecycline as a Catheter-Lock Solution for Treatment of Hemodialysis Catheter – Associated Bacteremia. Infect Control Hosp Epidemiol. 2008; 29(9):894–897. [CrossRef]
- Haimi-Cohen Y, Husain N, Meenan J, Karayalcin G, Lehrer M, Rubin LG. Vancomycin and ceftazidime bioactivities persist for at least 2 weeks in the lumen in ports: Simplifying treatment of port-associated bloodstream infections by using the antibiotic lock technique. Antimicrob Agents Chemother. 2001; 45(5):1565–1567. [CrossRef]
- Fernandez-Hidalgo N, Gavalda J, Almirante B, et al. Evaluation of linezolid, vancomycin, gentamicin and ciprofloxacin in a rabbit model of antibiotic-lock technique for Staphylococcus aureus catheter-related infection. J Antimicrob Chemother. 2010; 65(3):525–530. [CrossRef]
- Droste JC, Jeraj HA, MacDonald A, Farrington K. Stability and in vitro efficacy of antibiotic-heparin lock solutions potentially useful for treatment of central venous catheter-related sepsis. J Antimicrob Chemother. 2003; 51(4):849–855. [CrossRef]
- Pozo, J.L.; Alonso, M.; Serrera, A.; Hernaez, S.; Aguinaga, A.; Leiva J. Effectiveness of the antibiotic lock therapy for the treatment of port-related enterococci, Gram-negative, or Gram-positive bacilli bloodstream infections. Diagn Microbiol Infect Dis. 2009; 63(2):208–212. [CrossRef]
- He J, Gao S, Hu M, Chow DS-L, Tam VH. A validated ultra-performance liquid chromatography-tandem mass spectrometry method for the quantification of polymyxin B in mouse serum and epithelial lining fluid: application to pharmacokinetic studies. J Antimicrob Chemother. 2013; 68:1104–10. [CrossRef]
- Justo JA, Bookstaver PB. Antibiotic lock therapy: Review of technique and logistical challenges. Infect. Drug Resist. 2014. p. 343–363. [CrossRef]
- Ash SR. Fluid mechanics and clinical success of central venous catheters for dialysis–answers to simple but persisting problems. Semin Dial. 2007; 20(3):237–256. [CrossRef]
- Canut Blasco A, Aguilar Alfaro L, Cobo Reinoso J, Gimenez Mestre MJ, Rodriguez-Gascon A. Pharmacokinetic/pharmacodynamic analysis in microbiology: a tool for the evaluation of the antimicrobial treatment. Enferm Infecc Microbiol Clin. 2015; 33(1):48–57. [CrossRef]
- Peters, G; Locci RP. Microbial colonization of prosthetic devices. II. Scanning electron microscopy of naturally infected intravenous catheters. Zbl Bakt Hyg, I Abt Orig B. 1981; 173:293–299.
- Armijo JA. Farmacocinética: absorción, distribución y eliminación de los fármacos. In: Flórez J, Armijo JA, Mediavilla A, editors. Farmacol Humana. Barcelona, España: Elsevier Masson; 2008. p. 57–85.
- Cantas L, Shah SQA, Cavaco LM, et al. A brief multi-disciplinary review on antimicrobial resistance in medicine and its linkage to the global environmental microbiota. Front Microbiol. 2013; 4(May 14):96. [CrossRef]
- Polaschegg H-D, Shah C. Overspill of catheter locking solution: safety and efficacy aspects. ASAIO J. 2003; 49:713–715. [CrossRef]
- Polaschegg H-DD. Diffusion study. Hemodial Int. 2004; 8(3):304–305. [CrossRef]
- Polaschegg H-D. Loss of catheter locking solution caused by fluid density. ASAIO J. 2005; 51:230–235. [CrossRef]
- Wagner M, Schilcher G, Ribitsch W, Horina J, Polaschegg HD. In-vivo verification of catheter lock spillage by gravity. 39th EDTNA/ERCA Int. Conf. Dublin, Ireland. Poster P 132.2010.
