1. Introduction
Total knee arthroplasty (TKA) is the gold standard surgical treatment for end-stage knee osteoarthritis, effectively reducing pain and restoring functional mobility in patients with advanced degenerative joint disease [
1,
2]. Although long-term implant survival rates exceed 90–95% at 10–15 years of follow-up, patient satisfaction and measured gait biomechanics often do not fully match native knee biomechanics or the walking performance of healthy, age-matched controls [
1,
3]. As a result, modern orthopedic research has increasingly focused on optimizing prosthetic design to improve in vivo kinematics, functional outcomes, and long-term durability, aiming to reduce the biomechanical and functional differences between current prosthetic technology and natural knee physiology.
Among the various prosthetic design options for primary TKA, the clinical decision between fixed-bearing (FB) and rotating-bearing (RB)—also known as mobile-bearing—tibial inserts remains a subject of significant debate in the orthopedic literature [
3,
4]. Rotating-bearing designs were initially introduced with the theoretical aim of mechanically separating flexion-extension motion from axial rotation, potentially reducing contact stresses across the polyethylene articulation and enabling physiological self-alignment during gait [
5,
6].
Proponents of rotating-bearing technology argue that the rotational freedom provided by the platform’s kinematic design could promote a more natural walking pattern, better dynamic stability, and longer-lasting wear characteristics compared to fixed-bearing options. Conversely, fixed-bearing designs maintain a stable relationship between the femoral and tibial components, offering proven mechanical stability, reliable implant fixation, and a simpler surgical process with well-documented long-term survivorship data spanning several decades [
3,
7].
Despite these theoretically different design approaches, the clinical superiority of one design philosophy over the other remains debated, with the orthopedic literature showing conflicting and inconsistent results regarding functional and kinematic benefits [
4]. A major methodological limitation noted in many comparative prosthesis studies is the heavy dependence on subjective patient-reported outcome measures (PROMs), including tools such as the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and the Knee Society Score (KSS) [
8].
These patient-centered assessment tools, while valuable for capturing perceived functional status and symptom severity, are inherently subject to ceiling effects—particularly in successful TKA cohorts where postoperative scores cluster near the maximum end of the rating scale—and may consequently fail to detect subtle biomechanical and kinematic differences between implant designs that could be objectively quantified through more sensitive instrumentation [
8]. Objective gait analysis using inertial measurement units (IMUs)—miniature wearable accelerometers and gyroscopes positioned at the center of mass or lower extremity segments—offers a quantifiable, highly reproducible, and clinically practical assessment of spatiotemporal gait parameters including velocity, cadence, stride length, stance phase duration, and symmetry indices in both laboratory and community-based settings [
9,
10].
Such objective instrumentation facilitates the detection and characterization of gait impairments that patient-reported measures cannot reliably capture, thus providing complementary data to subjective outcomes assessments. Additionally, a significant gap in the comparative prosthesis literature is the lack of prospective longitudinal studies that systematically monitor the trajectory and progression of gait recovery beyond the initial 6–12 months postoperatively, extending through the extended intermediate-term follow-up period (12–24 months) to determine whether specific implant design features affect the timing, magnitude, or quality of functional maturation during the extended neuromotor adaptation and motor learning phase.
Previous studies have shown that gait recovery after TKA follows a biphasic pattern, with quick improvements in function during the immediate postoperative period (6–12 weeks), followed by slower but significant improvements that continue through the first year after surgery and possibly beyond. These changes reflect ongoing neuromotor adaptation, the resolution of pain-related movement restrictions, and the enhancement of dynamic joint stability [
11,
12]. However, the long-term course of this recovery process and the possible impact of prosthesis design on recovery trajectory have not been fully understood in the current literature.
Recent technological advances in wearable inertial sensors have significantly improved the feasibility and practicality of obtaining objective, standardized gait assessments in clinical settings, including outpatient orthopedic clinics, without the need for expensive, specialized laboratory-based motion capture systems or costly fluoroscopic imaging equipment [
10,
13]. The G-WALK and similar IMU-based systems have demonstrated excellent validity, reliability, and responsiveness for measuring spatiotemporal gait parameters across diverse patient populations, including those with musculoskeletal impairments, neurological disorders, and post-surgical conditions [
13,
14].
Furthermore, emerging literature indicates that specific spatiotemporal parameters—particularly gait velocity and stride length—show stronger correlations with patient-perceived functional outcomes and quality of life than other objective measures. This supports the clinical importance of these parameters as indicators of functional outcomes. The main goal of this prospective, longitudinal comparative study was to systematically assess spatiotemporal gait parameters—namely gait velocity, cadence, and stance phase duration—between patients receiving fixed-bearing and rotating-bearing total knee arthroplasty prostheses, using validated inertial measurement unit (IMU) technology.
