Submitted:
03 January 2026
Posted:
05 January 2026
You are already at the latest version
Abstract
Background: Cocaine is the second most widely abused illicit substance worldwide and exerts potent sympathomimetic effects by inhibiting the reuptake of norepinephrine, dopamine, and serotonin. While cardiovascular and neurological complications are well recognized, gastrointestinal (GI) manifestations are increasingly reported. These arise from multifactorial mechanisms including vasospasm, endothelial dysfunction, thrombosis, ischemia, and direct mucosal toxicity, often with severe clinical consequences. Objective: This narrative review summarizes the mechanisms, pharmacokinetics, pharmacodynamics, routes of use, and spectrum of GI complications associated with cocaine exposure, with emphasis on ischemic, ulcerative, hemorrhagic, inflammatory, fibrotic, hepatobiliary, and pancreatic sequelae. Methods: We reviewed published case reports, cohort studies, and systematic reviews indexed in PubMed and major databases up to 2023. Articles focusing on pathophysiology, clinical presentation, diagnostic features, and outcomes of cocaine-induced GI disorders were included. References with available abstracts were prioritized. Results: Cocaine induces GI injury through vasoconstriction, pro-thrombotic effects, microvascular dysfunction, and direct cytotoxicity. Pharmacokinetically, cocaine demonstrates rapid absorption via intranasal, inhalational, or intravenous routes, with hepatic metabolism and elimination through benzoylecgonine and ecgonine methyl ester. Clinical gastrointestinal complications include: • Ischemic/Vascular: Mesenteric ischemia/infarction, colonic ischemia, ischemic/ hemorrhagic colitis, Vascular thrombosis • Ulcerative/Perforative: Peptic ulcer disease, Gastric, duodenal, small and large bowel perforations • Inflammatory/Fibrotic: Enteritis, enterocolitis, strictures, retroperitoneal fibrosis • Hepatobiliary & Pancreatic • Splenic • Other: GAVE, IBD mimic Rare complications such as intussusception and small bowel hematomas have also been described. Cocaine adulteration with levamisole increases risk of agranulocytosis and ischemic necrosis. Mortality is particularly high in cases of acute mesenteric ischemia, infarction, and fulminant ischemic colitis. Conclusion: Cocaine use is a significant and under-recognized contributor to severe GI morbidity and mortality. Its complications span from ischemia and perforation to hepatopancreatic injury, often requiring emergent intervention. Clinicians should maintain high suspicion for cocaine-related GI disease in young patients presenting with abdominal pain or ischemic features, as early recognition and management may improve outcomes.
Keywords:
cocaine
; gastrointestinal complications
; ischemic colitis
; mesenteric ischemia
; bowel perforation
; pancreatitis
; retroperitoneal fibrosis
; hemorrhage
1. Introduction
Cocaine is one of the most consumed stimulants throughout the world, as official sources report [1]. Cocaine, a potent sympathomimetic, exerts profound systemic vasoconstrictive effects by blocking presynaptic reuptake of norepinephrine, dopamine, and serotonin. The latest edition of the European Monitoring Centre for Drug and Drug Addiction (EMCDDA) Drug Report states that it remains the second most abused substance in the EU, second only to cannabinoid. According to the world drug report, 0.4% of the global population between 15-64 reports cocaine use in 2019, corresponding to approximately 20 million people [1]. In the US, 1 in 5 overdose deaths were due to cocaine with over 5 million americans reporting cocaine use which is around 2% of the population. [2] While its cardiovascular and neurological sequelae are well-recognized, gastrointestinal (GI) complications are increasingly described, particularly within the lower GI tract. These manifestations arise from a spectrum of mechanisms including vasospasm, endothelial injury, thrombosis, ischemia, and direct mucosal toxicity.
Mechanism of Action:
Cocaine is a naturally occurring sympathomimetic tropane alkaloid derived from the leaves of Erythroxylon coca, which has been used by South American locals for millennia [1]. Cocaine was first isolated in 1800s and at the time considered safe and was used in toothache drops, nausea pills and as energy tonics. Cocaine exerts its effects by blocking the reuptake of catecholamines, such as norepinephrine and dopamine, at presynaptic nerve terminals. This leads to an accumulation of these neurotransmitters at the postsynaptic receptors, resulting in a state of heightened sympathetic nervous system activity. This sympathetic overdrive is responsible for many of the drug's systemic effects, including tachycardia, hypertension, and vasoconstriction.
While its effect on neurotransmitters are the most studies mechanism, it affects multiple other pathway and are summarized below,
- Neurotransmitter reuptake inhibition: Cocaine blocks presynaptic reuptake of dopamine, norepinephrine, and serotonin by inhibiting their transporters (DAT, NET, SERT) [1].
Figure 1.
Effect on cocaine on synaptic terminals.
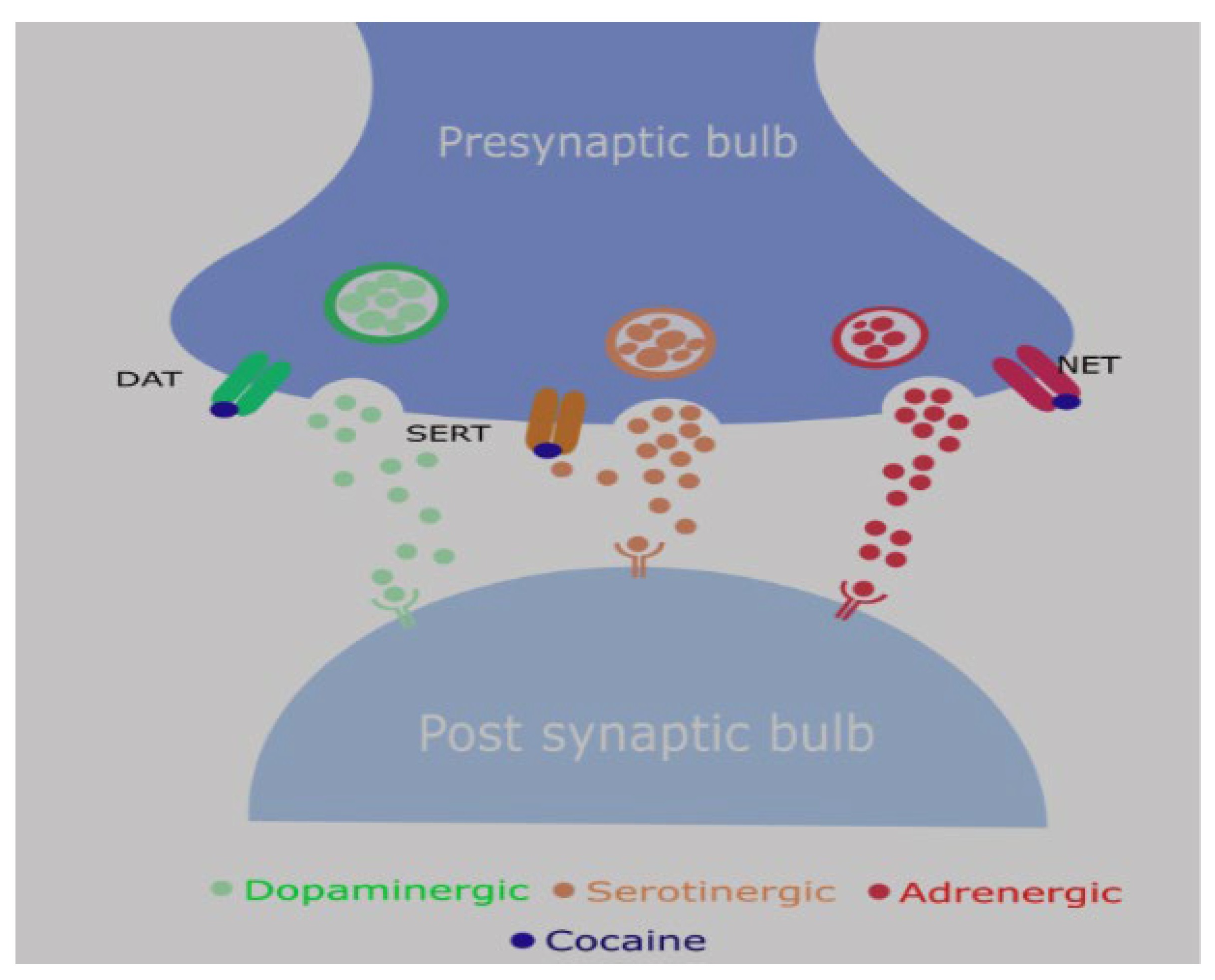
Sympathomimetic effects: Elevated synaptic norepinephrine → vasoconstriction, hypertension, tachycardia.