- Soriano A, Bregada E, Marques JM, et al. Decreasing gradient of antibiotic concentration in the lumen of catheters locked with vancomycin. Eur J Clin Microbiol Infect Dis. 2007; 26(9):659–661. [CrossRef]
- Sánchez-Muñoz A, Aguado JM, López-Martín A, et al. Usefulness of antibiotic-lock technique in management of oncology patients with uncomplicated bacteremia related to tunneled catheters. Eur J Clin Microbiol Infect Dis. 2005; 24(4):291–293. [CrossRef]
- Onder AM, Chandar J, Billings AA, et al. Comparison of early versus late use of antibiotic locks in the treatment of catheter-related bacteremia. Clin J Am Soc Nephrol. 2008; 3(4):1048–1056. [CrossRef]
- Cargill JS, Upton M. Low concentrations of vancomycin stimulate biofilm formation in some clinical isolates of Staphylococcus epidermidis. J Clin Pathol. 2009; 62(12):1112–1116. [CrossRef]
- Institute C and LS. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-Fourth Informational Supplement M100-S24. CLSI. Wayne, PA, USA; 2014.
- Keren I, Shah D, Spoering A, Kaldalu N, Lewis K. Specialized persister cells and the mechanism of multidrug tolerance in Escherichia coli. J Bacteriol. 2004; 186(24):8172–8180. [CrossRef]
- Moreno RB, Rives S, Justicia A, et al. Successful port-a-cath salvage using linezolid in children with acute leukemia. Pediatr Blood Cancer. 2013; 60(9):E103-105. [CrossRef]
- Castagnola E, Bandettini R, Lorenzi I, Caviglia I, Macrina G, Tacchella A. Catheter-related bacteremia caused by methicillin-resistant coagulase negative staphylococci with elevated minimal inhibitory concentration for vancomycin. Pediatr Infect Dis J. 2010; 29(11):1047–1048. [CrossRef]
- Sofroniadou S, Revela I, Smirloglou D, et al. Linezolid versus vancomycin antibiotic lock solution for the prevention of nontunneled catheter-related blood stream infections in hemodialysis patients: a prospective randomized study. Semin Dial. 2012; 25(3):344–350. [CrossRef]
- Morata L, Tornero E, Martínez-Pastor JC, García-Ramiro S, Mensa J, Soriano A. Clinical experience with linezolid for the treatment of orthopaedic implant infections. J Antimicrob Chemother. 2014; 69(SUPPL1):i47–52. [CrossRef]
- San-Juan R, Fernández-Ruiz M, Gasch O, et al. High vancomycin MICs predict the development of infective endocarditis in patients with catheter-related bacteraemia due to methicillin-resistant Staphylococcus aureus. J Antimicrob Chemother. 2017; 72(7):2102–2109. [CrossRef]
- Huang YT, Hsiao CH, Liao CH, Lee CW, Hsueh PR. Bacteremia and infective endocarditis caused by a non-daptomycin-susceptible, vancomycin-intermediate, and methicillin-resistant Staphylococcus aureus strain in Taiwan. J Clin Microbiol. 2008; 46(3):1132–1136. [CrossRef]
- Wilcox MH, Winstanley TG, Spencer RC, et al. Binding of teicoplanin and vancomycin to polymer surfaces. J Antimicrob Chemother. 1994; 33(3):431–441. [CrossRef]
- Grau S, Gil MJ, Mateu-de Antonio J, Pera M, Marin-Casino M. Antibiotic-lock technique using daptomycin for subcutaneous injection ports in a patient on home parenteral nutrition. J Infect. 2009; 59(4):298–299. [CrossRef]
- Parra-Ruiz J, Bravo-Molina A, Peña-Monje A, Hernández-Quero J. Activity of linezolid and high-dose daptomycin, alone or in combination, in an in vitro model of Staphylococcus aureus biofilm. J Antimicrob Chemother. 2012; 67:2682–2685. [CrossRef]
- Kao TM, Wang JT, Weng CM, Chen YC, Chang SC. In vitro activity of linezolid, tigecycline, and daptomycin on methicillin-resistant Staphylococcus aureus blood isolates from adult patients, 2006-2008: stratified analysis by vancomycin MIC. J Microbiol Immunol Infect. 2011; 44(5):346–351. [CrossRef]
- LaPlante KL, Mermel L a. In vitro activity of daptomycin and vancomycin lock solutions on staphylococcal biofilms in a central venous catheter model. Nephrol Dial Transplant. 2007; 22:2239–2246. [CrossRef]
- Raad I, Hanna H, Jiang Y, et al. Comparative activities of daptomycin, linezolid, and tigecycline against catheter-related methicillin-resistant Staphylococcus bacteremic isolates embedded in biofilm. Antimicrob Agents Chemother. 2007; 51(5):1656–1660. [CrossRef]
- Meije Y, Almirante B, Pozo JL Del, et al. Daptomycin is effective as antibiotic-lock therapy in a model of Staphylococcus aureus catheter-related infection. J Infect. 2014; 68(6):548–552. [CrossRef]
- Rosa, F. G.; Corcione, S.; Di Perri, G.; Scaglione F De. Re-defining tigecycline therapy. New Microbiol. 2015; 38(2):121–136.