We specifically aimed to characterize the postoperative gait recovery trajectory at three standardized follow-up timepoints (6, 12, and 24 months postoperatively) to determine whether rotating-bearing prostheses offer objective functional advantages over fixed-bearing designs in terms of gait restoration, recovery trajectory, or intermediate-term functional outcomes. Our primary hypothesis was that rotating-bearing designs, thanks to enhanced mechanical properties and improved articulation geometry, would show superior spatiotemporal gait parameters and a more favorable recovery trajectory compared to fixed-bearing prostheses. Secondary objectives included analyzing the relationship between objective gait metrics and patient-reported functional outcomes (WOMAC, Geriatric Locomotive Function Scale 10-Point [GLFS-1]), investigating potential differences across demographic groups (age, body mass index, sex), and providing Level I evidence to aid in the choice of prosthesis for primary TKA.
4. Discussion
This detailed biostatistical analysis of a prospective comparative study comparing fixed-bearing, posterior-stabilized (PS) and rotating-platform, ultracongruent (UC) total knee arthroplasty (TKA) prostheses showed that both implant designs provided similar functional outcomes and gait performance at 24 months postoperatively. Although the study included various aspects of postoperative recovery, such as spatiotemporal gait analysis using the WALK test, patient-reported outcome measures (PROMs), long-term functional changes, and subgroup analyses, the results demonstrate notable consistency in clinical effectiveness between the two prosthetic designs.
Most gait parameters — including cadence, velocity, gait cycle duration, step length, stride length, and propulsion metrics — showed no statistically significant differences between the two groups at any follow-up timepoint. Likewise, patient-reported outcomes measured by the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and the Geriatric Locomotive Function Scale 10-Point (GLFS-1) showed similar improvements in both groups, with only isolated statistically significant differences that might not be clinically meaningful.
These findings provide important evidence for the ongoing discussion about the best prosthesis choice in primary TKA and suggest that multiple well-designed implants can deliver satisfactory functional recovery regardless of bearing design philosophy. Between-Group Gait Analysis The present study’s observation that spatio-temporal gait parameters did not significantly differ between fixed-bearing and rotating-platform prostheses aligns with current orthopedic research on the convergence of outcomes across various TKA designs.
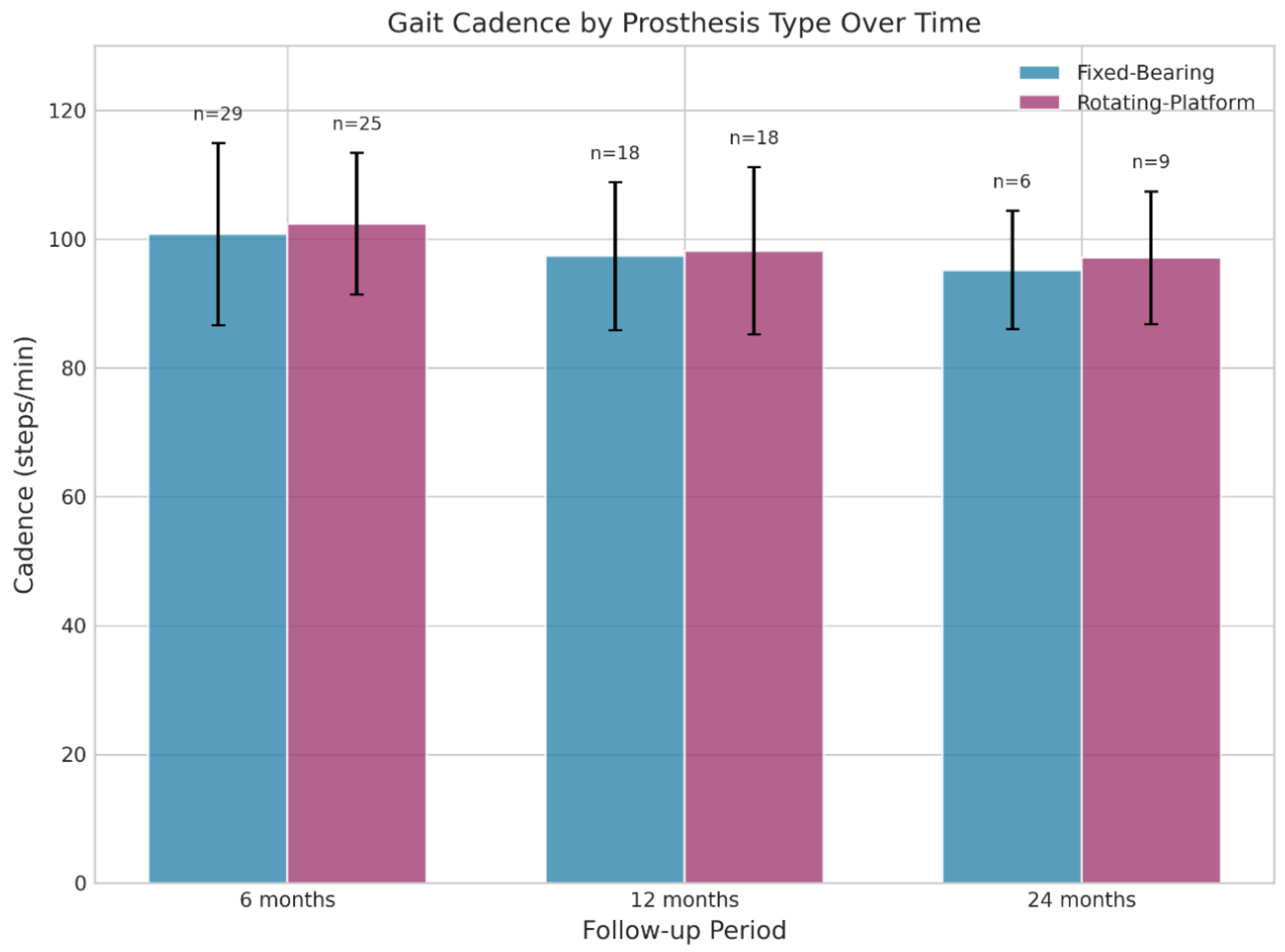