- Reward pathway: Increased dopamine in the mesolimbic system due to blockade of dopamine transporter → euphoric rush (addictive potential) followed by dysphoric crash
- Local anesthetic effect: Sodium channel blockade in excitable membranes → used historically in ophthalmology and ENT.
Citations for the above pathways
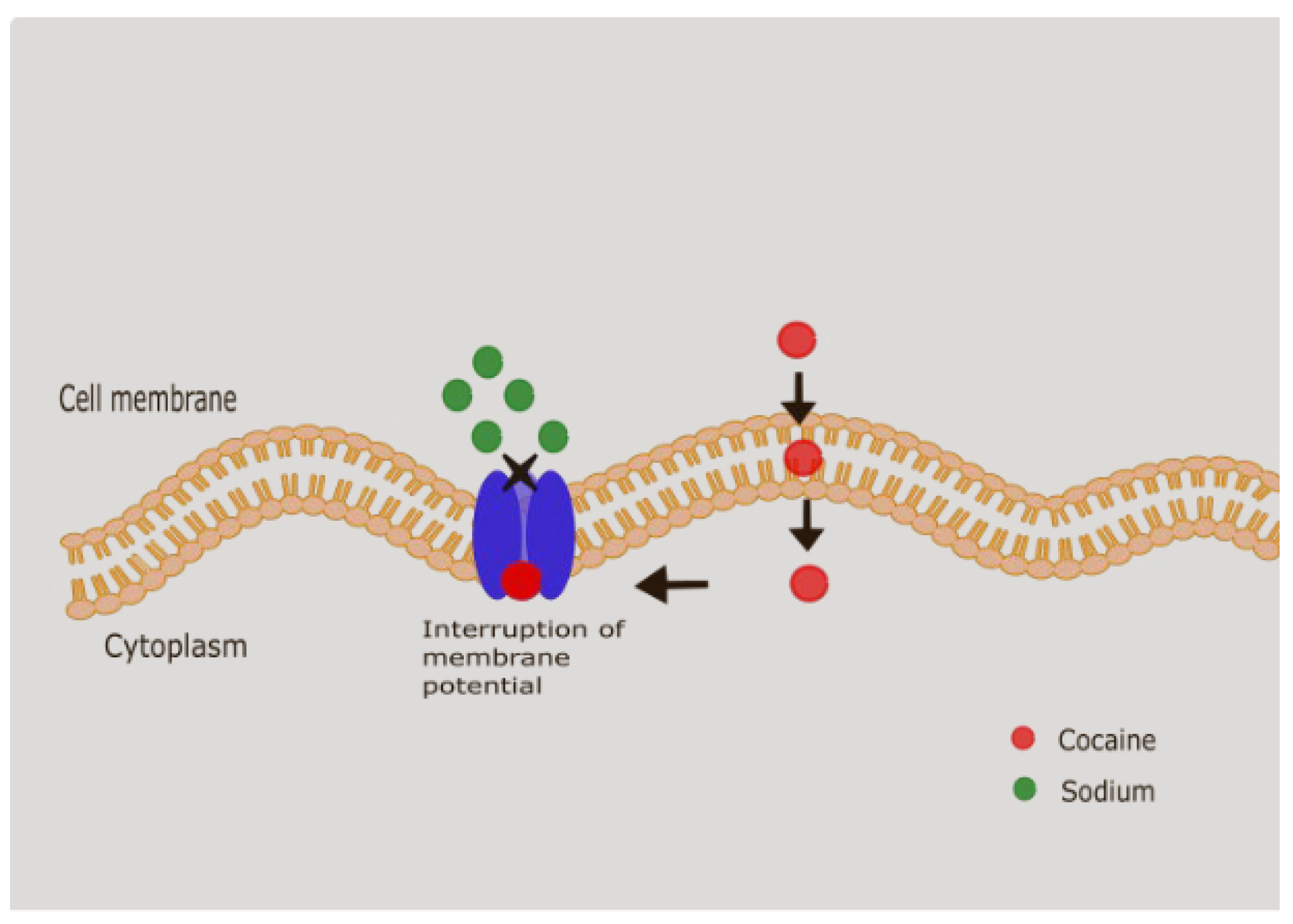
Figure 2.
Cocaine and its local anesthetic effect.
- Cocaine can also target NMDA, sigma and kappa opioid receptors. The clinical implications of these are still being explored.
- Thrombosis and Platelet Aggregation: It activates platelets by increasing the expression of platelet factor 4, thromboglobulin B, and P-selectin. It has been shown to induce endothelial dysfunction by increasing endothelin-1 expression with concurrent decrease in nitric oxide [3]. It also increases the levels of fibrinogen, von Willebrand factor, and plasminogen activator inhibitor-1, and decreasing the levels of protein C and antithrombin III. These changes in the coagulation and fibrinolytic systems create a pro-thrombotic state, which increases the risk of thrombosis [4,5]. It can also increase the sensitivity of platelets to other agonists, such as ADP and collagen [4].
