Submitted:
15 January 2026
Posted:
16 January 2026
You are already at the latest version
Abstract
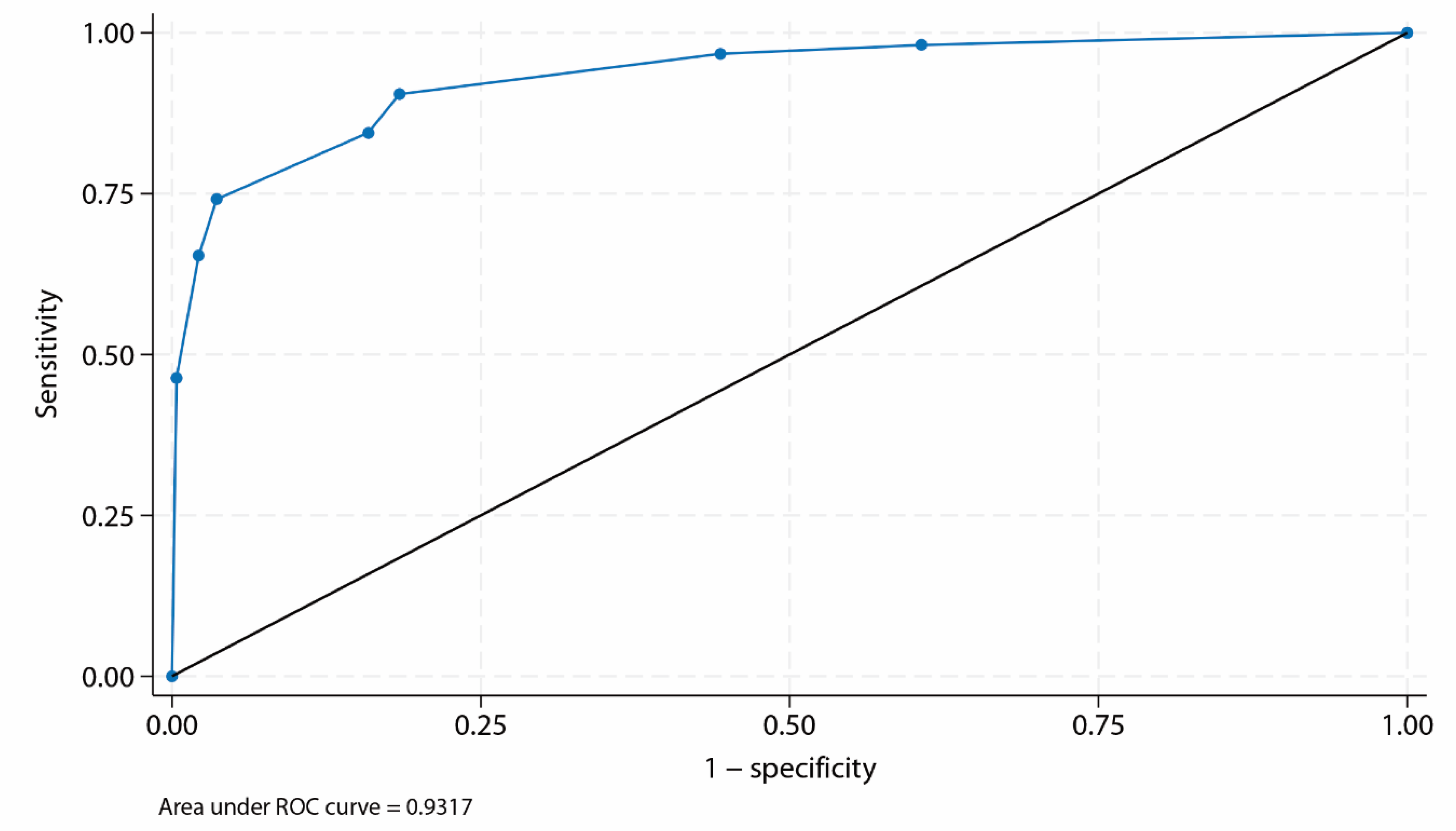
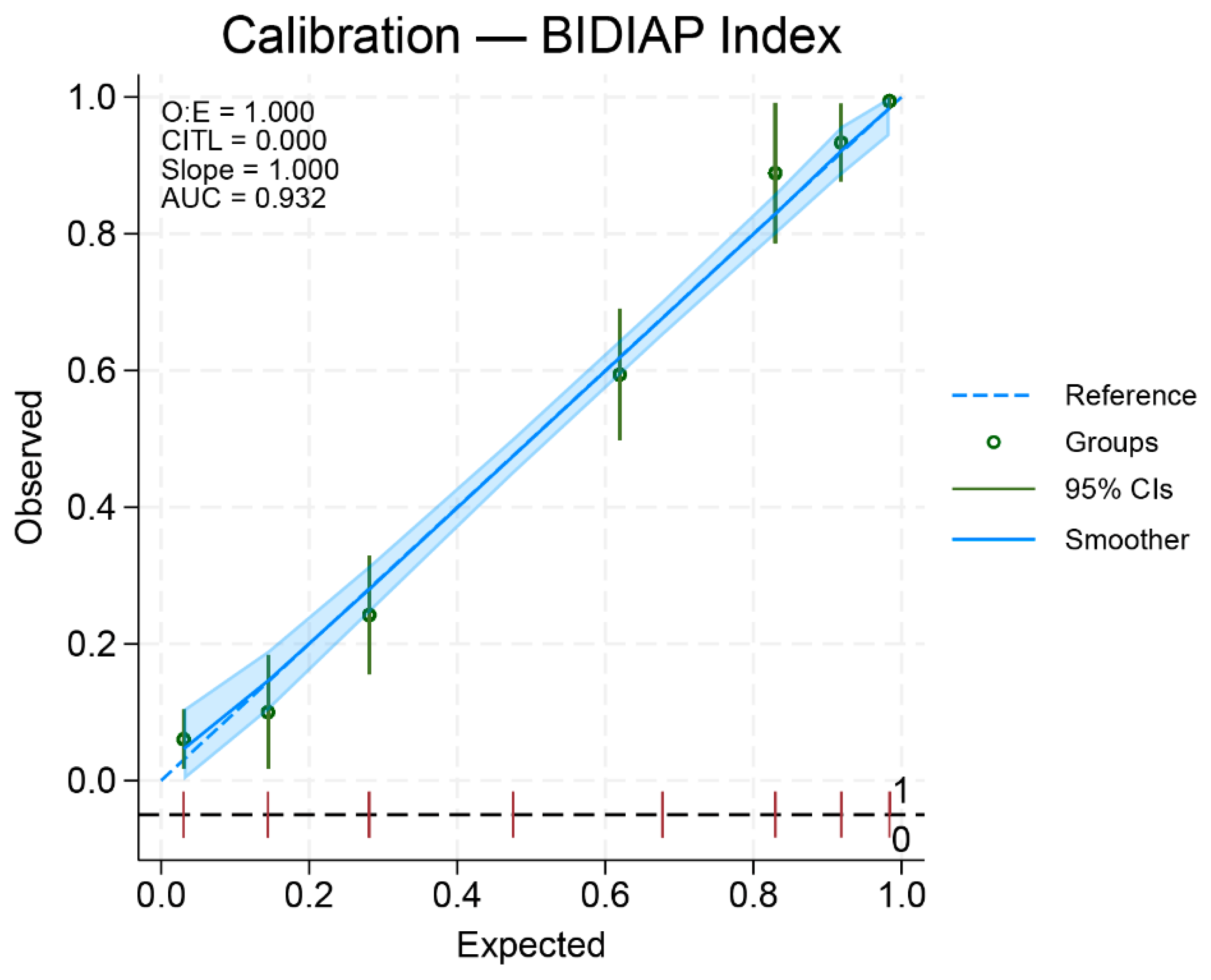
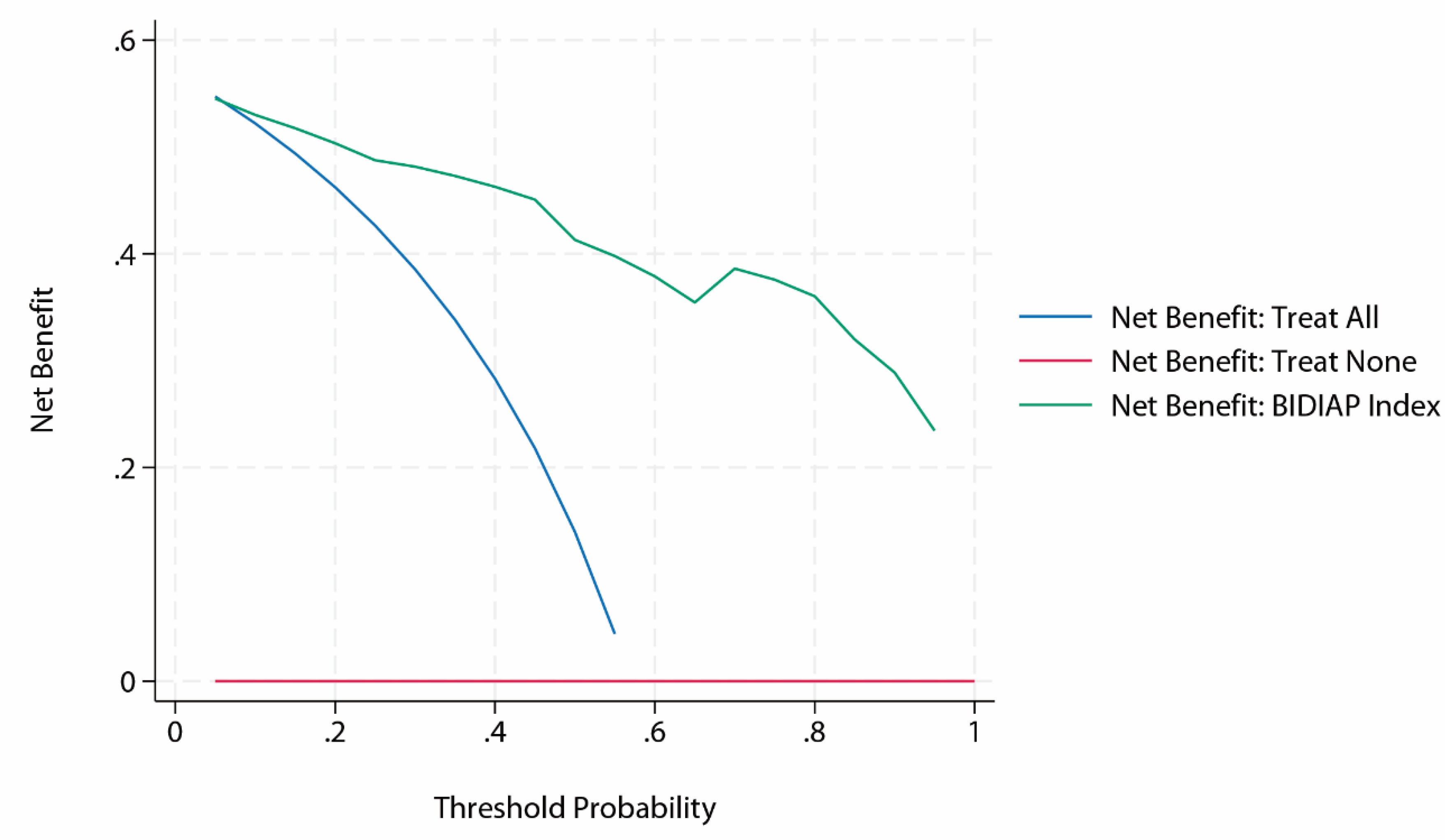
Introduction: Pediatric acute appendicitis (PAA) remains challenging to diagnose despite existing diagnostic scores. The BIDIAP index is a three-item diagnostic tool with very high discriminative performance in a derivation cohort. This study aimed to prospectively and externally validate the BIDIAP index in a multicenter pediatric population.Material and Methods: We conducted a prospective, multicenter observational study across four tertiary pediatric centers, enrolling children presenting with suspected PAA. Two groups were analyzed: patients with histopathologically confirmed PAA and patients in whom appendicitis was confidently excluded after diagnostic work-up, classified as non-surgical abdominal pain (NSAP). The BIDIAP index was applied using a predefined cutoff (≥ 4 points), and diagnostic performance was assessed using ROC analysis, calibration metrics, and decision curve analysis (DCA).Results: A total of 644 patients meeting the prespecified analytical criteria were included in the primary analysis. The BIDIAP index demonstrated excellent diagnostic performance, with an area under the ROC curve of 0.93 (95% CI, 0.92–0.95). The calibration slope was 1.00, and the intercept was close to zero, indicating close agreement between predicted and observed risks. At the prespecified cutoff value of ≥ 4 points, the BIDIAP index achieved a sensitivity of 90.5% and a specificity of 81.6%. DCA showed a positive net clinical benefit of the BIDIAP index over treat-all and treat-none strategies across the full range of clinically relevant threshold probabilities. Conclusions: The BIDIAP index demonstrated excellent diagnostic performance for PAA. Its simplicity, based on only three items, and its potential applicability even when the appendix is not visualized on ultrasonography make the BIDIAP index a promising tool for supporting clinical decision-making in routine pediatric emergency practice.