At the six-month mark, only one isolated significant finding was observed: the fixed-bearing group showed a statistically significant longer stride length on the left side compared to the rotating-platform group (1.17 ± 0.12 m vs. 1.10 ± 0.12 m, p=0.049). However, this difference, although statistically significant, is unlikely to be clinically meaningful due to its small absolute size (0.07 m) and the lack of corresponding differences in other spatiotemporal parameters such as velocity (0.99 ± 0.14 m/s vs. 0.95 ± 0.15 m/s, p=0.315) or cadence (100.79 ± 14.77 vs. 103.81 ± 12.17 steps/min, p=0.409).
Similarly, at 24 months, the fixed-bearing group showed a significantly longer step length on the right side (52.16 ± 1.58 m vs. 33.18 ± 24.98 m, p=0.038). However, the very high standard deviation in the rotating-platform group (24.98 m) indicates considerable variability and possible outliers, so this result should be interpreted with caution. Importantly, key gait parameters, including walking velocity and cadence — widely recognized as sensitive indicators of lower extremity function and quality of life — showed no significant differences between prosthesis types at any follow-up point. The steady cadence values at 6 months (about 102 steps/min for both groups) and their slight decrease by 12 months (around 98 steps/min for both groups) reflect normal age-related walking patterns and suggest that both prosthetic designs support similar locomotive efficiency [
15].
A recent meta-analysis evaluating gait analysis in patients undergoing TKA showed that improvements in cadence, stride length, walking speed, and step length are key indicators of successful gait recovery, with significant reductions in double support time reflecting better gait stability [
16]. The neutral results of the current study regarding these main gait parameters support the clinical conclusion that modern TKA prostheses, regardless of bearing design, have achieved enough biomechanical complexity to effectively restore walking function in most patients with advanced osteoarthritis.
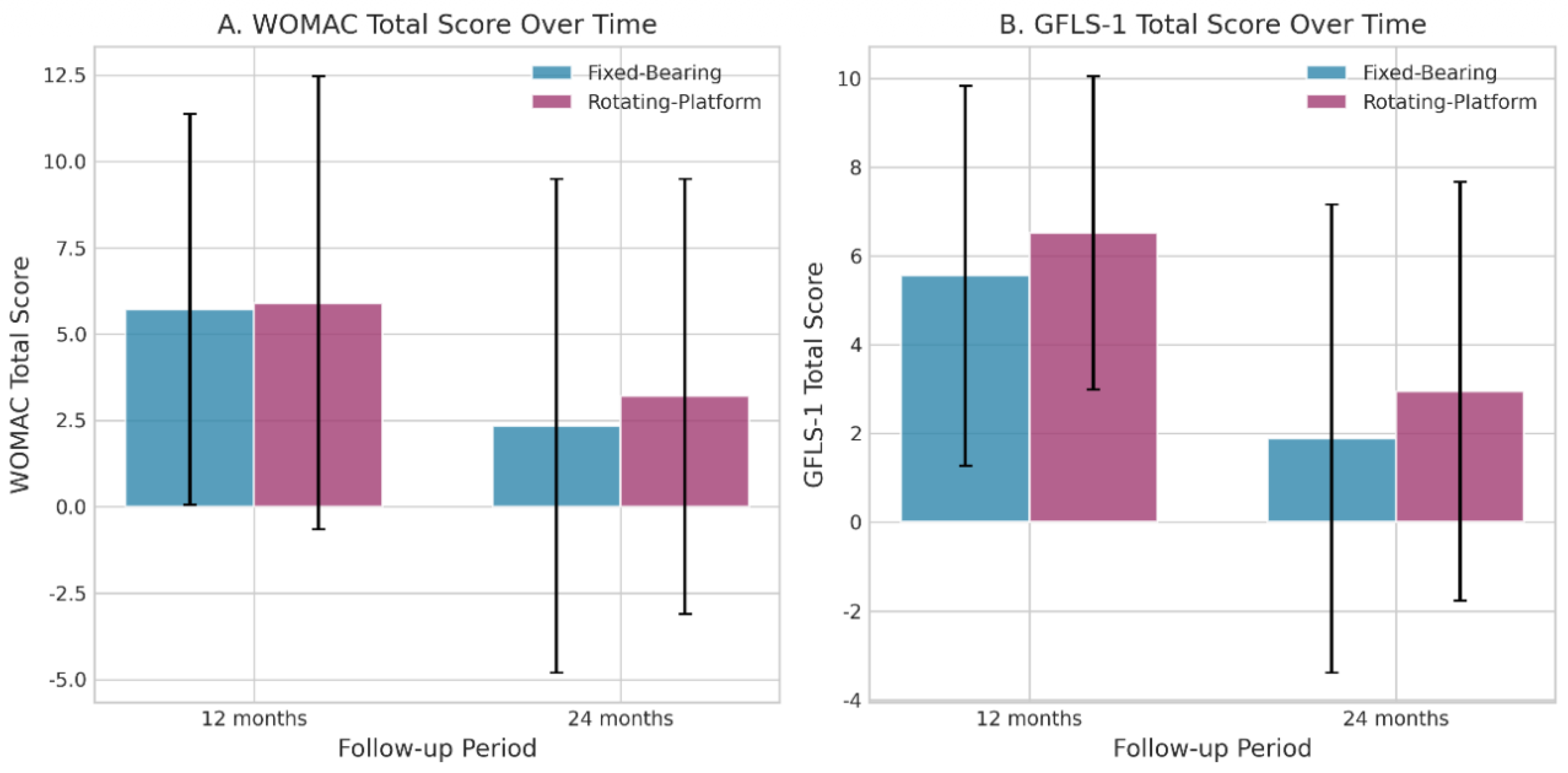
Patient-Reported Outcomes Assessment The evaluation of patient-reported outcomes using validated tools showed similar results between the two prosthetic groups, both demonstrating significant improvements from preoperative baseline to postoperative follow-up. At the 12-month assessment, the WOMAC pain subscale showed minimal difference between groups (1.65 ± 1.62 in fixed-bearing vs. 1.36 ± 1.76 in rotating-platform, p=0.477), and stiffness scores remained very low in both groups with no clinically meaningful differences.
The WOMAC functional subscale showed similar scores (4.06 ± 4.66 vs. 5.09 ± 5.08, p=0.354), indicating that patients in both groups found similar ease in performing daily activities [