- Oxidative Stress: Cocaine has been shown to increase the production of reactive oxygen species (ROS) in a variety of cell types, including hepatocytes and endothelial cells. This increase in oxidative stress can lead to cellular damage and death, and it may play a role in the direct cytotoxic effects of the drug.
- Hepatotoxic Metabolites: Cocaine is metabolized in the liver by cytochrome P450 enzymes, and some of its metabolites, such as norcocaine and cocaethylene, are more hepatotoxic than the parent compound. These metabolites can cause direct injury to the hepatocytes, leading to a spectrum of liver injury, from mild hepatitis to acute liver failure.
Routes/Modalities of Use
It is available in two forms: cocaine hydrochloride and cocaine free base.
- Intranasal insufflation (“snorting”)
- Common recreational route.
- Onset: 5–10 min; Duration: 30–60 min.
- 2.
- Smoking (crack cocaine)
- Rapid pulmonary absorption.
- Onset: seconds; Duration: 5–15 min.
- Intense “rush” but short-lived → high addictive potential.
- 3.
- Intravenous injection
- Immediate bioavailability, peak plasma concentration within seconds.
- High risk of overdose, infection, and vascular injury.
- 4.
- Oral ingestion
- Less common recreationally; sometimes seen in “body packers/mules.”
- Erratic absorption due to first-pass metabolism; slower onset.
- 5.
- Rectal (“plugging”) or vaginal use
- Reported in some cases.
- Leads to unpredictable absorption, sometimes severe toxicity.
Pharmacokinetics:
-
Absorption:
- ○
- Inhalation/smoking (crack) → rapid absorption via pulmonary circulation.
- ○
- Intranasal insufflation → slower absorption, bioavailability ~30–60%.
- ○
- Intravenous injection → immediate systemic availability.
- ○
- Oral/rectal → erratic absorption due to first-pass metabolism. [6]
- Distribution: Highly lipophilic → rapidly crosses blood–brain barrier. Volume of distribution ~1–3 L/kg.
-
Metabolism:
- ○
- Primarily in liver via plasma and hepatic esterases.
- ○
- Major metabolites: benzoylecgonine (inactive, urinary marker), ecgonine methyl ester [6].
- ○
- With alcohol co-use → cocaethylene forms (longer half-life, more cardiotoxic).
-
Elimination:
- ○
- Plasma half-life: ~40 to 90 mins. [6]
- ○
- Metabolites excreted in urine; detectable for 2–3 days, longer in chronic users.
Pharmacodynamics:
- CNS effects: Euphoria, increased alertness, hypervigilance, decreased fatigue, but also anxiety, agitation, and seizures at high doses. The intense vasoconstriction caused by cocaine can cause ischemic infarctions, intracerebral and subarachnoid hemorrhage, movement disorders (crack dancing) and seizures (by lowering seizure potential). [7]
- Cardiovascular effects: Tachycardia, hypertension, coronary vasospasm, arrhythmias, myocardial ischemia/infarction.
- GI effects: Mesenteric vasoconstriction → ischemia, infarction, perforation,small bowel hematomas, intussusception, hemorrhage, acute pancreatitis.
- Other systemic effects: Hyperthermia, rhabdomyolysis, renal injury.
Gastrointestinal Complications of Cocaine Use
While the cardiovascular and neurological consequences of cocaine are well established, its gastrointestinal (GI) manifestations are increasingly recognized yet often underappreciated. Cocaine-induced GI injury arises from a combination of intense mesenteric vasoconstriction, endothelial dysfunction, microvascular thrombosis, oxidative stress, and direct mucosal toxicity. These mechanisms create a spectrum of pathology ranging from transient ischemia to full-thickness infarction and perforation. Moreover, chronic use predisposes to fibrotic strictures, inflammatory enterocolitis, hepatotoxicity, and pancreatic injury.
They can be summarized as
- Ischemic/Vascular: Mesenteric ischemia/infarction, colonic ischemia, ischemic/ hemorrhagic colitis, Vascular thrombosis
- Ulcerative/Perforative: Peptic ulcer disease, Gastric, duodenal, small and large bowel perforations
- Inflammatory/Fibrotic: Enteritis, enterocolitis, strictures, retroperitoneal fibrosis
- Hepatobiliary & Pancreatic
- Splenic
- Other: GAVE, IBD mimic
- ▪
- Ischemic/ Vascular
Cocaine's chronic effects on the vessel consist of repeated endothelial damage leading to premature and severe atherosclerosis in various organs [5]. It releases endothelin-1 which leads to potent vasoconstriction and this along with release of fibrinogen and vWF lead to platelet aggregation and clot formation, exacerbating the ischemic injury and increasing the likelihood of tissue necrosis [8,9]. Kaufman et al demonstrated that cocaine induces splenic constriction and increases the hematocrit and hemoglobin level, This along with blood flow reduction due to vasoconstriction and cocaine’s prothrombotic effects can worsen the hypoperfusion and ischemia [10].
Cocaine's ability to induce intense and prolonged vasospasm in the mesenteric arteries leads to a critical reduction in blood flow to the intestines, causing a spectrum of ischemic damage that can range from transient mucosal injury to full-thickness bowel infarction and gangrene . This ischemic insult can affect any part of the GI tract, from the esophagus to the rectum, with certain areas being more susceptible due to their vascular anatomy. Wattoo et al in their case series reported that cocaine induced ischemia affects small intestine more than the large intestine [8]. The clinical consequences of this ischemia are severe and include mesenteric ischemia, ischemic colitis, and, in extreme cases, massive pan-gastrointestinal ischemia. Intestinal ischemia occurs when there is 75% reduction in intestinal blood flow for more than 12 hours [2]. The symptoms of ischemia starts 1 hours to 2 days from drug use. Sometimes the symptoms are delayed for 72 hours [11].
The clinical presentation can be acute, with sudden onset of severe abdominal pain, or chronic, with recurrent episodes of postprandial pain and weight loss. The ischemic process can progress to bowel infarction and gangrene if the blood supply is not restored, leading to a life-threatening condition that requires emergency surgical intervention. The incidence of these complications is likely underreported, as the symptoms can be non-specific and may be attributed to other causes, especially in a population with a high prevalence of polysubstance abuse.
Acute Mesenteric Ischemia
Acute mesenteric ischemia (AMI) is a medical emergency that can be precipitated by cocaine use. Patients typically present with sudden, severe abdominal pain that is often out of proportion to the physical findings on examination. This "pain out of proportion" is a classic sign of AMI and should raise a high index of suspicion in any cocaine user presenting with acute abdominal symptoms.
Angel at al described a case of cocaine enteropathy diagnosed by characteristic CT findings of small bowel edema and luminal dilatation, mucosal enhancement, venous engorgement, free fluid with symptoms resolution with supportive therapy [12]. Cocaine induced vascular thrombosis leading to acute mesenteric ischemia has been reported in a few case reports. Cocaine induced thrombosis preferentially affects arteries more than the veins [13]. Edgecombe et al described a case of fatal SMA thrombosis in a chronic cocaine user [14].