Keywords:
Introduction
Material and Methods
Study Design
Sample Collection
Data Collection, Storage, And Processing
Systemic-Immune Index Calculation
Ultrasonographic Measurements and Data Collection
Calculation of the BIDIAP Index
Statistical Analysis
Sample Size
Analytical Sample Definition and Missing Data Handling
Statistical Analysis for Group Comparisons
Data Visualization and Graphical Analysis
Receiver Operating Characteristic Curve Analysis
Calibration
Decision Curve Analysis
Sensitivity Analyses
Statistical Significance Level and Software
Results
Study Population
Baseline Sociodemographic and Clinical Characteristics
Diagnostic Performance of the BIDIAP Index

| Sociodemographics | Group 1 (NSAP) n = 305 |
Group 2 (PAA) n = 414 |
P-value |
| Age, y | 10.0 (2.87) | 10.13 (3.1) |
0.59* |
| Sex, M/F | 156/158 | 243/161 |
0.005** |
| Duration of abdominal pain, h1 | 24 (12-48) | 24 (12-48) | 0.22*** |
| Hyporexia, Yes/No | 149/157 | 250/146 | <0.001** |
| Fever at home (>37.8 °C), Yes/No | 88/224 | 118/284 | 0.74** |
| Vomiting, Yes/No | 121/192 | 229/172 | <0.001** |
| Diarrhea, Yes/No | 60/253 | 75/327 | 0.81** |
| Peritoneal irritation (Blumberg sign), Yes/No/Unclear | 85/108/86 | 249/57/67 | <0.001** |
| Absolute leukocyte count (1x109/L)1 | 9.1 (6.9-13.2) | 15.5 (12.4-18.4) | <0.0001*** |
| Absolute lymphocyte count (1x109/L)1 | 2.13 (1.38-2.9) | 1.6 (1.08-2.13) | <0.0001*** |
| Absolute neutrophil count (1x109/L)1 | 5.55 (3.89-10) | 12.6 (9-15.6) | <0.0001*** |
| Absolute platelet count (1x109/L) | 290.15 (74.72) | 297.57 (73.56) | 0.19* |
| SII1 | 759.33 (410.03-1721) | 2383.24 (1239.5-4114.53) | <0.0001*** |
| Appendiceal ultrasonographic transverse diameter, mm1 | 5 (4-6.25) | 9 (7.5-10) | <0.0001*** |
| C-Reactive Protein (mg/L)1 | 5 (0.6-21.5) | 24.8 (8-64.7) | <0.0001*** |
| BIDIAP score1 | 2 (0-3) | 7 (5-9) | <0.0001*** |
| BIDIAP Index cut-off value | Correctly classified (%) |
Sensitivity (%) |
Specificity (%) |
LR+ | LR- | PPV (%) | NPV (%) |
| ≥2 | 72.8 | 98.1 | 39.4 | 1.62 | 0.05 | 68.2 | 94.0 |
| ≥3 | 79.0 | 96.7 | 55.6 | 2.18 | 0.06 | 74.3 | 92.8 |
| ≥4 | 86.7 | 90.5 | 81.6 | 4.91 | 0.12 | 86.7 | 86.6 |
| ≥5 | 84.3 | 84.5 | 84.1 | 5.32 | 0.19 | 87.6 | 80.3 |
| ≥6 | 83.7 | 74.1 | 96.4 | 20.5 | 0.27 | 96.5 | 73.8 |
| ≥7 | 79.4 | 65.4 | 97.8 | 30.2 | 0.35 | 97.6 | 68.1 |
| BIDIAP Index cut-off value | PAA | NSAP | Total |
| ≥4 | 332 (TP) | 51 (FP) | 383 |
| <4 | 35 (FN) | 226 (TN) | 261 |
| Total | 367 | 277 | 644 |
Calibration of the BIDIAP Index
Decision Curve Analysis of the BIDIAP Index
Sensitivity Analyses
Discussion
Supplementary Materials
Financial Statement/Funding
Ethical Approval
Statement of Availability of the Data Used During the Study
Conflicts of Interest
References