17]. At the 24-month mark, a statistically significant difference appeared in the WOMAC total score (2.22 ± 7.17 in fixed-bearing vs. 2.10 ± 4.77 in rotating-platform, p=0.044), with the rotating-platform group reporting slightly better outcomes; however, the small difference of 0.12 points on a scale where higher scores mean worse outcomes is not clinically meaningful. These results highlight the well-known fact that both modern fixed-bearing and mobile-bearing TKA designs provide significant pain relief and improved function, with the degree of improvement greatly outweighing the minor differences between the two designs.
The WOMAC instrument, originally created for osteoarthritis evaluation, has shown excellent validity, reliability, and responsiveness in the total knee arthroplasty group, with preoperative scores usually between 40 and 60 points [
8,
18]. The postoperative scores of about 2–6 points in both groups indicate reductions of 90–95%, representing significant functional improvements regardless of prosthetic philosophy.
The Geriatric Locomotive Function Scale 10-Point (GLFS-10), a patient-centered assessment of joint awareness and perceived function during walking derived from the validated 25-question Geriatric Locomotive Function Scale (GLFS-25), similarly showed no significant differences between groups at either 12-month (5.56 ± 4.41 vs. 6.23 ± 3.79, p=0.607) or 24-month follow-ups (1.89 ± 5.43 vs. 2.30 ± 4.42, p=0.514). The GLFS-25, on which the GLFS-1 is based, has been validated in elderly populations, demonstrating excellent Cronbach’s alpha reliability coefficients of 0.961 and strong concurrent validity with quality-of-life measures [
19,
20].
The significant long-term improvements in GLFS-1 scores seen in both groups from 12 to 24 months (fixed-bearing: p=0.030; rotating-platform: p=0.026) indicate a gradual normalization of gait mechanics and reduced joint awareness during functional activities as the postoperative recovery progresses. This pattern of improvement supports the idea that neural adaptation and refinement of compensatory mechanisms continue to develop during the extended postoperative period [
16,
21,
22].
The convergence of objective gait parameters and subjective patient perceptions showing similar improvements across both prosthetic types strengthens the evidence that prosthetic design choice is not a primary factor in determining functional outcomes in primary TKA, provided both implants are properly positioned and balanced. Longitudinal Recovery Patterns within-group analysis revealed distinct recovery trends that offer important insights into the functional evolution after TKA. The rotating-platform group demonstrated a statistically significant decrease in cadence from 6 to 12 months (103.81 ± 12.17 vs. 98.19 ± 12.62 steps/min, p=0.038), while the fixed-bearing group showed a non-significant trend in the same direction (100.79 ± 14.77 vs. 97.36 ± 11.13 steps/min, p=0.210).