Chronic Mesenteric Ischemia
Chronic mesenteric ischemia (CMI), also known as intestinal angina, is a less common but equally debilitating complication of long-term cocaine use. In contrast to the acute form, CMI is characterized by recurrent episodes of abdominal pain, typically occurring after meals (postprandial angina), as the increased demand for blood flow to the intestines during digestion cannot be met due to the chronic vasoconstriction and potential structural changes in the mesenteric arteries. Myers et al described a case of chronic mesenteric ischemia due to SMA thrombosis managed successfully with visceral revascularization [15].
Ischemic Colitis
Ischemic colitis is a specific form of intestinal ischemia that primarily affects the large intestine. It is one of the more common GI complications of cocaine use and can present with a wide range of severity, from a self-limited, transient colitis to a fulminant, life-threatening condition . The pathophysiology is similar to that of mesenteric ischemia, with cocaine-induced vasoconstriction leading to a reduction in blood flow to the colonic mucosa. The colon is particularly susceptible to ischemic injury due to its relatively low blood flow and the presence of "watershed" areas, such as the splenic flexure and the rectosigmoid junction, which are supplied by the terminal branches of the major arteries and have limited collateral circulation . Elramah et al in their hybrid cohort/case control study reported that compared to non cocaine ischemic colitis , cocaine cohort has higher mortality rate (OR 5.77) with higher need for surgical intervention [16].
Niazi et al in their retrospective study, described the spectrum of ischemic colitis in Cocaine users. Of the total 7 patients 2 had acute presentation and 5 were subacute to chronic. Acute phase in characterized by regenerative activity in the crypts and at the surface with chronic phase characterized by distorted and regenerative crypts with fibrosis [17].
Acute Ischemic Colitis
Acute ischemic colitis is the most common presentation of cocaine-induced colonic injury. It is characterized by a sudden onset of symptoms, including crampy abdominal pain, urgency to defecate, and the passage of bloody or maroon-colored stool . The ischemic injury is typically confined to the mucosa and submucosa, and in most cases, it is transient and self-limiting. However, in a subset of patients, the ischemic process can be more severe, leading to transmural involvement, necrosis, and perforation . The mortality rate for cocaine-induced ischemic colitis has been reported to be as high as 26%, which is significantly higher than that for ischemic colitis from other causes [16].
Hemorrhagic Ischemic Colitis
Hemorrhagic ischemic colitis is a more severe form of ischemic colitis, characterized by significant bleeding from the ischemic and ulcerated colonic mucosa. The pathophysiology involves vasospasm causing hypoperfusion and hypoxia leading to necrosis of mucosal villi followed by transmural, mural or mucosal infarction. The sloughing of infarcted mucosa can present with rectal bleeding [2]. Patients with this condition often present with large-volume bloody diarrhea, which can lead to hemodynamic instability and the need for blood transfusions . The diagnosis is confirmed by colonoscopy, which reveals a friable, hemorrhagic, and ulcerated mucosa. Treatment varies from conservative management to surgical resection depending on the severity of the ischemia [18].
Histologically, cocaine-associated colitis presents with oedema, congestion, inflammatory infiltrate in the lamina propria, loss of goblet cells and submucosal haemorrhage. Deivasigamani et al described a case of ischemic hemorrhagoc colitis with these hisological findings along with colonoscopic features of diffuse small bowel ischemia and inflammation extending from ileum to ascending colon and was treated effectively with conservative management [19].
Cocaine-Induced Enterocolitis
Cocaine-induced enterocolitis is a condition characterized by inflammation of both the small intestine and the colon. The pathophysiology is similar to that of enteritis, involving chronic ischemia and inflammation. The clinical presentation can be variable, with symptoms ranging from mild abdominal discomfort to severe, bloody diarrhea. The diagnosis is often made by endoscopy and biopsy, which can reveal inflammatory changes consistent with ischemia. The treatment is supportive, with a focus on the cessation of cocaine use. Fishel et al described a case of cocaine colitis in a patient presenting with lower abdominal pain and bloody diarrhea on whom the histopathological findings were consistent with mixed pattern of pseudomembranous enterocolitis and ischemic colitis [20]. This peculiar findings were not described ever since.
Ellis et al in their retroscpective analysis on 2002, showed that most patients with cocaine induced enterocolitis where treated conservatively but those develop peritonitis requiring surgery had 50% mortality. The anatomical location varied from right colon (46%), transverse colon (20%), Descending colon (18%), Sigmoid colon (24%) and rectum in 3.6%. The mortality with conservative management is 9% in their study. This relative rectal sparing is similar to other studies and may be due to rich arterial supply to rectum [17].
Ischemic Injury to the Upper GI Tract
While ischemic colitis is a more commonly recognized complication, cocaine can also cause significant ischemic injury to the upper GI tract, including the esophagus, stomach, and duodenum. The same vasoconstrictive mechanisms that affect the mesenteric arteries and colonic vessels also impact the blood supply to these organs, leading to a range of conditions from mild ischemia to full-thickness necrosis and perforation.
Acute Esophageal Necrosis (Black Esophagus)
Acute esophageal necrosis (AEN), also known as "black esophagus," is a rare but potentially fatal condition that has been associated with cocaine use . It is characterized by the circumferential black discoloration of the distal esophagus, which is typically seen on endoscopy . The pathogenesis is thought to be multifactorial, involving a combination of ischemia from cocaine-induced vasoconstriction and direct mucosal injury from gastric acid reflux, often exacerbated by vomiting . The distal esophagus is particularly vulnerable due to its relatively weaker blood supply . Patients typically present with upper GI bleeding (hematemesis) and may have a history of heavy cocaine and alcohol use . The mortality rate is high, around 30-50%, often due to the serious comorbid conditions that predispose patients to this condition . the main treatment option is conservative with strict NPO for 24 hours and PPIs/ sucralfate to enable healing. Around 7% of the patients develop esophageal perforation. Around 4 cases of acute esophageal necrosis due to cocaine were described [21].
Massive Pan-Gastrointestinal Ischemia
In the most severe cases, cocaine use can lead to a massive, pan-gastrointestinal ischemic injury, affecting multiple segments of the GI tract simultaneously. This is a rare but catastrophic event with an extremely high mortality rate. The underlying mechanism is likely a systemic and profound vasoconstrictive response that affects the entire splanchnic circulation. The high mortality associated with this condition is due to the extensive nature of the injury, the difficulty in diagnosis, and the challenges in managing such widespread ischemia. Bathobakae et al reported a combined esophageal, gastric and small bowel necrosis in a patient with chronic intranasal cocaine use [22]. Similarly Naidu et al reported a case of gastric ulcer, duodenal ulcer and stenosis with mesenteric ischemia, jejunal/ileal perforation requiring surgical exploration and embolization of gastroduodenal artery in an incarcerated male with 15 years of cocaine use [23].