- Campos RP, Nascimento MM do, Chula DC, Riella MC. Minocycline-EDTA lock solution prevents catheter-related bacteremia in hemodialysis. J Am Soc Nephrol. 2011; 22(10):1939–45. [CrossRef]
- Chatzinikolaou I, Zipf TF, Hanna H, et al. Minocycline-Ethylenediaminetetraacetate Lock Solution for the Prevention of Implantable Port Infections in Children with Cancer. Clin Infect Dis. 2003; 36(1):116–119. [CrossRef]
- Singh R, Ray P, Das A, Sharma M. Penetration of antibiotics through Staphylococcus aureus and Staphylococcus epidermidis biofilms. J Antimicrob Chemother. 2010; 65(9):1955–1958. [CrossRef]
Figure 1.
Study flow diagram.
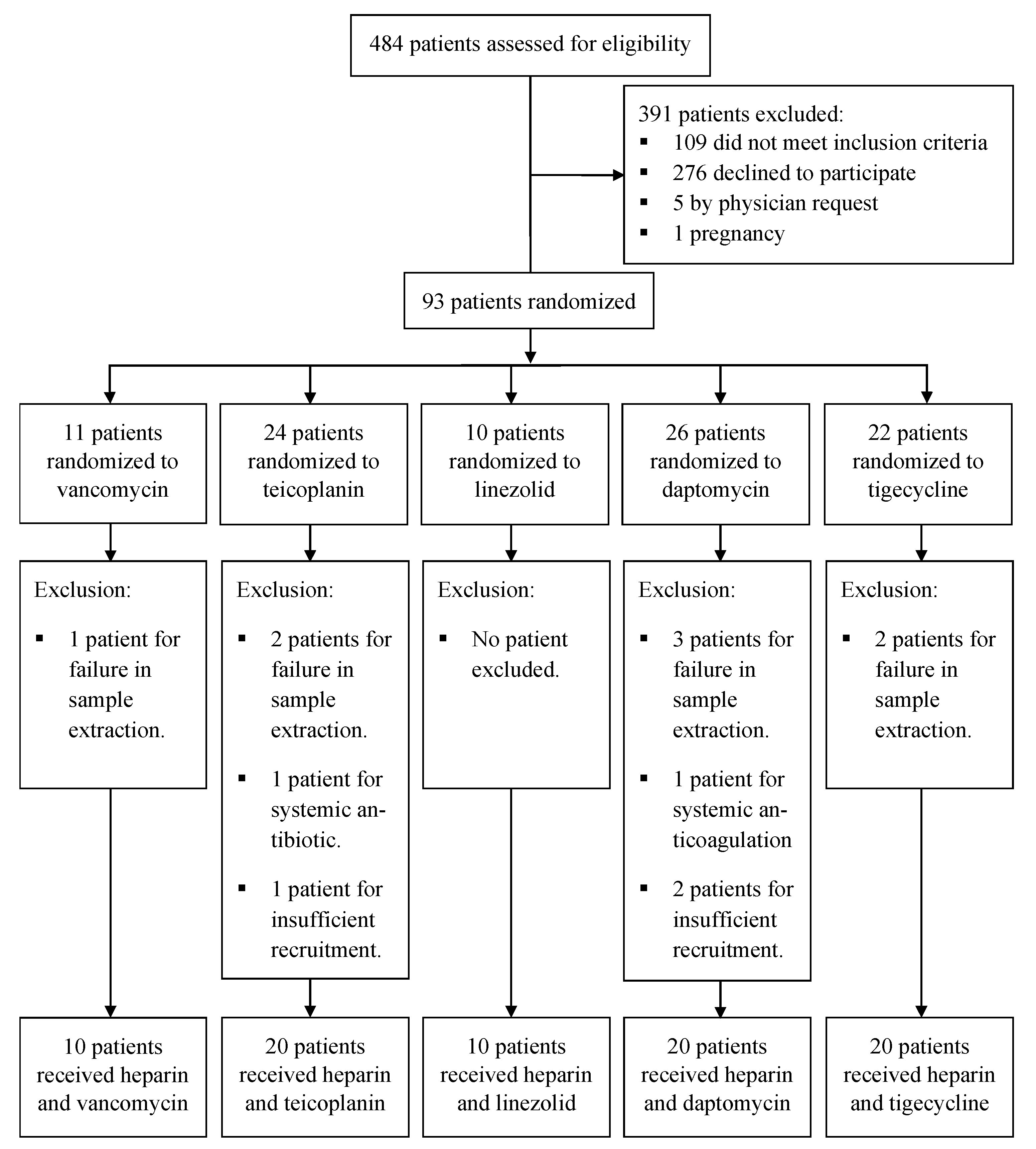

Table 1.