This transition toward lower cadence during the extended recovery period may reflect a shift to more economical, stable gait patterns typical of skilled neuromotor learning and adaptation. Rather than indicating functional decline, this finding likely shows that patients naturally adopt more efficient walking strategies that reduce compensatory muscle activity and joint reaction forces [
12,
16]. Analysis of patient-reported outcomes over time revealed significant improvements from 12 to 24 months, with both the fixed-bearing and rotating-platform groups achieving statistically significant reductions in GLFS-1 scores (fixed-bearing: 5.56 ± 4.28 to 1.89 ± 5.28, p=0.030; rotating-platform: 6.52 ± 3.53 to 2.95 ± 4.72, p=0.026), indicating ongoing improvement in perceived locomotive function and joint awareness.
These long-term improvements align with the well-known biphasic recovery pattern after TKA, in which rapid functional gains happen within the first 6 months, followed by slower but steady improvements that continue through 12–24 months as patients gradually return to normal activities, increase their activity levels, and address ongoing motor control issues [
7,
11,
12]. The similar recovery paths in both groups highlight that prosthetic design does not significantly change the core neurobiological and biomechanical recovery processes after knee arthroplasty.
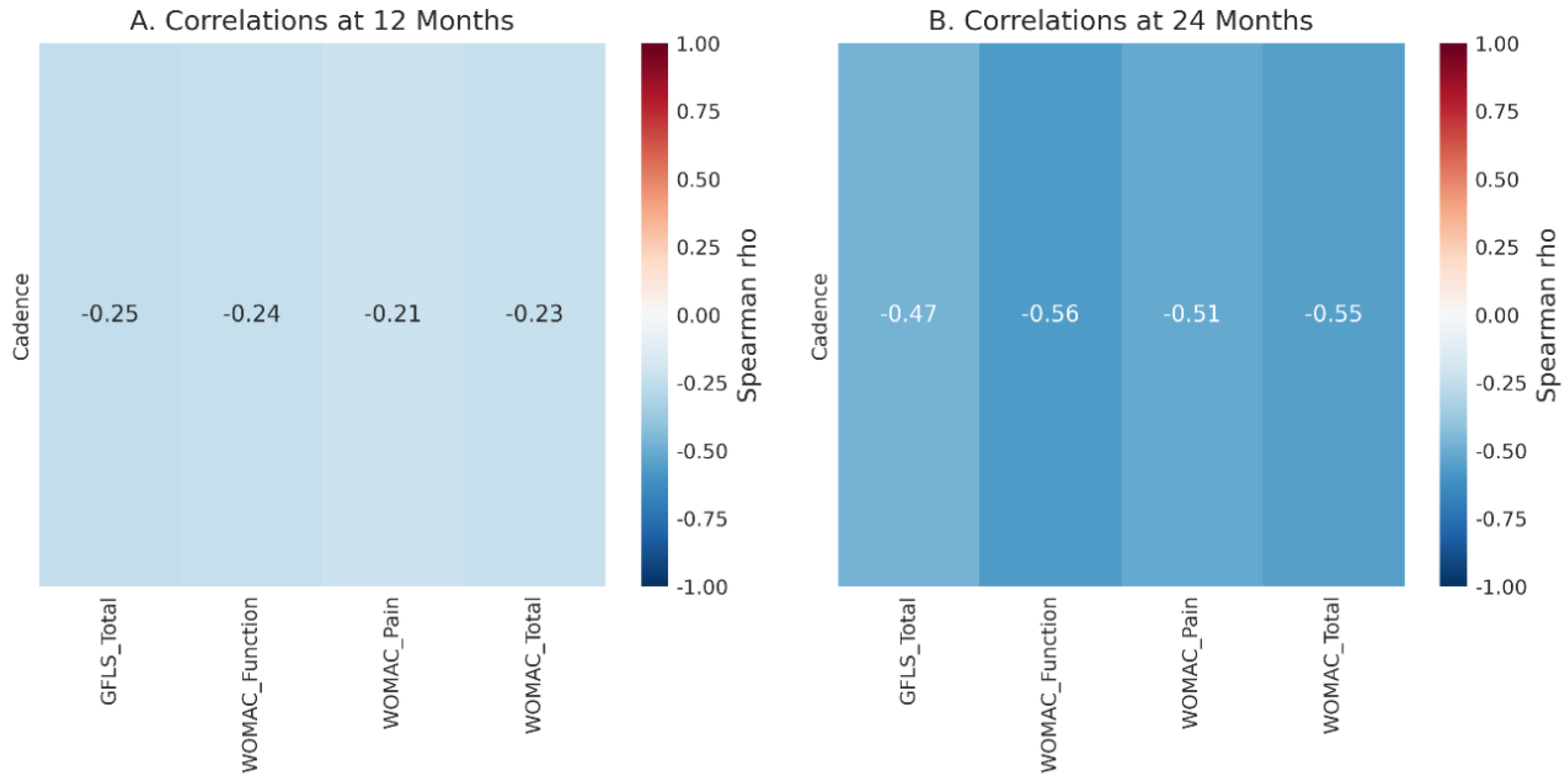
A significant finding emerged from the correlation analysis between objective gait parameters and patient-reported outcomes. At the 12-month mark, no statistically significant correlations were found between key gait metrics (cadence and velocity) and PROM scores. However, at the 24-month mark, a statistically significant moderate negative correlation was observed between cadence and WOMAC function (Spearman’s rho = -0.563, p=0.036) and WOMAC total score (rho = -0.551, p=0.041). This relationship suggests that patients with lower cadence values — typically interpreted as more controlled, economical gait patterns — reported better functional outcomes and lower symptom burden. This finding contrasts with conventional assumptions that higher cadence universally indicates better functional status, instead suggesting that gait quality and efficiency may be more important than stepping frequency as indicators of successful postoperative function [
16,
21].