Bowel Infarction and Gangrene
Bowel infarction and gangrene represent the most severe and life-threatening consequences of cocaine-induced mesenteric ischemia. When the ischemic insult is severe and prolonged, it can lead to transmural necrosis of the intestinal wall, resulting in bowel infarction . This process is often irreversible and can rapidly progress to gangrene, where the affected bowel segment becomes necrotic and infected. The clinical presentation is that of an acute abdomen, with severe abdominal pain, fever, signs of peritonitis (such as rebound tenderness and guarding), and septic shock . Histopathological findings as described by Martinex et al include transmural necrosis and necrotizing phlebitis [24]. The presence of pneumatosis intestinalis (air within the bowel wall) on imaging is a ominous sign that suggests transmural infarction. Bowel infarction and gangrene are surgical emergencies that require immediate laparotomy and resection of the necrotic bowel . Despite aggressive surgical management, the mortality rate for this condition remains high, particularly in the setting of cocaine use, where the underlying vasoconstrictive effects can continue to compromise the blood supply to the remaining bowel . The high mortality underscores the critical importance of early diagnosis and intervention to prevent the progression from ischemia to infarction and gangrene. Khan et al reported a case of levamisole induced agranulocytosis and bowel ischemia in a patient with rectal cocaine abuse. As of July 2009, the Drug Enforcement Administration (DEA) of the US Department of Justice isolated levamisole in up to 69% of cocaine coming to the United States [25]. Levamisole is a known adulterant of cocaine and is notorious to cause agranulocytosis [3,25]. This increases the risk of enterocolitis and bowel necrosis in patients with levamisole adulterated cocaine use.
2. Ulcerative and Perforative Complications
In addition to its ischemic effects, cocaine is also implicated in the development of a range of ulcerative and perforative complications throughout the GI tract. These conditions are thought to arise from a combination of factors, including direct mucosal injury from cocaine and its adulterants, ischemia from vasoconstriction, and increased gastric acid secretion. Gastroduodenal perforations associated with crack cocaine use most often affect the first portion of the duodenum or pylorus [26].
Gastroduodenal Perforation
Gastroduodenal perforation is one of the most common and serious GI complications of cocaine use, particularly with the smoked form, crack cocaine. The pathological relationship between crack and gastroduodenal perforations were under scrutiny from 1989 when Lee et al published a case series on this very presentation [27]. The pathophysiology is multifactorial, involving ischemia from vasoconstriction, direct chemical injury to the mucosa, and potentially increased intragastric pressure from altered motility and air swallowing associated with smoking crack . The clinical presentation is typically that of an acute abdomen, with sudden onset of severe, sharp epigastric pain that may radiate to the back or shoulder . Sharma et al in their retrospective observation study of patients presenting with acute abdomen showed that patient with cocaine use has higher incidence of duodenal perforations compared to non-users [28].
Gastric Perforation
Prepyloric perforation, occurring in the gastric antrum just proximal to the pylorus, is a particularly common site for cocaine-induced perforations. In one study, prepyloric ulcers accounted for 42% of all gastric perforations in patients with a history of cocaine use [29]. The reasons for this predilection are not entirely clear. Patients present with severe upper abdominal pain, and the diagnosis is often confirmed by the presence of free intraperitoneal air on plain abdominal X-rays or CT scans. Surgical repair, either by open laparotomy or laparoscopy, is the standard of care. Other sites of gastric include Incisura and gastric body [26,30,31]. Schuster et al studied the effect of surgical interventions on cocaine induced gastric perforation which showed that antiulcer procedures were associated with no occurrence whereas omental patch closure results in 50% recurrence rate [32]. In a retrospective study about 16% of patients with perforated PUD had cocaine exposure [29].
Duodenal Perforation
Duodenal perforation is another common manifestation of cocaine-induced GI injury. The first portion of the duodenum is the most frequently affected site. The clinical presentation and management are similar to that of prepyloric perforation, with patients presenting with an acute abdomen and requiring emergent surgical intervention. The high incidence of both prepyloric and duodenal perforations in cocaine users suggests a common underlying pathophysiologic mechanism, likely related to the intense vasoconstriction and ischemia that affects the gastroduodenal region. Hurtado et al in their case report described a case of combined pyloric stenosis with prepyloric and duodenal perforation [33].
Small Bowel Perforation
Small bowel perforation is a rare but serious complication of cocaine abuse . It is typically a result of severe, prolonged ischemia of the small intestine, leading to gangrene and perforation. The distal ileum is the most common site of involvement [19]. The management is surgical, with resection of the affected segment of the small bowel.
Colonic Perforation
Colonic perforation can also occur as a result of cocaine-induced ischemic colitis. The perforation is typically a result of transmural infarction of the colon, which then ruptures. The management is surgical, with resection of the affected segment of the colon. Mabrouk et al described a case of sigmoid perforation requiring a colostomy and peritoneal lavage [34].
3. Fibrotic and Obstructive Conditions
Chronic inflammation and ischemia in the GI tract can lead to the development of fibrosis, which is the formation of excess fibrous connective tissue. This fibrosis can cause strictures (narrowing) of the bowel lumen, leading to obstruction.
Age , Sex and any other relevant comparable columns can be added for the below case reports cited
| Study | Findings |
| Silva et al [35] | esophageal stricture following an episode of gastric ulcer |
| Hurtado et al [33] | combined pyloric stenosis with prepyloric and duodenal perforation. |
| Aldana et al [36] | Gastric outlet obstruction/ duodenal stenosis due to chronic cocaine abuse requiring roux-en-Y anastomosis. |
| Perysinakis et al [37] | chronic bowel ischemia manifesting as small bowel obstruction due to extensive intestinal wall fibrosis. |
| Ruiz-tovar et al [38] | sigmoid colon stenosis due to chronic ischemic colitis. |
4. Hepatobiliary and Pancreatic Complications
Cocaine use can also have significant effects on the hepatobiliary and pancreatic systems. The drug's vasoconstrictive properties can lead to ischemic injury to the liver and pancreas, and its metabolites can be directly toxic to these organs.
Pancreatic Injury
The pancreas is a highly vascular organ that is susceptible to the vasoconstrictive effects of cocaine. Cocaine-induced pancreatitis is a well-recognized complication of the drug, and it can range from a mild, self-limiting illness to a severe, life-threatening condition with necrosis and multi-organ failure.
Acute Pancreatitis
Cocaine associated acute pancreatitis is rarely reported. Only 7 published case reports was available as of 2021 [39]. Bernad et al. first recognized cocaine-associated acute pancreatitis in 1990. It is postulated that the pathophysiological changes causing cocaine-induced pancreatitis involve mechanisms such as vasoconstriction and thrombotic microangiopathy [39].