- Waseem M, Wang CF. Pediatric appendicitis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jun 17 [Accessed 2025 Dec 29]. Available from: StatPearls Publishing. PMID: 28722894.
- Michelson KA, Reeves SD, Grubenhoff JA, Cruz AT, Chaudhari PP, Dart AH, Finkelstein JA, Bachur RG. Clinical Features and Preventability of Delayed Diagnosis of Pediatric Appendicitis. JAMA Netw Open. 2021 Aug 2;4(8):e2122248. PMID: 34463745; PMCID: PMC8408667. [CrossRef]
- Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986 May;15(5):557-64. PMID: 3963537. [CrossRef]
- Pogorelić Z, Rak S, Mrklić I, Jurić I. Prospective validation of Alvarado score and Pediatric Appendicitis Score for the diagnosis of acute appendicitis in children. Pediatr Emerg Care. 2015 Mar;31(3):164-8. PMID: 25706925. [CrossRef]
- Bai S, Hu S, Zhang Y, Guo S, Zhu R, Zeng J. The Value of the Alvarado Score for the Diagnosis of Acute Appendicitis in Children: A Systematic Review and Meta-Analysis. J Pediatr Surg. 2023 Oct;58(10):1886-1892. Epub 2023 Mar 6. PMID: 36966018. [CrossRef]
- Samuel M. Pediatric appendicitis score. J Pediatr Surg. 2002 Jun;37(6):877-81. PMID: 12037754. [CrossRef]
- Bhatt M, Joseph L, Ducharme FM, Dougherty G, McGillivray D. Prospective validation of the pediatric appendicitis score in a Canadian pediatric emergency department. Acad Emerg Med. 2009 Jul;16(7):591-6. Epub 2009 Jun 22. PMID: 19549016. [CrossRef]
- Kharbanda AB, Vazquez-Benitez G, Ballard DW, Vinson DR, Chettipally UK, Kene MV, Dehmer SP, Bachur RG, Dayan PS, Kuppermann N, O’Connor PJ, Kharbanda EO. Development and Validation of a Novel Pediatric Appendicitis Risk Calculator (pARC). Pediatrics. 2018 Apr;141(4):e20172699. Epub 2018 Mar 13. PMID: 29535251; PMCID: PMC5869337. [CrossRef]
- Cotton DM, Vinson DR, Vazquez-Benitez G, Margaret Warton E, Reed ME, Chettipally UK, Kene MV, Lin JS, Mark DG, Sax DR, McLachlan ID, Rauchwerger AS, Simon LE, Kharbanda AB, Kharbanda EO, Ballard DW; Clinical Research on Emergency Services and Treatments (CREST) Network. Validation of the Pediatric Appendicitis Risk Calculator (pARC) in a Community Emergency Department Setting. Ann Emerg Med. 2019 Oct;74(4):471-480. Epub 2019 Jun 19. PMID: 31229394; PMCID: PMC8364751. [CrossRef]
- Michelson KA, Bachur RG, Rangel SJ, Finkelstein JA, Monuteaux MC, Goyal MK. Disparities in Diagnostic Timeliness and Outcomes of Pediatric Appendicitis. JAMA Netw Open. 2024 Jan 2;7(1):e2353667. PMID: 38270955; PMCID: PMC10811560. [CrossRef]
- Arredondo Montero J, Bardají Pascual C, Antona G, Ros Briones R, López-Andrés N, Martín-Calvo N. The BIDIAP index: a clinical, analytical and ultrasonographic score for the diagnosis of acute appendicitis in children. Pediatr Surg Int. 2023 Apr 10;39(1):175. PMID: 37038002; PMCID: PMC10085908. [CrossRef]