Such observations highlight the limitations of using isolated spatiotemporal parameters as outcome measures and support the integration of various assessment methods—including gait quality indices, kinematic analyses, and patient-centered measures—in postoperative functional evaluations [
16]. Demographic stratification analyses examining potential differences in prosthetic design effects across age groups, body mass index categories, and sex showed no statistically significant interactions or variations in key gait parameters between fixed-bearing and rotating-platform designs within any demographic group. This consistent similarity across diverse patient groups improves the generalizability of the findings and indicates that neither prosthetic design provides a clear advantage or disadvantage in specific demographic cohorts [
4,
23,
24].
Prosthesis selection in primary TKA should be individualized based on surgeon expertise, anatomical considerations, and patient-specific factors rather than solely optimizing design selection based on demographic characteristics. The current findings showing equivalent outcomes between fixed-bearing and rotating-platform designs support an emerging consensus in orthopedic literature that multiple well-engineered prosthetic platforms can achieve similar clinical success. A comprehensive systematic review and meta-analysis of mobile-bearing versus fixed-bearing TKA designs found no significant differences in all-cause revision rates, aseptic loosening, knee functional scores (Oxford Knee Score, Knee Society Score, Hospital for Special Surgery score), maximum knee flexion, or radiographic outcomes at short-term (<5 years), mid-term (5-9 years), and long-term (≥10 years) follow-up periods [
4].
A landmark 12-year prospective randomized controlled trial comparing fixed-bearing and rotating-platform designs found no statistically significant differences between the implant types in terms of functional Knee Society Scores, WOMAC scores, SF-36 scores, satisfaction, or implant survival, with a 93% probability of success for the rotating-platform implant at 15 years compared to 91% in the fixed-bearing group [
3]. These findings emphasize the maturity of modern knee arthroplasty technology, where both traditional and innovative bearing designs have achieved similar clinical success when properly implanted and balanced [
3,
4].
Recent evidence comparing posterior-stabilized versus cruciate-retaining designs in patients with preoperative genu recurvatum shows that while PS-TKA offers better flexion and lower rates of hyperextension recurrence, there are no significant differences in functional outcomes, patient satisfaction, or revision rates [
23]. This highlights that implant choice should remain tailored based on intraoperative findings and patient-specific anatomy, rather than driven by claims of universal superiority of any single design. The mechanical benefits of PS-TKA, especially its post-cam mechanism, may provide advantages in certain complex anatomical cases, but in typical primary osteoarthritis, both fixed-bearing and rotating-platform designs deliver excellent clinical results.
The observed improvements in both prosthetic groups highlight the importance of systematic postoperative rehabilitation in TKA outcomes. Current evidence clearly shows that high-intensity, early mobilization-based rehabilitation programs lead to better strength recovery, range of motion, and functional performance compared to standard rehab protocols [
7,
11,
12]. Bade and colleagues demonstrated that high-intensity rehab following total knee arthroplasty, started after hospital discharge, resulted in superior strength and functional outcomes without increasing pain or decreasing knee range of motion. Patients in the high-intensity group showed clinically better performance on the stair climb test and six-minute walk test at 52 weeks after TKA.
The American Physical Therapy Association (APTA) has published clinical practice guidelines recommending that physical therapists develop early mobility plans and include motor function training, such as balance, walking, and movement symmetry, with strong evidence supporting this approach [
25]. Recent studies have shown that early physical therapy started within 24 hours after surgery, especially ultra-early therapy within 12 hours, results in shorter hospital stays without sacrificing functional outcomes [
12]. The consistent improvements in both groups suggest that factors beyond prosthetic design—such as surgical technique, intra-operative soft tissue management, postoperative pain control, and structured rehabilitation—are key determinants of functional results. This realization has significant implications for surgical practice and health system planning, indicating that optimizing perioperative care and rehabilitation protocols could lead to more meaningful functional improvements than simply chasing small gains through prosthetic design refinement.