Liver Injury
The liver is the primary site of cocaine metabolism, and it is therefore susceptible to the toxic effects of the drug and its metabolites. Cocaine-induced liver injury can range from mild, asymptomatic elevations in liver enzymes to severe, life-threatening acute liver failure. In 1987, Perino and coworkers reported the first case of human cocaine-mediated hepatotoxicity, showing mild diffuse fatty infiltration, and marked peri- portal (zone 1) inflammation and necrosis. The histopathological findings in subsequent studies were dissimilar to those from the first report, with predominant perivenular (zone 3) and midzonal (zone 2) necrosis. In contrast to other xenobiotics, cocaine was determined to be able to induce differential hepatic zonal necrosis, dependent on dose, sex and enzyme induction and inhibition [40].
- Cocaine is N-demethylated to norcocaine (NCOC) in liver and kidney.
- NCOC undergoes further oxidation to N-OH-NCOC and NCOC-NO·.
-
These metabolites:
- ○
- Enter redox cycling, generating ROS → oxidative stress → cell death.
- ○
- Or form highly reactive ions that bind irreversibly to proteins → hepatocyte death.
Mitochondrial Involvement
- Mitochondria might be the major target of cocaine hepatotoxicity.
-
Cocaine can mediate mitochondrial cytotoxicity by the following mechanism
- ○
- Inhibiting mitochondrial respiration → ATP depletion → necrosis.
- ○
- ROS generation → oxidative stress.
- ○
- Activation of apoptosis (caspase-3 activation, cytochrome c release).
Alternatively, the cellular cytotoxicity may be mediated by, endoplasmic reticulum oxidative metabolism. Carpano et al described a correlation between cocaine induced hepatotoxity and heat shock protein in the hepatocytes, but further investigations is needed for evaluating HSP as biochemical marker for cocaine induced hepatotoxicity [41].
Cocaine is metabolized in the liver by esterases and cytochrome P450 enzymes, and some of its metabolites, such as norcocaine and cocaethylene (a metabolite formed when cocaine and alcohol are used together), are more hepatotoxic than the parent compound. Cocaethylene is a cocaine metabolite produced in the liver when cocaine and ethanol (alcohol) are co-ingested, and is capable of enhancing ischemic tissue damage (Hearn et al., 1991). Cocaethylene has a half-life of 2–4 hr and an LD50 of 60–68.8 mg/kg as compared to 93.0 mg/kg for cocaine, therefore its potency and potential for toxicity is greater than cocaine itself [42].These metabolites can cause direct injury to the hepatocytes, leading to a spectrum of liver injury, from mild hepatitis to acute liver failure. The management is typically supportive, with cessation of cocaine and alcohol use being the most important intervention.
Tamargo et al performed a cross sectional analysis if the Miami adult studies on HI cohort (MASH) which revelaed that in concomitant cocaine and alcohol users in whom COC+/CE+ was positive, there was 4.97 OR of liver fibrosis, compared to 1.3 OR in only cocaine user compared to coaine non user. It is possible that cocaine use may increase the hepatotoxicity of alcohol by altering the CYP450 activity [43].
Acute Hepatitis
Acute hepatitis is a common complication of cocaine use. The pathophysiology is thought to be multifactorial, involving a combination of ischemia from vasoconstriction, direct cytotoxic effects of cocaine and its metabolites on the hepatocytes, and immune-mediated injury.
5. Splenic Complications
While not part of the GI tract proper, the spleen is an intra-abdominal organ that is frequently affected by the same vasoconstrictive and thrombotic processes that damage the bowel. Cocaine use has been associated with a range of splenic pathologies, including infarction, hematoma, and atraumatic rupture. These conditions can present with acute abdominal pain and can be life-threatening if not recognized and managed promptly. The spleen's rich blood supply and its role in the reticuloendothelial system make it susceptible to the effects of circulating vasoactive substances like cocaine.
Cocaine-induced splenic injury is a rare phenomenon that can manifest as splenic infarct, hematoma, or rupture. First reported by Novielle and Chambers in 1991,these injuries include vasospasm-induced splenic infarct or hematoma(s) with or without rupture [46]. Followed by homler et al who described a case of atraumatic splenic hematoma without rupture or hemorrhage indicating a contained bleed [47]. The majority of these reported cases have an underlying hemoglobinopathy. Although the mechanism for these injuries in not known, cocaine use has been shown to cause up to 20% transient reduction of splenic volume through vasoconstriction [10]. Ballard et al described a case of combined atraumatic splenic laceration/ hemoperitoneum and ileal volvus after an IV cocaine use [48]. Bruno et al described a case of splenic subcapsular hematoma and spontaneous hemoperitoneum in a 23-year-old cocaine user [49]. Ramos et al had a similar 23-year-old with atraumatic splenic laceration and hemoperitoneum following intranasal cocaine use [50]. Karthik et al described a case of splenic hemorrhage in a chronic cocaine user [51]. Though all of these cases are managed surgically, Azar et al described a case of splenic hemorrhage which was managed conservatively owing to hemodynamically stable presentation [52]. Khan et al described another such case of splenic hemorrhage and hemoperitoneum managed non surgically with transcatheter splenic artery embolization (TSAE) [53].
6. Other Complications
GAVE (Gastric Antral Vascular Ectasia)
Gastric antral vascular ectasia (GAVE), also known as “Watermelon stomach”, is a rare cause of upper gastrointestinal bleeding (UGIB). It was first reported in 1953. It commonly manifests as chronic anemia with endoscopic appearance of linear, erythematous strips of ectatic vessels radiating from the pylorus to the antrum. Kravchenko described a case of UGI bleeding from GAVE after cocaine use [54].
IBD mimic:
Cocaine can induce a state of chronic inflammation in the GI tract, which can mimic other inflammatory conditions, such as inflammatory bowel disease. The inflammation is thought to be a result of a combination of ischemia, direct mucosal injury, and alterations in the gut microbiome . it increases the pro-inflammatory cytokines (IL-18, IL-1β) and chemokines (CCL-2, CCL-7, CXCL-10, CCL-11) and further-more, this involved increased activation of the transcription factors NF-κB and CDX-2. All these affects the mucosal barrier integrity and alters the gut microbiota [55]. Also Cocaine creates an elevated immune system inflammatory state with decreased basal anti-inflammatory markers (e.g., interleukin-10), and increased pro-inflammatory cytokines (e.g., tumor necrosis factor alpha, Interleukin 1β) [5] . It was recently demonstrated that cocaine elicits autophagy involving nitric oxide and glyceraldehyde-3-phosphate dehydrogenase signaling cascade [5].
Conclusion
Cocaine is a potent vasoactive and cytotoxic agent capable of inducing a broad spectrum of gastrointestinal injuries through mechanisms involving intense vasospasm, endothelial dysfunction, thrombosis, oxidative stress, and direct mucosal toxicity. The resultant clinical manifestations range from self-limited ischemic colitis to catastrophic mesenteric ischemia, bowel infarction, and perforation. Extraintestinal involvement, including hepatotoxicity, pancreatitis, and splenic infarction, further underscores the systemic impact of cocaine use.