- Cohen JF, Korevaar DA, Altman DG, Bruns DE, Gatsonis CA, Hooft L, Irwig L, Levine D, Reitsma JB, de Vet HC, Bossuyt PM. STARD 2015 guidelines for reporting diagnostic accuracy studies: explanation and elaboration. BMJ Open. 2016 Nov 14;6(11):e012799. PMID: 28137831; PMCID: PMC5128957. [CrossRef]
- Collins GS, Moons KGM, Dhiman P, Riley RD, Beam AL, Van Calster B, Ghassemi M, Liu X, Reitsma JB, van Smeden M, Boulesteix AL, Camaradou JC, Celi LA, Denaxas S, Denniston AK, Glocker B, Golub RM, Harvey H, Heinze G, Hoffman MM, Kengne AP, Lam E, Lee N, Loder EW, Maier-Hein L, Mateen BA, McCradden MD, Oakden-Rayner L, Ordish J, Parnell R, Rose S, Singh K, Wynants L, Logullo P. TRIPOD+AI statement: updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ. 2024 Apr 16;385:e078378. Erratum in: BMJ. 2024 Apr 18;385:q902. doi: 10.1136/bmj.q902. PMID: 38626948; PMCID: PMC11019967. [CrossRef]
- Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982 Apr;143(1):29-36. PMID: 7063747. [CrossRef]
- Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983 Sep;148(3):839-43. PMID: 6878708. [CrossRef]
- Vickers AJ, Elkin EB. Decision curve analysis: a novel method for evaluating prediction models. Med Decis Making. 2006 Nov-Dec;26(6):565-74. PMID: 17099194; PMCID: PMC2577036. [CrossRef]
- Mittal MK, Dayan PS, Macias CG, Bachur RG, Bennett J, Dudley NC, Bajaj L, Sinclair K, Stevenson MD, Kharbanda AB; Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. Performance of ultrasound in the diagnosis of appendicitis in children in a multicenter cohort. Acad Emerg Med. 2013 Jul;20(7):697-702. PMID: 23859583; PMCID: PMC5562364. [CrossRef]
- Balbo S, Pini CM, Raffaldi I, Delmonaco AG, Castagno E, Guanà R, Di Rosa G, Bondone C. Accuracy of point-of-care ultrasound in the diagnosis of acute appendicitis in a pediatric emergency department. J Clin Ultrasound. 2024 Jun;52(5):485-490. Epub 2024 Mar 4. PMID: 38436504. [CrossRef]
- Arredondo Montero J, Ros Briones R, Fernández-Celis A, López-Andrés N, Martín-Calvo N. Diagnostic Performance of Serum Leucine-Rich Alpha-2-Glycoprotein 1 in Pediatric Acute Appendicitis: A Prospective Validation Study. Biomedicines. 2024 Aug 11;12(8):1821. PMID: 39200285; PMCID: PMC11352011. [CrossRef]
- Chekmeyan M, Liu SH. Artificial intelligence for the diagnosis of pediatric appendicitis: A systematic review. Am J Emerg Med. 2025 Jun;92:18-31. Epub 2025 Feb 17. PMID: 40048888. [CrossRef]
- Pfeifer CM, Xie L, Atem FD, Mathew MS, Schiess DM, Messiah SE. Body mass index as a predictor of sonographic visualization of the pediatric appendix. Pediatr Radiol. 2022 Jan;52(1):42-49. Epub 2021 Sep 15. PMID: 34524472. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