The lack of clinically significant differences between fixed-bearing and rotating-platform prostheses supports a practical approach to prosthesis selection in primary TKA that focuses on surgeon experience, patient anatomy and deformity, and the availability of suitable instruments. For patients with primary knee osteoarthritis without severe deformity or ligamentous weakness, choosing between fixed-bearing and mobile-bearing designs does not need to be based on expectations of significantly better functional results. Surgeon confidence with the technique, the specific implant platform’s track record in clinical use, and patient-specific factors are appropriate criteria for selection. Posterior-stabilized designs may be considered more suitable in knees with severe flexion contractures, deficient posterior cruciate ligaments, or severe varus/valgus deformities where the mechanical stability of the cam-post mechanism offers predictable balancing benefits [
6,
7,
23]. Conversely, rotating-platform designs with anatomically responsive geometries may be especially appropriate for patients with high demands for deep flexion activities or those where long-term polyethylene durability is a concern due to younger age or high activity levels [
3,
4].
This investigation included several methodological strengths that improve the quality and relevance of the findings. The prospective comparative design with well-matched baseline demographics reduces selection bias compared to retrospective cohort studies. The study achieved a substantial follow-up duration (24 months), capturing the extended recovery period needed for gait patterns and functional outcomes to stabilize. A thorough assessment of both objective gait parameters using validated WALK test methodology and subjective patient-reported outcomes offers complementary insights into functional recovery.
Utilization of standardized, validated assessment tools (WOMAC, GLFS-1) with established psychometric properties ensures comparability with existing literature [
8,
17,
18,
19,
20]. The WOMAC instrument has demonstrated excellent validity, reliability, and responsiveness across multiple studies and populations. The GLFS-1, derived from the validated GLFS-25, has shown Cronbach’s alpha reliability coefficients exceeding 0.94 and excellent concurrent validity in elderly populations [
19,
20]. Subgroup analyses considering age, BMI, and sex heterogeneity further enhance generalizability by showing consistent effects across various demographic groups.
Choosing appropriate statistical methods — including non-parametric testing for non-normally distributed variables, Wilcoxon signed-rank test for paired comparisons, and Spearman’s correlation analysis to examine relationships between objective and subjective measures — reflects solid biostatistical practice and strengthens the credibility of the findings. Several limitations should be considered when interpreting these results and their clinical application.
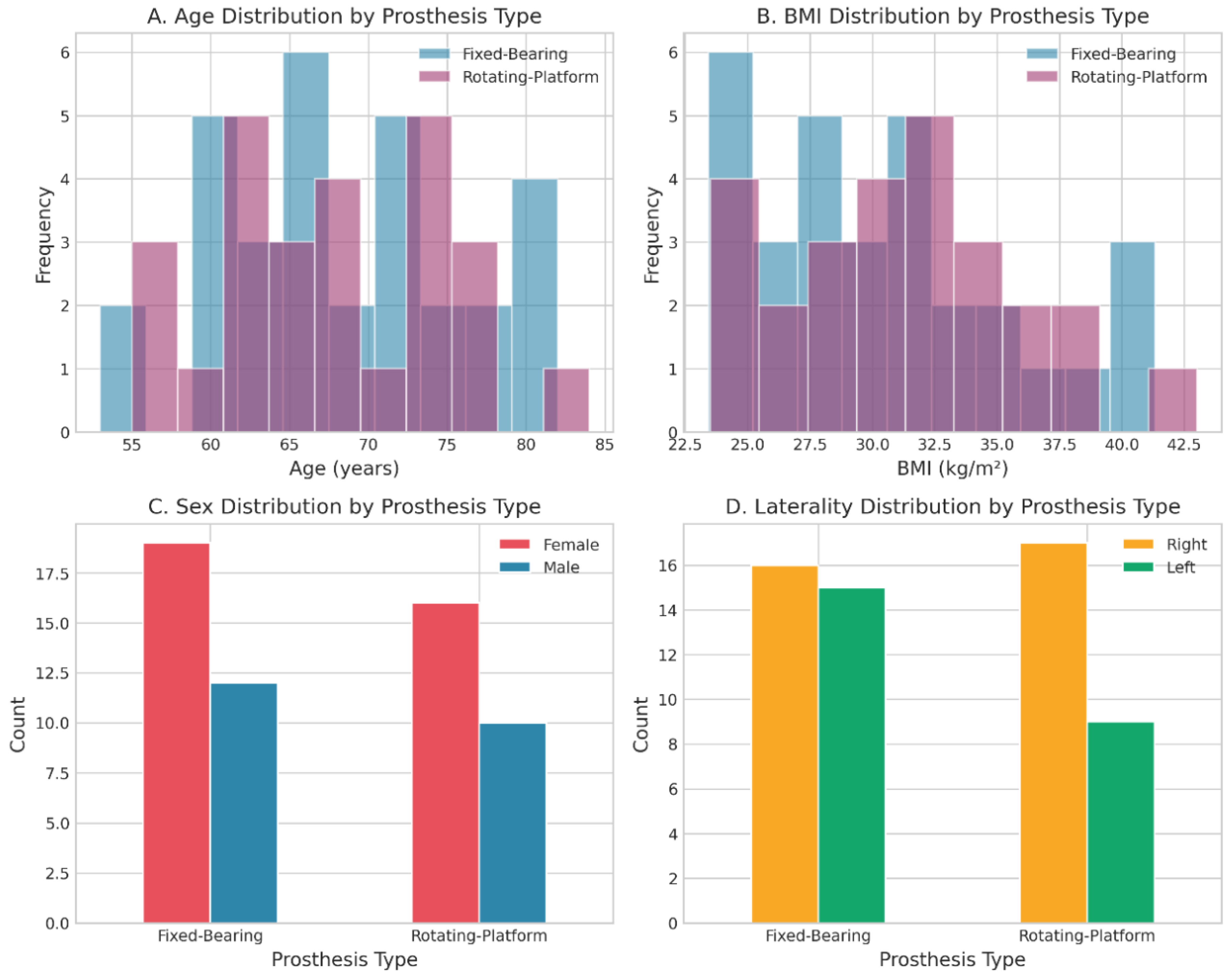
First, the small sample size (57 patients total; 31 fixed-bearing, 26 rotating-platform) offers limited statistical power to detect small-to-moderate effect sizes that could have clinical significance. While the similarity of outcomes across multiple domains and timepoints suggests that type II error is unlikely to hide true differences, larger sample sizes would increase confidence in the null results and allow for more accurate estimation of treatment effects.