Given the often atypical presentation and rapid progression, clinicians must maintain a high index of suspicion for cocaine-related gastrointestinal pathology, particularly in younger patients presenting with unexplained abdominal pain or ischemic findings. Early recognition, prompt diagnostic imaging, and timely intervention remain critical to improving outcomes.
Future studies should focus on elucidating the molecular pathways underlying cocaine-induced gastrointestinal injury, identifying predictive biomarkers, and establishing evidence-based management protocols to mitigate morbidity and mortality associated with this underrecognized yet significant clinical entity.
References
- Roque Bravo R, Faria AC, Brito-Da-costa AM, Carmo H, Mladěnka P, Dias da Silva D, et al. Cocaine: An Updated Overview on Chemistry, Detection, Biokinetics, and Pharmacotoxicological Aspects including Abuse Pattern. Vol. 14, Toxins. MDPI; 2022. [CrossRef]
- Ali AA, Flint A, Elmasry M, Ghali M. Acute haemorrhagic ischaemic colitis secondary to cocaine use. BMJ Case Rep [Internet]. 2023 Sep 4;16(9):e255704. Available from: https://casereports.bmj.com/lookup/doi/10.1136/bcr-2023-255704. [CrossRef]
- Dy IA, Wiernik PH. Cocaine-levamisole thrombotic vasculopathy. Semin Thromb Hemost. 2012;38(8):780–2. [CrossRef]
- Bhullar A, Nahmias J, Kong A, Swentek L, Chin T, Schellenberg M, et al. Cocaine use in trauma: the vices-paradox revisited. Surgery (United States). 2023 Oct 1;174(4):1056–62. [CrossRef]
- Bachi K, Mani V, Jeyachandran D, Fayad ZA, Goldstein RZ, Alia-Klein N. Vascular disease in cocaine addiction. Vol. 262, Atherosclerosis. Elsevier Ireland Ltd; 2017. p. 154–62. [CrossRef]
- Cone EJ. Pharmacokinetics and Pharmacodynamics of Cocaine [Internet]. Vol. 19, Journal of Analytical Toxicology. 1995. Available from: https://academic.oup.com/jat/article/19/6/459/774170. [CrossRef]
- Büttner A. Neuropathological alterations in cocaine abuse. Curr Med Chem [Internet]. 2012;19(33):5597–600. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22856656. [CrossRef]
- Wattoo MA, Osundeko O. Cocaine-induced intestinal ischemia. West J Med [Internet]. 1999 Jan;170(1):47–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9926736.
- Osorio J. Cocaine-Induced Mesenteric Ischaemia [Internet]. 2000. Available from: http://karger.com/dsu/article-pdf/17/6/648/2668335/000051980.pdf.
- Kaufman MJ, Siegel AJ, Mendelson JH, Rose SL, Kukes TJ, Sholar MB, et al. Cocaine administration induces human splenic constriction and altered hematologic parameters [Internet]. Vol. 85, J. Appl. Physiol. 1998. Available from: http://www.jap.org. [CrossRef]
- Ellis CN, McAlexander WW. Enterocolitis associated with cocaine use. Vol. 48, Diseases of the Colon and Rectum. 2005. p. 2313–6.
- Angel W, Angel J, Shankar S. Ischemic bowel: Uncommon imaging findings in a case of cocaine enteropathy. J Radiol Case Rep. 2013;7(2):38–43. [CrossRef]
- Hoang MP, Lee EL, Anand A. Histologic spectrum of arterial and arteriolar lesions in acute and chronic cocaine-induced mesenteric ischemia: report of three cases and literature review. Am J Surg Pathol. 1998 Nov;22(11):1404–10.
- Edgecombe A, Milroy C. Sudden death from superior mesenteric artery thrombosis in a cocaine user. Forensic Sci Med Pathol. 2012 Mar;8(1):48–51. [CrossRef]
- Myers SI, Clagett GP, James Valentine R, Hansen ME, Anand A, Chervu A, et al. Chronic intestinal ischemia caused by intravenous cocaine use" Report of two and review of the literature cascs. 1996. [CrossRef]
- Elramah M, Einstein M, Mori N, Vakil N. High mortality of cocaine-related ischemic colitis: A hybrid cohort/case-control study. Gastrointest Endosc. 2012 Jun;75(6):1226–32. [CrossRef]
- Niazi M, Kondru A, Levy J, Bloom AA. Spectrum of Ischemic Colitis in Cocaine Users. [CrossRef]
- Endress C, Gray DGK, Wollschlaeger G. Bowel lschemia and Perforation After Cocaine Use [Internet]. 1992. Available from: www.ajronline.org.
- Deivasigamani S, Irrinki S, Shah J, Sakaray Y. Rare cause of acute abdomen-cocaine-induced small intestinal perforation with coexisting lower gastrointestinal bleed: An unusual presentation. BMJ Case Rep. 2021 Feb 10;14(2). [CrossRef]
- Fishel R, Hamamoto G, Barbui A, Jijl V. Cocaine Colitis Is This a New Syndrome?
- Ullah W, Abdullah HMA, Rauf A, Saleem K. Acute oesophageal necrosis: A rare but potentially fatal association of cocaine use. BMJ Case Rep. 2018;2018. [CrossRef]
- Bathobakae L, Ozgur SS, Bashir R, Wilkinson T, Phuu P, Yuridullah R, et al. Cocaine Gut: A Rare Case of Cocaine-Induced Esophageal, Gastric, and Small Bowel Necrosis. J Investig Med High Impact Case Rep. 2024 Jan 1;12. [CrossRef]
- Naidu PK, Frankel LR, Roorda S, Renda M, Mckenney MG. Cocaine Use and Incarceration: A Rare Cause of Bowel Ischemia, Perforation, and Gastrointestinal Hemorrhage. Cureus. 2022 Aug 29; [CrossRef]
- Martínez-Vieira A, Camacho-Ramírez A, Díaz-Godoy A, Calvo-Durán A, Pérez-Alberca CM, de-la-Vega-Olías C, et al. Bowel ischaemia and cocaine consumption; case study and review of the literature. Revista espanola de enfermedades digestivas. 2014 May;106(5):354–8.
- Saud Khan M, Khan Z, Khateeb F, Moustafa A, Taleb M, Yoon Y. Recurrent levamisole-induced agranulocytosis complicated by bowel ischemia in a cocaine user. American Journal of Case Reports. 2018 Jun 1;19:630–3.
- Chander B, Aslanian HR. Gastric perforations associated with the use of crack cocaine. Gastroenterol Hepatol (N Y) [Internet]. 2010 Nov;6(11):733–5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21437024.