Baseline characteristics of patients by treatment group.
| Characteristic | Treatment groups | ||||
| Vancomycin | Teicoplanin | Linezolid | Daptomycin | Tigecycline | |
| Sex [no. (%) of patients] | |||||
| Male | 7 (70) | 12 (60) | 6 (60) | 14 (70) | 8 (40) |
| Female | 3 (30) | 8 (40) | 4 (40) | 6 (30) | 12 (60) |
| Age | |||||
| Mean (yr) | 58 | 57.8 | 62.3 | 48 | 55.2 |
| Median (yr) | 61.8 | 62.9 | 64.2 | 52.7 | 55.1 |
| Underlying malignancy [no. (%) of patients] | |||||
| Solid neoplasia | 10 (100) | 19 (95) | 7 (70) | 15 (75) | 17 (85) |
| Hematologic | 0 (0) | 1 (5) | 3 (30) | 5 (25) | 3 (15) |
| Site of port implantation [no. (%) of patients] | |||||
| Right subclavian vein | 6 (60) | 15 (75) | 4 (40) | 9 (45) | 9 (45) |
| Right jugular vein | 2 (20) | 3 (15) | 4 (40) | 4 (20) | 4 (20) |
| Other locations | 2 (20) | 2 (20) | 2 (20) | 7 (35) | 7 (35) |
| Duration of catheterization prior to randomization (days) | |||||
| Mean | 21.6 | 42.1 | 11.4 | 39.5 | 42.2 |
| Median | 12.6 | 122.5 | 21.1 | 83 | 35.7 |
Table 2.
Antimicrobial concentration recovered from lock solutions after the time of dwelling.
| Antimicrobial concentration administered | Antimicrobial concentration recovered after dwelling time (mg/ml) | |||||||
| 1 Day | 3 Days | 5 Days | 7 Days | |||||
| media (median) | Pvaluea | media (median) | Pvaluea | media (median) | Pvaluea | Media (median) | Pvaluea | |
| Vancomycin 2 mg/ml |
1548.0 (1537.5) | 0.80 | 646.7 (461.8) | 0.04 | * | * | * | * |
| Teicoplanin 10 mg/ml |
6755.7 (7183.4) | 0.04 | 6201.9 (5684.4) | 0.04 | 7566.6 (7677.1) | 0.13 | 10541.2 (9904.6) | 0.89 |
| Linezolid 1.8 mg/ml |
886.1 (1032.5) | 0.04 | 669.1 (727) | 0.04 | * | * | * | * |
| Daptomycin 5 mg/ml |
4029.3 (4385.8) | 0.04 | 2788.7 (2860) | 0.04 | 2697.6 (2814.9) | 0.04 | 2900.8 (2729.7) | 0.04 |
| Tigecycline 4.5 mg/ml |
2405.5 (2415.9) | 0.04 | 1441.8 (1402) | 0.04 | 1092 (1180.4) | 0.04 | 1101.1 (1062.6) | 0.04 |
| a p values are from the Wilcoxon test. | ||||||||
| * The vancomycin and linezolid groups stopped after 3 days of dwelling time. | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