Second, the 24-month follow-up duration, while capturing the extended acute recovery period, does not address long-term durability and revision rates—critical endpoints that may diverge between designs only after extended follow-up periods (10–15 years or longer). Wear-related complications of polyethylene inserts, aseptic loosening of components, and other degenerative processes may manifest at later timepoints not captured in this intermediate-term analysis.
Third, the study population characteristics were not thoroughly detailed in the biostatistical report, which limits the ability to assess potential selection biases or demographic constraints that could affect generalizability. Including information on preoperative deformity severity, range of motion, comorbidity burden, functional status, and specific surgical techniques used would improve interpretability.
Fourth, the study did not evaluate important secondary endpoints such as radiographic alignment, component positioning accuracy, or imaging markers of polyethylene wear that could provide mechanistic insights into the equivalence of designs.
Fifth, detailed specifications for rehabilitation protocols, physical therapy intensity, and patient adherence metrics were not provided, which prevents assessing rehabilitation as a potential confounding or effect-modifying variable.
Sixth, the study did not report on key patient satisfaction metrics, expectations alignment, or post-operative complications that influence overall surgical success beyond functional outcomes.
Seventh, analysis of the correlation between gait parameters and PROMs was done post hoc on subsets of patients with complete data (n=14 at 24 months), raising concerns about reduced power and the risk of spurious associations from multiple comparisons. Formal correction for multiple comparisons (e.g., Bonferroni adjustment) was not reported, which increases the chance of a type I error.
Finally, the apparent loss of participants from 6-month to 24-month follow-up suggests potential attrition bias, which should be considered when interpreting longitudinal results. Despite these limitations, the study offers valuable Level II evidence regarding prosthesis equivalence and makes an important contribution to the comparative effectiveness literature in orthopedic surgery, especially given the variability of results in previous studies and the lack of high-quality prospective comparative data in many institutional settings.
Future research should fill key gaps in the comparative prosthesis literature. Long-term follow-up studies (≥10 years) that include radiographic assessment, revision outcomes, and durability endpoints would conclusively determine if initial functional equivalence lasts throughout the lifespan of implants and if design-specific complications develop over time. Prospective randomized controlled trials comparing modern high-constraint designs with traditional ones, and incorporating three-dimensional gait analysis, kinematic fluoroscopy, and advanced neurophysiologic assessments, would offer a detailed mechanistic understanding of how implant design affects knee kinematics and muscular adaptation.
Investigation of rehabilitation intensity, early mobilization protocols, and targeted neuromuscular training as primary factors influencing functional outcomes—with prosthetic design as a secondary stratification variable—would clarify the relative contributions of technical and rehabilitative interventions. Evaluating patient expectations, shared decision-making processes, and satisfaction trajectories would shed light on the psychological and expectancy-related factors that affect outcome satisfaction, independent of objective functional improvements. Lastly, health economic analyses that include implant costs, revision rates, reoperation rates, and quality-adjusted life years would guide resource allocation and procurement decisions in health systems with limited budgets.