- Lee HS, LaMaute HR, Pizzi WF, Picard DL, Luks FI. Acute gastroduodenal perforations associated with use of crack. Ann Surg [Internet]. 1990 Jan;211(1):15–7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/2403771. [CrossRef]
- Sharma R, Organ CH, Hirvela ER, Henderson VJ. Clinical Observation of the Temporal Association between Crack Cocaine and Duodenal Ulcer Perforation. [CrossRef]
- Mao RMD, Roberts GJ, Hranjec T, Hennessy SA. Incidence of Cocaine Use in Perforated Peptic Ulcer Disease at a Large Safety-Net Hospital. J Am Coll Surg. 2018 Oct;227(4):e136–7. [CrossRef]
- Uzzaman MM, Alam A, Nair MS, Meleagros L. Gastric Perforation in a Cocaine User. Vol. 6, Gastroenterology & Hepatology. 2010.
- Gaduputi V, Tariq H, Ihimoyan A. Atypical Gastric Ulcer in an Elderly Cocaine User. Case Rep Gastrointest Med. 2013;2013:1–3. [CrossRef]
- Schuster KM, Feuer WJ, Barquist ES. Outcomes of cocaine-induced gastric perforations repaired with an omental patch. Journal of Gastrointestinal Surgery. 2007 Nov;11(11):1560–3. [CrossRef]
- Berdugo Hurtado F, Barrientos Delgado A, López Peña C. A large perforated gastric ulcer due to cocaine use. Rev Esp Enferm Dig. 2022 Jul 1;114(7):431–2.
- Mabrouk MY, Guellil A, Haitam S, Deflaoui T, Jabi R, Bouziane M. Peritonitis on sigmoidal perforation in a cocaine user: A rare case report. Int J Surg Case Rep. 2024 Feb 1;115. [CrossRef]
- Appel-Da-Silva MC, D’Incao RB, Antonello VS, Cambruzzi E. Gastrointestinal complications and esophageal stenosis after crack cocaine abuse. Vol. 45, Endoscopy. 2013. [CrossRef]
- Tolaque-Aldana YP, Hernández-Rodarte V, Jáquez-Quintana JO. Crack cocaine abuse as an undescribed cause of gastric outlet obstruction. Revista Espanola de Enfermedades Digestivas. 2022;114(9):550–1. [CrossRef]
- Perysinakis I, Saridakis G, Giannarakis M, Kritikou G, de Bree E. Cocaine-Induced Chronic Bowel Ischemia Manifesting As Small Bowel Obstruction. Cureus. 2024 Apr 25; [CrossRef]
- Ruiz-Tovar J, Candela F, Oliver I, Calpena R. Sigmoid colon stenosis: a long-term sequelae of cocaine-induced ischemic colitis. Am Surg. 2010 Sep;76(9):E178-9. [CrossRef]
- Goraya MHN, Malik A, Inayat F, Ishtiaq R, Zaman MA, Arslan HM, et al. Acute pancreatitis secondary to cocaine use: a case-based systematic literature review. Clin J Gastroenterol. 2021 Aug 1;14(4):1269–77. [CrossRef]
- Valente MJ, Carvalho F, Bastos M d L, de Pinho PG, Carvalho M. Contribution of oxidative metabolism to cocaine-induced liver and kidney damage. Curr Med Chem [Internet]. 2012;19(33):5601–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22856659. [CrossRef]
- Carpano F, Giacani E, Moro D, Gurgoglione G, De Simone S. Heat shock protein (HSP) and its correlation to cocaine-related death: a systematic review. Clinica Terapeutica. 2024;175(4):10–5.
- Verma A, Bennett J, Örme AM, Polycarpou E, Rooney B. Cocaine addicted to cytoskeletal change and a fibrosis high. Vol. 76, Cytoskeleton. John Wiley and Sons Inc; 2019. p. 177–85. [CrossRef]
- Tamargo JA, Sherman KE, Sékaly RP, Bordi R, Schlatzer D, Lai S, et al. Cocaethylene, simultaneous alcohol and cocaine use, and liver fibrosis in people living with and without HIV. Drug Alcohol Depend. 2022 Mar 1;232. [CrossRef]
- Cocaine-Induced Acute Hepatitis and Thrombotic Microangiopathy. JAMA [Internet]. 2005 Feb 16;293(7):793. Available from: http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.293.7.797. [CrossRef]
- Patel KH, Thomas KC, Stacey SK. Episodic Cocaine Use as a Cause of Venous Thromboembolism and Acute Liver Injury. American Journal of Case Reports. 2023;24. [CrossRef]
- Novielli KD, Chambers C V. Splenic infarction after cocaine use. Ann Intern Med [Internet]. 1991 Feb 1;114(3):251–2. Available from: http://www.ncbi.nlm.nih.gov/pubmed/1984755. [CrossRef]
- Homler HJ. Nontraumatic splenic hematoma related to cocaine abuse. West J Med [Internet]. 1995 Aug;163(2):160–2. Available from: http://www.ncbi.nlm.nih.gov/pubmed/7571571.
- Ballard DH, Smith JP, Samra NS. Atraumatic splenic rupture and ileal volvulus following cocaine abuse. Clin Imaging. 2015 Nov 1;39(6):1112–4. [CrossRef]
- Ribeiro BN de F, Correia RS, Salata TM, Antunes FS, Marchiori E. Subcapsular splenic hematoma and spontaneous hemoperitoneum in a cocaine user. Radiol Bras [Internet]. 2017 Apr;50(2):136–7. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0100-39842017000200136&lng=en&tlng=en. [CrossRef]
- Lee Ramos J, Farr M, Shin SH, Ahmed N. Atraumatic splenic rupture in young adult following cocaine use. Int J Surg Case Rep. 2019 Jan 1;65:168–70.
- Karthik N, Gnanapandithan K. Cocaine Use and Splenic Rupture: A Rare Yet Serious Association. Clin Pract. 2016 Aug 11;6(3):868. [CrossRef]
- Azar F, Brownson E, Dechert T. Cocaine-associated hemoperitoneum following atraumatic splenic rupture: A case report and literature review. Vol. 8, World Journal of Emergency Surgery. 2013. [CrossRef]
- Khan AN, Casaubon JT, Paul Regan J, Monroe L. Cocaine-induced splenic rupture. J Surg Case Rep. 2017 Mar 1;2017(3).
- Kravchenko T, Chaudhry A, Khan Z. Upper gastrointestinal bleeding from gastric antral vascular ectasia following cocaine use: case presentation and review of literature. Folia Med (Plovdiv). 2023 Aug 31;65(4):681–5. [CrossRef]
- Chivero ET, Ahmad R, Thangaraj A, Periyasamy P, Kumar B, Kroeger E, et al. Cocaine Induces Inflammatory Gut Milieu by Compromising the Mucosal Barrier Integrity and Altering the Gut Microbiota Colonization. Sci Rep. 2019 Dec 1;9(1). [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



